Embed Size (px)
Citation preview

Serratia marcescens is an important cause of nosocomial infections,especially in critically ill neonates [1-3]. Most infections are acquiredexogenously [1,2]. The organism is widespread in the environment but isnot a common constituent of the human intestinal flora [1,3]. S.marcescens may cause a wide spectrum of infections includingbacteremia, pneumonia, meningitis and urinary tract infections and isassociated with significant morbidity and mortality, especially in low-birthweight neonates [1-3]. Outbreaks in the neonatal intensive care unit aremore commonly being described and have been linked to contaminatedbreast pumps, breast milk, disinfectants and air conditioner vents [1-3].We report the investigation and control of an outbreak of S. marcescensinfection on the neonatal platform associated with inadequately re-processed ventilator tubing.
Microbiological Studies and GenotypingCultures of environmental sources were performed, which included sinks, counter-tops, ventilators andrespiratory care equipment. The latter included “used” ventilator circuits and “clean”, re-processed,packaged circuits. Isolates were identified and antimicrobial susceptibility testing were performed usingthe automated Vitek 2 System (bioMérieux, Hazelwood, MO).
A selective number of clinical isolates and S. marcescens isolated from the ventilator tubing weregenotyped using pulsed-field gel electrophoresis (PFGE) and analyzed using the GelCompar II software(Applied Maths NV). Patterns produced by PFGE were interpreted based on the criteria for bacterial straintyping by Tenover et al. – closely related isolates should have ≤ 3 differences in banding pattern [4].
Cut-off values have been previously described by Aucken et al. where 75–78% similarity overall, suggestsrelated isolates, while the closest similarity for unrelated strains was 70% for S. marcescens isolatesdigested using the enzyme, XbaI [5]. However, more stringent criteria (>91% similarity suggesting relatedisolates) were adopted as Aucken et al. acknowledged that the described cut-off values were low, asisolates were from an outbreak that lasted 10 years [5].
1. Voelz A, Müller A, Gillen J, Le C, Dresbach T, Engelhart S, Exner M, Bates CJ, Simon A: Outbreaks of Serratia marcescens in neonatal and pediatric intensive care units: clinical aspects, risk factors and management. Int J Hyg Environ Health 2010, 213(2):79-87
2. Maragakis LL, Winkler A, Tucker MG, Cosgrove SE, Ross T, Lawson E, Carroll KC, Perl TM: Outbreak of multidrug-resistant Serratia marcescens infection in a neonatal intensive care unit. Infect Control Hosp Epidemiol 2008, 29(5):418-23
3. Fleisch F, Zimmermann-Baer U, Zbinden R, Bischoff G, Arlettaz R, Waldvogel K, Nadal D, Ruef C: Three consecutive outbreaks of Serratia marcescens in a neonatal intensive care unit. Clin Infect Dis 2002, 34(6):767-73
4. Tenover FC, Arbeit RD, Goering RV, Mickelsen PA, Murray BE, Persing DH, Swaminathan B: Interpreting chromosomal DNA restriction patterns produced by pulsed-field gel electrophoresis: criteria for bacterial strain typing. J. Clin. Microbiol 1995, 33:2233–2239.
5. Auken HM, Boquete T, Kaufmann ME, Pitt TL: Interpretation of band differences to distinguish strains of Serratia marcescens by pulsed-field gel electrophoresis of XbaI DNA digests. Epidemiol Infect 2000, 125:63-70
A single circulating strain of S. marcescens was identified using PFGE andimplicated the ventilator equipment as the reservoir thereof. On the 25th
October 2012, a week after the outbreak investigation began, disposable, single-patient use ventilator circuits were introduced and the washer-disinfectormachines were condemned from use. SSD staff were educated about the use ofvarious disinfectants.
Prompt case identification, appropriate infection control interventions and theuse of disposable, single-patient ventilator circuits, were the key factors that ledto the timely and successful control of this outbreak.
BackgroundIn October 2012, the Unit for Infection Prevention and Control (UIPC) atTygerberg Hospital in Cape Town, South Africa, was alerted to clinicallysignificant S. marcescens infections, in patients hospitalized in theneonatal wards. Microbiology laboratory results were reviewed to identifycases and to determine the baseline rate of infection. Twelve neonateswere identified with cultures of S. marcescens over a 4 month periodbetween July and October 2012.
Case DefinitionCases were defined as patients admitted to the neonatal unit in whom ≥1clinical specimens showed the presence of S. marcescens. Data frommedical records were reviewed to assess for potential risk factorsincluding the ward location, previous surgery, central venouscatheterization, urinary catheterization, previous mechanical ventilationand antibiotic exposure.
INTRODUCTION
PURPOSE
METHODS
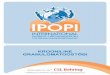
PFGE patterns of S. marcescens isolatesrecovered from patients and ventilator tubing samples during the outbreak period
CONCLUSIONS
REFERENCES
Characteristics of patients involved in the outbreak
Samples were taken from “clean”, ready-for-use, re-processed ventilator circuits. Fluid condensates,present in the tubing, were sent for culture. In the absence of adequate cleaning and heat disinfection, thecultures yielded Acinetobacter baumannii and Bacillus species. Used ventilator tubes yielded S.marcescens, A. baumannii, Enterobacter cloacae and methicillin-resistant S. aureus isolates.
