Embed Size (px)
Citation preview

The American Journal of Human Genetics, Volume 98
Supplemental Data
A Syndromic Intellectual Disability Disorder
Caused by Variants in TELO2, a Gene Encoding
a Component of the TTT Complex
Jing You, Nara L. Sobreira, Dustin L. Gable, Julie Jurgens, Dorothy K. Grange, NewellBelnap, Ashley Siniard, Szabolcs Szelinger, Isabelle Schrauwen, Ryan F.Richholt, Stephanie E. Vallee, Mary Beth P. Dinulos, David Valle, MaryArmanios, and Julie Hoover-Fong

SupplementalMaterials
CaseReports
Family1:IndividualsII-2andII-3(17yearold,maleandfemale,respectively)are
fraternaltwins(seeFigure1)borntoa21yearoldmotherbyvaginaldeliveryfollowing
a35weekpregnancycomplicatedbypreeclampsia.Againstnormativebirthparameters
fortwingestation,birthweightswere1.9kg(10-25%)and1.7kg(5-10%),respectively,
andbirthlengthswere43.8cm(25%)and38.7cm(<3%).IndividualII-2had‘low’Apgar
scoresandremainedhospitalizedfor2-1/2weeksduetopoorfeedingandapnea.
IndividualII-3hadpoorrespiratoryeffortatbirthandrequiredresuscitationfor15
minuteswith‘low’Apgarscores.Acleftpalateandshrillcrywerenotedafterher
resuscitationandsheremainedhospitalizedfor1.5monthswithnasogastrictube
feeding.IndividualII-4wasbornattermwithbirthweightof2.8kg(10-25%)andbirth
length47.0cm(25%)anddischargedat1weekwithdifficultyfeedingandhypotonia.
Hehad10hypospadiasandfailedhisnewbornhearingscreen.
Frominfancy,individualII-2hadsymmetricalpoorgrowthanddelayeddevelopment.He
satindependentlyat2years,crawledat3yearsandstoodat4years,butwas
wheelchair-dependentbymid-childhoodduetoimpairedbalancethathasbecome
morepronouncedwithage.At17years,hecanholdapencilorutensilbutisunableto
writeorfeedhimselfindependently.Heoccasionallyusessinglewords,rarelymakes
eyecontact,andisdescribedas‘distantandwithdrawn’exceptintheevenings,when
hisbehaviorchangesdramaticallytouncontrollablelaughingandhugging.Whileawake,

hisbodyisconstantlymovingwithoutpurposebutwithoutoverttremororchorea.
Therehasbeenslowacquisitionbutnoregressionofskills.Hewasbornwithapatent
ductusarteriosus(PDA)andaventricularseptaldefect(VSD).Bothclosed
spontaneously,buthealsowasfoundtohaveadoubleaorticarchwithvascularring
andcleftmitralvalvewithmitralregurgitation.Thusfar,nocardiacsurgeryhasbeen
required.Hehasbilateralhearinglossandcorticalvisualimpairment(CVI).A
comprehensive,dilatedophthalmologicexamat17yearsofagerevealedgrosslynormal
eyestructure,butvisualacuitycouldnotbeassessedduetopoortracking/jerkypursuits
andnocompliance.Hewasdiagnosedwithautisminlatechildhood,basedonno
languageorcommunicationandrepetitive,self-stimulatorymovements.
Hypothyroidismwasdiagnosedat15years.Uponexaminationatage17years,weight
was28.7kg(-7.6SD),height130.4cm(-5.6SD)andOFC48.0cm(<<3%;50%for1.5
years).Hehasbrittlehair,bluesclera,darkcirclesunderhiseyes,anintactpalate,
pectuscarinatum,decreasedelbowextensionbutotherwisejointlaxity,broadgreat
toeswith4/5toesyndactyly,eczema,andgeneralizedhypotoniawithspasticity.Hehas
sparsefacialandpubichair.PriortoenrollmentforresearchWES,hehadseveral
normaltestsandstudiesincluding:brainMRI(2yearsofage),comparativegenomic
hybridization(10years),EEG(12years),serumuricacid,andmoleculartestingfor
fragileX.
IndividualII-3alsoexperiencedsymmetricpooroverallgrowthafterbirthassociated
withdelayeddevelopmentwithoutregression.Shesatindependentlyat5yearsofage

