Embed Size (px)
Citation preview

Journal of Molecular Medicine
Volume 85, Number 12 / December, 2007 , pp. 1291-1435
What is life? On Erwin Schrödinger, his cat, and the Journal of Molecular Medicine DOI 10.1007/s00109-007-0288-9 Author Detlev Ganten
1291-1292
Hypoxia and human disease—and the Journal of Molecular Medicine DOI 10.1007/s00109-007-0285-z Author G. L. Semenza
1293-1294
Hypoxia and gastrointestinal disease DOI 10.1007/s00109-007-0277-z Authors Cormac T. Taylor and Sean P. Colgan
1295-1300
Hypoxia and cancer DOI 10.1007/s00109-007-0281-3 Authors M. Christiane Brahimi-Horn, Johanna Chiche and Jacques Pouysségur
1301-1307
Keeping the engine primed: HIF factors as key regulators of cardiac metabolism and angiogenesis during ischemia DOI 10.1007/s00109-007-0279-x Authors Ralph V. Shohet and Joseph A. Garcia
1309-1315
Hypoxia and chronic lung disease DOI 10.1007/s00109-007-0280-4 Author Rubin M. Tuder, Jeong H. Yun, Anil Bhunia and Iwona Fijalkowska
1317-1324
Hypoxia and the HIF system in kidney disease DOI 10.1007/s00109-007-0278-y Authors Masaomi Nangaku and Kai-Uwe Eckardt
1325-1330

Harnessing hypoxic adaptation to prevent, treat, and repair stroke DOI 10.1007/s00109-007-0283-1 Authors Rajiv R. Ratan, Ambreena Siddiq, Natalya Smirnova, Ksenia Karpisheva, Renee Haskew-Layton, Stephen McConoughey, Brett Langley, Alvaro Estevez, Patricio T. Huerta, Bruce Volpe, Sashwati Roy, Chandan K. Sen, Irina Gazaryan, Sunghee Cho, Matthew Fink and Joseph LaManna
1331-1338
Hypoxia inducible factor (HIF) function in innate immunity and infection DOI 10.1007/s00109-007-0282-2 Authors Annelies S. Zinkernagel, Randall S. Johnson and Victor Nizet
1339-1346
The “brain–skin connection”: nerve growth factor-dependent pathways for stress-induced skin disorders DOI 10.1007/s00109-007-0270-6 Authors Emmanouil Zoumakis, Sophia N. Kalantaridou and George P. Chrousos
1347-1349
IDO expression in the brain: a double-edged sword DOI 10.1007/s00109-007-0229-7 Authors Erik Kwidzinski and Ingo Bechmann
1351-1359
Primary immune surveillance: some like it hot DOI 10.1007/s00109-007-0245-7 Authors Joseph J. Skitzki, Qing Chen, W. C. Wang and Sharon S. Evans
1361-1367
Neuronal plasticity of the “brain–skin connection”: stress-triggered up-regulation of neuropeptides in dorsal root ganglia and skin via nerve growth factor-dependent pathways DOI 10.1007/s00109-007-0236-8 Authors Ricarda A. Joachim, Arne Kuhlmei, Q. Thai Dinh, Bori Handjiski, Tanja Fischer, Eva M. J. Peters, Burghard F. Klapp, Ralf Paus and Petra C. Arck
1369-1378
Cannabinoid CB1 receptor stimulation affords neuroprotection in MPTP-induced neurotoxicity by attenuating S100B up-regulation in vitro DOI 10.1007/s00109-007-0233-y Authors Teresa Iuvone, Giuseppe Esposito, Daniele De Filippis, Tiziana Bisogno, Stefania Petrosino, Caterina Scuderi, Vincenzo Di Marzo, Luca Steardo and Endocannabinoid Research Group
1379-1392
Effects of transcription factor activator protein-1 on interleukin-8 expression and enteritis in response to Clostridium difficile toxin A DOI 10.1007/s00109-007-0237-7 Authors Jin Young Lee, Hye Ri Park, Yu-Kyoung Oh, Yeong-Jeon Kim, Jeehee Youn, Joong-Soo Han and Jung Mogg Kim
1393-1404

Modulation of muscle contraction by a cell-permeable peptide DOI 10.1007/s00109-007-0238-6 Authors Gisela Tünnemann, Peter Karczewski, Hannelore Haase, M. Cristina Cardoso and Ingo Morano
1405-1412
Accumulation of dietary glycotoxins in the reproductive system of normal female rats DOI 10.1007/s00109-007-0246-6 Authors Evanthia Diamanti-Kandarakis, Christina Piperi, Penelope Korkolopoulou, Eleni Kandaraki, Georgia Levidou, Apostolos Papalois, Efstratios Patsouris and Athanasios G. Papavassiliou
1413-1420
Celastrol inhibits polyglutamine aggregation and toxicity though induction of the heat shock response DOI 10.1007/s00109-007-0251-9 Authors Yu-Qian Zhang and Kevin D. Sarge
1421-1428
Immunoadsorption and subsequent immunoglobulin substitution decreases myocardial gene expression of desmin in dilated cardiomyopathy DOI 10.1007/s00109-007-0263-5 Authors Angela Kallwellis-Opara, Alexander Staudt, Christiane Trimpert, Michel Noutsias, Uwe Kühl, Matthias Pauschinger, Heinz-Peter Schultheiss, Markus Grube, Michael Böhm, Gert Baumann, Uwe Völker, Heyo K. Kroemer and Stephan B. Felix
1429-1435

EDITORIAL
What is life? On Erwin Schrödinger, his cat,and the Journal of Molecular Medicine
Detlev Ganten
Published online: 22 November 2007# Springer-Verlag 2007
What is Life? was the title of a little pamphlet that ErwinSchrödinger, a theoretical physicist, published over 60 yearsago [1]. In my generation, every serious student of biologyand medicine read, and was deeply influenced by, What IsLife? James Watson claims that What is life? brought himto pursue and to answer this fundamental question.Schrödinger based his material on a seminal paper byNikolai Timoféeff-Ressovsky, Karl Zimmer, and MaxDelbrück published in 1935 in Berlin [2]. The three haddrawn conclusions from the observation that Drosophilaflies, when irradiated, exhibit an increased mutation ratethat is linearly related to the number of particles adminis-tered in terms of total radiation dose, rather than on theintensity. There exists an analogy to Einstein’s conclusionthat the photoelectric effect depends on the frequency of thelight source rather than on its intensity. The three authorsconcluded that genes had a definable, albeit unknown,chemical structure and a specific locus on the chromosome,and they calculated about how large a gene might be.Schrödinger wondered how many molecules it takes to makea living being, what these molecules might possess asproperties, and whether viruses are living, dead, or neither–nor. What provoked Schrödinger to even ask these questions?
We gain insight into his mind by revisiting the famousSchrödinger cat. Schrödinger wrestled in Berlin in the1920s with quantum mechanics, a discipline that necessar-ily deals with the duality of a material (if I may call light amaterial) that exists as both a wave and a particle. Thisnotion was termed “complimentarity” by those who
suffered with it. Werner Heisenberg, with close supportfrom Niels Bohr, had published his matrix mechanics,which showed that the position of a particle (say, anelectron) could never be determined with certainty even ifits impulse is known. On the other hand, when theelectron’s position is known, its impulse cannot bedetermined. Does biology also feature complimentarity?
Schrödinger approached the quantum mechanics mysteryfrom the wave aspect. He derived an elucidating equationthat predicts about where electrons might be when theyorbit the atom. Schrödinger’s approach does not contradictthat of Heisenberg’s; as a matter of fact, the two notionssupport one another. Schrödinger brooded over quantummechanics. He attempted to reconcile the scurrilous worldof the quanta with the macroscopic tangible world byconstructing the cat paradox; a typical thought experiment(“Gedankenexperiment”) like Einstein’s studies. Imagine asingle atom of a radioactive element that has a half-life of60 min. The single atom, along with a Geiger counter, acrude mechanical hammer, a flask of cyanide gas, and aliving cat, are all housed within a box. The question is, after60 min, is the cat alive or dead? Here, we have a quantum-sized component discharging quanta, a device that cancount the quanta, and a machine that converts these quantainto a mechanical action that can kill the cat. Can wecalculate whether or not the cat is alive in 1 h? Well, everyschool child can tell us that the cat’s chances are 50–50.However, this estimate is imprecise (uncertain). The half-life was determined by observing billions of atoms. Ourprediction of a single atom’s behavior is uncertain. We canapply Schrödinger’s equation along with notation from PaulDirac and calculate how alive or dead the cat will be.However, the result is absurd: the cat is either dead or alive.These notions were the thought content that brought ErwinSchrödinger to biology.
J Mol Med (2007) 85:1291–1292DOI 10.1007/s00109-007-0288-9
D. Ganten (*)Charité-Universitätsmedizin Berlin,Charitéplatz 1,10117 Berlin, Germanye-mail: [email protected]