• Isolates 7-13 show genetic relatedness and the identification of a single major clone of S. marcescens from outbreak case samples and ventilator tubing samples from Tygerberg Hospital.
• Isolates 14-15 are closely related strains, with 100% homology, and no visible differences in banding. These isolates were from patients admitted to the paediatric and adult respiratory care units at Tygerberg Hospital during the time of the outbreak.
• Isolates 1-6 and 16 are contemporary isolates from a variety of hospitals in Cape Town. Of theses outliers, 4-5 appear closely related (>95% similarity) but different to the Tygerberg isolates, and are from the neonatal ward at Groote Schuur Hospital in Cape Town.
http://edenprairieweblogs.org/scottneal/post/1338/
1.7
1.3
0.8
1.5
1.2
1.41.5
0.0
1.0
1.3
1.0
1.1
1.3
0.7
1.3
1.3
1.1
2.4
2.1
0.9
1.6
0.0
0.5
1.0
1.5
2.0
2.5
Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep
IR b
y 1
00
0 I
PD
Quarterly rate of S. marcescens isolated from all wards at Tygerberg Hospital
CRUDE INF RATE
20122011
Washer-disinfector
not functional
RESULTS
Ten of the 12 patient isolates were from blood cultures, 1 from an umbilical vascular catheter tip and 1from a tracheal aspirate sample. All cases were low-birth weight infants and mechanical ventilation was anindependent risk factor for S. marcescens infection. The crude patient mortality rate was found to be 4/12(33%).
Patient Specimen Date Site of isolation of
S. marcescens
Mode of ventilation Outcome
1 02 July 2012 Blood CPAP, Intubated Survived
2 02 July 2012 Blood No Survived
3 19 July 2012 Blood CPAP, Intubated Died
4 22 July 2012;
22 July 2012
Blood CPAP, Intubated Died
5 19 September 2012;
01 October 2012
Blood;
CVC tip
CPAP, Intubated Survived
6 27 September 2012 Blood CPAP, Intubated Died
7 02 October 2012 Blood CPAP, Intubated Survived
8 02 October 2012 Blood Intubated Died
9 12 October 2012 Blood CPAP Survived
10 19 October 2012 UVC tip CPAP Survived
11 21 October 2012 Blood CPAP Survived
12 22 October 2012 Tracheal aspirate CPAP, Intubated Survived
Eleven of the 12 cases received assisted ventilation during their hospitalization.
Investigation of the current procedures for re-processing ventilator tubing
revealed inadequate disinfection processes. The source of this infection was
identified to be poorly re-processed ventilator tubing. Most of the washer-
disinfector machines used at the hospital’s Sterile Services Department (SSD)
were not functional since May 2012. The only operational machine had the
temperature inappropriately set to 550C to prevent damage to the plastic tubing.
Suboptimal disinfection practices compounded the problem because the tubing
that was not processed in the washer-disinfector machine, was inappropriately
soaked in Endozime® (not a high-level disinfectant) for 4 hours and hung in a
drier for a further 6 hours prior to packaging and distribution.`
Dice (Opt:2.00%) (Tol 4.0%-4.0%) (H>0.0% S>0.0%) [0.0%-100.0%]
PFGE 1 SpeI
100
95
90
85
80
75
70
PFGE 1 SpeI
13. Du Plessis
16. Jantjies
11. Tawule
14. Williams
15. Ndaza
10. Flepu
01. Nibidyala
02. Filane
03. Markus
04. Spekboom
05. Vent Tubing
06. Fredericks
07. Mabongo
08. Van Der Schyff
09. Persens
12. Mapini
Serratia
Serratia
Serratia
Serratia
Serratia
Serratia
Serratia
Serratia
Serratia
Serratia
Serratia
Serratia
Serratia
Serratia
Serratia
Serratia
marcescens
marcescens
marcescens
marcescens
marcescens
marcescens
marcescens
marcescens
marcescens
marcescens
marcescens
marcescens
marcescens
marcescens
marcescens
marcescens
SCH6196046
STY5037861
SCH5850989
SCH6201798
SCH6278076
STY4981845
STY4939602
STY4931468
STY4965600
STY4984184
STY4975804
STY4985000
STY4983050
STY4985005
STY4983071
SCH5966094
Isolate
1
2
3
4
5
6
7
8
9
10
11
12
13
14
15
16
Investigation of an outbreak of Serratia marcescens on the neonatal and paediatric platform
Catherine M Samuel1, Preneshni R Naicker1, Angela Dramowski2, Magdalena Aucamp2, Shaheen Mehtar2
1. Division of Medical Microbiology, Stellenbosch University, National Health Laboratory Services, Tygerberg Hospital, Cape Town, South Africa
2. Unit for Infection Prevention and Control, Stellenbosch University, Tygerberg Hospital, Cape Town, South Africa
Abbreviations: CPAP, continuous positive airway pressure; CVC, central venous catheter; UVC, umbilical vein catheter
ACKNOWLEDGEMENTS: We thank Dr Colleen Bamford and Dr Clinton Moodley from the Centre for Opportunistic, Tropical and Hospital Infections, National Institute for
Communicable Diseases at Groote Schuur Hospital, for their assistance with the molecular typing.