Embed Size (px)
Citation preview
J Clin Pathol 1994;47:827-833
Pathology of endometrium treated with tamoxifen
S M Ismail
Department ofPathology, UniversityofWales College ofMedicine, Heath Park,CardiffCF4 4XNS M IsmailCorrespondence to:Dr S M IsmailAccepted for publication19 April 1994
AbstractAims-To determine the type of endome-trial abnormalities associated with pro-longed tamoxifen treatment and toinvestigate the correlation betweentamoxifen dose and any abnormalitiesdetected.Methods-Endometria from 19 prospec-tively collected breast cancer patientstreated with tamoxifen were ascribed apathological diagnosis and the findingscompared with those in a control groupmatched for age and presentation. Theabnormalities were related to cumulativetamoxifen dose.Results-The two asymptomatic treatedpatients had generalised simple endo-metrial hyperplasia at necropsy. Noendometrial abnormalities were seen atnecropsy in the two control cases. Of the17 patients treated with tamoxifen whounderwent surgery for gynaecologicalsymptoms, 11 had hyperplastic endome-trial polyps characterised by epithelialmetaplasias and patchy periglandularcondensation of stroma. Two women hadprimary endometrial malignancies with
myometrial invasion, and three women,one of whom had previously presentedwith a benign polyp, had an endometrialpolyp-cancer on a background of hyper-plasia. Endometrial malignancies wereconfined to women who had taken morethan 35 g of tamoxifen. The control groupincluded no endometrial polyp-cancers,only one patient with an endometrialpolyp, four women with endometrialhyperplasia and four with primaryendometrial malignancy.Conclusions-These findings support alink between prolonged tamoxifen treat-ment and endometrial malignancy andidentify a subgroup of patients-that is,those who have taken more than 35 g oftamoxifen, who may be at increased riskof endometrial cancer. The spectrum ofpathological findings in patients treatedwith tamoxifen suggests that the drugpromotes endometrial growth and thatendometrial polyps may be an importantintermediate step in endometrial car-cinogenesis.
(7 Clin Pathol 1994;47:827-833)
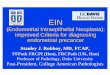
Figure I Postmortemuterus ofan 85 year oldwoman treated withtamoxifen. The uterus isenlarged and shows diffuseendometrial thickeningwith numerous cysticspaces.
827
on 1 Septem
ber 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.47.9.827 on 1 S
eptember 1994. D
ownloaded from
828
Tamoxifen is a non-steroidal triphenylethyl-ene derivative with predominant anti-oestro-gen activity.' It has long been in widespreaduse in the management of established breastcarcinoma. Perceived as safe, effective, andwith negligible side effects,2 it has recentlybeen advocated as of potential value in breastcancer prevention' and its efficacy as a pre-ventive agent is currently being evaluated inasymptomatic women deemed to be atincreased risk of breast cancer.4
Although an oestrogen antagonist in thebreast, tamoxifen is structurally closely relatedto the synthetic oestrogen diethylstilbestrolland is known to have oestrogen agonist activityin the vaginal epithelium57 and endo-
metrium8 9 of postmenopausal women. Inkeeping with such an effect, recent studieshave reported an increased incidence ofendometrial carcinoma,'0 polyps,911 andhyperplasia9 11 in women treated with tamox-ifen. However, existing publications on thepathology of endometrium in women treatedwith the drug are few and far between,' 2-14 andthe association between tamoxifen dose andendometrial disease has not been studied.This study investigates the relation betweentamoxifen dose and the endometrial abnor-malities detected in a group of breast cancer
patients who received prolonged tamoxifentreatment.
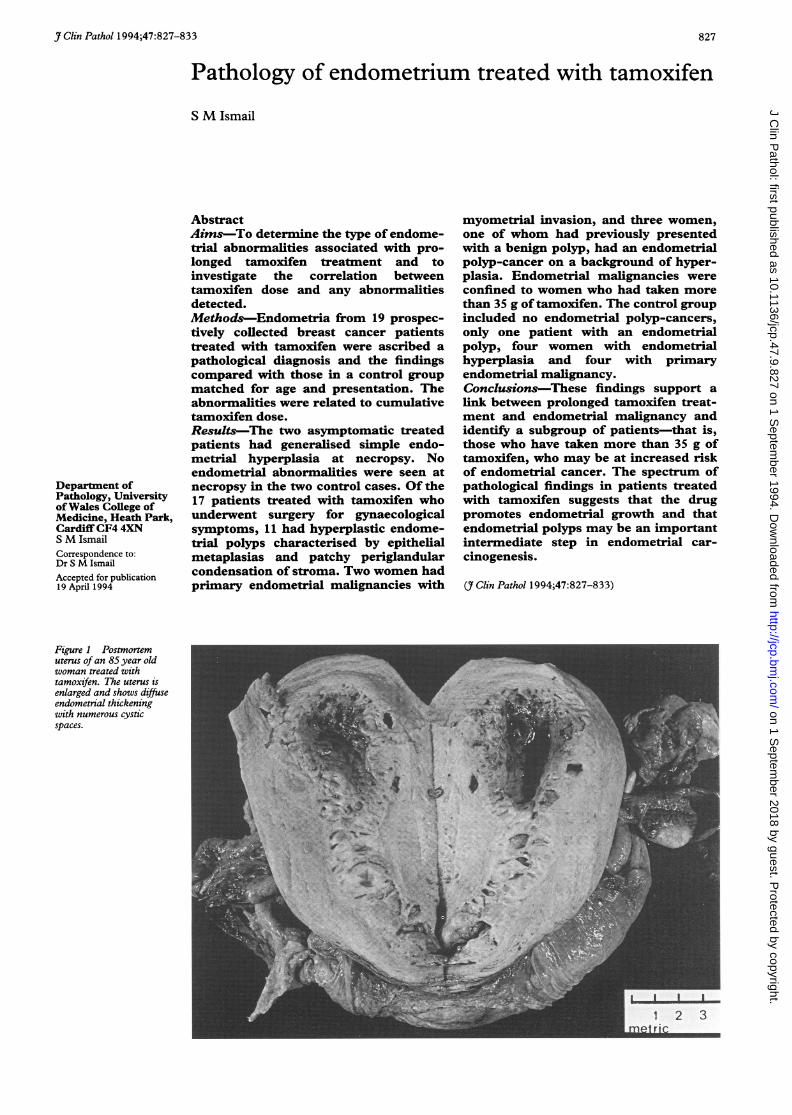
Figure 2 A benignendometrial polyp in a 54year old woman treatedwith tamoxifen whounderwent hysterectomy forpostmenopausal bleeding.
