Embed Size (px)
Citation preview
Irregular Pacemaker Tachycardia ina Patient with WPW Syndrome andan A-V Universal Pacemaker
MICHAEL WEHR, CLAUS-G. SCHMITT,* and J. HERMANN PETERFrom the Department of Cardiology, Center for Internal Medicine, and Center for OperativeMedicine I,* Philipps University. Marburg. Federal Republic of Germany
WEHR, M., SCHMITT, C.-G., AND PETER, J.H.: Irregular pacemaker tachycardia in a patient with WPWsyndrome and an A-V universal pacemaker. We describe a case of an irreguJar pacemaker circus move-ment tachycardia in a patient with the Woi/f-Parkinson-White syndrome and a normalJy functioning A-V universal [DDD] pacemaker (Cordis Sequicor 233 D). The mechanism of the artificial circus movementtachycardia, which uses the pacemaker as the anterograde Jimb and a septalJy iocaled accessory atrio-ventricuJar pathway as the retrograde limb, is discussed. [PACE, Vol. 7, May-/une, 1984]
A-V universai pacing, pacemaker tachycardia. WPW syndrome, Cordis Sequicor 233 D pacemaker
Introduction
Several A-V universal (DDD) pulse generatorsare now available which sense and pace in bothatrium and ventricle and which can synchronizeatrial and ventricular events. These sophisticateddevices can maintain A-V synchrony and thus pre-serve atrial kick in patients with ventricular dys-function. Ventricular pacing rate can respondphysiologically in the presence of normal sinusnode function. In addition, symptomatic brady-cardia and drug-resistant tachycardias may be pre-vented. In the presence of ventriculo-atrial con-duction via the A-V node or an accessory A-Vpathway, a pacemaker circus movement tachy-cardia is made possible using the pacemaker asthe anterograde limb.^ - In this report we describean unusual irregular pacemaker tachycardia.
Dr. Wehr was recipient of a grant of the Deutsche Forschungs-gemeinschaft at St. Annadal Hospital, Department of Cardiol-ogy. Maastricht. The Netherlands.
Address for reprints: Dr. Michael Wehr. Dept. of Cardiology,Center for Internal Medicine. Mannkopffstrasse 1, D-3550 Mar-burg, Germany (KRG)-
Received November 15. 1982; revision received June 16,1983;accepted August 14. 1983.
Case Report
An A-V universal pulse generator (Cordis** Se-quicor 233 D] was implanted in a 58-year-old manto prevent recurrent syncope caused by a hyper-sensitive carotid sinus. He also had episodes ofshort-lasting paroxysmal supraventricular tachy-cardia due to WPW syndrome, Type B. The fol-lowing was found at electrophysiological studyprior to pacemaker implantation: (1) Massage ofthe right carotid sinus in the basal state resultedin a symptomatic sinus node arrest of 5 s. (2) Whenusing right atrial premature stimulation at a basicpacing cycle length of 600 ms the anterograde re-fractory period of the septal accessory pathwaywas 280 ms. (3) During atrial fibrillation, whichwas initiated by incremental atrial pacing, theshortest coupling of two consecutively preexcitedbeats was 260 ms. (4) One-to-one ventriculo-atrialconduction over the accessory pathway was notedup to a paced ventricular rate of 220 bpm. (5) Acircus movement tachycardia at 135-180 bpm, us-ing the normal A-V conduction system in antero-grade and the accessory pathway in retrogradedirection, could be initiated by programmed atrialstimulation, using single atrial premature stimuli.The ventriculo-atrial conduction time during cir-
'*Cordis Corp., Miami, Florida, U.S.A.
