Embed Size (px)
Citation preview

Journal of Neuroimmunology xxx (2014) xxx–xxx
JNI-475986; No of Pages 7
Contents lists available at ScienceDirect
Journal of Neuroimmunology
j ourna l homepage: www.e lsev ie r .com/ locate / jneuro im
Intravenous immunoglobulin G improves neurobehavioral andhistological outcomes after traumatic brain injury in mice
Seongtae Jeong a,b, Beilei Lei a,c, Haichen Wang a,d, Hana N. Dawson a,d, Michael L. James a,c,d,⁎a Multidisciplinary Neuroprotection Laboratories, Duke University, Durham, NC, United Statesb Department of Anesthesiology and Pain Medicine, Chonnam National University Medical School, Gwangju, South Koreac Department of Anesthesiology, Duke University, Durham, NC, United Statesd Department of Neurology, Duke University, Durham, NC, United States
⁎ Corresponding author at: DUMC3094, Durham,NC 27943 7898.
E-mail address: [email protected] (M.L. James)
http://dx.doi.org/10.1016/j.jneuroim.2014.08.6260165-5728/© 2014 Elsevier B.V. All rights reserved.
Please cite this article as: Jeong, S., et al., Intbrain injury in mice, J. Neuroimmunol. (201
a b s t r a c t
a r t i c l e i n f oArticle history:Received 21 March 2014Received in revised form 25 August 2014Accepted 27 August 2014Available online xxxx
Keywords:Traumatic brain injury (TBI)Intravenous immunoglobulin (IVIG)NeuroinflammationBlood–brain barrier (BBB)Murine modelLong-term outcome
Intravenous immunoglobulin (IVIG)may improve neuroinflammation after traumatic brain injury (TBI). IVIG ad-ministration after TBI improved rotarod latencies over thefirst 7 days (p= 0.039) andwatermaze latencies over29–32 days (p = 0.027), decreased F4/80-positive cells at 2 (p = 0.001) and 7 days (p b 0.001), decreasedFluoro-Jade B-positive cells (p = 0.020), increased NeuN-positive cells (p = 0.014), decreased IL-6 productionat 4 (p = 0.032) and 24 h (p = 0.023), and decreased blood–brain barrier breakdown by IgG extravasation(p= 0.001) and brain edema (p= 0.006); however, TNF-α concentration was unchanged. IVIG administrationwas associated with long-term neurobehavioral and histological improvement through modulation of neuroin-flammation and blood–brain barrier permeability in a murine TBI model.
© 2014 Elsevier B.V. All rights reserved.
1. Introduction
Traumatic brain injury (TBI) is a major health problem around theworld with high mortality and morbidity (Hardman and Manoukian,2002). Therapies that improve outcome have not yet been developed;thus, treatment remains supportive (Felker et al., 2010). Brain damageafter TBI initially results from mechanical injury; however, secondaryinjury occurs hours or days after impact and induces further damage.The mechanisms of secondary injury are complex and not fully under-stood but include excitotoxicity, oxidative stress, and neuroinflammation(Loane and Faden, 2010).
Neuroinflammation is triggered by various stimuli, and is character-ized by glial activation, increased proinflammatory cytokine production,activation of the complement system, and upregulation of adhesionmol-ecules (Morganti-Kossmann et al., 2001; Schmidt et al., 2005). Theseneuroinflammatory responses can induce blood–brain barrier (BBB)breakdownand increase cerebral edema formation, resulting in increasedintracranial pressure. These factors then contribute to hypoxic braindamage, hemorrhage, and neuronal cell death (McIntosh et al., 1996).
Intravenous immunoglobulin (IVIG) is a polyspecific immunoglobulinG (IgG) preparation obtained from pooled human plasma that is used tomanage autoimmune and inflammatory diseases (Misra et al., 2005). In
710, United States. Tel.:+1 919
.
ravenous immunoglobulin G4), http://dx.doi.org/10.1016/
addition, IVIG is effective in treating neurological diseases associatedwith acute and chronic inflammation, such as Guillain–Barre syndrome,multi-focal neuropathy, and chronic inflammatory demyelinating poly-neuropathy (Hughes et al., 2009; van der Meche and Schmitz, 1992).Further, IVIG treatment has been shown to modulate inflammatoryreactions, providing beneficial effects in preclinical models of stroke(Arumugam et al., 2007) and multiple sclerosis, (Dudesek and Zettl,2006) as well as in Alzheimer's disease in humans(Relkin et al.,2009).
Though the exact mechanism is unclear, IVIG appears to modulateseveral components of neuroinflammation. Since neuroinflammationplays a central role in secondary injury after TBI, IVIG may affect brainpathology in this setting as well. In the present study, we tested thehypothesis that IVIG improves functional and histological outcomes byinhibiting microglial activation and BBB permeability in a murine modelof TBI.
2. Materials and methods
2.1. Animal preparation
Animal handling and experimental procedures were approved byDuke University Institutional Animal Care andUse Committee, Durham,North Carolina. Male 10- to 11-week-old C57BL/6J mice (Jackson Labo-ratory, Bar Harbor, ME) were used in all experiments. Animals wereacclimatized to the laboratory environment for more than 1 week
improves neurobehavioral and histological outcomes after traumaticj.jneuroim.2014.08.626

2 S. Jeong et al. / Journal of Neuroimmunology xxx (2014) xxx–xxx
prior to injury. During this period, animals were housedwith free accessto a standard diet and tap water in a room under a 12/12-hour light/darkcycle.