I am happy to announce that, contrary to Schrödinger’scat, the fate of the Journal of Molecular Medicine (J MolMed) is not only predictable but also certain. J Mol Med,published by Springer International, builds on the greattradition of its predecessor, the prestigious German journalfor clinical medicine, the Berliner Klinische Wochenschrift,which was founded in 1864. Nobel laureates such as RobertKoch, Emil v. Behring, Paul Ehrlich, and many other greatscientists have published their seminal papers in our parentjournal. The successor, Klinische Wochenschrift, was themost important forum for the publication of articles inclinical medicine and it was one of the few journals inwhich basic science and patient-oriented clinical researchwere published. J Mol Med – from its inception as BerlinerKlinische Wochenschrift – will continue this tradition [3].
Many of J Mol Med’s readers, authors, and reviewerswill have noted the recent developments concerning thejournal. The impact point factor has increased steadily(currently 5.157) in each of the past 5 years. We haveestablished a new workflow process that involves theAssociate Editors more actively in manuscript handling.As a result, we can report more rapid handling of manu-scripts both by the editorial office and in production. Mostof all you are aware of the excellent papers the journal hasbeen publishing recently. This state of affairs documents thefact that the journal is becoming more attractive to an ever-increasing readership.
The Journal already has a distinct editorial niche, and wewill focus on the molecular basis of human disease and itstreatment, particularly the genetics of disease and suscepti-bility to disease. We aim to address some of the keyquestions in molecular medicine, such as: What phenotypescan a disease gene cause? How does a genotype lead to adisease phenotype? How can disease phenotypes be definedin a genetically meaningful way? The possibilities have beenincreased exponentially through the discovery of micro-RNAs and their regulatory potential. MicroRNAs and theireffects on protein construction bring us to “proteomics,”which will concern us to increasing degrees in the nearfuture. Nonetheless, we welcome theoretical contributionsand would surely have considered Schrödinger’s cat, had hesubmitted his reflections to us.
A largely new editorial team will be guiding the journalon this next stage in its journey. Frank McCormick andKazua Nakao have lent their time and intellect to J MolMed, and we thank them warmly for their contribution. It isthe Journal’s good fortune to have enlisted new editors ofthe same outstanding caliber. We are very pleased toannounce the appointment of Gregg L. Semenza, M.D.,Ph.D., as the new US Co-Editor-in-Chief, as of January,2008. Dr. Gregg Semenza is Director of the Program inVascular Cell Engineering at Johns Hopkins University
Medical School and is a world-renowned oncologist. Asyou will see, he is already making his mark on the journalby organizing and editing this special issue on hypoxia.
We are also fortunate to have a team of internationallyrecognized scientists serving as Associate Editors. Throughtheir individual expertise we cover the broad spectrum ofmolecular medicine. One important role of the AssociateEditors is handling manuscripts. This activity includes as-sessing manuscript quality, selecting and inviting reviewers,and then making a recommendation to the Editors-in-Chief. Currently, Dr. Cornelia Weyand covers immunology,Dr. Victor Nizet handles infectious diseases, Dr. Kai-UweEckardt handles nephrology, Drs. Jun Liu and WalterRosenthal provide expertise in pharmacology, Dr. ValinaDawson covers neurosciences, Drs. Jörg T. Epplen andStylianos Antonarakis are our experts for hereditary dis-eases, and Drs. Stefan-Martin Brand-Herrmann and HaraldSchmidt handle cardiovascular sciences and their genetics.Dr. Giovanni Melillo is an expert in oncology and cancertherapeutics, and Drs. Chi V. Dang and W. Michael Kornwill continue their support in the area of oncology. Dr.Friedrich Luft is our resident editorialist–physician punditwho picks a paper for each issue to pontificate upon. Hemaintains impartiality by not participating in article selection.The staff is fine and the managing editor, Dr. Christiane Nolte,is in efficient control of all manuscripts and keeps processingtime short and authors happy. The quality of a journal,however, depends on a committed and active reviewer team.You, the readers, form the reviewers upon which we depend.Reviewers are the decisive element of any successful journal;no journal can be better than its reviewers are.
Our activity flourishes in the wake of visionaries likeSchrödinger, Delbrück, Watson, and many others, includingyou, the readership. What about Schrödinger and his cat?He was a most gentle person who could not hurt a flea,even if residing on a cat. I do not believe that Schrödingerfelt that his cat was in jeopardy. After all, cats do have ninelives don’t they—or was it nine half-lives?
Yours,
Detlev Ganten
References
1. Schrödinger E (1948) What is life? The physical aspect of theliving cell. Cambridge University Press, Cambridge
2. Timoféeff-Ressovsky NW, Zimmer KG, Delbrück M (1935) Überdie Natur der Genmutation und der Genstruktur. In: Nachr. Ges.Wiss. Göttingen NF, (1):189–245
3. Ganten D (1995) The Journal of Molecular Medicine; tradition,continuity, and renaissance. J Mol Med 73:1–3
1292 J Mol Med (2007) 85:1291–1292

EDITORIAL
Hypoxia and human disease—and the Journalof Molecular Medicine
G. L. Semenza
Received: 29 October 2007 /Accepted: 29 October 2007 / Published online: 20 November 2007# Springer-Verlag 2007
This special issue of the Journal of Molecular Medicine isfocused on the role of hypoxia in the pathogenesis ofhuman disease. Oxygen homeostasis is a critical organizingprinciple of metazoan evolution, development, and phys-iology. The seven invited reviews in this issue highlight therapid progress that is being made in delineating themolecular mechanisms that result in disruption of oxygenhomeostasis in different disease states, the extent to whichthis disruption contributes to disease pathogenesis, and theprospects for novel therapies that target pathways involvedin adaptive (or maladaptive) responses to hypoxia. In theirreview, entitled “Hypoxia and Gastrointestinal Disease,”Cormac Taylor and Sean Colgan summarize the results ofpublished studies analyzing hypoxia-induced gene expres-sion in intestinal epithelial cells and the role of hypoxia inthe pathogenesis of inflammatory bowel disease. In“Hypoxia and Cancer,” Christiane Brahimi-Horn, JohannaChiche, and Jacques Pouyssegur discuss the causes andconsequences of intratumoral hypoxia. Joseph Garciadiscusses ischemic heart disease with a specific focus onalterations in cardiac metabolism that promote the survivalof ischemic cells. In “Hypoxia and Chronic Lung Disease,”Rubin Tuder and colleagues review the role of hypoxia inrespiratory distress syndrome, high altitude pulmonaryedema, pulmonary arterial hypertension, and chronicobstructive pulmonary disease. It is remarkable that despitereceiving oxygen from the bronchial circulation anddirectly from the alveolar air sacs, hypoxia can developwithin the lungs (even at sea level) and contribute to
pathogenic tissue remodeling. Masaomi Nangaku andKai-Uwe Eckardt discuss the role of the kidney in oxygenhomeostasis, particularly in the production of erythropoie-tin, which is the glycoprotein hormone that controls redblood cell production. They also summarize recent dataindicating that chronic hypoxia in the tubulointerstitiumrepresents a final common pathway to end-stage kidneydisease. Rajiv Ratan and his colleagues discuss novelstrategies for promoting hypoxic adaptation in neurons asa means to prevent or treat brain injury after stroke. Thesestrategies are based on recent advances in our understand-ing of the molecular physiology of oxygen sensing.Annelies Zinkernagel, Randall Johnson, and Victor Nizetreview data indicating that the same transcriptional regula-tory system that promotes adaptive responses to hypoxia,which are described in the other six papers in this issue, isalso required for neutrophil inflammatory and innateimmune functions. They also review data indicating thatobligate intracellular bacteria and oncogenic viruses mod-ulate hypoxia response pathways in host cells.
Hypoxia-inducible factor 1 (HIF-1) is a transcriptionfactor that plays an important role in cellular and systemicresponses to reduced oxygen availability in all metazoanspecies. Purification of HIF-1 from human cells revealedthat it is heterodimer composed of HIF-1α and HIF-1βsubunits, which dimerize and bind to DNA containing thecore sequence 5′-(A/G)CGTG-3′. Database searches forproteins that were homologous to HIF-1α led to theidentification of HIF-2α, which can also dimerize withHIF-1β and bind to an overlapping but distinct set of targetgenes. HIF-1α and HIF-2α are each negatively regulatedby O2-dependent hydroxylation of key proline and aspar-agine residues that dramatically reduce protein half-life andtranscriptional activity, respectively, under aerobic condi-tions. Although I admit my bias in focusing on the role of
J Mol Med (2007) 85:1293–1294DOI 10.1007/s00109-007-0285-z
G. L. Semenza (*)Vascular Program, Institute for Cell Engineering,The Johns Hopkins University School of Medicine,Broadway Research Building, Suite 671, 733 North Broadway,Baltimore, MD 21205, USAe-mail: [email protected]

HIF-1 in disease pathogenesis, the seven outstanding papersin this issue provide abundant evidence that this line ofinvestigation is leading to greater insight into the patho-genesis of gastrointestinal, neoplastic, cardiac, pulmonary,renal, cerebral, and infectious diseases. As discussed inseveral of the reviews in this issue, novel strategies thatincrease HIF-1 activity, either by gene therapy or bypharmacologic inhibition of hydroxylase activity, mayprovide therapeutic benefit in patients with heart, inflam-matory bowel, and kidney diseases, whereas inhibitors ofHIF-1 may be useful as anti-cancer agents.
This special issue of the Journal of Molecular Medicinewas designed with two goals in mind. First, we sought tohighlight one of the most dynamic areas of contemporarybiomedical research and to illustrate the extent to whichdisruption of oxygen homeostasis represents a key elementin the pathogenesis of the common causes of mortality inthe industrialized world. Indeed, this issue has seven papersby virtue of editorial, not scientific, limitations, and wecould easily have covered twice as many areas ofbiomedical research. Similarly, the role of pathways otherthan those involving HIF-1 and its hydroxylases could fillanother issue. The role in hypoxia in other human diseasesand other signaling pathways will be covered in futureissues of the journal. This issue could not have beenproduced without the generous assistance of expertreviewers who were willing to provide helpful comments
on very short deadlines, and we would like to thank ValinaDawson, Serpil Erzurum, Amato Giaccia, Mark Gillespie,Volker Haase, Jan-Steffen Juergensen, Victor Nizet, NanduriPrabhakar, and Mikhail Sitkovsky for their efforts.
The second major purpose for producing this special issuewas to encourage investigators studying the role of hypoxiain human disease to view the Journal of Molecular Medicineas a preferred vehicle for dissemination of scientificadvances in this exciting area of biomedical research. Iam grateful to Detlev Ganten for the opportunity to workwith him as Editor in Chief of the Journal of MolecularMedicine and for his enthusiastic support of this new focuson oxygen-related pathobiology. To support this new focus,our illustrious team of Associate Editors has been expandedby the addition of Stylianos Antonarakis (Genetics), ValinaDawson (Neuroscience), Jun Liu (Pharmacology and SignalTransduction), Giovanni Melillo (Oncology), Victor Nizet(Immunology and Infectious Disease), and Harald Schmidt(Cardiovascular Pharmacology). With the help of all of ourAssociate Editors around the world, along with ManagingEditor Christiane Nolte and the Editorial Office staff inBerlin, the Journal of Molecular Medicine will strive toprovide rapid, objective, and constructive critiques of allsubmitted manuscripts through the online ManuscriptCentral submission system, which can be accessed athttp://mc.manuscriptcentral.com/jmm. For now, take a deepbreath and dive into this exciting issue.
1294 J Mol Med (2007) 85:1293–1294