320 May-June 1984, Part I PACE, Vol. 7

IRREGULAR PACEMAKER TACHYCARDIA
cus movement tachycardia was not measured. Thetachycardia terminated after intravenous injectionof 50 mg amiodarone: subsequently, symptomaticsinus bradycardia at a rate of 40 bpm occurred butcould be reversed by 1 mg of IV atropine. (6) Afteramiodarone the anterograde refractory period ofthe accessory pathway was 340 ms, and the short-est coupling of two consecutively preexcited beatsduring atrial fibrillation was 320 ms. Circus move-ment tachycardia could no longer be initiated.
Because of the risk of pacemaker circus move-ment tachycardia due to the excellent retrogradeconduction over the accessory pathway, the elec-trophysiologist suggested implantation of a VVIpacemaker to prevent syncope while continuingoral treatment with amiodarone. However, anA-V universal pacemaker [Cordis Sequicor 233 D]had been mistakenly implanted in another hos-pital. The pulse generator was programmed in theDDD mode in order to preserve atrial kick. The
lower pacing rate was set at 60 bpm, the upperpacing rate was set at 130 bpm, and the fall-backrate was set at 65 bpm. The atrial refractory periodduring the fall-back mode was 305 ms and theA-V delay was programmed to 120 ms.
Five months later the patient was admitted be-cause of incessant tachycardia. The admissionelectrocardiogram (Fig. 1) showed an irregularpacemaker tachycardia with cycle lengths be-tween 680 and 340 ms. There were regular pausesof 680 ms duration after every 11 stimulated ven-tricular complexes. The P-wave morphology whichwas positive in the precordial leads (Figs. 1, 2]was compatible with retrograde activation of theatria via a septally located accessory pathway, viathe A-V node or by fusion of the two routes. Thispattern (atrial activation via V-A conduction fromthe ventricular paced beat and ventricular acti-vation via the right ventricular pacing lead syn-chronized to sensed atrial depolarization) was