2.2. TBI model
Themouse TBI model (Lynch et al., 2005) was adapted from a previ-ously described model of closed cranial trauma for the rat (Foda andMarmarou, 1994). After anesthesia induction under 4.6% isoflurane,the trachea was intubated with 20-gauge intravenous catheter(Becton-Dickinson, Sandy, UT), and the lungs were mechanically venti-latedwith 1.6% isoflurane in 30%O2 and 70%N2. Rectal temperaturewasmaintained at 37 °C ± 0.2 °C. After midline incision of the scalp, a con-cave 3-mm metal disc was adhered to the skull immediately caudal tothe bregma. A 2.0-mm diameter pneumatic impactor (Air-Power, Inc.,High Point, NC) was used to deliver a single midline impact to the discsurface. The impactor was discharged at 6.8 ± 0.2 m/s with a headdisplacement of 3mm. After injury, the animals were allowed to recoverspontaneous ventilation, and the trachea was extubated. Followingrecovery, mice were allowed free access to food and water.
2.3. Drug dosing and delivery
IVIG (Gammagard Liquid®)was provided by Baxter US (Deerfield, IL).Gammagard is composed of IgG (N98%) and trace amount of immuno-globulin A andM. Prior to injury,micewere randomized to one of 3 treat-ment groups for neurobehavioral testing: 300 mg/kg IVIG, 600 mg/kgIVIG, and vehicle (saline). For all other experiments, mice were random-ized to receive either 600 mg/kg IVIG or vehicle (saline). These dosageswere chosen based on clinical dosage for autoimmune diseases. Drug orvehicle was administered via tail vein injection in a volume of 6 mL/kgsaline by a blinded observer. Tail vein injection was performed within30 min after TBI.
2.4. Neurobehavioral testing
An automated Rotarod (RR; Ugo Basile, Comerio, Italy) was used byanoperator blinded to treatment assignment to assess the effects of IVIGadministration on vestibulomotor function (Hamm et al., 1994). RRtesting was performed beginning in the morning over the first 7 daysafter injury (n = 18–420 mice/group). On the day before injury, themice underwent training trials at a set rotational speed (16 rpm) for60 s, followed by accelerating rotational speed (4–40 rpm) for 300 s.Three additional trials with an accelerating rotational speed were per-formed. The average time to fall from the rotating cylinder in the latter3 trials was recorded as baseline latency. After injury, mice underwentconsecutive daily testing with 3 trials of accelerating rotational speedand a minimum inter-trial interval of 15 min. Average latency to fallfrom the rod was recorded. Mice unable to stand on the rotating rodwere given a latency of 0 s.
2.5. Morris Water Maze (MWM) testing
In the same cohort ofmice used in RR testing, an examiner blinded totreatment assignment used the MWM task to assess the effects of IVIGadministration on spatial learning and memory. MWM was performedin the morning over days 29–32 after injury, since motor deficits arenot seen at 28 days after injury in this model. MWMwas evaluated in ablack aluminum pool (105 cm in diameter, 60 cm deep) filled withwater opacified with powdered milk and containing a platform (7.5 cmin diameter) submerged 1 cm below the water surface (25–27 °C). Themaze was kept in a room dedicated to behavioral testing to decreasestress. Mice were tested for 4 consecutive days with 4 trials per day andan inter-trial interval of 1 h. For each trial, mice were placed in 1 of 4different quadrants. Mice were allowed to search for the platform for90 s. If unable to locate the platform, mice were guided to the platform
Please cite this article as: Jeong, S., et al., Intravenous immunoglobulin Gbrain injury in mice, J. Neuroimmunol. (2014), http://dx.doi.org/10.1016/
where they remained for 15 s. A computerized video tracking system(KeilSoft LLC, Chapel Hill, NC) recorded latency from entering the mazeto finding the platform and swimming speed. On the final day, afterhidden platform testing, a probe trial was conducted, which consistedof removing the escape platform and releasing themouse at a point diag-onally opposite the previous location of the platform. The time spentsearching all 4 quadrants and the number of crossings into the platformquadrant was recorded.
2.6. Immunohistochemistry
Fluoro-Jade B (FJB; a marker for neuron degeneration), F4/80 (amicroglial/macrophage marker), and anti-neuronal-specific nuclearprotein (NeuN; a neuronal marker) were used for immunohistochemicalstaining by an examiner blinded to treatment assignment on 1, 7 and33 days after injury, respectively. Timepoints were chosen to captureearly neuronal degeneration, subacute microglial activation/macrophagerecruitment, and long-term neuronal survival, respectively, based onmodel experience (Indraswari et al., 2012; James et al., 2010, 2012;Laskowitz et al., 2007; Lynch et al., 2005; Wang et al., 2007, 2013). Sepa-rate cohorts of mice were used for FJB (n = 8/group) and F4/80 staining(n = 6/group); NeuN staining occurred in the same cohort as MWM(n = 6/group). Additionally, IgG staining to investigate BBB integrityand F4/80 staining were done at 48 h after TBI using a separate cohortof mice (n = 6/group).
