Embed Size (px)
Citation preview

Indexed in:Scopus, EMBASE/Excerpta Medica, Índice Médico Español (IME), Índice Bibliográfico Español en Ciencias de la Salud (IBECS)
DSINTERNATIONAL MEDICAL REVIEW
ON DOWN’S SYNDROME
Volume 17•Number 3
September-December
2013Contents Editorial35 Dr. Pueschel and the Foundation M. Trueta
We have lost a great friend A. Serés
Original article36 Down syndrome due to rare inherited 15/21 Robertsonian
translocation: genetics and reproductive counseling L.M. Azevedo Moreira, L. Damasceno Espirito Santo
and A. Fernandes Lacerda Carvalho
Case report39 Marriage and reproduction in a woman with Down
syndrome L.M. Azevedo Moreira and L. Damasceno Espirito Santo
Clinics and practice43 Trajectory and challenges of the Leisure Service:
The first 25 years C. Herreros and M.J. Miquel
www.elsevier.es/sd
INTERNATIONALMEDICAL REVIEW ON DOWN’S SYNDROMESD
ISSN: 1138-011X
www.fcsd.org

FUNDACIÓ CATALANA SÍNDROME DE DOWN21
INTERNATIONALMEDICAL REVIEW ON DOW'N SYNDROMESD
Editorial CommitteeEditor: Josep M. CorretgerEditor-in-Chief: Agustí SerésEditorial and Coordination: Katy Trias Trueta
Medical AdvisersF. Ballesta MartínezM. Cruz HernándezJ. Moreno Hernando
Psycho-pedagogy advisersFCSD TeamJ. M. JarqueT. Vilà L. Brown (USA)
Editorial SecretaryMar Cabezas
The aim of SD REVISTA MÉDICA INTERNACIONAL SOBRE EL SÍNDROME DE DOWN (INTERNATIONAL MEDICAL JOURNAL ON DOWN’S SYNDROME) is, on the one hand, to gather cur-rent knowledge on the medical aspects of Down’s Syndrome, and to continuously review and update this, from the most promising advances in basic sciences, such as molecular biology and genetics, to daily clinical practice; and on the other hand, to look at those psychopedagogical ���������������� ���������� ���������������������� ����� ������������������� �������������������������������������� ������with Down’s Syndrome. SD will consider publishing clinical or research articles associated with all branches of Down’s Syndrome.
�����������������Cardiology: J. CasaldàligaDermatology: J. FerrandoDietetics-nutrition: N. EgeaEndocrinology: A. GodayMaxillofacial Surgery: A. MonnerGenetics: A. SerésGeriatrics: C. FarriolsGynaecology: J. CararachGeneral Medicine: A. GarnachoChild Neurology: A. NascimentoAdult Neurology: S. FernándezDentistry and Orthodontics: M. A. MayoralChild Ophthalmology: A. GalánAdult Ophthalmology: J. Puig, S. SimónEar, Nose and Throat: J. DomènechPaediatrics: J. M. Corretger, M. Hernández, J. García PérezPsychology: B. GarvíaPsychiatry: J. BarbaTraumatology and Orthopaedics: F. Torner
Travessera de Gràcia, 17-2108021 Barcelona Tel.: +34 932 000 711
Available on internet: www.elsevier.es/sd
Annual subscription ratesProfessionals 87,16 €Institutions 220,66 €(VAT included. Prices only apply to Spain)
Subscriptions and customer care:Elsevier España, S.L.������������������������!"#"��$����� ��%Tel.: 902 888 740E-mail: [email protected]
Data protection: Elsevier España, S.L., declares that it complies with that established by Organic Law 15/1999, 13 December, Protection of Personal Data.
Chlorine-free ecological paper.
This publication is printed on acid-free paper.
E-mail: [email protected]
Printed in Spain. Legal deposit: B-40257-1986
ISSN: 1138-011X
© Copyright 2013 Fundació Catalana Síndrome de Down
All rights reserved. The contents of this publication may not be reproduced or transmitted by any elec-tronic or mechanical procedure, including photoco-pying and magnetic tape, or recorded in any informa-tion recovery system in any form or by any medium, without previous written authorisation of the owner of the exploitation rights of the same.ELSEVIER ESPAÑA, in accordance to that set out in Article 32.1, second para- graph of the current Reformulated Text of the Intellectual Property Law TRLPI, expressly prohibits the use or partial use of the pages of SD, Revista Médica Internacional sobre el Síndrome de Down with the aim of preparing printed abstracts for commercial purposes.
Any form of reproduction, distribution, public presen-tation or transformation of this journal can only be done with the approval of its owners, unless there is
an exception envisaged in the law. Get in touch with &'*<= >&���� '���? � �� *���� � <��� ��Q�� ��www.cedro.org) if you need to photocopy or scan any part of this journal.
No responsibility is assumed by the Publisher or the Catalonian Down’s Syndrome Foundation (FCSD) for any injury and/or damage to persons or property as a matter of products liability, negligence or otherwise, or from any use or operation of any methods, pro-ducts, instructions or ideas contained in the mate-rial herein. Because of rapid advances in the medical ��������� �� ����������� ����������� ��������� � �diagnoses and drug dosages should be made.
Although all advertising material is expected to con-form to ethical (medical) standards, inclusion in this publication does not constitute a guarantee or endor-sement of the quality or value of such product or of the claims made of it by its manufacturer.
José Abascal nº 45, 3ª28003 MadridTel.: +34 914 021 212
Published every 4 months(3 issues per year).

Rev Med Int Sindr Down. 2013;17(3):35
1138-011X/$ - see front matter © 2013 Fundació Catalana Síndrome de Down. Published by Elsevier España, S.L. All rights reserved.
www.fcsd.org
INTERNATIONALMEDICAL REVIEW
ON DOWN’S SYNDROMEwww.elsevier.es/sd
EDITORIAL
Dr. Pueschel and the Foundation
Dr. Pueschel was a pioneer in the research and improve-ment of the health of people with Down’s syndrome, dedi-cating his life to publications and advice that have had an international influence.
Sig was a constant personal friend of mine. We met at numerous conferences: Rome, United States, etc. We al-ways maintained a close and continued correspondence. The loss of his son had a devastating effect on him and I believed that he never got over it.
I feel a very deep sense of loss of this irreplaceable friend. I will always remember him.
All of us who have a child with Down’s syndrome need help. Sig was a special support for me, and I would like to think that I was also a little for him.
Thank You Sig for all you have given us. Rest in Peace.
Montserrat Trueta
We have lost a great friend
On the 2nd of September 2013, we lost someone who has fought more for people with Down’s syndrome, their health and their social integration, Dr. Siegfried M. Pueschel.
Dr. Pueschel was born in 1931 in Silesia, Germany, now part of Poland. His family were admitted into Germany as
refugees, where he had to work in several positions, and graduated in Medicine in Dusseldorf in 1960. He emigrated to the USA, and was a medical intern in New Jersey, where he met his wife, Eny Vergara, with whom he had 4 children, one of them with Down’s syndrome. He specialised in Pae-diatrics and Biomedical Genetics in Harvard and Montreal Universities. In 1965 he returned to Harvard as Professor of Paediatrics, working mainly on mental handicaps due to in-born errors of metabolism, and Down’s syndrome, especial-ly after his son Chris was born with this syndrome. He was also a specialist in Developmental Psychology and Jurispru-dence.