\\V
I 1s I
Figure 1. Electro cardiogram on admission showing the /all-back mode behavior of \he CordisSequicor pacemaker during pacemaker circus movement tachycardia. There are regular episodesof 11 /oJiowing beats with dij^erent cycle lengths which are interrupted by regular pauses. Thepacing modes of Ihe pacemaker are marked, The arrows point lo the retrograde P-waves. Seetext for further discussion.
PACE, Vol. 7 May-June 1984. Part I 321
WEHR. SCHMITT. AND PETER
^—r
440 440 440 440 510 440 340 340340340 680
t VVI If DDD
atrialrate
max.
1*
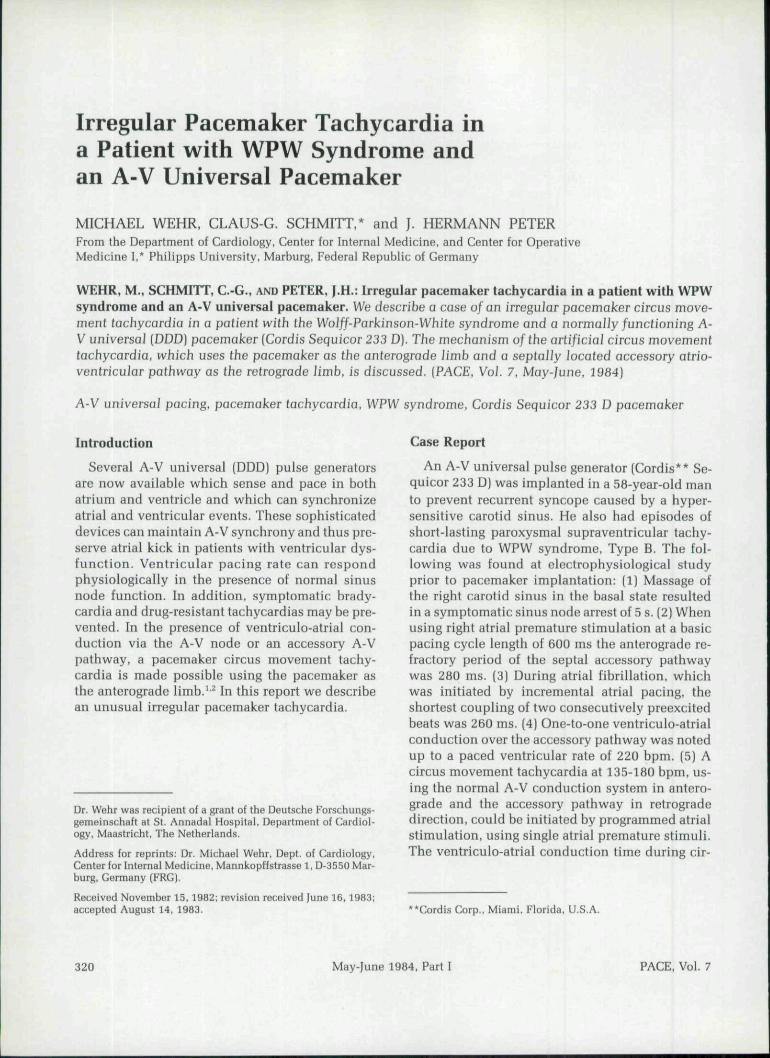
Figure 2. Ltud V, during un ll-beul epiaodt^. Thv luder diagram [AVN: A-V node; V: venlriclo]demonstraUts that this tacbycardio is consistent witb a pacemaker circus movement tacbycardiawhich use.s fhe pacemaker ivith a programmed A-V delay a.s theonlerogradt! fimb [dashed i/nes),and fhe accessory pafhivay, fhe A-V node or both os relrograde limb (solid lines). 7'he arrowspoint io tbe P-ivav'e.s H'hich are fhe results of retrograde aclivalion af tbe atria. Tbt; retrogradeconduction time.s remain consfant and the irregu/ar ventricular rate (the changing cycle Jengthsare indicated be(oiv) is caused by (he fall-back mode of fhe pacemaker.
consistent with artificial circus movement tachy-cardia.' ^
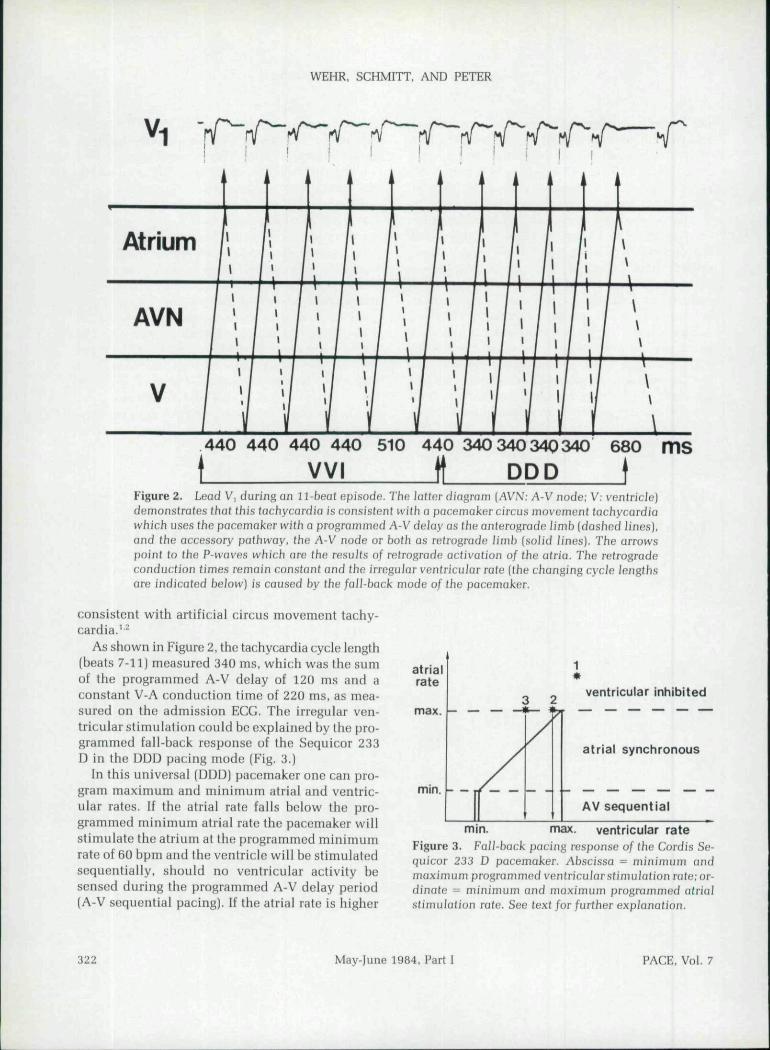
As shown in Figure 2, the tachycardia cycle length(beats 7-11) measured 340 ms, which was the sumof the programmed A-V delay of 120 ms and aconstant V-A conduction time of 220 ms. as mea-sured on the admission ECG. The irregular ven-tricular stimulation could be explained by the pro-grammed fall-back response of the Sequicor 233D in the DDD pacing mode [Fig, 3.)
