Embed Size (px)
Citation preview

Investor & Analyst Event
ESMO 2017 Presentation
September 2017

Disclaimer
The statements made in this presentation may include forward-looking statements regarding
the future operations of ERYTECH Pharma S.A., including estimates of target market
opportunity, timing of planned clinical trials and results from those trials, regulatory strategy
and timing of planned regulatory submissions, manufacturing capabilities and strategy for
expansion of the ERYCAPS platform. Although we believe that the expectations contained in
this presentation are reasonable, these forward-looking statements are only estimations
based upon the information available to ERYTECH Pharma S.A. as of the date of this
presentation. Except as required by law, we expressly disclaim any responsibility to publicly
update or revise our forward-looking statements, whether as a result of new information,
future events or otherwise. Thus, the forward-looking statements herein involve known and
unknown risks and uncertainties and other important factors such that actual future
operations, opportunities or financial performance may differ materially from these forward-
looking statements. Undue reliance should not be placed on forward looking statements,
which speak only as of the date hereof. All forward-looking statements contained herein are
qualified in their entirety by the foregoing cautionary statement.
2
Agenda
6:30 – 6:40 PM Welcome & Corporate Overview
Gil Beyen, Chairman & CEO
6:40 – 6:55 PM Eryaspase for Pancreatic Cancer
Iman El-Hariry, MD, PhD, CMO
6:55 – 7:20 PM Full Phase 2b Trial Results of eryaspase in Second-Line Metastatic Pancreatic Cancer
Prof. Pascal Hammel, MD, PhD, Principal Investigator
7:20 – 7:25 PM Financial & Operational Update
Eric Soyer, CFO & COO
7:25 – 7:30 PM Next Steps & Milestones