andhasneverwalked,butcanstandwithsupport.Shehasnowordsbutmakessounds
tocommunicate.Sheisthemostattentivetoherenvironmentofthethreeaffected
childreninFamily1.Sheoftenexhibitshandflappingwhensheisfrustrated,throws
herselfbackintoherwheelchairwhensheisangry,andhasanaffinityforwater.Her
cleftpalatewasrepairedat14monthsandsherequiredafrenulectomyfor
ankyloglossiaat3yearsofage.Sherequiredmultiplesetsoftypanostomytubesfor
otitismedia.Inearlychildhood,shewasfoundtohaveadoubleaorticarchwithan
atreticleftarchcreatinganincompletevascularringimpingingontheupperesophagus
butnotthetrachea.Hermedicalcoursewascomplicatedbyseveregastrointestinal
refluxdiseaseandrecurrentepisodesofaspirationpneumoniathatdiminished
followingG-tubeplacementatage12years.ShehasbilateralhearinglossandCVI.On
examat12and1/3years,herheightwas108.5cm(-6.1SD),weight18.1kg(-6.6SD),
andOFC47.0cm(<<3%,50%for1.5years).Shehadsynophrys,bluesclera,up-slanting
palpebralfissures,downturnedmouth,largetonguewithtetheredsublingualfrenulum,
torticollis,pectusexcavatum,anteriorlyplacedrectum,brachydactyly(middledigit<<
3%ile),4/5toesyndactyly,jointlaxity,andgeneralizedhypotonia.She,too,isin
constantmotionwhileawakewithspasticityinherlowerextremities.Shehasrotatory
nystagmus.Priortoenrollmentinthisresearch,shehadmultiplenormalclinicalstudies
including:karyotype,subtelomereand22q11FISH,7dehydrocholesterollevels,and
BACarray(4,000probes).

Followingbirth,individualII-4remainedinhospitalfordifficultyfeedingandhypotonia
untilage1week.Hisexamwasnotableforhypospadias.Hesatat15monthsbuthas
neverambulated.Hefailedhisnewbornhearingscreenandallsubsequenthearing
tests,andhasnospeech.Basedonhisbehavior,itisthoughtthathealsohasCVI.He
wasnotedtohaveanaccessoryoralfrenuliandcoarctationoftheaorta.Onexamat
age9years,hewassymmetricallysmallwithheight100.4cm(-5.9SD),weight15.1kg(-
6.3SD)andOFC46.5cm(<<3%for1year).Hehadbluesclera,alargemouthwiththin
upperlip,loosejoints,hypotonia,brachydactylyand5thfingerclinodactyly.Heexhibited
self-injuriousbehaviorduringtheexamwithconstantmotormovementandnowords.
Hehad3+patellarreflexesbutnospasticity.
Family2:
IndividualII-2isa5yearoldwhitefemalewhowasbornattermafteranuncomplicated
pregnancy.Shewasdeliveredvaginallytoa30yearold,gravida2,para1woman.Her
birthweightwas3.71kg(50%);length50.8cm(60%);andOFC35cm(60%).Concerns
regardingdelayeddevelopmentbeganat2months.Sherolledoverat5months,sat
aloneat8months,andwalkedat14months.At20monthssheknewabout20words,
butherparentsfeltherverbalskillsregressed.Ahearingtestat2yearsofagewas
normal.Atage30months,shehadformaltestingusingtheDevelopmentalAssessment
ofYoungChildren(DAYC-2)testwithadevelopmentalquotient(DQ)of55inexpressive
andlanguageskills,40infineandgrossmotorskills,40insocialskillsand37in
cognition.Shewasre-testedatage60monthsandscored<50inalldomains.

ShehadanormalcranialMRIatage2andstrabismussurgeryatage3.5yearsfor
intermittentesotropia.Shehashadachronicsleepdisturbancewithdifficultyfalling
asleepandoftenstayedawakescreamingduringthenight.AnEEGatage3and10/12
showedslightlyslowbackgroundactivitywith2briefburstsofbifrontalepileptiform
activity.Therehavebeennoclinicallydetectableseizures.
Physicalexamatage4and9/12revealedaheightof106cm(50%),aweightof16.8kg
(45%),andaheadcircumferenceof47.5cm(<3%,50%for18months).Shewasnon-
dysmorphicandambulatorywithintermittentabnormaltruncalmovements.
Examinationofherchest,spine,heartandabdomenwasnormalaswereherdeep
tendonreflexes.
Pertinentlaboratorytestingincludednormalchemistries;normal15qmethylation
testingforPraderWillisyndromeandAngelmansyndrome;normalMECP2sequencing
anddeletion/duplicationtesting;normaltransferrinisoelectricfocusingfor
carbohydratedeficienttransferrin;normalcreatinedisorderspanel;andnormalurine
purinesandpyrimidines.
Family3:
IndividualII-1isa17yearoldfemalewhowasbornat37.5weeksofgestationafteran
uncomplicatedpregnancy.Shewasdeliveredwithvacuumandforcepsassistancedue

