Embed Size (px)
DESCRIPTION
PAPER RESINA INFILTRANTE
Citation preview

INTRODUCTION
During the development of subsurface caries lesions, mineral is dissolved
out of the enamel, resulting in increased porosities that appear clinically
as the so-called 'white-spot' lesions (Ten Cate et al., 2003). Today, these
lesions are commonly treated by enhancing remineralization, e.g., by
improving the individual's oral hygiene or fluoridation. However, in non-
compliant individuals with cavitated proximal lesions and greater lesion
extension, this strategy has considerable limitations.
A promising alternative therapy for the arrest of caries lesions might be
the infiltration of subsurface lesions with low-viscous light-curing resins.
Since porosities of enamel caries act as diffusion pathways for acids and
dissolved minerals, infiltration of these lesions with resins might occlude the
pathways, thus leading to an arrest of caries progression.
Several studies have demonstrated that artificial caries lesions can be
infiltrated by commercially available adhesives and fissure sealants (Davila
et al., 1975; Robinson et al., 2001; Schmidlin et al., 2004; Meyer-Lueckel etal., 2006). Moreover, it has been shown that infiltrated artificial lesions do
not progress in a cariogenic environment (Mueller et al., 2006; Paris et al.,2006). Thus far, only two in vitro studies have addressed the infiltration of
natural lesions. However, these early reports were mainly descriptive
(Davila et al., 1975), or used materials which were not clinically applicable
due to their unsanitary nature (Robinson et al., 1976). Since there are
substantial structural differences between both lesion types, it is not
applicable to transfer findings from artificial to natural lesions.
The surface layer of enamel caries lesions has a lower pore volume
compared with that of the lesion body underneath (Bergman and Lind, 1966;
Silverstone, 1973). Since the infiltration of enamel caries with light-curing
resins is mainly driven by capillary forces, the pore diameter and volume
influence the penetration speed (Paris et al., 2007). Therefore, the surface
layer forms a barrier, which might hamper the infiltration of the lesion body.
From this follows that removing or perforating the surface layer might be
essential for a successful infiltration of the lesion body. In artificial lesions,
brief etching with 37% phosphoric acid enhanced resin penetration (Gray
and Shellis, 2002). With thicker and more mineralized surface layers in
natural lesions (Bergman and Lind, 1966), it was assumed that this etching
procedure would not be effective in eroding the surface layer (Meyer-
Lueckel et al., 2007). The latter study confirmed that etching with 15%
hydrochloric acid gel leads to a more effective erosion of the surface layer
compared with 37% phosphoric acid gel, but did not focus on the
subsequent infiltration of resins into the lesions.
Therefore, the aim of the present study was to evaluate the penetration
of a commercial adhesive into natural proximal caries lesions, without pre-
treatment and with prior conditioning by two different etching gels in vitro.
The working hypotheses were:
(Hypothesis 1) The surface layer of natural un-cavitated caries is a
diffusion barrier, which hampers the penetration of resin. Therefore, no
ABSTRACTInfiltration of non-cavitated caries lesions with
light-curing resins could lead to an arrest of lesion
progression. The aim of this study was to evaluate
the penetration of a conventional adhesive into
natural enamel caries after pre-treatment with two
different etching gels in vitro. Extracted human
molars and premolars showing proximal white-
spot lesions were cut across the lesions
perpendicular to the surface. Corresponding lesion
halves were etched for 120 sec with either 37%
phosphoric acid gel (H3PO
4) or 15% hydrochloric
acid gel (HCl), and subsequently infiltrated with
an adhesive. Specimens were observed by
confocal micro scopy. Mean penetration depths
(SD) in the HCl group [58 (37) �m] were
significantly increased compared with those of the
H3PO
4group [18 (11) �m] (p < 0.001; Wilcoxon).
It can be concluded that etching with 15%
hydrochloric acid gel is more suitable than 37%
phosphoric acid gel as a pre-treatment for caries
lesions intended to be infiltrated.
KEY WORDS: caries, resin infiltration, etching,
acid gel.
Received July 23, 2006; Last revision February 9, 2007;
Accepted March 6, 2007
A supplemental appendix to this article is published
electronically only at http://www.dentalresearch.org.