Gil Beyen, Chairman & CEO
7:30 – 8:00 PM Q&A
3

Corporate Overview
Gil Beyen, Chairman & CEO
4

ERYTECH, leveraging red blood cells to improve cancer therapies
Innovative and versatile ERYCAPS technology platform, encapsulating drugs in red blood cells
1
Targeting indications with high unmet medical need, focusing on cancer metabolism
2
Lead product candidate eryaspase (GRASPA®) in late-stage development3
Expansive opportunities in oncology and beyond5
Positive Phase 2b data in pancreatic cancer (PDAC)4
5

ERYCAPS, an innovative and versatile technology platform
Entrapment of drug substance inside donor-derived red blood cellsusing hypotonic/hypertonic stress
Resealing
(hypertonic stress)
Controlled lysis
(hypotonic stress)
Proprietary ‘osmoticfragility’ process ensuresrequired amount of drugin each RBC batch
Molecules from 1 to 500 kDalton (peptides, enzymes, antigens, ...)
Protected by 13 patent families
Industrialized in commercial scale GMP manufacturing facility
6
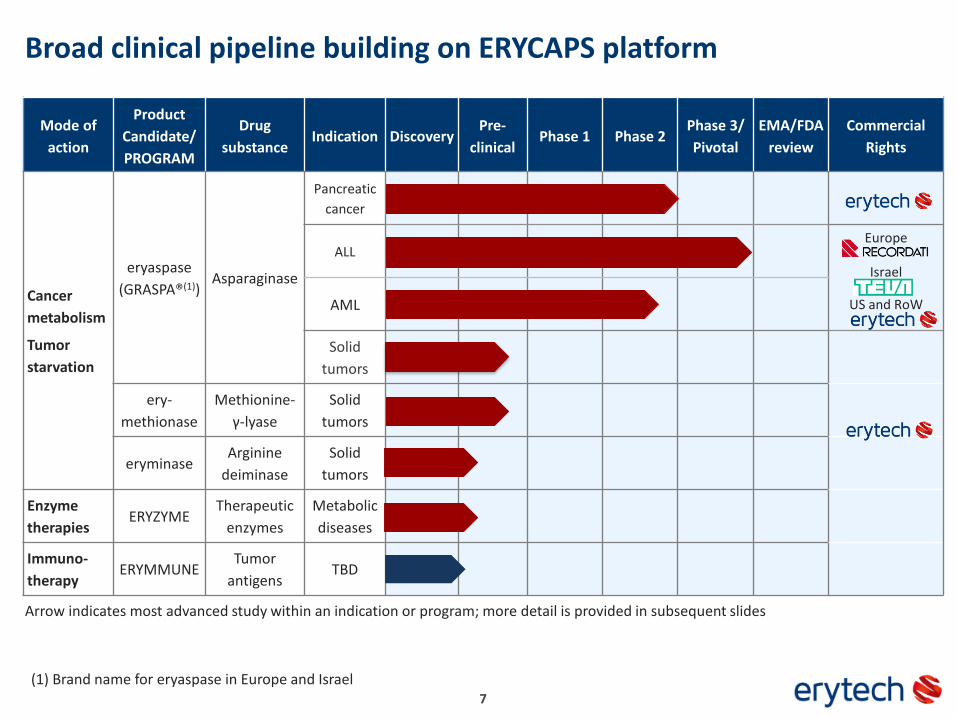
Broad clinical pipeline building on ERYCAPS platform
Mode of
action
Product
Candidate/
PROGRAM
Drug
substanceIndication Discovery
Pre-
clinicalPhase 1 Phase 2
Phase 3/
Pivotal
EMA/FDA
review
Commercial
Rights
Cancer
metabolism
Tumor
starvation
eryaspase
(GRASPA®(1))Asparaginase
Pancreatic
cancer
ALLEurope
Israel
US and RoWAML
Solid
tumors
ery-
methionase
Methionine-
γ-lyase
Solid
tumors
eryminaseArginine
deiminase
Solid
tumors
Enzyme
therapiesERYZYME
Therapeutic
enzymes
Metabolic
diseases
Immuno-
therapyERYMMUNE
Tumor
antigensTBD
(1) Brand name for eryaspase in Europe and Israel7
Arrow indicates most advanced study within an indication or program; more detail is provided in subsequent slides

Eryaspase for Pancreatic Cancer
Iman El-Hariry, MD, PhD, CMO
8
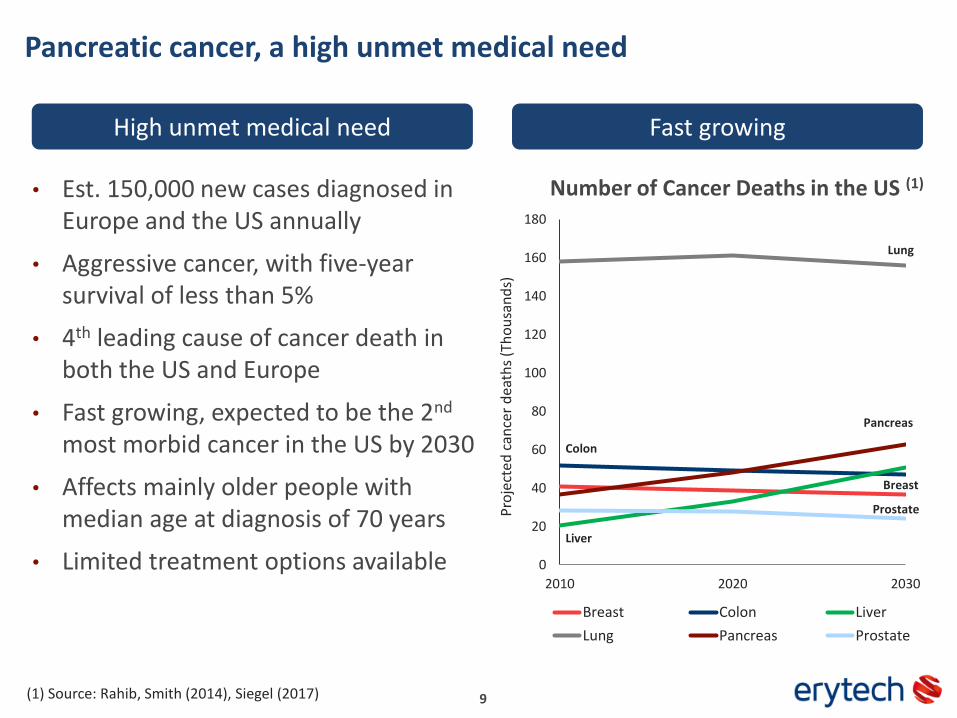
Pancreatic cancer, a high unmet medical need
