Embed Size (px)
Citation preview

18
Investigation of AsymptomaticProteinuria in Adults
A National Clinical Guidelinerecommended for use
in
Scotlandby the
Scottish IntercollegiateGuidelines Network
Pilot EditionAugust 1997
Getting validated guidelines into local practice

This guideline was issued in August 1997 and will be reviewed in 1999. Comments areinvited to assist the review process. All correspondence and requests for further backgroundinformation regarding the guideline should be sent to:
Mrs Christina Pottinger, SIGN SecretariatRoyal College of Physicians, 9 Queen Street, Edinburgh, EH2 1JQ
The definitions of the types of evidence and the grading of recommendations used in thisguideline originate from the US Agency for Health Care Policy and Research(1) and are setout in the following tables.

18
Investigation of AsymptomaticProteinuria in Adults
A National Clinical Guidelinerecommended for use
in
Scotlandby the
Scottish IntercollegiateGuidelines Network
Pilot EditionAugust 1997
Getting validated guidelines into local practice

Scottish Intercollegiate Guidelines Network
ISBN 1 899893 75 X
First published 1997
SIGN consents to the copying of this guideline forthe purpose of producing local protocols for use in Scotland
Published by the Scottish Intercollegiate Guidelines Network (SIGN)9 Queen Street, Edinburgh EH2 1JQ
Desktop published by Anne Farquharson, SIGN

Contents
PageSummary of Recommendations
1 Introduction ... ... ... ... 1
2 Definitions ... ... ... ... 2
3 Background ... ... ... ... 3
4 Detection ... ... ... ... 4
5 Diagnosis ... ... ... ... 6
6 Initial Clinical Management ... ... 9
7 Referral ... ... ... ... 10
8 Follow up and Monitoring ... ... ... 11
9 Implementation of the Guideline ... ... 12
10 Development of the Guideline ... ... 14
References ... ... ... ... 17
Quick Reference Guide ... ... ... 19

Summary of Recommendations
Grade
All patients in whom persistent proteinuria is confirmed should beinvestigated
When persistent proteinuria is confirmed, and orthostatic proteinuriaexcluded, a third urine sample or 24-hour sample should be obtainedand sent for laboratory estimation of proteinuria and/or protein:creatinineratio
Initial clinical management should include history taking andexamination with assessment of blood pressure. Blood should bewithdrawn for urea, electrolytes and creatinine estimation, and amidstream urine sample sent for microscopy and culture
Referral for nephrology opinion should be sought if proteinuria is
• >500 mg/l or protein:creatinine ratio >30mg/mmol
• >250 mg/l or protein:creatinine ratio >20mg/mmolwith co-existent raised serum creatinine or hypertension
If the patient has an active urinary tract infection investigations shouldbe repeated, after treatment of the infection, before a referral is made
Patients with co-existent haematuria in the absence of simple urinarytract infection should also be referred initially to a nephrologist
If there is co-existent glycosuria, fasting plasma glucose should bechecked and referral also to a diabetologist considered
Follow up for patients with intermittent proteinuria, or for whomimmediate nephrology referral is not appropriate, should be undertakenafter six months and thereafter annually, to include assessment of bloodpressure, reassessment of proteinuria and estimation of serum urea,electrolytes and creatinine.
Note: These recommendations are based on the finding of asymptomaticproteinuria when urinalysis has been undertaken as part of a generalmedical examination. They are not designed for nor intended to advocatepopulation screening.
C
C
B
C
C
Summary of Recommendations
Grade
All patients in whom persistent proteinuria is confirmed should beinvestigated
When persistent proteinuria is confirmed, and orthostatic proteinuriaexcluded, a third urine sample or 24-hour sample should be obtainedand sent for laboratory estimation of proteinuria and/or protein:creatinineratio
Initial clinical management should include history-taking andexamination with assessment of blood pressure. Blood should bewithdrawn for urea, electrolytes and creatinine estimation, and amidstream urine sample sent for microscopy and culture
Referral for nephrology opinion should be sought if proteinuria is
• >500 mg/l or protein:creatinine ratio >30mg/mmol
• >250 mg/l or protein:creatinine ratio >20mg/mmolwith co-existent raised serum creatinine or hypertension
If the patient has an active urinary tract infection investigations shouldbe repeated, after treatment of the infection, before a referral is made
Patients with co-existent haematuria in the absence of simple urinarytract infection should also be referred initially to a nephrologist
If there is co-existent glycosuria fasting plasma glucose should bechecked and referral also to a diabetologist considered
Follow up for patients with intermittent proteinuria, or for whomimmediate nephrology referral is not appropriate, should be undertakenafter six months and thereafter annually, to include assessment of bloodpressure, reassessment of proteinuria and estimation of serum urea,electrolytes and creatinine.
Note: These recommendations are based on the finding ofasymptomatic proteinuria when urinalysis has been undertaken aspart of a general medical examination. They are not designed fornor intended to advocate population screening.
C
C
B
C
C