In 1975 he was appointed as Director of the Child Devel-opment Center of Rhode Island Hospital, where he prac-ticed in Paediatrics until his retirement in January 2013. Dr. Pueschel explained and defended the world of individu-als with Down’s syndrome with Pope John Paul II and Queen Sofia of Spain. He was also a member of the National Down Syndrome Congress, the National Down Syndrome Society, and the Association for Retarded Citizens. In his hospital he attended to thousands of individuals with Down’s syndrome, and without a doubt he had the most clinical histories of Down’s syndrome in the USA.
Dr. Pueschel was a person who loved sport, had run 38 mara- thons, climbed Kilimanjaro, reached the Mt. Everest base camp, and was also a black belt in Tae Kwan Do.
His extensive scientific activity can be found in the 15 books and more than 200 articles written by him. He also took part in hundreds of scientific conferences and meetings all over the world. He was an active contributor in the Catalan Down’s Syndrome Foundation, participating in many of the conferences that the Foundation has organised over the past 30 years. He was currently a consultant for our Inter-national Medical Journal.
His humanity and closeness were, without a doubt, his most outstanding qualities, always ready to help all those who asked for it, and always supporting individuals with Down’s syndrome. We have lost a great person, and for us, one of our best friends. Dr. Pueschel has gone, but his work will still be valid for many years, “the man passes away, his deeds remain”.
Dr. Agustí Serés

Rev Med Int Sindr Down. 2013;17(3):36-38
1138-011X/$ - see front matter © 2013 Fundació Catalana Síndrome de Down. Published by Elsevier España, S.L. All rights reserved.
www.fcsd.org
INTERNATIONALMEDICAL REVIEW
ON DOWN’S SYNDROMEwww.elsevier.es/sd
ORIGINAL ARTICLE
Down syndrome due to rare inherited 15/21 Robertsonian translocation: genetics and reproductive counselinga
L.M. Azevedo Moreira*, L. Damasceno Espirito Santo and A. Fernandes Lacerda Carvalho
Laboratory of Human Genetics and Mutagenesis, Institute of Biology, Federal University of Bahia, Salvador, Bahia, Brazil
Received on November 26, 2012; accepted on July 2, 2013
KEYWORDSDown’s syndrome; Abortion; Chromosomal rearrangement; Reproduction; Fertility
PALABRAS CLAVESíndrome de Down; Aborto; Reordenamiento cromosómico; Reproducción; Fertilidad
AbstractThe carriers of a rearrangement involving with chromosome 21 have a potential risk of genetically unbalanced conceptions, which may result in liveborn children with Down syndrome. Reproductive risks for couples carriers of a balanced Robertsonian translocation depends on the rearranged chromosomes and the sex of the carrier. This article aims to analyze the segregation and reproductive trend of a rare 15/21 translocation in five generations of a family. It was considered the current advances in reproductive technology as a possibility to prevent fetal aneuploidia. Given the genetic risk, the preimplantation diagnosis appears also as an alternative to avoid the option of an unwanted later abortion and to obtain a healthy progeny.
Síndrome de Down hereditario poco común debido a la translocación robertsoniana 15/21: asesoramiento genético y reproductivo
ResumenLos portadores de un reordenamiento que afecta al cromosoma 21 tienen un riesgo po-tencial de concepciones genéticamente desequilibradas que pueden dar origen a niños con síndrome de Down. Los riesgos reproductivos de las parejas portadoras de una trans-locación robertsoniana equilibrada dependen de los cromosomas reordenados y del sexo del portador. Este artículo tiene como objetivo analizar la tendencia de segregación y reproductiva de una rara translocación 15/21 en cinco generaciones de una familia. Se consideraron los avances actuales en tecnología reproductiva como una posibilidad para evitar la aneuploidía fetal. Dado el riesgo genético, el diagnóstico de preimplantación aparece también como una alternativa para evitar la posibilidad de un aborto posterior no deseado y para obtener una descendencia saludable.
aThis work has not been presented at any Conference or in any journal, nor has it received any award or financial support.
*Author for correspondence.E-mail: [email protected] (L.M. Azevedo).

Down syndrome due to rare inherited 15/21 Robertsonian translocation: genetics and reproductive counseling 37
Introduction
Balanced Robertsonian translocation (rob) is a frequent structural chromosome abnormality with a prevalence of 1 in 1000 health individuals, often referred for reproductive counseling1. The most common form of this translocation involves chromosomes 13 and 14 or 14 and 212. Bandyopad-hyay et al.3 classified the Robertsonian translocations (robs) in two groups, according their frequency of occurrence: common - rob (13q14q) and rob (14q21q) and rare forms as rob (15q21q). The carriers of a balanced rearrangement in-volving chromosome 21 presents a potential risk of geneti-cally unbalanced conceptions which may result in liveborn children with Down syndrome (DS).
Studies about parental origin, segregation and progeny outcome, for rare ROBs, have not been frequently carried out. Here we presented a family with segregation of a rob (15q21q) in five generations, because of the high occur-rence of DS cases, with the purpose of genetic and repro-ductive counseling. Possibilities of prenatal diagnosis and advances in preimplantation genetic diagnosis were consid-ered in order to predict the likelihood of having a liveborn healthy child.
Patients and Methods
The family was investigated from the propositus with a clinical diagnosis of DS, attended at the Program of Com-munity Genetics (Genetics & Society), Federal University of Bahia. Informations about the family history, pedigree, parental age, birth order, DS outcomes, were recorded. Cytogenetic studies from the propositus and family mem-bers were performed on cultured blood lymphocytes using standard method and chromosome identify by GTG band-ing4. At least 15 cells were analyzed for each individual and 5 karyotypes were prepared with photomicrographs take on a Zeiss Axiophot microscope. Informed consent was obtained from patients in the study after the nature of the procedure had been fully explained to them. Par-ticipation in the study was voluntary and in concordance to the ethical standards laid down in the 1964 Declaration of Helsinki.