After transcardial perfusion, brains were immediately dissected andremoved, immersion fixed in 10% formaldehyde for 24 h, transferredinto phosphate-buffered saline, and stored at 4 °C. For immunostaining,the brains were immersed in 30% sucrose buffer for at least 24 h, andthen sagittal sections (40 μm) were cut on a freezing microtome.Every eighth section was selected for immunohistochemistry. Tissuewas incubated in 1% H2O2 for 5 min, permeabilized by 0.1% Saponinfor 1 h, and blockedwith 10% goat serum for at least 30min. Primary an-tibodywas applied overnight at 4 °C. The next day, tissuewas incubatedat room temperature for 1 h, and then incubated in secondary antibody(biotinylated IgG antibody, 1:3000; Vector Laboratories, Inc., Burlin-game, CA) for 2 h, followed by avidin–biotin–peroxidase complex treat-ment for 1 h (ABC kit; Vector Laboratories, Inc., Burlingame, CA).Between treatments, tissue was washed 3 times for 5 min withTris-buffered saline. Staining was visualized with diaminobenzidine(DAB; Vector Laboratories, Inc.). The sections were mounted ontocharged slides and allowed to dry overnight. Slides were incubated inHematoxylin stain (Fisher Scientific, Fair Lawn, NJ) for 4min. After dehy-dration, the sections were cover-slipped using DPX mounting media(Fluka, Milwaukee, WI). For immunohistochemistry, the following anti-bodies were used: NeuN antibody (mouse monoclonal, 1:90,000;Chemicon, Temecula, CA) and anti-mouse F4/80 antibody (rat monoclo-nal, 1:10,000; Serotec, Raleigh, NC). For IgG immunostaining, biotinylatedgoat anti-mouse IgG (1:100; Vector Labs, Burlingame, CA)was usedwith-out primary antibody. FJB staining was performed using previouslydescribed protocols (Dawson et al., 2007).
2.7. Cell quantification and image analysis
Before counting, all slides were coded to avoid experimenter bias.Stereological analysis was performed by an examiner blinded totreatment assignment on a Nikon 218912 light microscope (NikonInstruments, Melville, NY) interfaced with the StereoInvestigatorsoftware package (MicroBrightField,Williston, VT). The number of pos-itive cells per volume in the dentate gyrus of the dorsal hippocampuswas estimated using the optical fractionalmethod by a blinded observer(West et al., 1991). IgG immunohistochemistrywas analyzed usingMCIDElite 7.0 (Imaging Research Inc., St. Catharines, Canada) for proportionalarea.
improves neurobehavioral and histological outcomes after traumaticj.jneuroim.2014.08.626

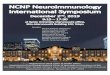
Fig. 1. Intravenous immunoglobulin (IVIG) treatment improves neurobehavioral outcomesafter traumatic brain injury (TBI). (A) Vestibularmotor function assessed by Rotarod latencyduring the first 7 days after TBI was significantly improved in mice treated with 600 mg/kgIVIG (n=20) compared to vehicle group (n=20). Therewasno significant difference in thegroup treatedwith 300 mg/kg IVIG (n=18). Sham animals are not presented for RR data asthey demonstrate latencies consistently greater than 280 s. (B) At 29–32 days after TBI, theMorrisWaterMaze (MWM) showed significant functional improvement in the group treat-ed with 600 mg/kg IVIG compared to vehicle, despite similar swim speeds. *p b 0.05 vs.vehicle group by repeatedmeasured ANOVA. All values are expressed asmeans± standarderror of mean (SEM).
3S. Jeong et al. / Journal of Neuroimmunology xxx (2014) xxx–xxx
2.8. Brain water content
Mice were anesthetized and euthanized by 4.6% isoflurane at 48 hafter injury (n = 7/group). This timepoint was chosen to fall withinthe period of peak edema based on model experience (Indraswariet al., 2012; James et al., 2010, 2012; Laskowitz et al., 2007; Lynchet al., 2005; Wang et al., 2007, 2013). Brains were excised and, after re-moving the cerebellum and brainstem, were weighed immediately(“wet”weight) by an examiner blinded to treatment assignment. Brainswere allowed to dehydrate over 24 h at 100 °C, and then reweighed(“dry” weight). Cerebral edema was expressed as water content calcu-lated as a percentage of wet weight ([wet weight − dry weight / wetweight] × 100).
2.9. Enzyme-linked Immunosorbent Assay (ELISA)
Mice (n = 6/group) were anesthetized with 1.6% isoflurane afterendotracheal intubation, and perfused transcardially with 30 mLphosphate-buffered saline for 5min. Brainswere excised andflash frozenin liquid nitrogen, and then stored at −80 °C. Pulverized whole brainswere sonicated on ice in homogenization buffer (20 mM Tris–HCl,pH 8.0, 137 mM NaCl, 2 mM EDTA, 10% glycerol, 1% Triton X-100, andcomplete protease cocktail tablets; Roche Diagnostics, Germany) for20 s. Brain homogenates were incubated on ice for 20 min and thencentrifuged (14,000 ×g) for 10 min at 4 °C. The supernatants werequantified for protein concentrations using bicinchoninic assay (PierceThermoFisher Scientific, Rockford, IL) and stored at−20 °C until analy-sis. The concentrations of tumor necrosis factor-alpha (TNF-α) andinterleukin-6 (IL-6)weremeasured by an examiner blinded to treatmentassignment at 4 h and 24 h after injury, using Quantikine ELISA kits (R&DSystems;Minneapolis, MN) according to themanufacturer's instructions.These timepoints were chosen to capture early microglial/macrophageactivation and fall within the period of peak edema based on modelexperience(Indraswari et al., 2012; James et al., 2010, 2012; Laskowitzet al., 2007; Lynch et al., 2005; Wang et al., 2007, 2013).