1
1 Introduction
1.1 Proteinuria is a cardinal sign of glomerular dysfunction but, whether discoveredas part of routine urine testing or in association with other signs and symptoms, itmay be entirely benign or indicate the presence of significant renal disease. Ineither case the demonstration of persistent proteinuria may affect the lifestyle ofthe sufferer leading to increased insurance premiums or disqualification from anew job.
1.2 Previous studies have shown that many patients with proteinuria have a benignprognosis(2-6) and it is important that investigation is targeted at those who willbenefit most. Unnecessary investigations, particularly if invasive, should beavoided.
1.3 Although there are few proven treatments for many primary renal diseases theidentification of the underlying cause of proteinuria may allow treatment of othersystemic diseases which can afflict the kidneys.
1.4 The purpose of this guideline is to advise on how to investigate and when to referadult patients who are found to have asymptomatic proteinuria at the GP surgery(e.g. during an insurance medical or at a well-person clinic) or outpatient clinic.It does not include recommendations on the treatment of asymptomatic proteinuria.The investigation and referral of pregnant women found to have proteinuria arealso excluded from this guideline.
1.5 The recommendations in this pilot guideline are aimed at general practitionersand general physicians.

2
2 Definitions
2.1 ProteinuriaThe presence of at least + protein on dipstix testing of fresh urine.
The Guideline Development Group has not included nephrotic range proteinuria(>3.5g/24hr) in this guideline because all patients with this degree of proteinuriarequire further investigation, usually including renal biopsy and follow up.
2.2 Functional proteinuriaProteinuria associated with other primary disease states which will resolve withresolution of the primary disease.
If the proteinuria resolves, this is not associated with an adverse prognosis.
2.3 Idiopathic transient proteinuriaProteinuria occurring in children and young adults which will resolvespontaneously over a short period of time and is not present on repeat testing ofurine.
These patients require no further investigation.
2.4 Orthostatic proteinuriaProteinuria associated with upright posture.
This should be excluded by testing the first urine sample passed after overnightrest. These samples will be negative for protein whereas samples taken duringthe day are likely to be positive. This finding is usually associated with a goodprognosis.
2.5 Persistent proteinuriaThe presence of at least + proteinuria on dipstix testing of two separate earlymorning samples of urine collected one week apart.
These patients should be investigated for an underlying cause of the proteinuria.

3
3 Background
3.1 Persistent proteinuria of >150 mg/day can reflect the presence of pathologicalchange within the urinary tract. In certain circumstances urinary protein may beassociated with the over-production of proteins—as in myeloma—or in the activetubular secretion of proteins—as in some uncommon renal tubular diseases.
3.2 The pathology in the renal tract may be localised to the lower urinary tract, whenit is often associated with infection, or may represent inflammatory change withinthe kidneys indicating a nephritic process which may progress to end stage renaldisease.
3.3 It is estimated that of the 80 per million population who are taken onto dialysisfor end stage renal disease in the UK annually, 20% are suffering fromglomerulonephritis.(7) It is possible that earlier recognition of these conditionsmay be associated with delay in the progression of end stage renal disease or maylead to successful treatment of the underlying renal disease.