Results
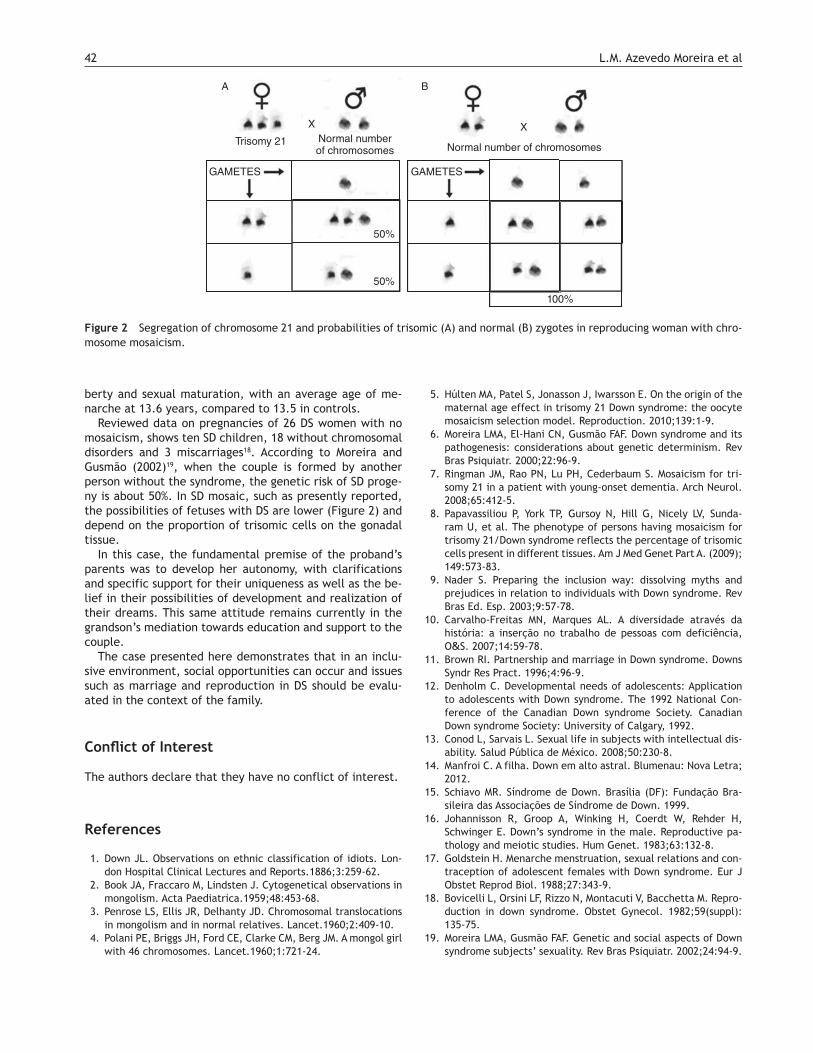
The genealogy is presented at Figure 1. The propositus was a 50 year old woman, with a clinical diagnosis of DS pre-senting signs as: microcephaly, flat occiput, up-slanting pal-pebral fissures, bilateral epicanthal folds, flat nasal bridge, small ears, tendency of tongue protrusion, short stature.
A total of 45 individuals descendants of the first known couple are shown in the pedigree, excluding the spouses. Of these, 6 (13%) showed the unbalanced translocation and DS, 3 were diagnosed by clinical examination and 3 others, by cytogenetic analyses; 39 (87%) showed no DS signals. Among relatives cytogenetically investigated or considered obli-gate carriers by having affected progeny, there were 9 cas-es of balanced translocations, 6 (67%) female and 3 (33%) male, due to alternate segregation, the meiotic behavior most common in all Robertsonian translocation. Among the other 30 individuals, 3 were confirmed as having nor- mal karyotype and the other were not examined for death (n = 3) or another reasons (n = 24).
Parental age at conception of DS children was below 30 years, in the last three generations, except for child born of second marriage of a man carrier of the balanced transloca-tion (IV-10). The parental origin of the oldest related DS patient could not be determined. In the others cases of 6 translocations DS patients, 4 (67%) were originated from the mother and 1, from the father. The abortion rate was low, even in couples of carriers of balanced translocation.
In the present family, none of the members performed prenatal chromosomal diagnosis, or had access to new re-productive technologies, even though there were young mothers with DS progeny. After the study these individuals learned the advances and the information about the possi-bility of health outcomes.
Discussion
According to Scriven et al.5, translocated couples need as-sisted conception for subfertility. Keymolen et al.1, consid-ering all pregnancy of ROB carriers with balanced transloca-tion, observed that 52,7% females carriers and 61,8% of males, led to the birth of a healthy child. The frequency
Figure 1 Family pedigree.
NN
N
3
1d
1d
I
II
III
IV
V
VI
2d 3d 4d 5
2d
6d 7d 8d
987654321
3*
*
4 5 6 7 8 9 10 11 12 13 14 15
11 12 13
16 17 18
12
14
87654321
1
21
10
2
Clinical diagnostic of Down Syndrome
Proband
Decesed, not examined
N N
d
*Not examined
Normal Chromosomes
Carrier “15/21” Translocation
21 Trisomy

38 L.M. Azevedo Moreira et al
of normal and balanced karyotype confirms the previous study of chromosome segregation in sperm6, showing alter-nate segregation, which results in gametes with balanced genetic material, as the most frequent mode of segregation in this chromosomal rearrangement. Furthermore occur an excess of balanced karyotypes when comparated to normal karyotypes1,7.
Jyothy et al.8 refer that translocated DS children are of-ten born from mothers aged bellow 25 years and argue that this can be explained by the high frequency of primigravi-dae in these women and the fact that the incidence of mis-carriage is low in women conceiving at first pregnancy for unknown reasons. The fact of the presently studied family does not mention abortion, confirms the referred reproduc-tive trend or can reflect an underestimation by the absence of prior genetic register.
Couples with a translocation carrier, often perform the prenatal diagnosis even fearing the possibility of option of pregnancy termination when the child has trisomy by trans-location. In these cases, the preimplantation genetic diag-nosis (PGD) can be a valuable screen to prevent the occur-rence of an unbalanced conception. The alternated embryos (normal/balanced) are the main types of conceptus and with PGD, these embryos can be selected for transfer into the uterus9. The donor of gametes in procedures of in vitro fertilization (IVF) offers an additional alternative to reduce the risk of fetal aneuploidy.
Conn et al.10 observed that couples that suffer repeated pregnancy termination are leaning forward genetic diagno-sis before implantation to avoid later abortion. PGD for Robertsonian translocations has been undertaken success-fully in some centers of advanced research, whether by po-lar body biopsy11 or blastomere at day 3, after fertiliza-tion12,13. These new methods however are still not routine procedures.
Despite these advances, Keymolen et al.1 observed that the likelihood of a healthy liveborn child of the pregnancy in couples with a Robertsonian translocation carrier is around 50-70%, either by spontaneous conception or assist-ed reproductive technologies, with or without PGD. Many couples do not use these technologies, either for lack of knowledge, economic reasons, or yet ethical and moral rea-sons.
Bernicot et al.14 studying 2 carriers of rare Robertsonian translocation rob (13;21) and rob (15;22) combining analy-sis of meiotic segregation in sperm and PGD, refered res-pectively 86,3% and 87,5%, of gametes with normal or bal-anced chromosome complement. The authors also observed a high rate of mosaic or chaotic embryos but both studied showed cases of normal pregnancy and outcomes, showing the benefices of the PGD advances.
Given the genetic risk for carriers of Robertsonian translo-cations, there is a real need for new studies about chromo-somal segregation especially because these rearrangements are becoming an important indication for pre-implantation genetic diagnosis. We also recommend additio nal studies
to establishing the success of the advances of assisted re-productive between carriers of rare Robertsonian translo- cations.
