Embed Size (px)
Citation preview

6Journal of Neurology, Neurosurgery, anid Psychiatry 1996;60:6-13
NEUROLOGICAL INVESTIGATIONS
Investigation of the neurogenic bladder
Clare J Fowler
Methods of examination which have beenused to investigate the neurogenic bladderinclude tests of bladder function, so-called"urodynamics", and neurophysiological tests
of sphincter and pelvic floor innervation. Apossible consequence of a neurogenic bladder isdamage to the upper urinary tract but theinvestigation of such complications is essen-
tially urological and is only briefly mentionedin this review.
The National Hospitalfor Neurology andNeurosurgery,Queen Square, LondonWC1N 3BG, UKC J Fowler
History of the development ofinvestigationsURODYNAMICSThe term "urodynamics" encompasses any
investigation of urinary tract function althoughit is often used colloquially as a synonym forcystometry. Cystometry, the measurement ofbladder pressure, has been the main tool usedto show abnormal behaviour of the neurogenicbladder.The earliest reference to a study measuring
bladder pressure is commonly given as thepaper by Mosso and Pellacani published in1882.1 With a water manometer they showedthat bladder pressure rose at the start of mic-turition and then gradually declined but thatduring storage the pressure measured withinthe organ gave little indication of what volumeit contained. However, the paper whichdescribed a technique for cystometry produc-ing what is regarded as the precursor of modemday urodynamic recordings was published inBrain in 1933 by Denny-Brown andRobertson2 from the National Hospital forNervous Diseases, Queen Square. By means
of an ingenious system of mirror manometersthey recorded intravesical and intraurethralpressure with two transurethral catheters (oneinside the other), as well as recording rectal,perineal, and abdominal wall pressures inthree neurologically normal men. From theirfindings they defined the physiologicalsequence of processes which occur with blad-der filling, the initiation of micturition, andvoiding to completion.The introduction of cystometry into clinical
practice was gradual and by the 1960s it wasbeing used in only a few specialised urologicalcentres.3 When commercial equipment firstbecame available it consisted of a series of penrecorders which recorded pressure changes as
analogue signals but with the advances inelectronics and development of microchiptechnology the machines have become pro-gressively more complex, more "intelligent",and mostly easier to use. Today measuredpressures are digitised allowing on line, realtime computer analysis of signals.
During the development of urodynamics animportant advance came with the introductionof facilities to record pressure measurementssuperimposed on the fluoroscopic appearancesof the bladder, a "videocystometrogram".This combination provides a complete pictureof the behaviour of the bladder both duringfilling and emptying although it is expensiveand exposes the patient to x rays. Much can belearnt from simple cystometry alone and it isthis investigation which is now a standardfacility in almost every district general hospitalwith a urology department.The hydrodynamic problems of measuring
fluid flow are different from measuring pres-sure within an organ. Introduction of simpleand cheap equipment for measuring urinaryflow rate' has led to this becoming routine;combined with ultrasound measurement ofthe postmicturition residual volume, it pro-vides a simple non-invasive means by whichmuch valuable information can be obtainedabout lower urinary tract function.
NEUROPHYSIOLOGICAL INVESTIGATIONSVarious types of neurophysiological investiga-tion of the pelvic floor and the sphincters havebeen developed over the years. A neurophysio-logical method for recording the bulbocaver-nosus reflex, regarded as clinically valuable inassessing patients with neurogenic bladder dis-orders, was first reported in 1967."Neurophysiological recordings of variouspelvic floor reflexes were much in vogue in the1970s but have since lapsed and have beentransiently replaced by an enthusiasm forrecording the pudendal evoked potential.
Recording from the striated muscle of theurethral sphincter or anal sphincter duringcystometry was first recommended as a meansof detecting inappropriate sphincter contrac-tion during detrusor contraction, the disorderknown as detrusor sphincter dyssynergia.7 Forseveral reasons this type of kinesiologicalEMG is now little used although sphincterEMG performed as a separate neurophysio-
6
on Septem
ber 3, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.1.6 on 1 January 1996. Dow
nloaded from

Investigation of the neurogenic bladder
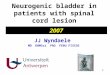
Figure 1 Fillingcystometry in a healthysubject. Vinfus = infusionat 50 mllminute;Pabd = intrabdominalpressure measured by therectal line; Pves =intravesical pressure;Pdet = Pves-Pabd.Respiratory movements,which were not recordedwith the intravesicalpressure measurements,were recorded with therectal pressure line so thatthese appear as an artefactdue to subtraction on Pdet.In the early part of the tracethe subject was asked tocough and the subtractionofPabdfrom Pves wascomplete so that no rise inPdet is recorded.
J ~~~~~~~~~~~~~~~~~~~~~...._......................... ....................... ....................
@. . . . . . @ ; @ @. . . . . . . . . . . . ....
1.... . . . . . . . . . . . . . . .. . . . . . . . . . . . . . . -..
........................................... .................. . @ -*........................
1:13 3:13
Cough
5:13 7:13
Time (min:s)
logical test remains a valuable investigation insome circumstances.
