Embed Size (px)
Citation preview
1
Chen Lugaccy-Waismann 5th Course, group 13
INTRUSION OF MAXILLARY INCISORS BY MINI-
IMPLANTS
A systematic review
Supervisor
PhD, Arūnas Vasiliauskas
Kaunas, 2018

2
LITHUANIAN UNIVERSITY OF HEALTH SCIENCES
MEDICAL ACADEMY
FACULTY OF ODONTOLOGY
THE CLINIC OF ORTHODONTICS
INTRUSION OF MAXILLARY INCISORS BY MINI-IMPLANTS
A systematic review
The thesis was done
by student …………………………... supervisor ……………………... (name surname, year, group) (degree, name surname)
……………………………………….. ……………………………………
(signature) (signature)
……………………… 20…. ……………………… 20….
(day/month) (day/month)
Kaunas, 2018
3
EVALUATION TABLE OF THE MASTER’S THESIS OF THE TYPE
OF SYSTEMIC REVIEW OF SCIENTIFIC LITERATURE
Evaluation:
…………………………………………………………………………………
Reviewer:
………………………………………………………………………………
(scientific degree. name and surname)
Reviewing date: ...........................................
No.
MT parts
MT evaluation aspects
Compliance with MT
requirements and
evaluation
Yes Partially No
1
Summary (0.5
point)
Is summary informative and in compliance with the
thesis content and requirements? 0.3 0.1 0
2 Are keywords in compliance with the thesis
essence? 0.2 0.1 0
3 Introduction, aim
and tasks (1
point)
Are the novelty, relevance and significance of the
work justified in the introduction of the thesis? 0.4 0.2 0
4 Are the problem, hypothesis, aim and tasks formed
clearly and properly? 0.4 0.2 0
5 Are the aim and tasks interrelated? 0.2 0.1 0
6 Selection criteria of
the studies, search
methods and
strategy
(3.4 points)
Is the protocol of systemic review present? 0.6 0.3 0
7
Were the eligibility criteria of articles for the
selected protocol determined (e.g., year, language,
publication condition, etc.)
0.4
0.2
0
8
Are all the information sources (databases with dates
of coverage, contact with study authors to identify
additional studies) described and are the last search
day indicated?
0.2
0.1
0
9
Is the electronic search strategy described in such a
way that it could be repeated (year of search, the last
search day; keywords and their combinations;
number of found and selected articles according to
the combinations of keywords)?
0.4
0.1
0
10
Is the selection process of studies (screening,
eligibility, included in systemic review or, if
applicable, included in the meta-analysis)
described?
0.4
0.2
0
4
11
Is the data extraction method from the articles (types
of investigations, participants, interventions,
analyzed factors, indexes) described?
0.4
0.2
0
12
Are all the variables (for which data were sought and
any assumptions and simplifications made) listed
and defined?
0.4
0.2
0
13
Are the methods, which were used to evaluate the
risk of bias of individual studies and how this
information is to be used in data synthesis,
described?
0.2
0.1
0
14 Were the principal summary measures (risk ratio,
difference in means) stated? 0.4 0.2 0
15
Systemization
and analysis of
data
(2.2 points)
Is the number of studies screened: included upon
assessment for eligibility and excluded upon giving
the reasons in each stage of exclusion presented?
0.6
0.3
0
16
Are the characteristics of studies presented in the
included articles, according to which the data were
extracted (e.g., study size, follow-up period, type of
respondents) presented?
0.6
0.3
0
17
Are the evaluations of beneficial or harmful
outcomes for each study presented? (a) simple
summary data for each intervention group; b) effect
estimates and confidence intervals)
0.4
0.2
0
18
Are the extracted and systemized data from studies
presented in the tables according to individual
tasks?
0.6
0.3
0
19
Discussion (1.4
points)
Are the main findings summarized and is their
relevance indicated? 0.4 0.2 0
20 Are the limitations of the performed systemic
review discussed? 0.4 0.2 0
21 Does author
results?
present the interpretation of the 0.4 0.2 0
22
Conclusions (0.5
points)
Do the conclusions reflect the topic, aim and tasks
of the Master’s thesis? 0.2 0.1 0
23 Are the conclusions based on the analysed material? 0.2 0.1 0
24 Are the conclusions clear and laconic? 0.1 0.1 0
25
Is the references list formed according to the
requirements? 0.4 0.2 0
5
26
References (1
point)
Are the links of the references to the text correct?
Are the literature sources cited correctly and
precisely?
0.2
0.1
0
27 Is the scientific level of references suitable for
Master’s thesis? 0.2 0.1 0
28
Do the cited sources not older than 10 years old
form at least 70% of sources, and the not older than
5 years – at least 40%?
0.2
0.1
0
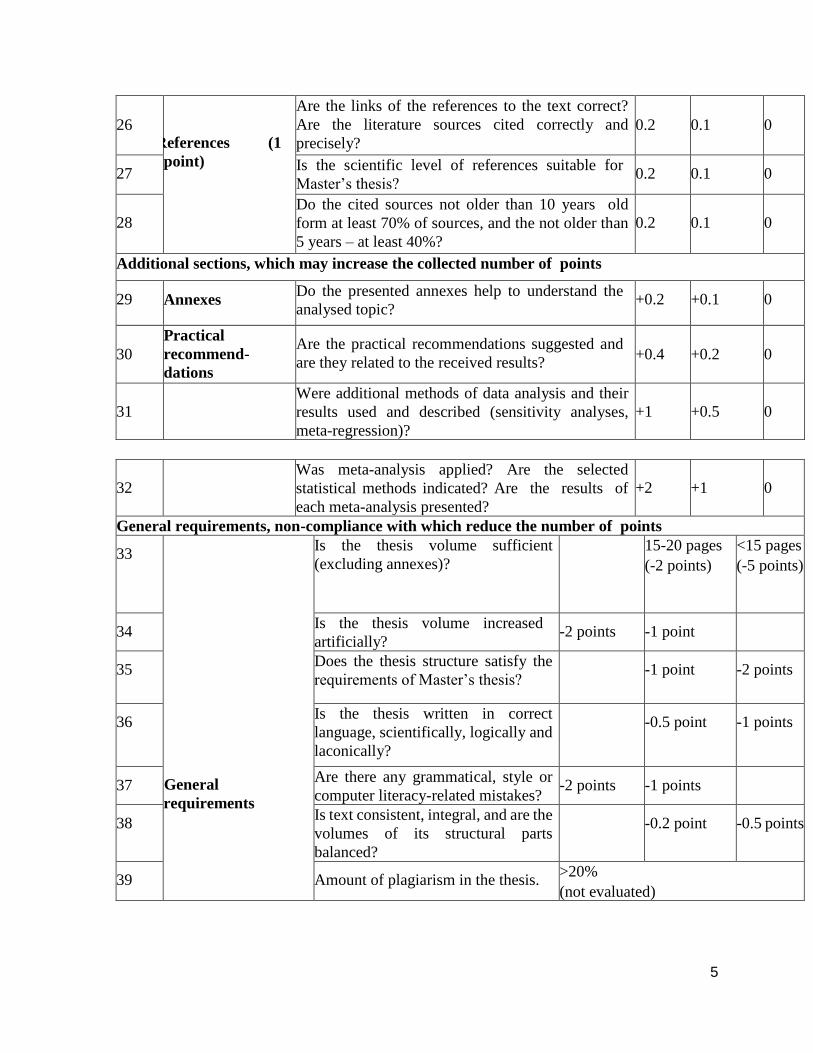
Additional sections, which may increase the collected number of points
29 Annexes Do the presented annexes help to understand the
analysed topic? +0.2 +0.1 0
30
Practical
recommend-
dations
Are the practical recommendations suggested and
are they related to the received results?
+0.4
+0.2
0
31
Were additional methods of data analysis and their
results used and described (sensitivity analyses,
meta-regression)?
+1
+0.5
0
32
Was meta-analysis applied? Are the selected
statistical methods indicated? Are the results of
each meta-analysis presented?
+2
+1
0
General requirements, non-compliance with which reduce the number of points
33
General
requirements
Is the thesis volume sufficient
(excluding annexes)?
15-20 pages
(-2 points)
<15 pages
(-5 points)
34 Is the thesis volume increased
artificially? -2 points -1 point
35 Does the thesis structure satisfy the
requirements of Master’s thesis?
-1 point -2 points
36 Is the thesis written in correct
language, scientifically, logically and
laconically?
-0.5 point -1 points
37 Are there any grammatical, style or
computer literacy-related mistakes? -2 points -1 points
38 Is text consistent, integral, and are the
volumes of its structural parts
balanced?
