Embed Size (px)
Citation preview

Is Neuromonitoring an expensive waste of
time in Severe Traumatic Brain Injury
Ross Bullock MD PhD Director Neurotrauma-
University of Miami Jackson Memorial Hospital Miami
EngorgementEngorgementEdemaEdema
DiffuseAxonal Injury
DiffuseAxonal Injury
HypoxiaHypoxia
HematomaHematoma ContusionContusion
Subcellular mechanisms in TBI SAH ICH Stroke
ldquoMonitors alone cannot save patients but wise application of the data from monitoring
the injured brain canrdquo Saul Ducker 1983 Monitoring vs serial imaging
Severe TBI-- Does it all make a difference
bull Mortality rates fallinghellip~80 before WWII ndash 60 in 1960rsquos 40 in 1980rsquos ~20 in 2000hellip ndash Most cost effective surgical procedure of all is craniotomy
for EDHhellip
Age (years)
Prob
abilit
y of
out
com
e (
)
20 40 60 80
0
20
40
60
80
100
Probability of deathhellipsevere TBI-2007
Ischemic Tissue Damage and Infarction is Dependent on Reduction of Oxygen Delivery
and the Duration of the Ischemic Insult
Substrate delivery Monitoringhellip pannecrosis
Why is ICP Monitoring so Important
bull 80 in hospital deaths from high ICP
bull ldquobarometerrdquo of ldquostandard of carerdquohelliprdquolevel II guidelinerdquo
bull Best way to implement more ICP monitoring maybe by concentrating patients at hospitals who do ithellip
bull ldquoGold bookrdquo requirement for Level 1 centershellip
Neuromonitoring Methodshellip bull Functional status of the CNShellip
ndash GCS Neuro exam EEG Evoked potentials EcoG Pupillometer
Substrate delivery to the injured Brainhellip -CBF ICP CPP MABP PtiO2 Jugular Bulb oximetry
AVDO2 NIR spectroscopy Microdialysis
Combined methodshellip ldquoBrain Biomarkersrdquo--the future S100B alpha Spectrin beta amyloid
The NIH-NINDS Trial of ICP Monitoring in BoliviaLABIChellip
4 hospitals PRCT~350 pts
bull ldquoWe are still likely to continue to doubt clinical
bull signs which indeed do not reflect global pressure inside the cranium but stupor coma posturing and dilatation of the pupils indicate compression of the midbrain and according to this study they are very suitable observations to
bull use in directing treatmentrdquohellip
ldquoIn the future there may be other means of detecting
early compression of the brain stem Until then
clinical methods are finerdquo
Why the Chesnut Bolivia ICP monitoring trial is not ldquogeneralisablerdquo to rest of the
worldhellip bull Only about 50 of severe TBI cases got into ICUhellipbed limitationshellip bull No prehospital care no rehab poor
ldquo subacute ldquophase care40 mortalityhellip bull ~47 decompressive craniotomy used in
both groups ~23 barbiturates 1 ventricular drainage
bull mean~ 20 hours with ICPgt20mmHg
bull Increased mortality in patients with severe traumatic brain injury treated without intracranial pressure monitoring
Arash Farahvar MD PhD1 Linda M Gerber PhD2 Ya-Lin Chiu MS2 bull Nancy Carney PhD3 Roger Haumlrtl MD4 and Jam shid Ghaja r MD PhD45 bull 1Department of Neurosurgery University of Rochester Medical Center Rochester Departments of 2Public bull Health and 4Neurological Surgery Weill Cornell Medical College and 5Brain Trauma Foundation bull New York New York and 3Department of Medical Informatics and Clinical Epidemiology Oregon bull Health amp Science University Portland Oregon bull Object Evidence-based guidelines recommend intracranial pressure (ICP) monitoring for patients with severe bull traumatic brain injury (TBI) but there is limited evidence that monitoring and treating intracranial hypertension
reduces bull mortality This study uses a large prospectively collected database to examine the effect on 2-week mortality bull of ICP reduction therapies administered to patients with severe TBI treated either with or without an ICP
monitor bull Methods From a population of 2134 patients with severe TBI (Glasgow Coma Scale [GCS] Score lt 9) 1446 bull patients were treated with ICP-lowering therapies Of those 1202 had an ICP monitor inserted and 244 were
treated bull without monitoring Patients were admitted to one of 20 Level I and two Level II trauma centers part of a New
York bull State quality improvement program administered by the Brain Trauma Foundation between 2000 and 2009 bull Results Age initial GCS score hypotension and CT scan findings were associated with 2-week mortality In bull addition patients of all ages treated with an ICP monitor in place had lower mortality at 2 weeks (p = 002)
than those bull treated without an ICP monitor after adjusting for parameters that independently affect mortality bull Conclusions In patients with severe TBI treated for intracranial
hypertension the use of an ICP monitor is associated with significantly lower mortality when compared with patients treated without an ICP monitor Based on these findings the authors conclude that ICP-directed therapy in patients with severe TBI should be guided by ICP monitoring
bull (httpthejnsorgdoiabs10317120127JNS111816)
Neuromonitoring Methodshellip bull Functional status of the CNShellip
ndash GCS Neuro exam EEG Evoked potentials EcoG Pupillometer
Substrate delivery to the injured Brainhellip -CBF ICP CPP MABP PtiO2 Jugular Bulb oximetry
AVDO2 NIR spectroscopy Microdialysis
Combined methodshellip ldquoBrain Biomarkersrdquo--the future S100B alpha Spectrin beta amyloid
Related Articles Links
Increased incidence and impact of nonconvulsive and convulsive seizures after traumatic brain injury as detected by continuous electroencephalographic monitoring Vespa PM Nuwer MR Nenov V Ronne-Engstrom E Hovda DA Bergsneider M Kelly DF Martin NA Becker DP Department of Neurology University of California at Los Angeles School of Medicine 90024 USA Convulsive and nonconvulsive seizures occurred in 21 (22) of the 94 patients with six of them displaying status epilepticus In more than half of the patients (52) the seizures were nonconvulsive and were diagnosed on the basis of EEG studies alone All six patients with status epilepticus died compared with a mortality rate of 24 (18 of 73) in the nonseizure group (plt0001) The patients with status epilepticus had a shorter mean length of stay (914+-59 days compared with 14+-9 days [t-test plt0031) Seizures occurred despite initiation of prophylactic phenytoin on admission to the emergency room with maintenance at mean levels of 166+-28 mgdlCONCLUSIONS Seizures occur in more than one in five patients during the 1st week after moderate-to-severe brain injury and may play a role in the pathobiological conditions associated with brain injury
J Neurosurg 1999 Nov91(5)750-60
Human TBIhellipand COSBID suppression of large amplitude delta activity (eg PLEDs)
EEG
DC
1 s
1 min
Temperature ranges
All temps during monitoring
Temp during CSD
lt 350 17 10
350-380 58 23
gt380 25 68
Chi-square plt0001
N=~130 USAEU
Expl
aine
d Va
rianc
e N
agel
kerk
ersquos R
2
Univariate Analysis-outcome
0002004006008
01012014016018
Significance at plt005
350355360365370375380385390395400
1800 00
060
012
0018
00 000
600
1200
1800 00
060
012
0018
00 000
600
Synergistic pathomechanisms are commonesthellip
Do we need synergistic THERAPIES For multiple damage Mechanisms
0
100
200
300
400
500
600
700
800
0 20 40 60 80 100
Between 24 - 48 h after Injury
Brain tissue oxygen tension (PtiO2)
0
50
100
150
200
250
300
350
0 20 40 60 80 100
Brain tissue oxygen tension (PtiO2)H
Between 6 -24 h after Injury
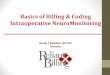
Tissue Oxygen Tension in Humans after TBI
Brain pO2 Outcome lt20 mmHg Poor 20-30 mmHg Moderate gt30 mmHg Good
Therapy in both patient groups was aimed at maintaining an ICP less than 20 mm Hg and a CPP greater than 60 mm Hg Among patients
whose brain tissue PO2 was monitored oxygenation was maintained at levels greater
than 25 mm Hg
J Neurosurg 103805ndash811 2005
Reduced mortality rate in patients with severe traumatic brain injury treated with brain tissue oxygen monitoring
M STIEFEL MD PHD M S GRADY MD AND P D LE ROUX MD U Penn
Patients treated with ICP and brain tissue PO2 monitoring
were compared with historical controls
The mortality rate in patients treated using conventional ICP and CPP management was 44 Patients who also
underwent brain tissue PO2 monitoring had a significantly reduced mortality rate of 25 (p 005)
PtO2
TBI Clinical Trials--ongoinghellip2013 Clinical trials Gov n= 762 (n= 307 in 2010) DOD effecthellip$120M in 2007hellip
80 observationalhellip
bull Brain 0xygen ndashdirected therapyhellipBOOSTUT NIH
bull COSBIDmdashEcoGhellipfor Spreading depolarisations
bull IMPACThellip bull TRACK II-III bull Non ndashinvasive ICPrdquoECHODIA ldquo systemX2 bull PET to trace Neuroinflammation in STBINIH
CBF monitoring
bull Transcranial Doppler Monitoring bull Easy to use noninvasive
repeatable bull Measures basal cerebral bld flow
velocity flow via doppler equation bull Used to differentiate vasospasm
from hyperaemia (Lindegaard Index)
What has been achieved by monitoring the injured Brain
bull Improved understanding of dynamic pathophysiology after HUMAN TBI SAH
bull Guide design of neuroprotection trialshellip bull Improved patient outcome
Age (years)
Pro
babi
lity
of o
utco
me
()
20 40 60 80
0
20
40
60
80
100
Death rate ndashsevere TBI
bull Australia and NZ bull The Alfred
Royal Melbourne Hospital Royal Adelaide Hospital Royal Perth Hospital Sir Charles Gairdner Hospital Nepean Hospital John Hunter Hospital Royal North Shore Hospital Liverpool Hospital Wollongong Hospital Princess Alexandra Hospital Gold Coast Hospital Flinders Medical Centre Auckland Hospital Waikato Hospital Wellington Hospital
bull Saudi Arabia King Fahad National Guard Hospital
Canada bull Hamilton General hospital
Vancouver General Hospital Sunnybrook Medical Centre Royal Columbian Hospital India
bull Christian Medical College Ludhiana
bull
bull
Early bifrontal decompression Vs medical management No benefit from surgeryhellipmore disabled and vegetative outcomes
3 editorials on the DECRA tria
bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

Subcellular mechanisms in TBI SAH ICH Stroke
ldquoMonitors alone cannot save patients but wise application of the data from monitoring
the injured brain canrdquo Saul Ducker 1983 Monitoring vs serial imaging
Severe TBI-- Does it all make a difference
bull Mortality rates fallinghellip~80 before WWII ndash 60 in 1960rsquos 40 in 1980rsquos ~20 in 2000hellip ndash Most cost effective surgical procedure of all is craniotomy
for EDHhellip
Age (years)
Prob
abilit
y of
out
com
e (
)
20 40 60 80
0
20
40
60
80
100
Probability of deathhellipsevere TBI-2007
Ischemic Tissue Damage and Infarction is Dependent on Reduction of Oxygen Delivery
and the Duration of the Ischemic Insult
Substrate delivery Monitoringhellip pannecrosis
Why is ICP Monitoring so Important
bull 80 in hospital deaths from high ICP
bull ldquobarometerrdquo of ldquostandard of carerdquohelliprdquolevel II guidelinerdquo
bull Best way to implement more ICP monitoring maybe by concentrating patients at hospitals who do ithellip
bull ldquoGold bookrdquo requirement for Level 1 centershellip
Neuromonitoring Methodshellip bull Functional status of the CNShellip
ndash GCS Neuro exam EEG Evoked potentials EcoG Pupillometer
Substrate delivery to the injured Brainhellip -CBF ICP CPP MABP PtiO2 Jugular Bulb oximetry
AVDO2 NIR spectroscopy Microdialysis
Combined methodshellip ldquoBrain Biomarkersrdquo--the future S100B alpha Spectrin beta amyloid
The NIH-NINDS Trial of ICP Monitoring in BoliviaLABIChellip
4 hospitals PRCT~350 pts
bull ldquoWe are still likely to continue to doubt clinical
bull signs which indeed do not reflect global pressure inside the cranium but stupor coma posturing and dilatation of the pupils indicate compression of the midbrain and according to this study they are very suitable observations to
bull use in directing treatmentrdquohellip
ldquoIn the future there may be other means of detecting
early compression of the brain stem Until then
clinical methods are finerdquo
Why the Chesnut Bolivia ICP monitoring trial is not ldquogeneralisablerdquo to rest of the
worldhellip bull Only about 50 of severe TBI cases got into ICUhellipbed limitationshellip bull No prehospital care no rehab poor
ldquo subacute ldquophase care40 mortalityhellip bull ~47 decompressive craniotomy used in
both groups ~23 barbiturates 1 ventricular drainage
bull mean~ 20 hours with ICPgt20mmHg
bull Increased mortality in patients with severe traumatic brain injury treated without intracranial pressure monitoring
Arash Farahvar MD PhD1 Linda M Gerber PhD2 Ya-Lin Chiu MS2 bull Nancy Carney PhD3 Roger Haumlrtl MD4 and Jam shid Ghaja r MD PhD45 bull 1Department of Neurosurgery University of Rochester Medical Center Rochester Departments of 2Public bull Health and 4Neurological Surgery Weill Cornell Medical College and 5Brain Trauma Foundation bull New York New York and 3Department of Medical Informatics and Clinical Epidemiology Oregon bull Health amp Science University Portland Oregon bull Object Evidence-based guidelines recommend intracranial pressure (ICP) monitoring for patients with severe bull traumatic brain injury (TBI) but there is limited evidence that monitoring and treating intracranial hypertension
reduces bull mortality This study uses a large prospectively collected database to examine the effect on 2-week mortality bull of ICP reduction therapies administered to patients with severe TBI treated either with or without an ICP
monitor bull Methods From a population of 2134 patients with severe TBI (Glasgow Coma Scale [GCS] Score lt 9) 1446 bull patients were treated with ICP-lowering therapies Of those 1202 had an ICP monitor inserted and 244 were
treated bull without monitoring Patients were admitted to one of 20 Level I and two Level II trauma centers part of a New
York bull State quality improvement program administered by the Brain Trauma Foundation between 2000 and 2009 bull Results Age initial GCS score hypotension and CT scan findings were associated with 2-week mortality In bull addition patients of all ages treated with an ICP monitor in place had lower mortality at 2 weeks (p = 002)
than those bull treated without an ICP monitor after adjusting for parameters that independently affect mortality bull Conclusions In patients with severe TBI treated for intracranial
hypertension the use of an ICP monitor is associated with significantly lower mortality when compared with patients treated without an ICP monitor Based on these findings the authors conclude that ICP-directed therapy in patients with severe TBI should be guided by ICP monitoring
bull (httpthejnsorgdoiabs10317120127JNS111816)
Neuromonitoring Methodshellip bull Functional status of the CNShellip
ndash GCS Neuro exam EEG Evoked potentials EcoG Pupillometer
Substrate delivery to the injured Brainhellip -CBF ICP CPP MABP PtiO2 Jugular Bulb oximetry
AVDO2 NIR spectroscopy Microdialysis
Combined methodshellip ldquoBrain Biomarkersrdquo--the future S100B alpha Spectrin beta amyloid
Related Articles Links
Increased incidence and impact of nonconvulsive and convulsive seizures after traumatic brain injury as detected by continuous electroencephalographic monitoring Vespa PM Nuwer MR Nenov V Ronne-Engstrom E Hovda DA Bergsneider M Kelly DF Martin NA Becker DP Department of Neurology University of California at Los Angeles School of Medicine 90024 USA Convulsive and nonconvulsive seizures occurred in 21 (22) of the 94 patients with six of them displaying status epilepticus In more than half of the patients (52) the seizures were nonconvulsive and were diagnosed on the basis of EEG studies alone All six patients with status epilepticus died compared with a mortality rate of 24 (18 of 73) in the nonseizure group (plt0001) The patients with status epilepticus had a shorter mean length of stay (914+-59 days compared with 14+-9 days [t-test plt0031) Seizures occurred despite initiation of prophylactic phenytoin on admission to the emergency room with maintenance at mean levels of 166+-28 mgdlCONCLUSIONS Seizures occur in more than one in five patients during the 1st week after moderate-to-severe brain injury and may play a role in the pathobiological conditions associated with brain injury
J Neurosurg 1999 Nov91(5)750-60
Human TBIhellipand COSBID suppression of large amplitude delta activity (eg PLEDs)
EEG
DC
1 s
1 min
Temperature ranges
All temps during monitoring
Temp during CSD
lt 350 17 10
350-380 58 23
gt380 25 68
Chi-square plt0001
N=~130 USAEU
Expl
aine
d Va
rianc
e N
agel
kerk
ersquos R
2
Univariate Analysis-outcome
0002004006008
01012014016018
Significance at plt005
350355360365370375380385390395400
1800 00
060
012
0018
00 000
600
1200
1800 00
060
012
0018
00 000
600
Synergistic pathomechanisms are commonesthellip
Do we need synergistic THERAPIES For multiple damage Mechanisms
0
100
200
300
400
500
600
700
800
0 20 40 60 80 100
Between 24 - 48 h after Injury
Brain tissue oxygen tension (PtiO2)
0
50
100
150
200
250
300
350
0 20 40 60 80 100
Brain tissue oxygen tension (PtiO2)H
Between 6 -24 h after Injury
Tissue Oxygen Tension in Humans after TBI
Brain pO2 Outcome lt20 mmHg Poor 20-30 mmHg Moderate gt30 mmHg Good
Therapy in both patient groups was aimed at maintaining an ICP less than 20 mm Hg and a CPP greater than 60 mm Hg Among patients
whose brain tissue PO2 was monitored oxygenation was maintained at levels greater
than 25 mm Hg
J Neurosurg 103805ndash811 2005
Reduced mortality rate in patients with severe traumatic brain injury treated with brain tissue oxygen monitoring
M STIEFEL MD PHD M S GRADY MD AND P D LE ROUX MD U Penn
Patients treated with ICP and brain tissue PO2 monitoring
were compared with historical controls
The mortality rate in patients treated using conventional ICP and CPP management was 44 Patients who also
underwent brain tissue PO2 monitoring had a significantly reduced mortality rate of 25 (p 005)
PtO2
TBI Clinical Trials--ongoinghellip2013 Clinical trials Gov n= 762 (n= 307 in 2010) DOD effecthellip$120M in 2007hellip
80 observationalhellip
bull Brain 0xygen ndashdirected therapyhellipBOOSTUT NIH
bull COSBIDmdashEcoGhellipfor Spreading depolarisations
bull IMPACThellip bull TRACK II-III bull Non ndashinvasive ICPrdquoECHODIA ldquo systemX2 bull PET to trace Neuroinflammation in STBINIH
CBF monitoring
bull Transcranial Doppler Monitoring bull Easy to use noninvasive
repeatable bull Measures basal cerebral bld flow
velocity flow via doppler equation bull Used to differentiate vasospasm
from hyperaemia (Lindegaard Index)
What has been achieved by monitoring the injured Brain
bull Improved understanding of dynamic pathophysiology after HUMAN TBI SAH
bull Guide design of neuroprotection trialshellip bull Improved patient outcome
Age (years)
Pro
babi
lity
of o
utco
me
()
20 40 60 80
0
20
40
60
80
100
Death rate ndashsevere TBI
bull Australia and NZ bull The Alfred
Royal Melbourne Hospital Royal Adelaide Hospital Royal Perth Hospital Sir Charles Gairdner Hospital Nepean Hospital John Hunter Hospital Royal North Shore Hospital Liverpool Hospital Wollongong Hospital Princess Alexandra Hospital Gold Coast Hospital Flinders Medical Centre Auckland Hospital Waikato Hospital Wellington Hospital
bull Saudi Arabia King Fahad National Guard Hospital
Canada bull Hamilton General hospital
Vancouver General Hospital Sunnybrook Medical Centre Royal Columbian Hospital India
bull Christian Medical College Ludhiana
bull
bull
Early bifrontal decompression Vs medical management No benefit from surgeryhellipmore disabled and vegetative outcomes
3 editorials on the DECRA tria
bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

