Embed Size (px)
Citation preview

Journalof the California Dental Hygienists’ AssociationVolume 22, Number 2Winter 2007
In this issue…ADHA Continues to Move Our Profession ForwardRDHAP JourneyMeth Mouth & Dental Considerations

Introducing an unmatchedrange of benefits. New Crest®
PRO-HEALTH™ Toothpaste.
Now with just one toothpaste, you can protect
your patients from gingivitis, caries, and sensitivity.
Introducing Crest PRO-HEALTH Toothpaste.
When it comes to your patients’ oral health,
why not stack the odds in their favor?
It’s no longer alevel playing field
Healthy, Beautiful Smiles For Life
For more information, including clinical resources, visit dentalcare.com.
“The ADA Council on Scientific Affairs’ Acceptance of Crest PRO-HEALTH Toothpaste is based on its finding that the product is effective in helping to prevent and reducetooth decay, gingivitis and plaque above the gumline, to relieve sensitivity in otherwise normal teeth, and to whiten teeth by removing surface stains, when used as directed.”
© 2006 P&G PGC-1610L OPAD06368
Cavities | Gingivitis | Plaque | Sensitivity | Tartar | Whitening | Freshens breath
THE FIRST AND ONLY ADA-ACCEPTED TOOTHPASTE WITH THIS RANGE OF BENEFITS:
idm607004_Ar1 11/22/06 12:35 PM Page 1

Editor Liz Moore, RDH, BS, MSEd
Associate Editor Linda Cryan, RDH
Advisory Board Cathy Draper, RDH, MS Debbi Frolove, RDH Holly Knauft, RDH Gail Starr, RDH
Contributions of scientific and original articles. The Journal of the California Dental Hygienists’ As-sociation is formatted by and published under the supervision of the Editor. The opinions expressed or implied in this publication are strictly those of the authors and do not necessarily reflect the opinion, position or official policies of the CDHA nor are claims or statements by authors verified.
The only permission granted for photocopying or storage of items is for personal use, or the use by libraries; all other uses require the written permission of the Editor or President. CDHA reserves the right to illustrate, reduce, revise or reject any manuscript submitted. Articles are considered for publication on condition they are contributed solely to the Journal. Contributors are notified within 90 days if a manu-script is accepted for publication.
Correspondence should be addressed directly to: • E-mail [email protected] • Fax 916-797-1852 • Mail 86 Hancock Dr. Roseville, CA 95678
Display and classified advertising. The California Dental Hygienists’ Association does not assume liability for contents of advertisements. Inquires re-garding display advertising should be directed to:
Shanda Wallace, RDH611 Bristol Ave., Stockton, CA 95204
[email protected] available @ cdha.org
Copyright 2006 by the California Dental Hygienists’ Association. The Journal is published on a regular schedule by the California Dental Hygienists’ Asso-ciation. Subscription rate is $12 for all active members of the Association, $25 for non- members. All change of name or address should be sent to:
California Dental Hygienists’ Association505 N. Brand Blvd., #740
Glendale, CA 91203 818-500-8217 FAX 818-247-2348
E-mail: [email protected]: http://www.cdha.org
“Advancing the art & science of dental hygiene”
In this issue of the…
Journalof the California Dental Hygienists’ Association
President’s Message: Professional Evolution Susan McLearan, RDHAP, MS ......................................... page 3
On the Road with Coast Smiles on Wheels Maureen Titus, RDHAP .................................................... page 6
SADHA Members Learn from Leadership Visits Kristy Menage Bernie, RDH, BS ...................................... page 9
ADHA Continues to Move Our Profession Forward Katie Dawson, RDH, BS .................................................. page 14
Home Study Course: Meth Mouth & Dental Care Considerations Noel Kelsch, RDH ............................................................ page 16

2 CDHA Journal Vol. 22, No. 2
Random thoughts...Liz Moore, RDH, BS, MSEd
I was struck by the quotation above from the new book by Dr. Robert Marx, Oral & Intrave-nous Bispohophonate-Induced Osteonecrosis of the the Jaws. In his excellent new book, he recounts having experienced just this set of circum-stances. He relates, “When I issued a medical alert that described modern-day intravenous bisphosphonate-induced exposed bone that failed to heal and even worsened with surgi-cal debridements, the reality of the condition was almost universally denied and the report widely disbelieved.” He states it was not until his colleague Dr. Salvatore Ruggiero published a report of cases he had seen, followed by other smaller reportings by other clincians, the real-ity could no longer be denied.
Dr. Marx is viewed as a leader of the oral sur-gery community, and I’ve heard surgeons say, “If Bob Marx says it’s so, that’s good enough for me.” So when I researched the article on Bisphosphonates published in our Fall CDHA Journal, I was astounded to see that dental organizations and individuals were saying we see a correlation but no direct link between the IV use of this medication and this disease. Even more interesting was the fact denial that oral bisphosphonates were even to be considered as a potential problem. I kept ask-ing myself – what does it take to say there’s a definite link? Egads!
When I first went online to the OsseoNews blog last fall, I printed out 3 pages of comments by dentists and concerned individuals. These people were saying, regardless of the pub-lished studies and the stated positions of the
The Three Stages of a Scientific TheoryStage 1: It is scoffed at and met with disbelief.Stage 2: It is accepted as true but insignificant and trivial.Stage 3: It is thought to be correct and even revolutionary. In fact, those who criticized it most now claim that they invented it and are the experts. –Anonymous
pharmaceutical company panel, they were see-ing patients in their offices with symptoms of ONJ following 4-5 years of oral bisphosphonate use. Three months later, I returned to that site and printed out 8 pages of similar comments, with increasing number of contributors saying they have patients exhibiting these symptoms. I found that telling.
In his book Dr. Marx devotes an entire chap-ter to cases of oral bispohphonate induced ONJ. He states on page 77 “In general, cases of osteonecrosis of the jaws induced by oral bisphosphonates differ dramatically in three significant ways from those induced by intra-venous bisphosphonates. First, a longer period of exposure to the bisphosphonates is necessary before exposed bone develops. Second, the amount of exposed bone is smaller and the symptoms are less severe. Third, discontinu-ation of the oral bisphosphonate may lead to gradual improvement and even spontaneous healing of the exposed bone, which is also more responsive to local debridements after about 6 months to 1 year.”
I urge clinicians to get a copy of this book to learn more about this issue, to be in the best position to help their patients. In my opinion it is the best book available with excellent draw-ings, case photos, and written so the compli-cated science is understandable. Published by Quintessence Publishing, it can be found on their website at www.quintpub.com.
A Biz Update

CDHA Journal Vol. 22, No. 2 3
Susan McLearan, RDHAP, MSCDHA President
Professional Evolution:Neither unique, radical nor impractical
In 1914 when the very first class of 27 women graduated from Dr. Fones’ School things were a bit different in many ways than
they are today.
• The equipment and supplies for their 40 week course came to a whopping $172.20.
• Only women were allowed to study dental hygiene (true until 1964)
• Women did not yet have the right to vote
In a report on the Bridgeport clinic recorded in The History of the American Dental Hygienists’ As-sociation 1923-1982, Fones said,
“this work in the schools is es-sentially woman’s work, and is the great field for the dental hygienist, to whom it open up paths of usefulness, activity and inspiration hitherto undreamed of, allying her with the workers of the world who are helping humanity in masses.”
The hygiene preventive clin-ics in the Bridgeport schools compared very favorably with “relief and repair” clinics. The woman’s work, as reported by Fones, proved to be statistically significant in reducing dental disease.
con’t on page 4
The first DH graduates referred to themselves as pioneers and in some ways parallels can be drawn to the suffragettes pioneering efforts to obtain the vote for the half of the population to which it had been denied.
In the struggle for the 19th Amendment, a few people, women and men, passionately pursued rights for all. We are very fortunate the suffragettes did not aban-don their goal – even though they did not have full support. It was a long effort, some 72 years, but the endeavor was finally successful.
The lack of full support and the reality of staunch opposition are as true for dental hygiene as it was for the people who fought for the vote.
Even though women hold a monopoly in dental hygiene (an-other situation that must end),
this is not a gender issue. This is a power issue.
Do we want to be dentists? Not I. Or, do we want power over our own
scope of practice? And, yes, some of us will want to develop additional competence and
extend our scope to better serve the public’s identified needs.
Nurses, Occupational and Respiratory Therapists have all gained independence before us. Our goal of
A Biz Update

4 CDHA Journal Vol. 22, No. 2
self determination (self regulation) is not unique. These health care providers have served the public well, providing care that is both more cost effective and practical than leaving every health care duty to the medical doctor. All of these professions are self regulated.
The same will hold true for the dental profession. Mid level, self-regulating practitioners must be legalized to serve the need. Ignoring the need and creating road blocks for proven solutions should not be acceptable. Why do we allow it?
In the 21st Century, dental hygienists must take a more active role on the path to professionalism. The world is too complicated and in many cases, too corrupt to leave leadership to the few, or even, to someone else.
CDHA “Anything is Possible” Raffle!
2 Prizes to be Awarded
Grand Prize ~ $2,000 Gift Voucher
2nd Prize ~ Dentsply SofTip Implant Insert
$10.00 voluntary donation per ticket Only 2,000 tickets will be sold!
Drawing at the conclusion of the CDHA House of Delegates ~ June 10, 2007
Winner need not be present to win Proceeds to benefit CDHA, a non-profit organization,
Advancing the art & science of dental hygiene
Tickets on sale now! See your Component Trustee Or CDHA Leader
There will be those who choose to take a passive role. We must wish them luck.
The rest of us must overcome our fear of taking a stand and begin taking a leadership role in the de-livery of health care.
Abstract thought and dreams are what separates us from lower animals. Let’s each develop our own mis-sion and goals rather than waiting until our role finds us or allowing ourselves to be swept up in someone else’s dream.
These are extraordinary times and such times de-mands extra ordinary behaviors from each of us.
Having a mission in life, a vision for ones’ future is having a dream with teeth.

