Embed Size (px)
Citation preview

JIKI Trial In Guinea Reaction Project
Daouda Sissoko, on behalf of JIKI group Center for tropical medicine and clinical international
health, University Hospital Center, Bordeaux INSERM 897, University of Bordeaux, France
INSERM Guinea/ National Task Force against Ebola
No conflict of interest to declare
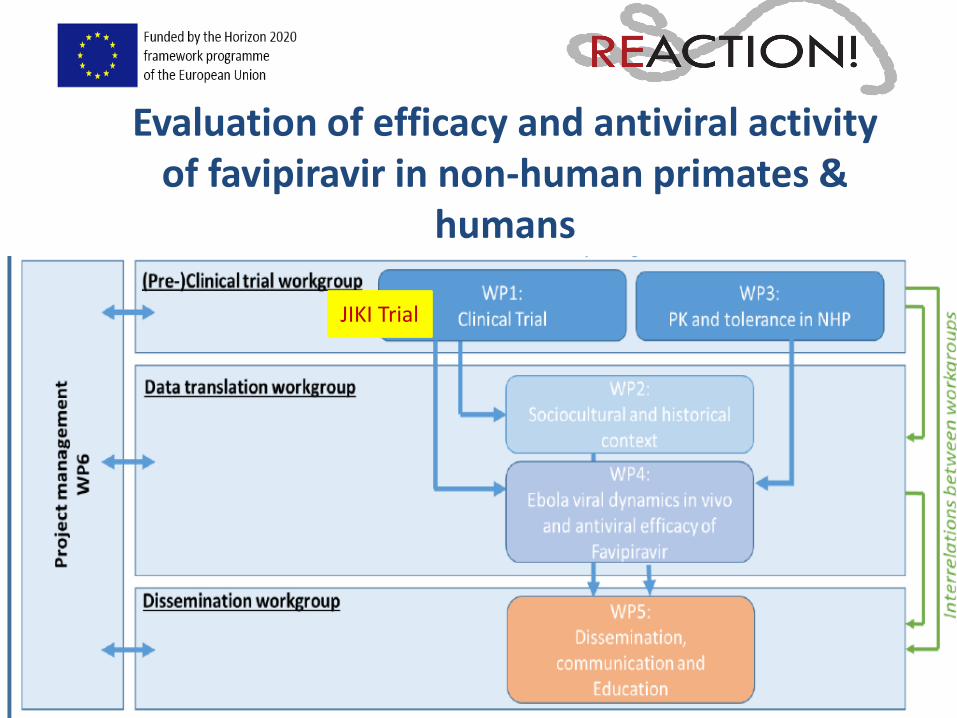
Evaluation of efficacy and antiviral activity
of favipiravir in non-human primates & humans
JIKI Trial

JIKI Trial preparation and progress
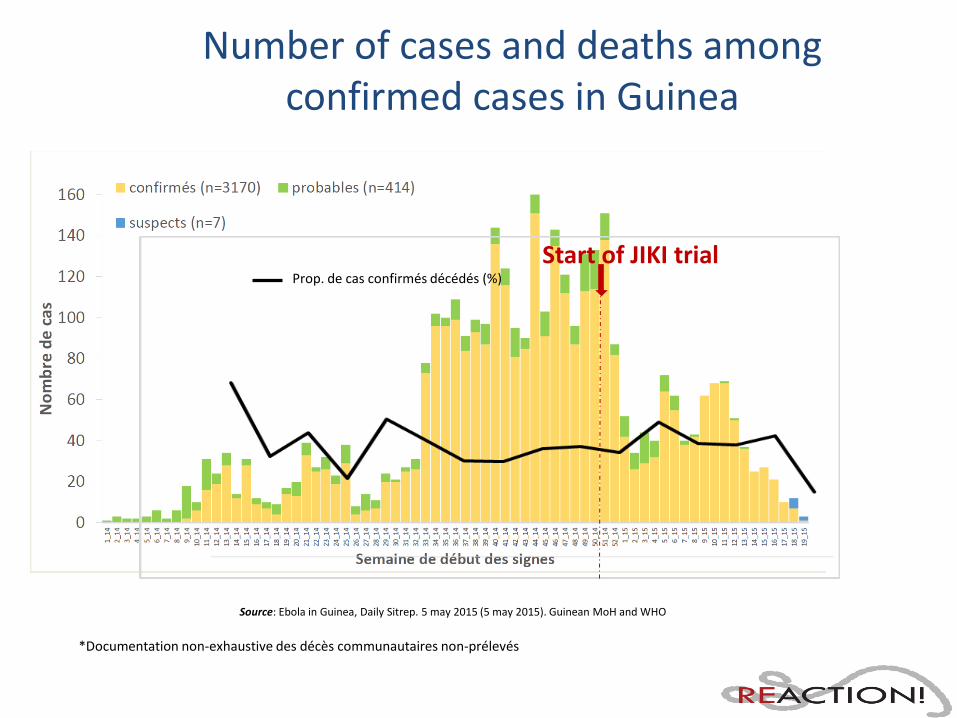
Number of cases and deaths among confirmed cases in Guinea
Source: Ebola in Guinea, Daily Sitrep. 5 may 2015 (5 may 2015). Guinean MoH and WHO
Start of JIKI trial Prop. de cas confirmés décédés (%)
*Documentation non-exhaustive des décès communautaires non-prélevés
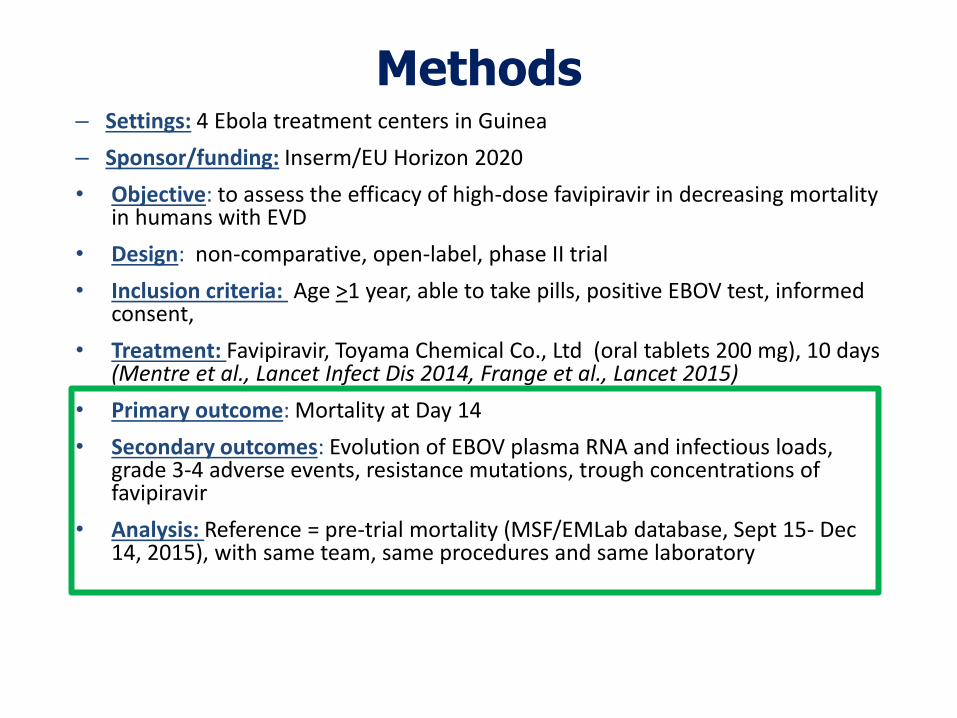
Methods – Settings: 4 Ebola treatment centers in Guinea
– Sponsor/funding: Inserm/EU Horizon 2020
• Objective: to assess the efficacy of high-dose favipiravir in decreasing mortality in humans with EVD
• Design: non-comparative, open-label, phase II trial