-0.2 point -0.5 points
39 Amount of plagiarism in the thesis. >20%
(not evaluated)
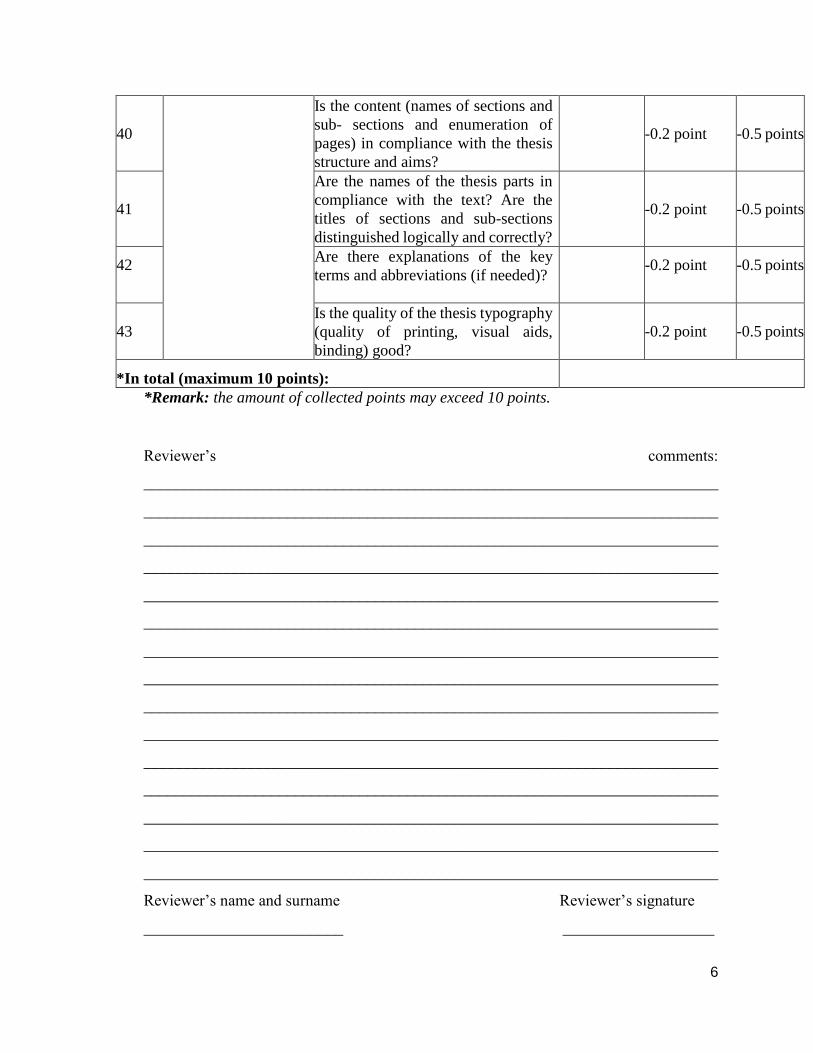
6
40
Is the content (names of sections and
sub- sections and enumeration of
pages) in compliance with the thesis
structure and aims?
-0.2 point
-0.5 points
41
Are the names of the thesis parts in
compliance with the text? Are the
titles of sections and sub-sections
distinguished logically and correctly?
-0.2 point
-0.5 points
42 Are there explanations of the key
terms and abbreviations (if needed)?
-0.2 point -0.5 points
43
Is the quality of the thesis typography
(quality of printing, visual aids,
binding) good?
-0.2 point
-0.5 points
*In total (maximum 10 points):
*Remark: the amount of collected points may exceed 10 points.
Reviewer’s comments:
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
________________________________________________________________________
Reviewer’s name and surname Reviewer’s signature
_________________________ ___________________
7
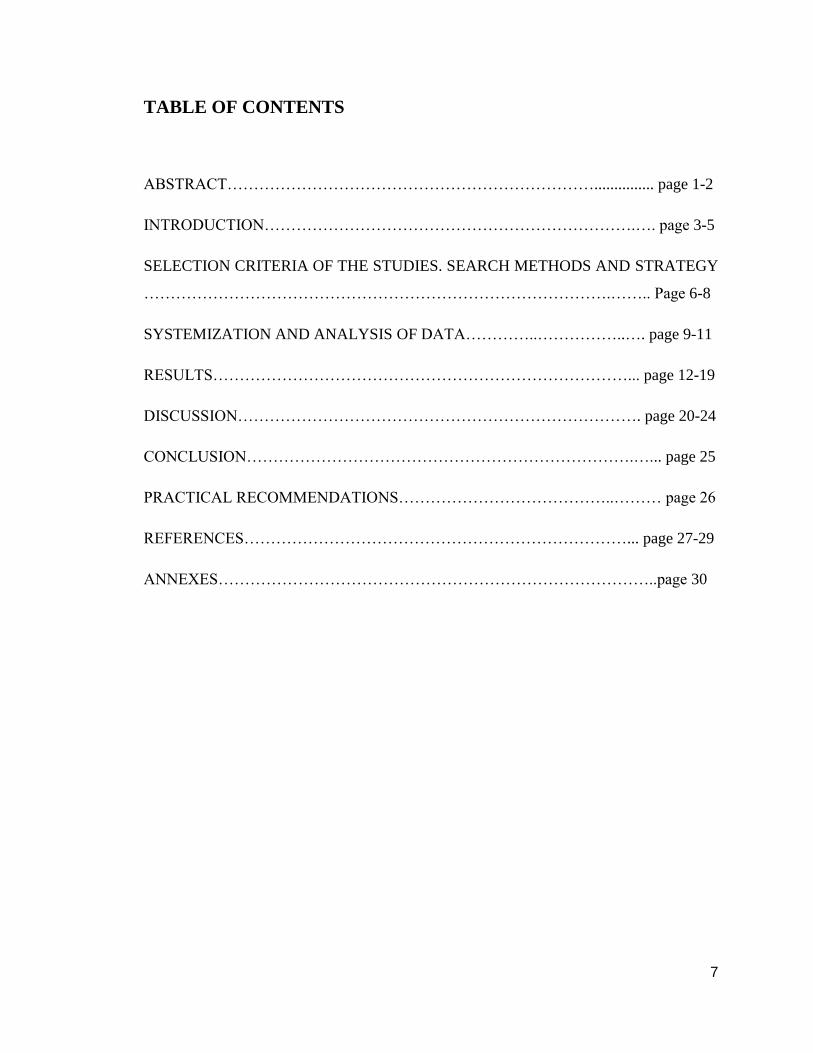
TABLE OF CONTENTS
ABSTRACT……………………………………………………………............... page 1-2
INTRODUCTION…………………………………………………………….…. page 3-5
SELECTION CRITERIA OF THE STUDIES. SEARCH METHODS AND STRATEGY
…………………………………………………………………………….…….. Page 6-8
SYSTEMIZATION AND ANALYSIS OF DATA…………..……………..…. page 9-11
RESULTS……………………………………………………………………... page 12-19
DISCUSSION…………………………………………………………………. page 20-24
CONCLUSION……………………………………………………………….…... page 25
PRACTICAL RECOMMENDATIONS…………………………………..……… page 26
REFERENCES………………………………………………………………... page 27-29
ANNEXES………………………………………………………………………..page 30

1
ABSTRACT
Objectives: The purpose of this systematic literature review is to evaluate the effects of
different insertion sites of mini-implants / TAD’s (temporary anchorage device) on the
treatment of deep overbite and/or gummy smile with maxillary incisors intrusion.
Material and methods: In this systematic review search performed of the published
data in several electronic databases included PubMed, Science Direct, Cochrane and other
sources as AJO-DO and European journal of orthodontics up to January 2017.
Inclusion criteria were: English language, only humans, articles published from January
1st, 2008 till 5th of January 2018, patients with deep overbite and/or gummy smile treated
with maxillary incisors intrusion by using temporary anchorage device and studies that
present records of pretreatment and posttreatment. Study selection, risk of bias assessment,
and data-extraction were performed.
Results: In total 297 scientific publications, articles, clinical trials reviews were identified
and were related to keywords used during the search. Out of the 34 articles that met the
initial eligibility criteria, 8 studies were finally selected. Low to moderate level of scientific
evidence was identified after risk of bias assessment on the included studies with no
relevant randomized controlled trial performed. In the final included studies, five mini
implants insertion sites possibilities used for maxillary incisors intrusion were presented
and a comparison between them was made. There were differences in the outcomes and
results. Treatment duration vary from four months to more than a year. Minimum force
applied on each mini implant was 40g while maximum force applied was 90g.
The highest result of total intrusion was 5.62mm, which was achieved by one mini implant
located 4mm superior to the free gingival margin between the central incisors, and the
lowest result of total intrusion was 1.56mm seen in the use of 2 mini implants inserted
between the second premolar and first molar. Some studies reported on no failure while
others reported on 6.25% to 14.3% of mini implants lost.
Conclusions: The decision regarding the insertion site of the mini-implants has an
2
important role when intrusion of 4 maxillary incisors are considered, it substantially affects
the mean of total intrusion, the treatment duration need, and the force required to apply on
each mini-implants.
In addition, by this systematic review we can conclude that the best results and outcomes
achieved when one mini-implant was inserted between the maxillary central incisors
Keywords: Maxillary incisors intrusion, mini implant, mini screw, TAD, SAD.

3
INTRODUCTION
Marcotte explained intrusion as an apical movement of the tooth which at infinity lies its
center of rotation. It is an axial type of translation [1]. Burstone roughly explained intrusion
as a movement based on the long axis of the apical tooth, or a geometric one with respect
to the occlusal plane [2].
Nikolai’s description for intrusion was that it is an apical movement paralleled to the long
axis of the tooth which is the tooth’s transitional form of movement [3].
An intrusion may be relative or true, and a tooth’s movement apically, along its long axis
is a true one. An intrusion that has the incisors remain on their place while there is a growth
of mandible and an eruption of the posterior teeth- is relative intrusion [4].
This systematic review will focus on true intrusion only. Intrusion is a common treatment
used in orthodontic management of Esthetic and functional problems, inclusive deep
overbite and gummy smile [5]. Deep overbite phenomenon can be described as a
substantial overlap by the incisors of the maxilla over the incisors of the mandible when
the mandible is at central occlusion or at habitual occlusion. [6]
The main reason to treat deep bite and/or gummy smile conditions by intrusion of maxillary
incisors is esthetic improvement, but there are some harmful effects such as: incisor wear,
palatal impingement, gingival recession [6], that can heal efficiently by treating the
beforementioned conditions with true intrusion of maxillary incisors.
In the past, dental intrusion was considered problematic or impossible and was associated
with side effects affecting the cementum and the periodontium, such as root resorption.