4
4 Detection
4.1 Detection of proteinuria
4.1.1Stix testingThis is most easily achieved by the use of test strips, such as multistix ordipstix. These will detect most proteins in the urine, especially albumin.The detecting chromophore is tetrabromophenol blue which changes fromyellow-green (–) to blue-green (++++) when viewed against a whitebackground in natural daylight. Bence Jones protein, as found in myeloma,and mucoproteins may not be detected.
Stix testing has been shown to be highly observer dependent and in onerecent study a false positive rate of 40% and false negative rate of 18%were demonstrated despite the use of experienced observers.(8) False positivesfor protein with dipstix can occur with very concentrated urine, in thepresence of gross haematuria, after contamination of urine with antiseptic,or with highly alkaline urine as may occur with some urinary tractinfections.(9)
4.1.2Laboratory testingLaboratory confirmation of stix tests uses a variety of techniques. Eachmethod for protein estimation in urine has drawbacks and advantages andthere is no technique which is completely accurate under all conditions.
Turbidometric assays involve reagent-mediated protein denaturation andmeasurement of the fine suspension by light scatter. The most sensitivereagent is benzethonium in alkali; sulfasalicylic acid overestimates albumin.Dye binding assays involve reaction with anion or ammonium groups suchas Ponceau S or Coomassie blue. The former assay is affected byaminoglycosides and the latter overestimates albumin. Chemical assays arebased on the biuret reaction or folin reagent. Urate can interfere with theseassays and the colour can vary with the aminoacid composition of the protein.
4.2 Detection of albuminuria
4.2.1 Specific measurement of albumin is undertaken in diabetic patients, in whomit indicates the clinical onset of diabetic nephropathy (see SIGN guidelineon management of diabetic renal disease(10)). Two techniques are available:

5
• Radioimmunoassay – this technique is sufficiently sensitive andaccurate to detect microalbuminuria and is reproducible.
• Dye binding – is primarily useful for research, but may also be used inroutine practice as an indicator of possible diabetic nephropathy.
4.2.2Stix testingIt should be remembered that stix testing has a lower limit of sensitivitywhich is above the upper limit of the reference range and urinary albuminlevels can increase up to five fold without an ‘abnormal’ result beingdetected.
From the analytical standpoint the measurement of albumin is preferable tothat of total protein in terms of accuracy of result(11) although this may beoffset by the problem of the inaccuracy of 24-hour urine collections.
4.3 Urinalysis for proteinuria
4.3.1 If any protein is detected in an initial urine specimen, urinalysis should berepeated on at least two further samples at weekly intervals to confirm thepresence of proteinuria. Transient or intermittent proteinuria has been shownto be less important prognostically than persistent proteinuria.(12) If twosubsequent dipstix tests confirm the presence of protein, an attempt shouldbe made to quantify the proteinuria by:
• 24-hour collection or a non-timed mid-stream sample
• protein:creatinine ratio.
4.3.2 Use of protein:creatinine ratio requires only an aliquot of urine which canbe passed at the time of consultation. This has been shown to correct forerrors caused by dilution of a non-timed sample(13) and avoids the problemsof incomplete collection and inconvenience of 24-hour collection.
4.3.3 Persistent proteinuia on dipstix testing of greater than + can, however, betaken as being significant and requires further investigation.

6
5 Diagnosis
5.1 ‘Normal’ proteinuriaThe reference range of proteinuria in healthy adults has been determined as 80 ±24 mg per 24 hours (mean ± SD) with the upper limit being 128 mg/24 hours.(14)
This mostly represents albumin and other plasma proteins, the albumin excretionrate being no more than 20 mg/24 hours. Other proteins which can be detectedinclude Tamm-Horsfall protein(15) and secretory IgA.(16)
Posture and exercise can increase albumin excretion significantly and, therefore,urinary protein excretion up to 150 mg/24 hours—roughly equivalent to aprotein:creatinine ratio <20mg/mmol—is probably not significant.(17) A marathonrunner may, however, transiently excrete as much as 2 mg/min after exercisewithout any obvious long term effects on the kidney.
5.2 Functional proteinuriaFunctional proteinuria may occur in the presence of high fever,(18) strenuousexercise,(19) cold exposure,(20) congestive cardiac failure,(18) emotional stress andhypertension.(21) In all of these cases proteinuria will remit with resolution of theunderlying cause. Only those patients who have persistent proteinuria shouldundergo further nephrological investigation because progressive renal disease isnot seen in the patients in whom proteinuria resolves.
5.3 Idiopathic transient proteinuriaIdiopathic transient proteinuria, which usually occurs in children and young adults,is a benign process.(22) In this condition proteinuria can occur intermittently but isnot consistent and usually resolves with increasing age. It has been suggestedthat most healthy young men have occasional positive proteinuria results if theurine is tested frequently enough.
5.4 Intermittent proteinuriaThe distinction between this entity and idiopathic transient proteinuria is ill-defined, as patients with seemingly transient proteinuria may continuesubsequently to demonstrate intermittent proteinuria. This group has not beenextensively studied but the prognosis for renal function seems to be good overall.Patients in this group have a variety of conditions. On renal biopsy 30% are normalwhereas the rest show interstitial fibrosis or minor definite glomerular changes.(23)
Most of these patients will be free from proteinuria after five years.(11)