Clinical presentation and pathologicalfindings in women treated with tamoxifen compared with untreated controls
Case No Symptoms Age Endometrial pathology Control pathology
1 PMB 54 Benign polyp (3 cm); background simple endometrial hyperplasia Endometrial hyperplasia2 PMB 52 Benign polyp (3 3 cm); background cystic atrophy Endometrial carcinoma3 PMB 54 Benign polyp (8 cm), focus of secondary carcinoma within polyp and Endometrial polyp
background simple endometrial hyperplasia4 Menorrhagia 54 Two benign polyps (5 cm and 1-5 cm); background cystic atrophy No endometrial abnormality5* PMB 74 Benign polyp (4 cm); no background endometrium Endometrial carcinoma6 PMB 59 Benign polyp (2-3 cm); no background aendometrium No endometrial abnormality7 PMB 52 Benign polyp (1-5 cm); no background endometrium Endometrial hyperplasia8t Clear discharge 59 Benign polyp (5 cm) and background simple endometrial hyperplasia No endometrial abnormality9t PMB 67 Benign polyp (6 cm), three previous polyps, and background simple endometrial Endometrial hyperplasia ?polyp
hyperplasia10 PMB 58 Two benign polyps (8 cm and 3 cm), and background simple endometrial hyperplasia No endometrial abnormality1 1 PMB 81 Three benign polyps (16 cm, 4 cm and 4 cm) and background simple hyperplasia Malignant mixed Mullerian
and progestogen changes tumour12 Menorrhagia 47 Progestogen changes onlyt No endometrial abnormality13 Menorrhagia 49 Progestogen changes onlyt No endometrial abnormality14 Necropsy 85 Simple endometrial hyperplasia No endometrial abnormality15 Necropsy 91 Simple endometrial hyperplasia No endometrial abnormality16 PMB 58 Adenocarcinoma with focal sarcomatous differentiation and extensive Endometrial hyperplasia
myometrial infiltration17 Menorrhagia 49 Invasive well differentiated adenocarcinoma with extensive mayometrial invasion No endometrial abnormality18 PMB 70 Background simple endometrial hyperplasia, multiple hyperplastic polyps with No endometrial abnormality
varying degrees of cytological atypia, and a polypoid superficial carcinoma19t PMB 62 Background simple endometrial hyperplasia and multiple benign polyps with foci Endometrial carcinoma
of superficial carcinoma20* Necropsy 76 Background hyperplasia with focal atypia and benign polyp with microscopic focus
of adenocarcinoma
*Same patienttExternal cases
tRecent progestogen therapy
Ismail
on 1 Septem
ber 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.47.9.827 on 1 S
eptember 1994. D
ownloaded from
Pathology of endometrium treated with tamoxifen
(A)
:<+ory. o i. 6 5 7 ^ * <*+~~o
¢s-r - -- St
o4
~ ~ ~ 4.^ * ,. * ¢4#
(B)
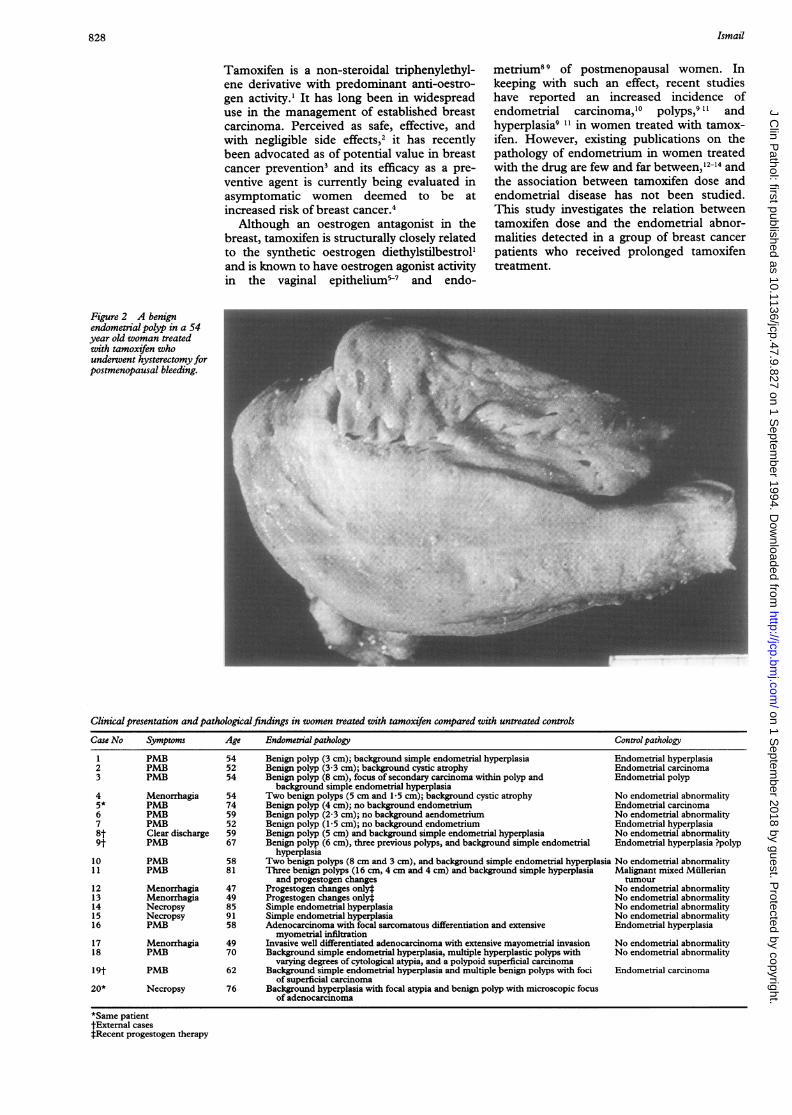
Figure 3 Microscopically, tamoxifen-associated benign endometrial polyps were
characterised by a combination of (A) focal periglandular condensation of stromal ce
(B) mitotic activity in epithelial and stromal cells, and a range of epithelial metapla(haematoxylin and eosin).
