Embed Size (px)
Citation preview

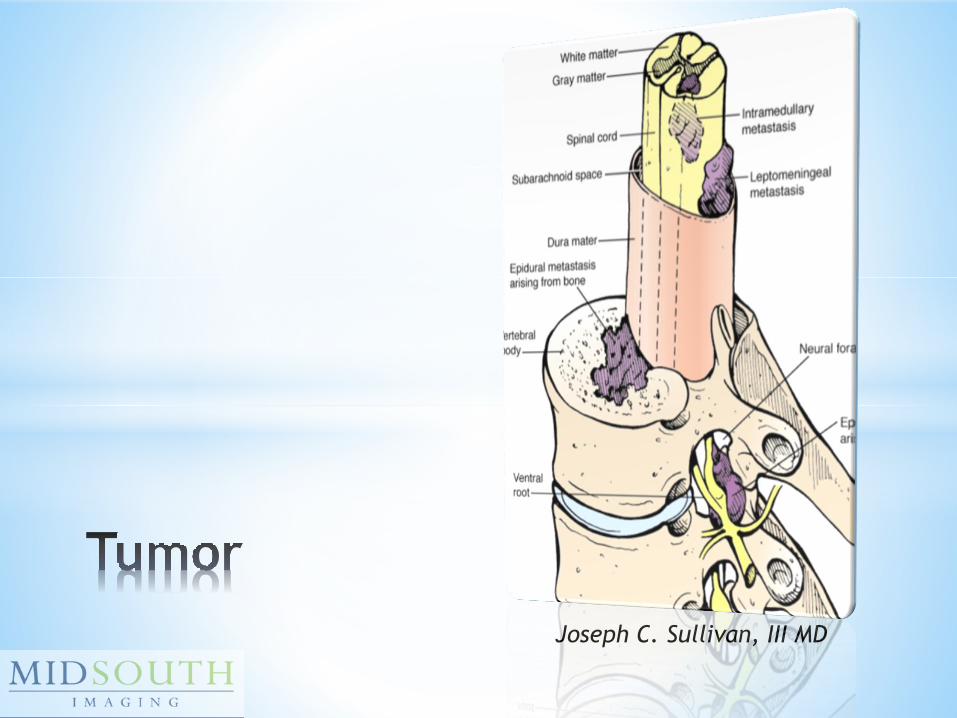
Joseph C. Sullivan, III MD

1. Headache2. Foreign object in the
body3. Skin infection4. Back pain5. Cuts and contusions
Health.Howstuffwoks.com/10most common reason for ER visits

65% increase in spending since
1997. That’s in line with cancer and
diabetes.
Only dwarfed by Heart disease
and Stroke
Web-md.com

Its 1AM, and your ER Doc
has a patient with back
pain, what are they
going to order?

Its 1AM, and your ER Doc
has a patient with back
pain, what are they
going to order?

A. Fall with pain
B. Radiculopathy/Pain
C. Epidural abscess
D. Cauda equina

1. Trauma
2. Infection
3. Tumor
4. Cauda Equina Syndrome
Joseph C. Sullivan, III MD

• Real or Assumed (Ass-U-Med)
• Triage or Lack thereof
• Neurological deficits
Joseph C. Sullivan, III MD

Joseph C. Sullivan, III MD

Joseph C. Sullivan, III MD

Joseph C. Sullivan, III MD

Joseph C. Sullivan, III MD

Joseph C. Sullivan, III MD

0. No movement contraction
1. Minimal movement
2. Active movement, but not against gravity
3. Active movement against gravity
4. Active movement against resistance
5. Active movement against full resistance
Joseph C. Sullivan, III MD

Joseph C. Sullivan, III MD

Joseph C. Sullivan, III MD

• Compression fracture
• Mets
• Muscle spasm
• Herniated disc
• Infection
• Ligamentous/muscle
Joseph C. Sullivan, III MD

• Cardiac
• Cholelithiasis, Peptic ulcer,
Pancreatitis
• Dissecting AAA
• Pyelonephritis
• PID, Ectopic, Fibroids
Joseph C. Sullivan, III MD

• Cancer History (or unexplained weight
loss)
• Trauma
• Immunosuppression (or long term
steroid use)
• Recent serious illness/infection
• IV Drug use
Joseph C. Sullivan, III MD

