Embed Size (px)
Citation preview
Issues in Early Medical Abortion
Mitchell Creinin, MDProfessor
Director of Gynecologic Specialties Director of Family Planning
University of PittsburghPittsburgh, PA
USA
Objectives
• Very early surgical abortion• Home use of misoprostol• Shortening the interval between
mifepristone and misoprostol• Follow-up intervals shorter than two
weeks
Medical Abortion
Early pregnancy termination (usually before 9 weeks gestation) performed without primary surgical intervention and resulting from the use of abortion-inducing medications

Early surgical abortion
• Manual vacuum aspirator with locking valve
• Portable and reusable• Generates vacuum
equivalent to electric pump
• Efficacy same as electric vacuum (98–99%)
• Semi-flexible plastic cannula
MVA
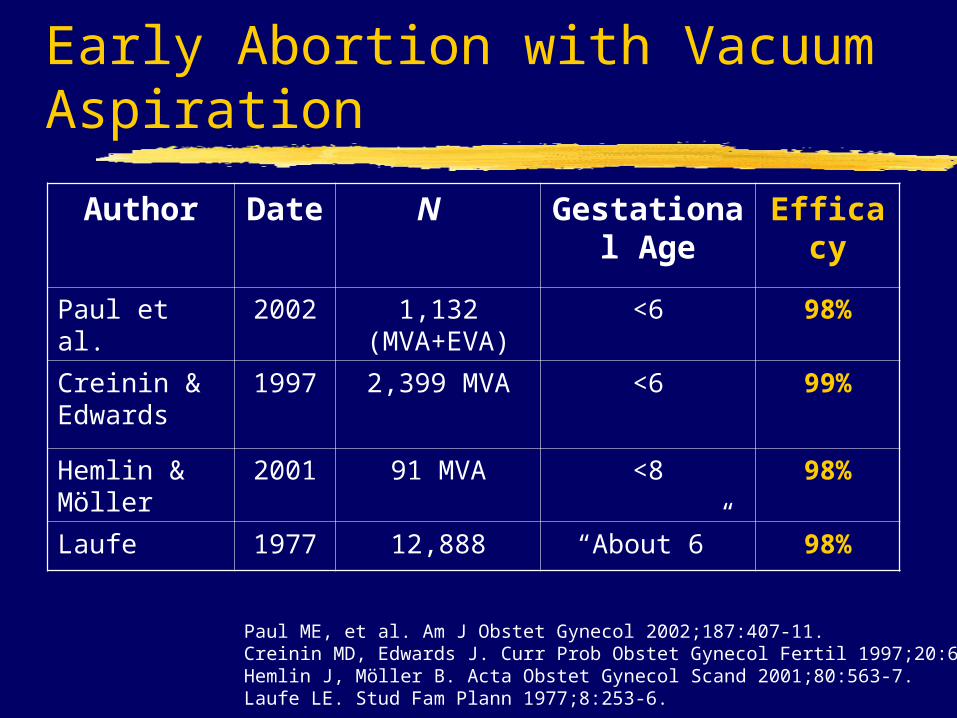
Early Abortion with Vacuum Aspiration
Author Date
N Gestational Age
Efficacy
Paul et al. 2002 1,132 (MVA+EVA)
<6 98%
Creinin & Edwards
1997 2,399 MVA <6 99%
Hemlin & Möller
2001 91 MVA <8 98%
Laufe 1977 12,888 “About 6” 98%
Paul ME, et al. Am J Obstet Gynecol 2002;187:407-11.Creinin MD, Edwards J. Curr Prob Obstet Gynecol Fertil 1997;20:6-32.Hemlin J, Möller B. Acta Obstet Gynecol Scand 2001;80:563-7. Laufe LE. Stud Fam Plann 1977;8:253-6.

Early Abortion with MVA
Methods• 2,399 MVA procedures• <6 weeks LMP, high sens UCG , vaginal sono• Meticulous inspection of products of conception
immediately after MVAResults• 99.2% effective in terminating pregnancy• 6 repeat aspirations (0.25%)• 14 ectopic pregnancies (0.6%) diagnosed &
treated
Creinin MD, Edwards J. Curr Prob Obstet Gynecol Fertil 1997;20:6-32.
Mifepristone abortion
Can we provide this regimen in an easier fashion and with less cost?
Variations:• mifepristone dose• non-oral misoprostol• gestational age limits• timing of misoprostol• easier follow-up
go together
- dependent on route
Objectives
• Very early surgical abortion• Home use of misoprostol• Shortening the interval between
mifepristone and misoprostol• Follow-up intervals shorter than two
weeks
Home use of misoprostol
•Majority of trials in North America• High acceptability• High efficacy
•Allowed in the regulatory labeling for mifepristone in the U.S.