Principle underlying investigationsCYSTOMETRYCystometry is the recording of the pressure-volume relation of the bladder. The intravesi-cal pressure is measured and by subtractingthe intra-abdominal pressure from this figurean estimate of the true pressure produced bythe smooth muscle of the detrusor is obtained.This is best seen by looking at the preparatorystages of cystometric recordings when thepatient is asked to cough (fig 1). Coughingraises the intra-abdominal pressure and thusthe measured intravesical pressure but underphysiological conditions the detrusor does notthen contract so that the derived detrusorpressure (Pdet) remains unchanged or
becomes slightly negative because the intra-abdominal pressure may rise more than theintravesical pressure. To measure the intraves-
ical and intrabdominal pressures a finecatheter is passed through the urethra into thebladder and another into the rectum. Thecatheter used to monitor intravesical pressureis passed, together with a somewhat widerdiameter catheter through which the bladder isfilled. Important information is obtained ifdetrusor pressure is measured both during fill-ing and while the patient attempts to mic-turate. In the interests of saving time an
unphysiologically rapid rate of filling of 50ml/min is commonly used in cystometricstudies.
Recently, methods have become availablefor recording bladder pressures over periods ofmany hours and the bladder is left to fill natu-rally, so-called "ambulatory urodynamics".8
In patients with neurogenic incontinencethe commonest finding is of an abrupt rise indetrusor pressure which the patient is unableto suppress and which is usually accompaniedby reports of urinary urgency (fig 2). If thepatient is recognised as having a neurological
Figure 2 Detrusorhyperreflexia in a womanwith multiple sclerosis.Afterfilling to 100 ml(vinfus) there was adetrusor contraction whichresulted in a pressure rise of90 cm H20.
............. ,i.
~~~~~~~~~~~~~~~. . . . .... ... .. . ...... .....--*-.....t*t* ---- -*v* @@*-~~~~~~~~~~~~~~......:1*\...''.''''..'........
@o@@@@v**-**-*vv*s~~~~~~~~~~~. . . . . . . . . . . .
1:02 2:02 3:02
Time (min:s)
4:02
. . . . . . . .
Q r
..... .. .5 m Is* . . . . . . .
Vinfus100 ml
Pves10 cm H20
Pdet10 cm H20
Padb10 cm H20
5:02
Pves10 cm H20
Pdet10 cm H20
Pabd10 cm H20
Vinfus100 ml9:13
7
. :I I I . :
. . . :
. . . . . . :I I I I I I I I :h.
. . . .
. . . .
. . . . .
I . . . . . . .
. . . . . . .
I I I . . I I I
. . . . . .
--A-P%&amLm&A-
. . . . . .
. . . . .
. . . . . .
. . .
. . . . .
I .
. . .
. .
.
. . .
. . .
. . . .
. .
.
. . . .
. . . . . . .
. . . . . . . .
. . .
. . . . .
. . .
. . . . . . . . . .
............
. . . . . . . . . :
. . . . . . . . . .
. . . . . . . . . .
. . . . . . . . .
. . . .
. . . . . .
. . . . . . .
. . . . . .
. . . . . . . . .
. . .
. . . .
A ...
on Septem
ber 3, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.1.6 on 1 January 1996. Dow
nloaded from

Fowler
Figure 3 Abramsnomogram. Using valuesfor the maximalflow(Qmax) and thecorresponding voidingdetrusor pressure (Pdet) apoint can be plotted on thenomogram that determineswhether the bladder outlet isobstructed, unobstructed, orequivocally obstructed.
aIE-0
CL
100 -
80 -
60 -
40 -
20 -
0-)
Obstructed
Equivocal Unobstructed/ 1
5 10 15 20Qmax (ml/s)
condition, this is called "detrusor hyper-reflexia", the condition is otherwise referred toas "detrusor instability"9-the cystometricchanges in the two conditions being indistin-guisable. The cause of detrusor instability isunknown but the weight of opinion is shiftingfrom thinking that it has a psychogenic causeor is due to an occult neurological lesion to theview that it may be due to a disorder of thedetrusor muscle itself.'0 Likewise the causes offailure of bladder emptying cannot be identi-fied from cystometry, and urological and neu-rological disorders can cause indistinguishablecystometric abnormality. Because bladderbehaviour cannot always be predicted from thepatient's history it has been argued that urody-namic investigations are important in theinvestigation of urinary complaints but thefailure of urodynamics to provide anythingmore than a description of bladder dysfunc-tion has not been properly acknowledged.
This has resulted in a large body of medicalliterature in which patients are classifiedaccording to their urodynamic findings ratherthan by the underlying pathophysiologicalcause and diagnosis.
In patients with suspected obstruction ofoutflow, particularly men with prostatic hyper-trophy, measurement of detrusor pressureduring voiding is important. This, togetherwith urinary flow rate provides informationabout the outflow tract" and an estimate ofthe presence of obstruction can be made(fig 3).
UROFLOWMETRYUroflowmetry is the measurement of urinaryflow rate. This is a non-invasive investigation.The patient presents with a full bladder andvoids into a receptacle in the base of which is aspinning wheel. Urinary flow slows the rate ofrotation and from this a graphical output offlow rate can be obtained (fig 4).
