Embed Size (px)
Citation preview

JNC-8 New Guidelines…Finally Let the controversies begin
Eric D Peterson, MD, MPH Director of DCRI
Feb, 2014 http://www.dcri.duke.edu/research/coi.jsp

All Rights Reserved, Duke Medicine 2007 sb/Strategy & Innovation Group | 2
• Affects 1 billion people worldwide • US – about 1 in 3 adults
– 73 million have hypertension (SBP >140/90) • A 55yo normotensive person has up to a 90% lifetime
risk of developing hypertension (Vasan 2001) • Number one reason listed for office visits • Causes/contributes to 457,000 admissions per year • A leading cause/contributor to death (MI, stroke,
vascular disease)

All Rights Reserved, Duke Medicine 2007 sb/Strategy & Innovation Group | 3
• “The greatest danger to a man with high blood pressure lies in its discovery, because then some fool is certain to try and reduce it.”- J.H. Hay, 1931.
• “Hypertension may be an important compensatory
mechanism which should not be tampered with, even were it certain that we could control it.” Paul Dudley White, 1937.
How Aggressive to Treat Hypertension Some Early Views on the Controversy

All Rights Reserved, Duke Medicine 2007 sb/Strategy & Innovation Group | 4
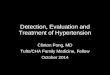
Stroke and IHD Mortality vs Systolic BP by Age
Mor
talit
y (F
loat
ing
abso
lute
risk
and
95%
CI)
Usual Systolic BP (mm Hg)
50-59 years
60-69 years
70-79 years
80-89 years
Stroke
Age at risk 256
128
64
32
16
8
4
2
1
0 120 140 160 180
Ischemic Heart Disease
Usual Systolic BP (mm Hg)
50-59 years
60-69 years
70-79 years
80-89 years Age at risk:
40-49 years
256
128
64
32
16
8
4
2
1
0 120 140 160 180
Lancet. 2002;360:1903-1913

All Rights Reserved, Duke Medicine 2007 sb/Strategy & Innovation Group | 5
BP Reductions as Small as 2 mmHg Reduce the Risk of CV Events by Up to 10%
▶ Meta-analysis of 61 prospective, observational studies
▶ 1 million adults
▶ 12.7 million person-years
Prospective Studies Collaboration. Lancet. 2002;360:1903-1913
2 mmHg increase in mean SBP
10% increase in risk of stroke mortality
7% increase in risk of ischemic heart disease mortality

All Rights Reserved, Duke Medicine 2007 sb/Strategy & Innovation Group | 6
Benefits of Treating Hypertension: RCT
-100-90-80-70-60-50-40-30-20-10
0
Heart failure Stroke Cardiovasculardeath
Ris
k re
duct
ion
(%)
↓ 50% ↓ 40%
↓ 20%
Hebert, Archives Int Med 1993; Moser, Am Coll Cardiol 1996

All Rights Reserved, Duke Medicine 2007 sb/Strategy & Innovation Group | 7
Lifestyle Modifications
Goal blood pressure <140/90 mm Hg <130/80 mm Hg with diabetes or chronic kidney disease*
Initial drug choices
Without Compelling indications
Stage 1 Hypertension (SBP 140-159 DBP 90-99 )
Diuretics for most; may consider ACE inhibitor,
ARB, beta blocker, CCB or combination
Stage 2 hypertension (SBP ≥ 160 or DBP ≥ 100)
2-drug combination for most (Diuretic +ACE, ARB,
beta blocker, or CCB)
With compelling indications
Drug(s) for compelling indications
Diuretics, ACE inhibitor, ARB, beta blocker, CCB as
needed
* Released in 2003

All Rights Reserved, Duke Medicine 2007 sb/Strategy & Innovation Group | 8
NHLBI Drops Out of Guidelines Business
JNC-8 Significantly Delayed

All Rights Reserved, Duke Medicine 2007 sb/Strategy & Innovation Group | 9
James et al JAMA December 13 2014

All Rights Reserved, Duke Medicine 2007 sb/Strategy & Innovation Group | 10
James et al JAMA December 13 2014

All Rights Reserved, Duke Medicine 2007 sb/Strategy & Innovation Group | 11
James et al JAMA December 13 2014
JNC-8 Hypertension Treatment Choices

All Rights Reserved, Duke Medicine 2007 sb/Strategy & Innovation Group | 12

All Rights Reserved, Duke Medicine 2007 sb/Strategy & Innovation Group | 13

All Rights Reserved, Duke Medicine 2007 sb/Strategy & Innovation Group | 14
The Evidence for Targets: JATOS Study • 2200 pts per arm • Baseline BP 170/90 • Target
<150 mild vs. <140 strict • Drugs:
– Ca++blocker 50-60% – Ace 30-40% – Alpha blocker 15% – Diuretic 15%
• Follow-up 2 yrs
Hypertens Res. 2008;31(12):2115-2127

All Rights Reserved, Duke Medicine 2007 sb/Strategy & Innovation Group | 15
JATOS Results
Hypertens Res. 2008;31(12):2115-2127

All Rights Reserved, Duke Medicine 2007 sb/Strategy & Innovation Group | 16
The Evidence for Targets: VALISH Trial
Hypertension. 2010;56(2):196-202
• 1630 pts per arm • Baseline BP 170/80 • Target
Mild <150, strict <140 • Drugs:
– Valsartan 100% – Ca++ blacker 30% – Diuretic 10-15%
• Median Follow-up 3 yrs

All Rights Reserved, Duke Medicine 2007 sb/Strategy & Innovation Group | 17
Hypertension. 2010;56(2):196-202
VALISH Trial

All Rights Reserved, Duke Medicine 2007 sb/Strategy & Innovation Group | 18
RCTs Evaluating SBP Targets in those Aged < 60
“Does the absence of evidence lead to the conclusion of evidence of absence?”
JNC-8 authors concluded: - Yes for those >60 - No for those <60

All Rights Reserved, Duke Medicine 2007 sb/Strategy & Innovation Group | 19

All Rights Reserved, Duke Medicine 2007 sb/Strategy & Innovation Group | 20
Guidelines, Performance Measures and Policy
• Guideline: – In past: practical advice on a course of action – Have become: RCT-based, rigorous
• Performance Measures:
– Distillation of guidelines: • Use strict criteria to define what should and must
be done to avoid a quality concern – Often applied to public reporting or financial
incentives

All Rights Reserved, Duke Medicine 2007 sb/Strategy & Innovation Group | 21
BP Treatment Targets Have Risks Both Ways
• If one votes to keep all at 140/90 – PM’s and incentives may encourage over-treatment
• Worse symptoms, falls, costs in elderly
• If one votes to move to 150/90 in elderly – Risk of under-treatment
• Despite existing guideline goals/PM’s, <50% of public reaches goal!

All Rights Reserved, Duke Medicine 2007 sb/Strategy & Innovation Group | 22
JNC-8 Implications for US
All US Adults Ages 18-59 Ages 60+ JNC 7: HTN 66.6 32.8 33.8 Controlled 26.6 (39.9%) 13.3 (40.5%) 13.3 (39.3%) JNC 8: HTN 60.8 30.8 30.0 Controlled 34.3 (56.4%) 14.6 (47.4%%) 19.7 (65.7%)

All Rights Reserved, Duke Medicine 2007 sb/Strategy & Innovation Group | 23
Major Findings
• Currently: 66.7 million in US have hypertension, – of which 39.9% met guideline targets.
• Using JNC 8: 60.8 million in US have hypertension, – of which 56.4% have controlled blood pressure.
• In 60+, switching to JNC-8 – improves BP control rates from 34.3% to 60.8% – reclassifying 13.6 million with previously
uncontrolled BP now seen as under control

All Rights Reserved, Duke Medicine 2007 sb/Strategy & Innovation Group | 24
Conclusions
• Hypertension: common, costly and modifiable
• Interpretation of existing evidence is challenging – Determining the optimal threshold will require
more RCTs.
• In interim: My view: – Aim for 140/90 but allow for individualization – What’s your take?







![H20youryou[2] · 2020. 9. 1. · 65 pdf pdf xml xsd jpgis pdf ( ) pdf ( ) txt pdf jmp2.0 pdf xml xsd jpgis pdf ( ) pdf pdf ( ) pdf ( ) txt pdf pdf jmp2.0 jmp2.0 pdf xml xsd](https://img.pdfslide.net/doc/110x75/60af39aebf2201127e590ef7/h20youryou2-2020-9-1-65-pdf-pdf-xml-xsd-jpgis-pdf-pdf-txt-pdf-jmp20.jpg)