CDHA Journal Vol. 22, No. 2 5
CDHA Presents...Spring Scientific Session 2007
“Drugs, Herbals and Nutraceuticals: New Issues for Dentistry”Featuring
Dick Wynn, Ph.D
Friday, May 4, 2007Up to 6 CEUs ~ Category I
7:30 a.m. - 4:00 p.m.Exhibits, Table Clinic Session, C.E. Course
The Sheraton Park Hotel, 1855 S. Harbor BoulevardAnaheim, CA (714) 750-1811
(Parking ranges from $6 ~ $12)
• This course will present a mix of the most recent reports describing conventional drugs, herbal supplements and nutraceuticalshaving impact on dental practice. For conventional drugs, the aspirin and Plavix patient will be discussed, newly approved dentaldrugs and products described including those for RAU, herpes labialis, new dentifrices, “remineralization” dentifrices, OTCwhitening/bleaching agents; Halcion and the new Z-drugs for sedation; articaine and paresthesias, the most recent FAQs onantibiotic prophylaxis presented, the latest on heart attacks, CRP, homocysteine levels and periodontal disease discussed includingantibiotic use and increased risk of breast cancer; and life after the Vioxx fiasco.
Payment Information: Mail Registration Form and California Dental Hygienists’ Association�Discover Card �Master Card �VISA �Check payable to CDHA payment information: 505 North Brand Boulevard, Suite 740Credit Card# _________ -_________ -________ -_________ Expiration:___________ Glendale, CA 91203-3948Name on Card:________________________________________ 3 Digit Code___________ (818) 500-8217 • (818) 247-2348 FAXSignature:__________________________________________________________ [email protected] www.cdha.org
Fee Schedule (includes course, morning refreshments, Postmarked After 4/20/07lunch, table clinics, and exhibits) by 4/20/07 and On-Site
� ADHA Member ............................................................. $130.00 ............ $150.00� Non-Member .............................................................. $190.00 ................ $210.00� Student/Guest .................................................................. $60.00 .................. $60.00
Name: Telephone:
Address: Membership ID:
City: State: Zip:
Professional Designation: � RDH ��RDHAP � DDS �� RDA �� Student �� Guest
E-Mail Address:Refund Policy: A refund will be made if the reservation is canceled by 5 p.m. on April 27, 2007
NO CONFIRMATION WILL BE SENT sss07pm
New Member Special!
Receive this course for only $60
by joining ADHA, CDHA and your
local component now! Questions?
Call (818) 500-8217
• List the new dental drugs and dental herbal products with their proven effectiveness and ineffectiveness • Describe the concept of free radicals and antioxidants and review their uses in medical and dental conditions • Outline those medical and dental conditions in which nutraceuticals have been show to be effective and those not effective • List the key considerations in treating the patient on antiplatelet therapy
By the completion of the course, each participant should be able to:
• Describe the most recent theory on the relationship between CRP, gingivitis and heart attacks • List the safety concerns by the medical profession about herbal use in patients and effects on surgery and recovery, including herbs
that cause bleeding
Table Clinics Supported Through an Educational Grant From:
Supported ThroughEducational Grants From:

6 CDHA Journal Vol. 22, No. 2
Photo courtesy of Char Bruzenak.
This is the next chapter on my road trip or journey which I began to share with you several months ago. Speed
bumps have been encountered along the way as well as new directions.
In January of 2006, I applied for the Denti-Cal provider number with forms I downloaded from their website, then waited. After a few weeks, I received a large packet of forms from Denti-Cal to, again, complete and return to them for a provider number. I then made a phone call and asked the representative at Denti-Cal what had happened to my previ-ously submitted forms and I was informed the website forms were outdated and no longer accepted. Of course I inquired as to why they were still on the website, wasn’t that confus-ing to future providers? I finally received my provider number in April, 2006.
While waiting for the Denti-Cal approval, I began the process of purchasing instruments and other supplies I would need. I sought the advice of experienced RDHAP’s for recom-mendations of portable equipments to use. It was suggested that I wait to buy the more advanced units after I started my practice to learn what I would really need. Many of the residents in skilled nursing facilities (SNF) would not like the loud sounds the compres-sor or vacuum would produce. I decided to go with the low key approach to begin with, since I was funding my business without a loan, only my savings. One of my funding sources was my little car, which had many miles on it, and I was concerned it was ready to leave me stranded. I sold it to a friend for her daughter, however her husband liked it so much it’s now his car.
The need to create a final brochure to promote my business was my next project. I had the business class I attended give me feedback on the draft version. Some graphics I had se-lected were removed and a more concise brochure evolved. After printing, I began to distribute my brochures to vari-ous individuals and groups involved with SNF’s or home health care agencies. Because the RDHAP is an unfamiliar position to many people, I spent additional time explain-ing and discussing my services at the time I presented my brochures. A physician who has many patients in one of the local SNF was thrilled about my business, saying she would write all the medical orders I needed.
From that encouragement I proceeded to schedule a meet-ing with the social service director at the SNF to explain the dental hygiene care I could provide for the residents. She seemed very interested and said that she would discuss the idea with the administrator. I had also learned that there was a dentist who had a mobile practice and was seeing the residents at this SNF. I finally received a phone mes-sage from the director and was told that the administrator decided that it could be a conflict of interest to promote me, since the dentist also provides oral health care and they cannot afford to have him be upset and stop coming to the SNF. The SNF’s are required to contract with a dentist to provide dental care and there are very few dentists willing to treat this population. While I understand the facility’s concerns, it also is a concern that a dentist can block a RDHAP from providing preventive oral health care.
In October, 2006 I received my first referral from a dentist in San Luis Obispo to see a long time patient of his at the very same SNF I mentioned above. A dental hygienist friend works for the referring dentist and she suggested that I could travel to his bedside for dental hygiene care. What a great way to start!!! I met with the patient and his family then made plans to provide a prophylaxis for him. I stopped by the social service director’s office to inform her I would be seeing a resident the following week. When the family or a referring dentist requests a RDHAP to
ON THE ROAD WITH COAST SMILES ON WHEELS... A JOURNAL - Chapter Two
by Maureen Titus, RDHAP