Abnormalities of flow can be due to localurological problems such as prostatic hyper-trophy, a urethral stricture, or neurogenic dis-orders of the bladder outlet mechanism.Detrusor sphincter dyssynergia, which occurswith spinal cord disease, is a common exampleof this and results in interrupted flow (fig 5).Uroflowmetry combined with ultrasoundscanning of the postmicturition residual vol-ume is used as a screening test to exclude seri-
Figure 4 Uroflowmetry.The lower trace shows therate of urinaryflow, whichreaches a maximum of 40mlls in three seconds andthen declines. The uppertrace is the result ofintegrating the flow rateand shows that a total of275 ml was passed.
Figure 5 Uroflowmetryin a patient with multiplesclerosis. He wasparaparetic and hadfrequency and urgency butalso symptoms of difficultyvoiding and was shown tohave incomplete bladderemptying. This interruptedflow pattern is the result ofcontractions of the striatedurethral sphincter occumngduring the detrusorcontraction that is,"detrusor sphincterdyssynergia ".
. . . . . . . .
. . . . . . . .
. . . . . . . .
. . . . . . . .
. . ..' ,....
. . .. .. ..
. ... .*.. ...--w. . . -
4 14 24 34
Vu ro100 ml
Qura5 ml/s
44
Time (s)
50 ml/s flow rate :: ::~~~~~~~~~~~~~...........................................................................
.............................................. ............... ................~~~~~.10 20 30 40 50 60 70 80 90
....................................................................................................................................-..............................I -I................ ;-.ar.
8
: . . . . . . . . . :I I I I I I I I I :. . . . . . . . . :I I I I I I I I I :. . . . . . . . . :I I I I I I I I I :
. . . . . . . . :---d
. . . . . . . . .
. . . . . . . .
. . . . . . . . .
. . . . . . . . .
. . . . . . .
. . . . . . . . .
. . . . . . . .
. . . . . . . . .
. . . . . . . . .
. . . . . . . . .
. . . . . . . . .
. . . . . . . . .
. . . . . . . . .
. . . . . . . . .
. . . . . . . . .
. . . . . . . . .
. . . . . . . . .
. . . . . . . . .
. . . . .
. . . .
:I I . . . . . . .
:. . . . . . . .
:I I I . . . . . .
-------------
. . . . . . . . .
. . . . . . . . . . . . . . . .
........ .........
......... ......... .........
. . . . . . . . . . . . . . . . . . . . . . .
. . . . . . . . .
. . . . . . . . .
. . . . . . . . .
. . . . . . . . .
. . . . . . . . .
. . . . . . . . .
. . . . . . . . .
. . . . . . . . .
. . . . . . . . .
. . . . . . . . .
. . . . . . . . .
on Septem
ber 3, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.1.6 on 1 January 1996. Dow
nloaded from

Investigation of the neurogenic bladder
ous outflow obstruction and can also provideinformation for planning bladder managementin patients with neurological disease.
ULTRASOUND SCANNING OF THE URINARY
TRACTThe residual volume left after voiding isimportant, and can readily be measured with a
small inexpensive ultrasound scanner. Greatprecision is not needed it is simply enough toknow whether there is more or less than 100ml an obvious abnormality on ultrasoundscanning which does not need great expertiseto recognise. Most scanners have cursors thatcan be placed on the black outline of the urinein the bladder and from this, assuming a
spherical shape to the bladder, bladder volumecan be calculated.
Ultrasound scanning has largely overtakenintravenous urography as the method ofchoice to examine the upper renal tract todetect dilatation but intravenous urographyremains the preferred method to look forureteric stones. With modern, highly complexthree dimensional scanning, details of thestructure of the lower urinary tract can
be made out.'2 This has exciting possibilitiesfor both urologists and urogynaecologists.
NEUROPHYSIOLOGICAL INVESTIGATIONS OF THE
SPHINCTERS AND PELVIC FLOOR
Clinical neurophysiological techniques forexamining the pelvic floor have been used formany years. These studies have greatlyenhanced our understanding of the physiologi-cal and pathophysiological mechanisms ofneural control of the lower urinary tract.The first neurophysiological measurements
made were of sacral reflexes starting with thebulbocavemosus reflex.6 '1 To record thisreflex either a surface or a needle electrode wasplaced over or in the bulbocavemosus muscleand electrical stimuli were applied to the dorsalnerve of the penis. The time taken for thereflex contraction of the muscle to occur afterthe stimulus was measured. After the intro-duction of this technique various other pelvicfloor reflex contractions were recorded14 and itwas shown that equally useful responses couldbe obtained by recording from the urethral or
anal sphincter or other parts of the striatedmuscle of the pelvic floor.') 1'It was arguedthat abnormalities of the sacral roots, bothefferent and afferent, would lead to a delay inthis reflex and this did indeed prove to be thecase in patients with established cauda equinalesions.'3 18 19 However, it was found that reflexresponses could still be elicited in patients withpartial cauda equina lesions20 and more impor-tantly these tests were of little value whenapplied to patients with uncertain neurologicallesions presenting with hypocontractile blad-ders or impotence. The explanation for this isprobably that, as with other reflexes measuredusing clinical neurophysiological techniques,only the responses mediated by large myeli-nated fibres are recorded. The small myeli-nated or unmyelinated fibres which eitherinnervate the smooth muscle or constitute thefunctionally important afferent nerve supply of
the region are not tested. Possibly tests of theautonomic innervation of the genital regionwill prove more useful.2'
Recording the pudendal evoked potential issimilar to recording tibial evoked potentials.The same cortical recording electrodes can beused and it is advisable to record the tibialevoked responses first to familiarise the patientwith the technique. The patient is then askedto hold the stimulating electrode on the dorsalnerve of the penis or clitoris and a similarnumber of stimuli as needed for obtaining thetibial evoked potentials are given. Surprisinglythe latency of tibial and pudendal responses issimilar despite the difference in conductiondistance. This is thought to be due to theslower conduction velocity of the pudendalafferents compared with fast conducting muscleafferents which respond when the tibial nerveat the ankle is stimulated.22The introduction of a method to record the