2.10. Statistical analysis
RR and MWM latencies were compared with repeated-measuresanalysis of variance (ANOVA) with time as the repeated variable.Pairwise testing was performed between groups, using Scheffe's F testpost hoc method to correct for multiple comparisons. Brain water con-tent, the numbers of NeuN- and F4/80-positive cells, cytokine concentra-tion, and IgG-stained area were analyzed by 2-tailed Student t-test. FJBstain was compared using nonparametric Mann–Whitney test. A prioriand post hoc exclusion criteria were limited to surgical complicationsand failure of drug/vehicle delivery or thermoregulation. Based onknown variance within this model, (Indraswari et al., 2012; James et al.,2010, 2012; Laskowitz et al., 2007; Lynch et al., 2005; Wang et al., 2007,2013) sample size of 15–19 mice per group was calculated to demon-strate a 30% treatment effect in MWM latencies over days 29–32 afterinjury for a 3-group repeatedmeasures ANOVA. A p value b 0.05was con-sidered statistically significant. All values are expressed asmeans± stan-dard deviation. Statistical analysis was performed using SPSS 16.0 (IBM,Armonk, NY).
3. Results
3.1. Neurobehavioral outcomes after TBI were improved in IVIG-treated mice
Seven animals died during the study (3 in vehicle, 1 in 300 mg/kgIVIG, 1 in 600 mg/kg IVIG, and 2 mice immediately after injury beforedrug administration) and were not included in the analyses. All otherinjured animals were used in the final statistical analyses. Mice treatedwith 600 mg/kg IVIG showed significantly improved RR performanceover the first 7 days (Fig. 1A; P = 0.039) and MWM performance over
Please cite this article as: Jeong, S., et al., Intravenous immunoglobulin Gbrain injury in mice, J. Neuroimmunol. (2014), http://dx.doi.org/10.1016/
days 29–32 (Fig. 1B; P = 0.027) after injury compared to vehicle-treated mice, despite similar swim speeds (300 mg/kg v. 600 mg/kg v.vehicle: 24.3 ± 4.7 v. 24.2 ± 4.7 v. 23.5 ± 4.2; p N 0.05). However,neither RR nor MWM performances were improved in mice treatedwith 300 mg/kg IVIG compared to vehicle-treated animals. Since neuro-behavioral improvement was found only in mice receiving 600 mg/kgof IVIG, this dosage was carried forward in all further experiments.
3.2. Neuronal degeneration and microgliosis after TBI were reduced inIVIG mice
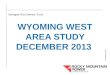
To assess whether improved neurobehavioral outcomes were asso-ciated with histological changes, immunohistochemisty was performedon separate cohorts of mice treated with 600 mg/kg IVIG or vehicle. Toevaluate acute neuronal injury, FJB stainingwas performed at 24 h afterinjury (Fig. 2A & B). There were significantly fewer FJB-positive cells inthe dentate gyrus of the dorsal hippocampus in the IVIG-treated group
improves neurobehavioral and histological outcomes after traumaticj.jneuroim.2014.08.626

Fig. 2. Intravenous immunoglobulin (IVIG) treatment decreases neuronal injury andmicrogliosis after traumatic brain injury (TBI). Fluoro-Jade B staining showed degenerating neurons inthe granular layer of dentate gyrus of thedorsal hippocampus in vehicle- (A) and IVIG-treated (B) animals at 24 h after TBI. F4/80 staining of thedentate gyrus of thedorsal hippocampus invehicle- (C) and IVIG-treated (D) animals at 7 days after TBI. All photomicrographs obtained at 20× magnification.
4 S. Jeong et al. / Journal of Neuroimmunology xxx (2014) xxx–xxx
(IVIG vs. vehicle: 9.2 ± 12.7 vs. 27.4 ± 18.4 cells/mm3, p = 0.020;Fig. 3A). To assess delayed neuronal injury, NeuN stainingwas performedat 33 days after injury (Fig. 2C & D). There was a significant increase inneuronal density in the dentate gyrus of the dorsal hippocampus inIVIG-treated mice (IVIG vs. vehicle: 50,403 ± 9384 vs. 37,990 ± 4144neurons/mm3, p = 0.014; Fig. 3B); however, there was no difference inneuronal density in the polymorphic region of the dorsal hippocampus(data not shown). At 48 h after injury, the number of F4/80-positivecells in the dentate gyrus of the dorsal hippocampus was significant-ly lower in IVIG-treated group (IVIG vs. vehicle: 5025 ± 2312 vs.10,774 ± 1699 cells/mm3, p = 0.001; Fig. 3C). Though the number ofF4/80-positive cells slightly increased in both group at 7 day after injury,the IVIG-treated group showed significant reduction in these cells com-pared to the vehicle-treated group (IVIG vs. vehicle: 6750 ± 905 vs.11,647 ± 1478 cells/mm3, p b 0.001; Figs. 2E & F. 3D).
