-
Update on Irritable Bowel Syndrome
Anthony Lembo, M.D. Beth Israel Deaconess Medical Center
Harvard Medical School Boston, MA
-
Highlights
• FDA approval for 2 new IBS-D treatments – Rifaximin and
eluxadoline
• Diagnostic test for IBS (IBSchek) • Controlled trials with the
FODMAP diet • Delayed release peppermint oil
-
Early description of symptoms defining IBS
• 1849 – W Cumming
“The bowels are at one time constipated, at another lax, in the
same person. How the disease has two such different symptoms I do
not profess to explain. . . .”
•Historical terms – mucous colitis – colonic spasm – neurogenic
mucous colitis – irritable colon
W. Cumming, London Medical Gazette, 1849;NS9;969-973.
– unstable colon – nervous colon – spastic colon – nervous
colitis – spastic colitis
-
Longstreth GF et al. Gastroenterology. 2006;130(5):1480-1491.
Rome Organization. Rome III Disorders and Criteria. Available at:
http://www.romecriteria.org/criteria/. Accessed February 29,
2013.
Rome III Criteria for IBS
*Criteria fulfilled for the last 3 months with symptom onset at
least 6 months prior to diagnosis
Onset associated with a change
in frequency of stool
Onset associated with a change
in form of stool
Recurrent abdominal pain or discomfort at least 3 days / month
in the last 3 months associated with 2 or more of the
following:
Improvement with
defecation
Additional IBS “testing,” including routine laboratory tests and
colonoscopy, unnecessary unless alarm features present
7
http://www.romecriteria.org/criteria/
-
Epidemiology • IBS is the most commonly diagnosed
gastrointestinal disorder1
1. Chey WD, et al. JAMA. 2015;313:949-958. 2. Lovell RM, et al.
Clin Gastroenterol Hepatol. 2012;10:712-721.
Prevalence of IBS in various countries2
5
-
Natural History of IBS • Chronic, relapsing disease1 • Data from
a systematic review of patients in long-term
follow-up1 – 2%-18% worsened – 30%-50% remained unchanged –
12%-38% improved
• Patients migrate between classifications – The majority of
patients change
subtypes over time2 – Most common migrations are
to and from IBS-M3 • Patients seldom migrate directly
between IBS-C and IBS-D
1. El-Serag HB, et al. Aliment Pharmacol Ther. 2004;19:861-870.
2. Engsboro AL, et al. Aliment Pharmacol Ther. 2012;35:350-359. 3.
Garrigues V, et al. Aliment Pharmacol Ther. 2007;25:323-332.
IBS-C
IBS-D IBS-M
6
-
Impact of IBS on quality of life compared with other medical
conditions
30
40
50
60
70
80
90
Mea
n SF
-36
scor
e
National norm
Diabetes type II
IBS
Clinical depression
Adapted from Wells et al., Alimentary Pharmacology Therapies,
1997; 11: 1019-1030.
-
IBS Pyramid Specialists
Primary care ~25% Consulters
~75% Nonconsulters
~70% Female
~30% Male
Pain
Psychological disturbance
Adapted from Drossman and Thompson, Ann Intern Med 1992; 116(pt
1): 1009 Sandler, Gastroenterology 1990; 99: 409
-
Economic burden of IBS
Healthcare costs Productivity costs
Billions of dollars 0 20 40 60 80 100 120
Arthritis
Hypertensive disease IBS
Stroke
Diabetes
Asthma
Migraine
-
Disordered CNS-ENS interactions in IBS
Psychological/ cognitive
Gut luminal/ mucosal
IBS Symptoms Heightened
Sensorimotor Activity
Adapted from Clouse RE. J Funct Syndrome 2001; 1:61-68
Brain-Gut Axis
-
Pathophysiology of IBS Environmental Contributors
to IBS Symptoms
• Early life stressors (abuse, psychosocial stressors)1,2
• Food intolerance2 • Antibiotics2 • Enteric infection2
Host Factors as Contributors to IBS Symptoms
• Enhanced stress response1 • Altered pain perception1,2 •
Altered brain-gut interaction2 • Dysbiosis2 • Increased
intestinal
permeability1,2 • Increased gut mucosal
immune activation2 • Visceral hypersensitivity2
1. Chang L. Gastroenterology. 2011;140:761-765. 2. Chey WD, et
al. JAMA. 2015;313:949-958.