pudendal evoked potential was initially hailedas promising.23 It was considered that thiswould provide a means of testing the afferentinnervation from the sacral region and cer-tainly the responses were delayed in patientswith conditions such as multiple sclerosis.2426Like the lower limb somatosensory evokedpotentials, the pudendal evoked potential isdelayed if there is spinal cord disease but thisis also usually apparent on clinical examina-tion. Recent studies have shown that thepudendal evoked potential is very rarelyabnormal unless there are other clinical signsof neurological disease27-29 and furthermore ifthe lesion is predominantly unilateral thepudendal evoked potential can be within nor-mal limits.29 It seems that there is little diag-nostic gain in recording the pudendal evokedpotential although it is sometimes reassuringto show that it is normal in patients in whomneurological problems are suspected.A technique for measurement of the termi-
nal motor latency of the pudendal and perinealnerves (PTML) was devised at St Mark'sHospital.30 It has been used to show patho-physiological changes in these nerves inwomen with faecal,30 urinary,3 or doubleincontinence.32 The pudendal nerve is stimu-lated transrectally near the ischial spinethrough the wall of the rectum using an elec-trode mounted on the tip of the examiner'sfinger. An electrode is mounted at the base ofthe finger, which records from the anal sphinc-ter, and a ring electrode mounted on a Foleycatheter can be used to record from the peri-urethral striated muscle. The latency of theresponse has been found to be prolonged inwomen with urinary stress incontinence afterchildbirth and women with faecal inconti-nence due to sphincter weakness. It is thoughtthat stretching of the nerves during parturitionand also with straining at defaecation inchronic constipation results in pudendal nerveinjury.33 Although of considerable researchvalue this test is not used in the routine assess-ment of women with urinary stress inconti-nence, nor has it proved to be as useful aselectromyography of the anal sphincter in theassessment of faecal incontinence.34
9
on Septem
ber 3, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.1.6 on 1 January 1996. Dow
nloaded from

Fozuler
Electromyography (EMG) of the striatedmusculature of the pelvic floor is of value inrecognising changes of denervation andchronic reinnervation in patients with caudaequina lesions as well those with suspectedmultiple system atrophy. A single fibre needlemay be used to show changes in fibre density3'or a concentric needle electrode to showchanges in configuration of individual motorunits which result from reinnervation.36The striated muscles of the sphincters are
innervated by anterior horn cells that lie inOnuf's nucleus in the sacral part of the spinalcord. Neurophysiological studies showed lossof cells in Onuf's nucleus in patients dyingwith Shy-Drager syndrome.7 These pathologi-cal changes may be reflected in abnormalitiesof sphincter EMG in life. This was first shownby Sakouta et aP8 and then in a systematicstudy by Kirby et al.39 Sphincter EMG is nowused to distinguish between patients withbladder symptoms and multiple system atro-phy and atypical parkinsonism and those withidiopathic Parkinson's disease,404' and a uro-logical disorder as in the first conditionchanges of reinnervation can be found whichare not present in the second. Changes of rein-nervation in multiple system atrophy are non-specific and some caution must be exercised ininterpreting EMG findings in multiparouswomen or patients who have had extensivepelvic surgery. However, the changes whichoccur in the motor units in multiple systematrophy are so extreme as to make the test reli-able and robust.
Using a concentric needle electrode 10 dif-ferent motor units are recorded from either theurethral or anal sphincter, the anal sphincterbeing more accessible and therefore lessuncomfortable for the patient but equally valu-able for giving a significant result. The meanduration of the 10 motor units is measured aswell as the number of units which exceed 10ms in duration. In multiple system atrophy,some motor units remain of normal duration,but others become excessively prolonged. Bycontrast with this-for example, after multipledeliveries all the units might be mildly pro-longed. The values used to define normal are amean duration of less than 8-5 ms and lessthan 20% of units having a duration of lessthan 10 ms.40 A mean duration of more than10 ms is highly abnormal and suggestive ofmultiple system atrophy but there is inevitablyan area of uncertainty when the mean value isless than this.The other condition in which urethral
sphincter EMG has proved to be of particularvalue is in the investigation of young womenwith urinary retention.42 These patients haveno neurological signs on clinical examinationand in particular no evidence of spinal corddisease.43 It was previously suggested that theywere either presenting with urinary retentionas the first symptom of multiple sclerosis orthat they had a hysterical disorder. The first isnow easy to disprove as imaging and neuro-physiological investigation in these womenshow no appropriate abnormality. SphincterEMG shows a myotonic-like activity which
has been called "complex repetitive dischargesand decelerating bursts".'" Detailed EMGanalysis of this activity, measuring the jitter ofthe component potentials, has shown that incommon with other complex repetitive dis-charges, it is due to ephaptic transmissionbetween muscle fibres"' and it has been sug-gested that it is this activity which can berecorded as a continuous phenomenon whichprevents the muscle from relaxing. The stri-ated muscle of the urethral sphincter is a cir-cularly placed horseshoe-like structure and itis not difficult to see how a failure of it to relaxwould result in either obstructed voiding orurinary retention. Why the abnormal activityshould develop remains unknown but it is notuncommon for women with urinary retentionto have clinical features of polycystic ovaries. 15
A speculative hypothesis is that the striatedmuscle of the urethral sphincter, being hor-monally sensitive, undergoes a breakdown inmembrane stabilisation secondary to the per-vading hormonal abnormality of polycysticovary syndrome allowing ephaptic transmis-sion between muscle fibres to occur.Unfortunately no specific treatment has yetbeen effective and the women manage best byperforming intermittent self catheterisation.A similar abnormality has not been found in
men and extensive neurophysiological testinghas failed to show a defect in the less com-monly encountered young men with urinaryretention without a urological explanation.The role of primary detrusor abnormality inthese men needs to be explored as it does inpatients with idiopathic detrusor instability.Unfortunately there is as yet no neurophysio-logical means of investigating detrusor smoothmuscle function.