7
In the young adult with intermittent proteinuria there is no increase in the risk ofdeath or renal failure compared to age-matched controls. In the older patientintermittent proteinuria is less frequent but it appears that the prognosis is lessgood with an increased risk of death compared to matched controls.(24)
All patients with intermittent proteinuria should be monitored at six monthsand thereafter yearly, with checks on blood pressure, urinalysis, andestimation of serum urea, electrolytes and creatinine until the proteinuriadisappears Grade B, level III (17)
If the proteinuria becomes constant the renal function and blood pressure willrequire close monitoring and referral for a nephrology opinion may becomenecessary (see recommendations for further research, section 10.8).
5.5 Orthostatic proteinuriaOrthostatic proteinuria is defined as abnormal protein excretion which occursonly when the patient is active and upright. A urine sample obtained from thesepatients after overnight recumbency will be negative for protein. If there is doubtit is possible to exclude orthostatic proteinuria by formalised testing using anexercise protocol.
While orthostatic proteinuria is generally associated with a good prognosis(25)
renal biopsy studies in these patients have identified mild nephritic changes inmany, indicating either a co-existent nephritis or recovery from nephritis.(26) Inothers, anatomical variants are thought to be the cause of the proteinuria.(27) Mostof these patients will experience resolution of proteinuria with time, 50% beingin remission at ten years. Some patients do develop persistent proteinuria whichmay indicate the development of significant renal disease.
5.6 Persistent proteinuriaPersistent proteinuria, including nephrotic range proteinuria (>3.5g/24h), isassociated with a higher incidence of mortality both generally and specificallyassociated with renal failure.(23, 24) Various renal lesions are associated with thisproteinuria.(2, 3) Hypertension will develop in 50% of patients with proteinuria(4, 28)
and 20% will develop impaired renal function within ten years of follow up.(29)
For these reasons, such patients should be investigated completely to identifyany potentially treatable problems. The patients who do not have treatable lesionsbut do have significant renal pathology should be followed up regularly to monitorhypertension and renal function.

8
All patients in whom persistent proteinuria is confirmed should beinvestigated Grade C, level IV
When persistent proteinuria is confirmed, and orthostatic proteinuriaexcluded, a third urine sample or 24-hour sample should be sent for laboratoryestimation of proteinuria and/or protein:creatinine ratio
Grade B, level III

9
6 Initial Clinical Management
6.1 Initial assessment and investigation in primary care should include history-takingand examination with assessment of blood pressure, blood and urine analysis.Urine must be tested at least twice to confirm persistent proteinuria.
The following minimum data set applies also to a finding of proteinuria in othercircumstances, e.g. as part of routine investigations on a general hospital ward.
The clinical history from the patient should include:
• Evidence of urinary symptoms suggesting infection, stones or obstruction
• Family history suggestive of familial renal disease including polycystickidneys, reflux nephropathy (chronic pyelonephritis) or hereditarynephritis
• Drug history to exclude nephrotoxic drugs including well recognisedand idiosyncratic reactions e.g. membranous nephritis associated withgold, penicillamine, and captopril; interstitial nephritis associated withmany agents including NSAIDs and penicillins
Examination for hypertension and oedema
Initial investigation should include:
• Urinalysis for haematuria and glycosuria, if not already done
• A fresh mid stream urine sample to be sent for culture and microscopy
• Blood withdrawn for urea, electrolytes, creatinine and glucoseestimation
• Exclude monoclonal gammopathy, especially in patients over 45years, by blood electrophoresis and urinary Bence Jones proteinestimation.
Grade C, level IV
6.2 It may be possible to exclude many benign causes of proteinuria on the basis ofthe clinical history. Benign causes of proteinuria include all causes of functionalproteinuria as listed in section 5.2. Orthostatic and transient proteinuria should beexcluded by repeated examination of the urine for proteinuria.