REVIEW
Hypoxia and gastrointestinal disease
Cormac T. Taylor & Sean P. Colgan
Received: 27 September 2007 /Revised: 17 October 2007 /Accepted: 22 October 2007 / Published online: 20 November 2007# Springer-Verlag 2007
Abstract The gastrointestinal mucosa is a richly perfusedvascular bed directly juxtaposed with the anaerobic andnonsterile lumen of the gut. As such, intestinal epithelialcells, which line the mucosa, experience a uniquely steepphysiologic oxygen gradient in comparison with other cellsof the body. Inflammation associated with a loss ofepithelial barrier function and unregulated exposure of themucosal immune system to luminal antigens leads toinflammatory bowel disease (IBD), a relatively commondisorder with severe morbidity and a limited therapeuticrepertoire. During IBD, increased tissue metabolism andvasculitis renders the chronically inflamed mucosa andparticularly the epithelium hypoxic, giving rise to theactivation of the hypoxia-responsive transcription factorhypoxia-inducible factor (HIF). Recent studies utilizingconditional intestinal epithelial hif1a-null mice haverevealed a protective role for epithelial HIF-1α in murinemodels of IBD. Such protection occurs, at least in part,through HIF-dependent induction of barrier-protectivegenes in the epithelium. More recently, studies employingpharmacologic activation of HIF via inhibition of HIFprolyl hydroxylases revealed a profoundly protective effect
of these agents in murine models of colitis. In this paper,we review this pathway in detail and examine thetherapeutic potential for targeting HIF hydroxylases inintestinal mucosal inflammatory disease.
Keywords Hypoxia . Inflammation . Gastroenterology
Tissue oxygenation in the gastrointestinal tract
The primary functions of the gastrointestinal tract are theprocessing and absorption of ingested nutrients, wasteremoval, fluid homeostasis, and the development of oraltolerance to nonpathogenic luminal antigens. The last ofthese functions involves the intestinal mucosa being uniqueamong tissues as it is in a constant state of controlledinflammation [1]. This occurs as the mucosal immunesystem is constantly exposed to new food-borne material inthe lumen, which is processed to avoid inappropriateinflammatory reactions to harmless ingested antigens [1].
As well as experiencing this sustained low-grade(physiologic) inflammation, the gut has a unique steady-state tissue oxygenation profile. Firstly, in the physiologicstate, the intestinal mucosa experiences multiple dailydynamic fluctuating rates of perfusion. When fasting, arelatively low blood volume is present in the gut; however,after the ingestion of a meal, perfusion rises significantly,resulting in large daily pO2 fluctuations. Secondly, becauseof its juxtaposition with the anoxic lumen of the gut, thegastrointestinal mucosa has a uniquely steep oxygengradient from the richly vascularized subepithelial mucosato the virtually anoxic luminal aspect of the epithelium(Fig. 1). Because of the impressive range of pO2 values thatthe intestinal mucosa is exposed to on a daily basis, it is
J Mol Med (2007) 85:1295–1300DOI 10.1007/s00109-007-0277-z
C. T. Taylor (*)UCD Conway Institute, School of Medicine and Medical Science,College of Life Sciences, University College Dublin,Belfield,Dublin 4, Irelande-mail: [email protected]
S. P. ColganMucosal Inflammation Program, Division of Gastroenterology,University of Colorado Health Sciences Center,Denver, CO, USA

perhaps not surprising that resident cells have evolved to bequite resiliant to altered levels of oxygenation.
A critical cell type in the maintenance of intestinalhomeostasis is the epithelial cell. The intestinal epitheliumis a monolayer of cells that covers an area of approximately250–300 m2 in an adult human and forms a critical barrierbetween the external (luminal) and internal (vascular)compartments. This dynamic barrier is maintained primar-ily by the existence of regulated intercellular tight junc-tions. As well as being a critical barrier, the epithelium isresponsible for the absorption of approximately 9 l of fluidfrom consumed liquids and secreted digestive fluids perday. This fluid transport function is carried out throughcoordinated ion transport events and the subsequentregulation of salt and water transport between the lumenof the gut and the bloodstream. Importantly, both the barrierand absorptive functions of the intestinal epithelium can bephysiologically regulated by oxygen [2–4].
Hypoxia and mucosal inflammation
Inflammatory bowel disease (IBD) is an umbrella term for arange of disorders including ulcerative colitis and Crohn’sdisease, which are characterized by a breakdown in theintestinal epithelial barrier with subsequent unregulatedexposure of the mucosal immune system to luminalantigenic material leading to inflammation and furtherbarrier breakdown. Thus, a self-perpetuating cycle ofinflammation is initiated leading to severe pathology[5–7]. Because of the limited number of current therapeuticoptions available, treatment often ultimately resorts tosurgical resection of significant amounts of chronicallyinflamed intestinal tissue.
Active inflammation is characterized by dramatic shiftsin tissue metabolism and perfusion. These changes includediminished availability of oxygen (hypoxia) [8–10] withsubsequent lactate accumulation and resultant metabolicacidosis. Such shifts in tissue metabolism result, at least inpart, from profound recruitment of inflammatory cells, inparticular myeloid cells such as neutrophils (polymorpho-nuclear cells) and monocytes. The vast majority ofinflammatory cells are not resident cells but are recruitedto inflammatory lesions [11]. As such, it is important tounderstand the interactions between microenvironmentalmetabolic changes (e.g., hypoxia) as they relate to molecularmechanisms of leukocyte recruitment and intestinal epithelialdysfunction during inflammation. More importantly, it isimperative to define whether mechanisms initiated byhypoxia might serve as potential therapeutic targets.
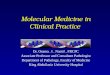
A number of studies have implicated the occurrence ofhypoxia in mucosal inflammatory diseases such as IBD[12]. Surgical specimens from patients with IBD haverevealed prominent hypoxia-inducible factor (HIF)-1 andHIF-2 activation associated with increased vascular densityin diseased areas [13]. Other studies in humans haverevealed that a number of microvascular abnormalitiesmay contribute to diminished blood flow to the intestine inIBD, including the loss of endothelial nitric oxide genera-tion and enhanced tissue vasoconstrictor production [12].Moreover, Vascular endothelial growth factor-dependentangiogenesis appears to be an integral part of human IBD[14]. In support of these hypotheses, studies in murinemodels have identified the epithelium as the central targetof hypoxia during active mucosal inflammation [15]. Aspart of our ongoing work, we have confirmed the existenceof mucosal hypoxia in murine models of IBD using 2-nitroimidazole dyes, a class of compounds known toundergo intracellular metabolism depending on the avail-ability of oxygen within tissue (Fig. 1). Nitroimidazolesenter viable cells where they undergo a single electronreduction, to form a reactive intermediate species. In thepresence of normal oxygen levels, the molecule is imme-
Fig. 1 Mucosal oxygen gradients in normal and inflamed intestinalmucosae. a Under normal physiologic conditions, there exists a steepoxygen gradient across the intestinal mucosa as demonstrated by EF5staining (red) of colonic epithelial cells (left). Nuclei are stained withDAPI (blue). Tissues from mice treated with TNBS to induce colitisdemonstrate dramatically increased EF5 staining reflecting significantinflammation-associated tissue hypoxia. Reproduced in part withcopyright permission from the Journal of Clinical Investigation.b Schematic representing mucosal perfusion (red) and inflammatorycell infiltrate (purple) in healthy (left) and inflamed (right) mucosaltissues. Vasculitis and increased inflammatory cell activity combine tocause tissue hypoxia in inflamed tissues
1296 J Mol Med (2007) 85:1295–1300

