Embed Size (px)
Citation preview
TRANSACTIONS OF THE ROYAL SOCIETY OF TROPICAL MEDICINE AND HYGIENE (1994) 88, 107-109 107
lvermectin 400 vglkg: long-term suppression of microfilariae in Bancroftian filariasis
J. P. Moulia-Pelat’, Ph. Glaziou’, L. N. Nguyen’, S. Chanteau’, R. Plichart’, I. Beylie$, P. M. V. Martin’ and J. L. Cartel’ ‘Institut Territorial de Recherches Mddicales Louis Malard&, BP. 30, Papeete, Tahiti, Polynt%e Fraqaise; 2Huehine, Tahiti, Polynksie Fratqaise
Abstract Forty-three Wuchereria bancrofti carriers were given 4 successive semi-annual single doses of ivermectin 100 pgikg (IVER 100). The geometric mean microfilaremia (mf) recurrence percentages, compared to the pre-in- ltial treatment mf level, were 35%, 21%, 17% and 17% at 6, 12, 18 and 24 months respectively. However, the recurrence of mf 6 months after the fourth treatment remained high in 15 individuals, considered as ‘bad responders’. At month 24, the subjects were randomly allocated into 2 groups: the first group was treated with a fifth dose of IVER 100 and the second with a first, single dose of 400 pg/kg of ivermectin (IVER 400). At month 30, the mf recurrence percentage was significantly higher in patients treated with IVER 100 than in those receiving IVER 400 (61% vs. 8%, FYO.05). In the IVER 100 group, 6 of the 8 ‘bad responders’ re- mained ‘bad responders’, whereas only 2 of 7 did so in the IVER 400 group. Only 3 additional patients in the IVER 100 group became consistently amicrofilaraemic, whereas 9 did so in the IVER 400 group. Two ‘good responders’ in the IVER 100 group became ‘bad responders’. A single dose of 400 pg/kg of ivermectin has been demonstrated to be efficient for the treatment of carriers refractory to repeated doses of 100 Kg/kg and to result in better long-term mf suppression. These results suggest a possible effect of 400 yglkg of ivermec- tin on macrofilaria.
Introduction Several trials have indicated that single dose treat-
ments with ivermectin were safe and effective against 1vmDhatic filariasis due to Wuchereria bancrofti (see ~)IA~LO et al., 1987; KUMARASWAMI et al., 1988; CAR- TEL et al., 1992a, 1992b). Ivermectin produced immedi- ate complete amicrofilaraemia at a d&age of 100 pgg/kg GIVER 100). However, 6 months after the drua adminis- fration, reappearen& of microfilaraemia at a-high level was observed in several individuals called ‘fast repopulat- ing’ or ‘bad responders’, whereas sustained reduction was observed in others called ‘slow repopulating’ or ‘good responders’; this reappearance of microfilariae might have been due, among-oiher causes, to insufficient drug dosane (CARTEL et al.. 1993). Recentlv. treatment wit6 a totd d&age of 400 w&kg oiivermecti~(IVER 400) given in success&e doses ;&tied in excellent ‘long-term reduction of microfilaraemia (RICHARDS et al.. 1991: EBERHARD et al., 1992). Furt‘hermore, IVER 460 as a single dose was reported to be safe and effective against W. bancrofti filariasis (CARTEL et al., 1992~). Thus, it was of interest to compare the efficacy of 100 ygikg with that of 400 Kg/kg of ivermectin in 43 carriers of W. ban- crofti previously treated with 4 semi-annual doses of IVER 100. The aim of our study was to compare the course of microfilaraemia following treatment and to assess whether a single dose of IVER 400 would result in consist- ent long-term decrease of microfilaraemia, particularly in ‘bad responders’.
Patients and Methods In June 1990 a trial was implemented in Huahine, one
of the Leeward Islands close to Tahiti, to assess the eff- cacy of repeated doses of IVER 100 given every 6 months for the treatment of W. bancrofti var. pacifica. Forty-six carriers, between 18 and 53 years of age, whose micro- filariae (mf) density was a20 mg/mL, were given 4 suc- cessive single doses of 100 pgikg of ivermectin at inter- vals of 6 months. Three patients were withdrawn from the study: one had taken carbamazine prescribed by his ohvsician for treatment of filariasis hvdrocele and the bth’er 2 had left Huahine.