• Atypical pain or tenderness (abdominal or thoracic; 4-6 wks; non-mechanical)
• Severe limited ROM
• Fever; Meningismus; Lhermitte’s
• Muscle atrophy; Loss of sensation or strength (especially saddle)
• Loss of bowel or bladder control
• Abnormal reflexes: Hoffman’s; Babinski sign; Bulbocavernous/Wink
Joseph C. Sullivan, III MD

• C2 – Back of skull cap
• C3 – Back of turtle neck
• C4 – T shirt collar
• C5-6 – Thumb
• C7 – Index and Middle fingers
• C8 - Ring and Pinky fingers
• T4 – Nipple
• T5 – Under line
• T6-7 – Xyphoid
• T10 – Umbilicus
• T12 – Pubis
• L1 – Inguinal
• L4 – Knee cap
• L5 - Top of foot
• S1 – Lateral foot
Joseph C. Sullivan, III MD

In the absence of acute trauma or
infection, usually associated with
spondylosis or OPLL resulting in
compression of the cord and/or roots
Joseph C. Sullivan, III MD

In the absence of acute trauma or
infection, usually associated with
spondylosis or OPLL resulting in
compression of the cord and/or roots
Joseph C. Sullivan, III MD

In the absence of acute trauma or
infection, usually associated with
spondylosis or OPLL resulting in
compression of the cord and/or roots
Joseph C. Sullivan, III MD

• Insidious onset
• Weak or Clumsy hands
• Lhermitte’s Sign
• May have gait or bowel/bladder dysfunction
• Upper Motor Signs (Hoffman’s, Babinski, hyper-reflexia, clonus)
• Lower Motor Signs (atrophy or hypo-reflexia
Joseph C. Sullivan, III MD

• Amyotrophic Lateral Sclerosis
• Multiple Sclerosis
• Spinal Tumors
• Syringohydromyelia
Joseph C. Sullivan, III MD

• Cervical lesions can affect all four limbs and risk respiratory paralysis (C3, C4 & C5)
• Cervico-Thoracic junction lesions can cause mixed UMN and LMN signs in upper limbs, while LMN in the lower extremities
• Thoracic lesions can produce spastic paralysis
• Lumbar lesions can produce mixed UMN and LMN neuron signs in the lower limbs
Joseph C. Sullivan, III MD

• Discitis/Osteomyelitis; Epidural abscess
• Hematologic spread
• 1/3 may have fever
• Up to 15% present already with neurologic deficit
• Involve the disc and endplate
• Occur in up to 1% of patients
• More often in immunocompromised
• Symptoms can last2-4 weeks after treatment
Joseph C. Sullivan, III MD

Joseph C. Sullivan, III MD

Joseph C. Sullivan, III MD

Joseph C. Sullivan, III MD
Joseph C. Sullivan, III MD

Joseph C. Sullivan, III MD

Joseph C. Sullivan, III MD

Joseph C. Sullivan, III MD

Joseph C. Sullivan, III MD

Sarcoid
Rosai Dorphman
Joseph C. Sullivan, III MD

Sarcoid
Rosai Dorphman
Joseph C. Sullivan, III MD

Sarcoid
Rosai Dorphman
Joseph C. Sullivan, III MD

Joseph C. Sullivan, III MD

Joseph C. Sullivan, III MD

The cauda equina is a bundle
of spinal nerves and spinal nerve
roots, consisting of the second
through fifth lumbar nerve pairs,
the first through fifth sacral nerve
pairs, and the coccygeal nerve, all
of which arise from the lumbar
enlargement and the conus
medullaris of the spinal cord.

Generally considered to be
comprised of nine pairs of nerve
roots, starting with L2 and
extending to and including S5 (ok,
and the coccyx root as well, so
9+1).

The “Cauda Equina” was so-named by
French anatomist Andreas Lazarius in
the 1600’s.

Cauda Equina Syndrome was first
described by Mixter and Barr in
1934.
A variable presentation consisting
of a constellation of symptoms
which includes lower back pain,
asymmetrical LE paralysis, variable
sensory deficits, and loss of bowel
and bladder control.

1 in 33000 to 100000
Lavy C, James A, Wilson-MacDonald J, Fairbank J. Cauda
equina syndrome. Brit Med J. 2009;338:b936

1 in 33000 to 100000
ER doc may not see a true one in
there entire career
Lavy C, James A, Wilson-MacDonald J, Fairbank J. Cauda
equina syndrome. Brit Med J. 2009;338:b936

Incidence of CES in U.S. is estimated between 2 and 4 cases per 10,000 patients with chief complaint which includes LBP.
Estimated to be present to some degree in as many as 2% of patients undergoing surgery for HNP.
High clinical suspicion must be kept in patients presenting with LBP and other symptoms. Good history and physical exam-taking is key!