diately reoxidized and diffuses out of the cell. In theabsence of adequate oxygen concentrations, the molecule isincompletely reoxidized, and the highly reactive reducedform associates with intracellular proteins, forming adductsthat can be localized with antibodies [16].
Localization of hypoxia utilizing these 2-nitroimidazoledyes revealed two interesting observations. First, in thesmall intestine and especially the colon, “physiologichypoxia” appears to predominate. Indeed, accumulation ofnitroimidazole adducts were readily evident in epithelialcells lining the lumenal aspect of the intestine. This was notthe case in other tissues (e.g., lung and liver, unpublishedobservation), confirming previous studies that the restingpO2 in the intestinal epithelium is quite low, likely becauseof the steep gradient of oxygen across the lumenal aspect.Second, these imaging studies revealed that cells overlyingmucosal lesions are considerably more hypoxic. Accumu-lation of nitroimidazole adducts, particularly in the epithe-lium, were as intense as those observed in some tumors,suggesting the existence of intense foci of hypoxiaassociated with these inflammatory lesions. While we donot yet know the basis for such inflammatory hypoxia,some evidence suggests that tissue vasculitis could predis-pose epithelia toward diminished oxygen delivery [15].
HIF is protective for mucosal inflammation
A number of studies have revealed that HIF elicits a barrierprotective program in the intestine [17–20]. While origi-nally guided by microarray analysis of differentiallyexpressed messenger ribonucleic acid (mRNA) in culturedepithelial cells subjected to hypoxia, these studies haveproven robust in a number of animal models of inflamma-
tion. Further interrogation of mechanisms related tohypoxia-elicted barrier protection have revealed threeimportant features. First, expression of the functionalproteins encoded by these mRNAs was localized to themost lumenal aspect of polarized epithelia (i.e., apicallyexpressed proteins). Second, molecular dissection of thehypoxia-elicited pathway(s) for this “apical gene cluster”revealed a high propensity for regulation by HIF. Third,HIF-dependent epithelial barrier-protective pathways drivenby hypoxia tend to be more “nonclassical” regulators ofbarrier function. Rather than classic junctional proteins suchas occludin or claudin(s), hypoxia-induced enhancement ofbarrier function occurs through diverse pathways, rangingfrom increased mucin production [21] and molecules thatmodify mucins (e.g., intestinal trefoil factor) [17], toxenobiotic clearance (P-glycoprotein) [18] to nucleotidemetabolism (ecto-5′-nucleotidase, CD73) [19–20] andnucleotide signaling (adenosine A2B receptor) [20] (Fig. 2).
To more fully understand the physiologic implications ofintestinal epithelial HIF, Karhausen et al. [15] generatedtwo mouse lines with intestinal epithelial-targeted expres-sion of either mutant Hif1a (constitutive repression of HIF-1) or mutant von Hippel-Lindau gene (Vhlh, constitutiveoverexpression of HIF, which includes HIF-1 and HIF-2).Studies of colitis in these mice revealed that the loss ofepithelial HIF-1 correlated with more severe clinicalsymptoms (mortality, weight loss, colon length, intestinalepithelial permeability), whereas an increase in epithelialHIF was protective for these individual parameters. Thesestudies clearly demonstrated that HIF-1α plays a criticalrole in barrier maintenance and provide evidence for ourinitial hypothesis of a HIF-1-controlled apical gene cluster.The role of HIF-2α in inflammatory lesions in the intestineremains less clear. However, given the differences in both
Fig. 2 HIF-dependent barrierprotective gene expression inintestinal epithelial cells.Under conditions of hypoxia,intestinal epithelial cells expressa number of barrier protectivegenes in a HIF-1 dependentmanner
J Mol Med (2007) 85:1295–1300 1297

tissue distribution patterns and target gene preferencesbetween HIF-1α and HIF-2α, it is likely that this isoformplays a distinct role in IBD. Future studies will address thisimportant question.
Further evidence in support of a protective role for HIFin mucosal disease are provided by studies directed at HIFprolyl hydroxylase (PHD) inhibitors [22, 23]. Theseenzymes were identified on the principle that othermammalian PHDs such as those which target extracellularcollagen were 2-oxoglutarate dependent [24], and it waspredicted that the HIF PHDs would also belong to thisfamily of enzymes. Based on conserved structural features[24], a candidate molecular approach was used to defineHIF-modifying enzymes. This approach identified the HIFPHDs as the products of genes related to C.elegans egl-9, agene that was first described in the context of an egg-layingabnormal phenotype [25]. In mammalian cells, three PHDisoforms were identified (PHD 1–3), and shown tohydroxylate HIF-α in vitro [26–27]. These enzymes havean absolute requirement for oxygen as the substrate. Theoverall reaction results in insertion of one oxygen atom intothe HIF-α peptide substrate at the proline residue, with theother oxygen molecule generating succinate from 2-OGwith the release of CO2. Reactions conducted in a limitedoxygen environment have revealed that the activity of thepurified enzyme is strikingly sensitive to diminished levelsof oxygen in vitro [26–27]. The three enzymes havedifferent tissue distributions and, at least under conditionsof overexpression, have distinct patterns of subcellularlocalization [15, 19]. PHD1 mRNA is expressed in manytissues, with especially high expression in the testis.Likewise, PHD2 mRNA is widely expressed, with partic-ularly abundant expression in adipose tissue [24, 28].PHD3 mRNA is also expressed in many tissues but ismost abundant in the heart and placenta [24, 28]. In mouseintestinal mucosal tissue, we have found expression allthree isoforms of PHDs with a distribution of PHD1<PHD2=PHD3 [22–23].
The discovery of HIF-selective PHDs as central regu-lators of HIF expression has now provided the basis forpotential development of PHD-based molecular tools andtherapies [29–30]. Pharmacological inactivation of thePHDs by 2-OG analogues is sufficient to stabilize HIF-α[29], but this action is nonspecific with respect to individualPHD isoforms. In vitro studies suggest significant differ-ences in substrate specificity. For example, comparison ofenzyme activity in vitro showed that the HIF ODDsequence is hydroxylated most efficiently by PHD2 [24,28]. These observations have generated interest in identi-fying enzyme-modifying therapeutics. Indeed, a number ofPHD inhibitors have been described, including direct inhib-itors of the PHDs [31–32], analogs of naturally occurringcyclic hydroxamates [23], as well as antagonists of α-keto-
glutarate [29]. As such, we hypothesized that pharmacol-ogic activation of HIF would provide a protective adapta-tion to murine colitic disease. For these purposes, we haveused PHD inhibitors that stabilize HIF-α and subsequentlydrive the expression of downstream HIF target genes.
Fig. 3 Hypoxia-dependent HIF and NF-κB activation in intestinalepithelial cells. Exposure of cells to hypoxia or the hydroxylaseinhibitor DMOG results in hydroxylase inhibition, which facilitatesactivation of both the HIF and NF-κB pathways. HIF-1-dependentpathways lead to enhanced epithelial barrier function through theexpression of barrier protective genes. NF-κB likely enhances barrierfunction by the prevention of apoptosis of intestinal epithelial cells. Inconcert, these two pathways effectively increase barrier function andare thus protective against colitis
Fig. 4 Interactions between HIF and NF-κB signaling pathways.Both HIF and NF-κB are activated in hypoxia through decreasedhydroxylase activity. Similarly, both HIF-1 and NF-κB are activatedby proinflammatory mediators such as cytokines and bacteriallipopolysaccharide. It is interesting to note that NF-κB activatestranscriptional upregulation of HIF-1a mRNA indicating one level atwhich these two pathways interact to regulate hypoxia-dependent genetranscription
1298 J Mol Med (2007) 85:1295–1300

Our results show that the PHD inhibition provides anoverall beneficial influence on clinical symptoms (weightloss, colon length, tissue tumor necrosis factor-α/interferon-γ) in multiple murine models of colitis. These effects aremost likely due to their barrier-protective function andenhancement of wound healing at the site of inflammation[22–23]. Taken together, these findings emphasize the roleof epithelial HIF-1α during inflammatory diseases in thecolon and may provide the basis for a therapeutic use ofPHD inhibitors in inflammatory mucosal disease.
Critically, HIF is not the only hypoxia-responsivetranscription factor, and the oxygen-dependent regulatoryrole of hydroxylases is not be restricted to HIF [33]. Indeed,recent studies have indicated that the nuclear factor (NF)κB pathway may also be regulated in a similar manner.Hypoxia activates NF-κB, and this appears at least in partto be mediated through altered hydroxylation of criticalcomponents of this pathway [33–34]. It is interesting tonote that like conditional HIF-1α-null mice, deletion of theNF-κB pathway in intestinal epithelial cells leads toincreased susceptibility to colitis indicating a protectiverole for epithelial NF-κB in colitis. This effect is likelymediated through increased expression of antiapoptoticgenes in the intestinal epithelium resulting in enhancedepithelial barrier function. Thus, a significant part of theprotective effect of hydroxylase inhibition in models ofcolitis may be through the promotion of intestinal epithelialNF-κB activity [22] (Fig. 3). Ongoing studies usingconditional knockout mice are investigating the relativeimportance of the HIF and NF-κB pathways in determiningthe protective effects of hydroxylase inhibition in colitis.
Signaling interactions between hypoxiaand inflammation
As outlined above, both the HIF and NF-κB pathways areactivated under conditions of hypoxia. While the role ofhydroxylases in the hypoxic sensitivity of the HIF pathwayhas been clearly demonstrated, recent data raises theintriguing possibility that components of the NF-κBpathway may also be substrates of hydroxylases includingPHD1 and FIH [33–34]. It is interesting to note that as wellas being hypoxia sensitive, both the HIF and NF-κBpathways are regulated by inflammatory mediators includ-ing cytokines and bacterial products such as lippopolysac-charide [35–36] (Fig. 4). A range of inflammatory stimuliactivate NF-κB through receptor occupation and activationof a complex and diverse array of receptor specific signaltransduction pathways. Critically, one of the gene targets ofNF-κB is HIF-1α. Thus, inflammatory stimuli activate theHIF pathway through transcriptional upregulation of the
HIF-1 mRNA expression in an NF-κB-dependent manner.Conversely, NF-κB activity in hypoxia can be regulated byHIF [37]. Clearly, an intimate relationship exists betweenNF-κB and HIF-1 signaling in the context of microenviron-ments where hypoxia and inflammation coexist such as theinflamed bowel. Intestinal epithelial cells are unique in thatthey are constantly exposed to inflammatory stimuli and asteep oxygen gradient, which may underscore the impor-tance of these pathways in the regulation of epithelial cellfunction both in physiology and disease.
Conclusions and perspectives
The gastrointestinal mucosa provides a unique setting tostudy tissue oxygenation and changes in disease states. Therelatively low baseline pO2 coupled with high blood flowand energy demand against a background of physiologicinflammatory activity identify this mucosal surface ashaving high potential for targeted HIF-based therapy.Results from animal models of IBD have demonstrated anoverall beneficial impact of hydroxylase inhibition. Keyissues remaining to be elucidated include identification ofthe critical gene targets involved, determination of therelative roles of HIF and NF-κB pathways, identification oftissue-specific expression of HIF PHD isoforms, andelucidation of the role of HIF-2α in this protectiveresponse. In summary, the endogenous adaptive pathwaysactivated in response to hypoxia represent potentiallyimportant new windows of therapeutic opportunity in IBD.
References
1. Poonam P (2007) The biology of oral tolerance and issues relatedto oral vaccine design. Curr Pharm Des 13:2001–2007
2. Friedman GB, Taylor CT, Parkos CA, Colgan SP (1998)Epithelial permeability induced by neutrophil transmigration ispotentiated by hypoxia: role of intracellular cAMP. J Cell Physiol176:76–84
3. Taylor CT, Dzus AL, Colgan SP (1998) Autocrine regulation ofepithelial permeability by hypoxia: role for polarized release oftumor necrosis factor alpha. Gastroenterology 114:657–668
4. Taylor CT, Lisco SJ, Awtrey CS, Colgan SP (1998) Hypoxiainhibits cyclic nucleotide-stimulated epithelial ion transport: rolefor nucleotide cyclases as oxygen sensors. J Pharmacol Exp Ther284:568–575
5. Xavier RJ, Podolsky DK (2007) Unravelling the pathogenesis ofinflammatory bowel disease. Nature 448:427–434
6. Baumgart DC, Carding SR (2007) Inflammatory bowel disease:cause and immunobiology. Lancet 369:1627–1640
7. Sartor RB (1995) Current concepts of the aetiology andpathogenesis of ulcerative colitis and Crohn's disease. Gastro-enterol Clin North Am 24:475–507
8. Haddad JJ (2003) Science review: redox and oxygen-sensitivetranscription factors in the regulation of oxidant-mediated lunginjury: role for hypoxia-inducible factor-1alpha. Crit Care 7:47–54
J Mol Med (2007) 85:1295–1300 1299