3.3. BBB integrity was improved and cerebral edema was decreased inIVIG mice
To evaluate BBB disruption and cerebral edema, IgG immunohisto-chemistry and brain water content measurements were performed at48 h after injury in mice treated with 600 mg/kg IVIG or vehicle. As pre-viously described, (Indraswari et al., 2012) TBI induced marked BBB per-meability; however, the area of IgG extravasation was significantlydecreased in the IVIG-treated group (IVIG vs. vehicle: 10.9 ± 7.6% vs.40.6 ± 11.3%, p= 0.001; Fig. 4A–C). There was a significant decrease incerebral edema as quantified by brain water content in the IVIG-treatedgroup (IVIG vs. vehicle: 78.29 ± 0.18% vs. 78.83 ± 0.30%, p = 0.006;Fig. 4D).
3.4. IL-6 was reduced in IVIG mice, but not TNF-α production
Neuroinflammatory responses may exacerbate BBB breakdown,cerebral edema, and secondary brain injury. To determine possibleeffects of IVIG on early neuroinflammation, IL-6 and TNF-α wholebrain concentrations were measured at 4 and 24 h after injury in mice
Please cite this article as: Jeong, S., et al., Intravenous immunoglobulin Gbrain injury in mice, J. Neuroimmunol. (2014), http://dx.doi.org/10.1016/
treated with 600 mg/kg IVIG or vehicle. IVIG treatment was associatedwith significantly lower IL-6 concentration compared to vehicle at 4 h(6.02 ± 1.81 vs. 10.79 ± 4.48 pg/mg protein, p = 0.032) and at 24 h(3.06±1.69 vs. 5.74±2.13 pg/mgprotein p= 0.023; Fig. 5A). However,there was no difference in TNF-α concentrations at either time point(Fig. 5B).
4. Discussion
In the present study, IVIG administration improved long-termneurobehavioral and histological outcomes in a murine model of TBI.These improvements were accompanied by a reduction in microglialactivation/macrophage recruitment, proinflammatory cytokine produc-tion, BBB permeability, and brain edema formation.
Microglia are activated immediately after TBI, with continued activa-tion over several months (Engel et al., 2000). While microglia are re-quired for removal of cellular debris after brain injury, profound andsustained activation can lead to increased production of proinflammatorycytokines, such as IL-6 and TNF-α, and subsequent neuronal cell injuryand activation of apoptotic pathways (Lu et al., 2001; Mannix andWhalen, 2012). Moreover, inflammatory responses associated withmicroglial activation alter BBB permeability and, consequently, increasecerebral edema formation. Not surprisingly then, inhibition of microglialactivation has been demonstrated to be a promising therapeutic strategyfor patients with TBI (James et al., 2010).
While the primary injury in this model results in a cortical contusionunder the impact site, intervention aimed at modifying the contusion isdifficult to translate due to time constraints in applying the therapy afterinjury. However, diffuse injury occurs throughout the brain at the timeof impact and evolves over the first few days after injury (Lynch et al.,2005). These secondary injury mechanisms, such as neuroinflamma-tion, result in damage to the hippocampus, among other areas and arepotentially amenable to intervention.
As previously demonstrated, (Indraswari et al., 2012) traumaticinjury induced marked BBB disruption in this model. This was signif-icantly improved in IVIG-treated mice, as evidenced by decreased
improves neurobehavioral and histological outcomes after traumaticj.jneuroim.2014.08.626

Fig. 3.Unbiased stereology evaluation of neuronal injury andmicroglial activationwith intravenous immunoglobulin (IVIG) treatment after traumatic brain injury (TBI). (A) Fluoro-JadeB-positive neurons in the dentate gyrus of the dorsal hippocampus were significantly lower in the IVIG-treated group compared to the vehicle-treated group by nonparametricMann–Whitney U test (n= 8/group). (B) Neuronal-specific nuclear protein (NeuN) staining in the dentate gyrus of the dorsal hippocampus at 33 days after TBI showed increased neu-ronal density in the IVIG-treated group compared to the vehicle-treated group (n = 6/group). F4/80 staining in the dentate gyrus of the dorsal hippocampus at 48 h (C) and 7 days(D) after TBI showed significantly decreased numbers of F4/80 positive cell in the IVIG-treated group compared to the vehicle-treated group (n = 6/group). *p b 0.05 and **p b 0.01vs. vehicle group by Student t-test. All values are expressed as means ± standard deviation.
Fig. 4. Intravenous immunoglobulin (IVIG) treatment decreases blood–brain barrier breakdown and brain edema formation after traumatic brain injury (TBI). (A–C) Immunoglobulin G (IgG)staining showed that the area of IgG extravasation was significantly decreased in the IVIG-treated group (B) compared to the vehicle-treated group (A) at 2 days after TBI (n = 6/group).(D) There was a significant decrease in brain water content in the IVIG-treated group compared to the vehicle-treated group at 2 days after TBI (n = 7/group). **p b 0.01 vs. vehicle groupby Student t-test. All values are expressed as means ± standard deviation.
5S. Jeong et al. / Journal of Neuroimmunology xxx (2014) xxx–xxx
Please cite this article as: Jeong, S., et al., Intravenous immunoglobulin G improves neurobehavioral and histological outcomes after traumaticbrain injury in mice, J. Neuroimmunol. (2014), http://dx.doi.org/10.1016/j.jneuroim.2014.08.626

Fig. 5. Intravenous immunoglobulin (IVIG) treatment decreases interleukin-6 (IL-6), butnot tumor necrosis factor-alpha (TNF-α), expression after traumatic brain injury (TBI).(A) IVIG administration was associated with a significant decrease in IL-6 production byEnzyme-linked Immunosorbent Assay (ELISA) compared to vehicle treatment at 4 h and24 h after TBI (n= 6/group). (B) No difference in TNF-α concentration. *p b 0.05 vs. vehiclegroup by Student t-test. All values are expressed as means ± standard deviation.