However, at present time, orthodontic intrusion is clinically documented as successful and
regarded to as safe [5] .
4
Before mini-implants (MI) or temporary anchorage device (TAD’s) were invented,
orthodontics primarily used other techniques for maxillary incisors intrusion, such as:
Rickett’s utility arch, Kalra's Simultaneous Intrusion & Retraction arch, Arch with Reverse
Curve of Spee and Cervical headgear and lever arches. [6-7]. A research that investigated
the differences between the intrusive effects of mini-implants to utility arches technique
established that: “mini-implant in contrast to others, produce true intrusion without any
other side effects” [8]. Another research showed that the amount of intrusion is
significantly higher in the group which was treated by mini-implant, had overall better
results and was easier in handling during intrusion. [9]
Thus, the treatment for gummy smile or anterior deep overbite by mini-implants in the
maxillary anterior region is crucial. [10]
The first MI of 1.2 mm diameter and 6 mm length were introduced in 1997. [11]
It was proved that mini-implants insertion is a versatile surgery which is minimally
invasive without any assault towards the dental roots, it has easy insertion and removal,
readily loaded after initial wound healing, and has a low cost. [12,13,14]. Contrarily, the
effects of mini-implants and their retention depend on many factors such as: location of
insertion, bone quality, force applied, treatment duration, mini-implant length and
diameter, angle of insertion, etc.
The goal of the current report is to systematically review the effects of different mini-
implant insertion sites on maxillary incisors intrusion.
Intrusion of maxillary incisors by mini-implants can be done by various techniques,
different types of mini-implant which vary in properties, and can differ in quantity of mini-
implants used and magnitude of force applied. In the following review a comparison will
be performed between the various insertion sites and which effect each to of the sites has
on the results. The insertion sites that will be compared and discussed are the following:
- 1) one mini-implant between maxillary central incisors.
- 2) two symmetrical mini-implants between 2nd premolar and 1st molar (U5-U6)
- 3) two symmetrical mini-implants between lateral incisor and canine (U2-U3)
- 4) two symmetrical mini-implants between central and lateral incisors (U1-U2)
- 5) four symmetrical mini-implants anteriorly between lateral incisor and canine (U2-U3),
posteriorly between 2nd premolar and 1st molar (U5-U6).
5
The hypothesis of this systematic review was that the insertion site of the mini-implant has
an important role when intrusion of 4 maxillary incisors is considered. (it can gradually
affect the results and outcomes of the treatment.)
Therefore, the main aim of this systematic review was to evaluate and compare the effects
of different insertion sites of mini-implant on the maxillary incisors intrusion results.
Our tasks were:
1) To evaluate the effect of different mini-implant insertion sites on the total maxillary
incisors intrusion amount.
2) To evaluate the effect of different mini-implant insertion sites on the time needed for
maxillary incisors intrusion.
3) To evaluate the effect of different mini-implant insertion sites on the force needed to apply
for maxillary incisors intrusion.
6
SELECTION CRITERIA OF THE STUDIES.
SEARCH METHODS AND STRATEGY
This systematic review was performed according to the protocol of PRISMA (Preferred
Reporting Items for Systematic Reviews and Meta-analyses) statement for reporting
systematic reviews of the health sciences. [15]
Search strategy:
The systematic literature review was based on a selection from a main information source.
The main information source was literature studies from electronic databases that were
found during a search in Google web browser.
The keywords that were used in the search were: maxillary incisors intrusion, mini implant,
mini screw, TAD, SAD. (TAD: temporary anchorage device, SAD: skeletal anchorage
device).
Comprehensive electronic searches up to January 5th, 2018 were conducted in the
following databases: PubMed, Cochrane, Scopus, Science direct, Journal seek and
MedlinePlus.
In addition, the following journals were searched individually to find out any missing
articles: American Journal of Orthodontics and Dentofacial Orthopedics (AJO-DO) and
European Journal of Orthodontics-OXFORD Journals. Moreover, references in found
articles that led to additional relevant articles.
The literature search included assessment of articles from dental journals that were in the
English language, studies that were performed on humans only and published in the years
from January 1st 2008 till 5th of January 2018 and included the selected keywords.
In PubMed database and other databases with the same method of Advanced search, search
strategy performed as:( “mini implant” OR “mini screw” OR “TAD” OR “SAD”) AND
“maxillary incisors intrusion”.
In ScienceDirect the method of Advanced search act differently, therefore the search
strategy in this case was: “maxillary incisor intrusion” in the main search, and in advanced
category of: “With words in title, abstract or keywords” we added: “mini implant OR mini
screw OR TAD OR SAD” .
Search strategy in American Journal of Orthodontics was the same as performed in
PubMed.
7
However, in European Journal of Orthodontic- OXFORD Academy, we could not perform
advanced search with combination of: AND and OR, therefore in this case, search keyword
was only:” maxillary incisor intrusion”.
In total after duplicates removed 297 scientific publications, articles and clinical trials
reviews were identified and were related to keywords used during the search.
Titles and abstracts derived from this broad search were independently screened to
eliminate irrelevant publications and individual case reports.
The final stage of screening involved reading the full texts to confirm the eligibility of each
study, based on inclusion and exclusion criteria. The focused aim was: To evaluate the
effect of different MI insertion sites on maxillary incisors intrusion results.
Selection criteria: (PICOS question: population, intervention, comparison, outcome, study
designs).
The following eligibility criteria were used to determine eligible reports for this systematic
review:
Population: Adolescent and adult patients with deep overbite malocclusion and/or gummy
smile. Only human studies were included without consideration of gender.
Intervention: Patients undergoing orthodontic treatment for deep overbite and/or gummy
smile correction by maxillary incisors intrusion using temporary anchorage devices.
Comparison: between temporary anchorage devices techniques and different insertions
sites for maxillary incisors intrusion.
Outcomes: there are different effects on total maxillary incisors intrusion, duration of
treatment and applied force on MI insertion in the different sites.
Study design: Randomized and non-randomized controlled trials, clinical trials
(prospective and retrospective), and case series studies. Excluded articles included case
reports with ≤ 5 subjects, animal studies, review articles, abstracts, and discussions.
The inclusion criteria for this systematic review are:
1. All the study subjects are humans.
2. Years of articles publication were chosen from January 1st 2008 till the 5th of January
2018.
3.patients with deep overbite and/or gummy smile treated by maxillary incisors intrusion

8
by using temporary anchorage device.
4. studies that present records of pretreatment and posttreatment.
5. English language.
The exclusion criteria are:
1. Non- human studies.
2. In vitro studies.
3. literature reviews, abstracts, single case reports, editorials, commentaries.
4. articles included case reports with ≤ 5 subjects.
9
SYSTEMIZATION AND ANALYSIS OF DATA
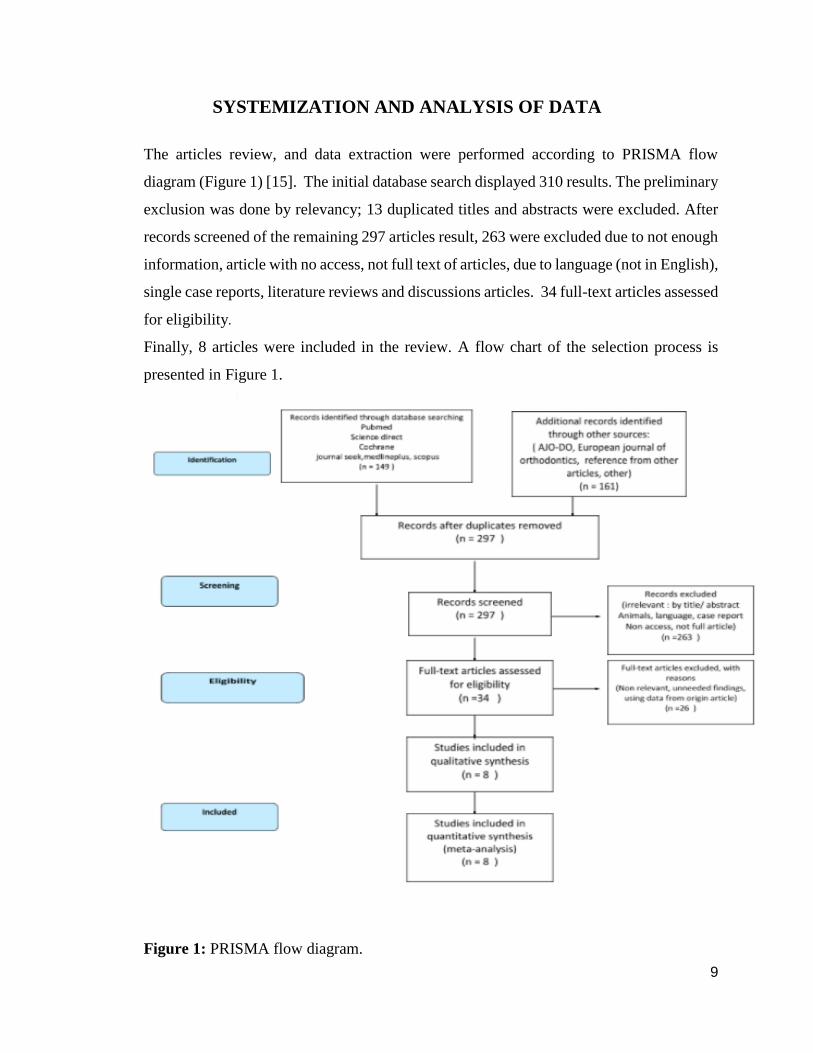
The articles review, and data extraction were performed according to PRISMA flow
diagram (Figure 1) [15]. The initial database search displayed 310 results. The preliminary
exclusion was done by relevancy; 13 duplicated titles and abstracts were excluded. After
records screened of the remaining 297 articles result, 263 were excluded due to not enough
information, article with no access, not full text of articles, due to language (not in English),
single case reports, literature reviews and discussions articles. 34 full-text articles assessed
for eligibility.