• Inclusion criteria: Age >1 year, able to take pills, positive EBOV test, informed consent,
• Treatment: Favipiravir, Toyama Chemical Co., Ltd (oral tablets 200 mg), 10 days (Mentre et al., Lancet Infect Dis 2014, Frange et al., Lancet 2015)
• Primary outcome: Mortality at Day 14
• Secondary outcomes: Evolution of EBOV plasma RNA and infectious loads, grade 3-4 adverse events, resistance mutations, trough concentrations of favipiravir
• Analysis: Reference = pre-trial mortality (MSF/EMLab database, Sept 15- Dec 14, 2015), with same team, same procedures and same laboratory
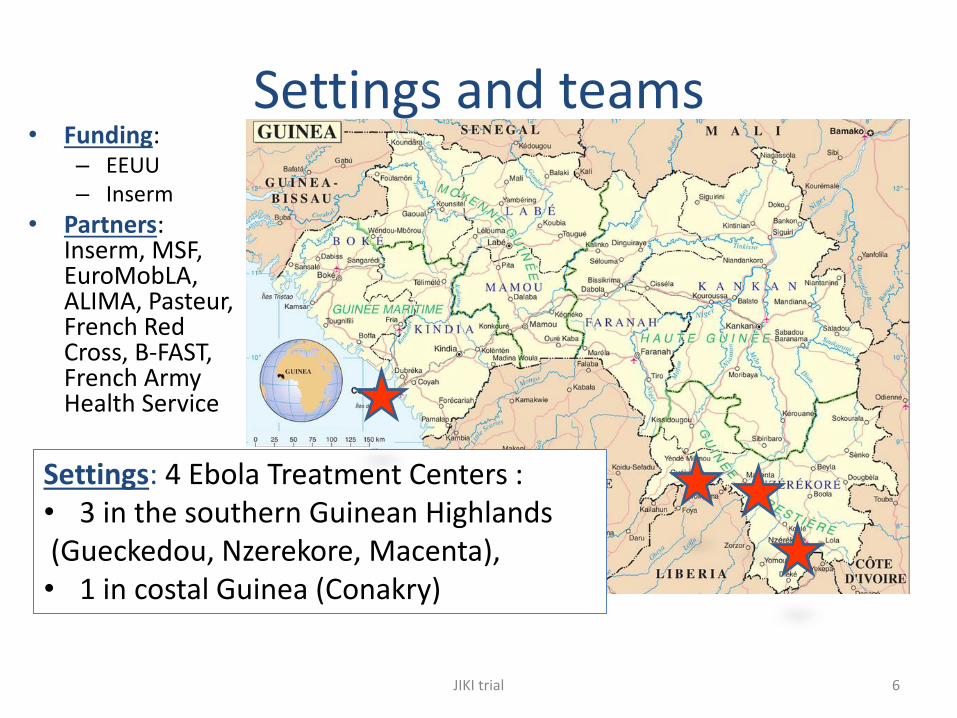
Settings and teams
JIKI trial 6
• Funding: – EEUU – Inserm
• Partners: Inserm, MSF, EuroMobLA, ALIMA, Pasteur, French Red Cross, B-FAST, French Army Health Service
Settings: 4 Ebola Treatment Centers : • 3 in the southern Guinean Highlands (Gueckedou, Nzerekore, Macenta), • 1 in costal Guinea (Conakry)
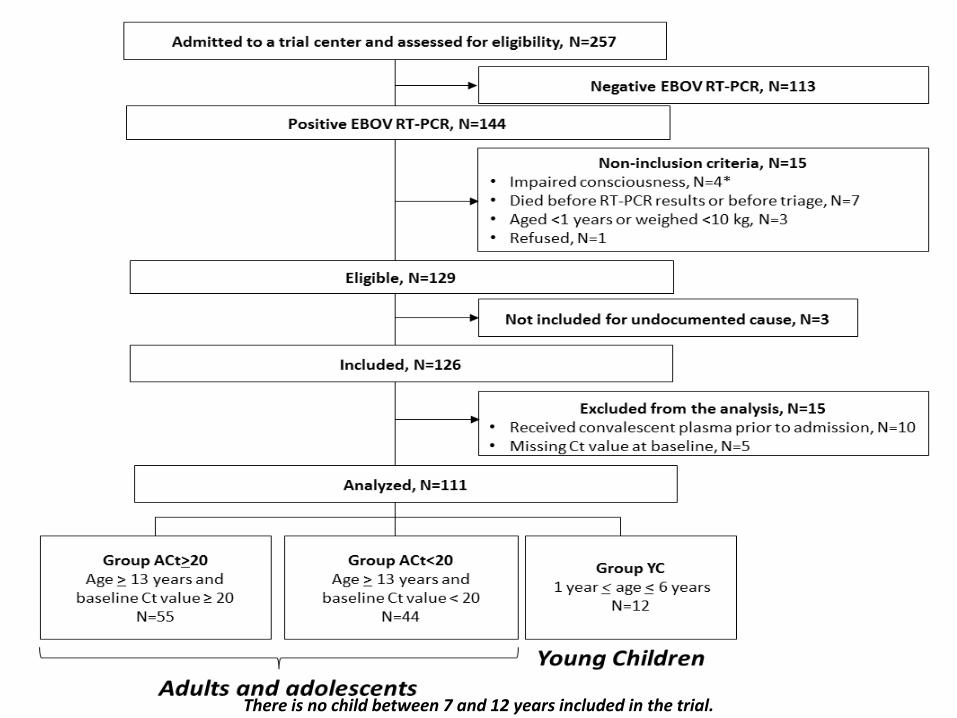
Flow chart
7
There is no child between 7 and 12 years included in the trial.
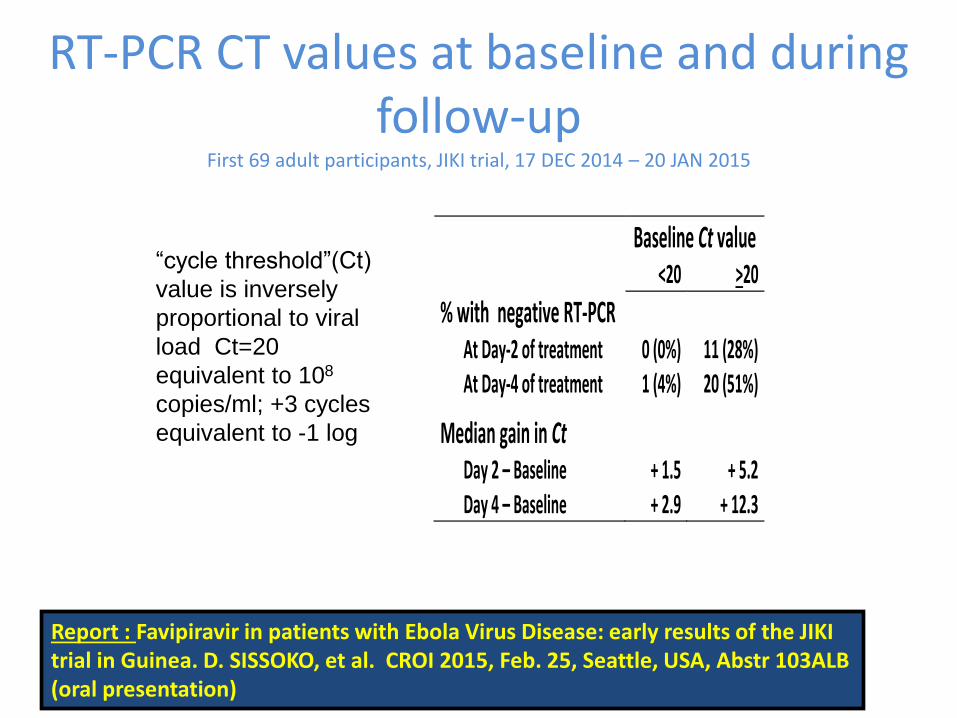
RT-PCR CT values at baseline and during follow-up