6 S. Jeong et al. / Journal of Neuroimmunology xxx (2014) xxx–xxx
IgG extravasation. Reduction in BBB permeability was associatedwith significantly decreased cerebral edema, which occurred in thesetting of neurobehavioral improvement. BBB integrity can be alteredby numerous stimuli in a wide range of neurological diseases. In fact,inflammatory mediators and cytokines may be associated with BBBdisruption related to neuroinflammation, (Banks and Erickson, 2010;Petty and Lo, 2002) including TNF-α (Ahishali et al., 2005; Ramiloet al., 1990). Indeed, a recent study showed that TNF-α antagonism de-creases cerebral edema formation with concomitant improvement inneurological outcome in a murine model of intracerebral hemorrhage(Lei et al., 2013).
However, in the present study, there was no difference in TNF-αconcentration at both 4 and 24 h after injury, whereas IVIG treatmentsignificantly reduced IL-6 production. These results were somewhatunexpected, as previous investigations showed upregulation of bothTNF-α and IL-6 mRNA after injury at these timepoints (James et al.,2010;Wang et al., 2007). A fewpossibilitiesmay explain this discrepancy.First, treatment administration may delay these responses; future re-search should fully define this time course. Second, themethod of mea-surement in the present study may be different. In previous studies,TNF-α and IL-6 mRNA were measured by PCR instead of protein con-centration. Second, the closed head injury model may be different. Inearlier studies, cytokine concentration was measured in an intracere-bral hemorrhagemodel. In fact, other studies using a closed-head injurymodel have found no change in TNF-α concentration after injury (Byeet al., 2007; Semple et al., 2010). However, when IL-6 production wasmarkedly increased after injury, a decrease in IL-6 was associated withattenuation of the neuroinflammatory response (Bye et al., 2007;Gatson et al., 2013). In addition,when the effect of IVIGonBBBpermeabil-ity was evaluated in an experimental sepsis model, marked BBB disrup-tion occurred without increase in brain TNF-α, and IVIG administrationsignificantly decreased BBB breakdown with no change in TNF-α (Esenet al., 2012).
While IL-6 is awell-known acute phase reactant, limited data supporta direct relationship between IL-6 and BBB permeability in murine TBImodels. Thus, it is difficult to confirmwhether decreased IL-6was associ-ated with decreased BBB permeability and brain edema formation. Asmentioned above, because microgliosis can induce BBB permeability viaseveral different pathways, (Lu et al., 2001; Mannix and Whalen, 2012)inhibition of microglial activation through IVIG administration could re-duce BBB permeability and subsequent brain edema formation; however,the exact mechanism remains unclear.
Please cite this article as: Jeong, S., et al., Intravenous immunoglobulin Gbrain injury in mice, J. Neuroimmunol. (2014), http://dx.doi.org/10.1016/
While the exactmechanism(s) after TBI are unclear, IVIG is a knowninhibitor of IgG constant fragment (Fc) receptor,which results inmultipleeffects including blocking immune complex cell surface signaling, modu-lation of dendritic cells, etc (Nimmerjahn and Ravetch, 2007) Further,IVIG modulates leukocyte recruitment into the brain (Lapointe et al.,2004) and inhibits complement. (Aschermann et al., 2010). Particularlyexciting is the prospect of IVIG-induced neurogenesis, supported by find-ing increased neuronal density at 33 days after injury. To distinguish thispossibility from reduced apoptosis, further mechanistic work will beneeded. Finally, since the BBB becomes increasingly disrupted acutelyafter impact, IVIG is likely able to act both centrally and systemicallyafter TBI.
One limitation of the present study is that Gammagard Liquid® con-tains glycine (1.8%, 240–300 mosmol/kg) as a stabilizing and bufferingagent. Gammagard Liquid®was dilutedwith normal saline, and normalsaline was used as the vehicle, with no glycine present. Glycine is an in-hibitory neurotransmitter especially in the spinal cord. However, thereare no reports that intravenous administration of glycine affects behav-ioral and neurologic outcomes. Further, 1.5%–2.2% glycine has beensafely administered in prior studies (Hahn et al., 1989; Stalberg et al.,1993).
In conclusion, the current study demonstrated intravenous injectionof IVIG after injury improves neurobehavioral and histological outcomesin amurinemodel of TBI. These results suggest that IVIGmayhave poten-tial as a promising therapeutic for translation into human clinical trials. Inaddition to validating the present results and outlining necessaryparameters for translation (e.g., dosing time course, etc.), future researchshould assess the timecourse of immunohistochemical outcomes anddefine exact mechanism(s) of action.
Disclosure statement
Seongtae — No conflicts of interest.Lei — No conflicts of interest.Wang — No conflicts of interest.Dawson — No conflicts of interest.James — No conflicts of interest.
Acknowledgments
This studywas funded by a grant from Baxter Biotherapeutics (MLJ).IVIG (Gammagard Liquid®) was provided by Baxter US (Deerfield, IL).The authors would like to acknowledge Kathy Gage for her generous as-sistance with medical editing.