10
7 Referral
7.1 To ensure that everyone who might have significant renal lesion is investigated,all patients with persistent proteinuria greater than 500 mg/l either on a morningsample or in a 24-hour collection, or a protein:creatinine ratio >30mg/mmol, shouldbe investigated further. This is also true for those patients who are found to haveco-existent hypertension or have abnormal renal function on the biochemicalscreen.
Referral for nephrology opinion should be sought if proteinuria is
• >500 mg/l or protein:creatinine ratio >30mg/mmol
• >250 mg/l or protein:creatinine ratio >20mg/mmolwith co-existent raised serum creatinine or hypertension
If the patient has an active urinary tract infection, investigations should berepeated, after treatment of the infection, before referral is made
Patients with co-existent haematuria in the absence of simple urinary tractinfection should also be referred initially to a nephrologist
If there is co-existent glycosuria, fasting plasma glucose should be checkedand the patient referred also to a diabetologist, if appropriate (see SIGNguideline on the management of diabetic renal disease(10))
Grade C, level IV
In certain circumstances, e.g. a very elderly patient or an isolated rural area, itmay be more appropriate for patients to be seen initially by a general physician orgeriatrician with access to nephrological investigations.
7.2 Nephrological InvestigationInvestigation of patients with persistent proteinuria is likely to include estimationof glomerular filtration rate, urine microscopy for red cells and casts, ultrasoundscanning of the renal tract, and serological screening including detection ofautoantibodies and estimation of complement.
Renal biopsy is likely to be required for patients who have proteinuria greaterthan 2g/day, or for other patients with less significant proteinuria if the glomerularfiltration rate (GFR) is impaired or if there is co-existent haematuria, hypertensionor systemic symptoms or disease.
7.2 Nephrological InvestigationInvestigation of patients with persistent proteinuria is likely to include estimation ofglomerular filtration rate (GFR), urine microscopy for red cells and casts, ultrasoundscanning of the renal tract, and serological screening including detection ofautoantibodies and estimation of complement.
Renal biopsy is likely to be required for patients who have proteinuria greater than2g/day, or for other patients with less significant proteinuria if the glomerular filtrationrate is impaired or if there is co-existent haematuria, hypertension or systemicsymptoms or disease.

11
8 Follow-up and Monitoring
Patients not referred for a nephrological opinion because they have idiopathictransient, orthostatic or intermittent proteinuria, or proteinuria less than 500mg/l,should be monitored at six months and thereafter annually for five years or untilproteinuria is no longer present, whichever is the shorter. Annual assessmentshould include the measurement of blood pressure and serum urea, electrolytesand creatinine, as well as rechecking the degree of proteinuria.
Patients with intermittent proteinuria, or for whom immediate nephrologyreferral is not appropriate, should receive an initial follow-up at six monthsand thereafter annual assessment of blood pressure, reassessment ofproteinuria and estimation of serum urea, electrolytes and creatinine
Grade B, level III for patients with intermittent proteinuria(17)
Grade C, level IV for other patients