The geometric mean microfilaraemia recurrence rates (MFR) for the 43 carriers, compared to the pre-initial treatment mf levels, were 35%, 21%, 17% and 17% at 6, 12, 18, and 24 months after treatment was started, re- spectively. However, the MFR 6 months after the fourth treatment remained high in some individuals (similar to, or higher than, the pre-treatment level in 13 of them). It was possible to classify the carriers at month 24 into 2
groups: 15 in whom the MFR was higher than 40% were considered as ‘bad responders’, and the remaining 28 were considered as ‘good responders’. The MFR, 6 months after each of the 4 treatments, were respectively 23%, 9%, 7% and 4% in the group of ‘good responders’, while they were 81%, 94%, 100% and 100% in the ‘bad responders’ group (CARTEL et al., 1993).
At month 24, the 43 carriers were randomly allocated into 2 groups. The first group of 22 (8 ‘bad resDonders’ and 14 ‘g&d responders’) was treated with I\;ER 100, while the second erouD of 21 (7 ‘bad resDonders’ and 14 ‘good responders’) wa’s treated with IVEi 400. Determi- nation of microfilaraemia by membrane filtration of venous blood samples was carried out at month 24, im- mediately before that month’s treatment, 2 d after it and 3 and 6 months later (months 27 and 30). The physician in charge of the patients, as well as the microscopists, re- mained ‘blind’ throughout the study.
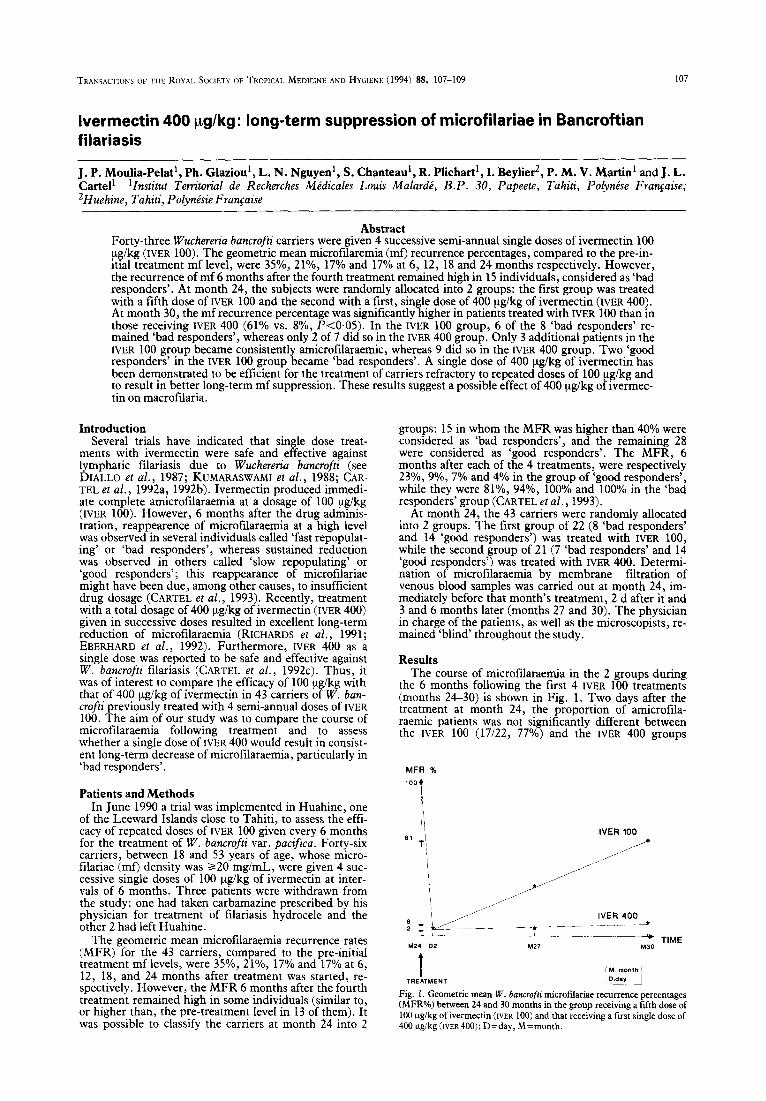
Results The course of microfilaraemia in the 2 groups during
the 6 months following the first 4 IVER 100 treatments (months 24-30) is shown in Fie. 1. Two davs after the treatment at month 24, the pioportion of’amicrofila- raemic patients was not significantly different between the IVER 100 (17122, 77%) and the IVER 400 groups
MFR % loo*
IVER 100
1 i,
Fig. 1. Geometric mean W. bancrofti microfilariae recurrence percentages (MFR%) between 24 and 30 months in the erouo receiving a fifth dose of 100 pg/kg of ivermecrin (IVER 100) and that receiving a first single dose of 400 ygikg (IVER400); D=day, M=month.