0
20
40
60
80
100
120
140
160
180
2010 2020 2030
Cancer mortality rates in the US
Breast Colon Liver
Lung Pancreas Prostate
Pro
ject
ed c
ance
r d
eath
s (T
ho
usa
nd
s)
Pancreas
• Est. 150,000 new cases diagnosed in Europe and the US annually
• Aggressive cancer, with five-year survival of less than 5%
• 4th leading cause of cancer death in both the US and Europe
• Fast growing, expected to be the 2nd
most morbid cancer in the US by 2030
• Affects mainly older people with median age at diagnosis of 70 years
• Limited treatment options available
Lung
Colon
Breast
Liver
Prostate
Number of Cancer Deaths in the US (1)
Fast growingHigh unmet medical need
(1) Source: Rahib, Smith (2014), Siegel (2017) 9
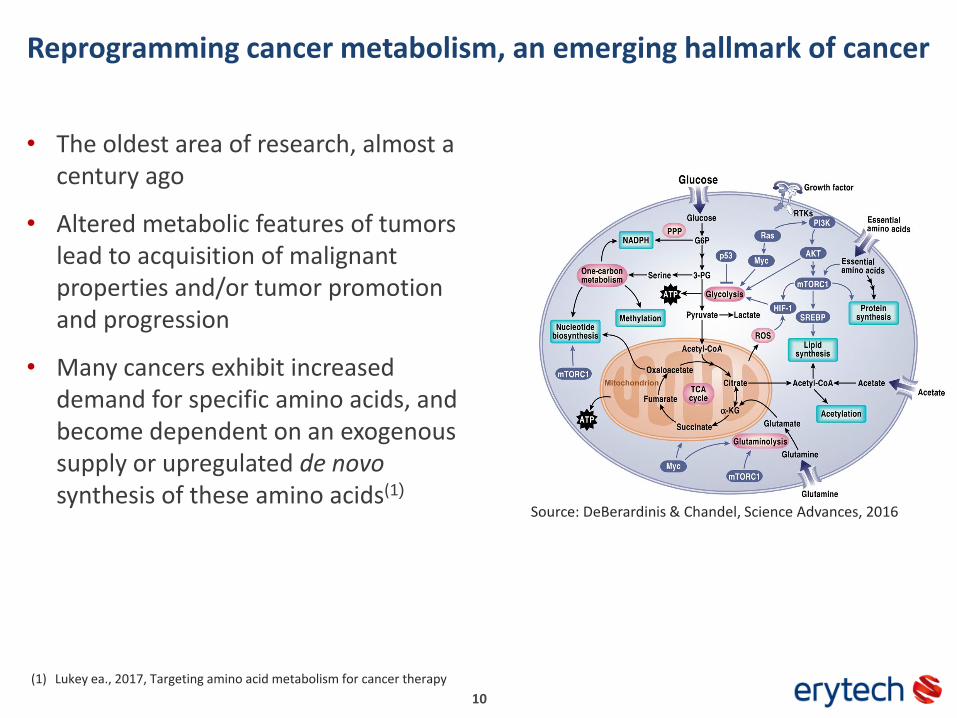
Reprogramming cancer metabolism, an emerging hallmark of cancer
10
• The oldest area of research, almost a century ago
• Altered metabolic features of tumors lead to acquisition of malignant properties and/or tumor promotion and progression
• Many cancers exhibit increased demand for specific amino acids, and become dependent on an exogenous supply or upregulated de novo synthesis of these amino acids(1)
Source: DeBerardinis & Chandel, Science Advances, 2016
(1) Lukey ea., 2017, Targeting amino acid metabolism for cancer therapy
Altered metabolic pathways in PDAC, a role for L-asparaginase?
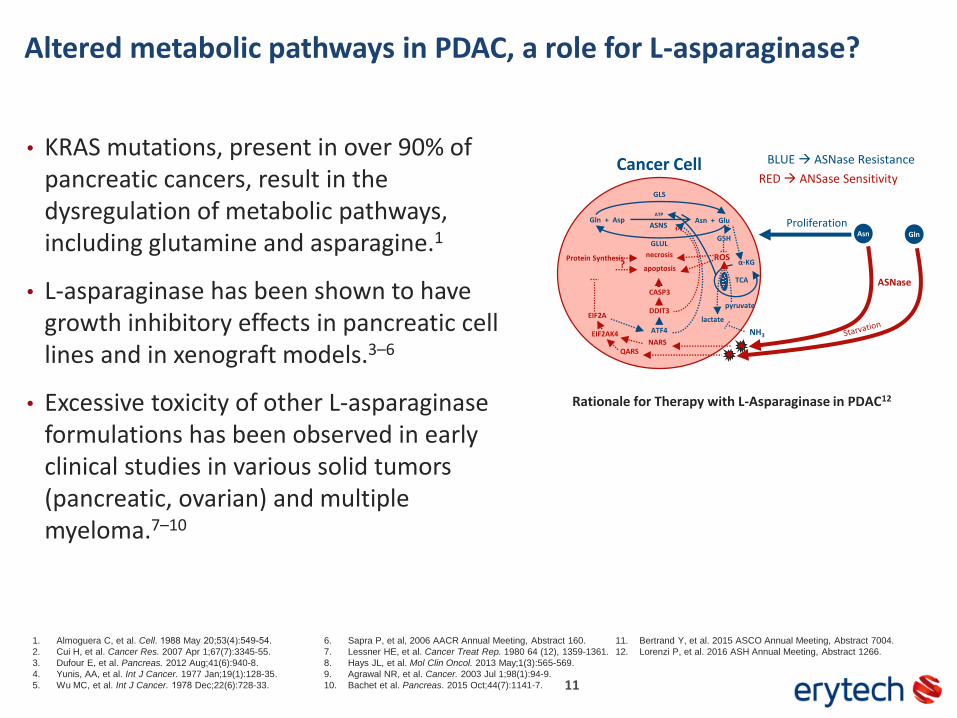
• KRAS mutations, present in over 90% of pancreatic cancers, result in the dysregulation of metabolic pathways, including glutamine and asparagine.1
• L-asparaginase has been shown to have growth inhibitory effects in pancreatic cell lines and in xenograft models.3–6
• Excessive toxicity of other L-asparaginase formulations has been observed in early clinical studies in various solid tumors (pancreatic, ovarian) and multiple myeloma.7–10