12
9 Implementation of the Guideline
9.1 Development of local protocolsIt is expected that the guideline will be adopted after local discussion involvingclinical staff and provider and purchaser management. The Area Clinical AuditCommittee should be fully involved. Local arrangements will then be made forthe derivation of specific local protocols to implement the national guideline inindividual hospitals, units and practices and for securing compliance with them.
This will be done by a variety of means including patient-specific reminders,continuing education and training, and clinical audit.
Service contracts will reflect the arrangements fully along with their related costs.
9.2 AuditThe recommended assessment and investigation strategy at section 6.1 providesa minimum data set for audit purposes.
Outcome audit in general practice might be based on the 5-year follow up, todetermine the proportion of patients:
• not referred for specialist investigation who did not develop renal disease
• referred for specialist evaluation who received an appropriate explanationor diagnosis and an appropriate care plan.
9.3 DisseminationThe guideline will be sent to
• named practitioners in each of the relevant staff groups throughout Scotland
• Chief Executives and Clinical Directors in Trust and other hospitals inScotland
• Board General Managers and Directors of Public Health and other chiefprofessional officers in each Health Board
• Chairmen of Area Clinical Audit Committees and of Area Medical and otherprofessional Advisory Committees
• Local Medical Committees
• Relevant education and training bodies
• Selected others.
9.1 Development of local protocolsIt is expected that the guideline will be adopted after local discussion involvingclinical staff and provider and purchaser management. The Area Clinical AuditCommittee should be fully involved. Local arrangements will then be made forthe derivation of specific local protocols to implement the national guideline inindividual hospitals, units and practices, and for securing compliance with them.
This will be done by a variety of means including patient-specific reminders,continuing education and training, and clinical audit.
Service contracts will reflect the arrangements fully, along with their related costs.

13
9.4 Statement of IntentThis guideline is not intended to be construed or to serve as a standard of medicalcare. Standards of medical care are determined on the basis of all clinical dataavailable for an individual case and are subject to change as scientific knowledgeand technology advance and patterns evolve.
These parameters of practice should be considered recommendations only.Adherence to them will not ensure a successful outcome in every case, nor shouldthey be construed as including all proper methods of care or excluding otheracceptable methods of care aimed at the same results. The ultimate judgementregarding a particular clinical procedure or treatment plan must be made by thedoctor in light of the clinical data presented by the patient and the diagnostic andtreatment options available.
Significant departures from the local protocol should be fully documented in thepatient’s case notes at the time the relevant decision is taken.
A background paper on the legal implications of guidelines, prepared by Dr PamelaAbernethy of Simpson & Marwick W.S., is available from the SIGN secretariat.

14
10 Development of the Guideline
10.1 Responsible bodiesThis pilot guideline was developed by the Royal College of Physicians ofEdinburgh acting on behalf of the Scottish Intecollegiate Guidelines Network(SIGN) and has been accepted by SIGN as the Scottish national guideline fromwhich local protocols should be derived.
10.2 Guideline Development Group
Name Discipline Location
Dr Neil Edward (Chairman) Nephrologist AberdeenDr Michael Jones Nephrologist DundeeDr Michael Boulton-Jones Nephrologist GlasgowDr Allan Cumming Nephrologist EdinburghDr John Dick Biochemical Medicine DundeeDr Garth Dyson General Practitioner EdinburghProfessor Anthony Martin General Practitioner SunderlandDr Stuart Rodger Nephrologist GlasgowDr Charles Swainson Nephrologist Edinburgh
Declarations of interests are held by the SIGN Secretariat.
10.3 Development ProcessThe Group met on five occasions between June 1994 and May 1995. Successivedrafts of the guideline were developed by synthesis of the literature,correspondence and full discussion within the Group and with colleagues inpractice. The draft recommendations were discussed on two occasions at meetingsof the Scottish Renal Association (secretary Dr John Anderton). Details of thedevelopment process and copies of references cited may be consulted at the officesof the SIGN secretariat.
10.4 Systematic reviewThe SIGN Editorial Board recognises that the systematic review undertaken in1994 and 1995 for this pilot edition does not fully meet the requirements of themethodology now prescribed by SIGN and this will be addressed in the firstreview of the guideline.