�� �������������
The authors declare that they have no conflict of interest.
����������
1. Keymolen K, Berkel KV, Vorsselmans A, Staessen C, Liebaers I. Pregnancy outcome in carriers of Robertsonian translocations. Am J Hum Genet Part A. 2011;155:2381-5.
2. Gardner RJM, Sutherland GR. Chromosome Abnormalities and Genetic Counselling. 3rd ed. New York: Oxford University Press; 2004.
3. Bandyopadhyay R, Heller A, Knox-DuBois C, McCaskill C, Ber-end SA, Page SL, et al. Parental origin and timing of de novo Robertsonian translocation formation. Am J Hum Genet. 2002; 71:1456-62.
4. Shaffer LG, Slovak ML, Campbell LJ. ISCN 2009 an international system for human cytogenetic nomenclature. Basel: Karger; 2009.
5. Scriven PN, Flinter FA, Braude PR, Ogilvie CM. Robertsonian translocations-reproductive risks and indications for preim-plantation genetic diagnosis. Hum Reprod. 2001;16:2267-73.
6. Ogur G, Van Assche E, Vegetti W, Tournaye H, Bonduelle M, Van Steirteghem A, et al. Chromosomal segregation in spermatozoa of 14 Robertsonian translocation carriers. Mol Hum Reprod. 2006;12:209-15.
7. Boué A, Gallano P. A collaborative study of the segregation of inherited chromosome structural rearrangments in 1356 prena-tal diagnoses. Prenat Diagn. 1984;4:45-67.
8. Jyothy A, Mallikarjuna R, Kumar K, Babu Rao V, Uma Devi B, Reddy PP. Translocation Down syndrome. Indian J Med Sci. 2002;56:225-9.
9. Huang J, Lian Y, Qiao J, Chen Y, Ren X, Liu P. Characteristics of embryo development in Robertsonian translocation’ preim-plantation genetic diagnosis cycles. Prenl Diagn. 2009;29:1167-70.
10. Conn CM, Cozzi J, Harper JC, Winston RML, Delhanty JDA. Pre-implantation genetic diagnosis for couples at high risk of Down syndrome pregnancy owing to parental translocation or mosai-cism. J Med Genet. 1999;36:45-50.
11. Munné S, Fung J, Cassel MJ, Márquez C, Weier HUG. Preimplan-tation genetic analysis of translocations: case-specific probes for interphase cell analysis. Hum Genet. 1998;102:663-74.
12. Escudero T, Lee M, Carrel, D, Blanco J, Munne A. Analysis of chromosome abnormalities in sperm and embryos from two 45, XY,t(13;14)(q10;q10) carriers. Pren Diagn. 2000;20:599-602.
13. Munné S, Sandalinas M, Escudero T, Fung J, Gianaroli L, Cohen J. Outcome of preimplantation genetic diagnosis of transloca-tions. Fertil Steril. 2000;73:1209-18.
14. Bernicot I, Schneider A, Mace A, Hamamah S, Hedon B, Pellestor F, et al. Analysis using fish of sperm and embryos from two car-riers of rare (13;21) and rob(15;22) robertsonian translocation undergoing PGD. Eur J Med Genet. 2012;55:245-51.

Rev Med Int Sindr Down. 2013;17(3):39-42
1138-011X/$ - see front matter © 2013 Fundació Catalana Síndrome de Down. Published by Elsevier España, S.L. All rights reserved.
www.fcsd.org
INTERNATIONALMEDICAL REVIEW
ON DOWN’S SYNDROMEwww.elsevier.es/sd
CASE REPORT
Marriage and reproduction in a woman with Down syndromea
L.M. Azevedo Moreira* and L. Damasceno Espirito Santo
Laboratory of Human Genetics and Mutagenesis, Institute of Biology, Federal University of Bahia, Salvador, Bahia, Brazil
Received on May 22, 2013; accepted on October 22, 2013
KEYWORDSDown syndrome; Intellectual disability; Marriage; Reproduction
AbstractSex life of people with Down syndrome (DS) or other conditions associated with intellectual disability is still a taboo, with few reports in the literature. Advances in knowledge of causal and nosological aspects, including its social achievements, have led to the strengthening of the inclusive movement aimed at those people. This paper presents an unusual case of successful marriage and reproduction of a woman with DS. The proband studied in special schools and communicates well verbally. She presented menarche at age of 13, showing autonomy in caring for her body. Eight years ago she met her current husband at the special school she attended. Two years after the wedding, the proband became pregnant of a male child without the syndrome. She is able to take care of her child needs, sharing this responsibility with her own mother, who was primarily responsible for her education directed towards autonomy. The proband’s karyotype revealed triso- my 21 with chromosomal mosaicism. New social achievements are occurring, among them the establishment of lasting emotional relationships. The reproductive chances and risks of recurrence of DS should be considered in genetic counseling. The breeding and rearing of any children born from these marriages become new responsibilities shared by these special parents and their families.
aThis investigation has not been presented at any Conference or in any journal, nor has it received any award or financial support.
*Correspondence author.E-mail: [email protected] (L.M. Azevedo).

40 L.M. Azevedo Moreira et al
Introduction
Down syndrome (DS) is an archetype of congenital genetic disorder. Advances in knowledge of causal and nosological aspects, including its social achievements, have led to the strengthening of inclusive movement aimed at people with intellectual disability and congenital disorders in general.
This syndrome was first described by the English physi-cian John Langdon Down (1866)1, but its etiology was clari-fied only in 1959, when the geneticist Jerome Lejeune and his collaborators associated this syndrome with the pres-ence of an extra chromosome 21, then becoming known as Trisomy 21. This was followed by other studies on the pathogenesis of this chromosomopathy characterizing it as a free trisomy, by translocation or mosaicism, when normal and trisomic cells are present, which occurs in 1-2% of the cases2-4. The free trisomy 21 constitutes the most common form of DS and has been associated with an increase on its rates when considering maternal age above 35 years5.
Down syndrome is characterized by mild to moderate in-tellectual disability, hypotonia and typical craniofacial signs such as oblique palpebral fissures. Heart disease and other severe systemic disorders occur in lower percentage of cas-es. The trisomy of 21q22 chromosomal band is considered pathognomonic and related with more severe disorders, al-though there is considerable phenotypic variation6. In cases of mosaicism, there are clinical manifestations ranging from a typical presentation of DS signals even very subtle, often only detected after birth7. The more severe symp-toms may be associated with a higher percentage of tri-somic cells8 or with loss of chromosome 21 in a zygote orig-inally with trisomy.
Social inclusion and education has also contributed to the development and adaptation of people with DS, often lead-ing to possibilities of working activities in conditions adapt-ed to their characteristics9. Nevertheless, the sex life of people with this syndrome or other conditions associated
with intellectual disability is still a taboo, with few reports in the literature. The objective of this paper is to review different aspects related to emotional and sexual develop-ment in DS reported through the life story of a DS woman with lasting marital relationship that led to the birth of a child without the syndrome, emphasizing the importance of the family in this process.