CDHA Journal Vol. 22, No. 2 7
treat a specific person, the SNF cannot refuse the request.
I have met with the nursing director in another private Alzheimer’s care facility at the request of a family member who brings her mother into one of the private offices where I practice. The nursing director was very enthusiastic and wanted to print my brochure in their newslet-ter that is sent out to families of the residents. The same dentist I spoke of earlier also sees this facility’s residents and his fee for a prophylaxis is less than what I would charge. That could be a concern; however, I will continue to promote my services for the skills I possess.
After awhile I decided to write this particular dentist a very nice letter introducing my self and suggested we could collaborate our efforts to provide access to dental care for these under-served SNF residents. I did copy the president of the local corporation who owns several of the SNF’s that the dentist contracts with, as well as Ron Mead, a respected oral surgeon from San Luis Obispo and the current presi-dent of California Dental Association (CDA). To date the only person who has contacted me regarding this letter is Ron Mead. I have left several messages with the dentist but have had no response. Although the president of the corporation has not spoken with me yet, I do plan on connecting with him.
I was recently told by several attending San Luis Obispo dentists and our CDHA officers that during the 2006 CDA House of Delegates, newly installed President Ron Mead spoke in support of RDHAP’s within California. At a recent lunch meeting with him, we discussed my local concerns as well as the problems many RDHAP’s in California are facing. He has given me permission to quote him on thoughts contained in his installation speech regarding RDHAP’s . He is aware of our efforts to be accepted as providers in SNF’s and how many of us have met resistance from the staff dentists. He stated in his speech at CDA, “ it would be ideal if the residents were receiving regular care from a dentist but I don’t believe this is the case”.
On the RDHAP/DDS collaboration issue, Dr. Mead’s comments included, “If a patient chooses to see a RDHAP, the dentist should communicate the patient’s need to the RDHAP. The patient may not be one of the most con-sistent patients. Ask the RDHAP to stress the need for a complete exam and treatment plan. If there is a good working relationship it will be
mutually beneficial. Keep them as part of your dental team. Don’t force them to be independent by your unwillingness to work with them. We must make the relationship as smooth as possible. Remember, we are moving forward, together.”
I do not believe CDA can “force” change upon any dentist who is unwill-ing to accept change, even with encouragement from their President. I do believe his comments to the House of Delegates are sincere and a step in the right direction. Access to oral health care, which can benefit many people in our communities, is a long term goal for me. RDHAP’s and DDS’s must work together for access to become reality. There can be a new approach with AB 1334, allowing RDHAP’s to provide care for 18 months before a formal prescription is required.
Since the SNF’s have presented me with a “speed bump,” I have a meeting in one week with a local care facility where developmentally disabled individuals live. I know there are many facilities and individu-als that can benefit from preventive oral health care which I can provide. These challenges will not stop me from continuing to pursue my goal. Dental hygienists are more than willing to collaborate with all health care professionals, however, there still seems to be fear or unwillingness with too many dentists to achieve this collaborative state.
The future is unknown, however, I will share my journey or road trip with anyone who wants to listen.
A TributeAt this time I would like to honor a special man who encouraged me to pursue a goal. To hold my license as a RDHAP I am required to have a relationship with a dentist, who could be called upon for consultation, emergencies and referral. During the fall of 2005 I asked Robert Campbell, DDS, to be my dentist of record and he was more than willing to be that person.
“Dr. Bob,” as he was referred to by patients, practiced with Ron Barbieri, DDS, in San Luis Obispo. He appreciated and supported the idea of thinking “outside of the box” to provide dental hygiene care to people in a non- traditional setting.
Unfortunately, Bob had been fighting colon cancer for almost 3 years, yet he was still treating his patients between chemotherapy treatments. What an amazing strength of character and commit-ment to his profession. There were days you could tell he wasn’t feeling well, but when asked,; he would only say he was “feeling pretty good today.” I work at Ron Barbieri’s office on Mondays, and knowing that it wasn’t my favorite day of the week, Bob would always say, “Happy Monday!” to me. Sadly, he lost his battle with colon cancer on December 5, 2005, and the loss for his wife and their three children was devastating. His patients, and those of us who were fortunate enough to have known him, will always be grateful for his kindness, compassion, sense of humor and love of people and God.

8 CDHA Journal Vol. 22, No. 2
Join The Nation’s Top Hygienists… Recommend BreathRx To Every Patient
Your patients can now also get BreathRx at these fine stores:
AD
V-21
00 0
1080
7
800-422-9448
www.discusdental.com/hygienist
F O R F R E S H B R E A T H
D E N T A L H Y G I E N I S T S
U N I T EEverybody wants fresh breath. When you recommend
BreathRx to your patients, you’re recommending
the system scientifically formulated to eliminate
oral malodor-causing bacteria and actively neutralize
the volatile sulfur compounds they emit.
This simple Brush - Scrape - Rinse solution has only
been available through dental offices like yours, but
now your patients can also find it in many drug stores
and grocery stores from coast-to-coast.
Every patient deserves
fresh breath and you can
give it to them…in your
office or from your
local retailer. Give Science a TryTM
C
M
Y
CM
MY
CY
CMY
K
ADV_2100_010807_brx.pdf 1/8/07 3:50:10 PM

CDHA Journal Vol. 22, No. 2 9
Programs Take Advantage of CDHA Leadership Visits
CDHA has always appreciated our future col-leagues and supports dental hygiene students through a variety of programs. One program that has received rave reviews is the CDHA Leadership Program Visits. This program provides students one-on-one access to CDHA leaders. Topics are tailored to each program as requested. Schools have gone as far as creating a full SADHA event with updates, fund raising review and establishing the year’s goals.
CDHA has enjoyed this outreach program, and been able to access nearly all students and fac-ulty at these schools. We look forward to these future colleagues becoming active members of ADHA/CDHA!
SADHA Members Learn from Leadership Visits
by
Kristy Menage Bernie, RDH, BS, RYT, SADHA Council Chair
CDHA Announces the Annual SADHA Regional Conferences
Put these on your calendar:
February 3, 2007 Concord Hilton, Concord, CA
February 4, 2007 Radisson Hotel, Culver City, CA
These events will feature a presentation regard-ing employment options within the profession. Co-sponsored by Philips/ Sonicare, this popu-lar annual event will include the opportunity for students, faculty and CDHA leaders to net-work and visit with exhibitors and each other. Registration information can be found online at: http://cdha.org/sadha/index.html
con’t on page 10
Cerritos SADHA members show their enthusiasm and camaraderie.

10 CDHA Journal Vol. 22, No. 2
CDHA Announces the 2007 Cora Ueland Scholarship Essay Competition
The California Dental Hygienists’ Association is pleased to announce the 6th annual Cora Ueland Scholarship for dental hygiene stu-dents. This scholarship was first established as a fund in the 1950’s in the memory of Cora Ueland, founder and director of the dental hygiene program at the University of Southern California. Supported by individual and com-ponent donations, the fund was distributed in recent years as a loan to eligible students. In 1998, the CDHA Board of Trustees voted to convert the loan into a scholarship. Two $1,000 awards will be awarded to one (1) first year and one (1) second year student. Applications must be postmarked by Feb. 15, 2007. Appli-cation and information are located online at: http://cdha.org/sadha/2007_cu.htm
Students from District XI (California & Arizona) are invited to apply for the District Student delegate position!
STUDENT DELEGATE & ALTERNATE DELEGATE
Students have a unique opportunity to apply for a position as Student Delegate or Alter-nate Student Delegate. As a Student Delegate, you not only represent all student members
of ADHA, but you also sit on the House of Delegates floor during all three meetings. In addition, dur-ing the Student House of Rep-resentatives, student dele-gates elect one Voting Student Delegate who votes on behalf of all SADHA members.
Student delegates and alternates are funded to attend their district workshop and ADHA’s Annual Session. Funding consists of airfare, lodging (two students per room), ground transportation and per diem. Because funds may vary annually, please contact your District Trustee for the exact dollar amounts.
In August each year, ADHA mails the criteria and applications for student delegate posi-tions to SADHA Advisors. The advisors are asked to distribute the information to SADHA members.
Qualifications:• Must be a SADHA member.• Must be a matriculating dental hygiene
student with a minimum of one semes-ter/trimester remaining after annual session.
• Must be in good standing in a dental hygiene program and have written approval of the program director for candidacy.
• Must be available to fulfill all obligations of a district workshop and full attendance at the ADHA Annual Session.
Completed applications are due to your ADHA District Trustee ([email protected]) by February 15. Applications can be accessed at: http://cdha.org/sadha/index.html
2006 Student Delegate and Alternate Student Delegate Reports
Allie Witt, the student delegate, was elected the voting student delegate to the ADHA House of Delegates and did an outstanding job representing student opinions and op-portunities!
This past year District XI was also represented by Arizona alternate student delegate Am-ber McCoog, who submitted the following report:
Amber McCoog, District XI Alternate Student Delegate, Phoenix College:
As an alternate student delegate, I was able to experience many opportunities. The first of which was traveling to Burbank, California for District XI’s caucus. After Burbank, it was off to San Francisco for California’s House of
Amber McCoog, Alternate Student Delegate(L), Shanda Wallace, Student Mentor and Allie Witt, Student Delegate (R) at the ADHA Annual Session where students participated and learned.

CDHA Journal Vol. 22, No. 2 11
Delegates, and then Orlando for the ADHA annual session. I learned a lot between these trips and am proud to be apart of the orga-nization.
Once I found out I was chosen, I left for Bur-bank, California. I was lost at first, but after the initial meeting I was able to settle in. I got a chance to meet with our district members and discuss different issues. I was happy to find the women in our district are very strong individuals. It’s nice to be apart of an organi-zation that will fight for what they believe in (whether they all agree or not). I am so proud of our district. These women do so much for our profession.
After the first caucus, I was able to attend Cal-ifornia’s House. This really helped prepare me for the annual session in Orlando. California has so much involvement and I can only hope that some day Arizona will be as involved. All the ladies from District XI helped me with any questions I had and helped prepare me for the SHOR meeting at the annual session.
I was able to meet several awesome students from California that are very passionate about our profession. I even saw some of the girls in Orlando. I was so well prepared from the
district members that I was able to answer a lot of the questions that other students didn’t know.
On the last trip, I headed to Orlando for our annual session. I didn’t realize how busy our schedule was going to be but I have learned so much about what the association has done for our career. All of us have a voice and can speak about issues that concern us. Without our association, hygienists would not have a strong voice. This is how we are able to give anesthesia, have affiliated practice, and hope-fully soon open the doors for an Advanced Dental Hygiene Practitioner.
This is such a great learning experience for individuals. It helps us understand that we need a voice to fight for what others are try-ing to take away from us. We are professionals and no one should be able to take that from us. Every hygienist should help contribute to our association. This is what keeps our career going, and it keeps our jobs safe and secure.
Upgrade® Disposable Prophy Angles
www.sultanhealthcare.com
Upgrade’s® beveled gearing runs cooler, quieter
and smoother, providing:• LESS noise• LESS vibration• LESS heat generation • LESS operator fatigue• Highest patient comfort• Best overall performance
Upgrade® Disposable Prophy Angles
100/pkg AD30100.....Firm Cups AD30101.....Soft Cups
1,200/pkg AD30503.....Firm Cup AD30502.....Soft Cups
The patented Upgrade angle with beveled gearing runs with less vibration than traditional straight gear angles.
STRAIGHT GEARING BEVELED GEARING
SC4578_UpgradeHalf 12/8/06 4:40 PM Page 1

