Embed Size (px)
Citation preview
Transition Presenter : Tera Bartelt
Children’s Hospital Transition Committee
Team members
• Transition Committee– Stacy Boyce, Julie Turkoske, Bob Rohloff, Terri
Couwenhoven, Stephanie Stroud, Tera Bartelt, Mary Beth Miranda, Cindy Griffith, Lisa Hacker, Elizabeth Horning
• Workshop Committee– Terri Couwenhoven, Julie Turkoske, Helen Peplinski,
Jake Peplinski, Deon McLaughlin, Katey Collins, Stephanie Stroud, Angela Stahl
• Adult Workgroup Committee– Jeff Whittle, Bob Rohloff, Maureen Collins, Mary
Beth Miranda, Kathleen Sawin
Projects
• Transition Committee– Policy– Staff Education
• Education Workshop– Saturday Youth/Parent Workshop– Transition Binder
• Adult Committee– Created Short Survey to gage interest– 4 Lunch and Learns completed
TRANSITION COMMITTEE
Policy
• 1st hospital policy implemented for Ambulatory and Children’s Medical Group effective 10/15/14.
Policy statement: All YSHCN will participate in the transition process that is developmentally appropriate and meaningful for them regardless of when they transfer care to an adult provider. The transition checklist should be used to guide the youth, family and health care team to develop appropriate goal setting, promote independence and monitor skill development. YSHCN will be provided a transition summary upon transfer of care to an adult provider.
Policy
• The policy defines the purpose of Transition.
• Definitions: Transition, Transfer of Care, Transition planning, Transition checklist, Transition summary, Transition coordinator
• Team Roles: Providers, RNs, Social Workers, Transition coordinator, youth and parent/guardians.
Procedure
• List Transition in the Problem List at age 12.
• Use the transition checklist as a guide to promote goal setting and independence.
• Supply family with the care plan at time of transfer.
• Provide family with transition summary at time of transfer
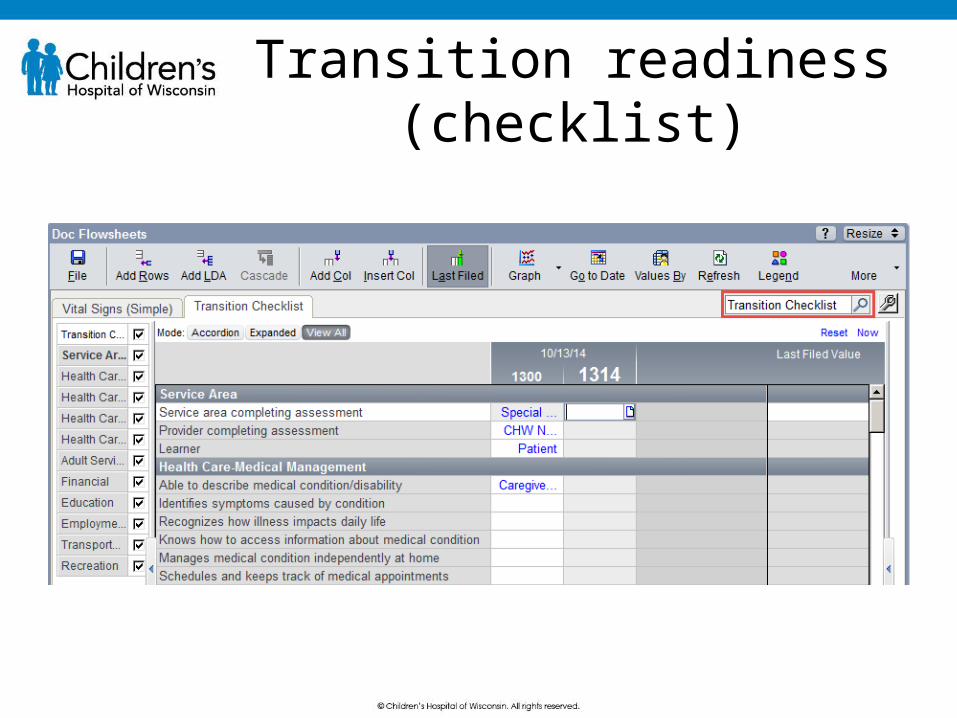
Transition readiness(checklist)

Transition Checklist Goal
• By December 2014 20% of youth 12 years and older who are cared for in the identified Specialty clinics (Trach-Vent, Spina Bifida, Kidney Transplant, Down Syndrome and Sickle cell will have an initiated Transition Checklist defined as documentation on at least one question
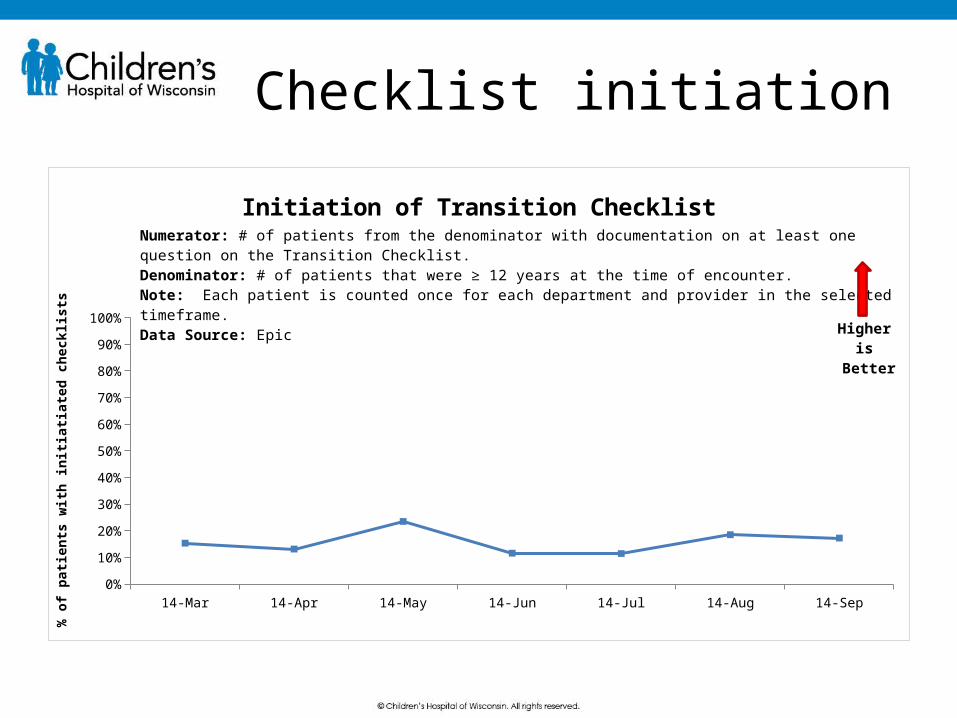
Checklist initiation
14-Mar 14-Apr 14-May 14-Jun 14-Jul 14-Aug 14-Sep
Total 0.1534 0.131 0.235 0.1158 0.1142 0.185 0.1726
5%
15%
25%
35%
45%
55%
65%
75%
85%
95%
Initiation of Transition Checklist
% o
f pati
ents
with
initi
atiat
ed ch
eckl
ists
Numerator: # of patients from the denominator with documentation on at least one question on the Transition Checklist.Denominator: # of patients that were ≥ 12 years at the time of encounter.Note: Each patient is counted once for each department and provider in the selected timeframe.Data Source: Epic
Higheris
Better
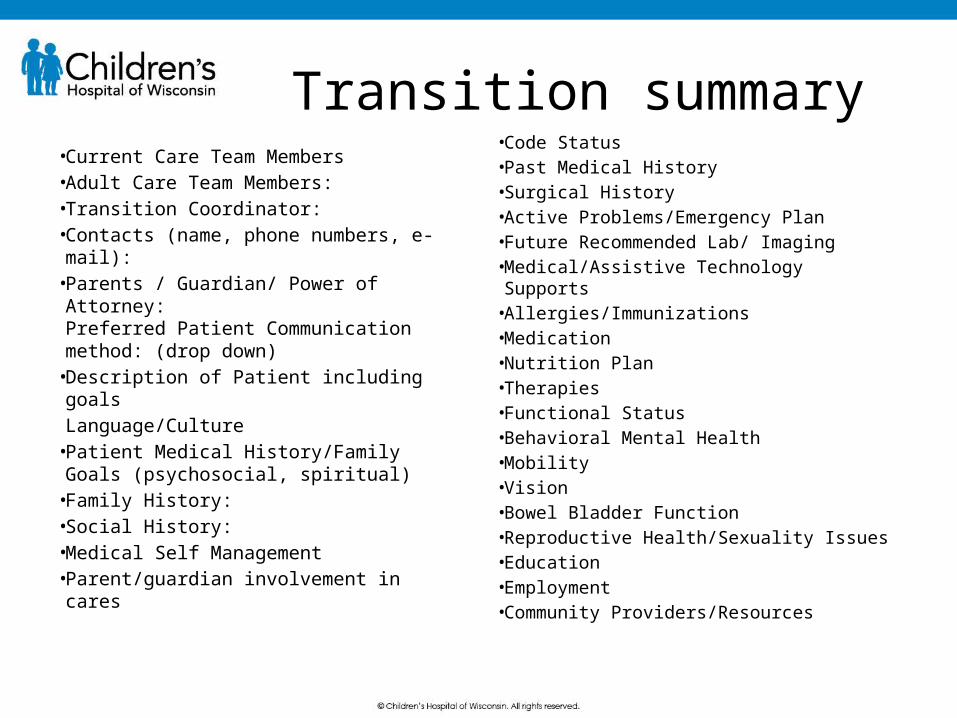
Transition summary
• Current Care Team Members • Adult Care Team Members: • Transition Coordinator: • Contacts (name, phone numbers, e-
mail): • Parents / Guardian/ Power of
Attorney:Preferred Patient Communication method: (drop down)
• Description of Patient including goalsLanguage/Culture
• Patient Medical History/Family Goals (psychosocial, spiritual)
• Family History: • Social History: • Medical Self Management• Parent/guardian involvement in
cares
• Code Status• Past Medical History• Surgical History• Active Problems/Emergency Plan• Future Recommended Lab/ Imaging• Medical/Assistive Technology
Supports • Allergies/Immunizations• Medication• Nutrition Plan• Therapies• Functional Status• Behavioral Mental Health• Mobility• Vision• Bowel Bladder Function• Reproductive Health/Sexuality Issues• Education• Employment• Community Providers/Resources
