-
7/30/2019 Is Complete Lymph Node Dissection After a Positive
Sentinel Lymph Node Biopsy for Cutaneous Melanoma Always
1/12
Review
Is complete lymph node dissection after a positive sentinel
lymph node biopsy forcutaneous melanoma always necessary? A
meta-analysis
V. Nagaraja, G.D. Eslick*
The Whiteley-Martin Research Centre, Discipline of Surgery, The
University of Sydney, Nepean Hospital, Penrith, New South Wales,
Australia
Accepted 20 February 2013
Available online---
Abstract
Background: The current recommendation for patients with
cutaneous melanoma and a positive sentinel lymph node (SLN) biopsy
is a com-plete lymph node dissection (CLND). However, metastatic
melanoma is not present in approximately 80% of CLND specimens. A
meta-
analysis was performed to identify the clinicopathological
variables most predictive of non-sentinel node (NSN) metastases
when the sen-
tinel node is positive in patients with melanoma.
Methods: A systematic search was conducted using MEDLINE,
PubMed, EMBASE, Current Contents Connect, Cochrane library,
Google
scholar, Science Direct, and Web of Science. The search
identified 54 relevant articles reporting the frequency of NSN
metastases in mel-
anoma. Original data was abstracted from each study and used to
calculate a pooled odds ratio (OR) and 95% confidence interval (95%
CI).
Findings: The pooled estimates that were found to be
significantly associated with the high likelihood of NSN metastases
were: ulceration
(OR: 1.88, 95% CI: 1.53e2.31), satellitosis (OR: 3.25, 95% CI:
1.86e5.66), neurotropism (OR: 2.51, 95% CI: 1.39e4.53), >1
positive
SLN (OR: 1.77, 95% CI: 1.2e2.62), Starz 3 (old) (OR: 1.83, 95%
CI: 0.89e3.76), Angiolymphatic invasion (OR: 2.46, 95% CI:
1.34e4.54), extensive location (OR: 2.22, 95% CI: 1.74e2.81),
macrometastases >2 mm (OR: 1.95, 95% CI: 1.61e2.35), extranodal
ex-
tension (OR: 3.38, 95% CI: 1.79e6.40) and capsular involvement
(OR: 3.16, 95% CI: 1.37e7.27). There were 3 characteristics not
asso-
ciated with NSN metastases: subcapsular location (OR: 0.51, 95%
CI: 0.38e0.67), Rotterdam Criteria
-
7/30/2019 Is Complete Lymph Node Dissection After a Positive
Sentinel Lymph Node Biopsy for Cutaneous Melanoma Always
2/12
numerous studies have been published trying to challenge
the standard approach of performing the CLND. Most of
these attempts are based on retrospective studies of pro-
spective databases.11e21 Sentinel node (SN) tumor burden
is the most important prognostic factor for patients with
early stage melanoma.22 Important morphometric classifi-
cations are based on the depth of tumor invasion measuredfrom
the capsule in the SLN (Starz Classification),23 the
microanatomic location (Dewar criteria)24 and the maxi-
mum diameter of the largest tumor lesion (Rotterdam
criteria).20
We sought to determine which of the clinicopathologic
prognostic factors could be used to predict the presence
of positive non-SLNs. We hypothesized that patients with
greater microscopic SLN tumor burden would be at in-
creased risk for non-SLN disease in their CLND specimen,
to assess which classification best predicts additional
lymph
node involvement and that a subset of patients could be
identified in whom the risk of positive non-SLNs is suffi-
ciently low that patients may be spared the morbidity
asso-ciated with lymphadenectomy,25e28 thus helping to identify
patients who would most likely benefit from CLND.
Methods
Study protocol
We followed the Preferred Reporting Items for System-
atic reviews and Meta-Analyses PRISMA guidelines in per-
forming our systematic review.29
We performeda systematic search through MEDLINE (from 1950),
PubMed (from 1946), EMBASE (from 1949), Current Con-
tents Connect (from 1998), Cochrane library, Google
scholar, Science Direct, and Web of Science to March 27,
2013. The search terms included Melanoma AND Sen-
tinel Lymph Node Biopsy AND Lymphatic Metastasis
AND Predictive OR complete lymph node dissection in
Melanoma OR positive non-sentinel lymph nodes in Mela-
noma, which were searched as text word and as exploded
medical subject headings where possible. No language re-
strictions were used in either the search or study
selection.
The reference lists of relevant articles were also searched
for appropriate studies.
Study selection
We included studies that met the following inclusion
criteria:
1. Studies identifying the population of patients with
a positive sentinel lymph node who underwent com-
pletion lymph node dissection; and
2. Original data (or odds ratios) reporting on the number
of SLN positive patients who had positive NSNs
stratified by various patient/tumor characteristics.