Resin Infiltration of Natural Caries Lesions
S. Paris, H. Meyer-Lueckel*, and A.M. Kielbassa
Dept. of Operative Dentistry and Periodontology,University School of Dental Medicine, Campus BenjaminFranklin, Charité-Universitätsmedizin Berlin,Assmannshauserstr. 4-6, 14197 Berlin, Germany;*corresponding author, [email protected]
J Dent Res 86(7):662-666, 2007
RESEARCH REPORTSBiomaterials & Bioengineering
662 at International Association for Dental Research on March 23, 2015 For personal use only. No other uses without permission.jdr.sagepub.comDownloaded from
International and American Associations for Dental Research

J Dent Res 86(7) 2007 Infiltration of Caries Lesions 663
resin penetration occurs without prior
etching; and (Hypothesis 2) pre-
treatment for 120 sec with 15%
hydrochloric acid gel leads to a more
pronounced resin penetration
compared with 37% phosphoric acid
gel.
MATERIALS & METHODSExtracted human molars and premolars
showing proximal white-spot lesions
were used in this study. The study
protocol conformed to the principles
outlined in the Central German Ethics
Committee's statement (2003) focusing
on the use of human body material in
medical research. After being carefully
cleaned of soft tissues, teeth were
stored in 20% ethanol solution until
used. Teeth were examined by 20
stereo microscopy (Stemi SV 11; Carl
Zeiss, Oberkochen, Germany), and
cavitated as well as damaged lesions
were excluded.
For radiographic examination,
teeth were positioned in a silicone base
with the buccal aspects facing a
radiographic tube (Heliodent MD;
Siemens, Bensheim, Germany). To
simulate cheek scatter, we placed a 15-
mm wall of clear Perspex between the
tube and the teeth. Standardized
radiographs (0.12 sec, 60 kV, 7.5 mA)
were taken of each tooth (Ektaspeed;
Kodak, Stuttgart, Germany) and
developed in an automatic processor
(XR 24-II; Dürr Dental, Bietigheim-
Bissingen, Germany). The radiographic
lesion depths were independently
assessed by two examiners and scored
(Marthaler and Germann, 1970): no
translucency (R0), translucency
confined to the outer half on enamel
(R1), translucency confined to the inner
half of enamel (R2), translucency
confined to the outer half of dentin
(R3), or translucency confined to the
inner half of dentin (R4). In case of
disagreement in an assessment of
radiographic lesion depth, a consensus
rank was reached.
The roots of the teeth were
removed, and the crowns were cut
across the caries lesions perpendicular
to the surface (Band Saw; Exakt
Apparatebau, Norderstedt, Germany),
providing two halves of each lesion
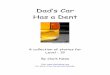
(Figs. 1a, 1b). Subsequently, the cut surfaces were examined
(stereo microscope, 20 ; Stemi SV 11) and classified with respect
to the histological lesion extension, according to the radiological
grading (Marthaler and Germann, 1970): C1, extension into the
outer half of enamel; C2, extension into the inner half of enamel;
or C3, extension into the outer half of dentin. Lesions extending
into the inner half of dentin (C4) were excluded. Corresponding
lesion halves showing the same grading level (C1-C3) in
Figure 1. Representative images of a lesion treated with the adhesive. (A) Clinical aspect of the mesialsurface of a human molar showing a white-spot lesion (dotted line). The lesion was cut in two halvesalong the dashed line. (B) Aspect of the cut surfaces of the same enamel lesion. (C-E) Confocalmicroscopic images of resin-infiltrated lesions (E, sound enamel; SL, surface layer; LB, lesion body; R,penetrated resin; S, lesion surface). (C) Deep resin penetration can be observed after etching withHCl. (D) The surface layer of this H3PO4-etched caries lesion was not eroded completely. Therefore,only superficial resin penetration occurred, as indicated by a fine rim of red fluorescence at the toothsurface. (E) Magnified image of an HCl-etched lesion (40x objective). The outermost 50-100 �m ofprism cores are filled with resin. In non-infiltrated parts of the lesion body, the highly porous prismcenters show green fluorescence.
at International Association for Dental Research on March 23, 2015 For personal use only. No other uses without permission.jdr.sagepub.comDownloaded from
International and American Associations for Dental Research

664 Paris et al. J Dent Res 86(7) 2007
histological caries extension were assigned to the treatment (TRT)
group (n = 10 each). In case the corresponding lesion halves
differed in lesion extension, the deeper lesion was used as the
control (CTR; n = 10), and the remaining half was disposed of.
Subsequently, the cut surfaces were covered with nail varnish.