ldquoMonitors alone cannot save patients but wise application of the data from monitoring
the injured brain canrdquo Saul Ducker 1983 Monitoring vs serial imaging
Severe TBI-- Does it all make a difference
bull Mortality rates fallinghellip~80 before WWII ndash 60 in 1960rsquos 40 in 1980rsquos ~20 in 2000hellip ndash Most cost effective surgical procedure of all is craniotomy
for EDHhellip
Age (years)
Prob
abilit
y of
out
com
e (
)
20 40 60 80
0
20
40
60
80
100
Probability of deathhellipsevere TBI-2007
Ischemic Tissue Damage and Infarction is Dependent on Reduction of Oxygen Delivery
and the Duration of the Ischemic Insult
Substrate delivery Monitoringhellip pannecrosis
Why is ICP Monitoring so Important
bull 80 in hospital deaths from high ICP
bull ldquobarometerrdquo of ldquostandard of carerdquohelliprdquolevel II guidelinerdquo
bull Best way to implement more ICP monitoring maybe by concentrating patients at hospitals who do ithellip
bull ldquoGold bookrdquo requirement for Level 1 centershellip
Neuromonitoring Methodshellip bull Functional status of the CNShellip
ndash GCS Neuro exam EEG Evoked potentials EcoG Pupillometer
Substrate delivery to the injured Brainhellip -CBF ICP CPP MABP PtiO2 Jugular Bulb oximetry
AVDO2 NIR spectroscopy Microdialysis
Combined methodshellip ldquoBrain Biomarkersrdquo--the future S100B alpha Spectrin beta amyloid
The NIH-NINDS Trial of ICP Monitoring in BoliviaLABIChellip
4 hospitals PRCT~350 pts
bull ldquoWe are still likely to continue to doubt clinical
bull signs which indeed do not reflect global pressure inside the cranium but stupor coma posturing and dilatation of the pupils indicate compression of the midbrain and according to this study they are very suitable observations to
bull use in directing treatmentrdquohellip
ldquoIn the future there may be other means of detecting
early compression of the brain stem Until then
clinical methods are finerdquo
Why the Chesnut Bolivia ICP monitoring trial is not ldquogeneralisablerdquo to rest of the
worldhellip bull Only about 50 of severe TBI cases got into ICUhellipbed limitationshellip bull No prehospital care no rehab poor
ldquo subacute ldquophase care40 mortalityhellip bull ~47 decompressive craniotomy used in
both groups ~23 barbiturates 1 ventricular drainage
bull mean~ 20 hours with ICPgt20mmHg
bull Increased mortality in patients with severe traumatic brain injury treated without intracranial pressure monitoring
Arash Farahvar MD PhD1 Linda M Gerber PhD2 Ya-Lin Chiu MS2 bull Nancy Carney PhD3 Roger Haumlrtl MD4 and Jam shid Ghaja r MD PhD45 bull 1Department of Neurosurgery University of Rochester Medical Center Rochester Departments of 2Public bull Health and 4Neurological Surgery Weill Cornell Medical College and 5Brain Trauma Foundation bull New York New York and 3Department of Medical Informatics and Clinical Epidemiology Oregon bull Health amp Science University Portland Oregon bull Object Evidence-based guidelines recommend intracranial pressure (ICP) monitoring for patients with severe bull traumatic brain injury (TBI) but there is limited evidence that monitoring and treating intracranial hypertension
reduces bull mortality This study uses a large prospectively collected database to examine the effect on 2-week mortality bull of ICP reduction therapies administered to patients with severe TBI treated either with or without an ICP
monitor bull Methods From a population of 2134 patients with severe TBI (Glasgow Coma Scale [GCS] Score lt 9) 1446 bull patients were treated with ICP-lowering therapies Of those 1202 had an ICP monitor inserted and 244 were
treated bull without monitoring Patients were admitted to one of 20 Level I and two Level II trauma centers part of a New
York bull State quality improvement program administered by the Brain Trauma Foundation between 2000 and 2009 bull Results Age initial GCS score hypotension and CT scan findings were associated with 2-week mortality In bull addition patients of all ages treated with an ICP monitor in place had lower mortality at 2 weeks (p = 002)
than those bull treated without an ICP monitor after adjusting for parameters that independently affect mortality bull Conclusions In patients with severe TBI treated for intracranial
hypertension the use of an ICP monitor is associated with significantly lower mortality when compared with patients treated without an ICP monitor Based on these findings the authors conclude that ICP-directed therapy in patients with severe TBI should be guided by ICP monitoring
bull (httpthejnsorgdoiabs10317120127JNS111816)
Neuromonitoring Methodshellip bull Functional status of the CNShellip
ndash GCS Neuro exam EEG Evoked potentials EcoG Pupillometer
Substrate delivery to the injured Brainhellip -CBF ICP CPP MABP PtiO2 Jugular Bulb oximetry
AVDO2 NIR spectroscopy Microdialysis
Combined methodshellip ldquoBrain Biomarkersrdquo--the future S100B alpha Spectrin beta amyloid
Related Articles Links
Increased incidence and impact of nonconvulsive and convulsive seizures after traumatic brain injury as detected by continuous electroencephalographic monitoring Vespa PM Nuwer MR Nenov V Ronne-Engstrom E Hovda DA Bergsneider M Kelly DF Martin NA Becker DP Department of Neurology University of California at Los Angeles School of Medicine 90024 USA Convulsive and nonconvulsive seizures occurred in 21 (22) of the 94 patients with six of them displaying status epilepticus In more than half of the patients (52) the seizures were nonconvulsive and were diagnosed on the basis of EEG studies alone All six patients with status epilepticus died compared with a mortality rate of 24 (18 of 73) in the nonseizure group (plt0001) The patients with status epilepticus had a shorter mean length of stay (914+-59 days compared with 14+-9 days [t-test plt0031) Seizures occurred despite initiation of prophylactic phenytoin on admission to the emergency room with maintenance at mean levels of 166+-28 mgdlCONCLUSIONS Seizures occur in more than one in five patients during the 1st week after moderate-to-severe brain injury and may play a role in the pathobiological conditions associated with brain injury
J Neurosurg 1999 Nov91(5)750-60
Human TBIhellipand COSBID suppression of large amplitude delta activity (eg PLEDs)
EEG
DC
1 s
1 min
Temperature ranges
All temps during monitoring
Temp during CSD
lt 350 17 10
350-380 58 23
gt380 25 68
Chi-square plt0001
N=~130 USAEU
Expl
aine
d Va
rianc
e N
agel
kerk
ersquos R
2
Univariate Analysis-outcome
0002004006008
01012014016018
Significance at plt005
350355360365370375380385390395400
1800 00
060
012
0018
00 000
600
1200
1800 00
060
012
0018
00 000
600
Synergistic pathomechanisms are commonesthellip
Do we need synergistic THERAPIES For multiple damage Mechanisms
0
100
200
300
400
500
600
700
800
0 20 40 60 80 100
Between 24 - 48 h after Injury
Brain tissue oxygen tension (PtiO2)
0
50
100
150
200
250
300
350
0 20 40 60 80 100
Brain tissue oxygen tension (PtiO2)H
Between 6 -24 h after Injury
Tissue Oxygen Tension in Humans after TBI
Brain pO2 Outcome lt20 mmHg Poor 20-30 mmHg Moderate gt30 mmHg Good
Therapy in both patient groups was aimed at maintaining an ICP less than 20 mm Hg and a CPP greater than 60 mm Hg Among patients
whose brain tissue PO2 was monitored oxygenation was maintained at levels greater
than 25 mm Hg
J Neurosurg 103805ndash811 2005
Reduced mortality rate in patients with severe traumatic brain injury treated with brain tissue oxygen monitoring
M STIEFEL MD PHD M S GRADY MD AND P D LE ROUX MD U Penn
Patients treated with ICP and brain tissue PO2 monitoring
were compared with historical controls
The mortality rate in patients treated using conventional ICP and CPP management was 44 Patients who also
underwent brain tissue PO2 monitoring had a significantly reduced mortality rate of 25 (p 005)
PtO2
TBI Clinical Trials--ongoinghellip2013 Clinical trials Gov n= 762 (n= 307 in 2010) DOD effecthellip$120M in 2007hellip
80 observationalhellip
bull Brain 0xygen ndashdirected therapyhellipBOOSTUT NIH
bull COSBIDmdashEcoGhellipfor Spreading depolarisations
bull IMPACThellip bull TRACK II-III bull Non ndashinvasive ICPrdquoECHODIA ldquo systemX2 bull PET to trace Neuroinflammation in STBINIH
CBF monitoring
bull Transcranial Doppler Monitoring bull Easy to use noninvasive
repeatable bull Measures basal cerebral bld flow
velocity flow via doppler equation bull Used to differentiate vasospasm
from hyperaemia (Lindegaard Index)
What has been achieved by monitoring the injured Brain
bull Improved understanding of dynamic pathophysiology after HUMAN TBI SAH
bull Guide design of neuroprotection trialshellip bull Improved patient outcome
Age (years)
Pro
babi
lity
of o
utco
me
()
20 40 60 80
0
20
40
60
80
100
Death rate ndashsevere TBI
bull Australia and NZ bull The Alfred
Royal Melbourne Hospital Royal Adelaide Hospital Royal Perth Hospital Sir Charles Gairdner Hospital Nepean Hospital John Hunter Hospital Royal North Shore Hospital Liverpool Hospital Wollongong Hospital Princess Alexandra Hospital Gold Coast Hospital Flinders Medical Centre Auckland Hospital Waikato Hospital Wellington Hospital
bull Saudi Arabia King Fahad National Guard Hospital
Canada bull Hamilton General hospital
Vancouver General Hospital Sunnybrook Medical Centre Royal Columbian Hospital India
bull Christian Medical College Ludhiana
bull
bull
Early bifrontal decompression Vs medical management No benefit from surgeryhellipmore disabled and vegetative outcomes
3 editorials on the DECRA tria
bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