Planning investigationsInvestigations of bladder symptoms are carriedout for two very different purposes: with blad-der symptoms and established neurologicaldisease urodynamic investigations may be per-formed to try and understand the pathophysio-logical basis for the patient's symptoms andobtain information on which to base recom-mendations for management of incontinence.When the question is being asked "is this a
neurogenic bladder?" a different approach isrequired. In this instance investigations are ofa neurological or neurophysiological nature.
URODYNAMIC INVESTIGATIONS IN PATIENTSWITH ESTABLISHED NEUROLOGICAL DISEASEPoor bladder control is a common and trou-blesome feature of many types of neurologicaldisease, especially of the spinal cord. Thecommonest complaints are of urgency, fre-quency, and urge incontinence and in estab-lished neurological disease these can beassumed to reflect detrusor hyperreflexia.However, patients with neurogenic bladderdisorders often have a disorder of emptying aswell; incomplete emptying is probably due to acombination of detrusor sphincter dyssynergiaand poorly sustained detrusor contractions. Ifthe bladder does not empty completely the
10
on Septem
ber 3, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.1.6 on 1 January 1996. Dow
nloaded from

Investigation of the neurogenic bladder
persistent postmicturition residual volume actsas a stimulus for repeated detrusor contrac-tions so that efforts to treat detrusor hyper-reflexia are unlikely to succeed until effectiveemptying is achieved. The most effective treat-ment for detrusor hyperreflexia is an anti-cholinergic drug (oxybutynin is currentlyrecommended) but there is no oral medicationwhich improves neurogenic voiding disordersand the best management is intermittentcatheterisation, performed by the patient orcarer.
In summary the presence of detrusor hyper-reflexia may be reliably deduced from clinicalhistory, but incomplete emptying, althoughcontributing appreciably to the problem, canbe largely asymptomatic. For this reason thesingle most important investigation whenplanning the management of patients withneurogenic incontinence is measurement ofthe postmicturition residual volume. This caneither be done by simple ultrasound (see ear-lier) or by "in-out" catheterisation. Theadvantage of using catheterisation is that itfamiliarises the patient with what is involved inintermittent self catheterisation.
Investigation of the postmicturition residualvolume is recommended before starting on ananticholinergic drug, as shown in the algo-rithm in fig 6. A further point about treatment
Figure 6 Algorithm formanagement ofpatientswith neurogenic bladderdisorders. By following thisboth aspects of bladderdysfunction-incompleteemptying andhyperreflexia-are treated.
with anticholinergic drugs is that althoughthey may be effective in lessening detrusorhyperreflexia they can adversely affect bladderemptying. It is advisable therefore if a patientstarts on these drugs and fails to respond torecheck the postmicturition residual volumeand make sure that this has not significantlyaccumulated.
If the patient has recurrent urinary tractinfections or fails to respond to the regimenoutlined in fig 6, it is advisable to refer thepatient to a urologist who will carry out investi-gations to exclude urinary tract stones or someother structural lesion.
Although cystometry is not critical in theroutine investigation and management ofpatients with neurological disability such asmultiple sclerosis, there are other neurologicalconditions in which measurements of bladderpressure are important. This is particularly thecase in patients with parkinsonian features andbladder symptoms. There must be a highindex of suspicion of multiple system atrophyin such a patient, best investigated by sphinc-ter EMG (see earlier). If, however, sphincterEMG is normal and the disorder seems to beidiopathic Parkinson's disease the question ofprostatic obstruction of outflow in men arisesand full cystometry with a voiding study isessential.
Cystometry is also of value when investigat-ing patients with an uncertain neurologicaldiagnosis who have among their symptomscomplaints of bladder dysfunction. Findingsensory urgency may provide an explanationfor bladder symptoms without suggesting aneurogenic basis.
IS THIS A NEUROGENIC BLADDER?The role of urodynamics in trying to decide if apatient has a neurogenic bladder disorder islimited. In most patients sent by urologists toneurologists, filling cystometry has disclosedbladder overactivity. In this instance the neu-rologist must try to confirm or refute thatthere is a neurological basis for the problem.Foremost in the patient's assessment is theclinical neurological examination.