12 CDHA Journal Vol. 22, No. 2
The #1power toothbrush brand personally used and recommended by dental proffessionals1 just got better.
Introducing the new Sonicare Elite e9000 series with the Custom Care system, designed to meet your patients’ unique brushing needs.
Experience the new Sonicare Elite e9800
2 brush head sizesStandard: ideal for a complete cleaningCompact: 30% smaller than standard brush head for improved access to hard-to-reach areas
2 cleaning modes
Max: for a thorough, everyday clean
Gentle: for sensitive areas of the mouth
NEW®
12005 data on file.
Exclusive offer for dental professionalsContact your local Sonicare representative or call 1-800-676-SONIC (7664) to order your Sonicare Elite e9800 trial unit. Visit www.sonicare.com for more information.

CDHA Journal Vol. 22, No. 2 13
For easy visual com-pliance use patented CitriSil Blue™ which provides a light blue color in the treated water.
APPROVED FOR SALE IN CALIFORNIA!Save time and money while simplifying waterline compliance!
SIMPLE – SAFE – EFFECTIVE1-877-755-PURE (7873)
www.sterisil.com
Buy 3 BoxesGet 1 FREE
CONTACT YOUR DEALER TODAY!CitriSil part No. C20-W, CitriSil Blue part No. C20-B
Cal_AD.indd 1 9/13/06 10:42:46 AM

14 CDHA Journal Vol. 22, No. 2
The ADHA “Clinical Practice Guideline” (CPG) continues through develop- ment by the CPG Task Force. This docu-
ment will serve to provide guidelines for the clinical practice of dental hygiene. One of the common requests coming from the branding campaign input was the desire for tools that will improve the clinicians’ quality of care pro-vided to patients and clients. The Task Force projects completion of the draft by early spring in time for review during the March 2007 meet-ing of the Board of Trustees; the guideline will also be presented to the general membership during the June 2007 annual session in New Orleans.
The ADHA 2007-2010 Strategic Plan was de-veloped by the Board of Trustees, councils and staff; also included in this process was the input provided by the general membership during the strategic planning forum at the 2006 annual session in Orlando.
The five new goals of the ADHA strategic plan are as follows:• The dental hygiene community will under-
stand the value of ADHA membership and choose to belong.
• ADHA will be the recognized community and resource for dental hygiene.
• ADHA will be a data driven, fiscally sound, effectively governed organization.
• The dental hygiene profession will advance through effective advocacy by ADHA.
• ADHA and its members will work in part-nership with dentists to advance the oral health of patients.
One of the major considerations in developing the strategic plan was utilizing the feedback provided by the branding campaign data. It became evident that ADHA can no longer do the same things the same ways we’ve always done – change is inevitable. One of the first changes will be the identification of the stra-tegic plan’s primary objectives.
The three primary objectives adopted by the board were as follows:• Expand collaborative opportunities for the
professional associations to work syner-gistically
• Establish our brand identity• Increase tangible membership benefits
The six secondary objectives adopted by the board were as follows:• Increase visibility and communications• Understand the values of dental hygiene
students and other potential members• Expand opportunities to promote quality
patient care delivered by the dentist and dental hygienist in partnership
• Increase our ability to collect and use data• Expand partnerships with stakeholders• Increase the public’s direct access to dental
hygienists (CPG)
The Advanced Dental Hygiene Practitioner (ADHP) Task Force continues with the devel-opment of the draft curriculum framework. Future meetings are scheduled for the spring of 2007; an update will be presented during the March 2007 BOT and June 2007 annual session
ADHA Continues to Move Our Profession Forward
by Katie L. Dawson, RDH, BSGovernment Relations Committee Co-Chair

CDHA Journal Vol. 22, No. 2 15
meetings. The ADHP Advisory Group is not funded for formal meetings during the current fiscal year, however dialogue continues with the group.
ADA Meeting Proposals Would Affect Dental Hygiene
The October 2006 American Dental Association annual session was attended by ADHA officers and senior staff. The annual session provided an opportunity for the ADA to introduce its proposal for addressing allied personnel work-force issues. Of interest to the ADHA were the resolutions calling for the development of two allied dental personnel – the Oral Preventive Assistant (OPA) and the Community Dental Health Coordinator (CDHC). These proposals expand the scope of practice of the dental as-sistant and broaden the description of current dental hygiene practice.
The OPA resolution called for the appointment of a work group to design and develop pilot projects that can be carried out to test the OPA model in selected states or locales. The OPA is envisioned to provide scaling of perio Type I (gingivitis) patients. The primary concern is that the educational component would be for 12 months with no requirement for the program’s accreditation.
The CDHC resolution calls for the develop-ment of three pilot training programs in 2007-2008 envisioned to work in community-based settings such as state/local health clinics or with private practitioners serving underserved communities. For the most part, the CDHC proposal, in nearly all cases from a scope of practice perspective, outlines duties that can be performed today by dental assistants and den-tal hygienists. The ADA Foundation provided over $300,000 for the immediate development of the pilot training programs.
Another issue of interest to ADHA is the ADA’s membership study proposal. This proposal will develop an allied dental health personnel category of membership within the ADA. The debate created a great deal of interest and was referred to the Council on
Membership for further study and a report to the 2007 House of Delegates. If adopted, the dental professional associations would offer membership to dental hygienists and dental assistants. Local constituents and components would be encouraged to offer the same mem-bership to their allied personnel.
The Calfiornia Government Relations Council (GRC) Legislative Update
GRC members, Katie Dawson, RDH, BS, JoAnn Galliano, RDH, M Ed., and Lori Gagliardi, RDH. M Ed., attended the No-vember 14-16 meetings of the Dental Board of California and the Committee on Dental Auxiliaries’ meetings in Sacramento. The GRC reminded DBC members of Governor Schwartzennegger’s message included in the veto of SB 1472 (Figueroa). His veto message included the following statement: “I believe the concerns of dentists and dental hygienists can be addressed within the existing regula-tory structure through the cooperation of all interested parties. I strongly encourage the Dental Board to work with the dental hygien-ists to provide the existing Committee on Dental Auxiliaries with a stronger voice on the Dental Board.” One of the recommendations suggested by COMDA was a reconfiguration of the current DBC. The current membership of the DBC includes eight dentists, four public members, one dental assistant and one dental hygienist. Please visit the CDHA website at http://www.cdha.org for the complete legislative update/report.
GRC is drafting new legislation to create a dental hygiene board or bureau that will allow self-regulation of dental hygiene by dental hygienists.

16 CDHA Journal Vol. 22, No. 2
Meth Mouth & Dental Care Considerations
As dental healthcare professionals, it is vital to be aware of the illegal use of Methamphetamines (MA). MA has
a direct effect on a person’s health, lifestyle, ability to function and mental status. Unlike many other street drugs, the use of MA is increasing. Dental professionals must have knowledge of the symptoms of use, possible side effects, drug interactions with medications and dental treatment considerations. This will aid in delivering appropriate dental treatment and patient education.
MA is a popular illegal drug choice because:1. It is cheap to produce ($600 of material =
$2,000 MA)2. The high it induces lasts on average twelve
hours (cocaine averaging one hour in comparison)
3. It’s easy to make4. Materials used to manufacture MA are read-
ily available5. It can be smoked, snorted, melted and
injected, taken orally, placed rectally, or vaginally1
6. It’s a very effective central nervous system (CNS) stimulant and gives the user a feeling of euphoria, strength and endur-ance
These MA facts have lead to a fi ve-fold in-crease in usage in the past decade.1 Side ef-fects of MA on the oral cavity and the CNS are severe and can include permanent brain damage.2 Results of MA use are devastating, and can have fatal consequences. MA users experience acute and chronic mental, physical, and behavioral changes.
History
As early as 3000 B.C. Chinese writings men-tioned the ephedra plant, the source of the alkaloids ephedrine and pseudoephedrine.3 First synthesized in 1887 as a medication for dealing with everything from “tired blood to breathing diffi culties,” MA was patented in the 1930’s for use in individuals with asthma, rhinitis and for its anorectic effects. MA’s eu-phoric and anorectic effects were quickly rec-ognized and led to severe abuse of the drug. During the Second World War, MA was used by soldiers to increase wakefulness and at-tention, resulting in many soldiers coming home addicted to the substance. The 1940’s followed as a pandemic of abuse, with this pattern spreading to countries such as Japan
By Noel Kelsch, RDH