This paper presents an unusual case of successful mar-riage and reproduction of a woman with DS attended at the Program of Community Genetics (Genetics & Society), Fed-eral University of Bahia, Brazil.
Clinical observation
The study refers to a women with DS, now with 41 years old. Family history is negative for congenital malforma-tions and genetic disorders. Mother aged 20 and father aged 25, in her birth. She was born of vaginal section with-out complications. Clinical diagnosis of DS, in absence of severe congenital malformations. Later, she had two sib-lings. She studied in special schools; made no speech ther-apy, but can communicate well verbally. She had swimming lessons and dance. The father is a musician and publicist and she was always passionate about music. At home she was treated in the same way that her brothers without the syndrome were. She could not be literate, but was pre-pared for the job market. She worked in commerce and recently retired.
The proband presented menarche at age of 13, showing autonomy in caring for her body. She dated three col-leagues, one with the same syndrome, but was looking for a companion for a family. Eight years ago she met her current husband at the special school she attended. He was a or-phaned boy with a history of mild learning deficit associat-ed with gestational events, which lived and worked in a specialized institution.
PALABRAS CLAVESíndrome de Down; Discapacidad intelectual; Matrimonio; Reproducción
El matrimonio y la reproducción en la mujer con síndrome de Down
ResumenLa vida sexual de las personas con síndrome de Down (SD) u otros trastornos asociados con la discapacidad intelectual sigue siendo un tabú, con pocos relatos en la literatura. Los avances en el conocimiento de los aspectos causales y nosológicos, incluidas sus con-quistas sociales, llevaron al fortalecimiento del movimiento inclusivo destinado a estas personas. En este artículo se presenta un caso inusual de un matrimonio de una mujer con SD que tiene un hijo. Esta mujer estudió en escuelas especiales y se comunica bien verbalmente. Presentó menarquía a los 13 años de edad, y demostró autonomía en el cuidado de su cuerpo. Ocho años atrás conoció a su actual esposo en una escuela espe-cial. Después de 2 años de matrimonio, ella quedó embarazada de un varón sin este sín-drome. La mujer es capaz de atender las necesidades de su hijo, responsabilidad que comparte con su madre, que fue la principal responsable de su educación hacia la auto-nomía. El cariotipo de la probanda reveló trisomía 21 con mosaicismo cromosómico. Se están produciendo nuevos logros sociales, incluido el establecimiento de relaciones afec-tivas perdurables. Las posibilidades de reproducción y el riesgo de recurrencia del SD deben ser considerados en el consejo genético. El cuidado de todos los niños nacidos de estos matrimonios genera responsabilidades compartidas por estos padres especiales y sus familias.
Marriage and reproduction in a woman with Down syndrome 41
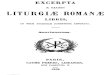
The wedding came naturally, as any couple (Figure 1 A). They married in a religious ceremony and came to live with the maternal family, dividing tasks and bringing some finan-cial contribution to the home. Two years after the wedding, the proband became pregnant at the same time as her sis-ter-in-law, surprising everyone, because the parents had received information that there was no need for contracep-tive methods because, due to the syndrome, there was no chance of pregnancy. The prenatal examination, performed at 5 months of gestation, indicated that it was a male child without the syndrome, news received with great joy by the entire family.
After the birth of her son, the proband, that since her birth had received only clinical diagnosis of DS, conducted the study of her karyotype, which revealed trisomy 21 with chromosomal mosaicism. Karyotype: 47,XX,+21/46,XX, with the majority of the trisomic lineage, present in 80% of examined cells. Currently, she enjoys good general health. Participates in literacy course for adults and is engaged in educational activities about DS. She is able to take care of her child needs, sharing this responsibility with her own mother, who was primarily responsible for her education directed towards autonomy. In six years of marriage, the couple maintains a stable and loving relationship, dedicat-ing their child to leisure time (Figure 1 B).
Discussion
A historical analysis of the development of people with DS shows a change of conceptions about this syndrome, ini-tially based on superstitions and prejudices, followed by a pathological conception of the disease; and currently con-sidered due to a genetic alteration compatible with life and possible adaptation in society as a part of human diversity, with rights and social duties. It sets up a new interpretation model for disability, in which it loses the character of indi-
vidual attribute and is now considered a contingent phe-nomenon that reshapes social actions and adjusts the envi-ronment regarding the nature of people with disabilities10.
Advances in life’s quality, longevity and inclusion meas-ures has enabled new social roles, however the issue of sexuality has been ignored or underestimated. Brown (1996)11 observes that relationships and marriages are in the context of quality of life in DS and calls attention to the need to prepare these people for life, so that these possi-bilities can happen. Denholm (1992)12 refer that adoles-cents with intellectual disabilities have the same expecta-tions in terms of moral codes, friendships, interests in fashion that young people without disabilities and argues that these trends may become more widespread, though they have less social opportunities. Conod and Servais (2008)13 report a lack of studies on people with intellectual disabilities in terms of sex as well as relationships, marriage and parenting, also remembering that these activities do not only depend on the people’s expectations, but also of socialization opportunities offered.
The families, especially the parents, are expected to be better prepared to attend the needs of their children in building their personality and evolutionary changes in vari-ous aspects of social life, and there must be no difference regarding to the DS’s ones. Even with all the independence that a person with DS can achieve, there is always a consid-eration, support, in which the family is requested with greater or lesser frequency14.
Today, depending on the case, the sexuality is more ac-cepted by the Down people relatives, but the issue of re-production is viewed with caution and seen as unfeasible by 70% of parents15. In men with DS, despite the normal devel-opment of secondary sexual characteristics, fertility is re-duced, possibly due to the anomalous behavior of chromo-some 21 in male meiosis16. Goldstein (1988)17 refer that in women with DS, sexual development occurs in a manner similar to people in the general population in terms of pu-
Figure 1 Couple in the beginning of the relationship (A) and gathering the family (B).
42 L.M. Azevedo Moreira et al
berty and sexual maturation, with an average age of me-narche at 13.6 years, compared to 13.5 in controls.