I. *7 ",,las
aI.!:*,.'. -.a *
(A)
Figure 4 The range of epithelial metaplasias seen in tamoxifen-associated benignendometrial polyps included (A) squamoid metaplasia.
MethodsThe study population comprised 19 breastcancer patients treated with tamoxifen. The
< data were collected prospectively between1987 and 1992. It includes two necropsies, 14
tz8 women who underwent surgery at the> University Hospital of Wales for tamoxifen-
Vl .'} associated gynaecological symptoms, ande. three patients treated at other hospitals in the
area.The two necropsy patients, aged 85 and 92,
.X4it. had died of myocardial infarction and lobarpneumonia, respectively. Neither was knownto have had any gynaecological symptoms andthere was no history in either woman of anyother hormone treatment.
:tvw The symptomatic patients ranged in<4L> age from 47 to 81 years (mean 58-5 years)j>ve. and presented with prolonged irregular
' perimenopausal bleeding (n = 4), postmenopausal bleeding (n = 12), or vaginal dis-
3W' charge (n = 1). Treatment consisted of eithere L polypectomy (n = 5) or hysterectomy (n =
12). Three patients had received progestogensF 0 ^ for menorrhagia but none had received any
' other form of endocrine treatment.b The specimens were fixed in 10% buffered
' *;, formalin and routinely processed. Every spec-imen was ascribed a pathological diagnosisfollowing examination of the haematoxylinand eosin stained sections and before tamox-ifen dose was known. Information about daily
M tamoxifen dose and duration of treatment wasobtained from the case notes. The cumulativedose of tamoxifen was calculated from thedaily dose of the drug and the duration oftreatment, taking into account recorded alter-ations in daily dose and assuming that thereare 30 days per calendar month.
+ A control group, matched as closely aspossible to the study group for age at presenta-tion, was selected for comparison. The meanage of the control patients was 608 years
tlls, while the mean age of the test group was 61 8siasyears.Two postmenopausal breast cancer
,\4 patients who had received no tamoxifen orany other endocrine treatment, had had nogynaecological symptoms, and who haddied over the study period were selected ascontrols for the two asymptomatic test
N< cases.The symptomatic group of study patients
was compared with a control group of age-* matched women presenting with identical%5~ symptoms over the last two years of the study.f None of the patients in this control group had
breast cancer and none had received tamox-!^' ifen, hormone replacement therapy, or any
- other endocrine treatment which might haveaffected endometrial morphology.
ResultsThe results are summarised in the table. One
'C test patient (case 5) features twice, having hada benign endometrial polyp after 16 monthsof tamoxifen treatment and a superficialendometrial carcinoma in a second endome-
829
#z.. 4p
$1
k.
6ANk 4.