CDHA Journal Vol. 22, No. 2 17
Methamphetamine user, 21 year old Chris, displaying classic oral symptoms from his drug use. As a result of his MA use, Chris suffered a series of strokes and memory loss so severe he doesn’t really remember those strokes. Photos courtesy of Dr. Mitchell Goodis.
These photos demonstrate the tremendous toll methamphetamine use takes on the overall health and physical appearance of the user. Photos courtesy of Sheriff’s
Department, Multnomah County, Oregon United States Department of Justice Meth
Awareness Program.
Methamphetamines and Cocaine are often confused in the eyes of the public but affect the user differently.
Methamphetamine
Man-made
Smoking produces a high that lasts 8-24 hours
50% of the drug is removed from the body in 12 hours
Limited medical use
Cocaine
Plant-derived
Smoking produces a high that lasts 20-30 minutes
50% of the drug is removed from the body in 1 hour
Used as a local anesthetic in some surgical procedures

18 CDHA Journal Vol. 22, No. 2
and Sweden. There were very few regu-lations on the use of MA which lead to the over-use. In the 1950’s, substance regulation became more stringent and yet the drug continued to be abused by students, athletes, truck drivers and oth-ers. The Controlled Substance Act of the 1970’s strictly regulated the manufactur-ing of this particular amphetamine. Even though there was a severe decline in the manufacturing of the drug, the use of street meth has increased notably.4
Composition
MA is a synthetic psychomotor stimulant and is closely related to decongestants, ephedrine and phenylpropanolamine.1 It is synthesized by converting ephedrine or psuedoephedrine into methamphet-amine through a process of distillation. This process can be achieved by simply following “cookbook” directions found on the Internet which include prepara-tion hints as well as the essential ingre-dients.3 The ingredients necessary are available at any hardware store, feed store or local pharmacy. Substances such as tincture of iodine, denatured alcohol, red phosphorus, psuedonepherine, lye, lithium, and anhydrous ammonia, are all readily available and relatively cheap (Table 2). Illicitly synthesized MA may be contaminated by inorganic compounds.
Bikers Coffee Stove TopChalk TrashChicken Feed Yellow BamCrank YabaCrystal Meth MethGlass Black BeautiesGo-Fast TweekMethlies Quick FirePoor Man’s Cocaine UppersShabu Psycho dopeSpeed
Table 3: Street Names for Methamphetamines
Product Hydrioic acid
Tincture of iodin
Acetone/Ethyl alcohol
Red phosphorus
Pseudonepherine
Phenylpropanoa-mine
Lithium
Anhydrous ammonia
Freon
Available From
Pool supply
Feed store
Paint store
Strike pad on match book
Pharmacy
Pharmacy
Batteries
Fertilizer
Automotive
Side effects
A corrosive acid with vapors that are irritating to the respiratory system, eyes, and skin. If ingested, causes severe internal irritation and damage that may cause death.
Give off vapor that is irritating to respiratory system and eyes. Solid form irritates the eyes and may burn skin. If ingested, cause severe internal damage.
Extremely flammable, posing a fire risk in and around the laboratory. Inhalation or ingestion of these solvents causes severe gastric irritation, narcosis, or coma.
May explode as a result of contact or friction. Vapor from ignited phosphorus severely irritates the nose, throat, lungs, and eyes.
Ingestion of doses greater than 240 mg causes hypertension, arrhythmia, anxiety, dizziness, and vomiting. Ingestion of doses greater than 600 mg can lead to renal failure and seizures
Ingestion of doses greater than 75 mg causes hypertension, arrhythmia, anxiety, and dizziness. Quantities greater than 300 mg can lead to renal failure, seizures, stroke, respiratory failure and death.
Extremely caustic to all body tissues. Reacts violently with water and poses a fire or explosion hazard.
A colorless gas with a pungent, suffocating odor. Inhalation causes edema of the intestinal tract and asphyxia. Contact with vapors damages eyes and mucous membranes
Inhalation can cause sudden cardiac arrest or severe lung damage. It is corrosive if ingested.
Table 2: Common ingredients in Methamphetamine production

CDHA Journal Vol. 22, No. 2 19
fulness, increased physical activity, decreased appetite, increased respiration, hyperthermia and euphoria. Other CNS effects include irri-tability, insomnia, confusion, tremors, convul-sions, anxiety, paranoia and aggressiveness. It is important to note that hyperthermia (with temperatures as high as 108 degrees) and con-vulsions can result in death.1
Physical/Mental Signs and Symptoms
Although we may have been unaware of it, most of us have treated a MA user. The signs and symptoms of MA use are sometimes subtle and other times clearly evident. Rec-ognizing the signs and symptoms of MA use is vital in keeping patients safe from harming themselves, as well as others and the create a treatment program that meets each patient’s needs.
People react to the presence of MA in the body just as they would with the fight or flight syn-
There have been cases of exposure to every-thing from lead to carcinogenic materials.4
Though many states have limited the distri-bution of some of the materials necessary to manufacture MA, many materials are available by simply crossing a state line.
Table 3 shows the street name for methamphet-amine varies from region to region (Table 3)
Interaction
At the cellular level, methamphetamines stimulate the release and blocks the reuptake of neurotransmitters called monoamines (dopa-mine, norepinephrine and serotonin). Several areas of the brain are affected by this cellular process and the result is a feeling of euphoria. The “rush” that many MA users report is a result of the high release of monoamines into the CNS.5
Brain imaging studies show that amphetamines increase a person’s dopamine level, especially within the nucleus acumen, the major reward center in the brain that is thought to be central to mediating addictive behavior. Supporting this hypothesis is the notion that stimulant-induced euphoria is related to the dopamine levels and occupancy of the dopamine recep-tor. While the acute use of MA results in an in-creased dopamine level, prolonged use results in a chronically depressed dopamine level. The chronically depressed dopamine level can result in symptoms like those of Parkinson’s disease, a severe movement disorder.3
The prolonged use of MA also results in chroni-cally depressed dopaminergic activity. The changes in dopamine level and activity are thought to be due to the neurotoxic effects of chronic methamphetamine use, which leads to the reduction of axonal dopamine transports, and synthesis pathways in dopaminergic neu-rons. Animal studies show repeated exposure to MA results in degeneration and destruction of dopamine axon terminals within the CNS. The CNS actions that result from taking even small amounts of MA include increased wake-
con’t on page 20
Long term physical and mental effects of methamphetamines
High blood pressure
Increased risk behavior
Stroke, heart infections, cardiac arrest
Liver disease, lung disease, kidney disease
Cracked teeth, destruction of oral cavity
Sores, skin infections, acne
Hallucinations, delusions, psychotic events
Violence
Anxiety, paranoia, insomnia
Weakened immune system
Brain damage
Short term physical and mental effects of methamphetamines
Euphoria, surge of energy
Seizures, tremors
Sweating, clammy feeling skin
Nausea, vomiting, diarrhea, loss of appetite
Breathing rate and blood pressure increase
Headaches, dilated pupils
Surge of energy, euphoric feeling
Elevated body temperature, increased wounds that do not heal
Dry mouth, bad breath, uncontrollable clenching
Compulsive behavior
Grinding and clenching of teeth
Table 4

20 CDHA Journal Vol. 22, No. 2
Photos courtesy of Sheriff’s Department, Multnomah County, Oregon United states department of Justice Meth Awareness Program Before and After One year
drome because MA floods the body with adrenaline, the hormone that aids in quick response during an emergency. This reaction gives the user great strength and endurance.1 One person interviewed reported staying awake for over 72 hours in order to complete the painting of his two-story home. Users often report needing less sleep and being able to withstand great amounts of work and strenuous tasks. This unreasonable sense of strength and ability can create an atmosphere for damage to the body and the brain.3
Short term effects of MA use include vomiting, tremors, hyperactivity, and decreased appetite. Long term effects are much more devastating, ranging from allergic reactions to strokes (Table 4). MA use causes increased heart rate and blood pressure and can cause irreversible damage to blood vessels in the brain, producing a stroke. Other effects of methamphetamine include respiratory problems, irregular heartbeat, lowered immune response and extreme anorexia. Its use can result in cardiovascular collapse and death.8
Quality of life is often altered due to the higher incidence of conditions such as Parkinson’s disease(3,6 and Human Immu-no-supressed Virus.7 Psychiat-ric symptoms include anxiety, psychosis, difficulty controlling anger, violent behavior, depres-sion and attempted suicide.9
Case study
A 27 year old male presented in the clinic with a draining apical abscess on #9. His chief complaint was pain with #9. Further investigation revealed that all his anterior teeth had rampant caries and most of his molars had been worn down to the gingival margin. His plaque level was extremely
Skin lesions resulting from the use of MA. Photo courtesy of Prairie View Prevention Services.
Photo courtesy of: Sharlee Shirley, RDH, MPH; Jim Cecil, DMD, MPH, University of Kentucky, School of Dentistry United states Department of Justice Meth Awareness Program