•Standard of care in North America
Home use of misoprostol
• Early studies of mifepristone and vaginal misoprostol in U.S.• Women allowed choice of returning• Only 3 (1.9%) of 158 women asked the
clinician to place the misoprostol. • Initial follow-up studies in the U.S.
• >4300 women with home use of vaginal misoprostol
• 90% home use acceptable; no difference by • prior abortion experience • gestational age• time between MIF and MIS (1, 2 or 3 days)
Schaff et al. Contraception 1999;59:1-6.Schaff et al. Contraception 2000;61:41-6.Schaff et al. JAMA 2000;284:1948-53 .
Home use of misoprostol
• Adverse events in the hours after MIS• 4/4365 women (0.1%) had emergencies:
• Two emergent aspiration for heavy bleeding• neither required a blood transfusion.
• One vasovagal reaction to cramping • treated with intravenous fluids.
• One syncopal episode while bleeding • fell and broke her nose.
Schaff et al. Contraception 1999;59:1-6.Schaff et al. Contraception 2000;61:41-6.Schaff et al. JAMA 2000;284:1948-53 .

Home use in Europe
• U.K.• 49 women up to 56 days • Lived within 12 miles of facility• Sublingual MIS at home• Contacted at 4 hour intervals by RN• 98% -- no trouble with the regimen
(1 woman came to hospital after MIS)• 93% -- would use it at home again
Hamoda et al. J Fam Plann Reprod Health Care 2005;31:189-92.

Home use in Europe
• Sweden and France• 130 women up to 49 days • oral MIS at home• 98% -- no trouble with the regimen • 98% -- would use it at home again
• In 2004, Sweden changed its regulatory guidelines to allow medical abortion at home up to 63 days gestation.
Fiala et al. Contraception 2004;70:387-92.Clark et al. Eur J Contracept Reprod Health Care 2005;10:184-91.
Objectives
• Very early surgical abortion• Home use of misoprostol• Shortening the interval between
mifepristone and misoprostol• Follow-up intervals shorter than two
weeks
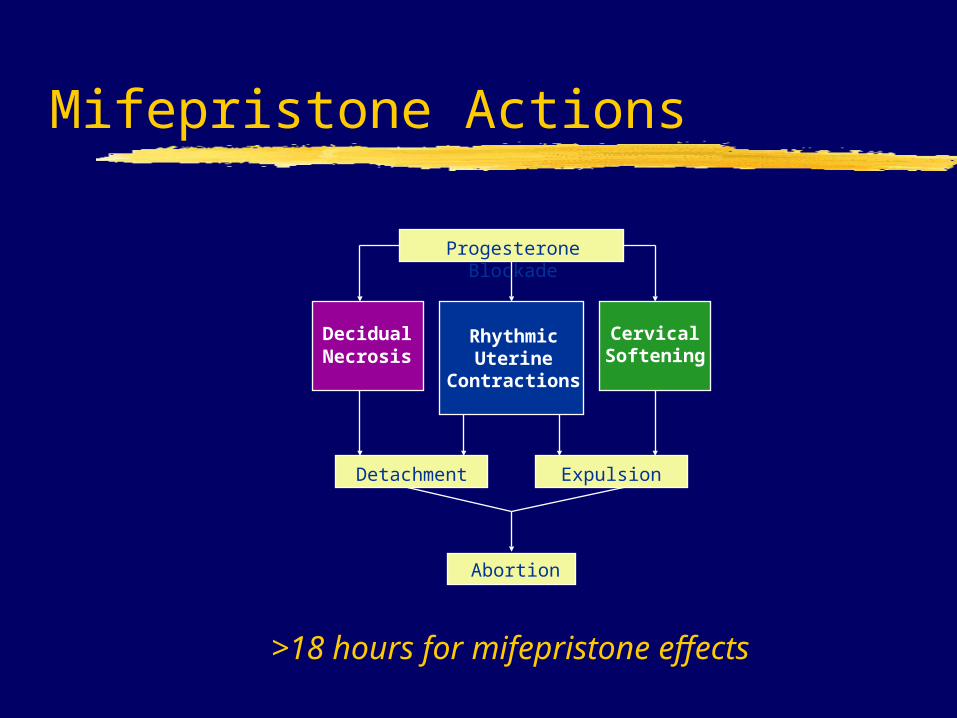
Mifepristone Actions
RhythmicUterine
Contractions
Progesterone Blockade
DecidualNecrosis