11
-
Role of Immune Activation in Post-Infectious IBS
0
50
100
150
200
Discomf Inflamm Psych
IBS + IBS - Control
*
* *
Gwee, Gut, 1999;44:400.
Control
3 wks post infectious
Spiller, Gut, 2000; 47(6): 807.
Increased Enterochromaffin Cells
Visceral Hypersensitivity chronic lymphocytes at f/u
psychological disturbance at baseline
http://gut.bmjjournals.com/cgi/content/full/47/6/804/F1
-
Key Organic Diseases in Differential Diagnosis of IBS
ACG Task Force on IBS. Am J Gastroenterol. 2009;104(suppl
1):S1-S35.
Organic disease in the absence of alarm features is uncommon
Lactose intolerance
Colorectal carcinoma
Celiac disease
Enteric infection
Inflammatory bowel disease
Thyroid dysfunction
13
-
Positive Diagnostic Strategy Was Non-inferior to Strategy of
Exclusion
• 302 primary care patients (18-50 years of age) who fulfilled
ROME III criteria for IBS with no alarm features
• A positive diagnostic strategy was non-inferior to using a
strategy of exclusion with regard to HRQoL and was associated with
lower direct costs
*Full blood count, C-reactive protein, plasma-calcium,
-bilirubin, -ALT, -alkaline phosphatase, -albumin, serum-TSH,
serum-tissue transglutaminase, lactase gene test.
†Full blood count, C-reactive protein.
Strategy of Exclusion Positive Strategy
Blood analysis Stool samples for parasite Sigmoidoscopy with
biopsies
Begtrup LM, et al. Clin Gastroenterol Hepatol.
2013;11:956-962.
* †
ALT=alanine aminotransferase; HRQoL=health-related quality of
life; TSH=thyroid-stimulating hormone.
-
American College of Gastroenterology Recommendations for
Diagnostic Testing in IBS Test Recommendation Complete blood
count Serum chemistries Thyroid function studies Stool for ova and
parasites Abdominal imaging
Not recommended in patients with typical IBS symptoms and no
alarm features
Serologic screening for celiac sprue
Pursue in IBS-D and IBS-M
Lactose breath testing Consider if symptoms persist after
dietary modification
Breath testing for SIBO Insufficient data to recommend Routine
colonoscopy Not recommended in patients
-
Alarm Features for Organic Disorders
• Symptom onset after age 50 years • Blood in stools • Nocturnal
symptoms • Anemia • Weight loss (unintentional) • Change in
symptoms • Family history of organic gastrointestinal disease
Patients with alarm features
should undergo further investigation
ACG Task force on IBS. Am J Gastroenterol. 2009;104(suppl
1):S1-S35. 16
-
T17
0
10
20
30
40
50
60
0 2 4 6 8 10 12 14 16
Week
% with relief
*P
-
Treatments for IBS
-
Diets in IBS • Pros:
– Non-pharmacological therapy – Symptom relief, at least short
term
• Cons: – No standard diet – Difficult and expensive to follow –
Nutrition consult often necessary – Long term impact on health is
unclear – Difficult to control for placebo effect in a dietary
trial
Barrett, JS. Nutr Clin Pract 2013, 28:300 Gibson, PR &SJ
Shepherd J Gastroenterol Hepatol 2010; 25(2):2
-
Dietary and Lifestyle Considerations
• Only a few well-controlled RCTs of elimination diets in IBS
have been conducted1
• Up to ⅔ of IBS patients associate symptom onset or worsening
with eating a meal2,3
• Maintaining a brief diary of dietary intake and symptoms may
help determine if a correlation exists between food and IBS
symptoms2 – Fatty/greasy food – Poorly absorbed carbohydrates –
Gas-producing foods – Soluble fiber
• One small study demonstrated improved IBS symptoms with
physical activity4
1. Moayyedi P, et al. Clin Transl Gastroenterol. 2015;6:e107. 2.
Somers SC, Lembo A. Gastroenterol Clin North Am. 2003;32:507-529.
3. ACG Task Force on IBS. Am J Gastroenterol. 2009;104(suppl
1):S1-S35. 4. Johannesson E, et al. Am J Gastroenterol.
2011;106:915-922.
FODMAPs=fermentable oligosaccharides, disaccharides,
monosaccharides, and polyols; RCT=randomized, controlled trial.
20
-
The FODMAP Diet Eliminate foods containing FODMAPs1-3
Excess Fructose Lactose Fructans Galactans Polyols
fruit apple, mango, pear, cherries, watermelon sweeteners sugar,
high-fructose corn syrup other honey, asparagus
milk milk from cows, goats, or sheep; custard, ice cream, yogurt
cheeses soft unripened cheeses (eg, cottage cheese, ricotta)
vegetables onion, leek, garlic, shallots, artichokes, asparagus,
peas, beetroot, chicory cereals wheat, barley, rye
legumes baked beans, chickpeas, kidney beans, lentils
fruit apple, pear, apricot, cherries, peaches, nectarines,
plums, watermelon vegetables cauliflower, mushrooms sweeteners
sorbitol, mannitol, xylitol, chewing gum
1. Shepherd SJ, et al. Am J Gastroenterol. 2013;108:707-717. 2.
Shepherd SJ, Gibson PR. J Am Diet Assoc. 2006;106:1631-1639. 3.
Barrett JS, Gibson PR. Ther Adv Gastroenterol. 2012;5:261-268.
21
-
-7 0 7 14 21 -7 0 7 14 21
Low-FODMAP vs Typical Australian Diet
Halmos EP, et al. Gastroenterology. 2014;146:67-75.
Mean overall GI symptoms improved with low-FODMAP diet in IBS
patients (≤0.5 g of FODMAPs per meal)
VAS
(0-1
00 m
m)
IBS Healthy Controls
Day Day
Baseline Typical Australian diet Low-FODMAP diet
60
40
20
60
40
20
P
-
Both Low-FODMAP and Traditional IBS Diets Reduced IBS Symptom
Severity
Böhn L, et al. Gastroenterology. 2015. doi:
10.1053/j.gastro.2015.07.054.
P=.002 Low FODMAPs
P
-
Psychological Therapy for IBS
Ford AC, et al. Am J Gastroenterol. 2014 Sep;109:1350-1365.
Therapy Trials N RR
(95% CI) NNT
(95% CI) Cognitive behavioral therapy (CBT) 9 610 0.60
(0.44-0.83) 3 (2-6)
Relaxation training or therapy 6 255 0.77 (0.57-1.04) –
Hypnotherapy 5 278 0.74 (0.63-0.87) 4 (3-8)
Multi-component psychological therapy 5 335 0.72 (0.62-0.83) 4
(3-7)
Self-administered, minimal-contact CBT 3 144 0.53 (0.17-1.66)
–
CBT via Internet 2 140 0.75 (0.48-1.17) –
Dynamic psychotherapy 2 273 0.60 (0.39-0.93) 3.5 (2-25)
Stress management 2 98 0.63 (0.19-2.08) –
Multi-component therapy via telephone 1 126 0.78 (0.64-0.93)
–
Mindfulness meditation training 1 75 0.57 (0.32-1.01) –
Total 36 2334 0.68 (0.61-0.76)
CI=confidence interval; NNT=number needed to treat; RR=risk
ratio; – = not provided.
24
-
Similar & significant differences for: Abdominal pain,
bloating, tiredness & satisfaction with stool consistency
Gluten Free Diet for Functional Disorders?
-
Bloating/ distension
Abdominal pain/
discomfort
Altered bowel function
Bloating • Probiotics • Antibiotics
Diarrhea • Loperamide • Probiotics • Rifaximin • Eluxadoline
1. Brandt LJ et al, for the ACG Task Force on IBS. Am J
Gastroenterol. 2009;104(Suppl 1):S1-S35. 2. Chey WS, et al. Gut and
Liver. 2011;253-266.
Abdominal pain/discomfort • Antispasmodics • Antidepressants •
Linaclotide
Constipation • Ispaghula/psyllium • Lubiprostone • Linaclotide •
Osmotic laxatives • Tegaserod
Pharmacologic Treatments for IBS
50
-
Probiotics
• Associated with benefits in global IBS, abdominal pain,
bloating, and flatulence scores
• NNT of 7 (95 % CI 4 – 12.5) – Subanalysis showed only
combination probiotics,
Lactobacillus plantarum DSM 9843 and E. coli DSM17252, to be
effective
• Probiotics improve global symptoms, bloating, and flatulence.
Recommendations regarding individual species, preparations, or
strains cannot be made
Ford AC, et al. Am J Gastroenterol. 2014;109:1547-1561. 27
-
Efficacy of Psyllium in IBS
• Bulking agents can exacerbate bloating, flatulence, abdominal
distention, and abdominal discomfort.2,3 Dose should be titrated
gradually2
1. Bijkerk CJ, et al. BMJ. 2009:339:B3154-B3160. 2. ACG Task
Force on IBS. Am J Gastroenterol. 2009;104(suppl 1):S1-S35. 3.
Eswaran S, et al. Am J Gastroenterol. 2013;108:718-727.
*P
-
Polyethylene Glycol (PEG) for IBS-C
Chapman RW, et al. Am J Gastroenterol.
2013;108(9):1508-1515.
Spontaneous Complete Bowel Movements
(SCBMs) Abdominal
Discomfort/Pain
*P
-
Antidepressants • Effective at reducing IBS symptoms and
abdominal pain1
• Adverse effect profiles may guide use in IBS subtypes2 – TCAs
may cause constipation and may
therefore not be well suited for patients with IBS-C
– SSRIs may cause diarrhea and are therefore not well suited for
patients with IBS-D
1. Ford AC, et al. Am J Gastroenterol. 2014;1350-1365. 2. Chey
WD, et al. JAMA. 2015;313:949-958.
RR=relative risk; SSRI=selective serotonin-reuptake inhibitor;
TCA=tricyclic antidepressant.
Patients Reporting Unimproved IBS
Symptoms1
0%
10%
20%
30%
40%
50%
60%
70%
Placebo Antidepressants R
espo
nden
ts (%
)
RR = 0.67 (95% CI=0.58-0.77)
NNT = 4
30
-
Antidepressants – Tips for improving Effectiveness
• Inform patients of expected AE (e.g. sedation, agitation,
anticholinergic)
• Start low (10-25 mg/d) and advance slowly, especially in the
elderly and those with somatization disorder
• Try to reach a daily dose of 50 mg • Switch to an alternative
TCA or SSRI if intolerance
or SE occur • Use adverse-effect profiles to help select
agents
Clouse, Gastroenterology, 1999
-
Osmotic Laxative Polyethylene glycol (PEG) Improves Bowel
Function But Not Pain in IBS-C
Chapman et al. Am J Gastroenterol 2013; 108:1508–1515
-
T33
Cl- Cl-
Na+
K+ K+
K+ 2Cl
Tight junction
H2O Na+
H2O Na
+
Ion Transport
Na+
CFTR channel Enterocytes Cl C2 channel
T168
Increasing Fluid in the GI Tract via Chloride Channels
-
Lubiprostone
• Activates luminal Cl-C2 channels (and possibly CFTR)
• 2 12-wk Phase III Trials • Overall responder =
monthly responder ≥2-3 mths
• Monthly responder = at least moderate relief 2-4 wk or
significant relief >2-4 wk
• FDA approved 8 ug BID in women with IBS-C
Drossman DA et al. Aliment Pharmacol Ther. 2009;29:329-341.
P = .001
Com
bine
d
Ove
rall
Resp
onde
rs, %
Chart1
Lubiprostone 8 µg BID n=780
Placebon=387
Column1
17.9
10.1
Sheet1
Column1
Lubiprostone 8 µg BID n=78017.9
Placebon=38710.1
To resize chart data range, drag lower right corner of
range.
-
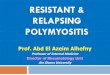
Linaclotide
13.9%
≥30% abdominal pain reduction + increase ≥1 CSBM from baseline;
in the same week for 50% of weeks (i.e, 6 out of 12 weeks)
% F
DA
Res
pond
ers
33.7%*
Placebo N=403
Lin 290 µg N=401
FDA Responder
CSBM +1 Responder
Abdominal Pain
Responder
Chey WD et al. AJG 2013.
FDA Approved dose 290 ug QD for IBS-C Adult men and women
Chart1
APC+1APC+1
Placebo
266 ug
13.9
33.7
Sheet1
Placebo266 ug
APC+113.933.7
To resize chart data range, drag lower right corner of
range.
-
T36
Alosetron Improves Global Symptoms in Women with Severe
IBS-D
Krause R et al. Am J Gastroenterol 2007; 102:1709
% GIS Responders
*P
-
T37
Safety Profile of Alosetron
•Black-box warning: serious GI effects •Ischemic colitis
• 2 per 1000 patients over 3 months • 3 per 1000 patients over 6
months
•Constipation •Alosetron (1 mg bid), 29% •Placebo, 6%
•No clinically relevant drug-drug interactions •Pregnancy
category B
Alosetron [package insert]. GlaxoSmithKline; 2006
-
T38
Antispasmodics for IBS
• May be effective for post-prandial pain; unlikely to be
effective for chronic pain
• Cause smooth-muscle relaxation by either • Direct effect (eg,
mebeverine, pinaverium) • Anticholinergic or antimuscarinic
properties
(eg, dicyclomine, hyoscamine) • Calcium channel blockade
(peppermint oil)
• Heterogeneous trials, small sample sizes, • Side effects: dry
mouth, constipation, urinary retention
and visual disturbances
-
T39
Loperamide for IBS with Diarrhea
•Only antidiarrheal studied in IBS
• Three RCTs of low-intermediate quality
•Decreased stool frequency and improved stool consistency but
not abdominal pain or global IBS symptoms
•Most appropriate for patients with diarrhea-predominant
symptoms
Brandt LJ et al. Am J Gastroenterol 2002; 97 suppl:S7
-
ACG Task Force Recommendations for IBS-D
Recommendation Quality Comments Diets Weak Very low Likely to
relate to only
some pts Prebiotics Insufficient
Evidence Probiotics Weak Very low Likely only some pts will
respond Rifaximin Weak Moderate Cost Antispasmodics Weak Low
Likely to be effective only
short-term Loperamide Strong Very low Improves bowel
function
with limited effects on pain Antidepressants Weak High Associate
with AE with a
NNH of 9 Alosetron Weak Moderate Ischemic colitis,
restricted
to women Ford et al., AJG, 2014
-
ACG Task Force Recommendations for IBS-C
Recommendation Quality Comments Diets Weak Very low Likely to
relate to only
some pts Fiber Weak Moderate Psyllium may be more
effective than insoluble fiber
Probiotics Weak Very low Likely only some pts will respond
Polyethylene glycol
Weak Very Low No evidence that PEG improves overall symptoms and
pain in IBS
Lubiprostone Strong Moderate Cost Linaclotide Strong High
Cost
Ford et al., AJG, 2014
-
Rifaximin • Broad spectrum antimicrobial agent
• Minimally absorbed (
-
• 2 identical phase 3, double-blind, placebo-controlled trials
(Target 1 and 2) • Randomized to rifaximin 550 mg or placebo, TID x
2 weeks
Rifaximin for IBS with Diarrhea
1. Pimintel M, Lembo A et al; TARGET Study Group. N Engl J Med.
2011;364:22-32.
-
∆ = 7.6
∆ = 9.0
∆ = 8.1
ReTreatment with Rifaximin in IBS-D IBS-related Abdominal Pain
and Stool Consistency (Worst Case Analysis)
Perc
enta
ge o
f Res
pond
ers
First and Second Repeat Treatment Phases Rifaximin Placebo
44 Responder: Patient responding to IBS-related Abdominal Pain
(>30%
improvement) nd Stool consistency (>50% decrease in # BMs
with type 6 or 7) from Consistency for ≥ 2 of the 4 weeks
Chart1
1st Repeat Tx(Primary Endpoint)1st Repeat Tx(Primary
Endpoint)
2nd Repeat Tx2nd Repeat Tx
Both 1st and 2nd Repeat TxBoth 1st and 2nd Repeat Tx
p = 0.0232
p = 0.0023
p = 0.0263
Rifaximin
Placebo
32.6
25
35.3
27.2
23.1
14.1
Primary ITT
PlaceboRifaximin
1st Repeat Tx(Primary Endpoint)25.032.6
2nd Repeat Tx27.235.3
Both 1st and 2nd Repeat Tx14.123.1
combined
PlaceboRifaximinRifaximinPlacebo
RFIB30073141Pooled Data4132
RFIB30083241
Primary ITT
p = 0.0125
p = 0.0263
∆ = 10
∆ = 9
p = 0.0008
∆ = 9
Rifaximin
Placebo
Percent of Responders