CDHA Journal Vol. 22, No. 2 21
high and he reported he did not know when he had brushed last. His eyes were dilated, his blood pressure was elevated to 165/89 and his temperature was 104.5 degrees. While waiting for his appointment he was observed pacing back and forth while picking at his skin. He explained he was trying to remove the bugs he was sure were embedded beneath his skin. (Author’s note: this feeling is a result of MA constricting capillaries near the surface of the skin, which causes intense itching.6)
Review of his health history revealed he had been using MA in the oral form for eight months. His diet consisted of high carbohy-drate intake in the form of soda to moisturize his dry mouth. His increased bacteria from the lack of care, dry mouth and lowered immune response resulted in rampant caries.
His clothing was stained and the remnants of his last meal remained on his chin. He con-tinued to pace for a short period of time and finally sat down and heaved a sigh of relief. Sweat was rolling down his face and he started to scratch his skin while he lifted his shirt. His skin was raw from constant scratching and his ribs protruded. His face was gaunt and deep lines chased his sagging skin. After the needs of the patient were assessed, he was re-ferred to a General Practitioner for evaluation
and drug intervention before starting dental treatment.
Oral Signs and symptoms The use of MA has a pattern of dam-age in the mouth. There are several factors which, when combined, create an environment that de-stroys the teeth, the blood supply and supporting tissues.
In the past the rampant caries associated with MA use were attributed to the acidic nature of MA in the oral cavity when it was smoked. Studies involving the oral intake of the drug for narcolepsy and attention deficient hyperac-tivity disorder revealed the same characteristic carious lesions seen in MA users. The current hypothesis involves a group of conditions that when combined create the perfect environ-ment for dental disease to occur.12
MA users are unable to take care of daily tasks, such as brushing and flossing, due to the crash affect of this drug which can last many days. When they are awake for long periods
of time the energy bursts they experi-ence do not allow them to concentrate on simple tasks.9 MA causes blood vessels to constrict, including those in the mouth. This in turn causes a lack of the blood that nourishes the periodontium and teeth properly. With repeated shrinking, the vessels will not recover, thus causing dental tissue to starve and break down. The end result is tooth decay, gum disease, and bone loss .12
The caries rate in MA abusers is four times higher than control
Photo courtesy of: Sharlee Shirley, RDH, MPH; Jim Cecil, DMD, MPH, Univer-sity of Kentucky, School of Dentistry United states Depart-ment of Justice Meth awareness program
con’t on page 22
Oral signs of MA use:
Angular Cheilitis
Glossitis
Candidia
Mucosal ulceration
Xerostomia
Facial pain, Trismus, and myofacial pain resulting in sever occlusal wear
Rapidly progressive periodontitis
Rampant caries often starting on the buccal smooth surfaces of posterior and the interprox-imal surfaces of anterior teeth
Table 5Physical and social signs of
MA use:
Malnourished appearance
Abnormal vital signs
Pale complexion, red eyes
Disheveled appearance
Irritability or euphoria
Nervousness, compulsive behavior, picking of skin
Fast aging of patient and sagging of skin
Sweaty, clammy, skin

22 CDHA Journal Vol. 22, No. 2
groups.13 The dry mouth accompanying the use of this drug leads to many prob-lems. Without saliva, acids accumulate, lowering the pH of the mouth and causing the breakdown of the surface of the teeth. Xerostomia is caused by the vasoconstric-tion and reduction of salivary gland func-tion. The tongue and lining of the mouth can become raw and irritated without the surfactant action of saliva. This can lead to secondary infections, limited ability to speak and eat.10
Many patients try to reduce the xerosto-mia by consuming sugary sodas. The soda, coupled with decreased home care, vomiting side effects of the drug and decreased immune response, creates the perfect environment for the disease of caries to occur. Some chemicals used to manufacture MA are caustic, causing chemical burns on the skin. These harmful chemicals will also come into contact with the soft tissue or mucosal lining of the oral cavity. Without the buffering effects of saliva present to protect the oral tissues, severe inflamma-tion, painful mouth sores, and ulcers can develop.3,4,8
The pattern of decay is distinctive in that, initially, it involves the smooth buccal surface of posterior teeth and the inter-proximal of the anterior teeth. It eventually leads to the complete destruction of the coronal portion of the tooth. 1,3,13 MA users are chronic grinders and clench-ers due to the muscle constriction accom-panying MA use. Grinding quickly wears down the teeth to small nubs. Grinding and clenching were once attributed to the impurities of the processing in homemade laboratories, however there is no current clinical evidence to support this.12
The other result of the constriction of blood vessels is the gaunt look and quick aging of the patients. Tissues of the face quickly die and sag from the lack of nutrients and blood supply. 2, 3, 9 This aging effect can be seen in “before and after” photos and is irreparable. The intense itching that many MA user experience is also from
Table 6: Resources for Treatment of Addiction
samhsa.gov Substance Abuse & Mental Health Services Administration
dasis3.samhsa.gov Rehab locations.
MethResources.gov The federal government’s comprehensive directory of information and
programs related to methamphetamine. Justthinktwice.com Just think twice is a youth oriented site created by the Drug Enforce-
ment Agency’s Demand Reduction Program.
Whitehousedrugpolicy.gov Office of National Drug Control Policy- Detailed description of
methamphetamine and other resources.
www.usdoj.gov/dea/concern/meth The Drug Enforcement Administration – MA Information, statistics
and resources.
nationaldec.org The National Alliance for Drug Endangered Children . Resources for
safety of children in MA environment.
naco.org National Association of Counties - MA Action Clearinghouse is committed to raising public awareness about and helping counties respond to drug problems.
drugabuse.gov/MethAlert/MethAlert.html National institute on drug abuse has resources and information on
tends in use, prevention, identifying users and treatment options.
asam.org American society of Addictive Medicine Studies, facts and resources.
SayNOtoMeth.com Say no to meth is devoted to the education of children and youth to
the devastating results of MA use.
crystalrecovery.com This website seeks to support and promote the recovery of MA addicts;
and to provide information to teens, adults, parents, teachers, professionals, or anyone who may be affected by their own or someone else’s MA use.

CDHA Journal Vol. 22, No. 2 23
have been assessed there are many things the clinician can do to prevent further damage.
Resources for Rehabilitation
It’s important for the dental healthcare pro-vider to be equipped with resources to refer the patient to the proper healthcare profes-sional for treating drug addiction. Having a list of area resources will help in delivering care. Health departments and social service agencies can aid in gathering this information (Table 6).
Pain control
No patient should have to live with pain. The typical MA patient may not experience the pain you would expect from such extensive decay because MA can block or lessen pain recep-tors. Other patients will have such severe pain that it is difficult for them to eat. James Hill, DDS, with the California Correction system has developed a special understanding of the pain needs of MA patients through his work in the prison system. Dr. Hill stated, “The most important thing that I can do is help to restore people’s self image and self esteem. It is so important that I treat them as I would want to be treated. I would not want to be in pain and I should do everything that I can to help my patients get out of pain.” Dr. Hill explained he is seeing an increasing number of patients with the severe effects of MA use. He stated “it is very frustrating to watch someone go through the process of extensive pain and losing all their teeth but, having a patient turn their life around after receiving treatment makes it all worth while.”
Unless there are contraindications, anti-inflam-matory medications should be the first drug of choice for pain control. Prescribing narcotics should be avoided. Cardiac reactions have been reported when mixing narcotics with MA. Patients addicted to MA will use narcotics to increase the high. Pain control in the office should include use of a long lasting anesthetic, such as Marcaine, if the patient has not had MA in the last 24 hours.14 Local anesthetics should not be administered if there is doubt
the constricting capillaries near the surface of the skin. Compulsive scratching often leads to infection and bacterial cellulitis.6
Treatment considerations and planning
Being aware of the signs and symptoms of MA abuse is the first step of treatment (see Tables 4 and 5). Updating the health history, commu-nicating concerns, assessing the current use of MA and referring for rehabilitation must occur before treatment begins.
MA users have a higher tolerance to an-esthetics, a reduced ability to metabolize medications, and a greater chance of a drug interaction.14 Dentists and hygienists must communicate with the patient and discover when the last dose of MA occurred. No vaso-constrictors should be used within 24 hours of MA use. An increase in blood pressure from vasoconstrictors can lead to a stroke or cardiac arrest.15 Sharing these facts with the patient may help them to feel comfortable sharing their MA habits.
Using frank, direct questions that are non-judgmental will aid in a quick diagnosis. The health history can help in the screening process. Include questions such as “Do you have a history of drug dependency?” on the health history. Document all conversations on drug use and history in the patient’s chart. It’s important to include the patient’s report of the last date of use and the names of the any medications prescribed for the patient or drugs taken by the patient.
After initial examination, ask open ended questions such as “How did your teeth get to be this way? Normally, we don’t see this kind of decay and/or tooth damage very often. It usually happens if someone drinks excessive amounts of sugary soda or takes drugs. Have you used Methamphetamines or are you using now?” Point out the signs of damage that can be seen clinically. Express concern and use the opportunity to educate patients while discuss-ing their dental findings. Present the facts (non-jundgementally), explaining how impor-tant it is to stop now. Once the patient’s needs
con’t on page 24