CervicalSoftening
Detachment Expulsion
Abortion
>18 hours for mifepristone effects
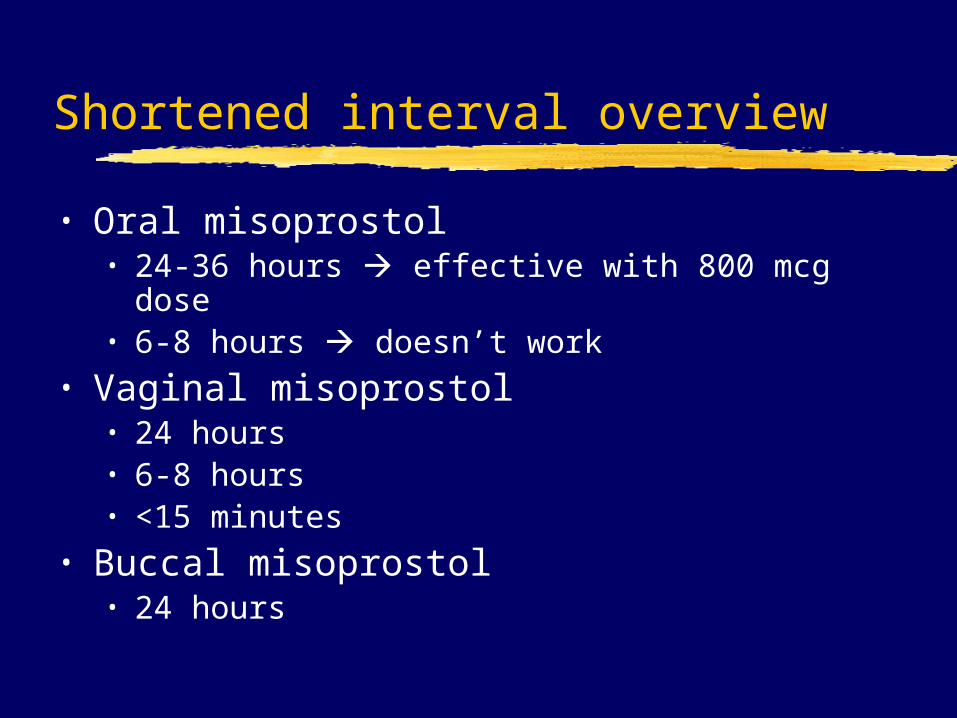
Shortened interval overview
• Oral misoprostol• 24-36 hours effective with 800 mcg dose• 6-8 hours doesn’t work
• Vaginal misoprostol• 24 hours• 6-8 hours• <15 minutes
• Buccal misoprostol• 24 hours

Timing of Misoprostol Dosing
• 2,255 women <56 days gestation• Mifepristone 200 mg PO, misoprostol 800
mcg PV • Interval randomized 24, 48 or 72 hours• Complete medical abortion
• 98% (95% CI 97, 99%) in the 24 hour group;• 98% (95% CI 97, 99%) in the 48 hour group;• 96% (95% CI 95, 97%) in the 72 hour group.
• Time waiting for expulsion acceptable• 86% in the 24 hour group;• 79% in the 48 hour group;• 76% in the 72 hour group (p=0.0001).
Schaff EA et al. JAMA 2000;284:1948-53.

Medical abortion in One Day
• 1,080 women enrolled at 4 centers (4/02 - 6/03)
• Women received mifepristone 200 mg followed• 6 to 8 hours later OR• 23 to 25 hours later
by misoprostol 800 mcg vaginally• Follow-up 7 (+ 1) days and 14 (+ 2) days after
mifepristone• Repeat misoprostol dose at first follow-up if no
expulsion• Follow-up phone call 5 weeks after
mifepristoneCreinin MD, et al. Obstet Gynecol 2004;103:851-9.

Abortion outcome (%)
23-25 hours 6-8 hours(n=531) (n=525)
Complete abortionTOTAL 98 (97, 99) 96 (94, 97)with 1 dose misoprostol 97 (95, 98) 95 (93, 97)
<49 days gestation 98 (96, 100) 97 (94, 99) 50-56 days gestation 98 (94, 99) 94 (89, 98)57-63 days gestation 98 (94, 100) 95 (90, 98)
Creinin MD, et al. Obstet Gynecol 2004;103:851-9.

Medical Abortion at the Same Time
• 1,128 women enrolled at 4 centers (4/04 – 5/06)
• Women received mifepristone 200 mg followed• within 15 minutes OR• 23 to 25 hours later
by misoprostol 800 mcg vaginally• Follow-up 7 (+ 1) days and 14 (+ 2) days after
mifepristone• Repeat misoprostol dose at first follow-up if no
expulsion• Follow-up phone call 5 weeks after mifepristone
Creinin MD, et al. Obstet Gynecol 2007;109:885-94.