The clinical neurological examinationThe neural organisation of control of bladderfunction is widely distributed throughout theneuraxis. The neural programmes whichdetermine whether the bladder is in storage orvoiding mode exist in centres in the dorsaltegmentum of the pons.46 For these pro-grammes to be effected there must be intactconnections between the sacral part of thespinal cord, which is the level of efferent andafferent neural connections to the lowerurinary tract, and the pons. Spinal cordabnormality is therefore a common causeof neurogenic bladder dysfunction. The influ-ence of higher centres and particularly inputfrom the mesial frontal lobes is thought tobe important in modulating the activity ofthe pontine micturition centres and thereis probably also input from other supra-pontine regions although these have beenless clearly defined. Thus any lesion between
I11
on Septem
ber 3, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.1.6 on 1 January 1996. Dow
nloaded from

12
the frontal lobes and the sacral part of thespinal cord is likely to result in bladder dys-function.
Because of the relative levels at which theinnervation of the lower limbs and the bladderarise, it is unusual to have a lesion between thepons and the sacral part of the cord giving riseto a neurogenic bladder that does not also pro-duce signs of an upper motor neuron lesion inthe lower limbs. This is undoubtedly the casein patients with multiple sclerosis47 but it alsoseems to hold for most other instances ofspinal abnormality unless the lesion is verysmall and intramedullary. A predictableexception to this rule might be expected from aconus or cauda equina lesion affecting onlyS2-S4. It seems, however, that even with suchextreme caudal lesions there are usually neuro-logical abnormalities in the lower limbs andfoot deformities may be present if the problemhas been of long duration.
Brain stem or pontine abnormalities givingrise to bladder dysfunction often cause otherneurological deficits but occasionally a lesioncan be sufficiently dorsal and discrete to pro-duce predominantly a defect of bladder func-tion.48 An internuclear ophthalmoplegia is afrequent additional sign, due presumably tothe proximity of the median longitudinal fasci-culus.The contribution of suprapontine disease to
neurogenic bladder dysfunction, with theexception of areas in the frontal lobes, ispoorly defined. Patients with incontinence dueto lesions of the frontal lobe usually have pro-found neuropsychological impairment includ-ing a change of personality but are notindifferent to their incontinence unless therehas been extensive frontal lobe damage.4'Hydrocephalus probably causes bladder dys-function by pressure effects from the dis-tended lateral ventricles on the frontal
501regions.The neurologist may be asked if a patient's
peripheral neuropathy is responsible for blad-der dysfunction. Many forms of neuropathyare length dependent, the maximum deficitbeing evident in the longest fibres whereas thenerve fibres to the bladder are comparativelyshort. For the innervation of the bladder tohave been affected as part of a generalisedneuropathy there should be clinical evidenceof extensive disease with loss of both knee andankle jerks and sensory impairment in smallfibres to a level well above the ankles. Even ifthe neuropathy is selective for small fibressymptomatic bladder involvement occurs rela-tively late and only in patients with other pro-found neuropathic symptoms.
Imaging of the nervous systemFrom the preceding section emphasising thevalue of clinical examination, it is apparentthat there are regions of the CNS where alesion can cause bladder symptoms and yetproduce only minor or equivocal physicalsigns. Imaging is particularly indicated toexclude a suprapontine abnormality or a sub-sacral cauda equina lesion. Magnetic reso-nance imaging of the lower cord and cauda
equina has replaced myelography as the inves-tigation of choice for imaging this region.51 Itseems that a congenital malformation of thelower spinal cord such as a tethered cord can-not be excluded by a plain radiograph as vari-ous forms of dysrraphism can occur withoutspina bifida.
Pelvic floor neurophysiological investigationisThere are two conditions in which neurophys-iological investigations can disclose an abnor-mality that might not otherwise be evident.
If there are any other neurological featuressuch as parkinsonism, cerebellar ataxia, pos-tural hypotension, or symptoms suggestinglaryngeal stridor, a diagnosis of multiple sys-tem atrophy should be considered.52 SphincterEMG has proved a valuable test in detectingthis disorder by showing pronounced changesof denervation and reinnervation in the motorunits (see earlier).
In young women with bladder disturbancebut no other convincing neurological deficit,EMG of the urethral sphincter may show themyotonic-like activity, decelerating bursts, andcomplex repetitive discharges described ear-lier.12 Even if sphincter EMG is not available,in a young woman with urinary retention sim-ply indicating an absence of spinal cord signson clinical examination makes a diagnosis ofmultiple sclerosis, a condition otherwise likelyto be considered as the cause, highly improba-ble.
ConclusionThe difficulty that neurologists have had withinvestigating the neurogenic bladder stemsfrom a combination of factors: the range of pre-senting symptoms is limited to either inconti-nence or retention, it is not possible to examinethe bladder clinically, and the impression thaturodynamics may prove a "diagnosis" hasobscured the fact that there are many bladderdisorders of unknown cause. Finally there hasbeen the neurologists' reluctance to becomeinvolved in the management of incontinence.In bladder dysfunction established neurologicaldisease should be regarded as an essentiallyneurological symptom and investigated andmanaged appropriately. Bladder symptoms areamong the most treatable of neurologicaldeficits and are an unpleasant and troublesomeburden for the patient and their carer.