15
10.5 External ConsultationThe guideline was submitted in draft to the following external referees:
Dr Joe Adu Nephrologist BirminghamProfessor J Stewart Cameron Nephrologist LondonDr Clare Campbell General Practitioner BroxburnProfessor Alex Davison Nephrologist LeedsDr Chris Isles Physician DumfriesDr Brian Junor Nephrologist GlasgowMr Leslie Moffat Urologist AberdeenDr Anthony Nicholls Nephrologist ExeterDr Anthony Rogers Urologist StirlingProfessor Andrew Rees Nephrologist AberdeenDr Alex Watson General Practitioner DundeeProfessor Robert Wilkinson Nephrologist Newcastle
The following also responded to invitations to comment on successive drafts:
Dr James Beattie General Practitioner AberdeenDr Anthony Breslin Public Health GrampianDr Kenneth Harden General Practitioner GlasgowDr Aileen Keel Senior Medical Officer Scottish OfficeDr I G Mackay Nephrologist KilmarnockDr Dorothy Moir Director of Public Health Lanarkshire
10.6 SIGN Editorial BoardThe guideline was reviewed prior to publication by the SIGN Editorial Board:
Professor James Petrie Royal College of Physicians of EdinburghChairman of SIGN
Dr Doreen Campbell CRAG secretariat, Scottish OfficeDr Patricia Donald Royal College of General PractitionersDr Jeremy Grimshaw Health Services Research Unit
University of AberdeenMr Douglas Harper Royal College of Surgeons of EdinburghDr Grahame Howard Royal College of Radiologists
Vice-Chairman of SIGN

16
10.7 Review proceduresThe Scottish Intercollegiate Guidelines Network will have continuingresponsibility for the review and updating of the guideline. The guideline will beformally reviewed in 1999, with increased general practitioner representation onthe guideline development group, and updated with reference to any newinformation which becomes available. Amendments will be disseminated asrequired at that time or, exceptionally, at any other time when significantamendment becomes necessary.
10.8 Recommendations for further researchA number of recommendations in the current guideline are based on clinicalexperience, due to the lack of published evidence. In particular, research is neededto determine:
• what levels of protein loss are significant
• the value of simultaneous measurement of urine creatinine in order to calculatethe protein/creatinine ratio
• if there is benefit in terms of improved patient outcomes resulting from earlyidentification and referral of patients with asymptomatic proteinuria.

17
References
1 US Department of Health and Human Services, Public Health Service, Agency for Health CarePolicy and Research. Acute Pain Management: Operative or Medical Procedures and Trauma.Rockville, The Agency; 1992. AHCPR Pub 92-0038.
2 Von Bonsdorrf M, Koskenvuo K, Salmi HA, Pasternack A. Prevalence and causes of proteinuriain 20-year-old Finnish men. Scand J Urol Nephrol 1981;15: 285-290.
3 Sinniah R, Law CH, Pwee HS. Glomevular lesions in patients with asymptomatic persistent andorthostatic proteinuria discovered on routine medical examination. Clin Nephrol 1977; 7: 1-14.
4 Phillippi PJ, Reynolds J, Yamauchi H, Beering SC. Persistent proteinuria in asymptomaticindividuals: renal biopsy studies on 50 patients. Mil Med 1966; 131: 1311-7.
5 Antoine B, Symvouildes A, Dardenne M. La stabilite evolutive des etats proteinurie permanenteisolee. Nephron 1969; 6: 526-536.
6 Robinson RR. Isolated proteinuria in asymptomatic patients. Kidney Int 1980; 18: 395-406.
7 Wing AJ, Brunner FP. Twenty-three years of dialysis and transplantation in Europe: experiencesof the EDTA Registry. Am J Kidney Dis 1989; 14: 341-346.
8 Kuo VS, Koumantakis G, Gallery ED. Proteinuria and its assessment in normal and hypertensivepregnancy. Am J Obstet Gynecol 1992; 167: 723-8.
9 Fogazzi GB. In: Oxford Textbook of Nephrology Eds Cameron JS, Davison AM, Grunfeld JP,Kerr D, Ritz E. Oxford University p18.
10 Scottish Intercollegiate Guideline Network (SIGN). Management of Diabetic Renal Disease.Edinburgh: SIGN, 1997. (SIGN publication no.11)
11 Shihabi ZK, Koren JC, O’Connor ML. Albuminuria vs urinary total protein for detecting chronicrenal disorders. Clin Chem 1991; 37: 621-4.
12 Levitt JI. The prognostic significance of proteinuria in young college students. Ann Intern Med1967; 66: 685-696.
13 Ginsberg JM, Chang BS, Matarese RA, Garella S. Use of single voided urine samples to estimatequantitative proteinuria. N Engl J Med 1983; 309: 1543-1546.
14 Berggard J. In: Proteins in Normal and Pathological Urine. Eds Manuel H, Betuel H, Revillard JP1970 pp 7-19.
15 Hoyer J, Seiler MW. Pathphysiology of Tamm-Horsfall protein. Kidney Int 1979; 16: 279-289.
16 Bienenstock J, Goldstein G, Tomasi TB. Urinary gammaA rheumatoid factor. J Lab Clin Med1969;73: 389-398.
17 Abuelo JG. Proteinuria in diagnostic principle and procedures. Ann Int Med 1983; 98: 186-191.
18 Reuben DB, Wachtel TJ, Brown P, Driscoll JL. Transient proteinuria in emergency medicaladmissions. N Engl J Med 1982; 306: 1031-1033.
19 Castenfors J, Mossfeldt F, Piscator M. Effect of prolonged heavy exercise on renal function andurinary protein excretion. Acta Physiol Scand 1967; 70 (Pt2): 194-206.
20 Sargent F, Johnson RE. The effects of diet on renal function in healthy men. Am J Clin Nutr1956; 4: 466-481.
3 Sinniah R, Law CH, Pwee HS. Glomerular lesions in patients with asymptomatic persistent andorthostatic proteinuria discovered on routine medical examination. Clin Nephrol 1977; 7: 1-14.