Severe TBI-- Does it all make a difference
bull Mortality rates fallinghellip~80 before WWII ndash 60 in 1960rsquos 40 in 1980rsquos ~20 in 2000hellip ndash Most cost effective surgical procedure of all is craniotomy
for EDHhellip
Age (years)
Prob
abilit
y of
out
com
e (
)
20 40 60 80
0
20
40
60
80
100
Probability of deathhellipsevere TBI-2007
Ischemic Tissue Damage and Infarction is Dependent on Reduction of Oxygen Delivery
and the Duration of the Ischemic Insult
Substrate delivery Monitoringhellip pannecrosis
Why is ICP Monitoring so Important
bull 80 in hospital deaths from high ICP
bull ldquobarometerrdquo of ldquostandard of carerdquohelliprdquolevel II guidelinerdquo
bull Best way to implement more ICP monitoring maybe by concentrating patients at hospitals who do ithellip
bull ldquoGold bookrdquo requirement for Level 1 centershellip
Neuromonitoring Methodshellip bull Functional status of the CNShellip
ndash GCS Neuro exam EEG Evoked potentials EcoG Pupillometer
Substrate delivery to the injured Brainhellip -CBF ICP CPP MABP PtiO2 Jugular Bulb oximetry
AVDO2 NIR spectroscopy Microdialysis
Combined methodshellip ldquoBrain Biomarkersrdquo--the future S100B alpha Spectrin beta amyloid
The NIH-NINDS Trial of ICP Monitoring in BoliviaLABIChellip
4 hospitals PRCT~350 pts
bull ldquoWe are still likely to continue to doubt clinical
bull signs which indeed do not reflect global pressure inside the cranium but stupor coma posturing and dilatation of the pupils indicate compression of the midbrain and according to this study they are very suitable observations to
bull use in directing treatmentrdquohellip
ldquoIn the future there may be other means of detecting
early compression of the brain stem Until then
clinical methods are finerdquo
Why the Chesnut Bolivia ICP monitoring trial is not ldquogeneralisablerdquo to rest of the
worldhellip bull Only about 50 of severe TBI cases got into ICUhellipbed limitationshellip bull No prehospital care no rehab poor
ldquo subacute ldquophase care40 mortalityhellip bull ~47 decompressive craniotomy used in
both groups ~23 barbiturates 1 ventricular drainage
bull mean~ 20 hours with ICPgt20mmHg
bull Increased mortality in patients with severe traumatic brain injury treated without intracranial pressure monitoring
Arash Farahvar MD PhD1 Linda M Gerber PhD2 Ya-Lin Chiu MS2 bull Nancy Carney PhD3 Roger Haumlrtl MD4 and Jam shid Ghaja r MD PhD45 bull 1Department of Neurosurgery University of Rochester Medical Center Rochester Departments of 2Public bull Health and 4Neurological Surgery Weill Cornell Medical College and 5Brain Trauma Foundation bull New York New York and 3Department of Medical Informatics and Clinical Epidemiology Oregon bull Health amp Science University Portland Oregon bull Object Evidence-based guidelines recommend intracranial pressure (ICP) monitoring for patients with severe bull traumatic brain injury (TBI) but there is limited evidence that monitoring and treating intracranial hypertension
reduces bull mortality This study uses a large prospectively collected database to examine the effect on 2-week mortality bull of ICP reduction therapies administered to patients with severe TBI treated either with or without an ICP
monitor bull Methods From a population of 2134 patients with severe TBI (Glasgow Coma Scale [GCS] Score lt 9) 1446 bull patients were treated with ICP-lowering therapies Of those 1202 had an ICP monitor inserted and 244 were
treated bull without monitoring Patients were admitted to one of 20 Level I and two Level II trauma centers part of a New
York bull State quality improvement program administered by the Brain Trauma Foundation between 2000 and 2009 bull Results Age initial GCS score hypotension and CT scan findings were associated with 2-week mortality In bull addition patients of all ages treated with an ICP monitor in place had lower mortality at 2 weeks (p = 002)
than those bull treated without an ICP monitor after adjusting for parameters that independently affect mortality bull Conclusions In patients with severe TBI treated for intracranial
hypertension the use of an ICP monitor is associated with significantly lower mortality when compared with patients treated without an ICP monitor Based on these findings the authors conclude that ICP-directed therapy in patients with severe TBI should be guided by ICP monitoring
bull (httpthejnsorgdoiabs10317120127JNS111816)
Neuromonitoring Methodshellip bull Functional status of the CNShellip
ndash GCS Neuro exam EEG Evoked potentials EcoG Pupillometer
Substrate delivery to the injured Brainhellip -CBF ICP CPP MABP PtiO2 Jugular Bulb oximetry
AVDO2 NIR spectroscopy Microdialysis
Combined methodshellip ldquoBrain Biomarkersrdquo--the future S100B alpha Spectrin beta amyloid
Related Articles Links
Increased incidence and impact of nonconvulsive and convulsive seizures after traumatic brain injury as detected by continuous electroencephalographic monitoring Vespa PM Nuwer MR Nenov V Ronne-Engstrom E Hovda DA Bergsneider M Kelly DF Martin NA Becker DP Department of Neurology University of California at Los Angeles School of Medicine 90024 USA Convulsive and nonconvulsive seizures occurred in 21 (22) of the 94 patients with six of them displaying status epilepticus In more than half of the patients (52) the seizures were nonconvulsive and were diagnosed on the basis of EEG studies alone All six patients with status epilepticus died compared with a mortality rate of 24 (18 of 73) in the nonseizure group (plt0001) The patients with status epilepticus had a shorter mean length of stay (914+-59 days compared with 14+-9 days [t-test plt0031) Seizures occurred despite initiation of prophylactic phenytoin on admission to the emergency room with maintenance at mean levels of 166+-28 mgdlCONCLUSIONS Seizures occur in more than one in five patients during the 1st week after moderate-to-severe brain injury and may play a role in the pathobiological conditions associated with brain injury
J Neurosurg 1999 Nov91(5)750-60
Human TBIhellipand COSBID suppression of large amplitude delta activity (eg PLEDs)
EEG
DC
1 s
1 min
Temperature ranges
All temps during monitoring
Temp during CSD
lt 350 17 10
350-380 58 23
gt380 25 68
Chi-square plt0001
N=~130 USAEU
Expl
aine
d Va
rianc
e N
agel
kerk
ersquos R
2
Univariate Analysis-outcome
0002004006008
01012014016018
Significance at plt005
350355360365370375380385390395400
1800 00
060
012
0018
00 000
600
1200
1800 00
060
012
0018
00 000
600
Synergistic pathomechanisms are commonesthellip
Do we need synergistic THERAPIES For multiple damage Mechanisms
0
100
200
300
400
500
600
700
800
0 20 40 60 80 100
Between 24 - 48 h after Injury
Brain tissue oxygen tension (PtiO2)
0
50
100
150
200
250
300
350
0 20 40 60 80 100
Brain tissue oxygen tension (PtiO2)H
Between 6 -24 h after Injury
Tissue Oxygen Tension in Humans after TBI
Brain pO2 Outcome lt20 mmHg Poor 20-30 mmHg Moderate gt30 mmHg Good
Therapy in both patient groups was aimed at maintaining an ICP less than 20 mm Hg and a CPP greater than 60 mm Hg Among patients
whose brain tissue PO2 was monitored oxygenation was maintained at levels greater
than 25 mm Hg
J Neurosurg 103805ndash811 2005
Reduced mortality rate in patients with severe traumatic brain injury treated with brain tissue oxygen monitoring
M STIEFEL MD PHD M S GRADY MD AND P D LE ROUX MD U Penn
Patients treated with ICP and brain tissue PO2 monitoring
were compared with historical controls
The mortality rate in patients treated using conventional ICP and CPP management was 44 Patients who also
underwent brain tissue PO2 monitoring had a significantly reduced mortality rate of 25 (p 005)
PtO2
TBI Clinical Trials--ongoinghellip2013 Clinical trials Gov n= 762 (n= 307 in 2010) DOD effecthellip$120M in 2007hellip
80 observationalhellip
bull Brain 0xygen ndashdirected therapyhellipBOOSTUT NIH
bull COSBIDmdashEcoGhellipfor Spreading depolarisations
bull IMPACThellip bull TRACK II-III bull Non ndashinvasive ICPrdquoECHODIA ldquo systemX2 bull PET to trace Neuroinflammation in STBINIH
CBF monitoring
bull Transcranial Doppler Monitoring bull Easy to use noninvasive
repeatable bull Measures basal cerebral bld flow
velocity flow via doppler equation bull Used to differentiate vasospasm
from hyperaemia (Lindegaard Index)
What has been achieved by monitoring the injured Brain
bull Improved understanding of dynamic pathophysiology after HUMAN TBI SAH
bull Guide design of neuroprotection trialshellip bull Improved patient outcome
Age (years)
Pro
babi
lity
of o
utco
me
()
20 40 60 80
0
20
40
60
80
100
Death rate ndashsevere TBI
bull Australia and NZ bull The Alfred
Royal Melbourne Hospital Royal Adelaide Hospital Royal Perth Hospital Sir Charles Gairdner Hospital Nepean Hospital John Hunter Hospital Royal North Shore Hospital Liverpool Hospital Wollongong Hospital Princess Alexandra Hospital Gold Coast Hospital Flinders Medical Centre Auckland Hospital Waikato Hospital Wellington Hospital
bull Saudi Arabia King Fahad National Guard Hospital
Canada bull Hamilton General hospital
Vancouver General Hospital Sunnybrook Medical Centre Royal Columbian Hospital India
bull Christian Medical College Ludhiana
bull
bull
Early bifrontal decompression Vs medical management No benefit from surgeryhellipmore disabled and vegetative outcomes
3 editorials on the DECRA tria
bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

Ischemic Tissue Damage and Infarction is Dependent on Reduction of Oxygen Delivery
and the Duration of the Ischemic Insult
Substrate delivery Monitoringhellip pannecrosis
Why is ICP Monitoring so Important
bull 80 in hospital deaths from high ICP
bull ldquobarometerrdquo of ldquostandard of carerdquohelliprdquolevel II guidelinerdquo
bull Best way to implement more ICP monitoring maybe by concentrating patients at hospitals who do ithellip
bull ldquoGold bookrdquo requirement for Level 1 centershellip
Neuromonitoring Methodshellip bull Functional status of the CNShellip
ndash GCS Neuro exam EEG Evoked potentials EcoG Pupillometer
Substrate delivery to the injured Brainhellip -CBF ICP CPP MABP PtiO2 Jugular Bulb oximetry
AVDO2 NIR spectroscopy Microdialysis
Combined methodshellip ldquoBrain Biomarkersrdquo--the future S100B alpha Spectrin beta amyloid
The NIH-NINDS Trial of ICP Monitoring in BoliviaLABIChellip
4 hospitals PRCT~350 pts
bull ldquoWe are still likely to continue to doubt clinical
bull signs which indeed do not reflect global pressure inside the cranium but stupor coma posturing and dilatation of the pupils indicate compression of the midbrain and according to this study they are very suitable observations to
bull use in directing treatmentrdquohellip
ldquoIn the future there may be other means of detecting
early compression of the brain stem Until then
clinical methods are finerdquo
Why the Chesnut Bolivia ICP monitoring trial is not ldquogeneralisablerdquo to rest of the
worldhellip bull Only about 50 of severe TBI cases got into ICUhellipbed limitationshellip bull No prehospital care no rehab poor
ldquo subacute ldquophase care40 mortalityhellip bull ~47 decompressive craniotomy used in
both groups ~23 barbiturates 1 ventricular drainage
bull mean~ 20 hours with ICPgt20mmHg
bull Increased mortality in patients with severe traumatic brain injury treated without intracranial pressure monitoring
Arash Farahvar MD PhD1 Linda M Gerber PhD2 Ya-Lin Chiu MS2 bull Nancy Carney PhD3 Roger Haumlrtl MD4 and Jam shid Ghaja r MD PhD45 bull 1Department of Neurosurgery University of Rochester Medical Center Rochester Departments of 2Public bull Health and 4Neurological Surgery Weill Cornell Medical College and 5Brain Trauma Foundation bull New York New York and 3Department of Medical Informatics and Clinical Epidemiology Oregon bull Health amp Science University Portland Oregon bull Object Evidence-based guidelines recommend intracranial pressure (ICP) monitoring for patients with severe bull traumatic brain injury (TBI) but there is limited evidence that monitoring and treating intracranial hypertension
reduces bull mortality This study uses a large prospectively collected database to examine the effect on 2-week mortality bull of ICP reduction therapies administered to patients with severe TBI treated either with or without an ICP
monitor bull Methods From a population of 2134 patients with severe TBI (Glasgow Coma Scale [GCS] Score lt 9) 1446 bull patients were treated with ICP-lowering therapies Of those 1202 had an ICP monitor inserted and 244 were
treated bull without monitoring Patients were admitted to one of 20 Level I and two Level II trauma centers part of a New
York bull State quality improvement program administered by the Brain Trauma Foundation between 2000 and 2009 bull Results Age initial GCS score hypotension and CT scan findings were associated with 2-week mortality In bull addition patients of all ages treated with an ICP monitor in place had lower mortality at 2 weeks (p = 002)
than those bull treated without an ICP monitor after adjusting for parameters that independently affect mortality bull Conclusions In patients with severe TBI treated for intracranial
hypertension the use of an ICP monitor is associated with significantly lower mortality when compared with patients treated without an ICP monitor Based on these findings the authors conclude that ICP-directed therapy in patients with severe TBI should be guided by ICP monitoring
bull (httpthejnsorgdoiabs10317120127JNS111816)
Neuromonitoring Methodshellip bull Functional status of the CNShellip
ndash GCS Neuro exam EEG Evoked potentials EcoG Pupillometer
Substrate delivery to the injured Brainhellip -CBF ICP CPP MABP PtiO2 Jugular Bulb oximetry
AVDO2 NIR spectroscopy Microdialysis
Combined methodshellip ldquoBrain Biomarkersrdquo--the future S100B alpha Spectrin beta amyloid
Related Articles Links
Increased incidence and impact of nonconvulsive and convulsive seizures after traumatic brain injury as detected by continuous electroencephalographic monitoring Vespa PM Nuwer MR Nenov V Ronne-Engstrom E Hovda DA Bergsneider M Kelly DF Martin NA Becker DP Department of Neurology University of California at Los Angeles School of Medicine 90024 USA Convulsive and nonconvulsive seizures occurred in 21 (22) of the 94 patients with six of them displaying status epilepticus In more than half of the patients (52) the seizures were nonconvulsive and were diagnosed on the basis of EEG studies alone All six patients with status epilepticus died compared with a mortality rate of 24 (18 of 73) in the nonseizure group (plt0001) The patients with status epilepticus had a shorter mean length of stay (914+-59 days compared with 14+-9 days [t-test plt0031) Seizures occurred despite initiation of prophylactic phenytoin on admission to the emergency room with maintenance at mean levels of 166+-28 mgdlCONCLUSIONS Seizures occur in more than one in five patients during the 1st week after moderate-to-severe brain injury and may play a role in the pathobiological conditions associated with brain injury
J Neurosurg 1999 Nov91(5)750-60
Human TBIhellipand COSBID suppression of large amplitude delta activity (eg PLEDs)
EEG
DC
1 s
1 min
Temperature ranges
All temps during monitoring
Temp during CSD
lt 350 17 10
350-380 58 23
gt380 25 68
Chi-square plt0001
N=~130 USAEU
Expl
aine
d Va
rianc
e N
agel
kerk
ersquos R
2
Univariate Analysis-outcome
0002004006008
01012014016018
Significance at plt005
350355360365370375380385390395400
1800 00
060
012
0018
00 000
600
1200
1800 00
060
012
0018
00 000
600
Synergistic pathomechanisms are commonesthellip
Do we need synergistic THERAPIES For multiple damage Mechanisms
0
100
200
300
400
500
600
700
800
0 20 40 60 80 100
Between 24 - 48 h after Injury
Brain tissue oxygen tension (PtiO2)
0
50
100
150
200
250
300
350
0 20 40 60 80 100
Brain tissue oxygen tension (PtiO2)H
Between 6 -24 h after Injury
Tissue Oxygen Tension in Humans after TBI
Brain pO2 Outcome lt20 mmHg Poor 20-30 mmHg Moderate gt30 mmHg Good
Therapy in both patient groups was aimed at maintaining an ICP less than 20 mm Hg and a CPP greater than 60 mm Hg Among patients
whose brain tissue PO2 was monitored oxygenation was maintained at levels greater
than 25 mm Hg
J Neurosurg 103805ndash811 2005
Reduced mortality rate in patients with severe traumatic brain injury treated with brain tissue oxygen monitoring
M STIEFEL MD PHD M S GRADY MD AND P D LE ROUX MD U Penn
Patients treated with ICP and brain tissue PO2 monitoring
were compared with historical controls
The mortality rate in patients treated using conventional ICP and CPP management was 44 Patients who also
underwent brain tissue PO2 monitoring had a significantly reduced mortality rate of 25 (p 005)
PtO2
TBI Clinical Trials--ongoinghellip2013 Clinical trials Gov n= 762 (n= 307 in 2010) DOD effecthellip$120M in 2007hellip
80 observationalhellip
bull Brain 0xygen ndashdirected therapyhellipBOOSTUT NIH
bull COSBIDmdashEcoGhellipfor Spreading depolarisations
bull IMPACThellip bull TRACK II-III bull Non ndashinvasive ICPrdquoECHODIA ldquo systemX2 bull PET to trace Neuroinflammation in STBINIH
CBF monitoring
bull Transcranial Doppler Monitoring bull Easy to use noninvasive
repeatable bull Measures basal cerebral bld flow
velocity flow via doppler equation bull Used to differentiate vasospasm
from hyperaemia (Lindegaard Index)
What has been achieved by monitoring the injured Brain
bull Improved understanding of dynamic pathophysiology after HUMAN TBI SAH
bull Guide design of neuroprotection trialshellip bull Improved patient outcome
Age (years)
Pro
babi
lity
of o
utco
me
()
20 40 60 80
0
20
40
60
80
100
Death rate ndashsevere TBI
bull Australia and NZ bull The Alfred
Royal Melbourne Hospital Royal Adelaide Hospital Royal Perth Hospital Sir Charles Gairdner Hospital Nepean Hospital John Hunter Hospital Royal North Shore Hospital Liverpool Hospital Wollongong Hospital Princess Alexandra Hospital Gold Coast Hospital Flinders Medical Centre Auckland Hospital Waikato Hospital Wellington Hospital
bull Saudi Arabia King Fahad National Guard Hospital
Canada bull Hamilton General hospital
Vancouver General Hospital Sunnybrook Medical Centre Royal Columbian Hospital India
bull Christian Medical College Ludhiana
bull
bull
Early bifrontal decompression Vs medical management No benefit from surgeryhellipmore disabled and vegetative outcomes
3 editorials on the DECRA tria
bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