A. Back pain
B. Bladder and bowel
dysfunction
C. Paralysis
D. Sexual dysfunction

A. Back pain
B. Bladder and bowel
dysfunction
C. Paralysis
D. Sexual dysfunction

A. Motor innervation of the hips but
not the knees
B. External anal sphincter but not
internal sphincter
C. Motor innervation of the
perineum
D. Partial innervations of the para-
sympathetics to the bladder
E. Sensory innervation of the
external sphincter, only

A. Motor innervation of the hips but
not the knees
B. External anal sphincter but not
internal sphincter
C. Motor innervation of the
perineum
D. Partial innervations of the para-
sympathetics to the bladder
E. Sensory innervation of the
external sphincter, only

The nerves that compose the cauda
equina innervate the pelvic organs
and lower limbs to include motor
innervation of the hips, knees,
ankles, feet, internal and the
external anal sphincter.
In addition, the cauda equina
extends to sensory innervation of
the perineum, and partially,
parasympathetic innervation of
the bladder.

Nerve roots of the Cauda Equina are susceptible to injury from compression partly due to a poorly developed epineurium (less protection from “outside stresses” or tension).

Proximal nerve roots are relatively hypovascularizedand are supplemented by increased vascular permeability in this area as well as diffusion from surrounding CSF (which is thought to contribute to swelling and edema in irritated nerve roots).

Unmyelinated, smaller
parasympathetic/pain fibers are
more susceptible to compression
and injury from compressive
forces.
Herniated lumbar disc
Tumor
Trauma
Spinal epidural hematoma
Infection
Other
Basic idea: Severe Canal
Stenosis (narrowing)

Acute presentation is most common,
and is most commonly seen in
patients with a prior history of LBP.
Acute presentation in patients with
no prior history of LBP and/or sciatica
occasionally seen.
Insidious onset and progression of
symptoms is rare, but is associated
with better chance of return of
function (especially bladder
function).

Caused by compression or injury to the nerve roots which descend from the conus medullaris.
Many different possible causes.
Underlying chronic conditions can predispose to CES, as well as cause it in some cases.

The most common symptom in
patients presenting with CES is Low
Back Pain (LBP).
>90% of patients
Nonspecific, yes, but index of suspicion
should be high and appropriate history
should be elicited, especially if
coexisting symptoms/complaints are
present.

The most consistent sign in cauda equina syndrome is urinary retention (incidence approaches 90%).
Check post-void residual – normal is between 50 and 100 mL and >200 is positive for retention.
Overflow incontinence can be seen as the bladder fills.
Anal sphincter tone is diminished in 50-75% of patients with CES.
Fecal incontinence can be seen.

“Saddle anesthesia” is the most commonly observed sensory deficit in patients with CES.
Roughly 75% of pts.
Sensory loss seen around the anus, lower genitalia, perineum, buttocks, sometimes even the posterior thighs.

LBP is a nonspecific finding.
New LBP is rarely seen in cases of
CES without other symptoms
being present.
Sciatica, when present, is usually
bilateral (but can be unilateral).

If Motor weakness – can be severe, and usually involves more than a single nerve root.
May be bilateral, but is rarely symmetric (one side is usually weaker/stronger than the other).
Untreated motor weakness can become permanent disability, and can progress to complete paralysis/paraplegia.
Reflexes are HYPO-active; no long tract signs!



Altered urinary sensation
Loss of desire to void
Poor urinary stream
Strain to micturate
Saddle anesthesia is partial or
unilateral

Painless urinary retention and
overflow
No longer able to execute
micturition
Complete saddle anesthesia
and genital sensory deficit

A. Anal sphincter tone
B. Full bladder on palpation
C. Bulbocavernosus reflex
D. Cremaster reflex
E. Anal wink reflex

A. Anal sphincter tone
B. Full bladder on palpation
C. Bulbocavernosus reflex
D. Cremaster reflex
E. Anal wink reflex
Uff CE (2009) Clinical assessment of cauda equina syndrome and the
bulbocavernosus reflex.
http://www.bmj.com/cgi/eletters/338/mar31_1/b396

Herniation of a [typically] massive portion of intervertebral disc material into the spinal canal causing compression of the descending nerves of the cauda equina.
Represents between 15 and 20% of CES cases.