11
ASNS
ASNase
AsnProliferationGln + Asp Asn + Glu
Gln
ATP
NH3EIF2AK4
EIF2A
Protein Synthesis
Cancer Cell
ATF4
?necrosis
apoptosis
RED ANSase Sensitivity
BLUE ASNase Resistance
NARSQARS
DDIT3
CASP3
GSH
GLS
GLUL
ROSα-KG
TCA
lactate
pyruvate
Rationale for Therapy with L-Asparaginase in PDAC12
1. Almoguera C, et al. Cell. 1988 May 20;53(4):549-54.
2. Cui H, et al. Cancer Res. 2007 Apr 1;67(7):3345-55.
3. Dufour E, et al. Pancreas. 2012 Aug;41(6):940-8.
4. Yunis, AA, et al. Int J Cancer. 1977 Jan;19(1):128-35.
5. Wu MC, et al. Int J Cancer. 1978 Dec;22(6):728-33.
6. Sapra P, et al, 2006 AACR Annual Meeting, Abstract 160.
7. Lessner HE, et al. Cancer Treat Rep. 1980 64 (12), 1359-1361.
8. Hays JL, et al. Mol Clin Oncol. 2013 May;1(3):565-569.
9. Agrawal NR, et al. Cancer. 2003 Jul 1;98(1):94-9.
10. Bachet et al. Pancreas. 2015 Oct;44(7):1141-7.
11. Bertrand Y, et al. 2015 ASCO Annual Meeting, Abstract 7004.
12. Lorenzi P, et al. 2016 ASH Annual Meeting, Abstract 1266.
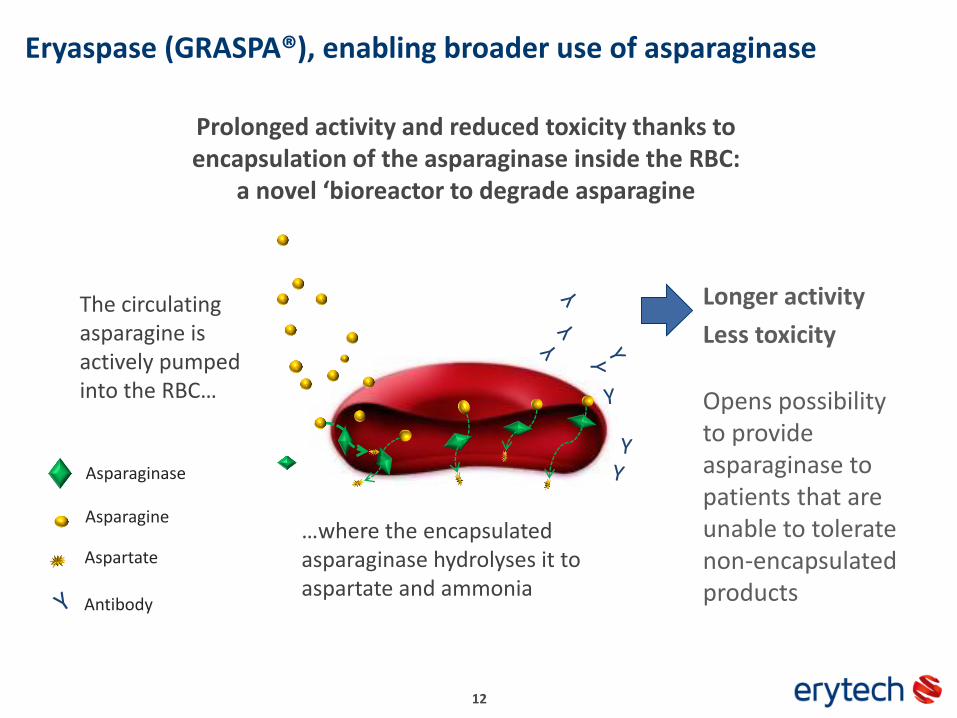
Eryaspase (GRASPA®), enabling broader use of asparaginase
The circulating asparagine is actively pumped into the RBC…
Y
Asparagine
Asparaginase
Antibody
…where the encapsulated asparaginase hydrolyses it to aspartate and ammonia
Prolonged activity and reduced toxicity thanks to encapsulation of the asparaginase inside the RBC:
a novel ‘bioreactor to degrade asparagine
Longer activity
Less toxicity
Opens possibility to provide asparaginase to patients that are unable to tolerate non-encapsulated products
12
Aspartate

Eryaspase, a targeted therapy of metabolic pathways in PDAC
13
• A Phase 1 study with eryaspase demonstrated a favorable safety profile(3)
• The randomized Phase 2b was launched in 2014 as a proof-of-concept study, the first Phase 2 study with an L-asparaginase based product in a solid tumorindication
• Hypothesis: expression of asparagine synthetase (ASNS) is a predictive factor for L-asparaginase sensitivity in PDAC.2
(1) Dufour e.a., 2012(2) Rahib & Smith, 2014`(3) Bachet e.a., 2015

Prof. Pascal Hammel, MD, PhD
• Pr Pascal Hammel is the head of the Digestive Oncology unit at Beaujon hospital (Clichy), Paris VII University, Denis Diderot
• Expert in digestive oncology, especially in the field of pancreatic diseases, particularly pancreatic tumours, preneoplastic lesions and genetic counselling
• Published 300+ articles in digestive oncology
• PI/investigator of several international clinical trials, such as LAP07 (Gemcitabine with or without chemoradiotherapy and with or without erlotinib)
• Active member of several groups (FFCD, GERCOR, PRODIGE, EPC, UEGW) and member of the U.S. Task Force for pancreatic cancer.