Why is ICP Monitoring so Important
bull 80 in hospital deaths from high ICP
bull ldquobarometerrdquo of ldquostandard of carerdquohelliprdquolevel II guidelinerdquo
bull Best way to implement more ICP monitoring maybe by concentrating patients at hospitals who do ithellip
bull ldquoGold bookrdquo requirement for Level 1 centershellip
Neuromonitoring Methodshellip bull Functional status of the CNShellip
ndash GCS Neuro exam EEG Evoked potentials EcoG Pupillometer
Substrate delivery to the injured Brainhellip -CBF ICP CPP MABP PtiO2 Jugular Bulb oximetry
AVDO2 NIR spectroscopy Microdialysis
Combined methodshellip ldquoBrain Biomarkersrdquo--the future S100B alpha Spectrin beta amyloid
The NIH-NINDS Trial of ICP Monitoring in BoliviaLABIChellip
4 hospitals PRCT~350 pts
bull ldquoWe are still likely to continue to doubt clinical
bull signs which indeed do not reflect global pressure inside the cranium but stupor coma posturing and dilatation of the pupils indicate compression of the midbrain and according to this study they are very suitable observations to
bull use in directing treatmentrdquohellip
ldquoIn the future there may be other means of detecting
early compression of the brain stem Until then
clinical methods are finerdquo
Why the Chesnut Bolivia ICP monitoring trial is not ldquogeneralisablerdquo to rest of the
worldhellip bull Only about 50 of severe TBI cases got into ICUhellipbed limitationshellip bull No prehospital care no rehab poor
ldquo subacute ldquophase care40 mortalityhellip bull ~47 decompressive craniotomy used in
both groups ~23 barbiturates 1 ventricular drainage
bull mean~ 20 hours with ICPgt20mmHg
bull Increased mortality in patients with severe traumatic brain injury treated without intracranial pressure monitoring
Arash Farahvar MD PhD1 Linda M Gerber PhD2 Ya-Lin Chiu MS2 bull Nancy Carney PhD3 Roger Haumlrtl MD4 and Jam shid Ghaja r MD PhD45 bull 1Department of Neurosurgery University of Rochester Medical Center Rochester Departments of 2Public bull Health and 4Neurological Surgery Weill Cornell Medical College and 5Brain Trauma Foundation bull New York New York and 3Department of Medical Informatics and Clinical Epidemiology Oregon bull Health amp Science University Portland Oregon bull Object Evidence-based guidelines recommend intracranial pressure (ICP) monitoring for patients with severe bull traumatic brain injury (TBI) but there is limited evidence that monitoring and treating intracranial hypertension
reduces bull mortality This study uses a large prospectively collected database to examine the effect on 2-week mortality bull of ICP reduction therapies administered to patients with severe TBI treated either with or without an ICP
monitor bull Methods From a population of 2134 patients with severe TBI (Glasgow Coma Scale [GCS] Score lt 9) 1446 bull patients were treated with ICP-lowering therapies Of those 1202 had an ICP monitor inserted and 244 were
treated bull without monitoring Patients were admitted to one of 20 Level I and two Level II trauma centers part of a New
York bull State quality improvement program administered by the Brain Trauma Foundation between 2000 and 2009 bull Results Age initial GCS score hypotension and CT scan findings were associated with 2-week mortality In bull addition patients of all ages treated with an ICP monitor in place had lower mortality at 2 weeks (p = 002)
than those bull treated without an ICP monitor after adjusting for parameters that independently affect mortality bull Conclusions In patients with severe TBI treated for intracranial
hypertension the use of an ICP monitor is associated with significantly lower mortality when compared with patients treated without an ICP monitor Based on these findings the authors conclude that ICP-directed therapy in patients with severe TBI should be guided by ICP monitoring
bull (httpthejnsorgdoiabs10317120127JNS111816)
Neuromonitoring Methodshellip bull Functional status of the CNShellip
ndash GCS Neuro exam EEG Evoked potentials EcoG Pupillometer
Substrate delivery to the injured Brainhellip -CBF ICP CPP MABP PtiO2 Jugular Bulb oximetry
AVDO2 NIR spectroscopy Microdialysis
Combined methodshellip ldquoBrain Biomarkersrdquo--the future S100B alpha Spectrin beta amyloid
Related Articles Links
Increased incidence and impact of nonconvulsive and convulsive seizures after traumatic brain injury as detected by continuous electroencephalographic monitoring Vespa PM Nuwer MR Nenov V Ronne-Engstrom E Hovda DA Bergsneider M Kelly DF Martin NA Becker DP Department of Neurology University of California at Los Angeles School of Medicine 90024 USA Convulsive and nonconvulsive seizures occurred in 21 (22) of the 94 patients with six of them displaying status epilepticus In more than half of the patients (52) the seizures were nonconvulsive and were diagnosed on the basis of EEG studies alone All six patients with status epilepticus died compared with a mortality rate of 24 (18 of 73) in the nonseizure group (plt0001) The patients with status epilepticus had a shorter mean length of stay (914+-59 days compared with 14+-9 days [t-test plt0031) Seizures occurred despite initiation of prophylactic phenytoin on admission to the emergency room with maintenance at mean levels of 166+-28 mgdlCONCLUSIONS Seizures occur in more than one in five patients during the 1st week after moderate-to-severe brain injury and may play a role in the pathobiological conditions associated with brain injury
J Neurosurg 1999 Nov91(5)750-60
Human TBIhellipand COSBID suppression of large amplitude delta activity (eg PLEDs)
EEG
DC
1 s
1 min
Temperature ranges
All temps during monitoring
Temp during CSD
lt 350 17 10
350-380 58 23
gt380 25 68
Chi-square plt0001
N=~130 USAEU
Expl
aine
d Va
rianc
e N
agel
kerk
ersquos R
2
Univariate Analysis-outcome
0002004006008
01012014016018
Significance at plt005
350355360365370375380385390395400
1800 00
060
012
0018
00 000
600
1200
1800 00
060
012
0018
00 000
600
Synergistic pathomechanisms are commonesthellip
Do we need synergistic THERAPIES For multiple damage Mechanisms
0
100
200
300
400
500
600
700
800
0 20 40 60 80 100
Between 24 - 48 h after Injury
Brain tissue oxygen tension (PtiO2)
0
50
100
150
200
250
300
350
0 20 40 60 80 100
Brain tissue oxygen tension (PtiO2)H
Between 6 -24 h after Injury
Tissue Oxygen Tension in Humans after TBI
Brain pO2 Outcome lt20 mmHg Poor 20-30 mmHg Moderate gt30 mmHg Good
Therapy in both patient groups was aimed at maintaining an ICP less than 20 mm Hg and a CPP greater than 60 mm Hg Among patients
whose brain tissue PO2 was monitored oxygenation was maintained at levels greater
than 25 mm Hg
J Neurosurg 103805ndash811 2005
Reduced mortality rate in patients with severe traumatic brain injury treated with brain tissue oxygen monitoring
M STIEFEL MD PHD M S GRADY MD AND P D LE ROUX MD U Penn
Patients treated with ICP and brain tissue PO2 monitoring
were compared with historical controls
The mortality rate in patients treated using conventional ICP and CPP management was 44 Patients who also
underwent brain tissue PO2 monitoring had a significantly reduced mortality rate of 25 (p 005)
PtO2
TBI Clinical Trials--ongoinghellip2013 Clinical trials Gov n= 762 (n= 307 in 2010) DOD effecthellip$120M in 2007hellip
80 observationalhellip
bull Brain 0xygen ndashdirected therapyhellipBOOSTUT NIH
bull COSBIDmdashEcoGhellipfor Spreading depolarisations
bull IMPACThellip bull TRACK II-III bull Non ndashinvasive ICPrdquoECHODIA ldquo systemX2 bull PET to trace Neuroinflammation in STBINIH
CBF monitoring
bull Transcranial Doppler Monitoring bull Easy to use noninvasive
repeatable bull Measures basal cerebral bld flow
velocity flow via doppler equation bull Used to differentiate vasospasm
from hyperaemia (Lindegaard Index)
What has been achieved by monitoring the injured Brain
bull Improved understanding of dynamic pathophysiology after HUMAN TBI SAH
bull Guide design of neuroprotection trialshellip bull Improved patient outcome
Age (years)
Pro
babi
lity
of o
utco
me
()
20 40 60 80
0
20
40
60
80
100
Death rate ndashsevere TBI
bull Australia and NZ bull The Alfred
Royal Melbourne Hospital Royal Adelaide Hospital Royal Perth Hospital Sir Charles Gairdner Hospital Nepean Hospital John Hunter Hospital Royal North Shore Hospital Liverpool Hospital Wollongong Hospital Princess Alexandra Hospital Gold Coast Hospital Flinders Medical Centre Auckland Hospital Waikato Hospital Wellington Hospital
bull Saudi Arabia King Fahad National Guard Hospital
Canada bull Hamilton General hospital
Vancouver General Hospital Sunnybrook Medical Centre Royal Columbian Hospital India
bull Christian Medical College Ludhiana
bull
bull
Early bifrontal decompression Vs medical management No benefit from surgeryhellipmore disabled and vegetative outcomes
3 editorials on the DECRA tria
bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

Neuromonitoring Methodshellip bull Functional status of the CNShellip
ndash GCS Neuro exam EEG Evoked potentials EcoG Pupillometer
Substrate delivery to the injured Brainhellip -CBF ICP CPP MABP PtiO2 Jugular Bulb oximetry
AVDO2 NIR spectroscopy Microdialysis
Combined methodshellip ldquoBrain Biomarkersrdquo--the future S100B alpha Spectrin beta amyloid
The NIH-NINDS Trial of ICP Monitoring in BoliviaLABIChellip
4 hospitals PRCT~350 pts
bull ldquoWe are still likely to continue to doubt clinical
bull signs which indeed do not reflect global pressure inside the cranium but stupor coma posturing and dilatation of the pupils indicate compression of the midbrain and according to this study they are very suitable observations to
bull use in directing treatmentrdquohellip
ldquoIn the future there may be other means of detecting
early compression of the brain stem Until then
clinical methods are finerdquo
Why the Chesnut Bolivia ICP monitoring trial is not ldquogeneralisablerdquo to rest of the
worldhellip bull Only about 50 of severe TBI cases got into ICUhellipbed limitationshellip bull No prehospital care no rehab poor
ldquo subacute ldquophase care40 mortalityhellip bull ~47 decompressive craniotomy used in
both groups ~23 barbiturates 1 ventricular drainage
bull mean~ 20 hours with ICPgt20mmHg
bull Increased mortality in patients with severe traumatic brain injury treated without intracranial pressure monitoring
Arash Farahvar MD PhD1 Linda M Gerber PhD2 Ya-Lin Chiu MS2 bull Nancy Carney PhD3 Roger Haumlrtl MD4 and Jam shid Ghaja r MD PhD45 bull 1Department of Neurosurgery University of Rochester Medical Center Rochester Departments of 2Public bull Health and 4Neurological Surgery Weill Cornell Medical College and 5Brain Trauma Foundation bull New York New York and 3Department of Medical Informatics and Clinical Epidemiology Oregon bull Health amp Science University Portland Oregon bull Object Evidence-based guidelines recommend intracranial pressure (ICP) monitoring for patients with severe bull traumatic brain injury (TBI) but there is limited evidence that monitoring and treating intracranial hypertension
reduces bull mortality This study uses a large prospectively collected database to examine the effect on 2-week mortality bull of ICP reduction therapies administered to patients with severe TBI treated either with or without an ICP
monitor bull Methods From a population of 2134 patients with severe TBI (Glasgow Coma Scale [GCS] Score lt 9) 1446 bull patients were treated with ICP-lowering therapies Of those 1202 had an ICP monitor inserted and 244 were
treated bull without monitoring Patients were admitted to one of 20 Level I and two Level II trauma centers part of a New
York bull State quality improvement program administered by the Brain Trauma Foundation between 2000 and 2009 bull Results Age initial GCS score hypotension and CT scan findings were associated with 2-week mortality In bull addition patients of all ages treated with an ICP monitor in place had lower mortality at 2 weeks (p = 002)
than those bull treated without an ICP monitor after adjusting for parameters that independently affect mortality bull Conclusions In patients with severe TBI treated for intracranial
hypertension the use of an ICP monitor is associated with significantly lower mortality when compared with patients treated without an ICP monitor Based on these findings the authors conclude that ICP-directed therapy in patients with severe TBI should be guided by ICP monitoring
bull (httpthejnsorgdoiabs10317120127JNS111816)
Neuromonitoring Methodshellip bull Functional status of the CNShellip
ndash GCS Neuro exam EEG Evoked potentials EcoG Pupillometer
Substrate delivery to the injured Brainhellip -CBF ICP CPP MABP PtiO2 Jugular Bulb oximetry
AVDO2 NIR spectroscopy Microdialysis
Combined methodshellip ldquoBrain Biomarkersrdquo--the future S100B alpha Spectrin beta amyloid
Related Articles Links
Increased incidence and impact of nonconvulsive and convulsive seizures after traumatic brain injury as detected by continuous electroencephalographic monitoring Vespa PM Nuwer MR Nenov V Ronne-Engstrom E Hovda DA Bergsneider M Kelly DF Martin NA Becker DP Department of Neurology University of California at Los Angeles School of Medicine 90024 USA Convulsive and nonconvulsive seizures occurred in 21 (22) of the 94 patients with six of them displaying status epilepticus In more than half of the patients (52) the seizures were nonconvulsive and were diagnosed on the basis of EEG studies alone All six patients with status epilepticus died compared with a mortality rate of 24 (18 of 73) in the nonseizure group (plt0001) The patients with status epilepticus had a shorter mean length of stay (914+-59 days compared with 14+-9 days [t-test plt0031) Seizures occurred despite initiation of prophylactic phenytoin on admission to the emergency room with maintenance at mean levels of 166+-28 mgdlCONCLUSIONS Seizures occur in more than one in five patients during the 1st week after moderate-to-severe brain injury and may play a role in the pathobiological conditions associated with brain injury
J Neurosurg 1999 Nov91(5)750-60
Human TBIhellipand COSBID suppression of large amplitude delta activity (eg PLEDs)
EEG
DC
1 s
1 min
Temperature ranges
All temps during monitoring
Temp during CSD
lt 350 17 10
350-380 58 23
gt380 25 68
Chi-square plt0001
N=~130 USAEU
Expl
aine
d Va
rianc
e N
agel
kerk
ersquos R
2
Univariate Analysis-outcome
0002004006008
01012014016018
Significance at plt005
350355360365370375380385390395400
1800 00
060
012
0018
00 000
600
1200
1800 00
060
012
0018
00 000
600
Synergistic pathomechanisms are commonesthellip
Do we need synergistic THERAPIES For multiple damage Mechanisms
0
100
200
300
400
500
600
700
800
0 20 40 60 80 100
Between 24 - 48 h after Injury
Brain tissue oxygen tension (PtiO2)
0
50
100
150
200
250
300
350
0 20 40 60 80 100
Brain tissue oxygen tension (PtiO2)H
Between 6 -24 h after Injury
Tissue Oxygen Tension in Humans after TBI
Brain pO2 Outcome lt20 mmHg Poor 20-30 mmHg Moderate gt30 mmHg Good
Therapy in both patient groups was aimed at maintaining an ICP less than 20 mm Hg and a CPP greater than 60 mm Hg Among patients
whose brain tissue PO2 was monitored oxygenation was maintained at levels greater
than 25 mm Hg
J Neurosurg 103805ndash811 2005
Reduced mortality rate in patients with severe traumatic brain injury treated with brain tissue oxygen monitoring
M STIEFEL MD PHD M S GRADY MD AND P D LE ROUX MD U Penn
Patients treated with ICP and brain tissue PO2 monitoring
were compared with historical controls
The mortality rate in patients treated using conventional ICP and CPP management was 44 Patients who also
underwent brain tissue PO2 monitoring had a significantly reduced mortality rate of 25 (p 005)
PtO2
TBI Clinical Trials--ongoinghellip2013 Clinical trials Gov n= 762 (n= 307 in 2010) DOD effecthellip$120M in 2007hellip
80 observationalhellip
bull Brain 0xygen ndashdirected therapyhellipBOOSTUT NIH
bull COSBIDmdashEcoGhellipfor Spreading depolarisations
bull IMPACThellip bull TRACK II-III bull Non ndashinvasive ICPrdquoECHODIA ldquo systemX2 bull PET to trace Neuroinflammation in STBINIH
CBF monitoring
bull Transcranial Doppler Monitoring bull Easy to use noninvasive
repeatable bull Measures basal cerebral bld flow
velocity flow via doppler equation bull Used to differentiate vasospasm
from hyperaemia (Lindegaard Index)
What has been achieved by monitoring the injured Brain
bull Improved understanding of dynamic pathophysiology after HUMAN TBI SAH
bull Guide design of neuroprotection trialshellip bull Improved patient outcome
Age (years)
Pro
babi
lity
of o
utco
me
()
20 40 60 80
0
20
40
60
80
100
Death rate ndashsevere TBI
bull Australia and NZ bull The Alfred
Royal Melbourne Hospital Royal Adelaide Hospital Royal Perth Hospital Sir Charles Gairdner Hospital Nepean Hospital John Hunter Hospital Royal North Shore Hospital Liverpool Hospital Wollongong Hospital Princess Alexandra Hospital Gold Coast Hospital Flinders Medical Centre Auckland Hospital Waikato Hospital Wellington Hospital
bull Saudi Arabia King Fahad National Guard Hospital
Canada bull Hamilton General hospital
Vancouver General Hospital Sunnybrook Medical Centre Royal Columbian Hospital India
bull Christian Medical College Ludhiana
bull
bull
Early bifrontal decompression Vs medical management No benefit from surgeryhellipmore disabled and vegetative outcomes
3 editorials on the DECRA tria
bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