In the treatment (TRT) group, corresponding lesion halves were
etched either with 37% phosphoric acid gel (H3PO
4; total etch;
IvoclarVivadent, Schaan, Liechtenstein), or with an experimental
15% hydrochloric acid gel (HCl). The HCl gel contained
hydrochloric acid 15%, glycerol 19%, highly dispersed silicon
dioxide 8%, and methylene blue 0.01% in aqueous solution. After
120 sec, the gels were rinsed thoroughly with water spray for 30
sec. In the control (CTR) group, no acid etching was performed.
Lesions were immersed in pure ethanol for 30 sec and
subsequently dried for 60 sec with oil-free compressed air.
A dental adhesive (Excite; IvoclarVivadent, Schaan,
Liechtenstein) labeled with 0.1% tetramethylrhodamine
isothiocyanate (TRITC; Sigma Aldrich, Steinheim, Germany) was
applied to the lesion surfaces. The resin was allowed to penetrate
the lesions for 5 min. Subsequently, excess material was removed
by means of cotton pellets, and the resin was light-cured for 30 sec
(Translux CL; Heraeus Kulzer, Hanau, Germany) at 400 mW/cm2.
The nail varnish was carefully removed, and specimen halves were
fixed on object holders parallel to the cut surface and polished
(Exakt Mikroschleifsystem, Abrasive Paper 2400, 4000; Exakt
Apparatebau, Norderstedt, Germany). To stain remaining pores,
we immersed the specimens in 50% ethanol solution containing
100 �M/L sodium fluorescein (Sigma Aldrich) for 3 hrs.
Specimens were observed by confocal laser scanning
microscopy (CLSM Leica TCS NT; Leica, Heidelberg, Germany)
in dual-fluorescence mode and with a 10x objective. The excitation
light had two wavelength maxima, at 488 and 568 nm. The emitted
light was split by a 580-nm reflection short-pass filter and passed
through a 525/50-nm band-pass filter for FITC and a 590-nm long-
pass filter for RITC detection. Images with a lateral dimension of
1000 x 1000 �m2 and a resolution of 1024 x 1024 pixels were
recorded and analyzed by AxioVision LE software (Zeiss,
Oberkochen, Germany). Penetration depths and thicknesses of the
(residual) surface layer for the lesion halves were measured at up
to 10 defined points (depending on the lesion size; indicated by a
100-�m grit), and mean values were calculated. Additionally to
CLSM analysis, acid-etched as well as infiltrated lesion surfaces
were observed by scanning electron microscopy (APPENDIX).
Statistical analysis was performed with SPSS software (SPSS
for Windows 11.5.1; SPSS, Chicago, IL, USA). Data were checked
for normal distribution by the Kolmogorov-Smirnov test. To
analyze differences in penetration depth between lesion halves/acid
gels, we used the Wilcoxon test for paired samples. For
comparison between unpaired groups, we performed Mann-
Whitney and Kruskal-Wallis tests. Penetration depths were
analyzed with regard to possible differences between various
histological lesion extensions (C1-C3) and radiological grades
(R0-R3). The level of significance was set at 5%.
RESULTSIn the CLSM images, the penetrated resin showed a red
fluorescence, whereas remaining pores within the lesion, as
well as dentin, appeared green (Figs. 1c-1e). Solid material,
such as sound enamel or the surface layer, was displayed black.
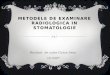
Penetration depths varied considerably. For lesion halves
etched with HCl gel, the mean penetration depth (standard
deviation) [58 (37) �m] was significantly higher compared
with that of those lesions treated with H3PO
4gel [18 (11) �m]
(p < 0.001; Wilcoxon) (Fig. 2). Without acid-etching, no resin
penetration was found [0 (1) �m]. Within treatment groups, no
significant differences for penetration depths could be observed
between various lesion extensions (C1-C3) (p > 0.05; Kruskal-
Wallis).
For radiological grading of lesion extensions, good inter-
observer agreement could be found (� = 0.804). Similar to
histological lesion extension (C1-C3), no significant
differences in penetration depth could be observed among
different radiological grades (R0-R3) (Table).
For those lesions where the surface layer was completely
removed (CTR, n = 0; H3PO
4, n = 2; HCl, n = 8), significantly
higher (p < 0.01; Mann-Whitney) penetration depths [65 (35)
�m] could be found compared with those lesions where
residues of the surface layer remained after etching [33 (31)
�m]. Surface layer thickness was significantly reduced after
HCl etching [20 (18) �m], compared with that in the lesions
etched with phosphoric acid [37 (25) �m] and with the non-
etched CTR group [42 (23) �m] (p > 0.05; Mann-Whitney).