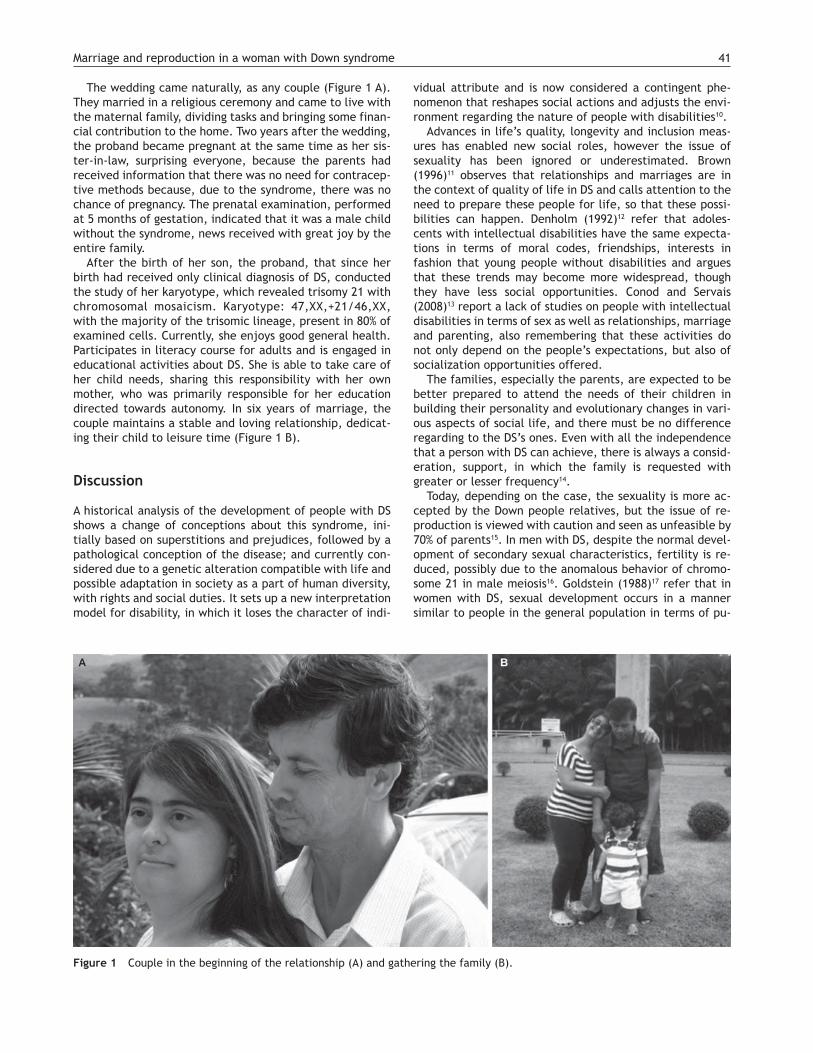
Reviewed data on pregnancies of 26 DS women with no mosaicism, shows ten SD children, 18 without chromosomal disorders and 3 miscarriages18. According to Moreira and Gusmão (2002)19, when the couple is formed by another person without the syndrome, the genetic risk of SD proge-ny is about 50%. In SD mosaic, such as presently reported, the possibilities of fetuses with DS are lower (Figure 2) and depend on the proportion of trisomic cells on the gonadal tissue.
In this case, the fundamental premise of the proband’s parents was to develop her autonomy, with clarifications and specific support for their uniqueness as well as the be-lief in their possibilities of development and realization of their dreams. This same attitude remains currently in the grandson’s mediation towards education and support to the couple.
The case presented here demonstrates that in an inclu-sive environment, social opportunities can occur and issues such as marriage and reproduction in DS should be evalu-ated in the context of the family.
�� �������������
The authors declare that they have no conflict of interest.
����������
1. Down JL. Observations on ethnic classification of idiots. Lon-don Hospital Clinical Lectures and Reports.1886;3:259-62.
2. Book JA, Fraccaro M, Lindsten J. Cytogenetical observations in mongolism. Acta Paediatrica.1959;48:453-68.
3. Penrose LS, Ellis JR, Delhanty JD. Chromosomal translocations in mongolism and in normal relatives. Lancet.1960;2:409-10.
4. Polani PE, Briggs JH, Ford CE, Clarke CM, Berg JM. A mongol girl with 46 chromosomes. Lancet.1960;1:721-24.
5. Húlten MA, Patel S, Jonasson J, Iwarsson E. On the origin of the maternal age effect in trisomy 21 Down syndrome: the oocyte mosaicism selection model. Reproduction. 2010;139:1-9.
6. Moreira LMA, El-Hani CN, Gusmão FAF. Down syndrome and its pathogenesis: considerations about genetic determinism. Rev Bras Psiquiatr. 2000;22:96-9.
7. Ringman JM, Rao PN, Lu PH, Cederbaum S. Mosaicism for tri-somy 21 in a patient with young-onset dementia. Arch Neurol. 2008;65:412-5.
8. Papavassiliou P, York TP, Gursoy N, Hill G, Nicely LV, Sunda- ram U, et al. The phenotype of persons having mosaicism for trisomy 21/Down syndrome reflects the percentage of trisomic cells present in different tissues. Am J Med Genet Part A. (2009); 149:573-83.
9. Nader S. Preparing the inclusion way: dissolving myths and prejudices in relation to individuals with Down syndrome. Rev Bras Ed. Esp. 2003;9:57-78.
10. Carvalho-Freitas MN, Marques AL. A diversidade através da história: a inserção no trabalho de pessoas com deficiência, O&S. 2007;14:59-78.
11. Brown RI. Partnership and marriage in Down syndrome. Downs Syndr Res Pract. 1996;4:96-9.
12. Denholm C. Developmental needs of adolescents: Application to adolescents with Down syndrome. The 1992 National Con-ference of the Canadian Down syndrome Society. Canadian Down syndrome Society: University of Calgary, 1992.
13. Conod L, Sarvais L. Sexual life in subjects with intellectual dis-ability. Salud Pública de México. 2008;50:230-8.
14. Manfroi C. A filha. Down em alto astral. Blumenau: Nova Letra; 2012.
15. Schiavo MR. Síndrome de Down. Brasília (DF): Fundação Bra-sileira das Associações de Síndrome de Down. 1999.
16. Johannisson R, Groop A, Winking H, Coerdt W, Rehder H, Schwinger E. Down’s syndrome in the male. Reproductive pa-thology and meiotic studies. Hum Genet. 1983;63:132-8.
17. Goldstein H. Menarche menstruation, sexual relations and con-traception of adolescent females with Down syndrome. Eur J Obstet Reprod Biol. 1988;27:343-9.
18. Bovicelli L, Orsini LF, Rizzo N, Montacuti V, Bacchetta M. Repro-duction in down syndrome. Obstet Gynecol. 1982;59(suppl): 135-75.
19. Moreira LMA, Gusmão FAF. Genetic and social aspects of Down syndrome subjects’ sexuality. Rev Bras Psiquiatr. 2002;24:94-9.
Figure 2 Segregation of chromosome 21 and probabilities of trisomic (A) and normal (B) zygotes in reproducing woman with chro-mosome mosaicism.
Trisomy 21 Normal numberof chromosomes Normal number of chromosomes
50%
50%
100%
GAMETES GAMETES
X X
A B

Rev Med Int Sindr Down. 2013;17(3):43-45
1138-011X/$ - see front matter © 2013 Fundació Catalana Síndrome de Down. Published by Elsevier España, S.L. All rights reserved.
www.fcsd.org
INTERNATIONALMEDICAL REVIEW
ON DOWN’S SYNDROMEwww.elsevier.es/sd
CLINICS AND PRACTICE
Trajectory and challenges of the Leisure Service: ��������������
C. Herreros a,* and M.J. Miquel b
a Coordinator of the Servei d’Oci de la Fundació Catalana Síndrome de Downb Professor specialist in Therapeutic Pedagogy and former Coordinator of the Servei d’Oci de la Fundació Catalana Síndrome de Down
Received on September 16, 2013; accepted on November 14, 2013
KEYWORDSLeisure; Down’s syndrome;Intellectual disability;Inclusion;Quality of life;Social relationships
AbstractWhenever there are new challenges it is important to stop to consider their priorities. This year the Leisure Service of the Catalan Down’s Syndrome Foundation celebrates its first 25 years. Thus, a short review of the history of the Service will be presented and what this leisure concept means. It will also comment on how the individuals and those around them feel when the former want to start enjoying their free time, and what the professional propose to do as a response. The challenges and new concepts of the Service will be presented at the end of this article.