The NIH-NINDS Trial of ICP Monitoring in BoliviaLABIChellip
4 hospitals PRCT~350 pts
bull ldquoWe are still likely to continue to doubt clinical
bull signs which indeed do not reflect global pressure inside the cranium but stupor coma posturing and dilatation of the pupils indicate compression of the midbrain and according to this study they are very suitable observations to
bull use in directing treatmentrdquohellip
ldquoIn the future there may be other means of detecting
early compression of the brain stem Until then
clinical methods are finerdquo
Why the Chesnut Bolivia ICP monitoring trial is not ldquogeneralisablerdquo to rest of the
worldhellip bull Only about 50 of severe TBI cases got into ICUhellipbed limitationshellip bull No prehospital care no rehab poor
ldquo subacute ldquophase care40 mortalityhellip bull ~47 decompressive craniotomy used in
both groups ~23 barbiturates 1 ventricular drainage
bull mean~ 20 hours with ICPgt20mmHg
bull Increased mortality in patients with severe traumatic brain injury treated without intracranial pressure monitoring
Arash Farahvar MD PhD1 Linda M Gerber PhD2 Ya-Lin Chiu MS2 bull Nancy Carney PhD3 Roger Haumlrtl MD4 and Jam shid Ghaja r MD PhD45 bull 1Department of Neurosurgery University of Rochester Medical Center Rochester Departments of 2Public bull Health and 4Neurological Surgery Weill Cornell Medical College and 5Brain Trauma Foundation bull New York New York and 3Department of Medical Informatics and Clinical Epidemiology Oregon bull Health amp Science University Portland Oregon bull Object Evidence-based guidelines recommend intracranial pressure (ICP) monitoring for patients with severe bull traumatic brain injury (TBI) but there is limited evidence that monitoring and treating intracranial hypertension
reduces bull mortality This study uses a large prospectively collected database to examine the effect on 2-week mortality bull of ICP reduction therapies administered to patients with severe TBI treated either with or without an ICP
monitor bull Methods From a population of 2134 patients with severe TBI (Glasgow Coma Scale [GCS] Score lt 9) 1446 bull patients were treated with ICP-lowering therapies Of those 1202 had an ICP monitor inserted and 244 were
treated bull without monitoring Patients were admitted to one of 20 Level I and two Level II trauma centers part of a New
York bull State quality improvement program administered by the Brain Trauma Foundation between 2000 and 2009 bull Results Age initial GCS score hypotension and CT scan findings were associated with 2-week mortality In bull addition patients of all ages treated with an ICP monitor in place had lower mortality at 2 weeks (p = 002)
than those bull treated without an ICP monitor after adjusting for parameters that independently affect mortality bull Conclusions In patients with severe TBI treated for intracranial
hypertension the use of an ICP monitor is associated with significantly lower mortality when compared with patients treated without an ICP monitor Based on these findings the authors conclude that ICP-directed therapy in patients with severe TBI should be guided by ICP monitoring
bull (httpthejnsorgdoiabs10317120127JNS111816)
Neuromonitoring Methodshellip bull Functional status of the CNShellip
ndash GCS Neuro exam EEG Evoked potentials EcoG Pupillometer
Substrate delivery to the injured Brainhellip -CBF ICP CPP MABP PtiO2 Jugular Bulb oximetry
AVDO2 NIR spectroscopy Microdialysis
Combined methodshellip ldquoBrain Biomarkersrdquo--the future S100B alpha Spectrin beta amyloid
Related Articles Links
Increased incidence and impact of nonconvulsive and convulsive seizures after traumatic brain injury as detected by continuous electroencephalographic monitoring Vespa PM Nuwer MR Nenov V Ronne-Engstrom E Hovda DA Bergsneider M Kelly DF Martin NA Becker DP Department of Neurology University of California at Los Angeles School of Medicine 90024 USA Convulsive and nonconvulsive seizures occurred in 21 (22) of the 94 patients with six of them displaying status epilepticus In more than half of the patients (52) the seizures were nonconvulsive and were diagnosed on the basis of EEG studies alone All six patients with status epilepticus died compared with a mortality rate of 24 (18 of 73) in the nonseizure group (plt0001) The patients with status epilepticus had a shorter mean length of stay (914+-59 days compared with 14+-9 days [t-test plt0031) Seizures occurred despite initiation of prophylactic phenytoin on admission to the emergency room with maintenance at mean levels of 166+-28 mgdlCONCLUSIONS Seizures occur in more than one in five patients during the 1st week after moderate-to-severe brain injury and may play a role in the pathobiological conditions associated with brain injury
J Neurosurg 1999 Nov91(5)750-60
Human TBIhellipand COSBID suppression of large amplitude delta activity (eg PLEDs)
EEG
DC
1 s
1 min
Temperature ranges
All temps during monitoring
Temp during CSD
lt 350 17 10
350-380 58 23
gt380 25 68
Chi-square plt0001
N=~130 USAEU
Expl
aine
d Va
rianc
e N
agel
kerk
ersquos R
2
Univariate Analysis-outcome
0002004006008
01012014016018
Significance at plt005
350355360365370375380385390395400
1800 00
060
012
0018
00 000
600
1200
1800 00
060
012
0018
00 000
600
Synergistic pathomechanisms are commonesthellip
Do we need synergistic THERAPIES For multiple damage Mechanisms
0
100
200
300
400
500
600
700
800
0 20 40 60 80 100
Between 24 - 48 h after Injury
Brain tissue oxygen tension (PtiO2)
0
50
100
150
200
250
300
350
0 20 40 60 80 100
Brain tissue oxygen tension (PtiO2)H
Between 6 -24 h after Injury
Tissue Oxygen Tension in Humans after TBI
Brain pO2 Outcome lt20 mmHg Poor 20-30 mmHg Moderate gt30 mmHg Good
Therapy in both patient groups was aimed at maintaining an ICP less than 20 mm Hg and a CPP greater than 60 mm Hg Among patients
whose brain tissue PO2 was monitored oxygenation was maintained at levels greater
than 25 mm Hg
J Neurosurg 103805ndash811 2005
Reduced mortality rate in patients with severe traumatic brain injury treated with brain tissue oxygen monitoring
M STIEFEL MD PHD M S GRADY MD AND P D LE ROUX MD U Penn
Patients treated with ICP and brain tissue PO2 monitoring
were compared with historical controls
The mortality rate in patients treated using conventional ICP and CPP management was 44 Patients who also
underwent brain tissue PO2 monitoring had a significantly reduced mortality rate of 25 (p 005)
PtO2
TBI Clinical Trials--ongoinghellip2013 Clinical trials Gov n= 762 (n= 307 in 2010) DOD effecthellip$120M in 2007hellip
80 observationalhellip
bull Brain 0xygen ndashdirected therapyhellipBOOSTUT NIH
bull COSBIDmdashEcoGhellipfor Spreading depolarisations
bull IMPACThellip bull TRACK II-III bull Non ndashinvasive ICPrdquoECHODIA ldquo systemX2 bull PET to trace Neuroinflammation in STBINIH
CBF monitoring
bull Transcranial Doppler Monitoring bull Easy to use noninvasive
repeatable bull Measures basal cerebral bld flow
velocity flow via doppler equation bull Used to differentiate vasospasm
from hyperaemia (Lindegaard Index)
What has been achieved by monitoring the injured Brain
bull Improved understanding of dynamic pathophysiology after HUMAN TBI SAH
bull Guide design of neuroprotection trialshellip bull Improved patient outcome
Age (years)
Pro
babi
lity
of o
utco
me
()
20 40 60 80
0
20
40
60
80
100
Death rate ndashsevere TBI
bull Australia and NZ bull The Alfred
Royal Melbourne Hospital Royal Adelaide Hospital Royal Perth Hospital Sir Charles Gairdner Hospital Nepean Hospital John Hunter Hospital Royal North Shore Hospital Liverpool Hospital Wollongong Hospital Princess Alexandra Hospital Gold Coast Hospital Flinders Medical Centre Auckland Hospital Waikato Hospital Wellington Hospital
bull Saudi Arabia King Fahad National Guard Hospital
Canada bull Hamilton General hospital
Vancouver General Hospital Sunnybrook Medical Centre Royal Columbian Hospital India
bull Christian Medical College Ludhiana
bull
bull
Early bifrontal decompression Vs medical management No benefit from surgeryhellipmore disabled and vegetative outcomes
3 editorials on the DECRA tria
bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

bull ldquoWe are still likely to continue to doubt clinical
bull signs which indeed do not reflect global pressure inside the cranium but stupor coma posturing and dilatation of the pupils indicate compression of the midbrain and according to this study they are very suitable observations to
bull use in directing treatmentrdquohellip
ldquoIn the future there may be other means of detecting
early compression of the brain stem Until then
clinical methods are finerdquo
Why the Chesnut Bolivia ICP monitoring trial is not ldquogeneralisablerdquo to rest of the
worldhellip bull Only about 50 of severe TBI cases got into ICUhellipbed limitationshellip bull No prehospital care no rehab poor
ldquo subacute ldquophase care40 mortalityhellip bull ~47 decompressive craniotomy used in
both groups ~23 barbiturates 1 ventricular drainage
bull mean~ 20 hours with ICPgt20mmHg
bull Increased mortality in patients with severe traumatic brain injury treated without intracranial pressure monitoring
Arash Farahvar MD PhD1 Linda M Gerber PhD2 Ya-Lin Chiu MS2 bull Nancy Carney PhD3 Roger Haumlrtl MD4 and Jam shid Ghaja r MD PhD45 bull 1Department of Neurosurgery University of Rochester Medical Center Rochester Departments of 2Public bull Health and 4Neurological Surgery Weill Cornell Medical College and 5Brain Trauma Foundation bull New York New York and 3Department of Medical Informatics and Clinical Epidemiology Oregon bull Health amp Science University Portland Oregon bull Object Evidence-based guidelines recommend intracranial pressure (ICP) monitoring for patients with severe bull traumatic brain injury (TBI) but there is limited evidence that monitoring and treating intracranial hypertension
reduces bull mortality This study uses a large prospectively collected database to examine the effect on 2-week mortality bull of ICP reduction therapies administered to patients with severe TBI treated either with or without an ICP
monitor bull Methods From a population of 2134 patients with severe TBI (Glasgow Coma Scale [GCS] Score lt 9) 1446 bull patients were treated with ICP-lowering therapies Of those 1202 had an ICP monitor inserted and 244 were
treated bull without monitoring Patients were admitted to one of 20 Level I and two Level II trauma centers part of a New
York bull State quality improvement program administered by the Brain Trauma Foundation between 2000 and 2009 bull Results Age initial GCS score hypotension and CT scan findings were associated with 2-week mortality In bull addition patients of all ages treated with an ICP monitor in place had lower mortality at 2 weeks (p = 002)
than those bull treated without an ICP monitor after adjusting for parameters that independently affect mortality bull Conclusions In patients with severe TBI treated for intracranial
hypertension the use of an ICP monitor is associated with significantly lower mortality when compared with patients treated without an ICP monitor Based on these findings the authors conclude that ICP-directed therapy in patients with severe TBI should be guided by ICP monitoring
bull (httpthejnsorgdoiabs10317120127JNS111816)
Neuromonitoring Methodshellip bull Functional status of the CNShellip
ndash GCS Neuro exam EEG Evoked potentials EcoG Pupillometer
Substrate delivery to the injured Brainhellip -CBF ICP CPP MABP PtiO2 Jugular Bulb oximetry
AVDO2 NIR spectroscopy Microdialysis
Combined methodshellip ldquoBrain Biomarkersrdquo--the future S100B alpha Spectrin beta amyloid
Related Articles Links
Increased incidence and impact of nonconvulsive and convulsive seizures after traumatic brain injury as detected by continuous electroencephalographic monitoring Vespa PM Nuwer MR Nenov V Ronne-Engstrom E Hovda DA Bergsneider M Kelly DF Martin NA Becker DP Department of Neurology University of California at Los Angeles School of Medicine 90024 USA Convulsive and nonconvulsive seizures occurred in 21 (22) of the 94 patients with six of them displaying status epilepticus In more than half of the patients (52) the seizures were nonconvulsive and were diagnosed on the basis of EEG studies alone All six patients with status epilepticus died compared with a mortality rate of 24 (18 of 73) in the nonseizure group (plt0001) The patients with status epilepticus had a shorter mean length of stay (914+-59 days compared with 14+-9 days [t-test plt0031) Seizures occurred despite initiation of prophylactic phenytoin on admission to the emergency room with maintenance at mean levels of 166+-28 mgdlCONCLUSIONS Seizures occur in more than one in five patients during the 1st week after moderate-to-severe brain injury and may play a role in the pathobiological conditions associated with brain injury
J Neurosurg 1999 Nov91(5)750-60
Human TBIhellipand COSBID suppression of large amplitude delta activity (eg PLEDs)
EEG
DC
1 s
1 min
Temperature ranges
All temps during monitoring
Temp during CSD
lt 350 17 10
350-380 58 23
gt380 25 68
Chi-square plt0001
N=~130 USAEU
Expl
aine
d Va
rianc
e N
agel
kerk
ersquos R
2
Univariate Analysis-outcome
0002004006008
01012014016018
Significance at plt005
350355360365370375380385390395400
1800 00
060
012
0018
00 000
600
1200
1800 00
060
012
0018
00 000
600
Synergistic pathomechanisms are commonesthellip
Do we need synergistic THERAPIES For multiple damage Mechanisms
0
100
200
300
400
500
600
700
800
0 20 40 60 80 100
Between 24 - 48 h after Injury
Brain tissue oxygen tension (PtiO2)
0
50
100
150
200
250
300
350
0 20 40 60 80 100
Brain tissue oxygen tension (PtiO2)H
Between 6 -24 h after Injury
Tissue Oxygen Tension in Humans after TBI
Brain pO2 Outcome lt20 mmHg Poor 20-30 mmHg Moderate gt30 mmHg Good
Therapy in both patient groups was aimed at maintaining an ICP less than 20 mm Hg and a CPP greater than 60 mm Hg Among patients
whose brain tissue PO2 was monitored oxygenation was maintained at levels greater
than 25 mm Hg
J Neurosurg 103805ndash811 2005
Reduced mortality rate in patients with severe traumatic brain injury treated with brain tissue oxygen monitoring
M STIEFEL MD PHD M S GRADY MD AND P D LE ROUX MD U Penn
Patients treated with ICP and brain tissue PO2 monitoring
were compared with historical controls
The mortality rate in patients treated using conventional ICP and CPP management was 44 Patients who also
underwent brain tissue PO2 monitoring had a significantly reduced mortality rate of 25 (p 005)
PtO2
TBI Clinical Trials--ongoinghellip2013 Clinical trials Gov n= 762 (n= 307 in 2010) DOD effecthellip$120M in 2007hellip
80 observationalhellip
bull Brain 0xygen ndashdirected therapyhellipBOOSTUT NIH
bull COSBIDmdashEcoGhellipfor Spreading depolarisations
bull IMPACThellip bull TRACK II-III bull Non ndashinvasive ICPrdquoECHODIA ldquo systemX2 bull PET to trace Neuroinflammation in STBINIH
CBF monitoring
bull Transcranial Doppler Monitoring bull Easy to use noninvasive
repeatable bull Measures basal cerebral bld flow
velocity flow via doppler equation bull Used to differentiate vasospasm
from hyperaemia (Lindegaard Index)
What has been achieved by monitoring the injured Brain
bull Improved understanding of dynamic pathophysiology after HUMAN TBI SAH
bull Guide design of neuroprotection trialshellip bull Improved patient outcome
Age (years)
Pro
babi
lity
of o
utco
me
()
20 40 60 80
0
20
40
60
80
100
Death rate ndashsevere TBI
bull Australia and NZ bull The Alfred
Royal Melbourne Hospital Royal Adelaide Hospital Royal Perth Hospital Sir Charles Gairdner Hospital Nepean Hospital John Hunter Hospital Royal North Shore Hospital Liverpool Hospital Wollongong Hospital Princess Alexandra Hospital Gold Coast Hospital Flinders Medical Centre Auckland Hospital Waikato Hospital Wellington Hospital
bull Saudi Arabia King Fahad National Guard Hospital
Canada bull Hamilton General hospital
Vancouver General Hospital Sunnybrook Medical Centre Royal Columbian Hospital India
bull Christian Medical College Ludhiana
bull
bull
Early bifrontal decompression Vs medical management No benefit from surgeryhellipmore disabled and vegetative outcomes
3 editorials on the DECRA tria
bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