Finally, 8 articles were included in the review. A flow chart of the selection process is
presented in Figure 1.
Figure 1: PRISMA flow diagram.
10
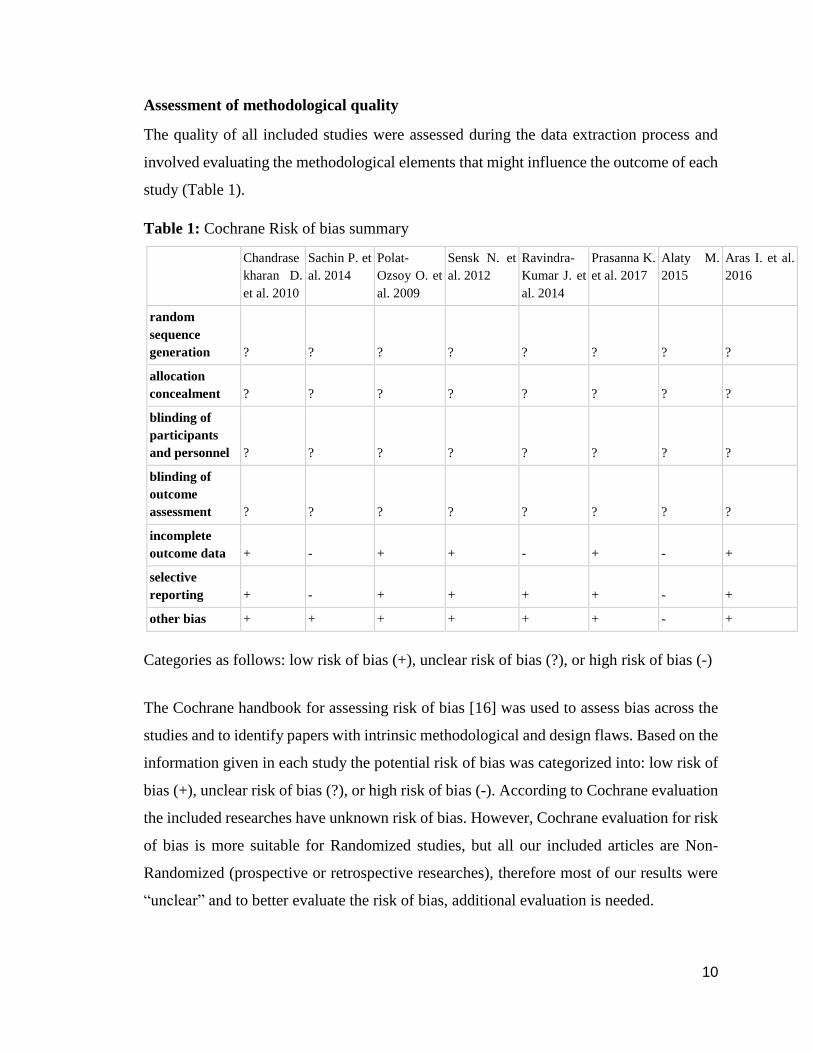
Assessment of methodological quality
The quality of all included studies were assessed during the data extraction process and
involved evaluating the methodological elements that might influence the outcome of each
study (Table 1).
Table 1: Cochrane Risk of bias summary
Chandrase
kharan D.
et al. 2010
Sachin P. et
al. 2014
Polat-
Ozsoy O. et
al. 2009
Sensk N. et
al. 2012
Ravindra-
Kumar J. et
al. 2014
Prasanna K.
et al. 2017
Alaty M.
2015
Aras I. et al.
2016
random
sequence
generation ? ? ? ? ? ? ? ?
allocation
concealment ? ? ? ? ? ? ? ?
blinding of
participants
and personnel ? ? ? ? ? ? ? ?
blinding of
outcome
assessment ? ? ? ? ? ? ? ?
incomplete
outcome data + - + + - + - +
selective
reporting + - + + + + - +
other bias + + + + + + - +
Categories as follows: low risk of bias (+), unclear risk of bias (?), or high risk of bias (-)
The Cochrane handbook for assessing risk of bias [16] was used to assess bias across the
studies and to identify papers with intrinsic methodological and design flaws. Based on the
information given in each study the potential risk of bias was categorized into: low risk of
bias (+), unclear risk of bias (?), or high risk of bias (-). According to Cochrane evaluation
the included researches have unknown risk of bias. However, Cochrane evaluation for risk
of bias is more suitable for Randomized studies, but all our included articles are Non-
Randomized (prospective or retrospective researches), therefore most of our results were
“unclear” and to better evaluate the risk of bias, additional evaluation is needed.

11
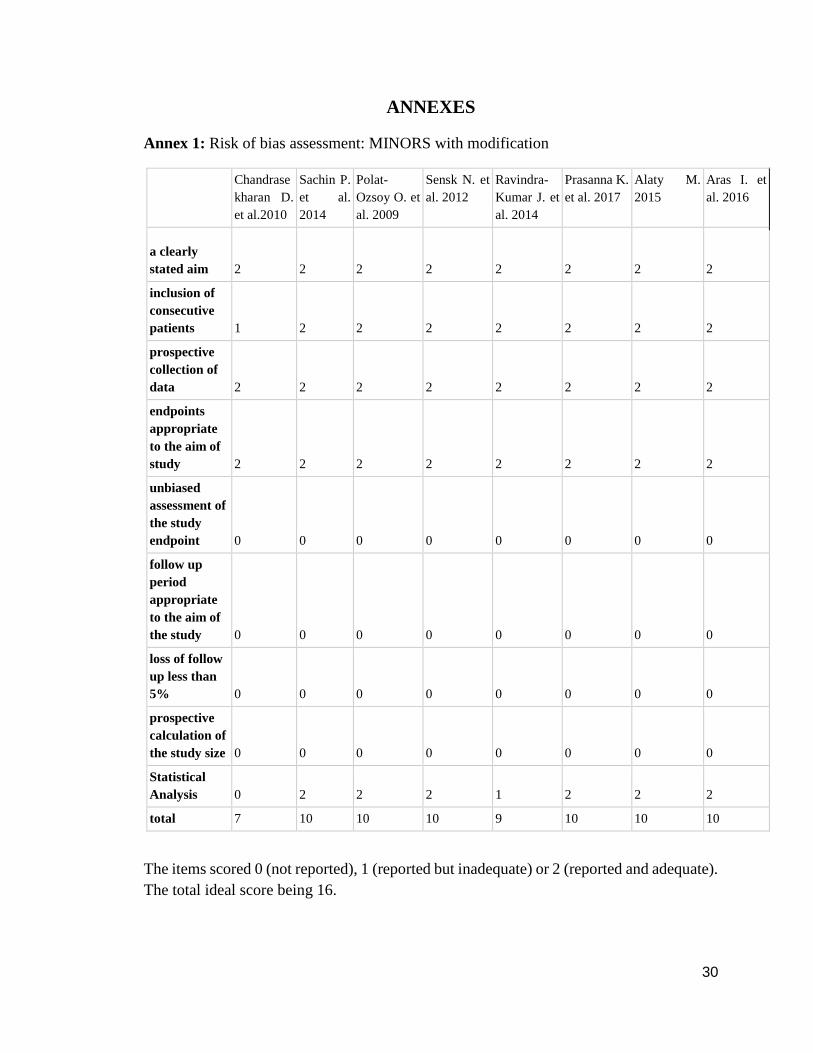
Additional assessment was done by using the methodological index for non-randomized
trials (MINORS) tool with a minor modification (Annex 1) [17].
Quality assessment
All studies included in our methodological scoring process have moderate quality as
presented in Annex 1. Randomization and blinding were not mentioned in any studies.
Follow up and evaluation after the end of treatment period was not done in any of the 8
included studies, although a long-term follow-up of these cases is needed to study the
possibility of a relapse. After a correction of deep overbite, as in all orthodontics treatment,
a relapse can occur and therefore an overcorrection should be taken into consideration.
.