18
21 Pedersen EB, Mogensen CE. Effect of antihypertensive treatment on urinary albumin excretion,glomevular filtration rates and renal plasma flow in patients with essential hypertension. Scand JClin Lab Invest 1976; 36: 231-237.
22 Wolman IJ. Incidence, causes and intermittency of proteinuria in young men. Am J Med Sci1945; 210: 86-100.
23 Von Bornsdorff M, Tornroth T, Pasternack A. Renal biopsy findings in orthostatic proteinuria.Acta Pathol Microbiol Immunol Scand 1982; 90: 11-18.
24 Shintaku N, Takahashi Y, Akaishi K, Sano A, Kuroda Y. Entrapment of left renal vein in childrenwith orthostatic proteinuria. Paediatr Nephrol 1990; 4: 324.
25 Muth RG. Asymptomatic mild intermittent proteinuria: a percutaneous renal biopsy study. ArchIntern Med 1965; 115: 569-574.
26 Gajewski J, Gonzales CI, Rich M. In: Medical Risks 1976 151-156.
27 Rytand DA, Spreiter S. Prognosis in postural (orthostatic) proteinuria: forty to fifty-year follow-up of six patients after diagnosis by Thomas Addis. N Engl J Med 1981; 305: 618-621.
28 King SE. Diastolic hypertension and chronic proteinuria. Am J Cardiol 1962; 9: 669-674.
29 King SE. Albuminuria (proteinuria) in renal diseases. Ann Intern Med 1959; 59: 395-406.

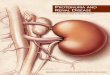
Quick Reference Guide
A B C refers to grade of recommendation
19
If glycosuriapresent, measurefasting plasmaglucose andconsider referralto diabetologist
Measure albuminin diabeticpatients
Persistentproteinuria
Intermittentproteinuria
Follow upRe-check after 6 months, then annual
monitoring until proteinuria disappears
Note: these recommendations for investigation and referral are made solely on the basis that significantpathology may be detected. It is presently unproven whether there is any effect on patient outcomes.
Persistent proteinuria
Referral to nephrologist:v if proteinuria >500mg/l or protein:creatinine >30mg/pmmolv if proteinuria >250mg/l or protein:creatinine >20mg/mmol
with raised serum creatinine or hypertensionv if co-existent haematuria
Initial assessment and investigationv Clinical historyv Examination for hypertension and oedemav Urinalysis for haematuria and glycosuriav Blood analysis for urea, electrolytes,
creatinine, glucose estimationv Exclude urinary tract infection
Laboratory confirmationv 24-hour collection orv protein:creatinine ratio
B
C
Exclude orthostatic, functional, oridiopathic transient proteinuria
Repeat testtwo morning urine samples,
one week apart
Dipstix testingindicates + protein
Intermittent proteinuria
BC
C