Abortion outcome (%)
23-25 hours witihin 15 min(n=546) (n=554)
Complete abortionTOTAL 97 (95, 98) 95 (93, 97)with 1 dose misoprostol 94 (92, 96) 91 (88, 93)
<49 days gestation 98 (96, 99) 96 (92, 98) 50-56 days gestation 95 (91, 98) 94 (90, 97)57-63 days gestation 97 (92, 99) 95 (90, 98)
Creinin MD, et al. Obstet Gynecol 2007;109:885-94.

Questioning results
• UK study• Randomized trial• 450 women up to 63 days gestation
• 6 hour interval (n=225) stayed in clinic• 36-48 hours (n=225) went home and
returned for misoprostol• Complete abortion rates
• 89% in 6 hour group• 96% in 36-48 hour group
Guest J et al. BJOG 2007;114:207-15 .
Why a difference?
• Smaller study (450 vs. 1056)• Ultrasound use
• U.S. study • Sonography at 7 days• Assess if sac present• If present, repeat dose of misoprostol and return in one
week.• U.K. study
• Sonography at 2-7 days • Assess for a gestational sac and also for evidence of
“nonviable products of conception.” • If present, could have a suction aspiration or more
misoprostol; however, women who wanted another dose of misoprostol were required to remain under observation for 4-6 hours with a follow-up in one week.
Creinin MD et al. Obstet Gynecol 2004;103:851-9.Guest J et al. BJOG 2007;114:207-15 .
Why a difference?
• Protocol biases results• success rate with a single dose of MIS in 6-8 h
group • U.S. study = 95%• U.K. study = 79%
• Incomplete abortion rates• U.S. study = 2%• U.K. study = 4%
• Aspiration for persistent sac• U.S. study = 0.6%• U.K. study = 4%
• Increased interventions in U.K. women b/o management schema
Creinin MD et al. Obstet Gynecol 2004;103:851-9.Guest J et al. BJOG 2007;114:207-15 .
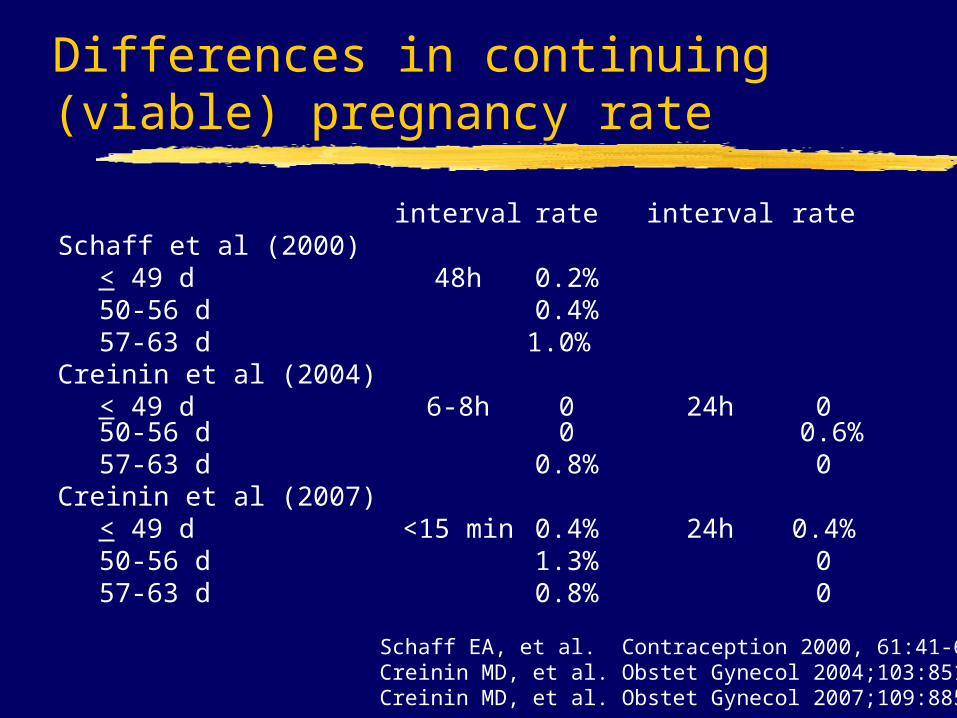
Differences in continuing (viable) pregnancy rate
interval rate interval rateSchaff et al (2000)
< 49 d 48h 0.2%50-56 d 0.4%57-63 d 1.0%
Creinin et al (2004)< 49 d 6-8h 0 24h 050-56 d 0 0.6%57-63 d 0.8% 0
Creinin et al (2007)< 49 d <15 min 0.4% 24h 0.4%50-56 d 1.3% 057-63 d 0.8% 0
Schaff EA, et al. Contraception 2000, 61:41-6. Creinin MD, et al. Obstet Gynecol 2004;103:851-9Creinin MD, et al. Obstet Gynecol 2007;109:885-94.