12
RESULTS
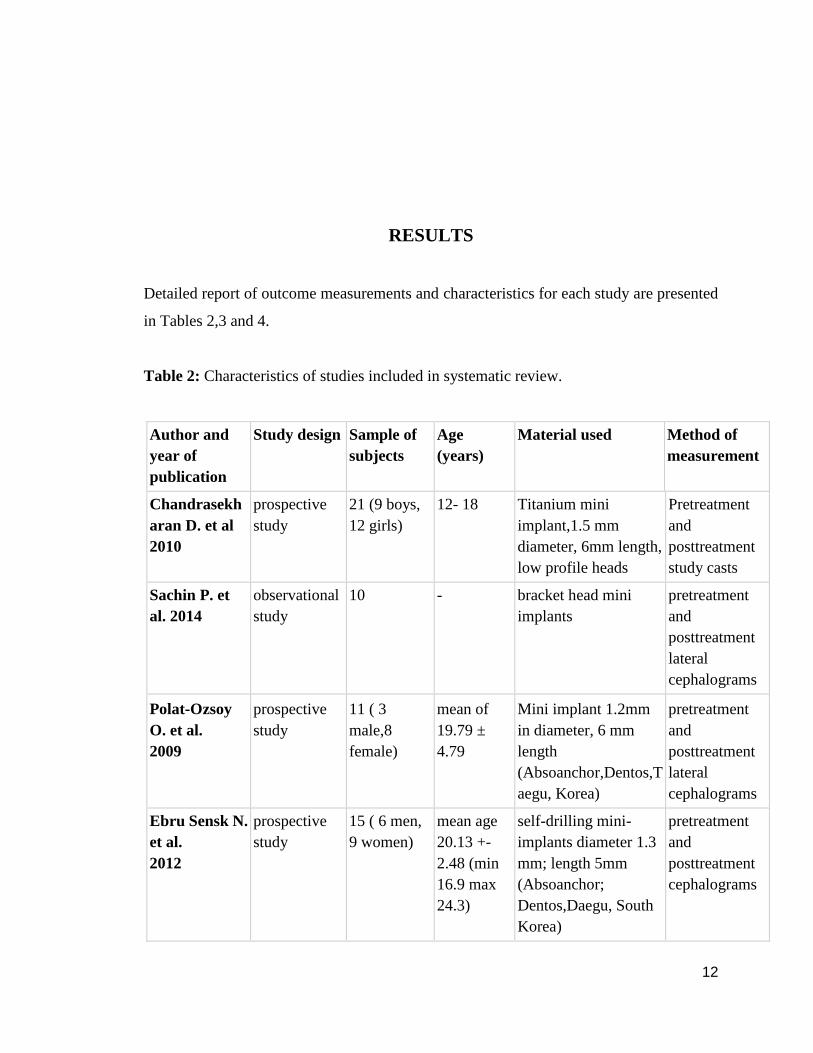
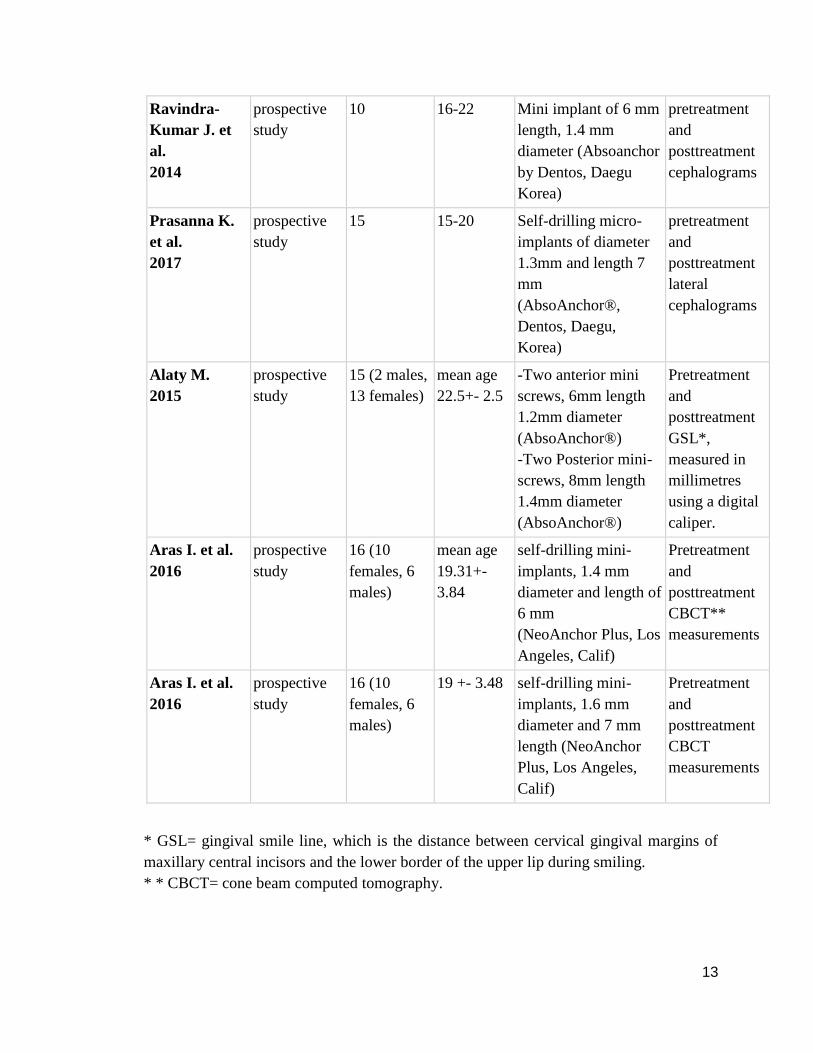
Detailed report of outcome measurements and characteristics for each study are presented
in Tables 2,3 and 4.
Table 2: Characteristics of studies included in systematic review.
Author and
year of
publication
Study design
Sample of
subjects
Age
(years)
Material used
Method of
measurement
Chandrasekh
aran D. et al
2010
prospective
study
21 (9 boys,
12 girls)
12- 18
Titanium mini
implant,1.5 mm
diameter, 6mm length,
low profile heads
Pretreatment
and
posttreatment
study casts
Sachin P. et
al. 2014
observational
study
10
-
bracket head mini
implants
pretreatment
and
posttreatment
lateral
cephalograms
Polat-Ozsoy
O. et al.
2009
prospective
study
11 ( 3
male,8
female)
mean of
19.79 ±
4.79
Mini implant 1.2mm
in diameter, 6 mm
length
(Absoanchor,Dentos,T
aegu, Korea)
pretreatment
and
posttreatment
lateral
cephalograms
Ebru Sensk N.
et al.
2012
prospective
study
15 ( 6 men,
9 women)
mean age
20.13 +-
2.48 (min
16.9 max
24.3)
self-drilling mini-
implants diameter 1.3
mm; length 5mm
(Absoanchor;
Dentos,Daegu, South
Korea)
pretreatment
and
posttreatment
cephalograms
13
Ravindra-
Kumar J. et
al.
2014
prospective
study
10
16-22
Mini implant of 6 mm
length, 1.4 mm
diameter (Absoanchor
by Dentos, Daegu
Korea)
pretreatment
and
posttreatment
cephalograms
Prasanna K.
et al.
2017
prospective
study
15
15-20
Self-drilling micro-
implants of diameter
1.3mm and length 7
mm
(AbsoAnchor®,
Dentos, Daegu,
Korea)
pretreatment
and
posttreatment
lateral
cephalograms
Alaty M.
2015
prospective
study
15 (2 males,
13 females)
mean age
22.5+- 2.5
-Two anterior mini
screws, 6mm length
1.2mm diameter
(AbsoAnchor®)
-Two Posterior mini-
screws, 8mm length
1.4mm diameter
(AbsoAnchor®)
Pretreatment
and
posttreatment
GSL*,
measured in
millimetres
using a digital
caliper.
Aras I. et al.
2016
prospective
study
16 (10
females, 6
males)
mean age
19.31+-
3.84
self-drilling mini-
implants, 1.4 mm
diameter and length of
6 mm
(NeoAnchor Plus, Los
Angeles, Calif)
Pretreatment
and
posttreatment
CBCT**
measurements
Aras I. et al.
2016
prospective
study
16 (10
females, 6
males)
19 +- 3.48
self-drilling mini-
implants, 1.6 mm
diameter and 7 mm
length (NeoAnchor
Plus, Los Angeles,
Calif)
Pretreatment
and
posttreatment
CBCT
measurements
* GSL= gingival smile line, which is the distance between cervical gingival margins of
maxillary central incisors and the lower border of the upper lip during smiling.
* * CBCT= cone beam computed tomography.
14
Out of the 8 selected studies one was designed as observational study, the rest as
prospective studies [8-9, 18-23].
In the last included article (Aras I. et al. 2016) [23] a comparison was made between two
groups of patients, with two different insertion sites of mini-implants, one group treated
with mini implants located between lateral incisor and the canine, while the second group
was treated with mini-implants located between the second premolar and the first molar.
Thus, in all the characteristics and outcome measurements tables, the study was mentioned
twice while assigned each group separately.
The average sample of subjects of all the included studies is 14.33, with the lowest sample
of 10 [19] and highest sample of 21 [18] with female predominance. The range of age is
varied from 12 to 25 years old. However, one study did not mention the age of the sampled
subjects (Sachin P. et al. 2014) [19].
Five out of the eight included studies chose TAD length of 6mm, one used 5mm [21] and
final two studies used TAD with more than 6mm in length (7mm and 8mm) [9,22-23].
The range of TAD’s diameter varied from 1.2 to 1.6 mm.