24 CDHA Journal Vol. 22, No. 2
whether the patient has used MA in the past 24 hours. When using anesthetic, vasoconstrictors should be avoided as they can lead to increased blood pressure, stroke or cardiac arrest. Cau-tion should be used when using general anes-thesia and nitrous oxide as adverse reactions may occur when mixing drugs.
If it becomes necessary to prescribe narcotics, consider asking permission to discuss any prescription with the patient’s drug counselor, sponsor, or medical doctor. It’s important to include in this discussion the proper use of the medication, limits of use, and side effects. Some patients will use the excuse of pain related to the extensive decay to get prescrip-tions for painkillers, so caution should be used when prescribing drugs, especially if they are not patients of record. Patients may go “doctor shopping” from one dental office to another to obtain drugs. The Substance Abuse and Mental Health Services Administration (SAMHSA) reported that pre-scription drugs are the second most popular category of recreational drugs (just behind marijuana). Surveys of recovery groups in 2002 revealed that fifty-four percent of addicts reported obtaining narcotics by manipulat-ing their dentist. Keep prescription pads in a locked place to limit access by patients. Do not print Drug Enforcement Agency (DEA) number on the prescription pad.17
Xerostomia
The vasoconstriction of the salivary glands, along with the drying effects of the agents from which MA is made, leaves the oral mu-cosa severely dry. Upon examination, patients with xerostomia may complain of generalized mouth soreness, dry mouth, painful or burning tongue, taste changes, difficulty in chewing, and problems with talking and swallowing. Clinical presentation of xerostomia includes oral fissuring, ulceration, and epithelial atro-phy. Saliva substitutes and moisturizers can reduce some symptoms. Encourage patients to drink water rather than trying to quench their thirst with sodas, sports drinks, or fruit juices that contain sugar. Preventive fluoride treatments, both in-office and at home, are strongly recommended to strengthen and remineralize the damaged enamel rods. Rec-
ommend the use of xylitol products to reduce the development of caries, resist the fermenta-tion of bacteria, reduce plaque formation and increase salivary flow.18
Decay
Patients may report that their teeth decayed “from the inside out.” A possible explanation may be from reduced blood supply to the tooth. With repeated shrinking, the vessels won’t re-cover and, without nutrients to the tooth, it will die. Treating carious lesions with conventional means is of little value with a patient who is using MA. The disease will reoccur under the filling material. Sealing the area with fluoride and a xylitol releasing fluoride varnish and/or Glass Ionomer Sealant & Surface Protectant are treatment modalities that may be of benefit un-til the patient stops drug use. Dr. Hill reported using both acrylic and composite temporary crowns with great success. Intermediate re-storative material (IRM) aids in relieving pain and serves as a temporary solution. IRM is easy to use and its strength properties are close to those of zinc phosphate cement, with good sealing properties, low solubility and excellent abrasion resistance with grinding.
Mitchell Goodis, DDS, of El Dorado County, California, treats hundreds of MA patients a year. He has made it his mission to educate dental professionals, youth and “anyone who will listen”. His experience has shown that most MA users end up losing their teeth. He suggests “comfort care” until it is time for extractions and dentures. Periodontal Disease
MA users do not generally seek regular dental treatment so will often present with gingivitis or periodontitis from lack of professional oral care and inadequate home care. Patient educa-tion on plaque control, nutrition and the etiol-ogy of disease can help the patient maintain the area until they are ready for treatment. Nutrition issues need to be addressed to aid in tissue healing after treatment. Dr. Hill sug-

CDHA Journal Vol. 22, No. 2 25
Table 7: Working with Tweakers
1. Keep your distance - coming too close can be perceived as threatening.
2. No bright lights - the tweaker is paranoid and bright lights
may cause them to react violently.
3. Slow your speech, lower your voice.
4. Slow your movements - the tweaker is paranoid and may misunderstand your movements.
5. Keep your hands visible, or they may feel threatened and become violent.
6. Keep the tweaker talking - a tweaker who falls silent can be extremely dangerous. Silence often means that his paranoid thoughts have taken over reality, and anyone present can become part of the tweaker’s paranoid delusions. If you are threatened, call the police and tell them that this person may be under the influence of Meth or other drugs.(16)
con’t on page 26
gested the use of alcohol-free Chlorhexidine until treatment can take place.
Oral mucosa
Oral mucosa wounds, angular cheilitis, muco-sitis, or Candida albicans (oral thrush) are the results of a compromised immune response coupled with exposure to a dry, acidic en-vironment. Having the patient swish with a mixture of liquid Kaopeptate and Benedryl mixed fifty-fifty will aid in healing and give relief from pain. Evaluate the patient for the presence of candida albicans. If present, treat oral candidiasis by prescribing either Nystatin suspensions or clotrimazole troches, both of which are extremely effective treatments.19
Tweakers
People who abuse MA regularly are known as ‘tweakers’. All offices need to have a protocol for the Tweaker patient as they often behave or react violently (see Table 7). Keep in mind, the tweaker may not have slept in three to fifteen days and may be irritable and paranoid. If the
tweaker is also using alcohol or other drugs, the danger may be intensified.
The tweaker craves more MA, but no dosage will help recreate the first rush. This may cause frustration and lead to unpredictable behavior and violence. To support their habits, tweak-ers often participate in spur-of-the-moment crimes, such as purse snatching or burglar-ies. Tweakers are often involved in domestic disputes and automobile accidents. They may also be present at raves or parties. They may at first appear to be normal but a closer look will reveal eye movement ten times faster than normal, a voice with a slight quiver and jerky movements (Table 7).16
If abuse or neglect is occurring as a result of meth use, dental professionals are mandated to report to the proper authorities.

26 CDHA Journal Vol. 22, No. 2
A website worth viewinghttp://www.mitchtv.net/index.html
Why would one man make it his life mission to get the word out on the effects of one drug? Why would one man spend his time, money and every resource avail-able to try to change the lives of drug abusers? Mitchell Goodin, DDS is doing just that. He has used his own money to create a website aimed at ending the cycle of METH MOUTH. It was not enough for him to devote his practice to helping the oral devastation of the oral effects of MA; he has gone much further by developing a video, power points, lesson plans, and slide shows of before and after.
“I have to educate the public on the devastat-ing results of the use MA, how can I not after I have seen what it does to peoples oral health, self esteem and lives?”
He volunteers at high schools, for dental professional organizations, at churches and conferences to teach the public and professionals just what MA does to health, mouths, family and life. When Dr. Goodin was asked why he does this he humbly replied “There is no greater satisfaction than preventing the spread of this horrendous drug.” This man has served the un-derserved of El Dorado County for years and has been spreading the message “to anyone who will listen! If I can help prevent just one person having to experience the devastation of this disease my life will be worth while.”
About the AuthorNoel Brandon Kelsch is a freelance cartoonist, writ-er, speaker and Registered Dental Hygienist. Noel’s cartoons can be seen in RDH magazine and many other publications. Her articles have been published in den-tal and nursing trade maga-zines, well as in books from Love is the Best Medicine to Especially for Women.
Noel has received many national awards including Colgate Bright Smiles Bright Futures, RDH Magazine Sun Star Butler Award of Distinction, USA Magazine Make a Difference Day award, President’s Service Award, Foster Parent of the Year, and is a five time winner of the Castro-ville Artichoke cook-Off!
Noel is the current Vice President of California Dental Hygienists Association, a member of Organization for Safety and Asepsis Procedures and board member of Simi Valley Free Clinic.
Her hobbies include under water basket weaving, naval contemplation and water colors. Noel received her dental hygiene degree from Cabrillo College and is currently at-tending Northern Arizona University.
Conclusion
Methamphetamine abuse is increasing and it affects all aspect of a patient’s life and health. Oral diseases includ-ing rampant caries, periodontal disease, severe xerostomia are key signs of chronic MA abuse and frequently lead to edentulousness. Understanding the disease process, treatment strategies and drug abuse referral system can assure appropriate intervention. Knowing the patient’s drug habits, health status and the recommended treatment strategies will ensure proper intervention, patient education and prevention of disease progression. MA use is also increasingly affecting our communities and society. The loss of these individuals as contributing members to society, and the need for social agencies to cope with their actions or rehabilitation cost taxpayers untold millions yearly.
The affect on the MA users families is devastating. If the dental healthcare provider can play a role in helping these patients or their families through alleviating their dental pain or disease, or by contributing to their drug use cessa-tion, everyone in our society wins.
The dental hygienist plays a vital role in identifying or aiding these individuals when they present in our clinical setting. As stated previously, we’ve probably all treated an MA user in our office unknowingly at one time. It’s the author’s hope the dental hygienist reading this will now be more knowledgeable and in a better position to properly treat and/or refer these patients.