Mifepristone Actions
RhythmicUterine
Contractions
Progesterone Blockade
DecidualNecrosis
CervicalSoftening
Detachment Expulsion
Abortion
WHAT REALLY IS IMPORTANT?

Objectives
• Very early surgical abortion• Home use of misoprostol• Shortening the interval between
mifepristone and misoprostol• Follow-up intervals shorter than two
weeks
Shorter Follow-up Intervals
• Most studies include follow-up at 1-7 days following treatment
• Earlier follow-up with transvaginal ultrasound
compare to standard regimen
Follow-up
No studies validate this practice• Does earlier evaluation result in high
rates of later intervention?• What is the best way to use
ultrasound?
Follow-up
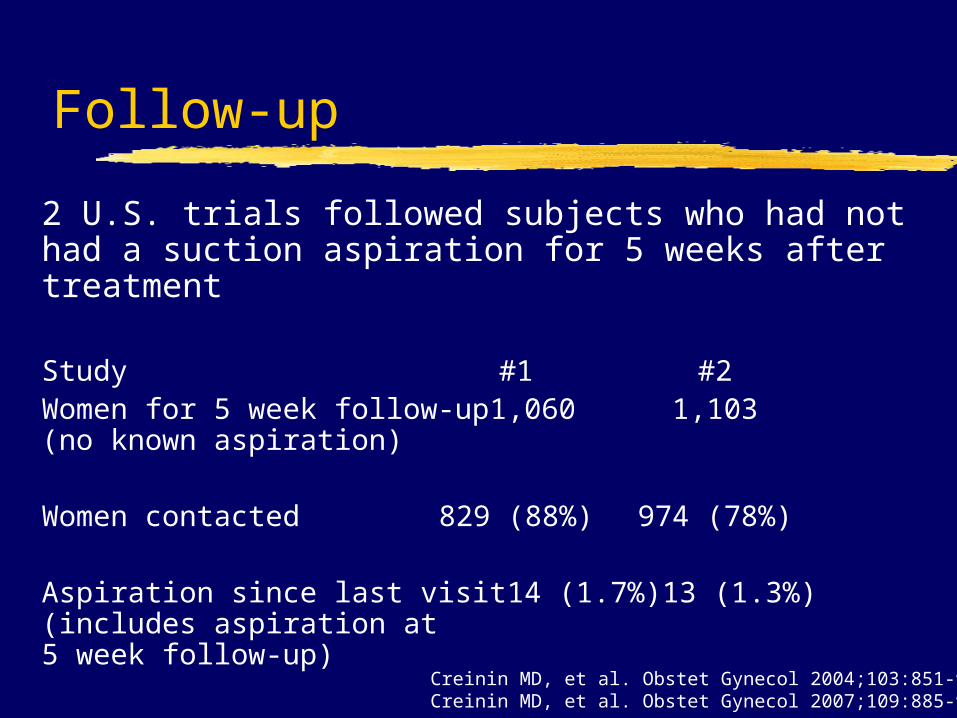
2 U.S. trials followed subjects who had not had a suction aspiration for 5 weeks after treatment
Study #1 #2Women for 5 week follow-up 1,060 1,103(no known aspiration)
Women contacted 829 (88%) 974 (78%)
Aspiration since last visit 14 (1.7%) 13 (1.3%)(includes aspiration at5 week follow-up)
Creinin MD, et al. Obstet Gynecol 2004;103:851-9.Creinin MD, et al. Obstet Gynecol 2007;109:885-94.