References
Ahishali, B., Kaya, M., Kalayci, R., Uzun, H., Bilgic, B., Arican, N., et al., 2005. Effects of lipo-polysaccharide on the blood–brain barrier permeability in prolonged nitric oxideblockade-induced hypertensive rats. Int. J. Neurosci. 115, 151–168.
Arumugam, T.V., Tang, S.C., Lathia, J.D., Cheng, A., Mughal, M.R., Chigurupati, S., et al.,2007. Intravenous immunoglobulin (IVIG) protects the brain against experimentalstroke by preventing complement-mediated neuronal cell death. Proc. Natl. Acad.Sci. U. S. A. 104, 14104–14109.
Aschermann, S., Lux, A., Baerenwaldt, A., Biburger, M., Nimmerjahn, F., 2010. The otherside of immunoglobulin G: suppressor of inflammation. Clin. Exp. Immunol. 160,161–167.
Banks, W.A., Erickson, M.A., 2010. The blood–brain barrier and immune function and dys-function. Neurobiol. Dis. 37, 26–32.
Bye, N., Habgood, M.D., Callaway, J.K., Malakooti, N., Potter, A., Kossmann, T., et al., 2007.Transient neuroprotection byminocycline following traumatic brain injury is associatedwith attenuated microglial activation but no changes in cell apoptosis or neutrophil in-filtration. Exp. Neurol. 204, 220–233.
Dawson, H.N., Cantillana, V., Chen, L., Vitek, M.P., 2007. The tau N279K exon 10 splicingmutation recapitulates frontotemporal dementia and parkinsonism linked to chro-mosome 17 tauopathy in a mouse model. J. Neurosci. 27, 9155–9168.
Dudesek, A., Zettl, U.K., 2006. Intravenous immunoglobulins as therapeutic option in thetreatment of multiple sclerosis. J. Neurol. 253 (Suppl. 5), V50–V58.
Engel, S., Schluesener, H., Mittelbronn, M., Seid, K., Adjodah, D., Wehner, H.D., et al., 2000.Dynamics ofmicroglial activation after human traumatic brain injury are revealed by de-layed expression of macrophage-related proteins MRP8 and MRP14. Acta Neuropathol.100, 313–322.
improves neurobehavioral and histological outcomes after traumaticj.jneuroim.2014.08.626

7S. Jeong et al. / Journal of Neuroimmunology xxx (2014) xxx–xxx
Esen, F., Senturk, E., Ozcan, P.E., Ahishali, B., Arican, N., Orhan, N., et al., 2012. Intravenousimmunoglobulins prevent the breakdown of the blood–brain barrier in experimentallyinduced sepsis. Crit. Care Med. 40, 1214–1220.
Felker, G.M., Pang, P.S., Adams, K.F., Cleland, J.G., Cotter, G., Dickstein, K., et al., 2010. Clinicaltrials of pharmacological therapies in acute heart failure syndromes: lessons learnedand directions forward. Circ. Heart Fail. 3, 314–325.
Foda, M.A., Marmarou, A., 1994. A new model of diffuse brain injury in rats. Part II: mor-phological characterization. J. Neurosurg. 80, 301–313.
Gatson, J.W., Liu, M.M., Abdelfattah, K., Wigginton, J.G., Smith, S., Wolf, S., et al., 2013.Resveratrol decreases inflammation in the brain of mice with mild traumatic braininjury. J. Trauma acute care Surg. 74, 470–474 (discussion 4–5).
Hahn, R.G., Stalberg, H.P., Gustafsson, S.A., 1989. Intravenous infusion of irrigatingfluids containing glycine or mannitol with and without ethanol. J. Urol. 142,1102–1105.
Hamm, R.J., Pike, B.R., O'Dell, D.M., Lyeth, B.G., Jenkins, L.W., 1994. The rotarod test: anevaluation of its effectiveness in assessing motor deficits following traumatic braininjury. J. Neurotrauma 11, 187–196.
Hardman, J.M., Manoukian, A., 2002. Pathology of head trauma. Neuroimaging Clin. N. Am.12, 175–187 (vii).
Hughes, R.A., Dalakas, M.C., Cornblath, D.R., Latov, N., Weksler, M.E., Relkin, N., 2009. Clinicalapplications of intravenous immunoglobulins in neurology. Clin. Exp. Immunol. 158(Suppl. 1), 34–42.
Indraswari, F., Wang, H., Lei, B., James, M.L., Kernagis, D., Warner, D.S., et al., 2012. Statinsimprove outcome in murine models of intracranial hemorrhage and traumatic braininjury: a translational approach. J. Neurotrauma 29, 1388–1400.
James, M.L., Wang, H., Venkatraman, T., Song, P., Lascola, C.D., Laskowitz, D.T., 2010. Brainnatriuretic peptide improves long-term functional recovery after acute CNS injury inmice. J. Neurotrauma 27, 217–228.
James, M.L., Wang, H., Cantillana, V., Lei, B., Kernagis, D.N., Dawson, H.N., et al., 2012. TT-301inhibitsmicroglial activation and improves outcome after central nervous system injuryin adult mice. Anesthesiology 116, 1299–1311.
Lapointe, B.M., Herx, L.M., Gill, V., Metz, L.M., Kubes, P., 2004. IVIg therapy in brain inflamma-tion: etiology-dependent differential effects on leucocyte recruitment. Brain 127,2649–2656.