9. Kokura S, Yoshida N, Yoshikawa T (2002) Anoxia/reoxygenation-induced leukocyte–endothelial cell interactions. Free Radic BiolMed 33:427–432
10. Saadi S, Wrenshall LE, Platt J (2003) Regional manifestations andcontrol of the immune system. FASEB J 16:849–856
11. Lewis JS, Lee JA, Underwood JC, Harris AL, Lewis CE (1999)Macrophage responses to hypoxia: relevance to disease mecha-nisms. J Leukoc Biol 66:889–900
12. Hatoum OA, Binion DG, Gutterman DD (2005) Paradox ofsimultaneous intestinal ischaemia and hyperaemia in inflammato-ry bowel disease. Eur J Clin Invest 35:599–609
13. Giatromanolaki A, Sivridis E, Maltezos E, Papazoglou D,Simopoulos C, Gatter KC, Harris AL, Koukourakis MI (2003)Hypoxia inducible factor 1alpha and 2alpha overexpression ininflammatory bowel disease. J Clin Pathol 56:209–213
14. Danese S, Dejana E, Fiocchi C (2007) Immune regulation bymicrovascular endothelial cells: directing innate and adaptive immu-nity, coagulation, and inflammation. J Immunol 178:6017–6022
15. Karhausen JO, Furuta GT, Tomaszewski JE, Johnson RS, ColganSP, Haase VH (2004) Epithelial hypoxia-inducible factor-1 isprotective in murine experimental colitis. J Clin Invest 114:1098–1106
16. Evans SM, Hahn S, Pook DR, Jenkins WT, Chalian AA, Zhang P,Stevens C, Weber R, Weinstein G, Benjamin I, Mirza N, MorganM, Rubin S, McKenna WG, Lord EM, Koch CJ (2000) Detectionof hypoxia in human squamous cell carcinoma by EF5 binding.Cancer Res 60:2018–2024
17. Furuta GT, Turner JR, Taylor CT, Hershberg RM, Comerford KM,Narravula S, Podolsky DK, Colgan SP (2001) Hypoxia-induciblefactor 1-dependent induction of intestinal trefoil factor protectsbarrier function during hypoxia. J Exp Med 193:1027–1034
18. Comerford KM, Wallace TJ, Karhausen J, Louis NA, MontaltoMC, Colgan SP (2002) Hypoxia-inducible factor-1-dependentregulation of the multidrug resistance (MDR1) gene. Cancer Res62:3387–3394
19. Synnestvedt K, Furuta GT, Comerford KM, Louis N, Karhausen J,Eltzschig HK, Hansen KR, Thompson LF, Colgan SP (2002)Ecto-5′-nucleotidase (CD73) regulation by hypoxia-induciblefactor-1 (HIF-1) mediates permeability changes in intestinalepithelia. J Clin Invest 110:993–1002
20. Eltzschig HK, Ibla JC, Furuta GT, Leonard MO, Jacobson KA,Enjyoji K, Robson SC, Colgan SP (2003) Coordinated adeninenucleotide phosphohydrolysis and nucleoside signaling in post-hypoxic endothelium: role of ectonucleotidases and adenosineA2B receptors. Exp Med 198:783–796
21. Louis NA, Hamilton KE, Canny G, Shekels LL, Ho SB, ColganSP (2006) Selective induction of mucin-3 by hypoxia in intestinalepithelia. J Cell Biochem 99:1616–1627
22. Cummins EP, Seeballuck F, Keely SJ, Mangan NE, Callanan JJ,Fallon PF, Taylor CT (2008) The hydroxylase inhibitor DMOG isprotective in a murine model of colitis. Gastroenterol (in press)
23. Robinson A, Keely S, Karhausen J, Gerich ME, Furuta GT,Colgan SP (2008) Mucosal protection by HIF prolyl hydroxylaseinhibition. Gastroenterology (in press)
24. Bruick RK (2003) Oxygen sensing in the hypoxic responsepathway: regulation of the hypoxia-inducible transcription factor.Genes Dev 17:2614–2623
25. Epstein AC, Gleadle JM, McNeill LA, Hewitson KS, O’Rourke J,Mole DR, Mukherji M, Metzen E, Wilson MI, Dhanda A, TianYM, Masson N, Hamilton DL, Jaakkola P, Barstead R, Hodgkin J,Maxwell PH, Pugh CW, Schofield CJ, Ratcliffe PJ (2001) C.elegans EGL-9 and mammalian homologs define a family ofdioxygenases that regulate HIF by prolyl hydroxylation. Cell107:43–54
26. Jaakkola P, Mole DR, Tian YM, Wilson MI, Gielbert J, GaskellSJ, Kriegsheim A, Hebestreit HF, Mukherji M, Schofield CJ,Maxwell PH, Pugh CW, Ratcliffe PJ (2001) Targeting of HIF-alpha to the von Hippel-Lindau ubiquitylation complex by O2-regulated prolyl hydroxylation. Science 292:468–472
27. Hon WC, Wilson MI, Harlos K, Claridge TD, Schofield CJ, PughCW, Maxwell PH, Ratcliffe PJ, Stuart DI, Jones EY (2002)Structural basis for the recognition of hydroxyproline in HIF-1alpha by pVHL. Nature 417:975–978
28. Schofield CJ, Ratcliffe PJ (2004) Oxygen sensing by HIFhydroxylases. Nat Rev Mol Cell Biol 5:343–354
29. Mole DR, Schlemminger I, McNeill LA, Hewitson KS, Pugh CW,Ratcliffe PJ, Schofield CJ (2003) 2-oxoglutarate analogue inhib-itors of HIF prolyl hydroxylase. Bioorg Med Chem Lett 13:2677–2680
30. Masson N, Ratcliffe PJ (2003) HIF prolyl and asparaginylhydroxylases in the biological response to intracellular O(2)levels. J Cell Sci 116:3041–3049
31. Nwogu JI, Geenen D, Bean M, Brenner MC, Huang X, ButtrickPM (2001) Inhibition of collagen synthesis with prolyl 4-hydroxylase inhibitor improves left ventricular function and altersthe pattern of left ventricular dilatation after myocardial infarction.Circulation 104:2216–2221
32. Schlemminger I, Mole DR, McNeill LA, Dhanda A, HewitsonKS, Tian YM, Ratcliffe PJ, Pugh CW, Schofield CJ (2003)Analogues of dealanylalahopcin are inhibitors of human HIFprolyl hydroxylases. Bioorg Med Chem Lett 13:1451–1454
33. Cummins EP, Berra E, Comerford KM, Ginouves A, FitzgeraldKT, Seeballuck F, Godson C, Nielsen JE, Moynagh P,Pouyssegur J, Taylor CT (2006) Prolyl hydroxylase-1 negativelyregulates IkappaB kinase-beta, giving insight into hypoxia-induced NFkappaB activity. Proc Natl Acad Sci USA103:18154–18159
34. Cockman ME, Lancaster DE, Stolze IP, Hewitson KS, McDonoughMA, Coleman ML, Coles CH, Yu X, Hay RT, Ley SC, Pugh CW,Oldham NJ, Masson N, Schofield CJ, Ratcliffe PJ (2006)Posttranslational hydroxylation of ankyrin repeats in IkappaBproteins by the hypoxia-inducible factor (HIF) asparaginyl hydrox-ylase, factor inhibiting HIF (FIH). Proc Natl Acad Sci USA103:14767–14772
35. Pouyssegur J, Mechta-Grigoriou F (2006) Redox regulation of thehypoxia-inducible factor. Biol Chem 387:1337–1346
36. Frede S, Stockmann C, Freitag P, Fandrey J (2006) Bacteriallipopolysaccharide induces HIF-1 activation in human monocytesvia p42/44 MAPK and NF-kappaB. Biochem J 396:517–527
37. Walmsley SR, Print C, Farahi N, Peyssonnaux C, Johnson RS,Cramer T, Sobolewski A, Condliffe AM, Cowburn AS, JohnsonN, Chilvers ER (2005) Hypoxia-induced neutrophil survival ismediated by HIF-1alpha-dependent NF-kappaB activity. J ExpMed 201:105–15
1300 J Mol Med (2007) 85:1295–1300