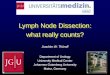
A summary of the search strategy is provided in Fig. 1.
Chu et al.30 and Van der pleog et al.31 were excluded
as the former did not differentiate between NSN positivity
clearly and in the later not all patients with sentinel
lymph positive underwent CLND. There was no extract-
able data in 12 papers6,32e42 and hence they were
excluded.
Data extraction
We performed the data extraction using a standardized
data extraction form, collecting information on the publica-
tion year, study design, number of cases, total sample size,
population type, country, continent, mean age, clinical data
(age, sex, Breslow thickness, SLN tumor burden, ulcera-
tion, satellitosis, regression, neurotropism, histology,
angio-
lymphatic invasion, primary site, sentinel lymph node (sln)
location, SLN tumor characteristic, number of tumor posi-
tive slns, extranodal extension, capsular involvement). Pre-
dominantly 4 SLN tumor burden classifications were used
in these studies namely Dewar classification24 [Subcapsu-
lar: metastasis confined to subcapsular sinus, Combined:
subcapsular and parenchymal metastases, Parenchymal:
Potentially relevant studies
identified and screened for
retrieval (n=507)
Studies excluded, did not meet
the inclusion criteria (n=438)
Studies retrieved for more
detailed evaluation (n=69)
Potentially appropriate studies
to be incl uded in the meta-
analysis (n=57)
Studies included in meta-
analysis (n=54)
Studies with usable
information, by
outcome (n=54)
Studies excluded, no extractable
data (n=12)
Study excluded, with reasons
(n=3)
Studies withdrawn by outcome
with reasons (n=0)
Figure 1. Flowchart of included studies.
2 V. Nagaraja, G.D. Eslick / EJSO xx (2013) 1e12
Please cite this article in press as: Nagaraja V, Eslick GD, Is
complete lymph node dissection after a positive sentinel lymph node
biopsy for cutaneous
melanoma always necessary? A meta-analysis, Eur J Surg Oncol
(2013), http://dx.doi.org/10.1016/j.ejso.2013.02.022
-
7/30/2019 Is Complete Lymph Node Dissection After a Positive
Sentinel Lymph Node Biopsy for Cutaneous Melanoma Always
3/12
metastasis entirely within paracortical area of parenchyma,
Multifocal: Multiple discrete deposits (must include some
parenchymal deposits) Extensive: any metastasis larger
than 5 mm, any node with extracapsular spread], old Starz
classification43 [consisted of three categories; S1, S2 andS3
and these categories were based on the number of pos-
itive sections (n) and the maximum distance from the inte-
rior margin to the capsule of the SN ( d). The criteria for
these respective categories was n < 1 and d< 1 mm for
S1, n > 2 and d > 1 mm for S2 and n > 2 and
d > 1 mm for S3], new Starz classification23
(d< 0.3 mm for SI, d> 0.3 mm and 1 mm for SIII) and
Rotterdam criteria20 [The size of
the SN tumor burden was also recorded, three different tu-
mor burden size groups were defined, sub-micrometastases
(clusters of more than 10 cells, but
1 mm]. The odds ratioand confidence intervals for the above
mentioned parame-
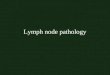
ters were calculated (Figs. 2e8).
Statistical analysis
Pooled odds ratios and 95% confidence intervals were
calculated for the Factors Predicting Positive Nonsentinel
Lymph Nodes using a random effects model.43 We
testedheterogeneity using the I2 statistic, which represents
the
percentage of the total variability across studies which is
due to heterogeneity. I2 values of 25, 50 and 75% corre-
sponded to low, moderate and high degrees of heterogene-
ity respectively.44 We quantified publication bias using the
Eggers regression model45 with the effect of bias assessed
using the fail-safe number method.46 All analyses were per-
formed with Comprehensive Meta-analysis (version 2.0).
Results
Fifty-four studies were included in the analysis (Table 1).The
total number of patients was 8388. The reported preva-
lence of NSN metastases ranges from 8% to 38%.
Figure 2. Extensive location.
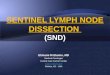
Figure 3. Macrometastases >2 mm.