CDHA Journal Vol. 22, No. 2 27
References
1. Colfax, Grant N. MD. Methamphetamine-The Scope of the Problem, Medscape HIV/AIDS, 2005;11(2)
2. Timothy E Albertson, MD, PHD, et al. Methamphet-amine and the Expanding Complications of Amphet-amines, WJM, April, 1999-Vol. 170, no. 4, p. 214-219
3. Curtis, Eric K DDS, MAGD. Meth Mouth; Review of methamphetamine abuse and its oral manifestations, Oral Medicine, Oral Diagnosis, 2006, March-April, p. 125-129
4. Derlet, Robert W., Heischober, Bruce, MD. Meth-
amphetamine Stimulant of the 1990s?, WJM 1990, December, Vol. 153, no.6, p. 625-627
5. Daberkow, DP, Kesner RP, Keefe KA. Relationship between Methamphetamine-induced monoamine de-pletions in the striatum and sequential motor learn-ing, Pharmacol Bio Chem Behavior, 2005, May;81:1, p.198-204
6. Prah, OPH. Methamphtamines: Are Tougher anti-meth Laws needed? CQ Researcher, 2005: july, Vol 15, p.589-612
7. Boddiger, D. Methamphetamine linked to rising HIV transmission. Lancet 2005: Vol.365, p. 1217-1218
8. National Institute on Drug Abuse, InfoFacts: Meth-amphetamine (Rockville, MD: US Department of Health and Human Services), from the web at http://www.nida.nih.gov/infofacts/methamphetamine.html last accessed Nov, 9, 2006
9. Zweben, J., et al. Methamphetamine Treatment Proj-ect, Psychiatric symptoms Methamphetamine users. AM J Addict, 2005, vol. 13, p. 181-190
10. National Institute on Drug Abuse, InfoFacts: Meth-amphetamine (Rockville, MD: US Department of Health and Human Services), http://www.nida.nih.gov/infofacts/methamphetamine.html last accessed Nov, 9, 2006
11. Diago, Steven. When your patient is an addict. AGD Impact, Dec, 2003, vol. 33, no. 9
12. J.W. Shaner DMD. Meth Mouth and Rampant Caries in Meth Abusers, APC, Vol. 20, No.3 p.146-150
13. De Cugno, F., et. al. Salivary secretion and dental caries experience in drug addicts. Arch Oral Bio.1981, vol.26, p. 363-367
14. Murphy D. Wilmer, S. Patients who are substance abusers. NYDentJ, 2002, vol. 68, p 24-27
15. Eyalka, T. Rural America’s Epidemic Destroying patients teeth, Ill Dental News, 2005, Vol. 74, p.4-5
16. http://www.mappsd.org/Treatment.htm, Accessed 10/11/2006
17. http://www.samhsa.gov/ accessed 10/11/2006
18. Creanor SL, Strang R, Gilmour W, et al. The effect of chewing gum use on in-situ enamel lesion reminer-alization. J Dent Res 1992;71:1895-1900
19. Jose A. Vazquez, M.D. Options for the Management of Mucosal Candidiasis in Patients With AIDS and HIV Infection Pharmacotherapy 19(1):76-87, 1999. © 1999 Pharmacotherapy Publications
Personal interview with Dr. James Hill DDS 11/03/2006 conducted by Noel Kelsch RDH
Personal interview with Dr. Mitchell Goodis 11/6/2006 conducted by Noel Kelsch RDH
Need a treatment referral?Call 1-800-662-HELP or Visit findtreatment.samhsa.gov

28 CDHA Journal Vol. 22, No. 2
Home Study Course:
Meth Mouth & Dental Care Considerations
2 Continuing Education Units
Please PrintName _____________________________________________________________ License # ___________________________
Address ______________________________________________ City ___________________________ State ____ Zip_____
ADHA Membership ID# _________________________ Expiration _____________________________
Home Phone Number ___________________________________ Email ____________________________
Signature _______________________________________________________________________________
CE Credit available: Members - $20 Non-members - $35Forward the answer sheet below (photo copies accepted), and completed information with your check made payable to CDHA: Mail to CDHA Home Study Course, 505 N. Brand Blvd., #740, Glendale, CA 91203 • 818-500-8217
A confirmation and CE certificate will be mailed within 4–6 weeks.------------------------
ANSWER SHEET: Circle the correct answer for questions 1– 10
1. Methamphetamines are synthesized by converting ephedrine or psuedoephedrine through the process of:
A. Carbonization B. Distillation C. Oxygenation D. Anabolism
2. The chronically depressed _____________ level seen in patients who chronically use Methamphetamines can lead to symptoms like those of Parkinsons disease: A. Glucose C. Dopamine B. Thyroid D. Histamine
3. Short term affects of methamphetamines do not include: A. Vomiting B. Hyperactivity C. Narcolepsy D. Decreased appetite
4. Methamphetamines cause blood vessels to: A. Expand C. Constrict B. Exfoliate D. Capsulate
5. The first drug of choice for dental pain control with metamphetamine users is: A. Nonsteroidal Anti-inflammatories B. Narcotics/Opiods C. Cannabis D. Nothing, they do not experience pain
6. The pattern of tooth destruction in the mouth of methamphetamine users includes:
A. Smooth buccal surfaces of posterior teeth B. The interproximal of anterior teeth C. The grinding down of occussal surfaces D. All of the above
7. The first step in providing dental treatment for a methamphetamine user is:
A. Ask if they used MA today. B. Use more anesthesia because they will have a high tolerance to it. C. Be aware of the signs and symptoms of use. D. Refer the patient, as the clinician can do nothing for them.
8. The signs of a patient actively using methamphetamine are so obvious you will always be able to tell. A. True B. False
9. Patients should not receive any vasoconstrictors within __________ of methamphetamine use:
A. 10 days C. 72 hours B. 24 hours D. All of the above
10. The clinician should do the following when treating “tweakers:” A. Keep your hands out of sight. B. Make sure you have bright lighting. C. Get close to them so you can see if they are listening. D. Slow your speech and keep the tweaker talking.

CDHA Journal Vol. 22, No. 2 29
Dentsply Professional

Rosie Tesselaar, Executive AdministratorCalifornia Dental Hygienists’ Association505 N. Brand Blvd., #740Glendale, CA 91203
CDHA2006
RETURN SERVICE REQUESTED
California Dental Hygienists’ Association2005 – 2006 Executive Officers
President Susan McLearan, RDHAP, MS
President Elect Jean Honny, RDH, BS
Vice President Education & Membership Lori Gagliardi, RDH, BS, MEd
Vice President Administration & Public Relations Noel Kelsch, RDH
Secretary-Treasurer Diana Thomson, RDH
Immediate Past President Lin Sarfaraz, RDH, AS
Speaker of the House Colleen Beasley, RDH
ADHA District XI Trustee Sharon Zastrow, RDH
Presorted STDU.S. Postage
PAIDPermit No. 104San Dimas, CA
Component TrusteesCentral Coast Maureen Titus, RDHAP, BS San Fernando Valley Denise Litwin, RDHEast Bay Teresa Irby, RDH San Francisco Susan Lopez, RDH, BSKern County Sarah Monson, RDH San Gabriel Valley Beverly Legg, RDHLong Beach Roz Mattson, RDH, BA San Joaquin Valley Cindy Andrews, RDHLos Angeles Adrienne Martasin, RDH Santa Barbara Daphne Von Essen, RDHMonterey Bay Mary Jo Cardinale, RDH Santa Clara Valley Susan Treleaven, RDH, BSMt. Diablo Patty Martin, RDH Six Rivers Darla Dale, RDHAPNapa-Solano Marsha Amster, RDH Shasta County Mary Jacobson, RDH, BSOrange County Helen McCracken, RDH South Bay Charmaine Young, RDH Peninsula Nicole Scoles, RDH Tri County Mary Ann Huffman, RDH, BSRedwood Karen Olson, RDH Valley Oaks Arlene Vianello, RDHSacramento Valley Gail Griffin, RDH Ventura County Elvira Cabelli, RDH San Diego County Diana Corley, RDH, BS
MASTER CALENDAR
February 23-25 Administration Council, Budget Committee & Executive Committee meeting Glendale
March 24 Board of Trustees meeting Glendale Hilton, Glendale
May 4 Spring Scientific Session Anaheim
June 8-10 CDHA Annual Session Costa Mesa












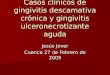








![Gingivitis Descamativa[1]](https://img.pdfslide.net/doc/110x75/55793005d8b42ad6678b4774/gingivitis-descamativa1.jpg)