Most of the studies measured pretreatment and posttreatment parameters using lateral
cephalometric radiograph, two used cone beam computed tomography (CBCT) [23], one
study measured pretreatment and posttreatment study casts [18], and in the study of Alaty
M. 2015, the method of measurement was before and after intrusion GSL- gingival smile
line which is the distance between cervical gingival margins of maxillary central incisors
and lower border of the upper lip during smiling (measured by digital caliper in
millimeters) [22]
15
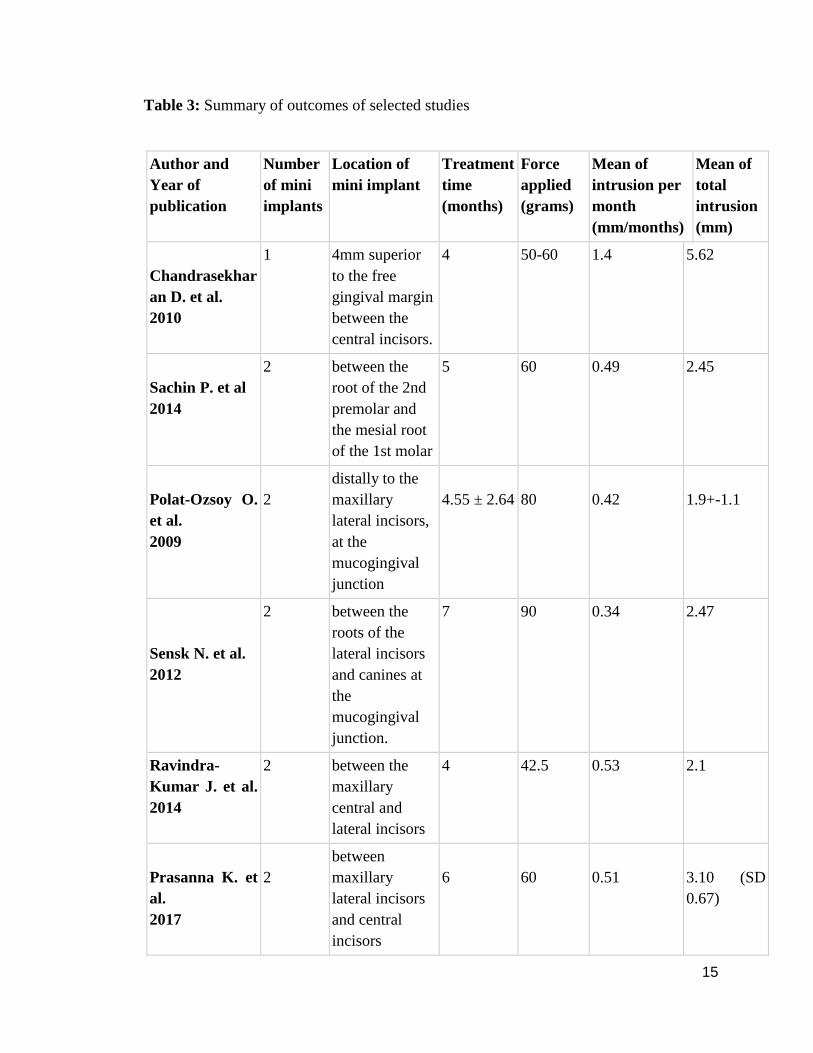
Table 3: Summary of outcomes of selected studies
Author and
Year of
publication
Number
of mini
implants
Location of
mini implant
Treatment
time
(months)
Force
applied
(grams)
Mean of
intrusion per
month
(mm/months)
Mean of
total
intrusion
(mm)
Chandrasekhar
an D. et al.
2010
1
4mm superior
to the free
gingival margin
between the
central incisors.
4
50-60
1.4
5.62
Sachin P. et al
2014
2
between the
root of the 2nd
premolar and
the mesial root
of the 1st molar
5
60
0.49
2.45
Polat-Ozsoy O.
et al.
2009
2
distally to the
maxillary
lateral incisors,
at the
mucogingival
junction
4.55 ± 2.64
80
0.42
1.9+-1.1
Sensk N. et al.
2012
2
between the
roots of the
lateral incisors
and canines at
the
mucogingival
junction.
7
90
0.34
2.47
Ravindra-
Kumar J. et al.
2014
2
between the
maxillary
central and
lateral incisors
4
42.5
0.53
2.1
Prasanna K. et
al.
2017
2
between
maxillary
lateral incisors
and central
incisors
6
60
0.51
3.10 (SD
0.67)

16
Alaty M.
2015
4
two anterior
TADs between
the roots of
lateral incisors
and canines;
two posterior
TADs between
the roots of 2nd
premolars and
1st molars.
13.133
-
0.34
4.4
Aras I. et al.
2016
2
between lateral
incisor and
canine
4
40
0.62
2.48
Aras I. et al.
2016
2
between the
second
premolar and
first molar
4
40
0.39
1.56
17
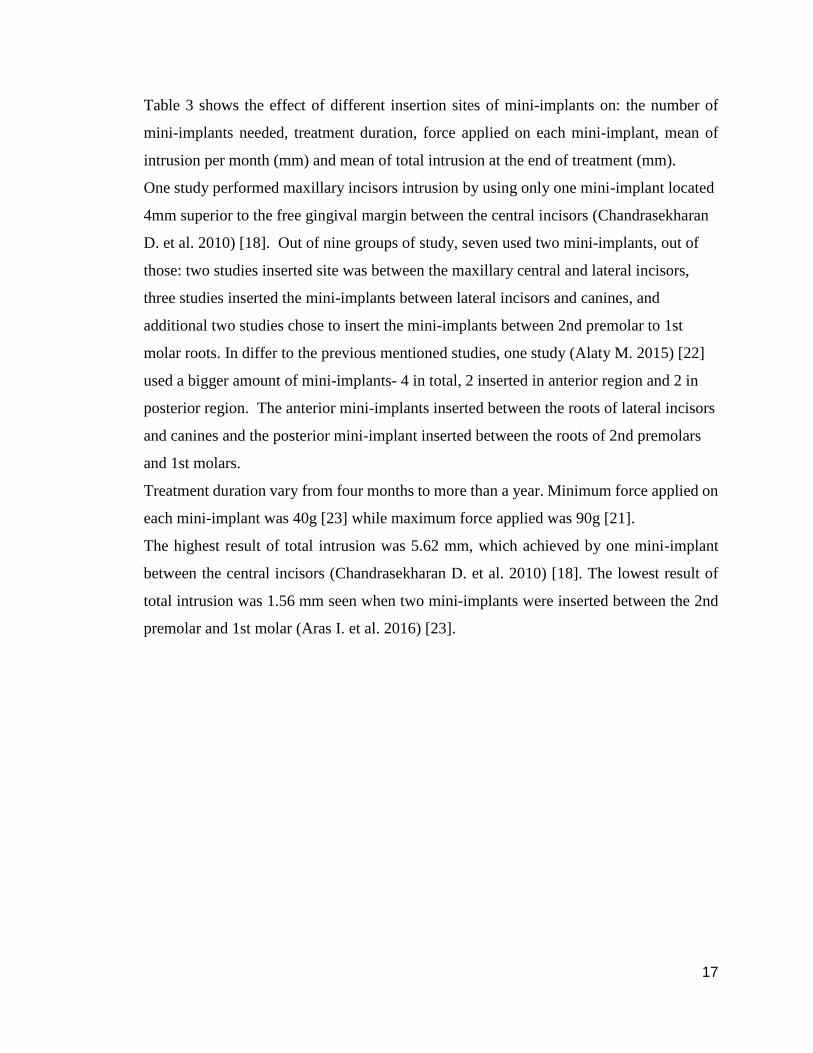
Table 3 shows the effect of different insertion sites of mini-implants on: the number of
mini-implants needed, treatment duration, force applied on each mini-implant, mean of
intrusion per month (mm) and mean of total intrusion at the end of treatment (mm).
One study performed maxillary incisors intrusion by using only one mini-implant located
4mm superior to the free gingival margin between the central incisors (Chandrasekharan
D. et al. 2010) [18]. Out of nine groups of study, seven used two mini-implants, out of
those: two studies inserted site was between the maxillary central and lateral incisors,
three studies inserted the mini-implants between lateral incisors and canines, and
additional two studies chose to insert the mini-implants between 2nd premolar to 1st
molar roots. In differ to the previous mentioned studies, one study (Alaty M. 2015) [22]
used a bigger amount of mini-implants- 4 in total, 2 inserted in anterior region and 2 in
posterior region. The anterior mini-implants inserted between the roots of lateral incisors
and canines and the posterior mini-implant inserted between the roots of 2nd premolars
and 1st molars.
Treatment duration vary from four months to more than a year. Minimum force applied on
each mini-implant was 40g [23] while maximum force applied was 90g [21].
The highest result of total intrusion was 5.62 mm, which achieved by one mini-implant
between the central incisors (Chandrasekharan D. et al. 2010) [18]. The lowest result of
total intrusion was 1.56 mm seen when two mini-implants were inserted between the 2nd
premolar and 1st molar (Aras I. et al. 2016) [23].
18
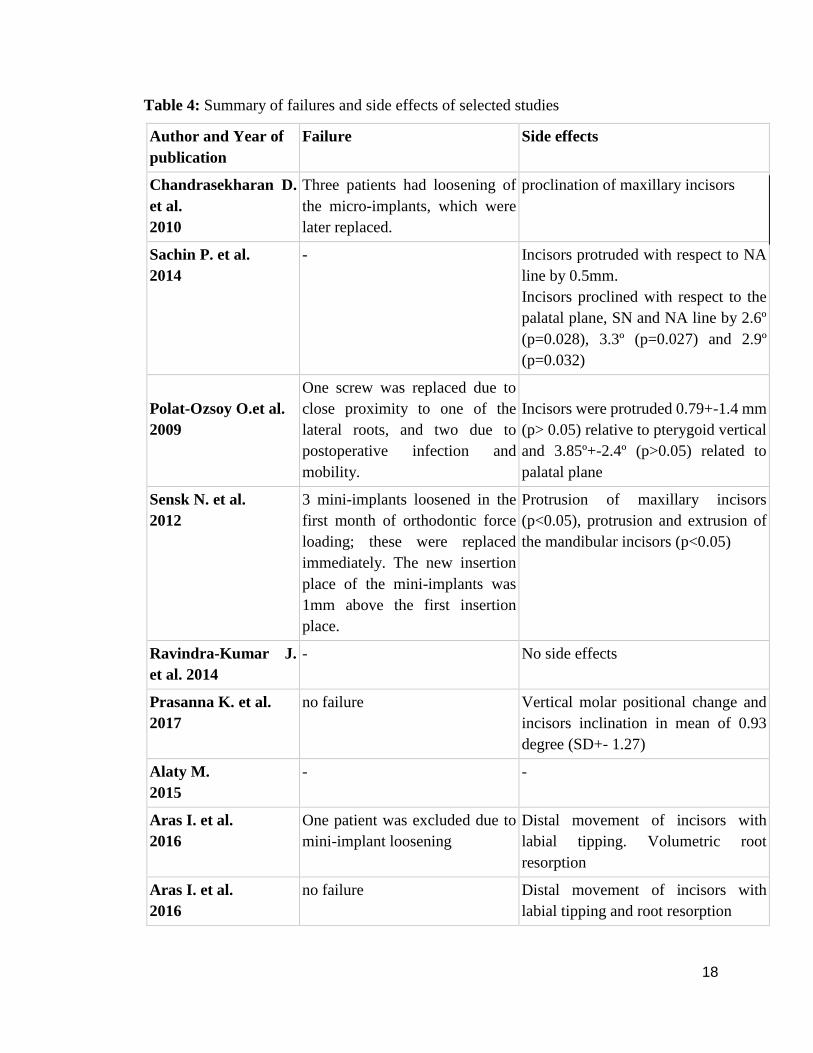
Table 4: Summary of failures and side effects of selected studies
Author and Year of
publication
Failure
Side effects
Chandrasekharan D.
et al.
2010
Three patients had loosening of
the micro-implants, which were
later replaced.
proclination of maxillary incisors
Sachin P. et al.
2014
-
Incisors protruded with respect to NA
line by 0.5mm.
Incisors proclined with respect to the
palatal plane, SN and NA line by 2.6º
(p=0.028), 3.3º (p=0.027) and 2.9º
(p=0.032)
Polat-Ozsoy O.et al.
2009
One screw was replaced due to
close proximity to one of the
lateral roots, and two due to
postoperative infection and
mobility.
Incisors were protruded 0.79+-1.4 mm
(p> 0.05) relative to pterygoid vertical
and 3.85º+-2.4º (p>0.05) related to
palatal plane
Sensk N. et al.
2012
3 mini-implants loosened in the
first month of orthodontic force
loading; these were replaced
immediately. The new insertion
place of the mini-implants was
1mm above the first insertion
place.
Protrusion of maxillary incisors
(p<0.05), protrusion and extrusion of
the mandibular incisors (p<0.05)
Ravindra-Kumar J.
et al. 2014
-
No side effects
Prasanna K. et al.
2017
no failure
Vertical molar positional change and
incisors inclination in mean of 0.93
degree (SD+- 1.27)
Alaty M.
2015
-
-
Aras I. et al.
2016
One patient was excluded due to
mini-implant loosening
Distal movement of incisors with
labial tipping. Volumetric root
resorption
Aras I. et al.
2016
no failure
Distal movement of incisors with
labial tipping and root resorption
19
Table 4 presents a summary of failures and side effects of selected studies.
The meaning of failure in this systematic review (and as mentioned in the included studies)
was: loosening of mini-implant during the treatment period.
Two studies declared: “No failure”.
In the study of Chandrasekharan D. et al. 2010 [18] with strategy method of one mini-
implant between central incisors, three patients had loosening of the mini-implants.
Failure of 3 inserted mini-implant has been seen in the study of Polat-Ozsoy O.et al. 2009,
[20] when using two mini implants inserted between the lateral incisor and the canine.
The same number of mini-implants loosening (three) were observed in the study of Sensk
N. et al. 2012 [21] while using the same insertion site of mini-implants (between lateral
incisor and canine).
All the cases of failure that were mentioned above, in all the three studies, were fixed with
replacing the mini implants. In contrast, in the study of Aras I. et al.2016, [23] one case
observed with loosening of mini-implant and it was not fixed by replacing the mini-
implants, but this patient excluded from the study.
The reasons for the loosening of mini-implants were:
1) Postoperative infection.
2) Postoperative mobility of mini-implant
3) Close proximity to one of the roots.
The rest of the studies not mentioned about failure or loosening of mini implants. [8,19,22].
The main side effect was protrusion of maxillary incisors, other side effects were: root
resorption, inclination of maxillary incisors, distal movement of incisors with labial
tipping, proclination of maxillary incisors, protrusion and extrusion of the mandibular
incisors and vertical molar positional changes.
Only one of all included studies (Ravindra-Kumar J. et al. 2014) [8] declared: No side
effects.
20
DISCUSSION
During our assessment and evaluation of the data in the including studies and while
working on this systematic review, we found an interesting fact: there were more female
participants in the researches samples.
Our assumption is that this fact stems from the innate nature of women towards esthetics
and not because women tend to suffer more from deep overbite and/or gummy smile
condition than men.
In addition, with the data we gathered, out of all TAD’s available at present time, we found
that the TAD which was used the most for maxillary incisors intrusion was mini implant
with characteristics of 6mm length and 1.2-1.4 mm of diameter.
Furthermore, we found that the different insertion sites of MI indeed influenced the results
and the outcomes of the intrusion treatment and those are explained separately in detail at
the following paragraphs.
The first insertion site that we evaluated, in the study of Chandrasekharan D. et al. [18]
was one mini implant between maxillary central incisors (U1-U1).
Among 21 patients, the mean of total intrusion was 5.62mm which is the highest result of
all the other data we have gathered and by a large margin, and under only four months of
treatment. In this method of treatment, the mini implant endured 50-60 grams of force
which is approximately the average amount of force applied in all the included studies.
(average is 58.4g). Chandrasekharan D. et al reported-on failure of 3 out of 21 patients
(~14.3%), and proclination of maxillary incisors as side effect.
Although the results of MI insertion in U1-U1 region were very stratified, the percentages
of failure were the highest and insertion at this site is not esthetically pleasing. However,
this method was found to be more conservative than others due to the fact that only one MI
insertion was needed.
The second insertion site that we evaluated was between the central and the lateral incisors
(U1-U2), in this technique two mini implants were used. The data presented in two of our
included studies: Ravinda-Kumar J. et al. and Prasanna K. et al. [8, 9]. The mean of total
intrusion achieved respectively was 2.1mm and 3.1mm and these results were found to be
satisfying.
21
Answering to question why a vastly different results (1 mm of difference) were achieved
when the same insertion site was used, we assume that the different results stem from the
differences in the duration of treatment and we could conclude this by observing the results
of the mean of intrusion per month values that were almost the same: 0.51mm and 0.53mm.
While in the study of Ravinda-Kumar J. et al. [8] the total duration of treatment was 4
months with 42.5g of force applied on each mini implant, in the study of Prasanna K. et
al. [9] the duration of treatment was 6 months, with 60g of force applied on each mini
implant. From that, we can conclude that to perform an intrusion of maxillary incisors by
using 2 mini implants located between the central and the lateral incisors, there is no need
to use force above 42.5g because it makes no difference at all when 60g are used. In
addition, if we want to increase the total amount of intrusion it is better to prolong the
duration of treatment by few more months.
In contrast to the other studies, Ravinda-Kumar J. et al. [8] was the only study that reported
on no side effects at all and the study of Prasanna K. et al. [9] was one of two studies, out
of 9, that had reported on no failure.
The third insertion site evaluated in this systematic review was 2 mini implants between
the lateral incisors and the canines (U2-U3). There were three involved studies: Polat-
Ozsoy O. et al, Sensk N. et al and Aras I. et al. [20, 21, 23]
The mean of total intrusion was respectively: 1.9mm, 2.47mm and 2.48mm.
Although the same insertion site was used, the treatment method used in the studies differed
by the force applied on each mini implant (80g, 90g and 40g), the duration of treatment
(4.55months, 7months and 4months) and the mean of intrusion per month (0.42mm/month,
0.34mm/month and 0.62mm/month).
From the summary of all the results and outcomes, we can deduce that: the bigger the force
and the longer the duration of treatment were, a smaller mean of intrusion per month was
observed.
In addition, the prospective studies of Polat-Ozsoy O. et al. and Sensk N. et al. [20, 21]
reported on a failure of 3 mini-implants.

22
In order to calculate the percentage of failure, a ratio between the number of loosen MI and
the total screwed MI must be done, doing this led to us the following results: 9.1% and
10% of failure respectively, while the prospective study of Aras I. et al. [23] showed only
6.25% failure. Moreover, according to the data we collected, the three studies that used
U2-U3 as MI insertion site reported on several side effects, including: protrusion of
maxillary incisors, protrusion and extrusion of mandibular incisors and root resorption.
The forth insertion site that we evaluated was: U5-U6, two mini implants were inserted
in between 2nd premolar and 1st molar.
This insertion site has the benefit of being more esthetically pleasing, due to the fact that
the mini implants are inserted in posterior region, hidden from sight during smiling,
laughing and speaking.
Two studies from our systematic review used this insertion site: Sachin P. et al. and Aras
I. et al. [19, 23]. The first study by Sachin P. et al. [19] resulted in 2.45mm mean of total
intrusion while applied 60g of force on each mini-implant and the treatment lasted for five
months. The second study by Aras I. et al. [23] resulted in only 1.56mm mean of total
intrusion while applied 40g of force in duration of four months. Out of nine studies, this
study earned the lowest amount of intrusion and therefore the least advisable to follow but,
on the other hand no failures were reported in contrast to the other studies.
A newly published systematic review done by: Gintautaitė G. and Gaidytė A. (2017)
found out that the success rate of mini-implant inserted in the maxilla between 2nd
premolar and 1st molar is 86.9-97.2%, which is satisfying. [24]
In conclusion, in order to preform intrusion of maxillary incisors by insertion of mini-
implants in the posterior region, a bigger force is needed, and a longer duration of treatment
is required.
Therefore, it will be better to follow the method seen in the study of Sachin P. et al. [19]
23
One study by Alaty M. [22] performed another method of treatment, using four mini-
implants: two located anteriorly: between the lateral incisors and the canines and two
located posteriorly between the 2nd premolars and the 1st molars. The fact that this study
had incomplete outcomes and data (missing: force applied in grams, failures and side
effects), makes the comparison difficult. Nonetheless, the achievement of 4.4mm mean
total intrusion is outstanding, but the duration of treatment was doubled and even tripled
compared to other techniques.
At the beginning of this study it was cited that one of the major advantage of mini-implants
over other orthodontic methods dealing with intrusion of maxillary incisors is the fact that
it holds no side effects. And while examining the studies used in this systematic review,
we surprisingly found several side effects that can be due to mini-implants use as a
treatment for deep bite and/or gummy smile. However, compared to other techniques the
side effects of mini-implants usage were reduced substantially.
While analyzing all the discussed data, its apparent that there are differences on the
achieved results if several insertion sites of mini-implants are compared.
Unfortunately, we cannot put our finger on the exact reason of why that is. It might be
influenced not only by the force applied and/or the treatment duration but also by the
difference in the age of the patients, materials used, changes in the proximity of the mini-
implant to the teeth’s roots and the density of the bone itself. All those and more should
be further investigated in future clinical researches.
Limitations:
There is no doubt that the number of studies available in our days are not enough to reliably
answer all the questions. There are no randomized clinical trials performed focused on the
deep bite and/or gummy smile treatment using temporary anchorage devices. Presence of
randomization is an important issue to consider when determining the best treatment
modality for maxillary incisors intrusion.
It is clinically important to investigate the amount of maxillary incisors protrusion,
inclination and bone resorption during deep overbite and/or gummy smile treatment while
using TAD’s in comparison between the different options of insertion sites,

24
as well as evaluation of the long-term stability of maxillary incisors intrusion by different
techniques. The drawbacks in most of the articles such as absence of untreated control
groups, absence of follow-up period, small sample size, and presence of confounding
factors should be avoided in future studies so as to reach a more accurate conclusion
concerning deep overbite and some of the gummy smile treatment.

25
CONCLUSIONS
Our hypothesis that the decision regarding the insertion site of the mini-implants has an
important role when intrusion of four maxillary incisors is considered and it can affect the
results and outcomes of the treatment was proven by the following findings:
1) The different total maxillary incisors intrusion amount was found when a different
insertion sites were used.
2) The treatment duration was found to be different when different insertion sites was
used.
3) The force required to apply was found to be different when different insertion site
was used.
In addition, by this systematic review we can conclude that:
The best results and outcomes achieved when one mini-implant was inserted between the
maxillary central incisors. In case that two mini-implants were inserted in U2-U3 area: the
bigger the force and the longer the duration of treatment was performed, a smaller mean of
intrusion per month was observed. In contrast, when mini-implant was inserted in posterior
region: U5-U6, a bigger force was needed for a bigger amount of total intrusion. However,
when mini-implant was inserted in the U1-U2 site, any addition of applied force made no
differences on the mean of intrusion per month.

26
PRACTICAL RECOMMENDATIONS
- In order to treat deep overbite and/or gummy smile with MI, it is recommended to insert
one mini implant between central incisors, 4mm superior to the free gingival margin, a load
of 50g on each MI and plan a treatment schedule for at least 4 months.
- To reduce the risk of failure it is recommended to insert 2 MI between the lateral incisors
and the canines, load each MI with not more than 40g of force and plan a treatment schedule
of 4 months.
- Only for a better visual esthetics during the treatment and to the preference and request of
the patient it is recommended to insert 2 MI in between 2nd premolar and 1st molar, load
each MI with 60g of force and plan a treatment schedule of 5 months.
27
REFERENCES
1. Marcotte MR. Biomechanics in Orthodontics. Philadelphia: PA;1990
2. Burstone, CR. Deep overbite correction by intrusion. American Journal of Orthodontics
1977;72(1), 1–22.
3. Nikolai RJ. Response of dentition and periodontium to force. Bioengineering Analysis of
Orthodontic Mechanics. Philadelphia: Lea and Febinger; 1985. p. 146-93.
4. Sunita S, Nivedita S, Pritam M, Snigdha G, Baratam S, Shuvesa S. Orthodontic Intrusion:
An Insight. International Journal of Oral Health and Medical Research 2017;6(3), 137-140.
5. Al-Zubair N. Orthodontic intrusion: A contemporary review. Journal of Orthodontic
Research 2014;2(3), 118.
6. Goel P, Tandon R, Agrawal K. A comparative study of different intrusion methods and
their effect on maxillary incisors. Journal of Oral Biology and Craniofacial Research. 2014; 4(3),
186–191.
7. Al-Buraiki H, Sadowsky C, Schneider B. The effectiveness and long-term stability of
overbite correction with incisor intrusion mechanics. American Journal of Orthodontics and
Dentofacial Orthopedics 2005; 127(1), 47–55.
8. Ravindra-Kumar J, Sridhar-Prem K, Manjula W. S. Comparison of intrusion effects on
maxillary incisors among mini implant anchorage, J-hook headgear and utility arch. Journal of
Clinical and Diagnostic Research 2014; 8(7), 21–24.
9. Prasanna K, Datana S, Londhe S.M, Kadu A. Rate of intrusion of maxillary incisors in
class II div 1 malocclusion using skeletal anchorage device and Connecticut intrusion arch.
Medical Journal Armed Forces India 2017;73(1), 65–73.
28
10. Choi J. H, Yu H.S, Lee K. J, Park Y. C. Three-dimensional evaluation of maxillary
anterior alveolar bone for optimal placement of mini screw implants. Korean Journal of
Orthodontics 2014;44(2), 54–61.
11. Adell R, Lekholm U, Rockler B, Brånemark PI. A 15-year study of osseointegrated
implants in the treatment of the edentulous jaw. Int J Oral Surg 1981;10(6):387-416.
12. Chatzigianni A, Keilig L, Reimann S, Eliades T, Bourauel C. Effect of mini-implant
length and diameter on primary stability under loading with two force levels. European Journal
of Orthodontics 2011;33(4), 381–387.
13. Tseng Y. C, Hsieh C. H, Chen C. H, Shen Y. S, Huang I. Y,Chen C. M. The application
of mini-implants for orthodontic anchorage. International Journal of Oral and Maxillofacial
Surgery 2006;35(8), 704–707.
14. Nosouhian S, Rismanchian M, Sabzian R, Shadmehr E, Badrian H, Davoudi A. A Mini-
review on the Effect of Mini-implants on Contemporary Orthodontic Science. Journal of
International Oral Health 2015;83–87.
15. Moher D, Liberati A, Tetzlaff J, Altman DG. PRISMA Group. Preferred reporting items
for systematic reviews and meta-analyses: the PRISMA statement. Int J Surg 2010;8(5):336-41.
16. Higgins J.P.T., Green S. Cochrane Handbook for Systematic Reviews of Interventions.
The Cochrane Collaboration 2011. URL:http://www.cochrane.org/cochrane-interventions-
handbook.
17. Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J. Methodological index
for non-randomized studies (minors): development and validation of a new instrument. ANZ J
Surg. 2003;73(9):712–6.
29
18. Chandrasekharan D, Balaji S. M. Intrusion of anterior teeth to improve smile esthetics.
Journal of Maxillofacial and Oral Surgery 2010; 9(1), 27–29.
19. Sachin P, Ravindra S, Gauri V, Amol P. Bracket head mini screw implants for intrusion
in anterior teeth for deep bite cases : An in vivo study. International Journal of Contemporary
Orthodontics 2014;25–31.
20. Polat-Ozsoy O, Arman-Ozcirpici A, Veziroglu F. Miniscrews for upper incisor intrusion.
European Journal of Orthodontics 2009;31(4), 412–416.
21. Şenşk N. E, Türkkahraman H. Treatment effects of intrusion arches and mini-implant
systems in deep bite patients. American Journal of Orthodontics and Dentofacial Orthopedics
2012;141(6), 723–733.
22. Alaty M. Temporary anchorage devices and gummy smile. The Libyan Dental Journal
2015;20918721(5), 1–8.
23. Aras I, Tuncer A.V.Comparison of anterior and posterior mini-implant-Assisted
maxillary incisor intrusion: Root resorption and treatment efficiency. Angle Orthodontist
2016;86(5), 746–752.
24. Gintautaitė G, Gaidytė A. Surgery-related factors affecting the stability of orthodontic
mini implants screwed in alveolar process interdental spaces : a systematic literature review.
Stomatologija, Baltic Dental and Maxillofacial Journal 2017;19(1), 25–30.
30
ANNEXES
Annex 1: Risk of bias assessment: MINORS with modification
Chandrase
kharan D.
et al.2010
Sachin P.
et al.
2014
Polat-
Ozsoy O. et
al. 2009
Sensk N. et
al. 2012
Ravindra-
Kumar J. et
al. 2014
Prasanna K.
et al. 2017
Alaty M.
2015
Aras I. et
al. 2016
a clearly
stated aim 2 2 2 2 2 2 2 2
inclusion of
consecutive
patients 1 2 2 2 2 2 2 2
prospective
collection of
data 2 2 2 2 2 2 2 2
endpoints
appropriate
to the aim of
study 2 2 2 2 2 2 2 2
unbiased
assessment of
the study
endpoint 0 0 0 0 0 0 0 0
follow up
period
appropriate
to the aim of
the study 0 0 0 0 0 0 0 0
loss of follow
up less than
5% 0 0 0 0 0 0 0 0
prospective
calculation of
the study size 0 0 0 0 0 0 0 0
Statistical
Analysis 0 2 2 2 1 2 2 2
total 7 10 10 10 9 10 10 10
The items scored 0 (not reported), 1 (reported but inadequate) or 2 (reported and adequate).
The total ideal score being 16.