.4
on 1 Septem
ber 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.47.9.827 on 1 S
eptember 1994. D
ownloaded from
830
T, ; * , > ,tA-X*
6t X |¢g, p
/;i 2 '
r'-atXl B1'> K ;gs
E.ti '4 .^ A t
; ~ ~w < _ .. * ;'Ai ~ t
tv A ',4
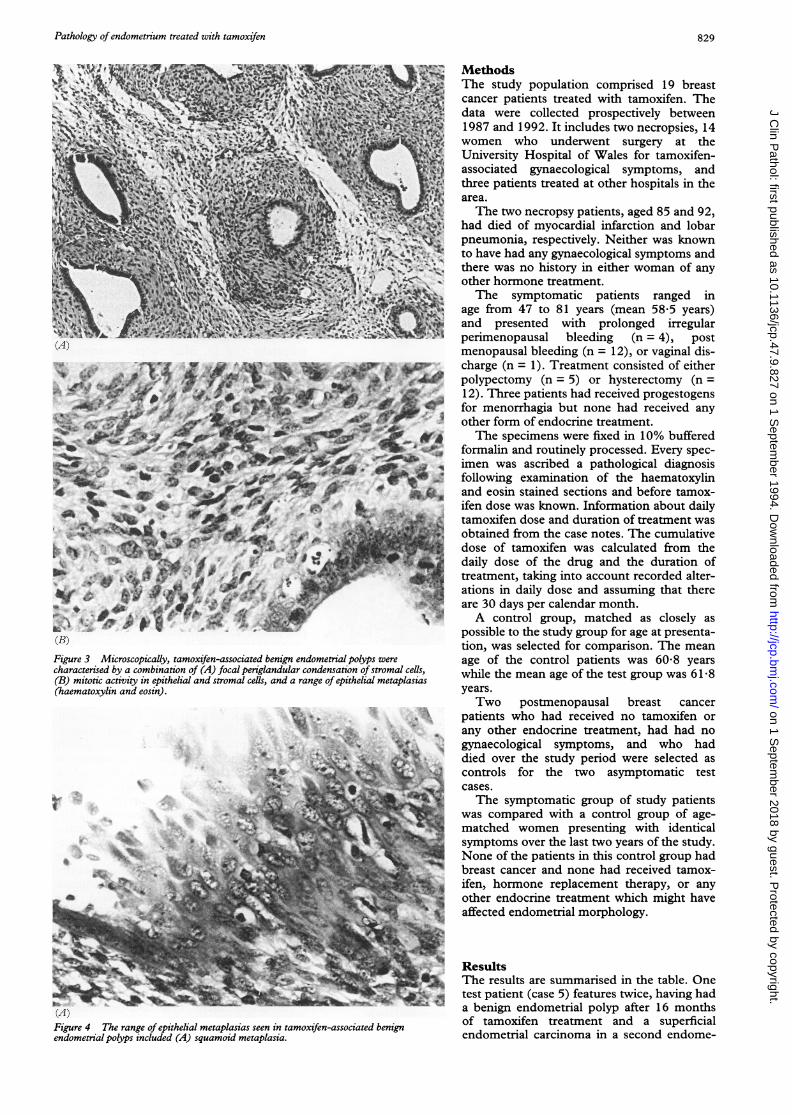
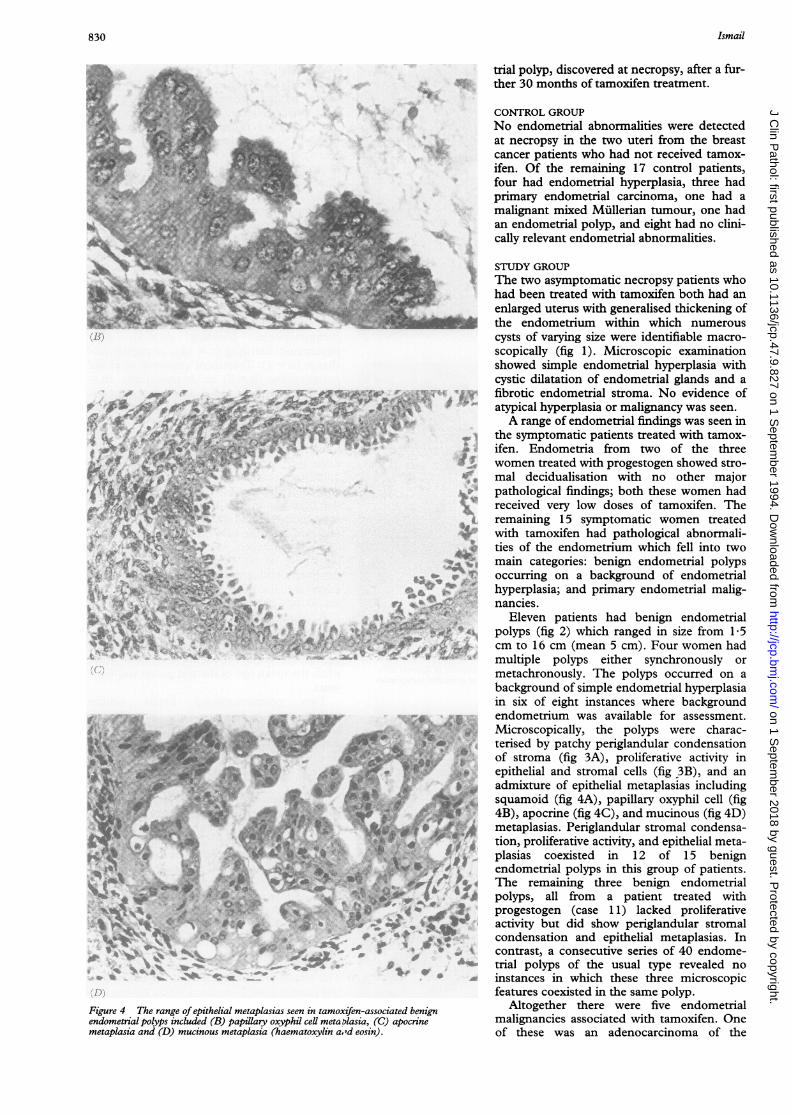
Figure 4 The range of epithelial metaplasias seen in tamoxifen-associated benignendometrial polyps included (B) papillary oxyphil cell meta plasia, (C) apocrinemetaplasia and (D) mucinous metaplasia (haematoxylin a.rd eosin).
trial polyp, discovered at necropsy, after a fur-ther 30 months of tamoxifen treatment.
CONTROL GROUPNo endometrial abnormalities were detectedat necropsy in the two uteri from the breastcancer patients who had not received tamox-ifen. Of the remaining 17 control patients,four had endometrial hyperplasia, three hadprimary endometrial carcinoma, one had amalignant mixed Miillerian tumour, one hadan endometrial polyp, and eight had no clini-cally relevant endometrial abnormalities.