Why the Chesnut Bolivia ICP monitoring trial is not ldquogeneralisablerdquo to rest of the
worldhellip bull Only about 50 of severe TBI cases got into ICUhellipbed limitationshellip bull No prehospital care no rehab poor
ldquo subacute ldquophase care40 mortalityhellip bull ~47 decompressive craniotomy used in
both groups ~23 barbiturates 1 ventricular drainage
bull mean~ 20 hours with ICPgt20mmHg
bull Increased mortality in patients with severe traumatic brain injury treated without intracranial pressure monitoring
Arash Farahvar MD PhD1 Linda M Gerber PhD2 Ya-Lin Chiu MS2 bull Nancy Carney PhD3 Roger Haumlrtl MD4 and Jam shid Ghaja r MD PhD45 bull 1Department of Neurosurgery University of Rochester Medical Center Rochester Departments of 2Public bull Health and 4Neurological Surgery Weill Cornell Medical College and 5Brain Trauma Foundation bull New York New York and 3Department of Medical Informatics and Clinical Epidemiology Oregon bull Health amp Science University Portland Oregon bull Object Evidence-based guidelines recommend intracranial pressure (ICP) monitoring for patients with severe bull traumatic brain injury (TBI) but there is limited evidence that monitoring and treating intracranial hypertension
reduces bull mortality This study uses a large prospectively collected database to examine the effect on 2-week mortality bull of ICP reduction therapies administered to patients with severe TBI treated either with or without an ICP
monitor bull Methods From a population of 2134 patients with severe TBI (Glasgow Coma Scale [GCS] Score lt 9) 1446 bull patients were treated with ICP-lowering therapies Of those 1202 had an ICP monitor inserted and 244 were
treated bull without monitoring Patients were admitted to one of 20 Level I and two Level II trauma centers part of a New
York bull State quality improvement program administered by the Brain Trauma Foundation between 2000 and 2009 bull Results Age initial GCS score hypotension and CT scan findings were associated with 2-week mortality In bull addition patients of all ages treated with an ICP monitor in place had lower mortality at 2 weeks (p = 002)
than those bull treated without an ICP monitor after adjusting for parameters that independently affect mortality bull Conclusions In patients with severe TBI treated for intracranial
hypertension the use of an ICP monitor is associated with significantly lower mortality when compared with patients treated without an ICP monitor Based on these findings the authors conclude that ICP-directed therapy in patients with severe TBI should be guided by ICP monitoring
bull (httpthejnsorgdoiabs10317120127JNS111816)
Neuromonitoring Methodshellip bull Functional status of the CNShellip
ndash GCS Neuro exam EEG Evoked potentials EcoG Pupillometer
Substrate delivery to the injured Brainhellip -CBF ICP CPP MABP PtiO2 Jugular Bulb oximetry
AVDO2 NIR spectroscopy Microdialysis
Combined methodshellip ldquoBrain Biomarkersrdquo--the future S100B alpha Spectrin beta amyloid
Related Articles Links
Increased incidence and impact of nonconvulsive and convulsive seizures after traumatic brain injury as detected by continuous electroencephalographic monitoring Vespa PM Nuwer MR Nenov V Ronne-Engstrom E Hovda DA Bergsneider M Kelly DF Martin NA Becker DP Department of Neurology University of California at Los Angeles School of Medicine 90024 USA Convulsive and nonconvulsive seizures occurred in 21 (22) of the 94 patients with six of them displaying status epilepticus In more than half of the patients (52) the seizures were nonconvulsive and were diagnosed on the basis of EEG studies alone All six patients with status epilepticus died compared with a mortality rate of 24 (18 of 73) in the nonseizure group (plt0001) The patients with status epilepticus had a shorter mean length of stay (914+-59 days compared with 14+-9 days [t-test plt0031) Seizures occurred despite initiation of prophylactic phenytoin on admission to the emergency room with maintenance at mean levels of 166+-28 mgdlCONCLUSIONS Seizures occur in more than one in five patients during the 1st week after moderate-to-severe brain injury and may play a role in the pathobiological conditions associated with brain injury
J Neurosurg 1999 Nov91(5)750-60
Human TBIhellipand COSBID suppression of large amplitude delta activity (eg PLEDs)
EEG
DC
1 s
1 min
Temperature ranges
All temps during monitoring
Temp during CSD
lt 350 17 10
350-380 58 23
gt380 25 68
Chi-square plt0001
N=~130 USAEU
Expl
aine
d Va
rianc
e N
agel
kerk
ersquos R
2
Univariate Analysis-outcome
0002004006008
01012014016018
Significance at plt005
350355360365370375380385390395400
1800 00
060
012
0018
00 000
600
1200
1800 00
060
012
0018
00 000
600
Synergistic pathomechanisms are commonesthellip
Do we need synergistic THERAPIES For multiple damage Mechanisms
0
100
200
300
400
500
600
700
800
0 20 40 60 80 100
Between 24 - 48 h after Injury
Brain tissue oxygen tension (PtiO2)
0
50
100
150
200
250
300
350
0 20 40 60 80 100
Brain tissue oxygen tension (PtiO2)H
Between 6 -24 h after Injury
Tissue Oxygen Tension in Humans after TBI
Brain pO2 Outcome lt20 mmHg Poor 20-30 mmHg Moderate gt30 mmHg Good
Therapy in both patient groups was aimed at maintaining an ICP less than 20 mm Hg and a CPP greater than 60 mm Hg Among patients
whose brain tissue PO2 was monitored oxygenation was maintained at levels greater
than 25 mm Hg
J Neurosurg 103805ndash811 2005
Reduced mortality rate in patients with severe traumatic brain injury treated with brain tissue oxygen monitoring
M STIEFEL MD PHD M S GRADY MD AND P D LE ROUX MD U Penn
Patients treated with ICP and brain tissue PO2 monitoring
were compared with historical controls
The mortality rate in patients treated using conventional ICP and CPP management was 44 Patients who also
underwent brain tissue PO2 monitoring had a significantly reduced mortality rate of 25 (p 005)
PtO2
TBI Clinical Trials--ongoinghellip2013 Clinical trials Gov n= 762 (n= 307 in 2010) DOD effecthellip$120M in 2007hellip
80 observationalhellip
bull Brain 0xygen ndashdirected therapyhellipBOOSTUT NIH
bull COSBIDmdashEcoGhellipfor Spreading depolarisations
bull IMPACThellip bull TRACK II-III bull Non ndashinvasive ICPrdquoECHODIA ldquo systemX2 bull PET to trace Neuroinflammation in STBINIH
CBF monitoring
bull Transcranial Doppler Monitoring bull Easy to use noninvasive
repeatable bull Measures basal cerebral bld flow
velocity flow via doppler equation bull Used to differentiate vasospasm
from hyperaemia (Lindegaard Index)
What has been achieved by monitoring the injured Brain
bull Improved understanding of dynamic pathophysiology after HUMAN TBI SAH
bull Guide design of neuroprotection trialshellip bull Improved patient outcome
Age (years)
Pro
babi
lity
of o
utco
me
()
20 40 60 80
0
20
40
60
80
100
Death rate ndashsevere TBI
bull Australia and NZ bull The Alfred
Royal Melbourne Hospital Royal Adelaide Hospital Royal Perth Hospital Sir Charles Gairdner Hospital Nepean Hospital John Hunter Hospital Royal North Shore Hospital Liverpool Hospital Wollongong Hospital Princess Alexandra Hospital Gold Coast Hospital Flinders Medical Centre Auckland Hospital Waikato Hospital Wellington Hospital
bull Saudi Arabia King Fahad National Guard Hospital
Canada bull Hamilton General hospital
Vancouver General Hospital Sunnybrook Medical Centre Royal Columbian Hospital India
bull Christian Medical College Ludhiana
bull
bull
Early bifrontal decompression Vs medical management No benefit from surgeryhellipmore disabled and vegetative outcomes
3 editorials on the DECRA tria
bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

bull Increased mortality in patients with severe traumatic brain injury treated without intracranial pressure monitoring
Arash Farahvar MD PhD1 Linda M Gerber PhD2 Ya-Lin Chiu MS2 bull Nancy Carney PhD3 Roger Haumlrtl MD4 and Jam shid Ghaja r MD PhD45 bull 1Department of Neurosurgery University of Rochester Medical Center Rochester Departments of 2Public bull Health and 4Neurological Surgery Weill Cornell Medical College and 5Brain Trauma Foundation bull New York New York and 3Department of Medical Informatics and Clinical Epidemiology Oregon bull Health amp Science University Portland Oregon bull Object Evidence-based guidelines recommend intracranial pressure (ICP) monitoring for patients with severe bull traumatic brain injury (TBI) but there is limited evidence that monitoring and treating intracranial hypertension
reduces bull mortality This study uses a large prospectively collected database to examine the effect on 2-week mortality bull of ICP reduction therapies administered to patients with severe TBI treated either with or without an ICP
monitor bull Methods From a population of 2134 patients with severe TBI (Glasgow Coma Scale [GCS] Score lt 9) 1446 bull patients were treated with ICP-lowering therapies Of those 1202 had an ICP monitor inserted and 244 were
treated bull without monitoring Patients were admitted to one of 20 Level I and two Level II trauma centers part of a New
York bull State quality improvement program administered by the Brain Trauma Foundation between 2000 and 2009 bull Results Age initial GCS score hypotension and CT scan findings were associated with 2-week mortality In bull addition patients of all ages treated with an ICP monitor in place had lower mortality at 2 weeks (p = 002)
than those bull treated without an ICP monitor after adjusting for parameters that independently affect mortality bull Conclusions In patients with severe TBI treated for intracranial
hypertension the use of an ICP monitor is associated with significantly lower mortality when compared with patients treated without an ICP monitor Based on these findings the authors conclude that ICP-directed therapy in patients with severe TBI should be guided by ICP monitoring
bull (httpthejnsorgdoiabs10317120127JNS111816)
Neuromonitoring Methodshellip bull Functional status of the CNShellip
ndash GCS Neuro exam EEG Evoked potentials EcoG Pupillometer
Substrate delivery to the injured Brainhellip -CBF ICP CPP MABP PtiO2 Jugular Bulb oximetry
AVDO2 NIR spectroscopy Microdialysis
Combined methodshellip ldquoBrain Biomarkersrdquo--the future S100B alpha Spectrin beta amyloid
Related Articles Links
Increased incidence and impact of nonconvulsive and convulsive seizures after traumatic brain injury as detected by continuous electroencephalographic monitoring Vespa PM Nuwer MR Nenov V Ronne-Engstrom E Hovda DA Bergsneider M Kelly DF Martin NA Becker DP Department of Neurology University of California at Los Angeles School of Medicine 90024 USA Convulsive and nonconvulsive seizures occurred in 21 (22) of the 94 patients with six of them displaying status epilepticus In more than half of the patients (52) the seizures were nonconvulsive and were diagnosed on the basis of EEG studies alone All six patients with status epilepticus died compared with a mortality rate of 24 (18 of 73) in the nonseizure group (plt0001) The patients with status epilepticus had a shorter mean length of stay (914+-59 days compared with 14+-9 days [t-test plt0031) Seizures occurred despite initiation of prophylactic phenytoin on admission to the emergency room with maintenance at mean levels of 166+-28 mgdlCONCLUSIONS Seizures occur in more than one in five patients during the 1st week after moderate-to-severe brain injury and may play a role in the pathobiological conditions associated with brain injury
J Neurosurg 1999 Nov91(5)750-60
Human TBIhellipand COSBID suppression of large amplitude delta activity (eg PLEDs)
EEG
DC
1 s
1 min
Temperature ranges
All temps during monitoring
Temp during CSD
lt 350 17 10
350-380 58 23
gt380 25 68
Chi-square plt0001
N=~130 USAEU
Expl
aine
d Va
rianc
e N
agel
kerk
ersquos R
2
Univariate Analysis-outcome
0002004006008
01012014016018
Significance at plt005
350355360365370375380385390395400
1800 00
060
012
0018
00 000
600
1200
1800 00
060
012
0018
00 000
600
Synergistic pathomechanisms are commonesthellip
Do we need synergistic THERAPIES For multiple damage Mechanisms
0
100
200
300
400
500
600
700
800
0 20 40 60 80 100
Between 24 - 48 h after Injury
Brain tissue oxygen tension (PtiO2)
0
50
100
150
200
250
300
350
0 20 40 60 80 100
Brain tissue oxygen tension (PtiO2)H
Between 6 -24 h after Injury
Tissue Oxygen Tension in Humans after TBI
Brain pO2 Outcome lt20 mmHg Poor 20-30 mmHg Moderate gt30 mmHg Good
Therapy in both patient groups was aimed at maintaining an ICP less than 20 mm Hg and a CPP greater than 60 mm Hg Among patients
whose brain tissue PO2 was monitored oxygenation was maintained at levels greater
than 25 mm Hg
J Neurosurg 103805ndash811 2005
Reduced mortality rate in patients with severe traumatic brain injury treated with brain tissue oxygen monitoring
M STIEFEL MD PHD M S GRADY MD AND P D LE ROUX MD U Penn
Patients treated with ICP and brain tissue PO2 monitoring
were compared with historical controls
The mortality rate in patients treated using conventional ICP and CPP management was 44 Patients who also
underwent brain tissue PO2 monitoring had a significantly reduced mortality rate of 25 (p 005)
PtO2
TBI Clinical Trials--ongoinghellip2013 Clinical trials Gov n= 762 (n= 307 in 2010) DOD effecthellip$120M in 2007hellip
80 observationalhellip
bull Brain 0xygen ndashdirected therapyhellipBOOSTUT NIH
bull COSBIDmdashEcoGhellipfor Spreading depolarisations
bull IMPACThellip bull TRACK II-III bull Non ndashinvasive ICPrdquoECHODIA ldquo systemX2 bull PET to trace Neuroinflammation in STBINIH
CBF monitoring
bull Transcranial Doppler Monitoring bull Easy to use noninvasive
repeatable bull Measures basal cerebral bld flow
velocity flow via doppler equation bull Used to differentiate vasospasm
from hyperaemia (Lindegaard Index)
What has been achieved by monitoring the injured Brain
bull Improved understanding of dynamic pathophysiology after HUMAN TBI SAH
bull Guide design of neuroprotection trialshellip bull Improved patient outcome
Age (years)
Pro
babi
lity
of o
utco
me
()
20 40 60 80
0
20
40
60
80
100
Death rate ndashsevere TBI
bull Australia and NZ bull The Alfred
Royal Melbourne Hospital Royal Adelaide Hospital Royal Perth Hospital Sir Charles Gairdner Hospital Nepean Hospital John Hunter Hospital Royal North Shore Hospital Liverpool Hospital Wollongong Hospital Princess Alexandra Hospital Gold Coast Hospital Flinders Medical Centre Auckland Hospital Waikato Hospital Wellington Hospital
bull Saudi Arabia King Fahad National Guard Hospital
Canada bull Hamilton General hospital
Vancouver General Hospital Sunnybrook Medical Centre Royal Columbian Hospital India
bull Christian Medical College Ludhiana
bull
bull
Early bifrontal decompression Vs medical management No benefit from surgeryhellipmore disabled and vegetative outcomes
3 editorials on the DECRA tria
bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

Neuromonitoring Methodshellip bull Functional status of the CNShellip
ndash GCS Neuro exam EEG Evoked potentials EcoG Pupillometer
Substrate delivery to the injured Brainhellip -CBF ICP CPP MABP PtiO2 Jugular Bulb oximetry
AVDO2 NIR spectroscopy Microdialysis
Combined methodshellip ldquoBrain Biomarkersrdquo--the future S100B alpha Spectrin beta amyloid
Related Articles Links
Increased incidence and impact of nonconvulsive and convulsive seizures after traumatic brain injury as detected by continuous electroencephalographic monitoring Vespa PM Nuwer MR Nenov V Ronne-Engstrom E Hovda DA Bergsneider M Kelly DF Martin NA Becker DP Department of Neurology University of California at Los Angeles School of Medicine 90024 USA Convulsive and nonconvulsive seizures occurred in 21 (22) of the 94 patients with six of them displaying status epilepticus In more than half of the patients (52) the seizures were nonconvulsive and were diagnosed on the basis of EEG studies alone All six patients with status epilepticus died compared with a mortality rate of 24 (18 of 73) in the nonseizure group (plt0001) The patients with status epilepticus had a shorter mean length of stay (914+-59 days compared with 14+-9 days [t-test plt0031) Seizures occurred despite initiation of prophylactic phenytoin on admission to the emergency room with maintenance at mean levels of 166+-28 mgdlCONCLUSIONS Seizures occur in more than one in five patients during the 1st week after moderate-to-severe brain injury and may play a role in the pathobiological conditions associated with brain injury
J Neurosurg 1999 Nov91(5)750-60
Human TBIhellipand COSBID suppression of large amplitude delta activity (eg PLEDs)
EEG
DC
1 s
1 min
Temperature ranges
All temps during monitoring
Temp during CSD
lt 350 17 10
350-380 58 23
gt380 25 68
Chi-square plt0001
N=~130 USAEU
Expl
aine
d Va
rianc
e N
agel
kerk
ersquos R
2
Univariate Analysis-outcome
0002004006008
01012014016018
Significance at plt005
350355360365370375380385390395400
1800 00
060
012
0018
00 000
600
1200
1800 00
060
012
0018
00 000
600
Synergistic pathomechanisms are commonesthellip
Do we need synergistic THERAPIES For multiple damage Mechanisms
0
100
200
300
400
500
600
700
800
0 20 40 60 80 100
Between 24 - 48 h after Injury
Brain tissue oxygen tension (PtiO2)
0
50
100
150
200
250
300
350
0 20 40 60 80 100
Brain tissue oxygen tension (PtiO2)H
Between 6 -24 h after Injury
Tissue Oxygen Tension in Humans after TBI
Brain pO2 Outcome lt20 mmHg Poor 20-30 mmHg Moderate gt30 mmHg Good
Therapy in both patient groups was aimed at maintaining an ICP less than 20 mm Hg and a CPP greater than 60 mm Hg Among patients
whose brain tissue PO2 was monitored oxygenation was maintained at levels greater
than 25 mm Hg
J Neurosurg 103805ndash811 2005
Reduced mortality rate in patients with severe traumatic brain injury treated with brain tissue oxygen monitoring
M STIEFEL MD PHD M S GRADY MD AND P D LE ROUX MD U Penn
Patients treated with ICP and brain tissue PO2 monitoring
were compared with historical controls
The mortality rate in patients treated using conventional ICP and CPP management was 44 Patients who also
underwent brain tissue PO2 monitoring had a significantly reduced mortality rate of 25 (p 005)
PtO2
TBI Clinical Trials--ongoinghellip2013 Clinical trials Gov n= 762 (n= 307 in 2010) DOD effecthellip$120M in 2007hellip
80 observationalhellip
bull Brain 0xygen ndashdirected therapyhellipBOOSTUT NIH
bull COSBIDmdashEcoGhellipfor Spreading depolarisations
bull IMPACThellip bull TRACK II-III bull Non ndashinvasive ICPrdquoECHODIA ldquo systemX2 bull PET to trace Neuroinflammation in STBINIH
CBF monitoring
bull Transcranial Doppler Monitoring bull Easy to use noninvasive
repeatable bull Measures basal cerebral bld flow
velocity flow via doppler equation bull Used to differentiate vasospasm
from hyperaemia (Lindegaard Index)
What has been achieved by monitoring the injured Brain
bull Improved understanding of dynamic pathophysiology after HUMAN TBI SAH
bull Guide design of neuroprotection trialshellip bull Improved patient outcome
Age (years)
Pro
babi
lity
of o
utco
me
()
20 40 60 80
0
20
40
60
80
100
Death rate ndashsevere TBI
bull Australia and NZ bull The Alfred
Royal Melbourne Hospital Royal Adelaide Hospital Royal Perth Hospital Sir Charles Gairdner Hospital Nepean Hospital John Hunter Hospital Royal North Shore Hospital Liverpool Hospital Wollongong Hospital Princess Alexandra Hospital Gold Coast Hospital Flinders Medical Centre Auckland Hospital Waikato Hospital Wellington Hospital
bull Saudi Arabia King Fahad National Guard Hospital
Canada bull Hamilton General hospital
Vancouver General Hospital Sunnybrook Medical Centre Royal Columbian Hospital India
bull Christian Medical College Ludhiana
bull
bull
Early bifrontal decompression Vs medical management No benefit from surgeryhellipmore disabled and vegetative outcomes
3 editorials on the DECRA tria
bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