108
(18/2 1,86%); the geometric mean percentage of residual microfilaraemia was 2% in both groups. The proportion of patients with side effects was also not significantly dif- ferent between the 2 groups. At month 30, the MFR (compared with the value at month 24) was significantly higher in the IVER 100 group (61%) than in the IVER 400 group (8%) (P<O.O5).
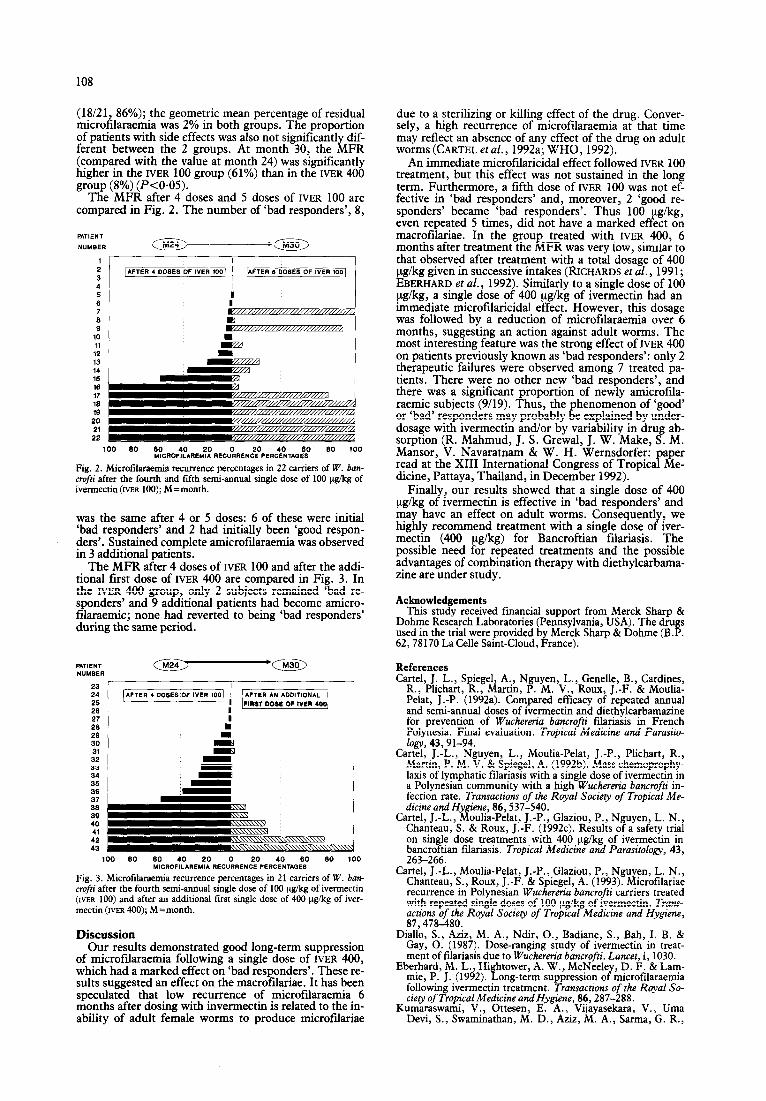
The MFR after 4 doses and 5 doses of IVER 100 are compared in Fig. 2. The number of ‘bad responders’, 8,
1 2 3 4 5 6 7 6 9
10 11
12 13 14 16 18 17 16 19
20 21
22
I I
100 60 60 20 40 60 60 MICROF:LOAREM::O RECUORRENCE PERCENTAQES
100 100 60 60 MICROF:LOAREM::O RECUORRENCE 20 40 60 60 100 PERCENTAQES
Fig. 2. Microtilaraemia recurrence percentages in 22 carriers of W. ban- Fig. 2. Microtilaraemia recurrence percentages in 22 carriers of W. ban- crofti after the fourth and fifth semi-annual single dose of 100 ug/kg of crofti after the fourth and fifth semi-annual single dose of 100 ug/kg of ivermectio (IVER 100); M=month. ivermectio (IVER 100); M=month.