Ten cases reported in the literature of CES being caused by very large disc fragment[s] which have migrated into the posterior epidural space causing posterior compression.
More than 100 cases of reports of intradural migration of herniated disc fragments.
Some estimates place prevalence of CES as high as 2% of herniated intervertebral discs!

Variability in presentation is a direct result of level of involvement.
Most common level of involvement is L4-5 (57%), followed by L5-S1 (30%), then L3-4 (13%).
Most common presentation of CES secondary to acute disc herniation is males age 30-40 with prior history of LBP. Most have NOT been operated on previously.

Ependymomas account for roughly
90% of primary tumors of the filum
terminale and cauda equina, the
majority of which (~60%) are of the
myxopapillary subtype. Still, CES
from this is rare.
Schwannomas in the area of the
conus or cauda equina can also
occur and cause CES, but are rare.

Tarlov cysts, while rarely
symptomatic, have been described
in the literature as causing CES.
Primary sacral neoplasms, such as
chordoma or a destructive bony
lesion, can cause CES through
collapse of bone and structure.
Again, in all cases, the mechanism
is compression of the nerve roots.
Anything that does this can cause
CES.

Incidence of spinal metastasis is
increasing due to improvements in
diagnostic modalities, imaging, and
treatment regimens.
The most common non-CNS metastatic
tumor causing spinal metastases is lung,
however, CES occurs in less than 1% of
cases involving spinal spread of
metastatic lung cancer.

Drop metastases from inctracranial
ependymomas, germinomas, and
other primary intraneural tumors
can cause CES from seeding via the
CSF space.

Primary genitourinary and
gynecologic tumor extension into
the cauda equina region is a rare
cause.

Mechanical disruption of the spine
from subluxation, spondylolisthesis,
and/or compression of the neural
elements from hematoma, etc.,
can cause CES.
True incidence in the trauma
setting is somewhat unclear due to
coexisting injuries.

Spinal Epidural Hematoma
Infection
Again…Anything that leads to
compression of the roots.

The major point of contention
with Cauda Equina surgical
intervention revolves around
timing – when is it most
appropriate to operate on these
lesions? IS THIS AN EMERGENCY???

Shapiro et al noted that patients who
underwent surgery within 48 hrs of
symptom onset, 95% recovered
continence and normal function within
six months. Conversely, 63% of those
patients whose surgery was delayed
beyond 48 hrs still required
catheterization after 6 months.
Generally, patients show improvement
first in pain, then with motor function –
while autonomic signs are last to
improve (and the least likely).
Shapiro S. Cauda equina syndrome secondary to lumbar
disc herniation. Neurosurgery. 1993;8:317–322

Meta-analysis that came out of Johns Hopkins University in 2000 (total 332 patients) that looked at patients with CES secondary to lumbar disc herniations, Ahn et al determined a significant improvement in outcome for patients operated on within 48 hours of onset of symptoms when compared with those operated on more than 48 hours after onset of symptoms.
Within those respective groups, there was no significant difference in outcomes for earlier or later times.

There is still debate about this in
the literature. In 2004, Radulovic
et al published a retrospective
analysis of their own series of
patients (47) where they found no
significant difference in outcome
regardless of time to operation.
This study, however, did not focus
on onset of symptoms; but rather,
time from presentation.

More recently, McCarthy et al
published their series of 42
patients with CES secondary to
disc herniation and found no
significant improvement in
patients’ outcome regardless of
time to surgery after onset of
symptoms.

Current recommendations outline
a goal of performing surgery within
24 hours of presentation if at all
possible.
A major line of thinking behind
this plan lies in the medical-legal
pitfalls of dealing with CES and the
residual deficits dealt with by the
patients.

The goal of the operation is to
decompress the nerve roots of the
cauda equina.
Instrumentation is rarely used for
acute disc herniations, but is more
commonly used in cases of CES
caused by trauma or severe
degenerative disease of the spine
from which CES has been the result
of instability.

Major point to keep in mind is this: Cauda Equina Syndrome has a variable presentation and is widely thought to be regularly misdiagnosed or just plain missed.

Failure to recognize spinal emergencies is an ongoing issue and the subject of continued litigation in patients who were eventually recognized but in whom deficits remain after surgery.

Appropriateness Criteria
Joseph C. Sullivan, III MD

Practice Parameters and
Technical Standards
Joseph C. Sullivan, III MD

Presentations can vary – Back Pain
Earlier intervention (before CES-R)
Be suspicious but knowledgeable