Related Articles Links
Increased incidence and impact of nonconvulsive and convulsive seizures after traumatic brain injury as detected by continuous electroencephalographic monitoring Vespa PM Nuwer MR Nenov V Ronne-Engstrom E Hovda DA Bergsneider M Kelly DF Martin NA Becker DP Department of Neurology University of California at Los Angeles School of Medicine 90024 USA Convulsive and nonconvulsive seizures occurred in 21 (22) of the 94 patients with six of them displaying status epilepticus In more than half of the patients (52) the seizures were nonconvulsive and were diagnosed on the basis of EEG studies alone All six patients with status epilepticus died compared with a mortality rate of 24 (18 of 73) in the nonseizure group (plt0001) The patients with status epilepticus had a shorter mean length of stay (914+-59 days compared with 14+-9 days [t-test plt0031) Seizures occurred despite initiation of prophylactic phenytoin on admission to the emergency room with maintenance at mean levels of 166+-28 mgdlCONCLUSIONS Seizures occur in more than one in five patients during the 1st week after moderate-to-severe brain injury and may play a role in the pathobiological conditions associated with brain injury
J Neurosurg 1999 Nov91(5)750-60
Human TBIhellipand COSBID suppression of large amplitude delta activity (eg PLEDs)
EEG
DC
1 s
1 min
Temperature ranges
All temps during monitoring
Temp during CSD
lt 350 17 10
350-380 58 23
gt380 25 68
Chi-square plt0001
N=~130 USAEU
Expl
aine
d Va
rianc
e N
agel
kerk
ersquos R
2
Univariate Analysis-outcome
0002004006008
01012014016018
Significance at plt005
350355360365370375380385390395400
1800 00
060
012
0018
00 000
600
1200
1800 00
060
012
0018
00 000
600
Synergistic pathomechanisms are commonesthellip
Do we need synergistic THERAPIES For multiple damage Mechanisms
0
100
200
300
400
500
600
700
800
0 20 40 60 80 100
Between 24 - 48 h after Injury
Brain tissue oxygen tension (PtiO2)
0
50
100
150
200
250
300
350
0 20 40 60 80 100
Brain tissue oxygen tension (PtiO2)H
Between 6 -24 h after Injury
Tissue Oxygen Tension in Humans after TBI
Brain pO2 Outcome lt20 mmHg Poor 20-30 mmHg Moderate gt30 mmHg Good
Therapy in both patient groups was aimed at maintaining an ICP less than 20 mm Hg and a CPP greater than 60 mm Hg Among patients
whose brain tissue PO2 was monitored oxygenation was maintained at levels greater
than 25 mm Hg
J Neurosurg 103805ndash811 2005
Reduced mortality rate in patients with severe traumatic brain injury treated with brain tissue oxygen monitoring
M STIEFEL MD PHD M S GRADY MD AND P D LE ROUX MD U Penn
Patients treated with ICP and brain tissue PO2 monitoring
were compared with historical controls
The mortality rate in patients treated using conventional ICP and CPP management was 44 Patients who also
underwent brain tissue PO2 monitoring had a significantly reduced mortality rate of 25 (p 005)
PtO2
TBI Clinical Trials--ongoinghellip2013 Clinical trials Gov n= 762 (n= 307 in 2010) DOD effecthellip$120M in 2007hellip
80 observationalhellip
bull Brain 0xygen ndashdirected therapyhellipBOOSTUT NIH
bull COSBIDmdashEcoGhellipfor Spreading depolarisations
bull IMPACThellip bull TRACK II-III bull Non ndashinvasive ICPrdquoECHODIA ldquo systemX2 bull PET to trace Neuroinflammation in STBINIH
CBF monitoring
bull Transcranial Doppler Monitoring bull Easy to use noninvasive
repeatable bull Measures basal cerebral bld flow
velocity flow via doppler equation bull Used to differentiate vasospasm
from hyperaemia (Lindegaard Index)
What has been achieved by monitoring the injured Brain
bull Improved understanding of dynamic pathophysiology after HUMAN TBI SAH
bull Guide design of neuroprotection trialshellip bull Improved patient outcome
Age (years)
Pro
babi
lity
of o
utco
me
()
20 40 60 80
0
20
40
60
80
100
Death rate ndashsevere TBI
bull Australia and NZ bull The Alfred
Royal Melbourne Hospital Royal Adelaide Hospital Royal Perth Hospital Sir Charles Gairdner Hospital Nepean Hospital John Hunter Hospital Royal North Shore Hospital Liverpool Hospital Wollongong Hospital Princess Alexandra Hospital Gold Coast Hospital Flinders Medical Centre Auckland Hospital Waikato Hospital Wellington Hospital
bull Saudi Arabia King Fahad National Guard Hospital
Canada bull Hamilton General hospital
Vancouver General Hospital Sunnybrook Medical Centre Royal Columbian Hospital India
bull Christian Medical College Ludhiana
bull
bull
Early bifrontal decompression Vs medical management No benefit from surgeryhellipmore disabled and vegetative outcomes
3 editorials on the DECRA tria
bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

Human TBIhellipand COSBID suppression of large amplitude delta activity (eg PLEDs)
EEG
DC
1 s
1 min
Temperature ranges
All temps during monitoring
Temp during CSD
lt 350 17 10
350-380 58 23
gt380 25 68
Chi-square plt0001
N=~130 USAEU
Expl
aine
d Va
rianc
e N
agel
kerk
ersquos R
2
Univariate Analysis-outcome
0002004006008
01012014016018
Significance at plt005
350355360365370375380385390395400
1800 00
060
012
0018
00 000
600
1200
1800 00
060
012
0018
00 000
600
Synergistic pathomechanisms are commonesthellip
Do we need synergistic THERAPIES For multiple damage Mechanisms
0
100
200
300
400
500
600
700
800
0 20 40 60 80 100
Between 24 - 48 h after Injury
Brain tissue oxygen tension (PtiO2)
0
50
100
150
200
250
300
350
0 20 40 60 80 100
Brain tissue oxygen tension (PtiO2)H
Between 6 -24 h after Injury
Tissue Oxygen Tension in Humans after TBI
Brain pO2 Outcome lt20 mmHg Poor 20-30 mmHg Moderate gt30 mmHg Good
Therapy in both patient groups was aimed at maintaining an ICP less than 20 mm Hg and a CPP greater than 60 mm Hg Among patients
whose brain tissue PO2 was monitored oxygenation was maintained at levels greater
than 25 mm Hg
J Neurosurg 103805ndash811 2005
Reduced mortality rate in patients with severe traumatic brain injury treated with brain tissue oxygen monitoring
M STIEFEL MD PHD M S GRADY MD AND P D LE ROUX MD U Penn
Patients treated with ICP and brain tissue PO2 monitoring
were compared with historical controls
The mortality rate in patients treated using conventional ICP and CPP management was 44 Patients who also
underwent brain tissue PO2 monitoring had a significantly reduced mortality rate of 25 (p 005)
PtO2
TBI Clinical Trials--ongoinghellip2013 Clinical trials Gov n= 762 (n= 307 in 2010) DOD effecthellip$120M in 2007hellip
80 observationalhellip
bull Brain 0xygen ndashdirected therapyhellipBOOSTUT NIH
bull COSBIDmdashEcoGhellipfor Spreading depolarisations
bull IMPACThellip bull TRACK II-III bull Non ndashinvasive ICPrdquoECHODIA ldquo systemX2 bull PET to trace Neuroinflammation in STBINIH
CBF monitoring
bull Transcranial Doppler Monitoring bull Easy to use noninvasive
repeatable bull Measures basal cerebral bld flow
velocity flow via doppler equation bull Used to differentiate vasospasm
from hyperaemia (Lindegaard Index)
What has been achieved by monitoring the injured Brain
bull Improved understanding of dynamic pathophysiology after HUMAN TBI SAH
bull Guide design of neuroprotection trialshellip bull Improved patient outcome
Age (years)
Pro
babi
lity
of o
utco
me
()
20 40 60 80
0
20
40
60
80
100
Death rate ndashsevere TBI
bull Australia and NZ bull The Alfred
Royal Melbourne Hospital Royal Adelaide Hospital Royal Perth Hospital Sir Charles Gairdner Hospital Nepean Hospital John Hunter Hospital Royal North Shore Hospital Liverpool Hospital Wollongong Hospital Princess Alexandra Hospital Gold Coast Hospital Flinders Medical Centre Auckland Hospital Waikato Hospital Wellington Hospital
bull Saudi Arabia King Fahad National Guard Hospital
Canada bull Hamilton General hospital
Vancouver General Hospital Sunnybrook Medical Centre Royal Columbian Hospital India
bull Christian Medical College Ludhiana
bull
bull
Early bifrontal decompression Vs medical management No benefit from surgeryhellipmore disabled and vegetative outcomes
3 editorials on the DECRA tria
bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

Expl
aine
d Va
rianc
e N
agel
kerk
ersquos R
2
Univariate Analysis-outcome
0002004006008
01012014016018
Significance at plt005
350355360365370375380385390395400
1800 00
060
012
0018
00 000
600
1200
1800 00
060
012
0018
00 000
600
Synergistic pathomechanisms are commonesthellip
Do we need synergistic THERAPIES For multiple damage Mechanisms
0
100
200
300
400
500
600
700
800
0 20 40 60 80 100
Between 24 - 48 h after Injury
Brain tissue oxygen tension (PtiO2)
0
50
100
150
200
250
300
350
0 20 40 60 80 100
Brain tissue oxygen tension (PtiO2)H
Between 6 -24 h after Injury
Tissue Oxygen Tension in Humans after TBI
Brain pO2 Outcome lt20 mmHg Poor 20-30 mmHg Moderate gt30 mmHg Good
Therapy in both patient groups was aimed at maintaining an ICP less than 20 mm Hg and a CPP greater than 60 mm Hg Among patients
whose brain tissue PO2 was monitored oxygenation was maintained at levels greater
than 25 mm Hg
J Neurosurg 103805ndash811 2005
Reduced mortality rate in patients with severe traumatic brain injury treated with brain tissue oxygen monitoring
M STIEFEL MD PHD M S GRADY MD AND P D LE ROUX MD U Penn
Patients treated with ICP and brain tissue PO2 monitoring
were compared with historical controls
The mortality rate in patients treated using conventional ICP and CPP management was 44 Patients who also
underwent brain tissue PO2 monitoring had a significantly reduced mortality rate of 25 (p 005)
PtO2
TBI Clinical Trials--ongoinghellip2013 Clinical trials Gov n= 762 (n= 307 in 2010) DOD effecthellip$120M in 2007hellip
80 observationalhellip
bull Brain 0xygen ndashdirected therapyhellipBOOSTUT NIH
bull COSBIDmdashEcoGhellipfor Spreading depolarisations
bull IMPACThellip bull TRACK II-III bull Non ndashinvasive ICPrdquoECHODIA ldquo systemX2 bull PET to trace Neuroinflammation in STBINIH
CBF monitoring
bull Transcranial Doppler Monitoring bull Easy to use noninvasive
repeatable bull Measures basal cerebral bld flow
velocity flow via doppler equation bull Used to differentiate vasospasm
from hyperaemia (Lindegaard Index)
What has been achieved by monitoring the injured Brain
bull Improved understanding of dynamic pathophysiology after HUMAN TBI SAH
bull Guide design of neuroprotection trialshellip bull Improved patient outcome
Age (years)
Pro
babi
lity
of o
utco
me
()
20 40 60 80
0
20
40
60
80
100
Death rate ndashsevere TBI
bull Australia and NZ bull The Alfred
Royal Melbourne Hospital Royal Adelaide Hospital Royal Perth Hospital Sir Charles Gairdner Hospital Nepean Hospital John Hunter Hospital Royal North Shore Hospital Liverpool Hospital Wollongong Hospital Princess Alexandra Hospital Gold Coast Hospital Flinders Medical Centre Auckland Hospital Waikato Hospital Wellington Hospital
bull Saudi Arabia King Fahad National Guard Hospital
Canada bull Hamilton General hospital
Vancouver General Hospital Sunnybrook Medical Centre Royal Columbian Hospital India
bull Christian Medical College Ludhiana
bull
bull
Early bifrontal decompression Vs medical management No benefit from surgeryhellipmore disabled and vegetative outcomes
3 editorials on the DECRA tria
bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

350355360365370375380385390395400
1800 00
060
012
0018
00 000
600
1200
1800 00
060
012
0018
00 000
600
Synergistic pathomechanisms are commonesthellip
Do we need synergistic THERAPIES For multiple damage Mechanisms
0
100
200
300
400
500
600
700
800
0 20 40 60 80 100
Between 24 - 48 h after Injury
Brain tissue oxygen tension (PtiO2)
0
50
100
150
200
250
300
350
0 20 40 60 80 100
Brain tissue oxygen tension (PtiO2)H
Between 6 -24 h after Injury
Tissue Oxygen Tension in Humans after TBI
Brain pO2 Outcome lt20 mmHg Poor 20-30 mmHg Moderate gt30 mmHg Good
Therapy in both patient groups was aimed at maintaining an ICP less than 20 mm Hg and a CPP greater than 60 mm Hg Among patients
whose brain tissue PO2 was monitored oxygenation was maintained at levels greater
than 25 mm Hg
J Neurosurg 103805ndash811 2005
Reduced mortality rate in patients with severe traumatic brain injury treated with brain tissue oxygen monitoring
M STIEFEL MD PHD M S GRADY MD AND P D LE ROUX MD U Penn
Patients treated with ICP and brain tissue PO2 monitoring
were compared with historical controls
The mortality rate in patients treated using conventional ICP and CPP management was 44 Patients who also
underwent brain tissue PO2 monitoring had a significantly reduced mortality rate of 25 (p 005)
PtO2
TBI Clinical Trials--ongoinghellip2013 Clinical trials Gov n= 762 (n= 307 in 2010) DOD effecthellip$120M in 2007hellip
80 observationalhellip
bull Brain 0xygen ndashdirected therapyhellipBOOSTUT NIH
bull COSBIDmdashEcoGhellipfor Spreading depolarisations
bull IMPACThellip bull TRACK II-III bull Non ndashinvasive ICPrdquoECHODIA ldquo systemX2 bull PET to trace Neuroinflammation in STBINIH
CBF monitoring
bull Transcranial Doppler Monitoring bull Easy to use noninvasive
repeatable bull Measures basal cerebral bld flow
velocity flow via doppler equation bull Used to differentiate vasospasm
from hyperaemia (Lindegaard Index)
What has been achieved by monitoring the injured Brain
bull Improved understanding of dynamic pathophysiology after HUMAN TBI SAH
bull Guide design of neuroprotection trialshellip bull Improved patient outcome
Age (years)
Pro
babi
lity
of o
utco
me
()
20 40 60 80
0
20
40
60
80
100
Death rate ndashsevere TBI
bull Australia and NZ bull The Alfred
Royal Melbourne Hospital Royal Adelaide Hospital Royal Perth Hospital Sir Charles Gairdner Hospital Nepean Hospital John Hunter Hospital Royal North Shore Hospital Liverpool Hospital Wollongong Hospital Princess Alexandra Hospital Gold Coast Hospital Flinders Medical Centre Auckland Hospital Waikato Hospital Wellington Hospital
bull Saudi Arabia King Fahad National Guard Hospital
Canada bull Hamilton General hospital
Vancouver General Hospital Sunnybrook Medical Centre Royal Columbian Hospital India
bull Christian Medical College Ludhiana
bull
bull
Early bifrontal decompression Vs medical management No benefit from surgeryhellipmore disabled and vegetative outcomes
3 editorials on the DECRA tria
bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