was the same after 4 or 5 doses: 6 of these were initial ‘bad responders’ and 2 had initially been ‘good respon- ders’. Sustained complete amicrofilaraemia was observed in 3 additional patients.
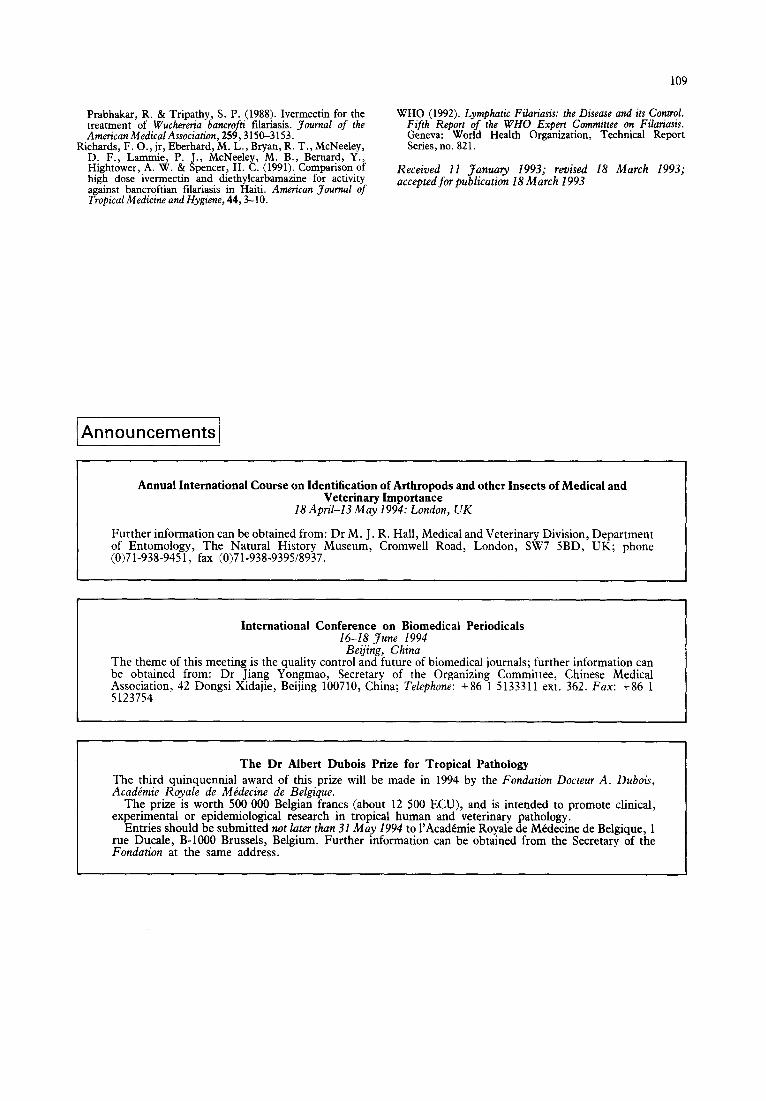
The MFR after 4 doses of IVER 100 and after the addi- tional first dose of IVER 400 are compared in Fig. 3. In the IVER 400 group, only 2 subjects remained ‘bad re- sponders’ and 9 additional patients had become amicro- filaraemic; none had reverted to being ‘bad responders’ during the same period.