REVIEW
Hypoxia and cancer
M. Christiane Brahimi-Horn & Johanna Chiche &
Jacques Pouysségur
Received: 28 September 2007 /Revised: 22 October 2007 /Accepted: 23 October 2007 / Published online: 20 November 2007# Springer-Verlag 2007
Abstract A major feature of solid tumours is hypoxia,decreased availability of oxygen, which increases patienttreatment resistance and favours tumour progression. Howhypoxic conditions are generated in tumour tissues and howcells respond to hypoxia are essential questions in under-standing tumour progression and metastasis. Massivetumour-cell proliferation distances cells from the vascula-ture, leading to a deficiency in the local environment ofblood carrying oxygen and nutrients. Such hypoxic con-ditions induce a molecular response, in both normal andneoplastic cells, that drives the activation of a keytranscription factor; the hypoxia-inducible factor. Thistranscription factor regulates a large panel of genes thatare exploited by tumour cells for survival, resistance totreatment and escape from a nutrient-deprived environment.Although now recognized as a major contributor to cancerprogression and to treatment failure, the precise role ofhypoxia signalling in cancer and in prognosis still needs tobe further defined. It is hoped that a better understanding ofthe mechanisms implicated will lead to alternative and moreefficient therapeutic approaches.
Keywords Angiogenesis . Autophagy . Bcl-2/adenovirusEIB 19 kDa-interacting protein 3 . Cancer .
Carbonic anhydrase . Hypoxia . Hypoxia-inducible factor .
Oxygen-sensor . Tumour metabolism . pH regulation
Introduction
Cancer is presently a major cause of mortality in developedcountries and will become even more so in low-incomecountries as the global population increases and ages and asimprovements in detection are implemented [1]. Althoughsome cancers occur in the young, most are associated withthe elderly, and both events represent the accumulation ofgenetic and epigenetic cell damage [2]. Cancer includes adiverse collection of diseases, from a cellular origin point ofview, rather than a single disease, the causes of which areequally as diverse [3]. Aberrant cell-cycle checkpointcontrol, overactivation of oncogenes and inhibition oftumour-suppressor genes are considered to be primordialin the initiation of tumourigenesis. However, other factorsrelated to the tumour microenvironment are now beingrecognized as fundamental in tumour progression, increasedresistance and metastasis. Hypoxia is one of these factors,the repercussions of which are shared by all cancer typesincluding haematological cancers [4].
The hypoxic tumour phenotype
Robust tumour growth requires the presence of a localvascular network that supplies both oxygen and nutrients totumour cells. However, a highly proliferating mass of tumourcells develops faster than the vasculature, and tumour cellsrapidly meet up with an avascular environment deficient inoxygen, i.e. hypoxic. This is a consequence of the diffusionlimit of oxygen within tissues, which has been measured to bearound 150 μm [5, 6] (Fig. 1). On histological examination,tumours often show a central core of necrotic cells, whichhas been suggested to result from a drop in the oxygenavailability to conditions of severe hypoxia and glucose
J Mol Med (2007) 85:1301–1307DOI 10.1007/s00109-007-0281-3
DO00281; No of Pages
M. C. Brahimi-Horn (*) : J. Chiche : J. PouysségurInstitute of Signaling, Developmental Biology and Cancer Research,University of Nice,CNRS UMR 6543, Centre A. Lacassagne,33 Avenue Valombrose,06189 Nice, Francee-mail: [email protected]

deprivation resulting in cell death. A number of methodshave been developed to measure the oxygen concentration intissues including chemical markers such as pimonidazolehydrochloride or EF5, oxygen miocroelectrodes or opticalpartial pressure of oxygen-measuring devices. Such hypoxiczones have been postulated to have a reduced response toradiotherapy due to a decrease in oxygen-free radicals thatare required to produce enough DNA damage to give celldeath [7]. In addition, cells of these regions are considered tobe chemotherapy-resistant due to limited delivery of drugsvia the circulation. Hypoxic tumours also show an extracel-lular pH (pHe) that is lower than that of correspondingnormal tissue [8]. The acidotic nature is the consequence of amodification in the metabolism of tumour cells, in particularthat of glucose [9] (Fig. 1).
Hypoxia-inducible factor, the molecular key to hypoxia
Hypoxia activates an alpha/beta heterodimeric transcriptionfactor termed appropriately the hypoxia-inducible factor(HIF). Activation resides in the inhibition of posttransla-tional hydroxylation of the alpha subunit that permitsstabilization, heterodimerisation and binding to hypoxia-response elements (HRE) in target genes. The details of themechanisms of regulation of the stability and activity ofHIF-α have been extensively reviewed by us [10–12] andothers [13–16]. Suffice it to say that posttranslationalhydroxylation by oxygen-dependent oxygenases, prolylhydroxylase domain proteins and factor inhibiting HIF
(FIH) destabilize and inactivate, respectively, HIF-α. Theformer, by favouring von Hippel-Lindau (VHL) E3ubiquitin ligase-mediated proteasomal degradation, andthe latter, by inhibiting interaction with co-activators suchas p300/CBP.
The HIF-mediated cellular response
Non-hydroxylated, active HIF-α/β targets about 1–2% ofthe human genome leading to induction or repression ofgenes with subsequent up- or down-regulation of expres-sion, respectively, of the corresponding gene products. Abroad range of genes that are implicated in events such asangiogenesis, cell survival/death, metabolism, pH regula-tion, adhesion, extracellular matrix remodeling, migrationand metastasis are targeted [12, 15, 17, 18]. The functionalconsequences of enhanced expression of a small selectionof some of these gene products are discussed below(Fig. 2).
Angiogenesis
HIF-mediated expression of gene products including thevascular endothelial growth factor-A (VEGF-A) and angio-poïetin-2 (Ang-2) allow tumour cells to turn around thehypoxic situation by inducing regrowth of the vascularnetwork, a phenomenon termed angiogenesis [19]. Therebyan oxygenated and nutritional environment is reestablishedfor maintenance of growth. However, the neo-vesselsformed are often distorted and irregular and thus lessefficient in oxygen, nutrient transport and drug delivery.
Cell survival or death
Thus, hypoxia initiates a cascade of events that allowstumour cells to continue to proliferate; however, if toosevere, hypoxia can also lead to cell death as shown by thepresence in tumours of a central necrotic zone. In fact, itcan be envisaged that highly variable levels of hypoxiaaccompany the dynamics of spatiotemporal development ofthe tumour mass so that a multitude of tumour cellresponses are manifested (Fig. 1). Interplay between FIHand the transcriptional activation domains of HIF-1α, basedon the degree of oxygen dependence of FIH for activity, hasbeen proposed to select for different gene profiles thatdetermine cell fate [20]. Gene-profile selectivity may alsoarise from differential action of the three HIF-α subunitsand, within the context, may promote cell proliferation ordeath [21, 22]. The genes bnip3, Bcl-2/adenovirus EIB19 kDa-interacting protein 3, and bnip3L (bnip3-like), theproducts of which are members of the BH3-only proteinfamily of cell death factors, are highly induced in hypoxia.
Fig. 1 The characteristics of a hypoxic tumour mass. Bloodcapillaries carry oxygen to tissues, but since oxygen has a diffusionlimit, its concentration decreases as the distance from capillariesincreases. Macroscopic examination of solid tumours reveals thepresence of expanding tumour cells in proximity to capillaries and acentral region of necrotic cells. This gradient of cell viability parallelsthat of a decreasing gradient of oxygen, which is accompanied by anincrease in HIF-1α levels, a decrease in the extracellular pH and anincrease in the resistance to radio- and chemo-therapy
1302 J Mol Med (2007) 85:1301–1307

Although many studies have pointed at the pro-apoptoticfeatures of these two gene products, these findings arelargely controversial. We propose instead that the BH3domains of BNIP3 and BNIP3L belong to another class,like the BH3 domain of Beclin1, that do not induce celldeath but survival by triggering autophagy [12, 23, 24].Macroautophagy is a process that allows cells to recycleintracellular organelles such as ribosomes and mitochondriafor nutritional and protective purposes [25]. Catabolism oforganelle components provides nutrient-depleted cells witha source of lipids, amino acids and sugars, and autophagyof mitochondria may protect cells from harmful reactiveoxygen species.
Metabolism
A substantial number of genes involved in cellularmetabolism, in particular those of glucose, are HIF-mediated. It has been known for many years that cancercells divert pyruvate metabolism away from mitochondrialoxidative phosphorylation (OXPHOS) toward cytoplasmicconversion of pyruvate to lactic acid [11]. Although thislatter simplified pathway produces less adenosine triphos-phate (ATP) per molecule of glucose, cells compensate fora reduced yield in ATP production by increasing both theuptake of glucose and the flux in conversion of glucose topyruvate, i.e. glycolysis. This is made possible through an
increase in HIF-mediated expression of both glucosetransporters and enzymes of the glycolytic pathway, givingtumours a “glycolytic” phenotype. Diversion of pyruvatetoward lactate and away from OXPHOS is also promotedthrough increased HIF-mediated expression of two keyenzymes; lactate dehydrogenase A (LDH-A) [26] andpyruvate dehydrogenase kinase 1 (PDK1) [27, 28]. LDH-A is the enzyme responsible for conversion of pyruvate tolactate, and PDK1 is an inhibitor of pyruvate dehydroge-nase that feeds pyruvate into the tricarboxylic acid cycleand thus toward OXPHOS. Thereby, HIF not only channelsglucose towards glycolysis by repressing mitochondrialrespiration but it also optimizes low levels of respiration byregulating the ratio of isoforms of cytochrome c oxidase,components of the electron transport chain [29]. Thisstrategy not only makes respiration more efficient but mayalso protect cells from oxidative damage under hypoxicconditions. Metabolic regulation via HIF also brings intoplay products of tumour suppressors and oncogenes such asp53, c-Myc, Ras and Akt [11, 21, 30].
Another pathway related to nutrient availability, which ismodified by HIF, is that of mammalian target of rapamycin(mTOR). On the one hand, growth factors and nutrientspotentiate the mTOR pathway in conveying signals ofgrowth and survival through increased protein synthesis,and on the other hand, energy depletion and hypoxiasuppress mTOR, saving on energy-consuming protein
Fig. 2 HIF-induced gene products and their function. The α/βheterodimer HIF bound to hypoxia-response elements (HRE) in targetgenes mediates the expression of a vast array of proteins implicated infunctions such as angiogenesis, cell survival/death, metabolism, pHhomeostasis and metastasis. A small selection of proteins (boxed, inblue) is shown and include: AMF autocrine motility factor; ANG-2angiopoïetin-2; BNIP3 Bcl-2/adenovirus EIB 19 kDa-interactingprotein 3; BNIP3L Bcl-2/adenovirus EIB 19 kDa-interacting protein
3 like; CA IX, XII carbonic anhydrase; CXCR4 cytokine (C-X-C motif)receptor 4; GLUT1 glucose transporter 1; LDH-A lactate dehydroge-nase-A; LON, a mitochondrial protease; LOX lysyl oxidase; MCT1, 4,monocarboxylate transporter; MMP matrix metalloproteinase; NOXApro-apoptotic member of Bcl-2 protein family; PDK1 pyruvatedehydrogenase kinase 1; REDD1/RTP801; VEGF vascular endothelialgrowth factor; VEGF-R1, vascular endothelial growth factor receptor
J Mol Med (2007) 85:1301–1307 1303