In this universal (DDD] pacemaker one can pro-gram maximum and minimum atrial and ventric-ular rates. If the atrial rate tails below the pro-grammed minimum atrial rate the pacemaker willstimulate the atrium at the programmed minimumrate ot 60 bpm and the ventricle will be stimulatedsequentially, should no ventricular activity besensed during the programmed A-V delay period(A-V sequential pacing]. If the atrial rate is higher
mm.
ventricular inhibited
atrial synchronous
AV sequential
mm. max. ventricular rateFigure 3. FaU-back pacing response of tbe Cordis Se-quicor 233 D pacemaker. Abscissa = minimum andmaximum programmed ventricular.stimufcifion rafe;or-dinate = minimum and maximum programmed atria]stimaJafion rate. See fext for further explanation.
322 May-June 1984. Part I PACE, Vol, 7

IRREGULAR PACEMAKER TACHYCARDIA
than the minimum but below the maximum atrialrate the pacemaker will sense the atrial activityand pace the ventricle accordingly, up to the max-imum ventricular rate of 130 bpm (atrial synchro-nous pacing), if there is no sensed QRS-complexbefore the end of the programmed A-V delay. Whenthe conducted rhythm exceeds the maximum atrialrate (130 bpm) for 5 beats, the Sequicor pacemakerautomatically switches over to VVI pacing mode(ventricular inhibited pacing) after a programmedpause of 680 ms. The ventricle is then stimulatedwith the so-called initial tachycardia rate whichis just below the maximum ventricular rate; in ourpatient It was programmed to a cycle length of 440ms {130 bpm) (Figs. 2, 3),
Then the ventricular rate is slowly reduced (fall-back mode) to the so-called tachycardia rate of 65bpm (Figs. 2, 3) or until the sensed atrial rate islower than the maximum atrial rate which reini-tiates the DDD pacing mode again. During the VVIpacing mode the Sequicor provides a prolongationof one stimulation interval by 71 ms —up to 510ms—in order to allow a better check of atrial ac-tivity in this longer period and to start DDD pacingmode again if atrial activity is absent, However,in our case, because of continuous retrograde con-duction from the paced ventricular beats, this pro-longation of pacing interval led to a fall in thefollowing sensed atrial rate below the programmedmaximum atrial rate and the DDD pacing modeagain reinitiated the sequence. This mechanismwas responsible for the incessant nature of thetachycardia.
Discussion
In the presence of ventriculo-atrial conductionvia the A-V node or an accessory pathway, a DDDpacemaker may cause a pacemaker circus move-ment tachycardia due to an artificial reentrant cir-cuit thus created.^'^ The retrograde arm of tbis ar-tificial circuit may be provided either by the normalA-V conduction system or by an accessory A-Vpathway, while the anterograde limb is by way ofA-V synchronization using the pacemaker. Theinitiation of the tachycardia with the Sequicor sys-tem is caused by a ventricular premature beat orby synchronization of a ventricular paced event toelectrical artifacts (pectoral muscle artifacts). Theseevents must fall outside of the programmed atrial
refractory period in order to he recognized and toenable the pacemaker to synchronize the atrialevents.