tounspecifieddystocia.BirthweightisunknownandApgarscoreswerereportedas
“low”.ShehadpoorrespiratoryeffortandwasobservedintheNICUforseveralhours
butdischargedat2daysofage.Herparentsnotedslowacquisitionofmilestones.She
satindependentlyat2years,neverdevelopedwordstocommunicate,canassistwith
transfersfromchairtofloorbutcannotstandorwalkindependently.Shehasnothad
formalpsychometricsbutcurrently(age17)sheisnon-ambulatory,non-verbal,and
incontinentandperformsnoactivitiesofdailyliving.Formalaudiologyassessmentin
earlychildhoodwasnormal.Sheisinspecialschool4hoursadayandhasanirregular
sleeppattern.Onoccasions,shedoesnotsleepatnightforseveraldays.Shehas
nighttimeoutburstsoflaughingifsheisawakeforprolongedperiods.
Seizuresbeganinearlychildhoodand,currently,sheexperiencesabsence,partial
complexandgeneralizedtonicclonicseizures.Attimesthefrequencyhasbeenashigh
as20or30perday,butcurrentlyshehas~6permonthonTrileptalandclonazepam.
Shehaskyphoscoliosiswithprogressivevertebraldeformation,whichbeganinmid-
childhood.Herkyphoscoliosisworsenedinpubertyinassociationwithalineargrowth
spurt.
Atage15,shehadaroutineechocardiogramandlabworkinpreparationforpossible
spinesurgery.Herparentsweretoldhercardiacfunctionwassufficienttotoleratethe
surgerybutareunawareifanystructuralanomalieswerenoted.Therewerenospecific
pre-operativelaboratoryabnormalitiesotherthanlowvitaminDandanemia.The

formerhasbeentreatedwithsupplementaloralvitaminD(50,000IUweekly)andthe
latterwithoraliron,thoughtheanemiawasreportedtobeminimallyresponsive.
Onexamatage17yearsofage,herheadcircumstanceis51cm(<3%,50%for7years
old).Herfaceisexpressionlesswithslightlyelongatedpalpebralfissuresandsheholds
hertongueoutsidehermouth.Herneckandthoraxaregrosslynormalwithnormal
breastdevelopment.Shehassmallhandswithwastingofherperipheralmuscles.Her
hearingisgrosslynormal.Shetrackspeoplemovingaroundherandcan‘spot’smalltoys
orobjects.Sheavoidseyecontactandhasdifficultyreachingobjectswithashaky,poor
grasp.
Family4:
IndividualII-1isan8yearoldwhitemalewhowasthe45.7cm(<3%)and3.09kg(25%)
productofa38week,uncomplicatedpregnancyanddelivery.Apgarscoreswere9at1
and5minutes.Herequiredphototherapyforhyperbilirubinemiabutwasdischargedat
age5days.Developmentwasslow:hesatat12months,crawledat3years,andwalked
at4years.Therehasbeennoregression.Hehasdysphagiawithdifficultyswallowing
thinliquidsandchronicrespiratorycongestion.Herequiredafrenulectomy,multiple
typanostomytubesforchronicotitismediaandunilateralnasolacrimalductprobingfor
anobstructedtearduct.Hedevelopedkyphoscoliosisinchildhoodandisnon-verbal.
HehasCVIandamovementdisorderdiagnosedasataxiabyconsultingneurologists.
MultiplecranialMRIshavebeenreadasnormalexceptforsmallbrainsize.Hehasnot

hadseizuresandanEEGatage7.5wasnegative.Hisphysicalexamatage7years9
monthswasremarkableforshortstature(height113.5cm,1%),smallsize(weight
20.6kg,8%)andOFC47cm(<<3%,50%of1year).HEENTexamwasremarkablefor
downslantingpalpebralfissures;ascaronhisrightuppereyelidfromsurgicalrepairof
trauma;short,smoothphiltrum;broadnasalbridge;andachronicallyopenmouth.
Chest,cardiovascularandabdominalexamswerenormal.Hehadasmallpeniswith
mildchordee.Histonewasmildlyincreasedinhislowerextremitieswithnormaldeep
tendonreflexesandabnormalcoordinationwithataxia.Anechocardiogramat8years
ofagewasnormalwithnoabnormalitiesofthegreatvessels.
Pertinentlaboratorytestingincludednormalchemistriesandplasmaaminoacids;
normal15qmethylationtestingforPraderWillisyndromeandUBE3Asequencingfor
Angelmansyndrome;normalNIPBLsequencingforCorneliadeLangesyndrome1;
normalMECP2sequencing;normal7-dehydrocholesterolanduricacidlevels;normal
transferrinisoelectricfocusingforcarbohydratedeficienttransferrin;andnormalFragile
Xtesting.Hiskaryotypewas46,XYandachromosomalmicroarrayrevealeda
heterozygous40kbdeletionat22q12.3thatremovedsegmentsofC22orf42andRFLP2.
Hisasymptomaticmotherhasthesamecopynumbervariant.

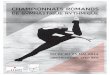
Family 1: c.2159A>T
Supplemental Data Figure S1
Family 1: c.1100G>T
Family 2:c.2296G>A
Family 3: c.779C>T
Family 2: c.1100G>T
Family 3: c.1826G>A
Figure S1. Sequence of TELO2 variants in Family 1 (II-3, II-4 and II-5), Family 2 (II-2) and Family 3 (II-1). Family.1: TELO2, p.Cys367Phe (c.1100G>T) in exon 8 and p.Asp720Val (c.2159A>T) in exon 18. Family.2: TELO2, p.Cys367Phe (c.1100G>T) in exon 8 and p.Val766Met (c.2296G>A) in exon 20. Family.3: TELO2, p.Pro260Leu (c.779C>T) in exon 5 and p.Arg609His (c.1826G>A) in exon 15.

0
0.2
0.4
0.6
0.8
1
Rel
ativ
e ex
pres
sion
TELO2 mRNA expression
C.1 C.2 C.3 II-2 II-3 II-4
Family 1 Controls
Figure S2
Figure S2. Comparison of TELO2 mRNA expression in affected individuals from Family 1 and controls Levels of TELO2 mRNA are within normal range in RNA extracted from primary affected individual-derived fibroblast cell lines in Family 1 (II-2, II-3 and II-4) (n=3 experiments, performed in triplicate; error bars indicate 1 SEM, Student’s t-test)

C.1 C.2 C.3 II-2 II-3 II-4
TELO2
TTI1
TTI2
β-Actin
Family 1
Figure S3
Figure S3. Repeated western blot of steady state expression of TTT complex in fibroblasts extracts in the affected individuals of Family 1 (II-2, II-3 and II-4) and three normal controls (C.1, C.2 and C.3).

0
0.2
0.4
0.6
0.8
1
1.2
0 0.5 1 1.5 2
SurvivingFrac,o
n
IRdosage(Gy)
Colony survival assay (8 days) Controlmean(n=3)
I-1
I-2
II-2
II-3
II-4
AtaxiaTelangiectasia
0
0.2
0.4
0.6
0.8
1
1.2
1.4
ATM ATR PRKDC mTOR TRRAP SMG
Rela,v
eexpression
controls(n=3)heterozygous(n=2)C367F/D720V(n=3)
Figure S4
Figure S5
Figure S5. Colony survival assay following exposure to ionizing irradiation. LCLs from affected individuals in Family 1 (II-2, II-3 and II-4) are labeled in red and the mean of three controls is labeled in green. LCLs from an affected individual with molecularly confirmed ataxia-telangiectasia (ATM nonsense variant) was used as a positive control.
Figure S4. Steady state expression of PIKKs in LCL extracts in the affected individuals of Family 1 (II-2, II-3 and II-4), their heterozygous parents (I-1 and I-2) and three normal controls (C.1, C.2 and C.3). There was no significant difference between control, affected individuals and heterozygous parents (Student’s t-test).

FigureS7
0.7
0.75
0.8
0.85
0.9
0.95
1
1.05
0 50 100 150 300 400 500
SurvivingFrac,o
n
MMCconcentraion(ng/ml)
MMC(MitomycinC)survivalassay(12hrs)
controls(n=3)
C367F/D720V(n=3)
Figure S6
Figure S7. Telomere length measurement in affected individuals’ primary lymphocytes and granulocytes. The percentile lines are derived from 200 normal controls. Affected individuals and heterozygous parents from Families 1 and 2 were measured.
Figure S6. Mitomycin C (MMC) survival assay Cultured skin fibroblasts from affected individuals in Family 1 (II-2, II-3 and II-4) and controls were used to measure the survival fraction following MMC treatment. The assay was performed in triplicate, and the plot shows the means of the 3 affected individuals and the 3 controls. There was no significant difference between controls and affected individuals in survival fraction to MMC treatment (Student’s t-test).