14
Full Results of Phase 2b Study of Eryaspase in Second-Line Metastatic Pancreatic Cancer
Prof. Pascal Hammel, MD, PhD
Principal Investigator
15
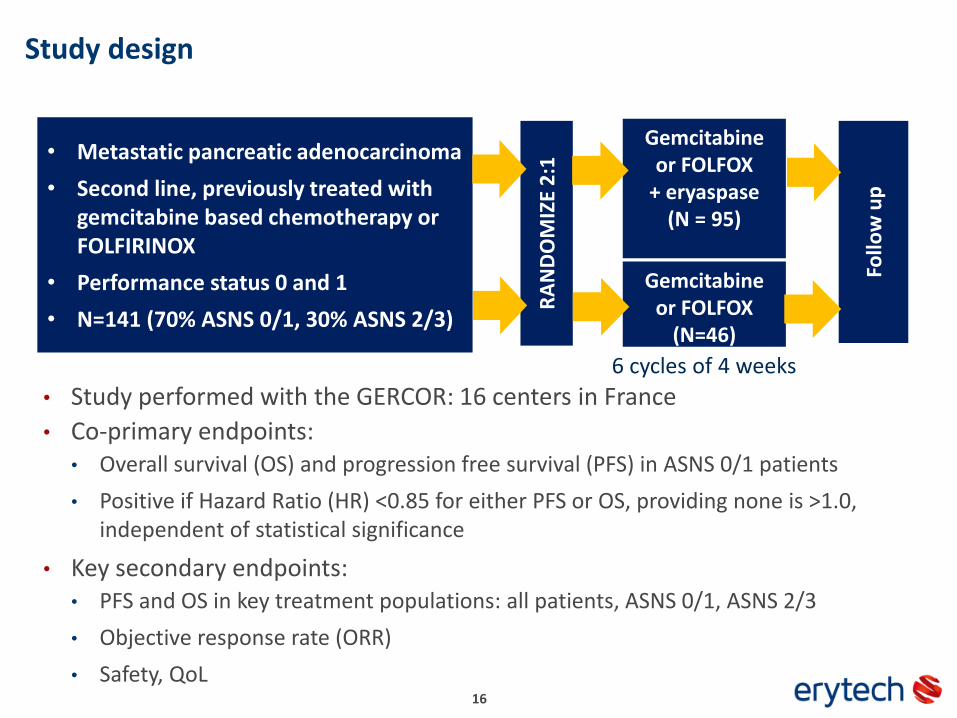
Study design
16
Gemcitabine or FOLFOX
(N=46)
Gemcitabine or FOLFOX
+ eryaspase(N = 95)
• Metastatic pancreatic adenocarcinoma
• Second line, previously treated with gemcitabine based chemotherapy or FOLFIRINOX
• Performance status 0 and 1
• N=141 (70% ASNS 0/1, 30% ASNS 2/3)
RA
ND
OM
IZE
2:1
Follo
w u
p
6 cycles of 4 weeks
• Study performed with the GERCOR: 16 centers in France
• Co-primary endpoints: • Overall survival (OS) and progression free survival (PFS) in ASNS 0/1 patients
• Positive if Hazard Ratio (HR) <0.85 for either PFS or OS, providing none is >1.0, independent of statistical significance
• Key secondary endpoints:• PFS and OS in key treatment populations: all patients, ASNS 0/1, ASNS 2/3
• Objective response rate (ORR)
• Safety, QoL
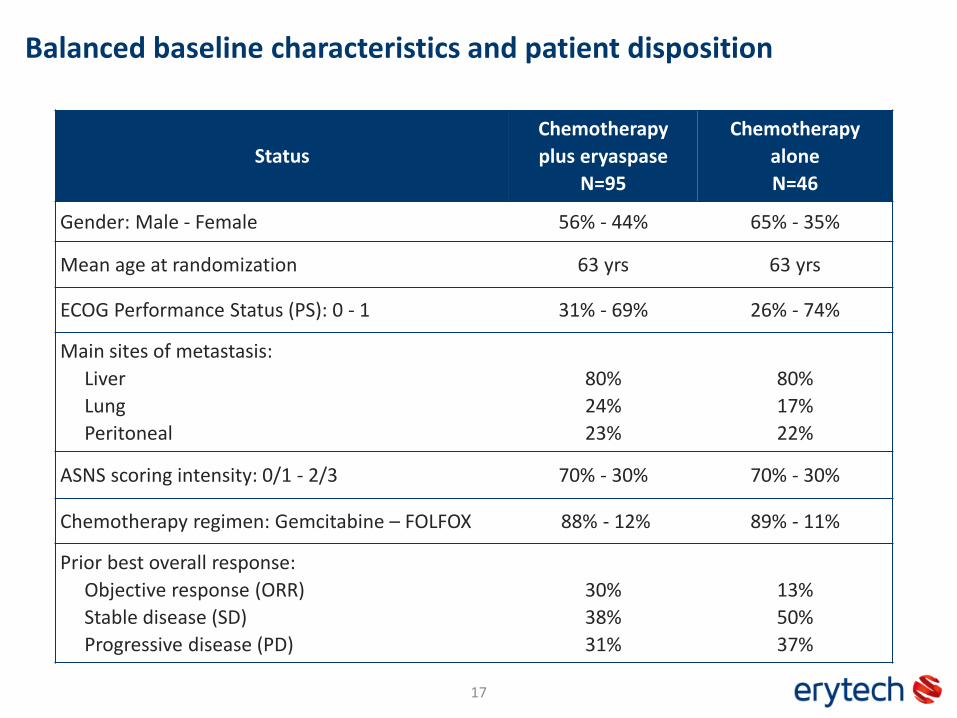
Balanced baseline characteristics and patient disposition
17
Status
Chemotherapy
plus eryaspase
N=95
Chemotherapy
alone
N=46
Gender: Male - Female 56% - 44% 65% - 35%
Mean age at randomization 63 yrs 63 yrs
ECOG Performance Status (PS): 0 - 1 31% - 69% 26% - 74%
Main sites of metastasis:
Liver
Lung
Peritoneal
80%
24%
23%
80%
17%
22%
ASNS scoring intensity: 0/1 - 2/3 70% - 30% 70% - 30%
Chemotherapy regimen: Gemcitabine – FOLFOX 88% - 12% 89% - 11%
Prior best overall response:
Objective response (ORR)
Stable disease (SD)
Progressive disease (PD)
30%
38%
31%
13%
50%
37%
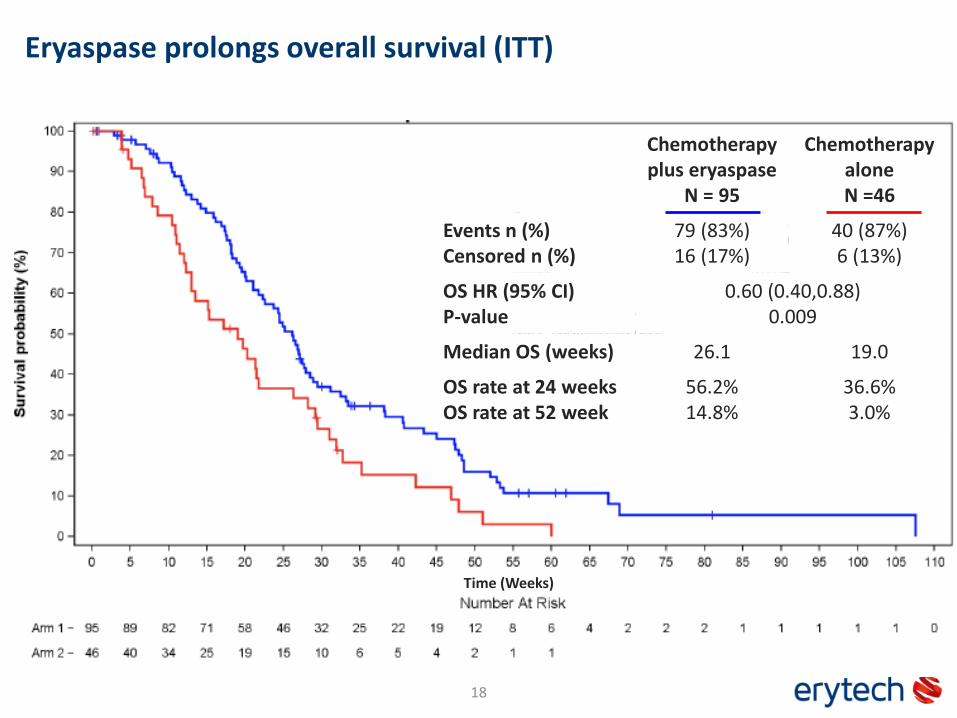
Eryaspase prolongs overall survival (ITT)
18
Time (Weeks)
Chemotherapyplus eryaspase
N = 95
ChemotherapyaloneN =46
Events n (%)Censored n (%)
79 (83%)16 (17%)
40 (87%)6 (13%)
OS HR (95% CI)P-value
0.60 (0.40,0.88)0.009
Median OS (weeks) 26.1 19.0
OS rate at 24 weeksOS rate at 52 week
56.2%14.8%
36.6%3.0%
19E + CT: Eryaspase Arm; CT : Chemotherapy Alone Arm
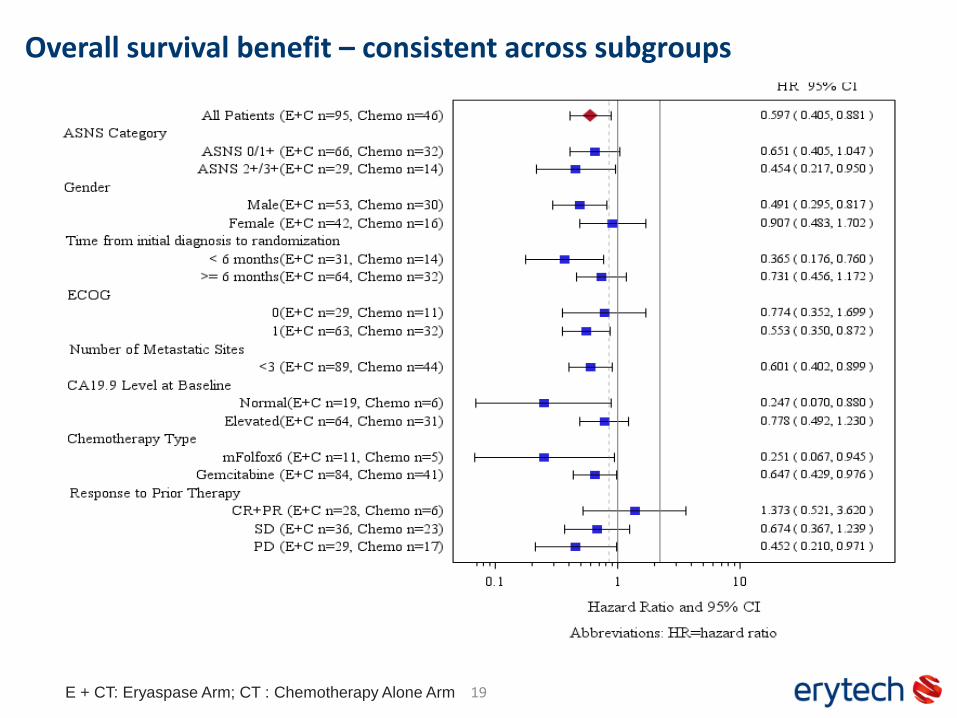
Overall survival benefit – consistent across subgroups

Eryaspase prolonged PFS and improved DCR (ITT)
20
Perc
ent
Change
-100
-80
-60
-40
-20
0
20
40
60
80
100
120
140
160
Patient (Ordered)
0 5 10 15 20 25 30 35 40 45
Figure 14.2.1.1.1.3: Change from Baseline in Sum of Longest Diameter (Independent Radiological Assessment)
Best Response (RECIST 1.1): Tumor % change from Baseline
Treatment = Chemotherapy Alone
() Best response was progressive disease due to new lesions. Percent change from baseline for these subjects was designated as 150%.
Per
cent
Chan
ge
-100
-80
-60
-40
-20
0
20
40
60
80
100
120
140
160
Patient (Ordered)
0 5 10 15 20 25 30 35 40 45 50 55 60 65 70 75 80 85 90
Figure 14.2.1.1.1.3: Change from Baseline in Sum of Longest Diameter (Independent Radiological Assessment)
Best Response (RECIST 1.1): Tumor % change from Baseline
Treatment = Eryaspase + Chemotherapy
() Best response was progressive disease due to new lesions. Percent change from baseline for these subjects was designated as 150%.
eryaspase
plus chemotherapy
chemotherapy
alone alone
* patient with complete remission () new lesions
*
new lesions
new lesions
Chemotherapy
plus eryaspase
N=95
Chemotherapy
alone
N=46
PFS HR (95% CI)
P-value
0.59 (0.40, 0.89)
0.011
Median PFS
(weeks)8.6 7.0
PFS rate at 24 wks 16.9% 5.8%
Response rate
(ORR)11.6% 6.5%
Disease control
rate (ORR+SD)47.4% 23.9%
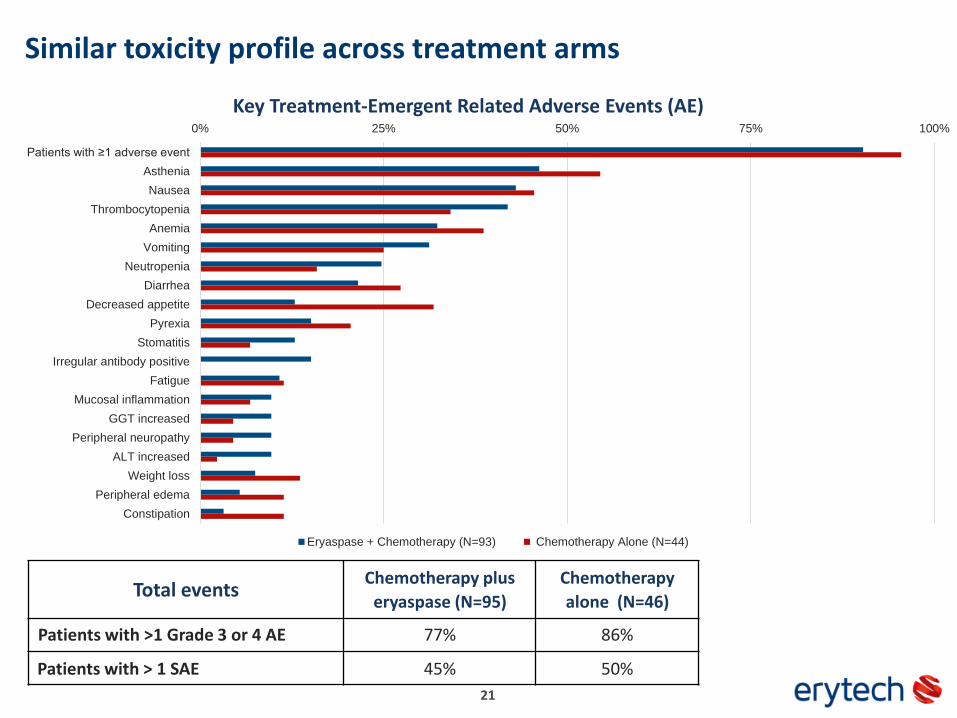
Similar toxicity profile across treatment arms
21
0% 25% 50% 75% 100%
Patients with ≥1 adverse event
Asthenia
Nausea
Thrombocytopenia
Anemia
Vomiting
Neutropenia
Diarrhea
Decreased appetite
Pyrexia
Stomatitis
Irregular antibody positive
Fatigue
Mucosal inflammation
GGT increased
Peripheral neuropathy
ALT increased
Weight loss
Peripheral edema
Constipation
Eryaspase + Chemotherapy (N=93) Chemotherapy Alone (N=44)
Key Treatment-Emergent Related Adverse Events (AE)
Total eventsChemotherapy plus
eryaspase (N=95)
Chemotherapy
alone (N=46)
Patients with >1 Grade 3 or 4 AE 77% 86%
Patients with > 1 SAE 45% 50%
Study conclusions
• Co-primary endpoints met
• Significantly prolonged OS and PFS in the entire population, and improved DCR
• Sensitivity analyses confirmed that results were robust and consistent across subgroups
• Similar safety profile in two treatment arms
• Biomarker work in progress to further decipher the effect of eryaspase, in particular the impact on metabolic pathways
• These data support the sponsor’s proposal to conduct a confirmatory study of eryaspase in pancreatic adenocarcinoma
22
Financial & Operational Update
Eric Soyer, CFO & COO
23

Preparing the company for the next stage
• In April 2017, we successfully completed a private placement resulting in gross proceeds €70.5 million from U.S. and European investors
• The net proceeds of approximately €65.2 million will be utilized to:
• Finance the preparatory steps for the launch of potential Phase 3 studies, notably for the pancreatic cancer indication
• Assess the clinical development opportunities for eryaspase for the treatment of other solid tumor indications, in addition to our ongoing preclinical and clinical programs
• Further strengthen the financial position for our continued development
• Cash balance of €88.5 million at end Q2 2017
• Expanding manufacturing capacity in U.S. and Europe, and strengthening the teams across all functions
24
Next Steps & Key Milestones
Gil Beyen, Chairman & CEO
25
Key milestones
Reporting of full Phase 2b pancreatic cancer data
Meeting with US and EU agencies on pancreatic cancer development plan
Resubmission of EU marketing authorization application in R/R ALL
Meeting with FDA on ALL further development plan
Results from EU Phase 2b AML study
Launch of potential Phase 3 study in pancreatic cancer
Launch of potential Phase 3 study in 1st line adult ALL
Launch of potential erymethionase Phase 1 study
26
✔

Q&A
27

www.erytech.com
ERYTECH Pharma SA60 Avenue Rockefeller
69008 LyonFrance
ERYTECH Pharma Inc1 Main Street
Cambridge, MA 01242USA





