In patients sent from urologists to neurolo-gists the emphasis should be on excludingspinal cord disease, which can be readily doneby clinical examination. A high index of suspi-cion for multiple system atrophy should bemaintained for older patients as this is a neu-rological disease which can present with blad-der dysfunction and the patients do not benefitfrom urological surgery.
1 Mosso A, Pellacani P. Sur les fonctions de la vessie.Arc/lives Itali'nnes ds Biologic 1882;i:98-128.
2 Denny-Brown D, Robertson E. On the physiology of mic-turition. Brain 1933;56:149-90.
3 Scott FB, Quesada EM, Cardus C. The use of combineduroflowmetry, cystometry and electromyography in evalu-ation of neurogenic bladder dysfunction. In: Boyarsky S,ed. The neuirogeniic bladder. Baltimore: Williams andWilkins, 1967:106-14.
Fowler
on Septem
ber 3, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.1.6 on 1 January 1996. Dow
nloaded from

Investigation of the neurogenic bladder
4 Bates CP, Whiteside CG, Turner-Warwick R.Synchronous cine-pressure flow cystourethrography. Br]7Urol 1970;42:714-23.
5 Christmas T, Chapple C, Rickards D, et al. Contemporaryflow meters: an assessment of their accuracy and reliabil-ity. Br]7 Urol 1989;63:460-1.
6 Rushworth G. Diagnostic value of the electromyographicstudy of reflex activity in man. Electroencephalogr ClinNeuirophysiol 1967;25:65-73.
7 Blaivas JG, Sinha HP, Zayed AAH, et al. Detrusor-externalsphincter dysynergia: a detailed electromyography study.]Urol 1981;125:545-8.
8 Griffiths C, Assi M, Styles R, et al. Ambulatory monitoringof bladder and detrusor pressure during natural filling.Urol 1989;142:780-4.
9 International Continence Society. Fourth report on thestandardisation of terminology of lower urinary tract. Br. Urol 1981;53:333-5.
10 Brading AF, Turner WH. The unstable bladder: towards acommon mechanism. Br]r Urol 1994;73:3-8.
11 Abrams P, Griffiths D. The assessment of prostaticobstruction from urodynamic measurements and fromresidual urine. Br] Urol 1979;51:129-34.
12 Ng K, Gardener J, Rickards D, et al. Three-dimensionalimaging of the prostatic urethra-an exciting new tool. Br] Urol 1994;74:604-8.
13 Ertekin C, Reel F. Bulbocavernosus reflex in normal menand in patients with neurogenic bladder and/or impo-tence. Neurol Sci 1976;28:1-15.
14 Bradley WE. Urethral electromyelography. ] Urol 1972;108:563-4.
15 Bilkey WJ, Awad EA, Smith AD. Clinical application ofsacral reflex latency. ] Urol 1983;129:1187-9.
16 Vodusek EB, Janko M, Lokar J. Direct and reflex responsesin perineal muscles on electrical stimulation. ] NeurolNeurosurg Psychiatry 1983;46:67-71.
17 Varma JS, Smith AN, McInnes A. Electrophysiologicalobservations on the human pudendo-anal reflex. ] NeurolNeurosurg Psychiatry 1986;49: 1411-6.
18 Bradley WE, Timm GL, Rockswold GL, Scott FB.Detrusor and urethral electromyelography. ] Urol1975;114:891-4.
19 Krane RJ, Siroky MB. Studies on sacral-evoked potentials.]Urol 1980;124:872-6.
20 Blaivas JG, Zayed AAH, Labib KB. The bulbocavernosusreflex in urology: A prospective study of 299 patients.] Urol 1981;126:197-9.
21 Ertekin C, Almis S, Ertekin N. Sympathetic skin potentialsand bulbocavernosus reflex in patients with chronic alco-holism and impotence. Eur Neurol 1990;30:334-7.
22 Guerit JM, Opsomer RJ. Bit-mapped imaging ofsomatosensory evoked potentials after stimulation of theposterior tibial nerves and dorsal nerve of the penis/cli-toris. Electroencephalogr Clin Neurophysiol 1991 ;8:228-37.
23 Haldeman S, Bradley WE, Bhatia N, et al. Pudendalevoked responses. Arch Neurol 1982,39:280-3.
24 Haldeman S, Glick M, Bhatia NN, et al. Colonometry, cys-tometry, and evoked potentials in multiple sclerosis. ArchNeurol 1982;39:698-701.
25 Kirkeby HJ, Poulsen EU, Petersen T, et al. Erectiledysfunction in multiple sclerosis. Neurol 1988;38:1366-71.
26 Eardley I, Nagendran K, Lecky B, et al. The neurophysiol-ogy of the striated urethral sphincter in multiple sclerosis.Br]7 Urol 1991;67:81-8.
27 Kunesch E, Reiners K, Muller-Mattheis V, et al.Neurological risk profile in organic erectile impotence.]Neurol Neurosurg Psychiatry 1992,55:275-81.
28 Pickard RS, Powell PH, Schofield IS. The clinical applica-tion of dorsal penile nerve cerebral-evoked responserecording in the investigation of impotence. Br] Urol1994;74:231-5.