DISCUSSIONIn previous studies where confocal microscopy was used, resin
penetration was visualized by labeling of the resin with
Figure 2. Mean penetration depths of resin for various pre-treatmentsand histological lesion extensions (box and whisker plots with quartilesand medians; n = 10 per group). Statistically significant differencesbetween groups are indicated with asterisks (*p < 0.05; **p < 0.01;***p < 0.001; Mann-Whitney). Abbreviations: C1, caries extension intothe outer half of enamel; C2, caries extension into the inner half ofenamel; C3, caries extension into the outer half of dentin.
at International Association for Dental Research on March 23, 2015 For personal use only. No other uses without permission.jdr.sagepub.comDownloaded from
International and American Associations for Dental Research

J Dent Res 86(7) 2007 Infiltration of Caries Lesions 665
fluorescent dyes (Schmidlin et al., 2004). In another
approach, the remaining (not infiltrated) pores were
marked with a dye-labeled polymer (Meyer-
Lueckel et al., 2006; Paris et al., 2006), or by
imbibition in a fluorescent solution (González-
Cabezas et al., 1998). In the present study, these
two methods were modified and combined. The
penetration of the resin was visualized by the red
fluorescence of TRITC. The remaining lesion pores
were indicated by the green fluorescence of sodium
fluorescein. Hard tissues with small pore volume
including the surface layer or sound enamel were
neither infiltrated by the resin nor stained by the
green solution and appeared black. Thus, the dual-
fluorescence technique used in the present study
allowed for the simultaneous observation of the
porous lesion structure, the penetrated resin, as well
as structures with small pore volume.
Caries infiltration might be a promising approach for the
treatment of uncavitated caries lesions. In contrast to fissure
sealing, where the diffusion barrier is placed on top of the
(lesion) surface, the infiltration technique aims to create the
diffusion barrier inside the lesion, replacing lost mineral with
resin. Therefore, the infiltration treatment should be
differentiated from sealing techniques, where a resin layer
(Goepferd and Olberding, 1989; García-Godoy et al., 1997;
Tantbirojn et al., 2000) was established on the caries lesions. A
recent clinical trial, where proximal enamel lesions were
superficially sealed with an adhesive, found a significantly
reduced but still relatively high (43.5%) lesion progression over
an 18-month observation period (Martignon et al., 2006).
Another clinical investigation did not find any significant
differences in lesion progression between the sealed and the
control group (Gomez et al., 2005). The latter authors
speculated that treatment failures might be due to incomplete
sealing or sealant disintegration over time. Moreover,
laboratory studies confirmed the inferior resistance of unfilled
resins to mechanical and chemical stress (Schmidlin et al.,2002, 2006). Therefore, it is questionable whether superficial
smooth-surface sealing with unfilled resins is, as yet, generally
applicable in daily practice.
Compared with the latter concepts, the infiltration
treatment might bear several advantages. With the infiltration
technique, excessive resin is removed from the tooth surface
before light-curing, whereby clinical application is greatly
simplified. With application strips coated on one side,
proximal lesions can be infiltrated without special protection
for the adjacent tooth, and after only minimal tooth
separation, e.g. , by means of a wooden wedge or an
orthodontic rubber band (unpublished results). Moreover,
with this treatment, no sealant margins are produced on the
tooth surface that could enhance plaque accumulation and
cause periodontal inflammation. Furthermore, infiltration of
the porous lesion structures might strengthen the lesion
mechanically and prevent cavitation.
To infiltrate a caries lesion, the penetrating resin needs
access to the porous spaces of the lesion body. It was assumed
that the penetration could be hampered by the highly
mineralized surface layer, where the pore volume is
considerably lower. In fact, in the present investigation, no
penetration was found without prior acid-etching. Moreover, it
could be demonstrated that penetration was significantly
increased in those parts of the lesion where the surface layer
was completely removed after acid-etching. Therefore,
hypothesis 1 could be corroborated.
Recently, 15% hydrochloric acid gel proved to erode the
surface layer more effectively than 37% phosphoric acid gel
(Meyer-Lueckel et al., 2007). In the present investigation, the
effects of etching with these acid gels on resin penetration were
compared. Phosphoric acid (37%) is frequently used in
restorative dentistry for adhesive purposes. Hydrochloric acid
has been previously used for enamel microabrasion
(McCloskey, 1984; Mathewson et al., 1987). Although short-
term contact of this strong acid with mucosa has been shown to
be harmless (Croll et al., 1990), safety precautions, such as a
rubber dam, should be used in clinical practice.
Since significantly higher penetration depths could be
found after etching with hydrochloric acid, hypothesis 2 could
be confirmed as well. However, the surface layer could not be
eroded completely in 67% of lesions in the HCl group. Thus,
longer application times should be considered to achieve
complete surface layer erosion. However, resin penetration was
not influenced by macroscopic or radiological lesion extension.
The penetration depths observed for Excite in natural
lesions in the present study were lower compared with those
observed in artificial lesions (104 �m/30 sec) in a previous
investigation (Meyer-Lueckel et al., 2006), although a ten-fold
longer penetration time was chosen in the present study. It
might be argued that the incomplete surface layer erosion in
natural lesions, even for those etched with HCl, could be
responsible for this contradiction. However, in specimens
where the surface layer could be totally removed, mean
penetration depths were lower as well. In contrast to artificial
lesions, the pores of natural caries might be contaminated with
organic materials, such as proteins and carbohydrates, that
might hamper resin penetration as well. This underlines that
findings from artificial lesions cannot necessarily be
extrapolated to natural lesions.
It can be concluded that the surface layer of a non-cavitated
natural caries lesion is a barrier that significantly hampers the
penetration of a light-curing resin. Therefore, no substantial
resin penetration could be observed without prior acid-
conditioning. Etching for 120 sec with hydrochloric acid gel led
to deeper resin penetration than etching with phosphoric acid
gel, although surface layers could not be removed in all cases.
Table. Mean Penetration Depths [�m (standard deviations)] for the VariousRadiological Caries Extensions
Group\Radiolucency R0* R1 R2 R3
CTR 0 ( 0)n = 8 0 ( 0) n = 10 1 ( 1) n = 8 0 ( 0) n = 4
TRTH3PO4 25 (15) n = 6 17 (12) n = 10 16 ( 7) n = 8 16 (10) n = 6HCl 47 (27) n = 6 65 (41) n = 10 52 (27) n = 8 67 (52) n = 6
* Abbreviations: R0, no radiographic translucency; R1, translucency confined tothe outer half of enamel; R2, translucency confined to the inner half of enamel;R3, translucency confined to the outer half of dentin; CTR, unetched controlgroup; TRT, treatment group; H3PO4, phosphoric acid etching; HCl, hydrochloricacid etching.
at International Association for Dental Research on March 23, 2015 For personal use only. No other uses without permission.jdr.sagepub.comDownloaded from
International and American Associations for Dental Research

666 Paris et al. J Dent Res 86(7) 2007
ACKNOWLEDGMENTSThis study was supported by the Deutsche Forschungs -
gemeinschaft (DFG; PA 1508/1-1). The authors are indebted to
Mrs. Anja Bartels and Mrs. Julia Heinrich (Dept. of Operative
Dentistry and Periodontology, CBF, Charité) for their excellent
contributions to the experiments, to Dr. Herbert Renz (Dept. of
Experimental Dentistry, CBF, Charité) for his assistance with
the SEM, and to Prof. Dr. Harald Stein (Institute for Pathology,
CBF, Charité) for providing the CLSM.
The Charité-Universitätsmedizin Berlin holds US
(US10/432,271) and European (EP06021966.4) patent
applications for an infiltration technique for dental caries lesions
in which the authors of this study are appointed as inventors.
REFERENCESBergman G, Lind PO (1966). A quantitative microradiographic study
of incipient enamel caries. J Dent Res 45:1477-1484.
Central German Ethics Committee (2003). Statement: [The use of
human body materials for the purposes of medical research].
20.02.2003 http://www.zentrale-ethikkommission.de/10/
31KoerpermatZ.html [site in German].
Croll TP, Killian CM, Miller AS (1990). Effect of enamel
microabrasion compound on human gingiva: report of a case.
Quintessence Int 21:959-963.
Davila JM, Buonocore MG, Greeley CB, Provenza DV (1975).
Adhesive penetration in human artificial and natural white spots. JDent Res 54:999-1008.
García-Godoy F, Summitt JB, Donly KJ (1997). Caries progression of
white spot lesions sealed with an unfilled resin. J Clin PediatrDent 21:141-143.
Goepferd SJ, Olberding P (1989). The effect of sealing white spot
lesions on lesion progression in vitro. Pediatr Dent 11:14-16.
Gomez SS, Basili CP, Emilson CG (2005). A 2-year clinical evaluation
of sealed noncavitated approximal posterior carious lesions in
adolescents. Clin Oral Investig 9:239-243.
González-Cabezas C, Fontana M, Dunipace AJ, Li Y, Fischer GM,
Proskin HM, et al. (1998). Measurement of enamel remineral -
ization using microradiography and confocal microscopy. A
correlational study. Caries Res 32:385-392.
Gray GB, Shellis P (2002). Infiltration of resin into white spot caries-
like lesions of enamel: an in vitro study. Eur J Prosthodont RestorDent 10:27-32.
Marthaler TM, Germann M (1970). Radiographic and visual
appearance of small smooth surface caries lesions studied on
extracted teeth. Caries Res 4:224-242.
Martignon S, Ekstrand KR, Ellwood R (2006). Efficacy of sealing
proximal early active lesions: an 18-month clinical study
evaluated by conventional and subtraction radiography. CariesRes 40:382-388.
Mathewson RJ, Morrison JT, Carpenter R (1987). Modification of
stained enamel surfaces: use of hydrochloric acid and pumice
mixture. J OK Dent Assoc 77:22-25.
McCloskey RJ (1984). A technique for removal of fluorosis stains. JAm Dent Assoc 109:63-64.
Meyer-Lueckel H, Paris S, Mueller J, Colfen H, Kielbassa AM (2006).
Influence of the application time on the penetration of different
dental adhesives and a fissure sealant into artificial subsurface
lesions in bovine enamel. Dent Mater 22:22-28.
Meyer-Lueckel H, Paris S, Kielbassa AM (2007). Surface layer
erosion of natural caries lesions with phosphoric and hydrochloric
acid gels in preparation for resin infiltration. Caries Res 41:223-
230.
Mueller J, Meyer-Lueckel H, Paris S, Hopfenmuller W, Kielbassa AM
(2006). Inhibition of lesion progression by the penetration of
resins in vitro: influence of the application procedure. Oper Dent31:338-345.
Paris S, Meyer-Lueckel H, Mueller J, Hummel M, Kielbassa AM
(2006). Progression of sealed initial bovine enamel lesions under
demineralizing conditions in vitro. Caries Res 40:124-129.
Paris S, Meyer-Lueckel H, Colfen H, Kielbassa AM (2007).
Penetration coefficients of commercially available and
experimental composites intended to infiltrate enamel carious
lesions. Dent Mater 23:742-748.
Robinson C, Hallsworth AS, Weatherell JA, Kunzel W (1976). Arrest
and control of carious lesions: a study based on preliminary
experiments with resorcinol-formaldehyde resin. J Dent Res55:812-818.
Robinson C, Brookes SJ, Kirkham J, Wood SR, Shore RC (2001). In
vitro studies of the penetration of adhesive resins into artificial
caries-like lesions. Caries Res 35:136-141.
Schmidlin PR, Gohring TN, Sener B, Lutz F (2002). Resistance of an
enamel-bonding agent to saliva and acid exposure in vitro assessed
by liquid scintillation. Dent Mater 18:343-350.
Schmidlin PR, Zehnder M, Pasqualetti T, Imfeld T, Besek MJ (2004).
Penetration of a bonding agent into de- and remineralized enamel
in vitro. J Adhes Dent 6:111-115.
Schmidlin PR, Kluck I, Zimmermann J, Roulet JF, Seemann R (2006).
Caries-preventive potential of an adhesive patch after
thermomechanical loading—a microbial-based in vitro study. JAdhes Dent 8:7-12.
Silverstone LM (1973). Structure of carious enamel, including the
early lesion. Oral Sci Rev 3:100-160.
Tantbirojn D, Rozzi SM, Mitra SB, Kedrowski BL, Douglas WH
(2000). In vitro inhibition of enamel demineralization by a
polymerizable amphiphilic film. Eur J Oral Sci 108:564-568.
Ten Cate JM, Larsen MJ, Pearce EIF, Fejerskov O (2003). Chemical
interactions between the tooth and oral fluids. In: Dental caries.
Fejerskov O, Kidd EAM, editors. Oxford: Blackwell Munksgaard,
pp. 49-69.
at International Association for Dental Research on March 23, 2015 For personal use only. No other uses without permission.jdr.sagepub.comDownloaded from
International and American Associations for Dental Research