3V. Nagaraja, G.D. Eslick / EJSO xx (2013) 1e12
Please cite this article in press as: Nagaraja V, Eslick GD, Is
complete lymph node dissection after a positive sentinel lymph node
biopsy for cutaneous
melanoma always necessary? A meta-analysis, Eur J Surg Oncol
(2013), http://dx.doi.org/10.1016/j.ejso.2013.02.022
-
7/30/2019 Is Complete Lymph Node Dissection After a Positive
Sentinel Lymph Node Biopsy for Cutaneous Melanoma Always
4/12
Risk factors for NSN metastases
Factors identified with nonsentinel node metastases were
ulceration (OR: 1.88, 95% CI: 1.53e2.31), satellitosis (OR:
3.25, 95% CI: 1.86e5.66), neurotropism (OR: 2.51, 95% CI:
1.39e4.53), >1 positive SLN (OR: 1.77, 95% CI:
1.2e2.62), Starz 3 (old) [n > 2 and d> 1 mm n (the
number
of 1-mm-thin sentinel lymph node slices with [immuno-]
histologicallydetectable tumor cells) and d(themaximum dis-
tance of tumor cells to the interior margin of the lymph
node
capsule). (OR: 1.83, 95% CI: 0.89e3.76), Angiolymphatic in-
vasion (OR: 2.46, 95% CI: 1.34e4.54), extensive location
(OR: 2.22, 95% CI: 1.74e2.81), macrometastases >2 mm
(OR: 1.95, 95% CI: 1.61e2.35), extranodal extension (OR:
3.38, 95% CI: 1.79e6.40) and capsular involvement (OR:
3.16, 95% CI: 1.37e7.27) as depicted in Table 2. Three char-
acteristics were associated with low risk of NSN metastases:
subcapsular location (OR: 0.51, 95% CI: 0.38e0.67), Rotter-
dam Criteria
-
7/30/2019 Is Complete Lymph Node Dissection After a Positive
Sentinel Lymph Node Biopsy for Cutaneous Melanoma Always
5/12
Discussion
As we try to extend the limits of minimally invasive pro-
cedures, efforts must be made to identify the subset of pa-
tients with a positive SLN who would be spared from the
burden CLND. During the past several years, clinicopatho-logical
variables in 54 well-described studieshave been iden-
tified in an attempt to select those patients most likely to
benefit from CLND when the SLN is positive. This meta-
analysis is the first to indicate that clinical and
pathologic
features of primary melanoma and SLN tumor predict
NSN positivity. Features like ulceration, satellitosis,
neuro-
tropism, >1 positive sln, starz 3 (old), extensive
location
(Dewar classification), macrometastases>2 mm, extranodal
extension, and capsular involvement were found to be signif-
icantly associated with the high likelihood of NSN metasta-
ses. Three characteristics: subcapsular location, rotterdam
criteria2 mm. In their study, no patient with an S/U
score of 0 had a positive NSLN. In addition, patients with
an S/U score of 2 were twice as likely for positive NSLNs
than patients with an S/U score of 1. Roka61 et al. patients
with sentinel node metastasis had a significantly lower S/U
Table 1
Characteristics of the 54 studies included in the systematic
review and meta-analysis.
Author Year Country %Female No. of CLND NSLN positivity%
Younan et al.15 2010 Canada 46.30% 81 12.34%
Fink et al.17 2011 Austria 44.60% 121 24.19%
Fink et al.16 2005 Austria e 26 15.36%
Franco et al.18 2010 Italy 40.42% 47 23.40%
Namikawa et al.19 2012 Japane
149 38.26%Van akkooi et al.91 2008 EORTC Melanoma
Group (MG)
47.00% 388 25.55%
Van der Pleog et al.12 2009 Netherlands e 116 12.93%
Pearlman et al.21 2006 USA e 80 21.25%
Page et al.90 2007 USA e 70 24.30%
Guggenheim et al.89 2008 Switzerland 42.05% 100 22.00%
Glumac et al.88 2008 Slovenia 51.35% 74 21.62%
Denis et al.87 2007 France e 35 14.28%
Francischetto et al.48 2010 Brazil 55.30% 103 25.24%
Scheri et al.60 2007 USA e 52 11.53%
Wiener et al.57 2010 Australia 38.70% 323 16.52%
Ghaferi et al.86 2009 USA 42.00% 429 16.55%
Elias et al.85 2004 USA e 80 15.00%
Debarbieux et al.50 2007 France 42.85% 98 22.20%
Cochran et al.55 2004 USAe
80 21.11%
Ariyan et al.84 2009 USA 34.20% 222 16.66%
Santinami et al.83 2009 Greece e 150 24.00%
Gershenwald et al.47 2008 USA 39.70% 359 14.00%
Frankel et al.82 2008 USA 34.60% 136 21.20%
Cascinelli et al.10 2006 Italy e 176 18.75%