29 Delodovici ML, Fowler CJ. The clinical value of thepudendal somatosensory evoked potential is examined.Electroencephalogr Clin Neurophysiol 1995;96:509-15.
30 Kiff ES, Swash M. Normal proximal and delayed distal
conduction in the pudendal nerves of patients withidiopathic (neurogenic) faecal incontinence. ] NeurolNeuirosurg Psychiatry 1984;47:820-3.
31 Snooks SJ, Badenoch DF, Tiptaft RC, et al. Perineal nervedamage in genuine stress incontinence. Br ] Urol1985,57:422-6.
32 Snooks SJ, Swash M, Setchell M, et al. Injury to the pelvicfloor sphincter musculature in childbirth. Lancet1984;ii:546-55.
33 Swash M, Snooks SJ, Henry MM. A unifying concept ofpelvic floor disorders and incontinence. ]f Roy Soc Med1985;78:906-1 1.
34 Cheong D, Vaccaro C, Salanga V, et al. Electrodiagnosticevaluation of fecal incontinence. Muscle Nerve 1995;18:612-9.
35 Neill ME, Swash M. Increased motor unit fibre density inthe external anal sphincter in ano-rectal incontinence: asingle fibre EMG study. ]f Neurol Neurosurg Psychiatry1980;43:343-7.
36 Fowler C. Pelvic floor neurophysiology. In: Osselton J, ed.Clinical neurophysiology. Oxford: ButterworthHienemann, 1995;233-52.
37 Sung JH, Mastri AR, Segal E. Pathology of the Shy-Dragersyndrome. ]f Neuropathol Exp Neurol 1 978;38:253-68.
38 Sakuta M, Nakanishi T, Tohokura Y. Anal muscle elec-tromyograms differ in amyotrophic lateral sclerosis andShy-Drager syndrome. Neurology 1978;28: 1289-93.
39 Kirby RS, Fowler CJ, Gosling J, et al. Urethro-vesical dys-function in progressive autonomic failure with multiplesystem atrophy. 7 Neurol Neurosurg Psychiatry 1986;49:554-62.
40 Eardley I, Quinn NP, Fowler CJ. The value of urethralsphincter electromyography in the differential diagnosisof parkinsonism. Br] Urol 1989;64:360-2.
41 Beck RO, Betts CD, Fowler CI. Genito-urinary dysfunc-tion in multiple system atrophy: clinical features andtreatment in 62 cases. ]f Urol 1994;151:1336-41.
42 Fowler CJ, Kirby RS. Electromyography of the urethralsphincter in women with urinary retention. Lancet1986;i: 1455-6.
43 Fowler CJ, Kirby RS. Abnormal electromyographic activity(decelerating bursts and complex repetitive discharges) inthe striated muscle of the urethral sphincter in 5 womenwith persistimg urinary retention. Br ]f Urol 1985;57:69-70.
44 Fowler CJ, Kirby RS, Harrison MJG. Decelerating burstsand complex repetitive discharges in the striated muscleof the urethral sphincter associated with urinary retentionin women. ]fNeurol Neurosurg Psychiatry 1985;48: 1004-9.
45 Fowler CJ, Christmas TJ, Chapple CR, et al. Abnormalelectromyographic activity of the urethral sphincter, void-ing dysfunction, and polycystic ovaries: a new syndrome?BM] 1988;297:1436-8.
46 de Groat WC. Central neural control of the lower urinarytract. In: Bock G, Whelan J, eds. Neurobiology of inconti-nence. Chichester: John Wiley and Sons, 1990:27-56.(Ciba Foundation Symposium 151.)
47 Betts CD, D'Mellow MT, Fowler CJ. Urinary symptomsand the neurological features of bladder dysfunction inmultiple sclerosis. ] Neurol Neurosurg Psychiatry1993;56:245-50.
48 Betts CD, Kapoor R, Fowler CI. Pontine pathology andmicturition dysfunction. Br] Urol 1992;70:100-2.
49 Andrew J, Nathan PW. Lesions of the anterior frontal lobesand disturbances of micturition and defaecation. Brain1964;87:233-62.
50 Ahlberg J, Norlen L, Blomstrand C. Outcome of shuntoperating on urinary incontinence in normal pressurehydrocephalus predicted by lumbar puncture. ] NeurolNeurosurg Psychiatry 1988;51:105-8.
51 Mathew P, Todd NV. Intradural conus and cauda equinatumours: a retrospective review of presentation, diagnosisand early outcome. ] Neurol Neurosurg Psychiatry1993;56:69-74.
52 Wenning G, Shlomo Y, Magalhaes M, et al. Clinical fea-tures and natural history of multiple system atrophy.Brain 1994;117:835-45.
13
on Septem
ber 3, 2020 by guest. Protected by copyright.
http://jnnp.bmj.com
/J N
eurol Neurosurg P
sychiatry: first published as 10.1136/jnnp.60.1.6 on 1 January 1996. Dow
nloaded from

















![Neurogenic bladder [Dr. Edmond Wong]](https://img.pdfslide.net/doc/110x75/554af038b4c90559058b4779/neurogenic-bladder-dr-edmond-wong.jpg)