TRANSITION WORKSHOP
Transition Workshop• Developed a Transition Workshop titled:
Taking Charge and Letting Go in collaboration with the CYSHCN Regional Center and Spina Bifida Wisconsin.
• Utilized the Transition to Adult health Care: A training in three parts as the foundation.
• Two young adults participated in the planning and the presentation of the youth part of the workshop.
• Transition Binder was developed
Workshop
http://www.youtube.com/watch?v=UAySTI9GSds&sns=em• Parent Panel• Small turnout: many barriers, freeway
was closed, two other competing workshops within the month
• Pearls: parents and youth that did attend found it helpful.
• The transition binder was useful and will be distributed to clinics
TRANSITION TO ADULT CARE
Adult practices
• Telephone survey developed • Email sent to Adult practices within
the Consortium.• Phone calls made to 6 practices and
asked set of survey questions.• Completed 4 lunch and learns.
Survey Questions• Questions included:
1. Do you accept young adults with chronic conditions into your practice? Yes, some were family practice and they already see these young adults as a continuation of care.
2. How do you receive past medical hx? Very rarely do they have past history with them when meeting family 1st time.
3. What barriers do you encounter? Insurance, slots open for Medicaid patients
4. Do you have a mechanism to track this population? No5. Do you have a special policy addressing this population? No6. What resources do you need to from us? We found that on the surface most adult practices did not find
transition an issue and were willing to take this population.Concern: Perhaps adult practices do not recognize the special
circumstances around the transfer of care and the transition process that young adults and parents go through.