Cadili et al.62 2010 Canada e 111 15.31%
Cadili et al.63 2009 Canada 47.00% 68 18.00%
Cadili et al.81 2010 Australia e 606 23.50%
Quaglino et al.80 2011 Italy e 100 31.00%
Murali et al.11 2011 Australia 38.80% 309 17.20%
Carlson et al.79 2003 USA e 104 15.38%
Van der ploeg et al.13 2011 EORTC Melanoma
Group (MG)
56.50% 1009 21.00%
Lee et al.9 2003 USA e 191 24.00%
Sabel et al.56 2005 USA e 221 15.00%
Van Akkooi et al.20 2006 Netherlands 44.78% 67 14.92%
Govindarajan et al.54 2006 Canada e 127 15.74%
Roka et al.61 2007 Austria 38.82% 85 21.17%
Rossi et al.14 2007 Italy 51.04% 96 20.83%
Satzger et al.49 2008 Germany 40.55% 180 15.55%
Scolyer et al.52 2004 Australia e 140 17.14%
Starz et al.78 2001 Germany e 53 20.75%
Starz et al.23 2004 Germany e 45 26.67%
Dewar et al.24 2004 United Kingdom 44.8% 146 16.43%
Vuylsteke et al.53 2005 Netherlands 48% 71 26.76%
Reeves et al.51 2003 USA 39% 98 16.32%
Pu et al.77 2003 USA e 23 8.69%
Nowecki et al.76 2003 Poland 21.13% 145 26.89%
McMaster et al.75 2002 USA 40.87% 282 15.95%
Kunte et al.74 2010 Germany 36.93% 176 14.77%
Joseph et al.73 1998 USA e 64 7.81%
Wagner et al.72 1999 USA 44.9% 147 17.00%
Wagner et al.93 2000 USA 37.03% 57 26.31%
Wagner et al.92 2003 USA e 90 20.00%
Wagner et al.94 2000 USA 16.67% 12 33.30%
Bogenrieder et al.71 2011 Netherlands 45.7% 70 25.71%
7V. Nagaraja, G.D. Eslick / EJSO xx (2013) 1e12
Please cite this article in press as: Nagaraja V, Eslick GD, Is
complete lymph node dissection after a positive sentinel lymph node
biopsy for cutaneous
melanoma always necessary? A meta-analysis, Eur J Surg Oncol
(2013), http://dx.doi.org/10.1016/j.ejso.2013.02.022
-
7/30/2019 Is Complete Lymph Node Dissection After a Positive
Sentinel Lymph Node Biopsy for Cutaneous Melanoma Always
8/12
score as compared to patients with positive NSLN (median
0 vs. 1; p < 0.04), but still 5 of 42 (12%) of patients
with
a S/U score of zero tested positive for additional lymph
node metastasis upon CLND. Ulceration was a significant
predictor of NSLN with an OR 1.88 of (95% CI
1.53e2.31) in our study.
Risk Score was by proposed The University of Alberta
Hospital.62,63 The score was calculated for each patient ac-
cording to the following criteria: one point for patient age
>55 years, one point for total SLN metastasis size
>5 mm; accordingly, each patient was awarded a score
of 0, 1, or 2. The total score was found to be highly pre-
dictive of CLND positivity with metastasis (p value
-
7/30/2019 Is Complete Lymph Node Dissection After a Positive
Sentinel Lymph Node Biopsy for Cutaneous Melanoma Always
9/12
development of a new model based on these 9 predictors
that is generally applicable among different populations.
Patients with a predicted low risk of further node involve-
ment could then be spared a CLND even if the SLN is
metastatic. Although this model allows stratification of
the risk of NSN involvement and therefore provides useful
prognostic information to aid in management decisions,a
recommendation not to perform CLND should be
made with great caution in patients with positive SNs
and should be based on clinical factors and patient prefer-
ences on a case-by-case basis.
Many retrospective studies (for e.g. Morton et al.,64
Kretschmer et al.,65 van Akkooi AC et al.,66 Nowecki et
al.,67
Faries et al.68 etc), 1 randomized controlled trial and 1
meta-
analysis (Pasquali et al.69) have assessed whether
differences
in survival and regional disease control exist between
patients
having SNB-guided CLND and TLND for clinically evident
lymph node disease. Morton et al.22 depicts that SNB-guided
CLND is associated with a significantly better outcome com-
pared with TLND for clinically evident lymph node diseaseand
strongly suggest that patients with SN-positive melanoma
who underwent immediate CLND had a survival advantage
over those who underwent CLND only when regional lymph
node metastases became clinically apparent.