Laskowitz, D.T., McKenna, S.E., Song, P., Wang, H., Durham, L., Yeung, N., et al., 2007.COG1410, a novel apolipoprotein E-based peptide, improves functional recovery ina murine model of traumatic brain injury. J. Neurotrauma 24, 1093–1107.
Lei, B., Dawson, H.N., Roulhac-Wilson, B., Wang, H., Laskowitz, D.T., James, M.L., 2013.Tumor necrosis factor alpha antagonism improves neurological recovery in murineintracerebral hemorrhage. J. Neuroinflammation 10, 103.
Loane, D.J., Faden, A.I., 2010. Neuroprotection for traumatic brain injury: translationalchallenges and emerging therapeutic strategies. Trends Pharmacol. Sci. 31, 596–604.
Lu, J., Moochhala, S., Kaur, C., Ling, E.A., 2001. Cellular inflammatory response associatedwithbreakdown of the blood–brain barrier after closed head injury in rats. J. Neurotrauma18, 399–408.
Please cite this article as: Jeong, S., et al., Intravenous immunoglobulin Gbrain injury in mice, J. Neuroimmunol. (2014), http://dx.doi.org/10.1016/
Lynch, J.R., Wang, H., Mace, B., Leinenweber, S., Warner, D.S., Bennett, E.R., et al., 2005. Anovel therapeutic derived from apolipoprotein E reduces brain inflammation andimproves outcome after closed head injury. Exp. Neurol. 192, 109–116.
Mannix, R.C., Whalen, M.J., 2012. Traumatic brain injury, microglia, and beta amyloid. Int.J. Alzheimers Dis. 2012, 608732.
McIntosh, T.K., Smith, D.H., Meaney, D.F., Kotapka, M.J., Gennarelli, T.A., Graham, D.I., 1996.Neuropathological sequelae of traumatic brain injury: relationship to neurochemicaland biomechanical mechanisms. Lab. Investig. 74, 315–342.
Misra, N., Bayry, J., Ephrem, A., Dasgupta, S., Delignat, S., Duong Van Huyen, J.P., et al.,2005. Intravenous immunoglobulin in neurological disorders: a mechanistic perspec-tive. J. Neurol. 252 (Suppl. 1), I1–I6.
Morganti-Kossmann, M.C., Rancan, M., Otto, V.I., Stahel, P.F., Kossmann, T., 2001. Role ofcerebral inflammation after traumatic brain injury: a revisited concept. Shock 16,165–177.
Nimmerjahn, F., Ravetch, J.V., 2007. The antiinflammatory activity of IgG: the intravenousIgG paradox. J. Exp. Med. 204, 11–15.
Petty, M.A., Lo, E.H., 2002. Junctional complexes of the blood–brain barrier: permeabilitychanges in neuroinflammation. Prog. Neurobiol. 68, 311–323.
Ramilo, O., Saez-Llorens, X., Mertsola, J., Jafari, H., Olsen, K.D., Hansen, E.J., et al., 1990.Tumor necrosis factor alpha/cachectin and interleukin 1 beta initiate meningealinflammation. J. Exp. Med. 172, 497–507.
Relkin, N.R., Szabo, P., Adamiak, B., Burgut, T., Monthe, C., Lent, R.W., et al., 2009. 18-Monthstudy of intravenous immunoglobulin for treatment of mild Alzheimer disease.Neurobiol. Aging 30, 1728–1736.
Schmidt, O.I., Heyde, C.E., Ertel, W., Stahel, P.F., 2005. Closed head injury—an inflammatorydisease? Brain Res. Brain Res. Rev. 48, 388–399.
Semple, B.D., Bye, N., Rancan, M., Ziebell, J.M., Morganti-Kossmann, M.C., 2010. Role ofCCL2 (MCP-1) in traumatic brain injury (TBI): evidence from severe TBI patientsand CCL2−/− mice. J. Cereb. Blood Flow Metab. 30, 769–782.
Stalberg, H.P., Hahn, R.G., Hjelmqvist, H., Ullman, J., Rundgren, M., 1993. Haemodynamicsand fluid balance after intravenous infusion of 1.5% glycine in sheep. Acta Anaesthesiol.Scand. 37, 281–287.
van der Meche, F.G., Schmitz, P.I., 1992. A randomized trial comparing intravenous immuneglobulin and plasma exchange in Guillain–Barre syndrome. Dutch Guillain–Barre StudyGroup. N. Engl. J. Med. 326, 1123–1129.
Wang, H., Lynch, J.R., Song, P., Yang, H.J., Yates, R.B., Mace, B., et al., 2007. Simvastatin andatorvastatin improve behavioral outcome, reduce hippocampal degeneration, and im-prove cerebral blood flow after experimental traumatic brain injury. Exp. Neurol. 206,59–69.
Wang, B., Dawson, H., Wang, H., Kernagis, D., Kolls, B.J., Yao, L., et al., 2013. Lacosamide im-proves outcome in a murine model of traumatic brain injury. Neurocrit. Care. 19,125–134.
West, M.J., Slomianka, L., Gundersen, H.J., 1991. Unbiased stereological estimation of thetotal number of neurons in the subdivisions of the rat hippocampus using the opticalfractionator. Anat. Rec. 231, 482–497.
improves neurobehavioral and histological outcomes after traumaticj.jneuroim.2014.08.626