First 69 adult participants, JIKI trial, 17 DEC 2014 – 20 JAN 2015
JIKI trial 8
Baseline Ct value <20 >20
% with negative RT-PCR
At Day-2 of treatment 0 (0%) 11 (28%) At Day-4 of treatment 1 (4%) 20 (51%)
Median gain in Ct
Day 2 – Baseline + 1.5 + 5.2 Day 4 – Baseline + 2.9 + 12.3
“cycle threshold”(Ct)
value is inversely
proportional to viral
load Ct=20
equivalent to 108
copies/ml; +3 cycles
equivalent to -1 log
Report : Favipiravir in patients with Ebola Virus Disease: early results of the JIKI trial in Guinea. D. SISSOKO, et al. CROI 2015, Feb. 25, Seattle, USA, Abstr 103ALB (oral presentation)
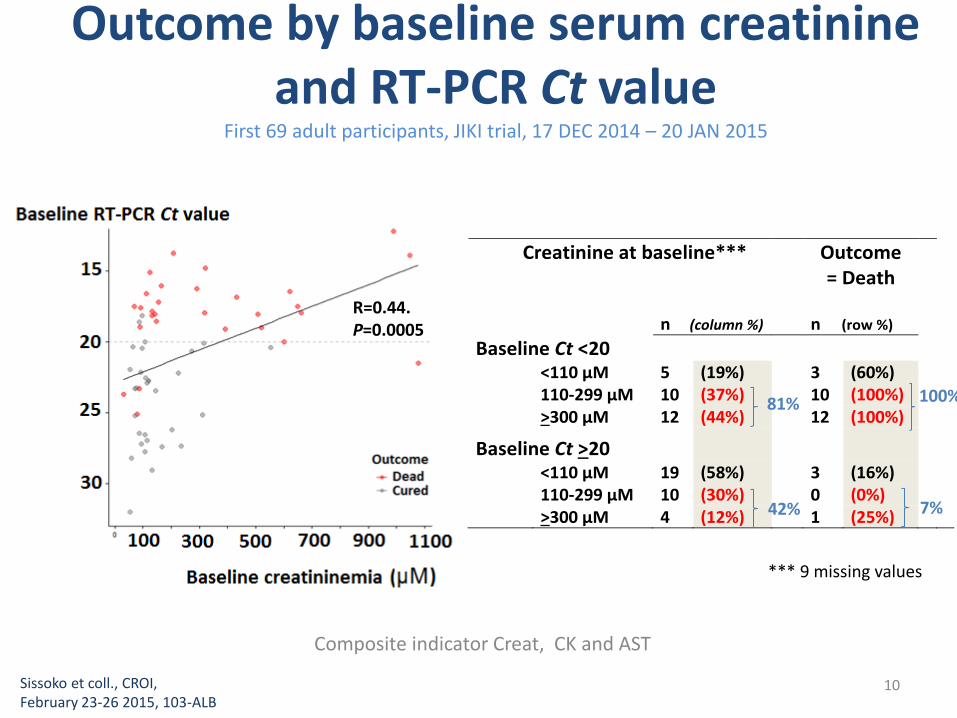
Outcome by baseline serum creatinine and RT-PCR Ct value
First 69 adult participants, JIKI trial, 17 DEC 2014 – 20 JAN 2015
Composite indicator Creat, CK and AST
10 Sissoko et coll., CROI, February 23-26 2015, 103-ALB
*** 9 missing values
Creatinine at baseline*** Outcome = Death
n (row %)
n (column %)
Baseline Ct <20
<110 μM 5 (19%) 3 (60%) 110-299 μM 10 (37%) 10 (100%) >300 μM 12 (44%) 12 (100%)
Baseline Ct >20
<110 μM 19 (58%) 3 (16%) 110-299 μM 10 (30%) 0 (0%) >300 μM 4 (12%) 1 (25%)
81%
42% 7%
R=0.44. P=0.0005
100%