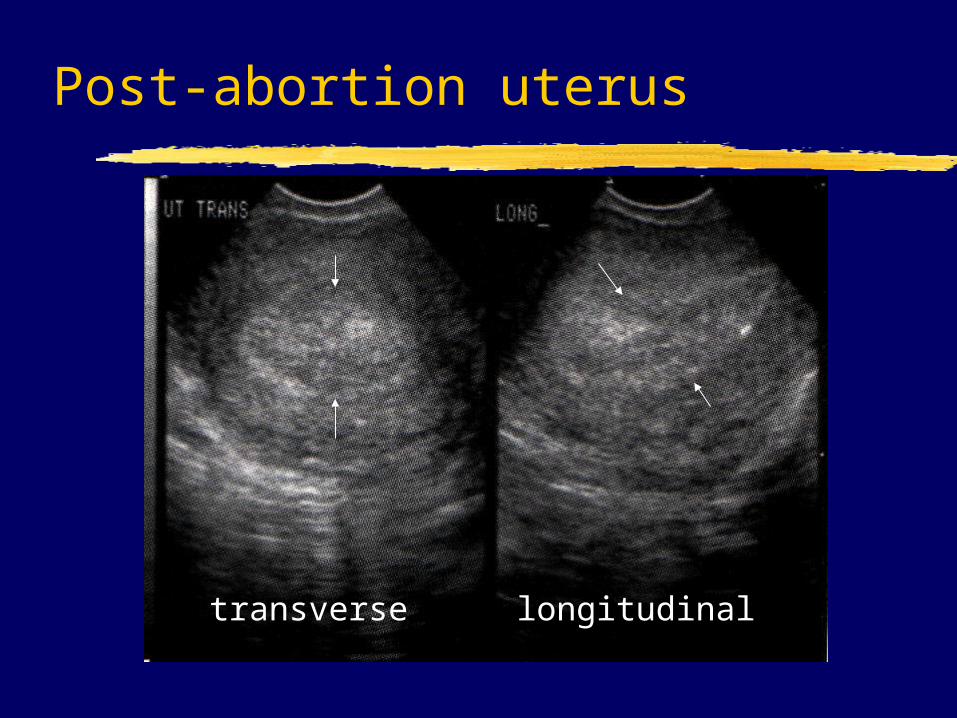
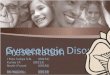
Post-abortion uterus
transverse longitudinal
Is follow-up exam necessary?
• Is the ultrasound examination necessary to evaluate for expulsion?
• Is a clinical examination necessary to evaluate for expulsion?
• Clinician and patient both feel pregnancy is expelled:• Happens in 95% of treatments• They are right 99% of time
Rossi et al. Contraception 2004;70:313-7.
Mifepristone regimens
Acceptable alternatives to theAcceptable alternatives to theStandard RegimenStandard Regimen
• Mifepristone 200 mg mifepristone• Home administration of misoprostol• Misoprostol 800 mcg vaginally through 63
days gestation 0-72 hours after the mifepristone
• Misoprostol 800 mcg buccally through 63 days gestation 24-48 hours after the mifepristone
• Follow-up within 1 week using ultrasound

Etienne-Emile Baulieu
"Choice is freedom, science cannot and must not dictate our beliefs. But science can provide choices.”