synthesis, allowing for cellular adaptation and subsequentsurvival [12].
Regulation of pH
One of the consequences of the predilection of cancer cellsfor cytoplasmic glucose metabolism in producing lactic acidis acidosis, a decrease in the extracellular pH [31]. Thisacidosis, generated by the increased production of carbonicand lactic acids, is exacerbated by the limiting vasculature.Despite a low pHe, the intracellular pH (pHi) of tumourcells is maintained at a relatively normal pH or evenslightly more alkaline pH, which is reported to result fromHIF-mediated up-regulation and activation of a number ofmembrane located transporters, exchanges, pumps andecto-enzymes that are implicated in pH homeostasis.Among these are the growth factor activatable andamiloride-sensitive Na+/H+ Exchanger (NHE-1) [32–34]and the H+/lactate cotransporter (monocarboxylate trans-porter, MCT1 and MCT4) [35]. In addition, one of themost highly HIF-induced proteins, carbonic anhydrase IX(CA IX), an enzyme that catalyzes the reversible conver-sion of CO2 to carbonic acid (Fig. 3), has been reported toregulate the pHe [36], and we propose that it maycontribute to an increase in the pHi through C1�
�HCO�
3
exchanger uptake of HCO�3 . Coupled interaction between
MCT1 [37] and CA II and between different CA isoformsand proteins of the superfamily of bicarbonate transporters,including the anion exchangers [38, 39] or sodiumbicarbonate co-transporter (NBCs) proteins [39] has beenreported. Such interplay would allow tumour cells tomaintain a more alkaline pH for subsequent cell growth[40].
Metastasis
Substantial data points toward hypoxic promotion of theinvasive potential of tumour cells. HIF activation isassociated with loss of E-cadherin, a component ofadherens junctions that acts as a suppressor of invasionand metastasis [41]. In this context, it is interesting thatTWIST1, a regulator of epithelial-mesenchymal transition[42], is induced in hypoxia [43]. In addition, cells thatsurvive acidosis not only develop a growth advantage butalso become more aggressive and invasive [6, 44]. Thisoccurs in part through the activation of HIF-up-regulatedproteins implicated in matrix remodeling, such as lysyloxydase (LOX) [12, 45], metalloproteases that disrupt cell–cell and cell–matrix (ECM) interactions [46]. HIF alsoactivates other genes known to be involved in metastasisand invasion such as the c-met proto-oncogene, thechemokine receptor CXCR4 and the autocrine motilityfactor (AMF) [41, 47].
Clinical significance of hypoxia, HIF and HIFdownstream gene products in prognosis
Since hypoxia in tumours and internalization of high levelsof glucose into tumours are considered to be indicators ofmore aggressive tumours, and thus of poor patientprognosis [48], attempts to detect these characteristics inpatients’ tumours have been developed using positronemission tomography (PET). Hypoxic zones are detectedafter injection of [fluorine-18] misonidazole (FMISO),while tumours that capture glucose can be detected afterinjection of [fluorine-18] deoxyglucose (FDG), a non-
Fig. 3 Tumour expression of carbonic anhydrase IX (CA IX) andhypoxia-inducible factor-1α (HIF-1α). Immunohistological detection ofCA IX and HIF-1α colocalized in hypoxic regions of a section of a human
colon adenocarcinoma (LS174) grown in nude mice (Dayan et al.,unpublished data). Note the hypoxic gradient that develops away from theblood vessel and the necrotic area around the most hypoxic ring
1304 J Mol Med (2007) 85:1301–1307

metabolizable analogue of glucose (Fig. 4). However, adirect correlation between high glucose uptake and hypoxicregions was not observed [49, 50]. This may result from thefact that only highly hypoxic regions, though not necrotic,are detected with FMISO, so areas where the oxygenconcentration is nonetheless sufficiently low for stablizationof HIF-α may not be identified. Alternatively, cycles ofhypoxia and angiogenic reoxygenation that give rise to ahigh glucose capture phenotype may have precededanalysis. The recognition that hypoxic areas are radiother-apy resistant has led to a number of strategies to increasethe oxygen availability or to deliver radiosensitizing agents[7].
Since HIF-α and HIF-induced proteins such as CA IX,CA XII and Glut1 are highly expressed in renal cellcarcinomas (RCC) and in multiple human cancers, theirexpression has been investigated as markers of tumouraggressiveness and in determining prognosis [22]. RCC is aprototype cancer for understanding the role of HIF incancer progression since it carries loss-of-function muta-tions in the VHL gene, the product of which is responsiblefor targeting HIF-α for proteasomal degradation [51]. Thus,in these cancers, HIF-α is stable, and downstream geneproducts are induced. To better appreciate the implicationof HIF in tumour progression and prognosis, immunohis-tochemical studies have been performed in several othercancer types to detect for both HIF-α and HIF-downstreamgene products such as BNIP3, CA IX and XII, Glut1 and
VEGF (Figs. 3 and 4). The inherent problem related to thedetection of HIF-α in tissue specimens is the short half-lifeof HIF-α not only in vivo but also when the specimencomes in contact with atmospheric oxygen during surgicalremoval. In fact, recent studies have established that thiswas not the case and make these studies reporting levels ofHIF-α relevant [52]. It was shown that HIF-1α and CA IXexpression correlate with poor prognosis in breast cancer[52]. The longer half-life of the other potential markerproteins may make interpretation difficult as detection mayreflect only past events. These markers were shown tocorrelate for both primary breast tumours and lymph nodemetastases [53], and further studies have demonstratedreduced survival correlated with CA IX expression in breastcancer [54]. In breast cancer, high BNIP3 expression wasassociated with good survival outcome in invasive carci-noma but with an increased risk of recurrence and shorterdisease-free survival in ductal carcinoma in situ [55], whilein non-small lung cancer, high expression was an indepen-dent factor for overall survival [56]. Further investigation isrequired to obtain a better appreciation of the value of HIFor HIF-related marker immunohistochemistry for prognosis.
Harnessing phenotype in combating tumour growth
Novel processes that engage perturbations in the tumourmicroenvironment may prove efficient as cancer therapies.Inhibition of angiogenesis, although not devoid of harmfulside effects, is showing potential in treatment of severaldifferent types of cancer when in combination with classicalchemotherapy [57]. Both intervention at the level of HIF[58] and HIF downstream genes, in addition to those thatregulate angiogenesis, merit investigation (Fig. 5). Alterna-tive strategies that target the particularities of the tumour
Fig. 4 Clinical significance of hypoxia and HIF in prognosis.Imaging by PET allows detection of hypoxic zones and zones ofhigh glucose uptake in tumours after injection to patients of[fluorine-18] misonidazole (FMISO) or [fluorine-18] deoxyglucose(FDG), respectively. Immunohistochemistry of surgical specimensallows detection of hypoxic regions using primonidazole HCl anddetection of HIF-target gene products such as BNIP3 Bcl-2/adenovirus EIB 19 kDa-interacting protein 3; CA IX carbonicanhydrase; GLUT1 glucose transporter 1; VEGF vascular endothelialgrowth factor. Further studies are required to determine the clinicalpotential of such imaging technologies in prognosis and treatment ofdifferent cancer types
Fig. 5 Potential novel approaches to turning around the hypoxictumour phenotype. By controlling the hypoxic nature of tumours andthe HIF-mediated cellular adaptation or microenvironmental conse-quences, such as acidosis, novel therapeutic approaches shouldpromote cell death
J Mol Med (2007) 85:1301–1307 1305