The considerable variation in reported predictors of NSN
positivity is due to differences in sample size, populations
studied, protocols for pathologic processing and examination
of primary tumors and SNs, and methods of data analysis, as
well asthe effects of interobserver variation in pathologic
in-
terpretation.70 Obviously, all retrospective studies have
the
disadvantage that can be overcome only by a prospective,
randomized controlled trial. Several prospective trials
arecurrently under way to further investigate the possibility
of
reducing the 80% of unnecessary CLND operations.
Whether CLND may be safely avoided in patients at low
risk of NSN positivity (as stratified by N-SNORE, Hannover
Scoring System, Rotterdam system, Dewar Classification,
Starz Classification, Size ulceration score and RD Criteria)
will require investigation in a prospective randomized
clini-
cal trial. The MSLT-II and EORTC MINITUB studies, cur-
rently in progress, are comparing CLND with close clinical
and ultrasound follow-up in patients with SN-positive dis-
ease, and the results may be helpful in determining which
pa-
tients may be safely spared a CLND.
We suggest the development of a new model based on
these 12 predictors that is generally applicable among dif-
ferent populations. Patients with a predicted low risk of
fur-
ther node involvement could then be spared a CLND even
if the SLN is metastatic. However, it is unclear how mini-
mal residual disease left in the axilla would affect the
local
recurrence rate and ultimate prognosis in patients predicted
to have only SLN metastases if the SLNs are involved.
Acknowledgments
None.
Contributors
Vinayak Nagaraja conceived and designed the study. Vi-
nayak Nagaraja provided study materials and identified
studies. Vinayak Nagaraja and Guy D. Eslick collected
and assembled data. Guy D. Eslick analyzed and inter-
preted the data. Vinayak Nagaraja drafted the manuscript.Guy D.
Eslick edited the manuscript.
Funding
Nil.
Conflicts of interest
We declare that we have no conflicts of interest.
References
1. Balch CM, Buzaid AC, Soong SJ, et al. Final version of the
Ameri-
can Joint Committee on Cancer staging system for cutaneous
mela-
noma. J Clin Oncol 2001;19(16):363548.
2. Morton DL, Wen DR, Wong JH, et al. Technical details of
intraoper-
ative lymphatic mapping for early stage melanoma. Arch Surg
1992;
127(4):3929.
3. Thompson JF. The Sydney Melanoma Unit experience of
sentinel
lymphadenectomy for melanoma. Ann Surg Oncol 2001;8(9
Suppl.):44S7S.
4. Thompson JF, Stretch JR, Uren RF, Ka VS, Scolyer RA.
Sentinel
node biopsy for melanoma: where have we been and where are
we
going? Ann Surg Oncol 2004;11(3 Suppl.):147S51S.
5. Morton DL, Thompson JF, Essner R, et al. Validation of the
ac-
curacy of intraoperative lymphatic mapping and sentinel
lympha-denectomy for early-stage melanoma: a multicenter trial.
Multicenter Selective Lymphadenectomy Trial Group. Ann Surg
1999;230(4):45363.
6. Testori A, De Salvo GL, Montesco MC, et al. Clinical
considerations
on sentinel node biopsy in melanoma from an Italian
multicentric
study on 1,313 patients (SOLISM-IMI). Ann Surg Oncol 2009;
16(7):201827.
7. Balch CM. Prognostic factors analysis of 17,600 melanoma
patients:
validation of the American Joint Committee on Cancer
melanoma
staging system. J Clin Oncol 2001;19(16):362234.
8. Balch CM,MortonDL, GershenwaldJE, et al. Sentinel node
biopsyand
standard of carefor melanoma.J Am Acad Dermatol
2009;60(5):8725.
9. Lee JH, Essner R, Torisu-Itakura H, Wanek L, Wang H, Morton
DL.
Factors predictive of tumor-positive nonsentinel lymph nodes
after
tumor-positive sentinel lymph node dissection for melanoma.J
Clin Oncol 2004;22(18):367784.
10. Cascinelli N, Bombardieri E, Bufalino R, et al. Sentinel and
nonsen-
tinel node status in stage IB and II melanoma patients: two-step
prog-
nostic indicators of survival. J Clin Oncol
2006;24(27):446471.
11. Murali R, DesilvaC, ThompsonJF,ScolyerRA. Non-Sentinel Node
Risk
Score (N-SNORE): a scoring system for accurately stratifying
risk of
non-sentinel node positivity in patients with cutaneous melanoma
with
positive sentinel lymph nodes. J Clin Oncol
2010;28(29):44419.
12. van der Ploeg IM, Kroon BB, Antonini N, Valdes Olmos RA,
Nieweg OE. Comparison of three micromorphometric pathology
classifications of melanoma metastases in the sentinel node.
Ann
Surg 2009;250(2):3014.
13. van der Ploeg AP, van Akkooi AC, Rutkowski P, et al.
Prognosis in
patients with sentinel node-positive melanoma is accurately
defined
9V. Nagaraja, G.D. Eslick / EJSO xx (2013) 1e12
Please cite this article in press as: Nagaraja V, Eslick GD, Is
complete lymph node dissection after a positive sentinel lymph node
biopsy for cutaneous
melanoma always necessary? A meta-analysis, Eur J Surg Oncol
(2013), http://dx.doi.org/10.1016/j.ejso.2013.02.022
-
7/30/2019 Is Complete Lymph Node Dissection After a Positive
Sentinel Lymph Node Biopsy for Cutaneous Melanoma Always
10/12
by the combined Rotterdam tumor load and Dewar topography
crite-
ria. J Clin Oncol 2011;29(16):220614.
14. Rossi CR, De Salvo GL, Bonandini E, et al. Factors
predictive of
nonsentinel lymph node involvement and clinical outcome in
mela-
noma patients with metastatic sentinel lymph node. Ann Surg
Oncol
2008;15(4):120210.
15. Younan R, Bougrine A, Watters K, et al. Validation study of
the s
classification for melanoma patients with positive sentinel
nodes:
the Montreal experience. Ann Surg Oncol 2010;17(5):141421.
16. Fink AM, Weihsengruber F, Spangl B, et al. S-classification
of sen-
tinel lymph node biopsy predicts the results of complete
regional
lymph node dissection. Melanoma Res 2005;15(4):26771.
17. Fink AM, Weihsengruber F, Duschek N, et al. Value of
micromor-
phometric criteria of sentinel lymph node metastases in
predicting
further nonsentinel lymph node metastases in patients with
mela-
noma. Melanoma Res 2011;21(2):13943.
18. Franco R, Cantile M, Scala S, et al. Histomorphologic
parameters
and CXCR4 mRNA and protein expression in sentinel node mela-
noma metastasis are correlated to clinical outcome. Cancer
Biol
Ther 2010;9(6):4239.
19. Namikawa K, Yamazaki N, Nakai Y, et al. Prediction of
additional
lymph node positivity and clinical outcome of micrometastases
in
sentinel lymph nodes in cutaneous melanoma: a
multi-institutional
study of 450 patients in Japan. J Dermatol 2012;39(2):1307.
20. van Akkooi AC, de Wilt JH, Verhoef C, et al. Clinical
relevance of
melanoma micrometastases (
-
7/30/2019 Is Complete Lymph Node Dissection After a Positive
Sentinel Lymph Node Biopsy for Cutaneous Melanoma Always
11/12
associated with status of the completion lymphadenectomy and
rate
of subsequent relapse. Ann Surg Oncol 2007;14(2):90612.
55. Cochran AJ, Wen DR, Huang RR, Wang HJ, Elashoff R, Morton
DL.
Prediction of metastatic melanoma in nonsentinel nodes and
clinical
outcome based on the primary melanoma and the sentinel node.
Mod
Pathol 2004;17(7):74755.
56. Sabel MS, Griffith K, Sondak VK, et al. Predictors of
nonsentinel
lymph node positivity in patients with a positive sentinel node
for
melanoma. J Am Coll Surg 2005;201(1):3747.
57. Wiener M, Acland KM, Shaw HM, et al. Sentinel node positive
mel-
anoma patients: prediction and prognostic significance of
nonsentinel
node metastases and development of a survival tree model. Ann
Surg
Oncol 2010;17(8):19952005.
58. Meier A, Satzger I, Volker B, Kapp A, Gutzmer R.
Comparisonof clas-
sification systems in melanoma sentinel lymph nodese an analysis
of
697 patients from a single center.
Cancer2010;116(13):317888.
59. Satzger I, Volker B, Al Ghazal M, Meier A, Kapp A, Gutzmer
R.
Prognostic significance of histopathological parameters in
sentinel
nodes of melanoma patients. Histopathology 2007;50(6):76472.
60. Scheri RP, Essner R, Turner RR, Ye X, Morton DL. Isolated
tumor
cells in the sentinel node affect long-term prognosis of
patients
with melanoma. Ann Surg Oncol 2007;14(10):28616.
61. Roka F, Mastan P, Binder M, et al. Prediction of
non-sentinel node
status and outcome in sentinel node-positive melanoma
patients.
Eur J Surg Oncol 2008;34(1):828.
62. Cadili A, McKinnon G, Wright F, et al. Validation of a
scoring sys-
tem to predict non-sentinel lymph node metastasis in
melanoma.
J Surg Oncol 2010;101(3):1914.
63. Cadili A, Smylie M, Danyluk J, Dabbs K. Prediction of
nonsentinel
lymph node metastasis in malignant melanoma. J Surg Res
2009;
154(2):3249.
64. Morton DL, Hoon DS, Cochran AJ, et al. Lymphatic mapping
and
sentinel lymphadenectomy for early-stage melanoma:
therapeutic
utility and implications of nodal microanatomy and molecular
stag-
ing for improving the accuracy of detection of nodal
micrometasta-
ses. Ann Surg 2003;238(4):53849.
65. Kretschmer L, Hilgers R, Mohrle M, et al. Patients with
lymphatic
metastasis of cutaneous malignant melanoma benefit from
sentinellymphonodectomy and early excision of their nodal disease.
Eur J
Cancer 2004;40(2):2128.
66. van Akkooi AC, Bouwhuis MG, de Wilt JH, Kliffen M, Schmitz
PI,
Eggermont AM. Multivariable analysis comparing outcome after
sentinel node biopsy or therapeutic lymph node dissection in
patients
with melanoma. Br J Surg 2007;94(10):12939.
67. Nowecki ZI, Rutkowski P, Michej W. The survival benefit to
patients
with positive sentinel node melanoma after completion lymph
node
dissection may be limited to the subgroup with a primary lesion
Bre-
slow thickness greater than 1.0 and less than or equal to 4 mm
(pT2-
pT3). Ann Surg Oncol 2008;15(8):222334.
68. Faries MB, Thompson JF, Cochran A, et al. The impact on
morbidity
and length of stay of early versus delayed complete
lymphadenec-
tomy in melanoma: results of the Multicenter Selective
Lymphade-
nectomy Trial (I). Ann Surg Oncol 2010;17(12):33249.69. Pasquali
S, Mocellin S, Campana LG, et al. Early (sentinel lymph
node biopsy-guided) versus delayed lymphadenectomy in
melanoma
patients with lymph node metastases: personal experience and
liter-
ature meta-analysis. Cancer 2010;116(5):12019.
70. Murali R, Cochran AJ, Cook MG, et al. Interobserver
reproducibility
of histologic parameters of melanoma deposits in sentinel lymph
no-
des: implications for management of patients with melanoma.
Can-
cer 2009;115(21):502637.
71. Bogenrieder T, vanDijk MR,Blokx WA, et al. No non-sentinel
node in-
volvement in melanoma patients with limited Breslow thickness
and
low sentinel node tumour load. Histopathology
2011;59(2):31826.
72. Wagner JD, Davidson D, Coleman 3rd JJ, et al. Lymph node
tumor
volumes in patients undergoing sentinel lymph node biopsy for
cuta-
neous melanoma. Ann Surg Oncol 1999;6(4):398404.
73. Joseph E, Brobeil A, Glass F, et al. Results of complete
lymph node
dissection in 83 melanoma patients with positive sentinel nodes.
Ann
Surg Oncol 1998;5(2):11925.
74. Kunte C, Geimer T, Baumert J, et al. Analysis of predictive
factors
for the outcome of complete lymph node dissection in melanoma
pa-
tients with metastatic sentinel lymph nodes. J Am Acad
Dermatol
2011;64(4):65562.
75. McMasters KM, Wong SL, Edwards MJ, et al. Frequency of
nonsen-
tinel lymph node metastasis in melanoma. Ann Surg Oncol
2002;
9(2):13741.
76. Nowecki ZI, Rutkowski P, Nasierowska-Guttmejer A, Ruka W.
Sen-
tinel lymph node biopsy in melanoma patients with clinically
nega-
tive regional lymph nodes e one institutions experience.
Melanoma Res 2003;13(1):3543.
77. Pu LL, Wells KE, Cruse CW, Shons AR, Reintgen DS. Prevalence
of
additional positive lymph nodes in complete lymphadenectomy
spec-
imens after positive sentinel lymphadenectomy findings for
early-
stage melanoma of the head and neck. Plast Reconstr Surg
2003;
112(1):439.
78. Starz H, Balda BR, Kramer KU, Buchels H, Wang H.
A micromorphometry-based concept for routine classification of
sen-
tinel lymph node metastases and its clinical relevance for
patients
with melanoma. Cancer 2001;91(11):211021.
79. Carlson GW, Murray DR, Lyles RH, Staley CA, Hestley A, Cohen
C.
The amount of metastatic melanoma in a sentinel lymph node: does
it
have prognostic significance? Ann Surg Oncol
2003;10(5):57581.