1991
Mifepristone and Buccal Misoprostol
• Mifepristone 200 mg• Misoprostol 800 mcg buccally or
orally 1-2 days later• Follow-up 7-14 days after
misoprostol• If no expulsion, aspiration or additional
misoprostol
• 966 women up to 63 days gestationDzuba et al (submitted for publication)
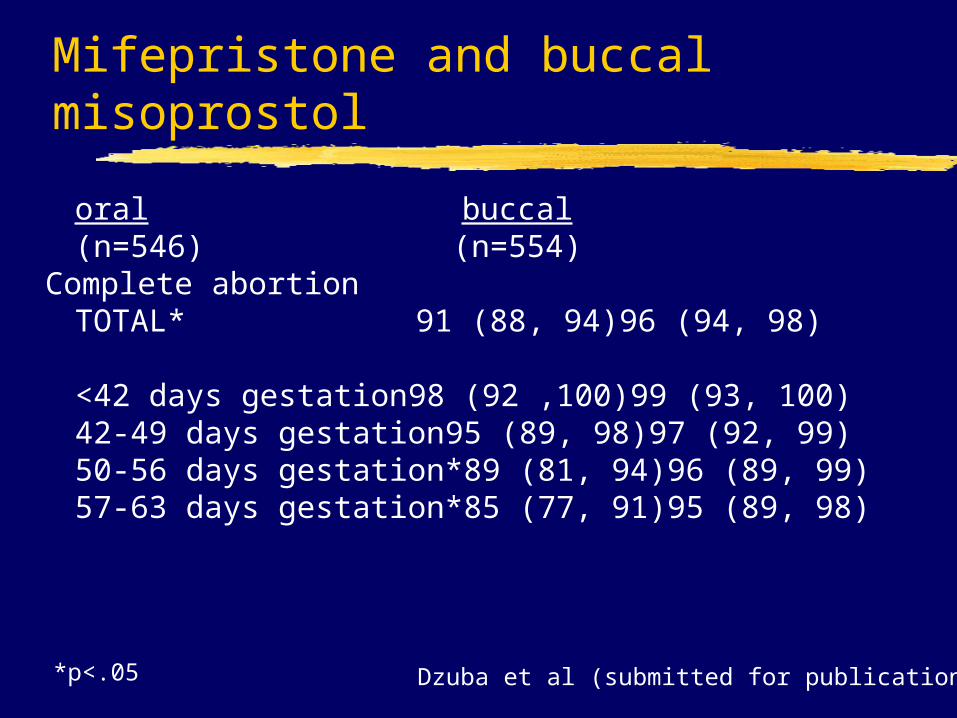
Mifepristone and buccal misoprostol
oral buccal(n=546) (n=554)
Complete abortionTOTAL* 91 (88, 94) 96 (94, 98)
<42 days gestation 98 (92 ,100) 99 (93, 100)42-49 days gestation 95 (89, 98) 97 (92, 99) 50-56 days gestation* 89 (81, 94) 96 (89, 99)57-63 days gestation* 85 (77, 91) 95 (89, 98)
Dzuba et al (submitted for publication) *p<.05
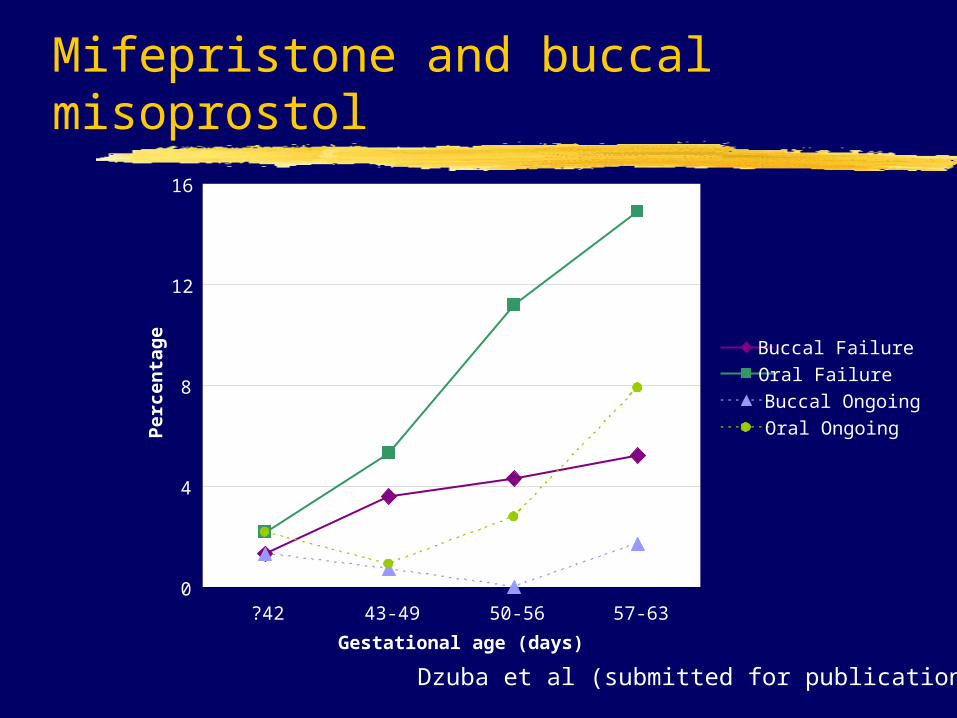
Mifepristone and buccal misoprostol
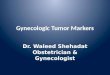
0
4
8
12
16
?42 43-49 50-56 57-63
Gestational age (days)
Per
cen
tag
e
Buccal Failure
Oral Failure
Buccal Ongoing
Oral Ongoing
Dzuba et al (submitted for publication)
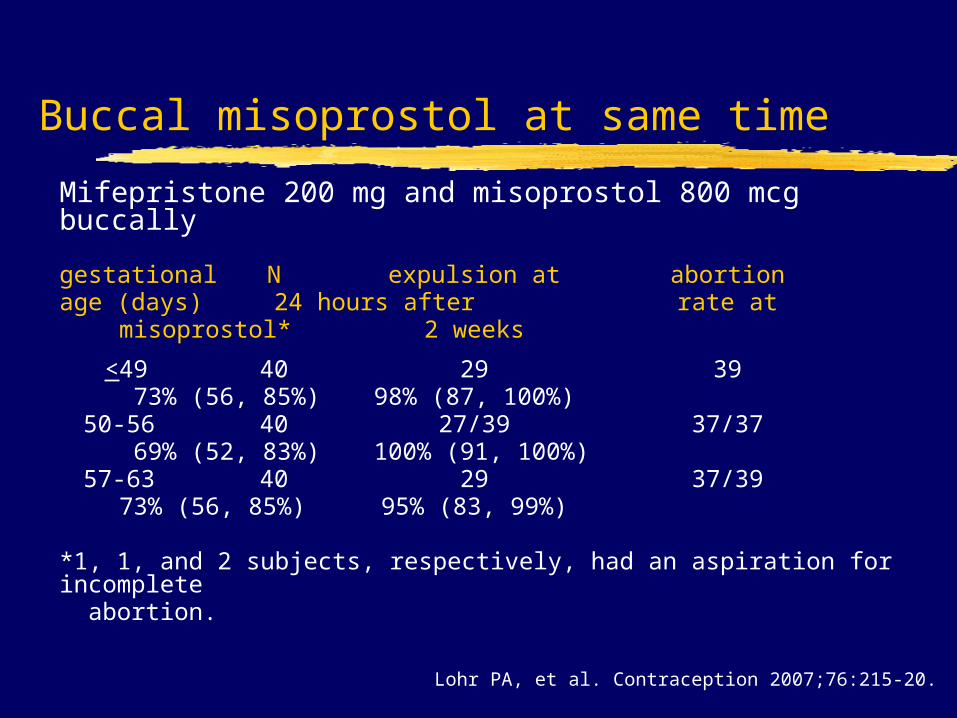
Buccal misoprostol at same time
Mifepristone 200 mg and misoprostol 800 mcg buccally
gestational N expulsion at abortionage (days) 24 hours after rate at
misoprostol* 2 weeks
<49 40 29 39 73% (56, 85%) 98% (87, 100%)
50-56 40 27/39 37/37 69% (52, 83%) 100% (91, 100%)
57-63 40 29 37/3973% (56, 85%) 95% (83, 99%)
*1, 1, and 2 subjects, respectively, had an aspiration for incomplete abortion.
Lohr PA, et al. Contraception 2007;76:215-20.
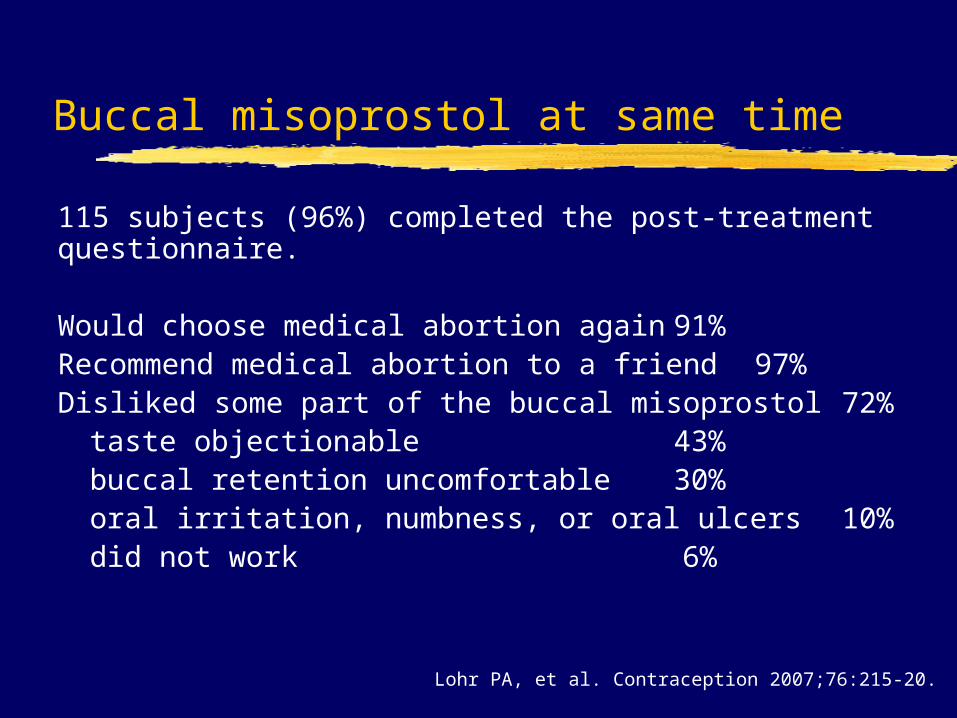
Buccal misoprostol at same time
115 subjects (96%) completed the post-treatment questionnaire.
Would choose medical abortion again 91%Recommend medical abortion to a friend 97%Disliked some part of the buccal misoprostol 72%
taste objectionable 43%buccal retention uncomfortable 30%oral irritation, numbness, or oral ulcers 10%did not work 6%
Lohr PA, et al. Contraception 2007;76:215-20.