STUDY GROUPThe two asymptomatic necropsy patients whohad been treated with tamoxifen both had anenlarged uterus with generalised thickening ofthe endometrium within which numerouscysts of varying size were identifiable macro-scopically (fig 1). Microscopic examinationshowed simple endometrial hyperplasia withcystic dilatation of endometrial glands and afibrotic endometrial stroma. No evidence ofatypical hyperplasia or malignancy was seen.A range of endometrial findings was seen in
the symptomatic patients treated with tamox-ifen. Endometria from two of the threewomen treated with progestogen showed stro-mal decidualisation with no other majorpathological findings; both these women hadreceived very low doses of tamoxifen. Theremaining 15 symptomatic women treatedwith tamoxifen had pathological abnormali-ties of the endometrium which fell into twomain categories: benign endometrial polypsoccurring on a background of endometrialhyperplasia; and primary endometrial malig-nancies.
Eleven patients had benign endometrialpolyps (fig 2) which ranged in size from 1-5cm to 16 cm (mean 5 cm). Four women hadmultiple polyps either synchronously ormetachronously. The polyps occurred on abackground of simple endometrial hyperplasiain six of eight instances where backgroundendometrium was available for assessment.Microscopically, the polyps were charac-terised by patchy periglandular condensationof stroma (fig 3A), proliferative activity inepithelial and stromal cells (fig 3B), and anadmixture of epithelial metaplasias includingsquamoid (fig 4A), papillary oxyphil cell (fig4B), apocrine (fig 4C), and mucinous (fig 4D)metaplasias. Periglandular stromal condensa-tion, proliferative activity, and epithelial meta-plasias coexisted in 12 of 15 benignendometrial polyps in this group of patients.The remaining three benign endometrialpolyps, all from a patient treated withprogestogen (case 11) lacked proliferativeactivity but did show periglandular stromalcondensation and epithelial metaplasias. Incontrast, a consecutive series of 40 endome-trial polyps of the usual type revealed noinstances in which these three microscopicfeatures coexisted in the same polyp.
Altogether there were five endometrialmalignancies associated with tamoxifen. Oneof these was an adenocarcinoma of the
Ismail
on 1 Septem
ber 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.47.9.827 on 1 S
eptember 1994. D
ownloaded from
Pathology of endometrium treated with tamoxifen
(A)
O
..1s.O
*--%r .~~~~~~~~~~~~~~~~~~-.vt-
4~~~41' .~~~~~~~~~~ sit'~~~~~~~~~~~j
c'!r~ ~~f'
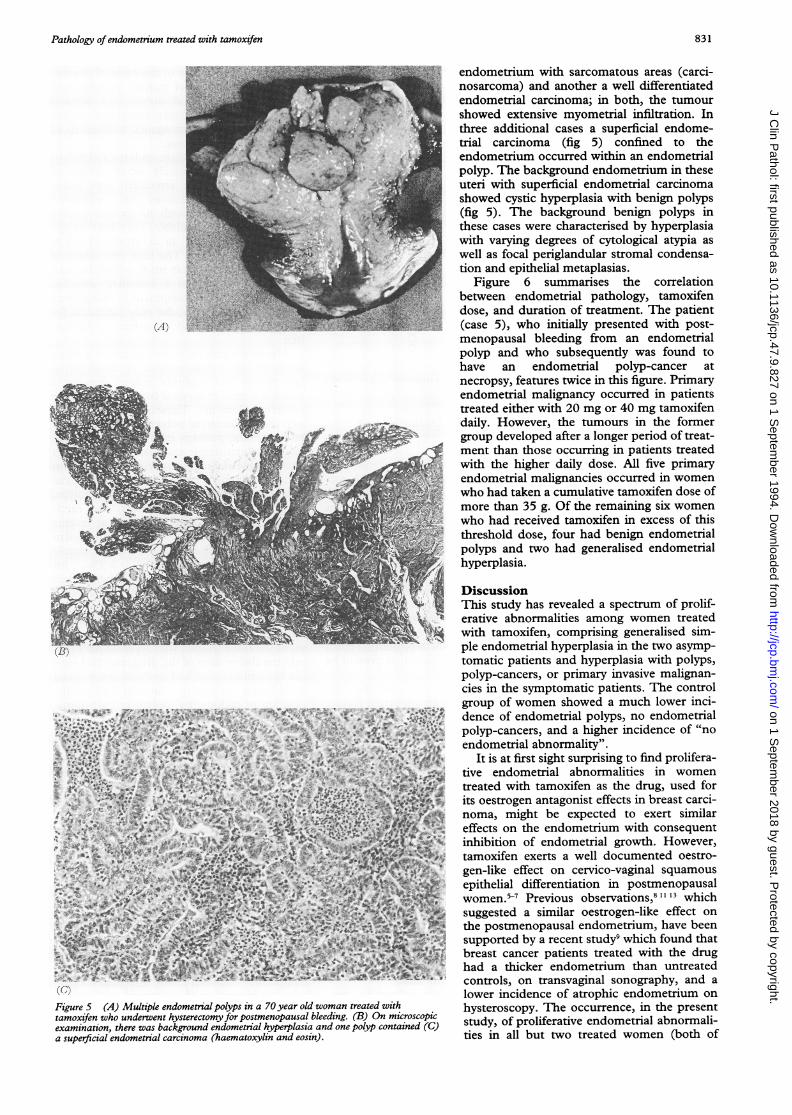
Figure 5 (A) Multiple endometrial polyps in a 70 year old woman treated withtamoxifen who underwent hysterectomy for postmenopausal bleeding (B) On microscopicexamination, there was background endometrial hyperplasia and one polyp contained (C)a superficial endometrial carcinoma (haematoxylin and eosin).
endometrium with sarcomatous areas (carci-nosarcoma) and another a well differentiatedendometrial carcinoma; in both, the tumourshowed extensive myometrial infiltration. Inthree additional cases a superficial endome-trial carcinoma (fig 5) confined to theendometrium occurred within an endometrialpolyp. The background endometrium in theseuteri with superficial endometrial carcinomashowed cystic hyperplasia with benign polyps(fig 5). The background benign polyps inthese cases were characterised by hyperplasiawith varying degrees of cytological atypia aswell as focal periglandular stromal condensa-tion and epithelial metaplasias.
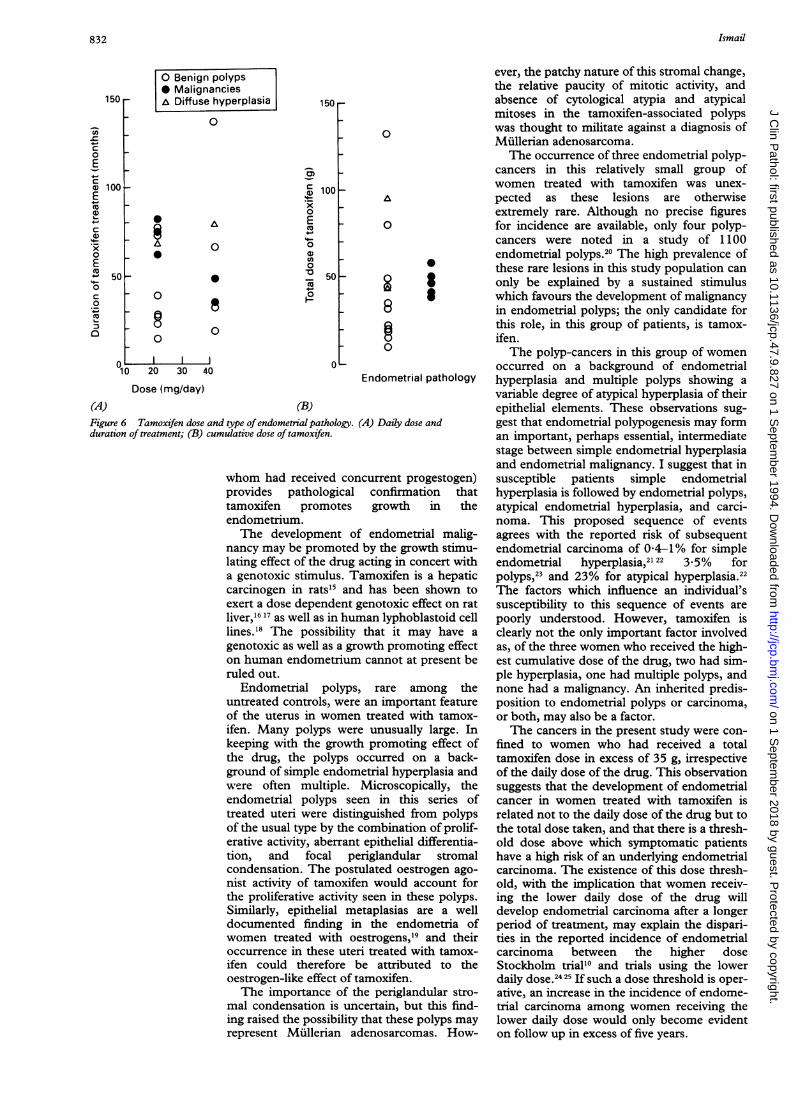
Figure 6 summarises the correlationbetween endometrial pathology, tamoxifendose, and duration of treatment. The patient(case 5), who initially presented with post-menopausal bleeding from an endometrialpolyp and who subsequently was found tohave an endometrial polyp-cancer atnecropsy, features twice in this figure. Primaryendometrial malignancy occurred in patientstreated either with 20 mg or 40 mg tamoxifendaily. However, the tumours in the formergroup developed after a longer period of treat-ment than those occurring in patients treatedwith the higher daily dose. All five primaryendometrial malignancies occurred in womenwho had taken a cumulative tamoxifen dose ofmore than 35 g. Of the remaining six womenwho had received tamoxifen in excess of thisthreshold dose, four had benign endometrialpolyps and two had generalised endometrialhyperplasia.
DiscussionThis study has revealed a spectrum of prolif-erative abnormalities among women treatedwith tamoxifen, comprising generalised sim-ple endometrial hyperplasia in the two asymp-tomatic patients and hyperplasia with polyps,polyp-cancers, or primary invasive malignan-cies in the symptomatic patients. The controlgroup of women showed a much lower inci-dence of endometrial polyps, no endometrialpolyp-cancers, and a higher incidence of "noendometrial abnormality".
It is at first sight surprising to find prolifera-tive endometrial abnormalities in womentreated with tamoxifen as the drug, used forits oestrogen antagonist effects in breast carci-noma, might be expected to exert similareffects on the endometrium with consequentinhibition of endometrial growth. However,tamoxifen exerts a well documented oestro-gen-like effect on cervico-vaginal squamousepithelial differentiation in postmenopausalwomen.5 Previous observations,81' 13 whichsuggested a similar oestrogen-like effect onthe postmenopausal endometrium, have beensupported by a recent study9 which found thatbreast cancer patients treated with the drughad a thicker endometrium than untreatedcontrols, on transvaginal sonography, and alower incidence of atrophic endometrium onhysteroscopy. The occurrence, in the presentstudy, of proliferative endometrial abnormali-ties in all but two treated women (both of
831
on 1 Septem
ber 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.47.9.827 on 1 S
eptember 1994. D
ownloaded from
832
O Benign polyps* MalignanciesA Diffuse hyperplasia
0
i A
0
50 _
0
8e
1o0300
10 20 30 40
C
a)x0E0
00en
0O
16
150
100
50
Dose (mg/day)
0
A
0
0
2 I8
Endometrial pathology
(B)Figure 6 Tamoxifen dose and type of endometrial pathology.duration of treatment; (B) cumulative dose of tamoxifen.
(A) Daily dose and
whom had received concurrent progestogen)provides pathological confirmation thattamoxifen promotes growth in theendometrium.The development of endometrial malig-
nancy may be promoted by the growth stimu-lating effect of the drug acting in concert witha genotoxic stimulus. Tamoxifen is a hepaticcarcinogen in rats"5 and has been shown toexert a dose dependent genotoxic effect on ratliver,'6 17 as well as in human lyphoblastoid celllines.'8 The possibility that it may have a
genotoxic as well as a growth promoting effecton human endometrium cannot at present beruled out.
Endometrial polyps, rare among theuntreated controls, were an important featureof the uterus in women treated with tamox-ifen. Many polyps were unusually large. Inkeeping with the growth promoting effect ofthe drug, the polyps occurred on a back-ground of simple endometrial hyperplasia andwere often multiple. Microscopically, theendometrial polyps seen in this series oftreated uteri were distinguished from polypsof the usual type by the combination of prolif-erative activity, aberrant epithelial differentia-tion, and focal periglandular stromalcondensation. The postulated oestrogen ago-nist activity of tamoxifen would account forthe proliferative activity seen in these polyps.Similarly, epithelial metaplasias are a welldocumented finding in the endometria ofwomen treated with oestrogens,'9 and theiroccurrence in these uteri treated with tamox-ifen could therefore be attributed to theoestrogen-like effect of tamoxifen.The importance of the periglandular stro-
mal condensation is uncertain, but this find-ing raised the possibility that these polyps mayrepresent Mullerian adenosarcomas. How-
ever, the patchy nature of this stromal change,the relative paucity of mitotic activity, andabsence of cytological atypia and atypicalmitoses in the tamoxifen-associated polypswas thought to militate against a diagnosis ofMiillerian adenosarcoma.The occurrence of three endometrial polyp-
cancers in this relatively small group ofwomen treated with tamoxifen was unex-pected as these lesions are otherwiseextremely rare. Although no precise figuresfor incidence are available, only four polyp-cancers were noted in a study of 1100endometrial polyps.20 The high prevalence ofthese rare lesions in this study population canonly be explained by a sustained stimuluswhich favours the development of malignancyin endometrial polyps; the only candidate forthis role, in this group of patients, is tamox-ifen.The polyp-cancers in this group of women
occurred on a background of endometrialhyperplasia and multiple polyps showing avariable degree of atypical hyperplasia of theirepithelial elements. These observations sug-gest that endometrial polypogenesis may forman important, perhaps essential, intermediatestage between simple endometrial hyperplasiaand endometrial malignancy. I suggest that insusceptible patients simple endometrialhyperplasia is followed by endometrial polyps,atypical endometrial hyperplasia, and carci-noma. This proposed sequence of eventsagrees with the reported risk of subsequentendometrial carcinoma of 04-1% for simpleendometrial hyperplasia,"2 3*5% forpolyps,2 and 23% for atypical hyperplasia."The factors which influence an individual'ssusceptibility to this sequence of events arepoorly understood. However, tamoxifen isclearly not the only important factor involvedas, of the three women who received the high-est cumulative dose of the drug, two had sim-ple hyperplasia, one had multiple polyps, andnone had a malignancy. An inherited predis-position to endometrial polyps or carcinoma,or both, may also be a factor.The cancers in the present study were con-
fined to women who had received a totaltamoxifen dose in excess of 35 g, irrespectiveof the daily dose of the drug. This observationsuggests that the development of endometrialcancer in women treated with tamoxifen isrelated not to the daily dose of the drug but tothe total dose taken, and that there is a thresh-old dose above which symptomatic patientshave a high risk of an underlying endometrialcarcinoma. The existence of this dose thresh-old, with the implication that women receiv-ing the lower daily dose of the drug willdevelop endometrial carcinoma after a longerperiod of treatment, may explain the dispari-ties in the reported incidence of endometrialcarcinoma between the higher doseStockholm trial'0 and trials using the lowerdaily dose.2425 If such a dose threshold is operative, an increase in the incidence of endome-trial carcinoma among women receiving thelower daily dose would only become evidenton follow up in excess of five years.
150
100
'ac0EC0
I.0CG)
4-.
x0Em0C0.0_4J
(A)
Ismail
5
0
on 1 Septem
ber 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.47.9.827 on 1 S
eptember 1994. D
ownloaded from

Pathology ofendometrium treated with tamoxifen
The ongoing breast cancer prevention trialsusing long term tamoxifen in asymptomaticwomen have imparted urgency to the study ofthe endometrial effects of this drug. The find-ings of this small study support a link betweentamoxifen and endometrial cancer and indi-cate that gynaecological symptoms in womentreated with tamoxifen warrant full investiga-tion. They suggest a pathogenetic relationbetween polypoid endometrial hyperplasiaand malignancy and identify a subgroup ofpatients (those who have taken more than 35 gof tamoxifen) who may be at increased risk ofharbouring endometrial cancer. It is recom-mended that tamoxifen registers be estab-lished to facilitate adequate follow up ofwomen receiving prolonged tamoxifen treat-ment and to determine the incidence ofendometrial pathology associated with the useof this drug.
I thank Professor Sir Dillwyn Williams and Dr RobertNewcombe for helpful discussions. Drs John Dinnen (CountyHospital, Hereford), Gareth Melville-Jones (WithybushGeneral Hospital), and Windsor Fortt (Royal Gwent Hospital)contributed the outside cases.
1 Furr BJA, Jordan VC. The pharmacology and clinical usesof tamoxifen. Pharnacol Ther 1984;25:127-205.
2 Baum M, Brinkley DM, Dosset JA, McPherson K, JacksonIM, Rubens RD, et al. Controlled trial of tamoxifen as asingle adjuvant agent in management of early breastcancer. BrJ Cancer 1988;57:608-11.
3 Nayfield SG, Karp JE, Ford LG, Dorr FA, Kramer BS.Potential role of tamoxifen in prevention of breast can-cer. JNCI 199 1;83:1450-9.
4 Powles TJ. The case for clinical trials of tamoxifen for pre-vention of breast cancer. Lancet 1992;340:1145-7.
5 Ferrazzi E, Cartei G, Mattarazzo R, Fiorentino M.Oestrogen-like effect of tamoxifen on vaginal epithelium.BrMedJ 1977;1:1351-2.
6 Boccardo F, Bruzzi P, Rubagotti A, Nicol6 G, Rosso R.Estrogen-like action of tamoxifen on vaginal epitheliumof breast cancer patients. Oncology 1981;30:281-5.
7 Eells TP, Alpern HD, Grzywacz C, MacMillan RW, OlsonJE. The effect of tamoxifen on cervical squamous matu-ration in Papanicolau stained cervical smears of post-menopausal women. Cytopathology 1990;1:263-8.
8 Boccardo F, Guarnieri D, Rubagotti A, Casertelli GL,Bentivoglio G, Conte N et al. Endocrine effects of
tamoxifen in postmenopausal breast cancer patients.Tumori 1984;70:61-8.
9 Lahti E, Blanco G, Kauppila A, Apala-Sarkkinen M,Taskinen PJ, Laatikainen T. Endometrial changes inpostmenopausal breast cancer patients receiving tamox-ifen. Obstet Gynecol 1993;81:660-4.
10 Fornander T, Rutqvist LE, Cedermark B, Glas V,Mattson A, Siltversward C, et al. Adjuvant tamoxifen inearly breast cancer: occurrence of new primary tumours.Lancet 1989;i: 117-20.
11 Neven P, De Muylder X, Van Belle Y, Venderick G, DeMuylder E. Tamoxifen and the uterus andendometrium. Lancet 1989;i:375.
12 Nuovo MA, Nuovo GJ, McCaffrey RM, Levine RU,Barron B, Winkler B. Endometrial polyps in post-menopausal patients receiving tamoxifen. Int J GynecolPathol 1989;8:125-31.
13 Cross SS, Ismail SM. Endometrial hyperplasia in anoophorectomized woman receiving tamoxifen therapy.Case report. BrJ Obstet Gynaecol 1990;97:551-2.
14 Corley D, Rowe J, Curtis MT, Hogan WM, NoumoffJS,Livolsi VA. Postmenopausal bleeding from unusualendometrial polyps in women on chronic tamoxifentherapy. Obstet Gynecol 1992;79: 111-6.
15 Williams GM, Iatropoulos MJ, Djordjevic MV, KaltenbergOP. The triphenylethylene drug tamoxifen is a strongliver carcinogen in the rat. Carcinogenesis 1993;13:315-7.
16 Han XH, Liehr JG. Induction of covalent DNA adducts inrodents by tamoxifen. Cancer Res 1992;52:1360-3.
17 White INH, De Matteis F, Davies A, et al. Genotoxicpotential of tamoxifen and analogues in female FischerF344/n rats, DBA/2 and C57BLt6 mice and in humanMCL-5 cells. Carcinogenesis 1992;13:2197-203.
18 Styles JA, Davies A, Lim CK, De Matteis F, Stanley LA,White INH, et al. Genotoxicity of tamoxifen, tamoxifenepoxide and toremifene in human lymphoblastoid cellscontaining human cytochrome P450s. Carcinogenesis1994;14:5-9.
19 Hendrickson MR, Kempson RL. Endometrial epithelialmetaplasias: Proliferations frequently misdiagnosed asadenocarcinoma. Report of 89 cases and proposed classi-fication. Am j Surg Pathol 1980;4:525-42.
20 Peterson WF, Novak ER. Endometrial polyps. ObstetGynecol 1956;8:40-9.
21 McBride JM. Pre-menopausal cystic hyperplasia andendometrial carcinoma. J Obstet Gynaecol Br Emp1959;66:288-96.
22 Kurman RJ, Kaminski PF, Norris HJ. The behavior ofendometrial hyperplasia. A long-term study of"untreated" hyperplasia in 170 patients. Cancer 1985;56:403-12.
23 Armenia CS. Sequential relationship between endometrialpolyps and carcinoma of the endometrium. ObstetGynecol 1967;30:524-9.
24 Breast Cancer Trials Committee, Scottish Cancer TrialsOffice (MRC), Edinburgh. Adjuvant tamoxifen in themanagement of operable breast cancer: The ScottishTrial. Lancet 1987ii: 171-5.
25 Fisher B, Costantino J, Redmond C, Bowman D, CoutureJ, Poisson R, et al. A randomized clinical trial evaluatingtamoxifen in the treatment of patients with nodenegative breast cancer who have estrogen-receptor-positive tumours. N Engl J Med 1989;320:479-84.
833
on 1 Septem
ber 2018 by guest. Protected by copyright.
http://jcp.bmj.com
/J C
lin Pathol: first published as 10.1136/jcp.47.9.827 on 1 S
eptember 1994. D
ownloaded from