80. Quaglino P, Ribero S, Osella-Abate S, et al.
Clinico-pathologic fea-
tures of primary melanoma and sentinel lymph node predictive
for
non-sentinel lymph node involvement and overall survival in
mela-
noma patients: a single centre observational cohort study. Surg
Oncol
2011;20(4):25964.
81. Cadili A, Scolyer RA, Brown PT, Dabbs K, Thompson JF. Total
sen-
tinel lymph node tumor size predicts nonsentinel node metastasis
and
survival in patients with melanoma. Ann Surg Oncol
2010;17(11):
301520.
82. Frankel TL,GriffithKA, Lowe L, et al. Do micromorphometric
features
of metastatic deposits within sentinel nodes predict nonsentinel
lymph
node involvement in melanoma?Ann Surg Oncol
2008;15(9):240311.83. Santinami M, Carbone A, Crippa F, et al.
Radical dissection after
positive groin sentinel biopsy in melanoma patients: rate of
further
positive nodes. Melanoma Res 2009;19(2):1128.
84. Ariyan C, Brady MS, Gonen M, Busam K, Coit D. Positive
nonsen-
tinel node status predicts mortality in patients with cutaneous
mela-
noma. Ann Surg Oncol 2009;16(1):18690.
85. Elias N, Tanabe KK, Sober AJ, et al. Is completion
lymphadenec-
tomy after a positive sentinel lymph node biopsy for cutaneous
mel-
anoma always necessary? Arch Surg 2004;139(4):4004.
86. Ghaferi AA, Wong SL, Johnson TM, et al. Prognostic
significance of
a positive nonsentinel lymph node in cutaneous melanoma. Ann
Surg
Oncol 2009;16(11):297884.
87. Denis MH, Dudrap E, Courville P, Auquit-Auckbur I, Joly
P,
Milliez PY. Influence of the size and the localization of
metastases
in melanoma sentinel lymph nodes on the results of
lymphadenec-tomy. Ann Chir Plast Esthet 2007;52(1):2834.
88. Glumac N, Hocevar M, Zadnik V, Snoj M. Sentinel lymph node
mi-
crometastasis may predict non-sentinel involvement in
cutaneous
melanoma patients. J Surg Oncol 2008;98(1):468.
89. Guggenheim MM, Hug U, Jung FJ, et al. Morbidity and
recurrence
after completion lymph node dissection following sentinel
lymph
node biopsy in cutaneous malignant melanoma. Ann Surg 2008;
247(4):68793.
90. Page AJ, Carlson GW, Delman KA, Murray D, Hestley A, Cohen
C.
Prediction of nonsentinel lymph node involvement in patients
with
a positive sentinel lymph node in malignant melanoma. Am
Surg
2007;73(7):6748.
91. van Akkooi AC, Nowecki ZI, Voit C, et al. Sentinel node
tumor bur-
den according to the Rotterdam criteria is the most
important
11V. Nagaraja, G.D. Eslick / EJSO xx (2013) 1e12
Please cite this article in press as: Nagaraja V, Eslick GD, Is
complete lymph node dissection after a positive sentinel lymph node
biopsy for cutaneous
melanoma always necessary? A meta-analysis, Eur J Surg Oncol
(2013), http://dx.doi.org/10.1016/j.ejso.2013.02.022
-
7/30/2019 Is Complete Lymph Node Dissection After a Positive
Sentinel Lymph Node Biopsy for Cutaneous Melanoma Always
12/12
prognostic factor for survival in melanoma patients: a
multicenter
study in 388 patients with positive sentinel nodes. Ann Surg
2008;
248(6):94955.
92. Wagner JD, Ranieri J, Evdokimow DZ, et al. Patterns of
initial recur-
rence and prognosis after sentinel lymph node biopsy and
selective
lymphadenectomy for melanoma. Plast Reconstr Surg
2003;112(2):
48697.
93. Wagner JD, Park HM, Coleman 3rd JJ, Love C, Hayes JT.
Cervical
sentinel lymph node biopsy for melanomas of the head and
neck
and upper thorax. Arch Otolaryngol Head Neck Surg
2000;126(3):
31321.
94. Wagner JD, Gordon MS, Chuang TY, et al. Predicting sentinel
and
residual lymph node basin disease after sentinel lymph node
biopsy
for melanoma. Cancer 2000;89(2):45362.
12 V. Nagaraja, G.D. Eslick / EJSO xx (2013) 1e12
Please cite this article in press as: Nagaraja V, Eslick GD, Is
complete lymph node dissection after a positive sentinel lymph node
biopsy for cutaneous
melanoma always necessary? A meta-analysis Eur J Surg Oncol
(2013) http://dx doi org/10 1016/j ejso 2013 02 022