Lunch and Learns
• 4 Lunch and Learns–Waukesha Family Practice (6 providers)– St Luke’s Family Practice (15 providers)– Sinai Family Practice (15 providers)– Sargeant Internal medicine Practice (12
providers)
Lunch and Learns
• Presented 6 core element information
• Information about the Transition website
• Discussion about Transition of care, What can we at CHW do better to support you during transition?
• Potential pilot clinics
VISITING PROFESSOR
Speaker
• Dr Carl Cooley, invited speaker visited on September 18th - 19th.
• Presented Pediatric Grand rounds to over 185 participants
• Met with Leadership team• Met with Solid Organ transplant team• Discussed Quality measures at a lunch
meeting• Wrap up, Next steps with Transition
Committee
Next Steps
• Transition Committee to determine goals for 2015.– Include: Potential assessment of all
clinics involved in transition, Wave 2 clinics presented with checklist, care plans, pilot clinics for transition to adult care.
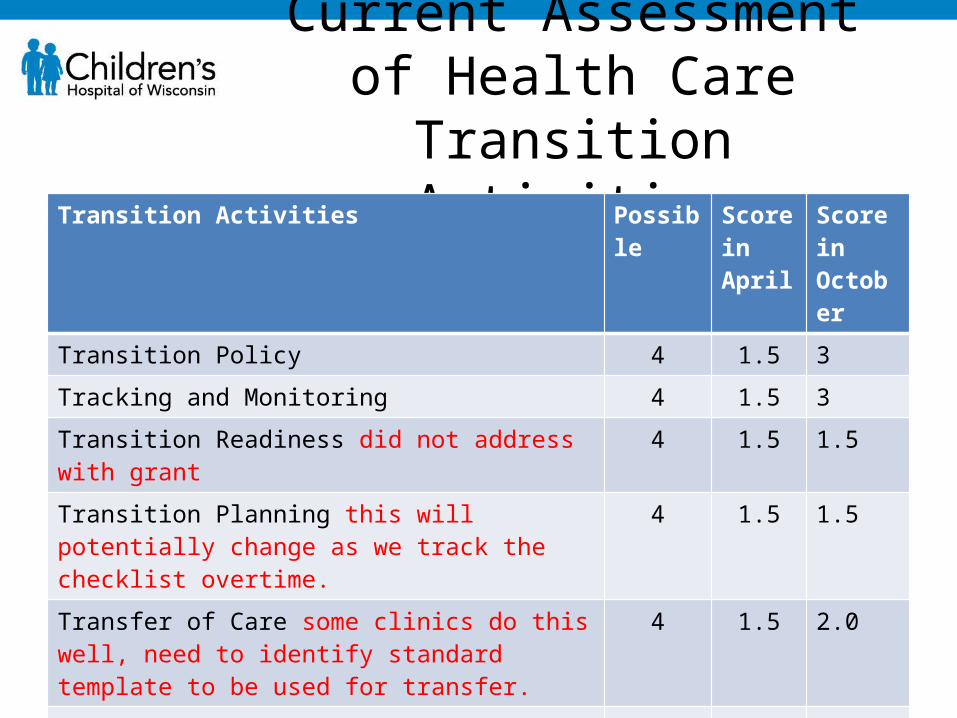
Current Assessment of Health Care Transition
ActivitiesTransition Activities Possible Score
in AprilScore in October
Transition Policy 4 1.5 3
Tracking and Monitoring 4 1.5 3
Transition Readiness did not address with grant 4 1.5 1.5
Transition Planning this will potentially change as we track the checklist overtime.
4 1.5 1.5
Transfer of Care some clinics do this well, need to identify standard template to be used for transfer.
4 1.5 2.0
Transfer Completion 4 2.0 2.0
Youth and Family Feedback 4 1.0 1.0
Youth and Family Leadership 4 1.0 3.0
Total 32 11.5 17
Lessons learned
• It takes a dedicated team to support the ongoing work of transition.
• Time needs to be allocated for this work by institutions in order for it to be a priority.
• Parents and youth are an invaluable contribution to the work around transition.

Thank you





