The hypothetic possibility of reentry (also calledendless-loop, because of its incessant character)tachycardia was first postulated by Castellanos andLemberg in 1973.' Since then, several reports oftachyarrhythmias associated with normally func-tioning atrioventricular universal demand pace-makers have been described.''^ Furman and Fisher^reported an endless-loop tachycardia in a pa-tient who had received a multiprogrammabte uni-polar A-V universal DDD pulse generator (Med-tronic* 7000) for cardiomyopathy with intermittentA-V block and sinus bradycardia. The tachycardiawas initiated by single ventricular premature beatsconducted retrogradely to the atria via the A-Vnode. The authors pointed out the importance ofthe pacemaker's atrial refractory period which madethe mediation of an endless-loop tachycardia pos-sible.
When physiologic pacing is indicated in a pa-tient with good retrograde conduction, severalelectrophysiologic parameters should carefully beconsidered before DDD pacemaker implantation.The refractory period of the V-A pathway, the con-duction time of an impulse from the site of stim-ulation in the right ventricular apex to the highright atrial electrode (not determined in our case)and the programmable properties of the pacingsystem (upper atrial rate, atrial refractory period,A-V delay, and programmed response to atrialtachycardia) determine if a pacemaker circusmovement tachycardia is possible. In the presenceof a normally conducting V-A pathway with a shortrefractory period, all ventricular events will beconducted back to the atrium and atrial triggeredventricular pacing will occur as long as the atrialdepolarization does not fall into the refractory pe-riod of the pacemaker. The programmed upper atrialrate will then determine the possible rate of thetachycardia thus created. If the tachycardia rateexceeds the upper atrial rate with the Cordis Se-quicor pacemaker system implanted in our pa-tient, two types of responses to atrial tachycardiacan be programmed: (1) In the fall-back mode, asshown in this case, a slow reduction of tachycardia
'Medtronic, Inc., Minneapolis. Minn,. U.S,A,
PACE, Vol, 7 May-June 1984, Part I 323

WEHR, SCHMITT, AND PETER
rate will occur. (2) In the 2:1 A-V block mode,sensed atrial rates faster than the programmed up-per atrial rate in the absence of A-V conductionwill lead to ventricular pacing at a rate which isat most half of the upper atrial rate. In this modethe duration of the atrial refractory period is equalto the cycle length of the programmed upper atrialrate. In our case an upper atrial rate of 130 ms (460ms) would have resulted in an atrial refractoryperiod of 460 ms, which would have resulted ina maximum ventricular rate of 130 hpm.
Perhaps the reason that it took so long to developthe tachycardia in this patient was due to an ab-sence of initiating factors such as spontaneousventricular premature beats.
Our observation shows the importance of athorough understanding of the new sophisticatedpacemaker, especially in the presence of goodretrograde conduction, and stresses the need forspecially trained physicians who may prevent andcorrect pacemaker-related tachyarrhythmias byappropriate programming measures.
References
1. den Dulk, K., Lindemans, F.W., Bar, F.W.H.M.. et al.:Pacemaker-related tachycardias. PACE. 5:476,1982.
2. Furman, S.. Fisher, ].D.: Endless-loop tachycardiain an AV universal (DDD) pacemaker. PACE, 5:486,1982.
3. Castellanos, A., and Lemberg. L.: Pacemaker ar-rhythmias and electrocardiographic recognition ofpacemakers. CircuJation, 42:1382, 1973.
324 May-June 1984, Part I PACE, Vol. 7






