Comments • RT-PCR Ct value and serum creatinine are two excellent markers of disease
severity :
– 50% of patients showed up with a Ct value < 20 (equivalent to 108 copies/ml)
– 52% of patients showed up with AKI
– 81% of patients with baseline Ct < 20 had persistent AKI; 100% died
– 42% of patients with baseline Ct > 20 had transient AKI; 97% recovered
• Final analyses stratified by baseline CT values
• Feasability of use, tolerability, safety, prospective standardized clinical, virology and biomarker data collection
• Further PK analysis undergoing to optimize the dosing
Concentrations measurements and link with viral load decrease and survival
• Final results over 200 (126 trial, 98 therapeutic cohort) patients to be produced
(data under reviewing, october 2015)
Sissoko et coll. CROI, February 23-26 2015, 103-ALB JIKI trial 11
Conclusions/ Perspectives • Emergency trials are feasible in the context of a
deadly contagious disease outbreak
• Efficay in patients with Ct≥20 (VL ≤ 7.7 log10 cp/ml) to be comforted by further studies (higher doses in RCT)
• Ongoing substudy: Clearance of semen among survivors
• Development of strong partnership with other European/West African teams (BNI/PHE, NGO, etc): cross-fertilization

Acknowledgements
JIKI trial 13 CROI, February 23-26 2015
Special thanks to:
• All patients who accepted to participate in the study
• Scientific Advisory Board: L Abel, G Carson, G Davies, A Diallo, P Frange, B Godard, A Kelly, F Le Marcis, N Morgensztejn,
A Ndjeyi Mbiguino, VK Nguyen, C Semaille, AM Taburet, JM Treluyer, Y Yazdanpanah
• Data Safety Monitoring Board: D Baush, B Bazin, E Bottieau, A Faye, R Garraffo, R Porcher, P Redfield
• Sponsor (Inserm): T Damerval, JF Delfraissy, Y Levy, C Levy-Marchal,
• Ethics Committees of Inserm (CEEI/IRB), MSF (MSF ERB), and Republic of Guinea (CNERS)
• Toyama Chemical Co., Ltd, for the donation of favipiravir: H Kitaguchi, K Yamada
The JIKI study group is constituted as follows:
– Guinea Ebola Task Force: S Keita
– Centre de Formation et de Recherche en Santé Rurale de Maferinyah: AH Beavogui
– MSF: I Arnould, A Antierens, N Bangoura, E Berbain, D Camara, FS Camara, S Carazo, AM Camara, L Delamou, B
Draguez, E Folkeson, MC Lamah, A Lefevre, T Leno, M Loua, K Malme, E Manfrin, A Maomou, S Ombelet, P Piguet,
M Poncin, OO Sakovogui, AY Sidiboun, A Tounkara, M Van Herp, D van Hoeydonck, I Verreckt
– ALIMA: B Abdoul, A Augier, G Baret, TS Barry, S Berrette, A Bongono, C Camara, M Conde, I Defourny, JM Dindart,
R Doumbouya, G Leduc, M Loua, R Lolamou FR Koundouno, S Harouna, V Massala, A Moumouni, P Mumbere, JP
Olele, R Palich, F Petitjean, O Peyrouset, C Provost, S Shepherd, C Sekou, A Soumah
– Croix Rouge Française: G Colin, D Dougo, P Gorovogui, E Olivier, Y Ruaux, B Simon, T Tran Minh, FT Simpogui
– Inserm: X Anglaret, M Cervantes-Gonzalez, S Eholie, X de Lamballerie, C Laouenan, D Malvy, F Mentre, R Moh, B
Murgue, C Nchot, L Nguessan, B Siloue, D Sissoko
– P4 Lyon Mérieux: S Baize, H Raoul
– EMLab: J Akoi Bore, M Carroll, S Diederich, S Duraffour, J Hinzmann, RF Koundouno, A Kraus, B Liedigk, P Maes, D
Ngabo, M Rudolf, R Thorn
– BFAST: Y Deccache, C Dumont, JF Durant JL Gala, L Irenge, B Smiths, N Toufic, S Van CauwenbergheSSA: H
Dampierre, V Foissaud, F Janvier, C Rapp, H Savini
– ADERA: O Fouassier, J Rivenc
– Solthis: A Abadie, R Benhamou, E Dortenzio, PE Martineau, L Pizarro

JIKI trial 14





