Primary Robust Pool
p = 0.0125
∆ = 10
p = 0.0263
∆ = 9
Rifaximin
Placebo
Percent Responders
Key Sec ITT
p = 0.0008
∆ = 9
Rifaximin
Placebo
Percent Responders
Key Sec Robust Pool
RifaximinPlacebo
PP (LOCF)4131
ITT (Observed Cases)4132
ITT (Multiple Imputation)4233
Key Sec Robust Pool
p = 0.0003
p = 0.0008
p = 0.0010
∆ = 10
∆ = 9
∆ = 9
Rifaximin
Placebo
Percent Responders
Monthly SGA IBS Sym-ITT
RifaximinPlacebo
RFIB30074029
RFIB30084132
Combined Data4030
RifaximinPlacebo
RifaximinPlaceboPooled Data4030
RFIB30074029
RFIB30084132
Monthly SGA IBS Sym-ITT
p = 0.0045
p = 0.0167
∆ = 11
∆ = 9
∆ = 10
p = 0.0002
Rifaximin
Placebo
Monthly SGA IBS Sym-PP
p = 0.0045
∆ = 11
p = 0.0167
∆ = 9
Rifaximin
Placebo
Percent Responders
Monthly SGA Bloating-ITT
∆ = 10
p = 0.0002
Rifaximin
Placebo
Percent Responders
Monthly SGA Bloating-PP
RifaximinPlacebo
PP (LOCF)4130p
-
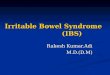
Eluxadoline for IBS-D • Mixed mu (μ) opioid receptor agonist /
delta (δ) opioid receptor
antagonist • Low systemic absorption and bioavailability
– Low potential for drug–drug interactions
• Animal studies suggest eluxadoline should improve the
diarrheal symptoms of IBS-D with limited constipation and durable
analgesia
• Phase IIb 100 and 200 mg BID doses showed efficacy
Activation reduces pain, gastric propulsion
μ opioid receptor
Inhibition restores G-protein signaling;
reduces μ agonist-related desensitization
δ opioid receptor
45
-
Eluxadoline, a mixed mu (μ) opioid receptor agonist / delta (δ)
opioid receptor antagonist for IBS-D
*p30% improvement) and Stool consistency (BSS score
-
Low-dose TCAs Contemporary Antidepressants Psychotherapy
Behavioral interventions
Alosetron Eluxadoline Rifaximin Linaclotide Loperamide
Lubiprostone Antispasmodics Fiber Antispasmodics Laxatives
Reassurance Reassurance
severe
moderate
mild
Diarrhea predominant Constipation predominant alternating
Summary Treatment Options in IBS
Update on Irritable Bowel SyndromeHighlightsEarly description
�of symptoms defining IBSRome III Criteria for IBSEpidemiology
Natural History of IBSImpact of IBS on quality of life �compared
with other medical conditionsSlide Number 8Economic burden of
IBSDisordered CNS-ENS interactions in IBSPathophysiology of IBS
Role of Immune Activation in Post-Infectious IBSKey Organic
Diseases in �Differential Diagnosis of IBSPositive Diagnostic
Strategy Was �Non-inferior to Strategy of Exclusion American
College of Gastroenterology Recommendations for �Diagnostic Testing
in IBSAlarm Features for Organic DisordersSlide Number 17Treatments
for IBSDiets in IBSDietary and Lifestyle Considerations The FODMAP
DietLow-FODMAP vs Typical Australian DietBoth Low-FODMAP and
Traditional IBS Diets Reduced IBS Symptom SeverityPsychological
Therapy for IBSSlide Number 25Pharmacologic Treatments for
IBS�Probiotics Efficacy of Psyllium in IBSPolyethylene Glycol (PEG)
for IBS-CAntidepressants Antidepressants – Tips for improving
EffectivenessOsmotic Laxative Polyethylene glycol (PEG) Improves
Bowel Function But Not Pain in IBS-CSlide Number
33LubiprostoneLinaclotideSlide Number 36Slide Number 37Slide Number
38Slide Number 39ACG Task Force Recommendations for IBS-DACG Task
Force Recommendations for IBS-CRifaximinRifaximin for IBS with
DiarrheaReTreatment with Rifaximin in IBS-D�IBS-related Abdominal
Pain and Stool Consistency (Worst Case Analysis)Eluxadoline for
IBS-DEluxadoline, a mixed mu (μ) opioid receptor agonist / delta
(δ) opioid receptor antagonist for IBS-DSummary Treatment Options
in IBS