PALABRAS CLAVEOcio;Síndrome de Down;Discapacidad intelectual;Inclusión;Calidad de vida;Relación social
�������������������������������������������������!��
ResumenCon tal de plantear nuevos retos es importante detenerse y conocer su precedencia. El Servicio de Ocio de la Fundación Catalana Síndrome de Down este año cumple sus prime-ros 25 años. Por lo tanto, se hará un breve repaso de la historia del Servicio y de cómo este entiende el concepto ocio. Además, se comentará cómo se siente la persona y su entorno cuando esta quiere empezar a disfrutar de su tiempo libre y qué fórmula propo-nen los profesionales como respuesta. Los retos y los nuevos proyectos del Servicio ocu-parán el final de este artículo.
*Author for correspondence.E-mail: [email protected] (C. Herreros).

44 C. Herreros et al
The Leisure Service of the Catalan Down’s Syndrome Foun-dation will be 25 years old this year. The Young Independ-ence Program pilot project (Programa de Autonomía Joven [PAJ]) set the standards. The young people who took part were those who asked for time to be able to discuss, pro-pose, organise, and prepare leisure activities. That is to say, they wanted leisure time, without commitments or re-sponsibilities, in order to be able to relate with, choose and enjoy the activity carried out.
The healthcare professionals started to introduce the Young Persons Space in 1989, a meeting point for the 12 young people of the program. Three Friends Groups were already formed in 1992, and in 1996, they made their first summer trips.
At the moment, the number of people interested in be-coming part of the Friends Groups and in travelling has not stopped increasing. There are currently 125 people active in the Leisure Service. Each one of them goes out at the weekend with their Friends Group to carry out activities chosen amongst them. They also have the option of going out for a weekend with the whole group, and when it comes to holiday time, they can have meetings to decide when and where to go.
The Service has also taken part in many congresses, con-ferences, meetings, chats and training sessions, where the theoretical perspective adopted has been presented, as well as how it has been updated over the years.
Of the many existing definitions of leisure, the Service has opted for the one proposed by Trilla (1991), who stated that “leisure, regardless of what the activity is, is a useful way of using free time by means of a chosen task, carried out freely and with a purpose, and by doing it when there is satisfaction and pleasure for the individual”.
Guirao and Vega (2012) completed this definition by stat-ing that leisure plays such an essential role in our lives that we cannot imagine being without it because: 1) it is a basic human right that helps the individual to develop; 2) it gives quality of life to these individuals so that they can live in a positive and rewarding way, as it leads to both physical and emotional well-being; and 3) it is an essential human expe-rience to be engaged in leisure activities influences all walks of life, on being in touch with very personal questions such as interests, hobbies, desires, etc.
Thus, leisure has been identified as an essential compo-nent of quality of life and, as such, we understand it in the same context of leisure in the life of people without a dis-ability.
When individuals with Down’s syndrome first show an in-terest in enjoying their free time, we must be aware of the feelings and emotions that it awakens, both in the individu-als themselves and in their surroundings.
It opens up a new world for the individuals, full of un-known experiences and sensations: to go out, meet with friends, carry out activities that they like… And all the ef-fort and responsibility that this brings: to have to arrive at the agreed time and to call if they are going to be late, or not going, to be responsible for money and personal docu-ments, etc.
It also opens a completely new way of life for the family, since they must provide the necessary support for the indi-vidual, but without invading their space. To know about the
activity that they will be carrying out that weekend by talk-ing to their family and not the reference group, to advise them and guide them in decisions as regards trips and ac-tivities, but not decide for them, to give them power over decisions so that, gradually, they will be more independent individuals. These are some of the examples that the family have to adjust to, so that they continue growing up and ask-ing for their own space.
To confront these new situations associated with leisure time, is necessary and welcome since, as has been men-tioned before, it is a time for connecting with other envi-ronments of life and is directly related with the quality of life of the individual.
The Leisure Service team are currently using a formula that includes the family and the individuals themselves to experience this entire process as an enriching one.
This formula consists of creating a comfort zone. This means that the person feels part of a group, which may be reflected in the other and feels accepted. This feeling will increase their enthusiasm and motivation to take part in the activities. Also, the fact of having a reference, a sup-port person, who is seen as a model for both the group and the family will help to eliminate a large part of the suffer-ing and the risk that the families and the participants them-selves may feel.
The formula is rounded off with continuous communica-tion and the alliance required by the three parties and with the constant message that the people responsible for choos-ing the activities are those who will enjoy them, thus gen-erating real pleasure and satisfaction to take part in them.
The stability of always forming part of a group, of the organisation, and of the methodology used has led to the continuity of the Leisure Service for all these years. Now is the time to expand the formula to offer more possibilities at an individual level and, above all, to involve society.
The view of the Service is gradually transforming to face new challenges. If the same experiences and situations set the route to follow 25 years ago, it is the same now, to-gether with the concept promoted by Guirao y Vega (2012): inclusive leisure, which is no more than including people with disabilities in the leisure, cultural, sport and recreation services of the community like the citizens that they are.
The proposal of these authors is a challenge for every-one. A challenge that must be promoted every day and needs preliminary work by all the parties involved.
The Leisure Service currently offers two programs: that of the Friends Group and that of tourism. In the first, there are a total of 13 groups, of which 11 meet every weekend, and the other two, which are the “young people’s spaces”, meet every two weeks. These groups are organised by age and interests. In the second program, trips are offered dur-ing holiday periods: summer and, this year, also Christmas. There is also the option of going out for a weekend.
Therefore, the individuals always carry out the activity and/or the trip in a group. The preliminary work for an in-clusive leisure is to take more note of the point of view of the individuals, that is, to actively listen to their interests, not only that of the whole group, and to help them to make it a reality.
The idea is to regularly in the program of group of friends offer the individual the possibility of choosing the activity

Trajectory and challenges of the Leisure Service: The first 25 years 45
independently from the group, in accordance with their motivations and interest. Furthermore, they will share this leisure space with individuals from other groups who will also be motivated with expectations to enjoy their choice.
This is a project that will be started in the next few months, and is compatible with the rest of it, since to set it in motion does not involve leaving everything else that is being done. It involves expanding the formula and introduc-ing other variables. It involves increasing the comfort and safety zone, both for the family and the individual. It in-volves everyone.
References
– Cuenca M. Temas de pedagogía de ocio. Bilbao: Univ de Deusto; 1995.
– Guirao I, Vega, B. Servicio de Ocio Inclusivo. Madrid: FEAPS; 2012.– Miquel MJ. Ocio y discapacidad. Rev Med Int Sindr Down. 2001;
5:10-13.– Trilla J. Revisión de los conceptos de tiempo libre y ocio. El caso
infantil. Infancia y Sociedad. 1991;8:17-31.

The purpose of SD, INTERNATIONAL MEDICAL JOURNAL ON DOWN’S SYNDROME is, on the one hand, to gather current knowledge on the medical aspects of Down’s Syndrome and make a continuous review and update, from the most promising advances in basic sciences, such as molecular biology and genetics, to daily clinical practice; and on the other, to look at those psycho-pedagogic aspects which, due to their relationship with the medical field may be of practical interest for general and specialist paediatricians associated with Down’s Syndrome. SD will consider for publication clinical or research works associated with Down’s Syndrome and all its branches.
Journal SectionsOriginals. Research work, preferably prospective, on the epidemiol-ogy, aetiology, pathophysiology, anatomical pathology, clinical, and diagnostic or therapeutic methods. The recommended designs are analytical type, in the form of cross-sectional surveys, case and con-trol studies, cohort studies, and controlled trials. Maximum length: 25,000 characters including spaces (including a structured abstract), a maximum of 10 tables and/or figures. It is recommended that there are no more than 6 signatories, and the number of literature refer-ences should not exceed 20.
Reviews. Review or reports on diverse aspects. Maximum length: 25,000 characters including spaces (including a structured abstract), a maximum of 10 tables and/or figures. It is recommended that there are no more than 6 signatories, and the number of literature refer-ences should not exceed 20.
Clinical cases. Maximum length: 8,000 characters including spaces (in-cluding abstract) and up to 4 tables and/or figures. The number of signa-tories must not exceed 6 and literature references no more than 8.
Special articles. Articles dealing with medical or psychological aspects of Down syndrome with opinions on relevant aspects of the syndrome, written by recognized experts and often presented at na-tional or international conferences or meetings. Maximum length: 25,000 spaces, including structured abstract.
Clinics and practice. Contributions from an practical perspective that, together with medical aspects, may improve the care of people with Down’s Syndrome: psychopedagogical, bioethics, legal, complementary, etc.
Maximum length 12,000 characters including spaces (including ab-stract) and up to 4 tables and/or figures. The number of signatories must not exceed 6 and literature references no more than 10.
Letters to the Editor. Short communications by readers concern-ing medical or psycho-pedagogic aspects of Down’s Syndrome, or on subjects published in the journal. They will have a maximum of 750 words and may be accompanied by 1 figure or table, and with a maxi-mum of 5 literature references. Whenever requested, or where ap-propriate, they will always be answered or commented upon by the Editorial Committee.
Presentation and structure of articlesThey will be adapted to the recommendations of the International Committee of Medical Journal Editors on the Uniform Requirements for Biomedical Journals (Vancouver style).
They must be submitted in digital form, double-spaced and with suf-ficient margins, always with the pages number consecutively, via the Journal Manuscript Management System (http://ees.elsevier.com/sd).
It will state: the title of the work, full name and surname(s) of all the signatories; full name and address of the work centre; address for correspondence (e-mail).
It will clearly state if part of the work has been presented at any meeting, symposium or congress, if has been awarded a prize or if has received any funding.
Abstract. Works published in the original works or review sections, clinical cases and psycho-pedagogic advances sections, must be ac-companied by an abstract of not more than 250 words in the presen-tation language and in English, preceded by the title of the work in the same languages. They should not contain data that are not found in the text. It will have up to 5 key words, in accordance with Index Medicus. In the case of Originals, the abstract will be structured.
Writing. It is recommended that the writing is in the impersonal. The works should be clearly divided into sections. Originals into: Intro-duction, Material or Patients and Methods, Results, and Discussion.
Clinical Cases into: Introduction, Clinical Observation, and Discus-sion. The text of Psychopedagogic Advances, after the Abstract, will be written freely by the author(s).
Acknowledgements. Contributions that require an acknowledge-ment must be mentioned briefly, specifying the type of help – techni-cal or material – where applicable.
Bibliography. The references of Original and Clinical Case articles will be numbered in the text in order of appearance and in parenthe-ses, and set out in a separate page, following the Vancouver regula-tions. In the Psychopedagogic Advances and in the Special articles, the references will not be numbered and will be set out on a separate page, in alphabetical order. In all cases, any quote mentioned in the text must be clearly referenced in the bibliography.
Tables. On separate pages, and numbered with Arabic numerals. They must be mentioned in the text. They will have a title in the up-per part. If there are abbreviations, they must be explained at the foot of the table. Repetitions between the tables, figures and text should be avoided.
Figures. These are essential for a better understanding of the text. They will be numbered in order of appearance and with Arabic nu-merals. The footnotes will be set out on a separate page. Graphs, drawings and photographs will be referenced as figures in consecu-tive order.
If photographs of people are used, these must not be identifiable, or must be accompanied by a permission for their use in writing. The format should preferably be, JPG or TIFF.
Acronyms, abbreviations, symbols and units. A minimum number of acronyms is desirable. In all cases, they must be defined when they first appear in the text. In haematology or biochemistry measure-ments the metric system in accordance with the international units system (SI) will be used.
Submission of OriginalsThe article will be sent with a cover letter in which it will state:
Originality of the material: a declaration by all the authors that the article is original and has not, wholly or any of its parts, been published or submitted previously, or whether it is subject to consid-eration by any other publication.
Conflict of interests: the authors must clearly declare if there is any funding or any other aspect that could lead to a conflict of interests.
Authorship: a declaration by all the authors that they have read and approved the manuscript and the requirements of authorship have been duly met.
Informed Consent: a declaration that informed consent has been obtained from the patients.
Research with Humans: the authors must indicate if the proce-dures and methods used are adapted to the ethical standards of the current Ethics Committee responsible in their institution for experi-ments on humans and in accordance with the Helsinki Declaration of the World Medical Association (1964 and subsequent versions http://www.wma.net/e/policy/b3.htm).
Research with animals: the authors must clearly indicated that the studies have been performed following the recommendations and policies on animal well-being in accordance with authorised guide-lines, such as the ILAR Guide for the Care and Use of Laboratory Ani-mals (1996 and subsequent versions) by the Institute of Laboratory Animal Research, Commission on Life Sciences, National Research Council (http://www.nap.edu/catalog/5140.html).
A proof of receipt of the originals will be given and you will be informed of its acceptance and possible publication date. When the article is in print, the author will receive proof copies to correct, which must be returned within the 48 hours following their receipt.
The Editors could suggest modifications to the text when they be-lieve they are necessary, and also may reject the publication of works which they consider inadequate.
All works accepted will become the property of SD, and may not be partially or wholly reproduced without permission from the pub-lisher. When a work is published, the author transfers, the rights of public reproduction, distribution, translation and communication (by any medium or support) to Elsevier España, S.L.
Instructions to Authors SDINTERNATIONAL MEDICAL REVIEW ON DOWN'S SYNDROME