23 24 25 26 27 26 29 30 31
32 33 34 35 36 37 36 39 40 4, 42 43
100 60 60 40 20 0 20 40 60 60 100 MICROFILAREMI* REC”RRENCE PERCENTADES
Fig. 3. Microtilaraemia recurrence percentages in 21 carriers of W. ban- crofti after the fourth semi-annual single dose of 100 vg/kg of ivennectin (IVER 100) and after an additional first single dose of 400 vgikg of iver- mectin (IVER 400); M=month.
Discussion Our results demonstrated good long-term suppression
of microfilaraemia following a single dose of IVER 400, which had a marked effect on ‘bad responders’. These re- sults suggested an effect on the macrofilariae. It has been speculated that low recurrence of microfilaraemia 6 months after dosing with invermectin is related to the in- ability of adult female worms to produce microfilariae
due to a sterilizing or killing effect of the drug. Conver- sely, a high recurrence of microfilaraemia at that time may reflect an absence of any effect of the drug on adult worms (CARTEL et al., 1992a; WHO, 1992).
An immediate microfilaricidal effect followed IVER 100 treatment, but this effect was not sustained in the long term. Furthermore, a fifth dose of IVER 100 was not ef- fective in ‘bad responders’ and, moreover, 2 ‘good re- sponders’ became ‘bad responders’. Thus 100 even repeated 5 times, did not have a marked !
g/kg, ef ect on
macrofilariae. In the group treated with IVER 400, 6 months after treatment the MFR was very low, similar to that observed after treatment with a total dosage of 400 ug/kg given in successive intakes (RICHARDS et al., 1991; EBERHARD et al., 1992). Similarly to a single dose of 100 ug/kg, a single dose of 400 ug/kg of ivermectin had an immediate microfilaricidal effect. However, this dosage was followed by a reduction of microlilaraemia over 6 months, suggesting an action against adult worms. The most interesting feature was the strong effect of IVER 400 on patients previously known as ‘bad responders’: only 2 therapeutic failures were observed among 7 treated pa- tients. There were no other new ‘bad responders’, and there was a significant proportion of newly amicrofila- raemic subjects (909). Thus, the phenomenon of ‘good’ or ‘bad’ responders may probably be explained by under- dosage with ivermectin and/or by variability in drug ab- sorption (R. Mahmud, J. S. Grewal, J. W. Make, S. M. Mansor, V. Navaratnam & W. H. Wernsdorfer: paper read at the XIII International Congress of Tropical Me- dicine, Pattaya, Thailand, in December 1992).
Finally, our results showed that a single dose of 400 kg/kg of ivermectin is effective in ‘bad responders’ and may have an effect on adult worms. Consequently? we highly recommend treatment with a single dose of iver- mectin (400 ug/kg) for Bancroftian filariasis. The possible need for repeated treatments and the possible advantages of combination therapy with diethylcarbama- zine are under study.
Acknowledgements This study received fmancial support from Merck Sharp &
Dohme Research Laboratories (Pennsylvania, USA). The drugs used in the trial were provided by Merck Sharp & Dohme (BP. 62,78170 La Celle Saint-Cloud, France).
References Cartel, J. L., Spiegel, A., Nguyen, L., Genelle, B., Cardines,
R., Plichart, R., Martin, P. M. V., Roux, J.-F. & Moulia- Pelat, J.-P. (1992a). Compared efficacy of repeated annual and semi-annual doses of ivermectin and diethylcarbamazine for prevention of Wuchereria bancrojii tilariasis in French Polynesia. Final evaluation. Tropical Medicine and Parasito- logy, 43,91-94.
Cartel, J.-L., Nguyen, L., Moulia-Pelat, J.-P., Plichart, R., Martin, P. M. V. & Spiegel, A. (1992b). Mass chemoprophy- laxis of lymphatic tilariasis with a single dose of ivermectin in a Polynesian community with a high Wuchereria bancrofii in- fection rate. Transactions of the Royal Society of Tropical Me- dicine and H#en f, s&537-540.
Cartel, J.-L., ouha Pelat, J.-P., Glaziou, P., Nguyen, L. N., Chanteau, S. & Roux, J.-F. (1992~). Results of a safety trial on single dose treatments with 400 ygikg of ivermectin in bancroftian tilariasis. Tropical Medicine and Parasitology, 43, 263-266.
Cartel, J.-L., Moulia-Pelat, J.-P., Glaziou, P., Nguyen, L. N., Chanteau, S., Roux, J.-F. & Spiegel, A. (1993). Microtilariae recurrence in Polynesian Wuchereria bancrofti carriers treated with repeated single doses of 100 ug/kg of ivermectin. Trans- actions of the Royal Sociery of Tropical Medicine and Hygiene, 87,478-480.
Diallo, S., Aziz, M. A., Ndir, O., Badiane, S., Bah, I. B. & Gay, 0. (1987). Dose-ranging study of ivermectin in treat- ment of filariasis due to Wuchereria bancrofti. Lancet, i, 1030.
Eberhard, M. L., Hi htower, A. W., McNeele mie, P. J. (1992). &
D. F. & Lam- ong-term suppression o Y’ mtcrotilaraemia
following ivermectin treatment. Transactions of the Royal So- ciety of Tropical Medicine and Hygiene, 86,287-288.
Kumaraswami, V., Ottesen, E. A., Vijayasekara, V., LJma Devi, S., Swaminathan, M. D., Aziz, M. A., Sarma, G. R.,
109
Prabhakar, R. & Tripatby, S. I’. (1988). Ivermectin for the treatment of Wuchereria bancrofti iilariasis. Journal of the American MedicalAssociation, 259,3150-3153.
Richards, F. O., jr, Eberhard, M. L., Bryan, R. T., McNeeley, D. F., Lanunie, P. J., McNeeIey, M. B., Bernard, Y., Hightower, A. W. & Spencer? H. C. (1991). Comparison of high dose ivermectin and dietbylcarbamazine for activity against bancroftian filariasis in Haiti. American Journal of Tropical Medicine and Hygiene, 44,3-10.
WHO (1992). Lymphatic Filariasis: the Disease and its Control. Fifth Report of the WHO Expert Committee on Filariasis. Geneva: World Health Organization, Technical Report Series, no. 821.
Received 11 January 1993; revised 18 March 1993; accepted for publication 18 March I993
Announcements
Annual International Course on Identification of Arthropods and other Insects of Medical and Veterinary Importance
18 Apri-13 May 1994: London, UK
Further information can be obtained from: Dr M. J. R. Hall, Medical and Veterinary Division, Department of Entomology, The Natural History Museum, Cromwell Road, London, SW7 SBD, UK; phone (0)71-938-9451, fax (0)71-938-939518937.
International Conference on Biomedical Periodicals 16-18 June 1994
Beijing, China The theme of this meeting is the quality control and future of biomedical journals; further information can be obtained from: Dr Jiang Yongmao, Secretary of the Organizing Committee, Chinese Medical Association, 42 Dongsi Xidajie, Beijing 100710, China; Telephone: +86 1 5133311 ext. 362. Fax: +86 1 5 123754
The Dr Albert Dubois Prize for Tropical Pathology The third quinquennial award of this prize will be made in 1994 by the Fondation Docteur A. Dubois, Academic Royale de Medecine de Belgique.
The prize is worth 500 000 Belgian francs (about 12 500 ECU), and is intended to promote clinical, experimental or epidemiological research in tropical human and veterinary pathology.
Entries should be submitted not later than 31 May 1994 to 1’Academie Royale de Medecine de Belgique, 1 rue Ducale, B-1000 Brussels, Belgium. Further information can be obtained from the Secretary of the Fondation at the same address.





