Synergistic pathomechanisms are commonesthellip
Do we need synergistic THERAPIES For multiple damage Mechanisms
0
100
200
300
400
500
600
700
800
0 20 40 60 80 100
Between 24 - 48 h after Injury
Brain tissue oxygen tension (PtiO2)
0
50
100
150
200
250
300
350
0 20 40 60 80 100
Brain tissue oxygen tension (PtiO2)H
Between 6 -24 h after Injury
Tissue Oxygen Tension in Humans after TBI
Brain pO2 Outcome lt20 mmHg Poor 20-30 mmHg Moderate gt30 mmHg Good
Therapy in both patient groups was aimed at maintaining an ICP less than 20 mm Hg and a CPP greater than 60 mm Hg Among patients
whose brain tissue PO2 was monitored oxygenation was maintained at levels greater
than 25 mm Hg
J Neurosurg 103805ndash811 2005
Reduced mortality rate in patients with severe traumatic brain injury treated with brain tissue oxygen monitoring
M STIEFEL MD PHD M S GRADY MD AND P D LE ROUX MD U Penn
Patients treated with ICP and brain tissue PO2 monitoring
were compared with historical controls
The mortality rate in patients treated using conventional ICP and CPP management was 44 Patients who also
underwent brain tissue PO2 monitoring had a significantly reduced mortality rate of 25 (p 005)
PtO2
TBI Clinical Trials--ongoinghellip2013 Clinical trials Gov n= 762 (n= 307 in 2010) DOD effecthellip$120M in 2007hellip
80 observationalhellip
bull Brain 0xygen ndashdirected therapyhellipBOOSTUT NIH
bull COSBIDmdashEcoGhellipfor Spreading depolarisations
bull IMPACThellip bull TRACK II-III bull Non ndashinvasive ICPrdquoECHODIA ldquo systemX2 bull PET to trace Neuroinflammation in STBINIH
CBF monitoring
bull Transcranial Doppler Monitoring bull Easy to use noninvasive
repeatable bull Measures basal cerebral bld flow
velocity flow via doppler equation bull Used to differentiate vasospasm
from hyperaemia (Lindegaard Index)
What has been achieved by monitoring the injured Brain
bull Improved understanding of dynamic pathophysiology after HUMAN TBI SAH
bull Guide design of neuroprotection trialshellip bull Improved patient outcome
Age (years)
Pro
babi
lity
of o
utco
me
()
20 40 60 80
0
20
40
60
80
100
Death rate ndashsevere TBI
bull Australia and NZ bull The Alfred
Royal Melbourne Hospital Royal Adelaide Hospital Royal Perth Hospital Sir Charles Gairdner Hospital Nepean Hospital John Hunter Hospital Royal North Shore Hospital Liverpool Hospital Wollongong Hospital Princess Alexandra Hospital Gold Coast Hospital Flinders Medical Centre Auckland Hospital Waikato Hospital Wellington Hospital
bull Saudi Arabia King Fahad National Guard Hospital
Canada bull Hamilton General hospital
Vancouver General Hospital Sunnybrook Medical Centre Royal Columbian Hospital India
bull Christian Medical College Ludhiana
bull
bull
Early bifrontal decompression Vs medical management No benefit from surgeryhellipmore disabled and vegetative outcomes
3 editorials on the DECRA tria
bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

0
100
200
300
400
500
600
700
800
0 20 40 60 80 100
Between 24 - 48 h after Injury
Brain tissue oxygen tension (PtiO2)
0
50
100
150
200
250
300
350
0 20 40 60 80 100
Brain tissue oxygen tension (PtiO2)H
Between 6 -24 h after Injury
Tissue Oxygen Tension in Humans after TBI
Brain pO2 Outcome lt20 mmHg Poor 20-30 mmHg Moderate gt30 mmHg Good
Therapy in both patient groups was aimed at maintaining an ICP less than 20 mm Hg and a CPP greater than 60 mm Hg Among patients
whose brain tissue PO2 was monitored oxygenation was maintained at levels greater
than 25 mm Hg
J Neurosurg 103805ndash811 2005
Reduced mortality rate in patients with severe traumatic brain injury treated with brain tissue oxygen monitoring
M STIEFEL MD PHD M S GRADY MD AND P D LE ROUX MD U Penn
Patients treated with ICP and brain tissue PO2 monitoring
were compared with historical controls
The mortality rate in patients treated using conventional ICP and CPP management was 44 Patients who also
underwent brain tissue PO2 monitoring had a significantly reduced mortality rate of 25 (p 005)
PtO2
TBI Clinical Trials--ongoinghellip2013 Clinical trials Gov n= 762 (n= 307 in 2010) DOD effecthellip$120M in 2007hellip
80 observationalhellip
bull Brain 0xygen ndashdirected therapyhellipBOOSTUT NIH
bull COSBIDmdashEcoGhellipfor Spreading depolarisations
bull IMPACThellip bull TRACK II-III bull Non ndashinvasive ICPrdquoECHODIA ldquo systemX2 bull PET to trace Neuroinflammation in STBINIH
CBF monitoring
bull Transcranial Doppler Monitoring bull Easy to use noninvasive
repeatable bull Measures basal cerebral bld flow
velocity flow via doppler equation bull Used to differentiate vasospasm
from hyperaemia (Lindegaard Index)
What has been achieved by monitoring the injured Brain
bull Improved understanding of dynamic pathophysiology after HUMAN TBI SAH
bull Guide design of neuroprotection trialshellip bull Improved patient outcome
Age (years)
Pro
babi
lity
of o
utco
me
()
20 40 60 80
0
20
40
60
80
100
Death rate ndashsevere TBI
bull Australia and NZ bull The Alfred
Royal Melbourne Hospital Royal Adelaide Hospital Royal Perth Hospital Sir Charles Gairdner Hospital Nepean Hospital John Hunter Hospital Royal North Shore Hospital Liverpool Hospital Wollongong Hospital Princess Alexandra Hospital Gold Coast Hospital Flinders Medical Centre Auckland Hospital Waikato Hospital Wellington Hospital
bull Saudi Arabia King Fahad National Guard Hospital
Canada bull Hamilton General hospital
Vancouver General Hospital Sunnybrook Medical Centre Royal Columbian Hospital India
bull Christian Medical College Ludhiana
bull
bull
Early bifrontal decompression Vs medical management No benefit from surgeryhellipmore disabled and vegetative outcomes
3 editorials on the DECRA tria
bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

Therapy in both patient groups was aimed at maintaining an ICP less than 20 mm Hg and a CPP greater than 60 mm Hg Among patients
whose brain tissue PO2 was monitored oxygenation was maintained at levels greater
than 25 mm Hg
J Neurosurg 103805ndash811 2005
Reduced mortality rate in patients with severe traumatic brain injury treated with brain tissue oxygen monitoring
M STIEFEL MD PHD M S GRADY MD AND P D LE ROUX MD U Penn
Patients treated with ICP and brain tissue PO2 monitoring
were compared with historical controls
The mortality rate in patients treated using conventional ICP and CPP management was 44 Patients who also
underwent brain tissue PO2 monitoring had a significantly reduced mortality rate of 25 (p 005)
PtO2
TBI Clinical Trials--ongoinghellip2013 Clinical trials Gov n= 762 (n= 307 in 2010) DOD effecthellip$120M in 2007hellip
80 observationalhellip
bull Brain 0xygen ndashdirected therapyhellipBOOSTUT NIH
bull COSBIDmdashEcoGhellipfor Spreading depolarisations
bull IMPACThellip bull TRACK II-III bull Non ndashinvasive ICPrdquoECHODIA ldquo systemX2 bull PET to trace Neuroinflammation in STBINIH
CBF monitoring
bull Transcranial Doppler Monitoring bull Easy to use noninvasive
repeatable bull Measures basal cerebral bld flow
velocity flow via doppler equation bull Used to differentiate vasospasm
from hyperaemia (Lindegaard Index)
What has been achieved by monitoring the injured Brain
bull Improved understanding of dynamic pathophysiology after HUMAN TBI SAH
bull Guide design of neuroprotection trialshellip bull Improved patient outcome
Age (years)
Pro
babi
lity
of o
utco
me
()
20 40 60 80
0
20
40
60
80
100
Death rate ndashsevere TBI
bull Australia and NZ bull The Alfred
Royal Melbourne Hospital Royal Adelaide Hospital Royal Perth Hospital Sir Charles Gairdner Hospital Nepean Hospital John Hunter Hospital Royal North Shore Hospital Liverpool Hospital Wollongong Hospital Princess Alexandra Hospital Gold Coast Hospital Flinders Medical Centre Auckland Hospital Waikato Hospital Wellington Hospital
bull Saudi Arabia King Fahad National Guard Hospital
Canada bull Hamilton General hospital
Vancouver General Hospital Sunnybrook Medical Centre Royal Columbian Hospital India
bull Christian Medical College Ludhiana
bull
bull
Early bifrontal decompression Vs medical management No benefit from surgeryhellipmore disabled and vegetative outcomes
3 editorials on the DECRA tria
bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

TBI Clinical Trials--ongoinghellip2013 Clinical trials Gov n= 762 (n= 307 in 2010) DOD effecthellip$120M in 2007hellip
80 observationalhellip
bull Brain 0xygen ndashdirected therapyhellipBOOSTUT NIH
bull COSBIDmdashEcoGhellipfor Spreading depolarisations
bull IMPACThellip bull TRACK II-III bull Non ndashinvasive ICPrdquoECHODIA ldquo systemX2 bull PET to trace Neuroinflammation in STBINIH
CBF monitoring
bull Transcranial Doppler Monitoring bull Easy to use noninvasive
repeatable bull Measures basal cerebral bld flow
velocity flow via doppler equation bull Used to differentiate vasospasm
from hyperaemia (Lindegaard Index)
What has been achieved by monitoring the injured Brain
bull Improved understanding of dynamic pathophysiology after HUMAN TBI SAH
bull Guide design of neuroprotection trialshellip bull Improved patient outcome
Age (years)
Pro
babi
lity
of o
utco
me
()
20 40 60 80
0
20
40
60
80
100
Death rate ndashsevere TBI
bull Australia and NZ bull The Alfred
Royal Melbourne Hospital Royal Adelaide Hospital Royal Perth Hospital Sir Charles Gairdner Hospital Nepean Hospital John Hunter Hospital Royal North Shore Hospital Liverpool Hospital Wollongong Hospital Princess Alexandra Hospital Gold Coast Hospital Flinders Medical Centre Auckland Hospital Waikato Hospital Wellington Hospital
bull Saudi Arabia King Fahad National Guard Hospital
Canada bull Hamilton General hospital
Vancouver General Hospital Sunnybrook Medical Centre Royal Columbian Hospital India
bull Christian Medical College Ludhiana
bull
bull
Early bifrontal decompression Vs medical management No benefit from surgeryhellipmore disabled and vegetative outcomes
3 editorials on the DECRA tria
bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

CBF monitoring
bull Transcranial Doppler Monitoring bull Easy to use noninvasive
repeatable bull Measures basal cerebral bld flow
velocity flow via doppler equation bull Used to differentiate vasospasm
from hyperaemia (Lindegaard Index)
What has been achieved by monitoring the injured Brain
bull Improved understanding of dynamic pathophysiology after HUMAN TBI SAH
bull Guide design of neuroprotection trialshellip bull Improved patient outcome
Age (years)
Pro
babi
lity
of o
utco
me
()
20 40 60 80
0
20
40
60
80
100
Death rate ndashsevere TBI
bull Australia and NZ bull The Alfred
Royal Melbourne Hospital Royal Adelaide Hospital Royal Perth Hospital Sir Charles Gairdner Hospital Nepean Hospital John Hunter Hospital Royal North Shore Hospital Liverpool Hospital Wollongong Hospital Princess Alexandra Hospital Gold Coast Hospital Flinders Medical Centre Auckland Hospital Waikato Hospital Wellington Hospital
bull Saudi Arabia King Fahad National Guard Hospital
Canada bull Hamilton General hospital
Vancouver General Hospital Sunnybrook Medical Centre Royal Columbian Hospital India
bull Christian Medical College Ludhiana
bull
bull
Early bifrontal decompression Vs medical management No benefit from surgeryhellipmore disabled and vegetative outcomes
3 editorials on the DECRA tria
bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

What has been achieved by monitoring the injured Brain
bull Improved understanding of dynamic pathophysiology after HUMAN TBI SAH
bull Guide design of neuroprotection trialshellip bull Improved patient outcome
Age (years)
Pro
babi
lity
of o
utco
me
()
20 40 60 80
0
20
40
60
80
100
Death rate ndashsevere TBI
bull Australia and NZ bull The Alfred
Royal Melbourne Hospital Royal Adelaide Hospital Royal Perth Hospital Sir Charles Gairdner Hospital Nepean Hospital John Hunter Hospital Royal North Shore Hospital Liverpool Hospital Wollongong Hospital Princess Alexandra Hospital Gold Coast Hospital Flinders Medical Centre Auckland Hospital Waikato Hospital Wellington Hospital
bull Saudi Arabia King Fahad National Guard Hospital
Canada bull Hamilton General hospital
Vancouver General Hospital Sunnybrook Medical Centre Royal Columbian Hospital India
bull Christian Medical College Ludhiana
bull
bull
Early bifrontal decompression Vs medical management No benefit from surgeryhellipmore disabled and vegetative outcomes
3 editorials on the DECRA tria
bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

bull Australia and NZ bull The Alfred
Royal Melbourne Hospital Royal Adelaide Hospital Royal Perth Hospital Sir Charles Gairdner Hospital Nepean Hospital John Hunter Hospital Royal North Shore Hospital Liverpool Hospital Wollongong Hospital Princess Alexandra Hospital Gold Coast Hospital Flinders Medical Centre Auckland Hospital Waikato Hospital Wellington Hospital
bull Saudi Arabia King Fahad National Guard Hospital
Canada bull Hamilton General hospital
Vancouver General Hospital Sunnybrook Medical Centre Royal Columbian Hospital India
bull Christian Medical College Ludhiana
bull
bull
Early bifrontal decompression Vs medical management No benefit from surgeryhellipmore disabled and vegetative outcomes
3 editorials on the DECRA tria
bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

3 editorials on the DECRA tria
bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

bull Study design-486 patientshellip ndash Blinded assessment of outcomes ndash Randomization completed in
blocks of 5 stratified according to center
ndash Compared bone flaps of dimension 12x15cm vs 6x8cm
ndash Necrotic tissue debrided ndash Dura closure with graft to expand ndash Otherwise managed as per 1996
AANS guidelines for head trauma ndash Blinded physiatrist performed
follow-up exam at 6 months after injury
Jiang et al 2005 Effect of Standard Trauma Craniotomy for refractory ICP with severe TBI-a multicenter Prospective randomised controlled study J Neurotrauma22623-6282005
Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

Cambridge ndash 34 Leeds ndash 20 Royal London ndash 12 Newcastle ndash 11 Southampton ndash 10 Singapore ndash 8 Milan Italy ndash 6 Manchester ndash 6 Saudi Arabia ndash 5 Edmonton Canada ndash 5 Calgary Canada ndash 4 Hong-Kong ndash 4 Old Church ndash 4 Plymouth ndash 4 Hurstwood Park ndash 3 Kings College ndash 3 Pavia Italy ndash 3 Barcelona Spain ndash 2 Livorno Italy ndash 1 Malaysia ndash 1 Oxford ndash 1 Queenrsquos Square ndash 1 Swansea ndash 1 Ulm Germany - 1
wwwRESCUEicpcom
357 patients recruited -january 2013 Results early 2014hellip
Unilateral large DC Includes High ICP Due to contusions
R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry

R 21 Grant NIH NINDS RNS069309ACapacity building for
Decompressive Craniotomy in Colombiahellip
The objective of this proposal is to create a standardized protocol for DC implementation with subsequent implementation of the protocol in three hospitals in Colombia The initial pilot study will accrue 40 adult patients with severe TBI and evaluate outcomes over a 2 year period using the
data registry