phenotype may provide tumour-specific agents that holdthe advantage of sparing normal tissue [59–61], which isnot the case with classical chemotherapy. Such strategiesmay prove beneficial alone or in combination withpresently employed cytotoxic agents [62].
Conclusions
The understanding of how hypoxia drives tumour progres-sion is attracting substantial investigation, and an impres-sive number of reviews have ensued; however, a lotremains to be done to clarify not only the mechanismsinvolved but also the implication for diagnosis andtreatment. Further investigation into the relevance of HIF-induced gene products as markers of prognosis shouldfollow. The development of anti-angiogenic agents withsignificant potential as a cancer therapy has led the way indemonstrating that the hypoxic response of tumours can betargeted. Additional targets involved in HIF signalling andin its consequences should also prove beneficial in slowingcancer progression and metastasis.
Acknowledgments The laboratory is funded by grants from theLigue Nationale Contre le Cancer (Equipe labellisée), the Centre A.Lacassagne, the Centre National de la Recherche Scientifique (CNRS),the Ministère de l’Education, de la Recherche et de la Technologie, theInstitut National de la Santé et de la Recherche Médicale (Inserm), andthe Institut National du Cancer (INCA). We apologize to the manyresearch groups whose work was cited indirectly by reference to reviewarticles.
References
1. Bray F, Moller B (2006) Predicting the future burden of cancer.Nat Rev Cancer 6:63–74
2. Finkel T, Serrano M, Blasco MA (2007) The common biology ofcancer and ageing. Nature 448:767–774
3. Colditz GA, Sellers TA, Trapido E (2006) Epidemiology—identifying the causes and preventability of cancer? Nat RevCancer 6:75–83
4. Moehler TM, Ho AD, Goldschmidt H, Barlogie B (2003)Angiogenesis in hematologic malignancies. Crit Rev OncolHematol 45:227–244
5. Folkman J, Hahnfeldt P, Hlatky L (2000) Cancer: looking outsidethe genome. Nat Rev Mol Cell Biol 1:76–79
6. Vaupel P (2004) Tumor microenvironmental physiology and itsimplications for radiation oncology. Semin Radiat Oncol 14:198–206
7. Moeller BJ, Richardson RA, Dewhirst MW (2007) Hypoxia andradiotherapy: opportunities for improved outcomes in cancertreatment. Cancer Metastasis Rev 26:241–248
8. Cardone RA, Casavola V, Reshkin SJ (2005) The role of disturbedpH dynamics and the Na+/H+ exchanger in metastasis. Nat RevCancer 5:786–795
9. Kim JW, Gao P, Dang CV (2007) Effects of hypoxia on tumormetabolism. Cancer Metastasis Rev 26:291–298
10. Bilton R, Trottier E, Pouyssegur J, Brahimi-Horn MC (2006)ARDent about acetylation and deacetylation in hypoxia signalling.Trends Cell Biol 16:616–621
11. Brahimi-Horn MC, Pouyssegur J (2007) Oxygen, a source of lifeand stress. FEBS Lett 581:3582–3591
12. Pouyssegur J, Dayan F, Mazure NM (2006) Hypoxia signalling incancer and approaches to enforce tumour regression. Nature441:437–443
13. Coleman ML, Ratcliffe PJ (2007) Oxygen sensing and hypoxia-induced responses. Essays Biochem 43:1–16
14. Schofield CJ, Ratcliffe PJ (2005) Signalling hypoxia by HIFhydroxylases. Biochem Biophys Res Commun 338:617–626
15. Schofield CJ, Ratcliffe PJ (2004) Oxygen sensing by HIFhydroxylases. Nat Rev Mol Cell Biol 5:343–354
16. Semenza GL (2003) Targeting HIF-1 for cancer therapy. Nat RevCancer 3:721–732
17. Manalo DJ, Rowan A, Lavoie T, Natarajan L, Kelly BD, Ye SQ,Garcia JG, Semenza GL (2005) Transcriptional regulation ofvascular endothelial cell responses to hypoxia by HIF-1. Blood105:659–669
18. Semenza GL (2007) Oxygen-dependent regulation of mitochon-drial respiration by hypoxia-inducible factor 1. Biochem J 405:1–9
19. Ferrara N, Kerbel RS (2005) Angiogenesis as a therapeutic target.Nature 438:967–974
20. Dayan F, Roux D, Brahimi-Horn MC, Pouyssegur J, Mazure NM(2006) The oxygen sensor factor-inhibiting hypoxia-induciblefactor-1 controls expression of distinct genes through thebifunctional transcriptional character of hypoxia-inducible factor-1alpha. Cancer Res 66:3688–3698
21. Gordan JD, Thompson CB, Simon MC (2007) HIF and c-Myc:sibling rivals for control of cancer cell metabolism and prolifer-ation. Cancer Cell 12:108–113
22. Brahimi-Horn MC, Pouyssegur J (2005) The hypoxia-induciblefactor and tumor progression along the angiogenic pathway. IntRev Cytol 242:157–213
23. Maiuri MC, Le Toumelin G, Criollo A, Rain JC, Gautier F, Juin P,Tasdemir E, Pierron G, Troulinaki K, Tavernarakis N, Hickman JA,Geneste O, Kroemer G (2007) Functional and physical interactionbetween Bcl-X(L) and a BH3-like domain in Beclin-1. EMBO J26:2527–2539
24. Mazure NM, Bellot G, Garcia-Medina R, Gounon P, Roux D,Pouyssegur J (2007) Hypoxia-induced autophagy is mediatedthrough the HIF-dependent induction of BNIP3 and BNIP3L. BullCancer 94:534
25. Maiuri MC, Zalckvar E, Kimchi A, Kroemer G (2007) Self-eatingand self-killing: crosstalk between autophagy and apoptosis. NatRev Mol Cell Biol 8:741–752
26. Fantin VR, St-Pierre J, Leder P (2006) Attenuation of LDH-Aexpression uncovers a link between glycolysis, mitochondrialphysiology, and tumor maintenance. Cancer Cell 9:425–434
27. Kim JW, Tchernyshyov I, Semenza GL, Dang CV (2006) HIF-1-mediated expression of pyruvate dehydrogenase kinase: ametabolic switch required for cellular adaptation to hypoxia. CellMetab 3:177–185
28. Papandreou I, Cairns RA, Fontana L, Lim AL, Denko NC (2006)HIF-1 mediates adaptation to hypoxia by actively downregulatingmitochondrial oxygen consumption. Cell Metab 3:187–197
29. Fukuda R, Zhang H, Kim JW, Shimoda L, Dang CV, Semenza GL(2007) HIF-1 regulates cytochrome oxidase subunits to optimizeefficiency of respiration in hypoxic cells. Cell 129:111–122
30. Kim JW, Gao P, Liu YC, Semenza GL, Dang CV (2007) HIF-1and dysregulated c-Myc cooperatively induces VEGF andmetabolic switches, HK2 and PDK1. Mol Cell Biol 27:7381–7393
1306 J Mol Med (2007) 85:1301–1307

31. Swietach P, Vaughan-Jones RD, Harris AL (2007) Regulation oftumor pH and the role of carbonic anhydrase 9. Cancer MetastasisRev 26:299–310
32. Counillon L, Pouyssegur J (2000) The expanding family ofeucaryotic Na(+)/H(+) exchangers. J Biol Chem 275:1–4
33. Sardet C, Franchi A, Pouyssegur J (1989) Molecular cloning,primary structure, and expression of the human growth factor-activatable Na+/H+ antiporter. Cell 56:271–80
34. Shimoda LA, Fallon M, Pisarcik S, Wang J, Semenza GL (2006)HIF-1 regulates hypoxic induction of NHE1 expression andalkalinization of intracellular pH in pulmonary arterial myocytes.Am J Physiol Lung Cell Mol Physiol 291:L941–L949
35. Ullah MS, Davies AJ, Halestrap AP (2006) The plasma membranelactate transporter MCT4, but not MCT1, is up-regulated byhypoxia through a HIF-1alpha dependent mechansm. J Biol Chem281:9030–9037
36. Ivanov S, Liao SY, Ivanova A, Danilkovitch-Miagkova A, TarasovaN, Weirich G, Merrill MJ, Proescholdt MA, Oldfield EH, Lee J,Zavada J, Waheed A, Sly W, Lerman MI, Stanbridge EJ (2001)Expression of hypoxia-inducible cell-surface transmembranecarbonic anhydrases in human cancer. Am J Pathol 158:905–919
37. Becker HM, Hirnet D, Fecher-Trost C, Sultemeyer D, Deitmer JW(2005) Transport Activity of MCT1 Expressed in XenopusOocytes Is Increased by Interaction with Carbonic Anhydrase. JBiol Chem 280:39882–39889
38. Morgan PE, Pastorekova S, Stuart-Tilley AK, Alper SL, Casey JR(2007) Interactions of transmembrane carbonic anhydrase, CAIX,with bicarbonate transporters. Am J Physiol Cell Physiol 293:C738–748
39. Piermarini PM, Kim EY, Boron WF (2007) Evidence against adirect interaction between intracellular carbonic anhydrase II andpure C-terminal domains of SLC4 bicarbonate transporters. J BiolChem 282:1409–1421
40. Chiche J, Laferrière J, Trottier E, Roux D, Mazure N, Brahimi-Horn MC, Pouysségur J (2007) The hypoxia-induced tumormarker carbonic anhydrase IX plays a critical role in tumormicroenvironmental pH homeostasis. Keystone Symposium Con-ference. Molecular Targets for Cancer. Abstract # 134, Whistler,British Columbia, 18–23 March
41. Sullivan R, Graham CH (2007) Hypoxia-driven selection of themetastatic phenotype. Cancer Metastasis Rev 26:319–331
42. Yang J, Mani SA, Weinberg RA (2006) Exploring a new twist ontumor metastasis. Cancer Res 66:4549–4552
43. Gort EH, van Haaften G, Verlaan I, Groot AJ, Plasterk RH,Shvarts A, Suijkerbuijk KP, van Laar T, van der Wall E, Raman V,van Diest PJ, Tijsterman M, Vooijs M (2007) The TWIST1oncogene is a direct target of hypoxia-inducible factor-2alpha.Oncogene (in press). DOI 10.1038/sj.onc.1210795
44. Walenta S, Mueller-Klieser WF (2004) Lactate: mirror and motorof tumor malignancy. Semin Radiat Oncol 14:267–274
45. Erler JT, Bennewith KL, Nicolau M, Dornhofer N, Kong C, LeQT, Chi JT, Jeffrey SS, Giaccia AJ (2006) Lysyl oxidase isessential for hypoxia-induced metastasis. Nature 440:1222–1226
46. Petrella BL, Lohi J, Brinckerhoff CE (2005) Identification ofmembrane type-1 matrix metalloproteinase as a target of hypoxia-inducible factor-2 alpha in von Hippel-Lindau renal cell carcino-ma. Oncogene 24:1043–1052
47. Chan DA, Giaccia AJ (2007) Hypoxia, gene expression, andmetastasis. Cancer Metastasis Rev 26:333–339
48. Larson SM (2004) Positron emission tomography-based molecularimaging in human cancer: exploring the link between hypoxia andaccelerated glucose metabolism. Clin Cancer Res 10:2203–2204
49. Cherk MH, Foo SS, Poon AM, Knight SR, Murone C, PapenfussAT, Sachinidis JI, Saunder TH, O, