Embed Size (px)
Citation preview

Introduction to the Introduction to the profession. profession. Regeneration of bone Regeneration of bone tissuetissue

Cartilage--function, types, locationCartilage--function, types, location Bone Tissue--structure, typesBone Tissue--structure, types Long Bone Structure and Long Bone Structure and
DevelopmentDevelopment Most common bone problemsMost common bone problems
– FracturesFractures– OsteoporosisOsteoporosis
Cartilage and Cartilage and BoneBone

What is cartilage?What is cartilage?
Skeletal tissue--maintains certain Skeletal tissue--maintains certain shape and formshape and form
Very resilient (bouncy or Very resilient (bouncy or rubbery), mostly waterrubbery), mostly water
Grows fast--forms embryonic Grows fast--forms embryonic skeletonskeleton

Kinds of cartilageKinds of cartilage
Hyaline cartilage--most common, Hyaline cartilage--most common, found in jointsfound in joints
Elastic cartilage--epiglottis, earElastic cartilage--epiglottis, ear Fibrocartilage--annular fibrosis of Fibrocartilage--annular fibrosis of
intervertebral disk, menisci of intervertebral disk, menisci of kneeknee

M & MFigure 6.1

Bones provide:Bones provide: Support and movement (limbs, Support and movement (limbs,
axial skeleton)axial skeleton) Protection (skull bones)Protection (skull bones) Mineral storageMineral storage Blood cell development (long bone Blood cell development (long bone
marrow)marrow)
Bone is made up of:35% collagen, ground substance and cells65% calcium (hydroxyapetite)

Bone is alive!! Bone Bone is alive!! Bone cell types:cell types: Osteoblasts: Make and deposit Osteoblasts: Make and deposit
components of bone extracellular components of bone extracellular matrixmatrix
Osteoclasts: Degrade and resorb Osteoclasts: Degrade and resorb bone for remodelingbone for remodeling
Osteocytes: “watcher cells” Sit Osteocytes: “watcher cells” Sit in bone and monitor its current in bone and monitor its current statusstatus

Types of bony tissueTypes of bony tissue
Compact BoneCompact Bone– Dense tissue at Dense tissue at
surface of bonessurface of bones– Haversian canalsHaversian canals– Osteocytes in Osteocytes in
lacunae lacunae – Highly Highly
vascularizedvascularized– Fig. 6.6, p. 138Fig. 6.6, p. 138


Types of bony tissueTypes of bony tissue Trabecular (“spongy”) Trabecular (“spongy”)
bonebone– Trabeculae (oriented to Trabeculae (oriented to
give mechanical strength)give mechanical strength)– Interior of long bones, Interior of long bones,
skull bonesskull bones– Epiphyses of long bonesEpiphyses of long bones– Intramembranous Intramembranous
ossification (osteoblasts ossification (osteoblasts lay down bone around lay down bone around blood vessels in blood vessels in connective tissues of connective tissues of dermis (after 8 weeks of dermis (after 8 weeks of development)development)

Structure of a long Structure of a long bonebone
Diaphysis (shaft)Diaphysis (shaft) Epiphysis Epiphysis
– ProximalProximal– DistalDistal
Compact boneCompact bone Spongy boneSpongy bone PeriosteumPeriosteum Medullary cavityMedullary cavity Articular/hyaline Articular/hyaline
cartilagecartilage Epyphyseal (growth) Epyphyseal (growth)
platesplates
Fig. 6.3, p. 135


Bone Tissue within a Bone

Why do bones need to Why do bones need to “remodel?”“remodel?”

Endochondral Endochondral OssificationOssification
1.1. Cartilage modelCartilage model2.2. Bone collar forms in diaphysis (dense bone)Bone collar forms in diaphysis (dense bone)
Cartilage chondrocytes in center of diaphysis die and Cartilage chondrocytes in center of diaphysis die and cartilage disintegratescartilage disintegrates
3.3. Periosteal bud enters diaphysisPeriosteal bud enters diaphysisMakes spongy bone at ends of diaphysis (primary Makes spongy bone at ends of diaphysis (primary ossification center)ossification center)
4.4. Epiphysis begins to ossify (secondary ossification Epiphysis begins to ossify (secondary ossification center)center)
5.5. Hyaline cartilage remains only atHyaline cartilage remains only atEpiphyseal surfaces (articular surfaces of joints)Epiphyseal surfaces (articular surfaces of joints)Epiphyseal growth plates between diaphysis and epiphysis Epiphyseal growth plates between diaphysis and epiphysis (primary and secondary ossification centers on either side)(primary and secondary ossification centers on either side)
Fig. 6.9, p. 141



Endochondral Endochondral ossification ossification centers—centers—newly formed newly formed bone within bone within cartilage cartilage shown is shown is stained redstained red

Osteoclasts Osteoclasts OsteoblastsOsteoblasts ““Dig holes” with Dig holes” with
hydrochloric acidhydrochloric acid Degrades Degrades
calciumcalcium Phagocytize Phagocytize
collagen fibers collagen fibers and dead and dead osteocytesosteocytes
Line tubes Line tubes (Haversian canals) (Haversian canals) left by osteoclastsleft by osteoclasts
Lay down new Lay down new bone in circular bone in circular concentric concentric lamellaelamellae
Unique to warm-Unique to warm-blooded animals--blooded animals--dinosaurs???dinosaurs???

Bone FracturesBone Fractures
Treatment is reductionTreatment is reduction– Closed--set in place by physical Closed--set in place by physical
manipulation from outside bodymanipulation from outside body– Open--surgical placement of pins or screwsOpen--surgical placement of pins or screws
HealingHealing– HematomaHematoma– Fibrocartilaginous callusFibrocartilaginous callus– Bony calllusBony calllus– Remodeling by osteoclasts/osteoblastsRemodeling by osteoclasts/osteoblasts
Types of FracturesTypes of Fractures




Fracture repairFracture repair

Calcium Calcium regulatioregulation is n is negative negative feedback feedback mechanimechanismsm

OsteoporosisOsteoporosis
Affects elderly, especially womenAffects elderly, especially women Bone resorption proceeds faster than Bone resorption proceeds faster than
depositiondeposition Low estrogen levels implicated but Low estrogen levels implicated but
estrogen replacement now considered estrogen replacement now considered riskyrisky
Importance of calcium in diet???Importance of calcium in diet??? Leads to fracturesLeads to fractures
– Compression fractures of vertebraeCompression fractures of vertebrae– Neck of femurNeck of femur

Bone grafts and Bone grafts and artificial boneartificial bone Widely used cutting-edge technologiesWidely used cutting-edge technologies Bone cells highly regenerative and move Bone cells highly regenerative and move
into any suitable matrixinto any suitable matrix– Use bone pieces from same body—fibulaUse bone pieces from same body—fibula– Use crushed bone from cadaversUse crushed bone from cadavers– Use bone substitutes—coral, syntheticsUse bone substitutes—coral, synthetics
—”nanotechnology”—”nanotechnology” Applications are numerousApplications are numerous
– Jaw bone filler for dental workJaw bone filler for dental work– Birth defectsBirth defects– OsteoporosisOsteoporosis– Bone repairBone repair

IntroductionIntroduction
Approximately 5% of all long Approximately 5% of all long bone fractures will result in bone fractures will result in nonunions and even more in nonunions and even more in delayed unionsdelayed unions

Delayed UnionDelayed Union
The exact time when a given fracture The exact time when a given fracture should be united cannot be definedshould be united cannot be defined
Union is delayed when healing has not Union is delayed when healing has not advanced at the average rate for the advanced at the average rate for the location and type of fracture (Btn 3-6 location and type of fracture (Btn 3-6 mths)mths)
Treatment usually is by an efficient cast Treatment usually is by an efficient cast that allows as much function as possible that allows as much function as possible can be continued for 4 to 12 additional can be continued for 4 to 12 additional weeksweeks

Delayed Union Delayed Union cont.cont.
If still nonunited a decision should be If still nonunited a decision should be made to treat the fracture as nonunionmade to treat the fracture as nonunion
External ultrasound or electrical External ultrasound or electrical stimulation may be consideredstimulation may be considered
Surgical treatment should be carried out Surgical treatment should be carried out to remove interposed soft tissues and to to remove interposed soft tissues and to oppose widely separated fragments oppose widely separated fragments
Iliac grafts should be used if plates and Iliac grafts should be used if plates and screws are placed but grafts are not screws are placed but grafts are not usually needed when using usually needed when using intramedullary nailing, unless reduction intramedullary nailing, unless reduction is done openis done open

NonunionNonunion
FDA defined nonunion as FDA defined nonunion as “established when a minimum of 9 “established when a minimum of 9 months has elapsed since fracture months has elapsed since fracture with no visible progressive signs of with no visible progressive signs of healing for 3 months”healing for 3 months”
Every fracture has its own timetable Every fracture has its own timetable (ie long bone shaft fracture 6 (ie long bone shaft fracture 6 months, femoral neck fracture 3 months, femoral neck fracture 3 months) months)

Delayed/NonunionDelayed/Nonunion
Factors contributing to Factors contributing to development:development:
SystemicSystemic LocalLocal

Delayed/Nonunion Delayed/Nonunion cont.cont.
Systemic factors:Systemic factors: MetabolicMetabolic Nutritional statusNutritional status General healthGeneral health Activity levelActivity level Tobacco and alcohol useTobacco and alcohol use

Delayed/Nonunion Delayed/Nonunion cont.cont.
Local factorsLocal factors OpenOpen InfectedInfected Segmental (impaired blood supply)Segmental (impaired blood supply) ComminutedComminuted Insecurely fixedInsecurely fixed Immobilized for an insufficient timeImmobilized for an insufficient time Treated by ill-advised open reductionTreated by ill-advised open reduction Distracted by (traction/plate and screws)Distracted by (traction/plate and screws) Irradiated boneIrradiated bone Delayed weight-bearing > 6 weeksDelayed weight-bearing > 6 weeks Soft tissue injury > method of initial treatmentSoft tissue injury > method of initial treatment

Nonunion Nonunion cont.cont.
Nonunited fractures form two types Nonunited fractures form two types of pseudoarthrosis:of pseudoarthrosis:
Hypervascular or hypertrophicHypervascular or hypertrophic Avascular or atrophicAvascular or atrophic

Nonunion Nonunion cont.cont.
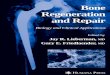
Hypervascular or Hypervascular or Hypertrophic:Hypertrophic:
1.1. Elephant foot Elephant foot (hypertophic, rich in (hypertophic, rich in callus)callus)
2.2. Horse foot (mildly Horse foot (mildly hypertophic, poor in hypertophic, poor in callus)callus)
3.3. Oligotrophic (not Oligotrophic (not hypertrophic, no hypertrophic, no callus)callus)
Hypervascular nonunions. Hypervascular nonunions. A,A, "Elephant "Elephant foot" nonunion. foot" nonunion. B,B, "Horse hoof" "Horse hoof" nonunion. nonunion. C,C, Oligotrophic nonunion (see Oligotrophic nonunion (see text). (Redrawn from Weber BG, Cech O, text). (Redrawn from Weber BG, Cech O, eds: eds: PseudarthrosisPseudarthrosis, Bern, Switzerland, , Bern, Switzerland, 1976, Hans Huber.) 1976, Hans Huber.)

Nonunion Nonunion cont.cont.
Avascular or AtrophicAvascular or Atrophic Torsion wedge Torsion wedge
(intermediate fragment)(intermediate fragment) Comminuted (necrotic Comminuted (necrotic
intermediate fragment)intermediate fragment) Defect (loss of fragment Defect (loss of fragment
of the diaphysis)of the diaphysis) Atrophic (scar tissue Atrophic (scar tissue
with no osteogenic with no osteogenic potential is replacing potential is replacing the missing fragment)the missing fragment) Avascular nonunions. Avascular nonunions. A,A, Torsion Torsion
wedge nonunion. wedge nonunion. B,B, Comminuted Comminuted nonunion. nonunion. C,C, Defect nonunion. Defect nonunion. D,D, Atrophic nonunion (see text). Atrophic nonunion (see text). (Redrawn from Weber BG, Cech O, (Redrawn from Weber BG, Cech O, eds: eds: PseudarthrosisPseudarthrosis, Bern, , Bern, Switzerland, 1976, Hans Huber.) Switzerland, 1976, Hans Huber.)

Nonunion Nonunion cont.cont.
Classification (Paley et al)Classification (Paley et al) Type A<2cm of bone lossType A<2cm of bone loss A1 (Mobile deformity)A1 (Mobile deformity) A2 (fixed deformity)A2 (fixed deformity) A2-1 stiff w/o A2-1 stiff w/o
deformitydeformity A2-2 stiff w/ fixed A2-2 stiff w/ fixed
deformitydeformity Type B>2cm of bone lossType B>2cm of bone loss B1 w/ bony defectB1 w/ bony defect B2 loss of bone lengthB2 loss of bone length B3 bothB3 both A,A, Type A nonunions (less than 1 cm of bone loss): Type A nonunions (less than 1 cm of bone loss): A1A1, lax (mobile); , lax (mobile);
A2A2, stiff (nonmobile) (not shown); , stiff (nonmobile) (not shown); A2-1A2-1, no deformity; , no deformity; A2-2A2-2, fixed , fixed deformity. deformity. B,B, Type B nonunions (more than 1 cm of bone loss): Type B nonunions (more than 1 cm of bone loss): B1B1, , bony defect, no shortening; bony defect, no shortening; B2B2, shortening, no bony defect; , shortening, no bony defect; B3B3, , bony defect and shortening. bony defect and shortening.


Nonunion Nonunion cont.cont.
Treatment:Treatment:1.1. ElecricalElecrical2.2. ElectromagnaticElectromagnatic3.3. UlrasoundUlrasound4.4. External fixation (ie deformity, infection, External fixation (ie deformity, infection,
bone loss)bone loss)5.5. SurgicalSurgical
Hypertrophic: stable fixation of fragmentsHypertrophic: stable fixation of fragments Atrophic: decortication and bone graftingAtrophic: decortication and bone grafting According to classification:According to classification: type A : restoration of alignment, compressiontype A : restoration of alignment, compression type B : cortical osteotomy, bone transport or type B : cortical osteotomy, bone transport or
lengthening lengthening

Nonunion Nonunion cont.cont.
Surgical guidelines:Surgical guidelines: Good reductionGood reduction Bone graftingBone grafting Firm stabilizationFirm stabilization

Nonunion Nonunion cont.cont.
Reduction of the fragments:Reduction of the fragments: Extensive dissection is Extensive dissection is
undesirable, leaving periosteum, undesirable, leaving periosteum, callus, and fibrous tissue to callus, and fibrous tissue to preserve vascularity and stability, preserve vascularity and stability, resecting only the scar tissue and resecting only the scar tissue and the rounded ends of the bonesthe rounded ends of the bones
External fixator, Intramedullary External fixator, Intramedullary nailing, Ilizarov framenailing, Ilizarov frame

Nonunion Nonunion cont.cont.
Bone Grafting origins:Bone Grafting origins: Autogenous “the golden Autogenous “the golden
standard”standard” AllograftAllograft Synthetic substituteSynthetic substitute

Nonunion Nonunion cont.cont.
Bone grafting techniques:Bone grafting techniques: OnlayOnlay Dual onlayDual onlay Cancellous insertCancellous insert Massive sliding graftMassive sliding graft Whole fibular transplantWhole fibular transplant Vascularized free fibular graftVascularized free fibular graft Intamedullary fibular graftIntamedullary fibular graft

Dual onlayDual onlay
Nonunion of tibial Nonunion of tibial shaft treated by shaft treated by dual onlay grafts dual onlay grafts

Massive sliding graftMassive sliding graft
Gill massive sliding graft Gill massive sliding graft

Whole fibular Whole fibular transplanttransplant Bridging of bone Bridging of bone
defect with whole defect with whole fibular transplant. fibular transplant. A,A, Defect in radius Defect in radius was caused by was caused by shotgun wound. shotgun wound. BB and and C,C, Ten months Ten months after defect was after defect was spanned by whole spanned by whole fibular transplant, fibular transplant, patient had 25% patient had 25% range of motion in range of motion in wrist, 50% wrist, 50% pronation and pronation and supination, and supination, and 80% use of fingers. 80% use of fingers.

Vascularized free Vascularized free fibular graftfibular graft Posteroanterior Posteroanterior
and lateral and lateral roentgenogramroentgenograms made 3 years s made 3 years after fibular after fibular transfer, transfer, showing showing excellent excellent remodeling remodeling with fracture with fracture healing. (From healing. (From Duffy GP, Duffy GP, Wood MB, Rock Wood MB, Rock MG, Sim FH: MG, Sim FH: J J Bone Joint Surg Bone Joint Surg 82A:544, 82A:544, 2000.) 2000.)

Intamedullary fibular Intamedullary fibular graftgraft Anteroposterior Anteroposterior
roentgenogram of roentgenogram of humerus 5 months humerus 5 months after insertion of after insertion of fibular allograft and fibular allograft and compression plating compression plating with a 4.5-mm with a 4.5-mm dynamic compression dynamic compression plate revealing plate revealing evidence of bridging evidence of bridging callus formation and callus formation and incorporation of the incorporation of the allograft. (From allograft. (From Crosby LA, Norris BL, Crosby LA, Norris BL, Dao KD, McGuire MH: Dao KD, McGuire MH: Am J Orthop Am J Orthop 29:45, 29:45, 2000.) 2000.)

Nonunion Nonunion cont.cont.
Stabilization of bone fragments:Stabilization of bone fragments: Internal fixation (hypertrophic #): Internal fixation (hypertrophic #):
intamedullary, or plates and intamedullary, or plates and screwsscrews
External fixation(defects External fixation(defects associated#):associated#):
ie Ilizarovie Ilizarov

Internal fixationInternal fixation
Roentgenograms Roentgenograms of patient with of patient with subtrochanteric subtrochanteric nonunion for 22 nonunion for 22 years treated with years treated with locked second locked second generation generation femoral nail. femoral nail. A,A, Preoperatively. Preoperatively. B,B, Postoperatively. Postoperatively.

IlizarovIlizarov
Bifocal osteosynthesis with Bifocal osteosynthesis with Ilizarov fixator after debridement Ilizarov fixator after debridement of necrotic segments, as of necrotic segments, as recommended by Catagni. recommended by Catagni.
Monofocal osteosynthesis with Ilizarov Monofocal osteosynthesis with Ilizarov fixator for hypertrophic nonunions with fixator for hypertrophic nonunions with minimal infection, as recommended by minimal infection, as recommended by
CatagniCatagni

Ilizarov Ilizarov cont.cont.
Type IIIB open tibial fracture in 30-year-old man struck by automobile. Initial treatment was Type IIIB open tibial fracture in 30-year-old man struck by automobile. Initial treatment was
with four-pin anterior half-pin external fixator that was later converted to six-pin fixator; with four-pin anterior half-pin external fixator that was later converted to six-pin fixator; this fixator was removed because of persistent infection. this fixator was removed because of persistent infection. B,B, One year after injury, infected One year after injury, infected nonunion with deformity. nonunion with deformity. C,C, Shape of tibial deformity is duplicated by Ilizarov frame and is Shape of tibial deformity is duplicated by Ilizarov frame and is gradually corrected as nonunion is compressed. gradually corrected as nonunion is compressed. D,D, Union obtained at 4½ months. Union obtained at 4½ months.

Nonunion Nonunion cont.cont.
Factors complicating nonunionFactors complicating nonunion InfectionInfection Poor tissue qualityPoor tissue quality Short periarticular fragmentsShort periarticular fragments Significant deformity Significant deformity

Infection managementInfection management
Treatment of nonunion of tibia in which sequestration or gross infection is present. Treatment of nonunion of tibia in which sequestration or gross infection is present. A,A, Bone is approached anteriorly and is saucerized, incision is closed, and infection is Bone is approached anteriorly and is saucerized, incision is closed, and infection is treated with antibiotics by irrigation and suction. treated with antibiotics by irrigation and suction. BB and and C,C, Tibia is grafted posteriorly. Tibia is grafted posteriorly. B,B, Skin incision. Skin incision. C,C, Tibia and fibula have both been approached posterolaterally. Tibia and fibula have both been approached posterolaterally. Posterior aspect of tibia (or tibia and fibula) is roughened and grafted with autogenous Posterior aspect of tibia (or tibia and fibula) is roughened and grafted with autogenous iliac boneiliac bone


Nonunion Nonunion cont.cont.
Specific Bones Management:Specific Bones Management: MetatarsalsMetatarsals TibiaTibia FibulaFibula PatellaPatella FemurFemur Pelvis and acetabulumPelvis and acetabulum ClavicleClavicle HumerusHumerus RadiusRadius UlnaUlna

TibiaTibia
Medial MalleolusMedial Malleolus One month after One month after
intraosseous graft for intraosseous graft for nonunion of fracture of nonunion of fracture of medial malleolus. medial malleolus. B,B, Failure of grafting Failure of grafting procedure. Medial procedure. Medial malleolus was resected. malleolus was resected. C,C, Seven years after Seven years after resection, ankle is resection, ankle is stable, although mild stable, although mild arthritic changes are arthritic changes are becoming evident. This becoming evident. This is maximal amount of is maximal amount of medial malleolus that medial malleolus that can be removed if can be removed if stability of ankle is to be stability of ankle is to be preserved. preserved.

Tibia Tibia cont.cont.
Technique for grafting nonunion of medial malleolus Technique for grafting nonunion of medial malleolus

Tibia Tibia cont.cont.
Medial malleolus Sliding graftMedial malleolus Sliding graft

Tibia Tibia cont.cont.
T.Shaft A,T.Shaft A, Nonunion after osteotomy. Nonunion after osteotomy. Failure to produce union by sliding inlay Failure to produce union by sliding inlay graft; fibula is intact. graft; fibula is intact. BB, Four years after , Four years after application of dual onlay grafts and application of dual onlay grafts and osteotomy of fibula. Note that fibula overlaps osteotomy of fibula. Note that fibula overlaps

Tibia Tibia cont.cont.
Oblique comminuted fracture of proximal third of tibia with Oblique comminuted fracture of proximal third of tibia with fracture of tibial plateau. fracture of tibial plateau. B,B, Satisfactory restoration of fragments. Satisfactory restoration of fragments. C,C, Fracture of shaft failed to unite; treated by dual onlay graft. Fracture of shaft failed to unite; treated by dual onlay graft.

Tibia Tibia cont.cont.
Patient with open tibial fracture treated initially with Patient with open tibial fracture treated initially with unreamed nailing. unreamed nailing. A,A, Broken distal screw indicated Broken distal screw indicated nonunion despite dynamization. nonunion despite dynamization. B,B, Union achieved Union achieved
after exchanging nailafter exchanging nail

Femur Femur (supracondylar)(supracondylar)
Deformity and nonunion 7 years after supracondylar Deformity and nonunion 7 years after supracondylar femoral fracture in 35-year-old woman; knee joint is femoral fracture in 35-year-old woman; knee joint is ankylosed. ankylosed. BB and and C,C, Application of Ilizarov external Application of Ilizarov external fixator for correction of length and offset deformity. fixator for correction of length and offset deformity. DD and and E,E, Union at 10 months. Union at 10 months.

Femoral shaftFemoral shaft
AA and and B,B, Femoral defect in 16-year-old boy; type IIIB injury was Femoral defect in 16-year-old boy; type IIIB injury was sustained in hunting accident. sustained in hunting accident. CC and and D,D, Six months after medullary Six months after medullary bone graft and fixation with static-locked, unreamed, intramedullary bone graft and fixation with static-locked, unreamed, intramedullary nailing nailing

ClavicleClavicle
Hypervascular nonunion of clavicle. Hypervascular nonunion of clavicle. A,A, Appearance 1½ Appearance 1½ years after fracture. Nonunion painful after recent fall. years after fracture. Nonunion painful after recent fall. B,B, Solid union 2½ months after compression plating Solid union 2½ months after compression plating and bone grafting and bone grafting

HumerusHumerus
Combination tension band and buttress plate technique for nonunion of proximal Combination tension band and buttress plate technique for nonunion of proximal
humerus, as described by Healy, Jupiter, Kristiansen, and White. Heavy nonabsorbable humerus, as described by Healy, Jupiter, Kristiansen, and White. Heavy nonabsorbable suture is woven through rotator cuff using Krackow stitch and is fixed to T-plate to reduce suture is woven through rotator cuff using Krackow stitch and is fixed to T-plate to reduce pull of rotator cuff on proximal fragment and avoid pullout of proximal metaphyseal screws pull of rotator cuff on proximal fragment and avoid pullout of proximal metaphyseal screws

HumerusHumerus
Ununited fracture-dislocation with fracture at anatomical neck of humerus. Ununited fracture-dislocation with fracture at anatomical neck of humerus. A,A, Appearance on admission; four-part fracture with dislocation. Appearance on admission; four-part fracture with dislocation. B,B, Solid union 6 Solid union 6 months after fixation with Neer I prosthesis. Function was satisfactory. months after fixation with Neer I prosthesis. Function was satisfactory.

Humeral shaftHumeral shaft
Nonunion of middle third of humeral shaft. Nonunion of middle third of humeral shaft. A,A, Nonunion with Nonunion with angulation and osteoporosis. angulation and osteoporosis. B,B, Solid union 5 months after open Solid union 5 months after open reduction, fixation with nine-hole compression plate, and application reduction, fixation with nine-hole compression plate, and application
of iliac bone grafts.of iliac bone grafts.

Humeral shaftHumeral shaft
Humeral nonunion. Humeral nonunion. B,B, After fixation with After fixation with
intramedullary nail.intramedullary nail.

Humerus Humerus cont.cont.
Large defect in distal metaphysis of humerus after open fracture with Large defect in distal metaphysis of humerus after open fracture with separation of large segment of bone. separation of large segment of bone. B,B, Twenty months after bridging of Twenty months after bridging of defect by whole fibular transplant. Cancellous bone was used to bridge defect by whole fibular transplant. Cancellous bone was used to bridge expanded portion of metaphysis and shaft. expanded portion of metaphysis and shaft.

Humeral condyleHumeral condyle
Old fracture of lateral condyle of humerus in childhood. Marked cubitus Old fracture of lateral condyle of humerus in childhood. Marked cubitus valgus and nonunion are present. valgus and nonunion are present. B,B, Immediately after reconstruction. Immediately after reconstruction. C,C, Twelve months later normal range of flexion and extension is restored, with Twelve months later normal range of flexion and extension is restored, with normal carrying angle, 50% supination and pronation, and fair stability normal carrying angle, 50% supination and pronation, and fair stability despite degenerative changes. despite degenerative changes.

Monteggia’sMonteggia’s
Nonunion of ulna after radial head excision. Proximal ulnar Nonunion of ulna after radial head excision. Proximal ulnar fracture treated with locked forearm nail and tricortical iliac fracture treated with locked forearm nail and tricortical iliac
crest bone graftcrest bone graft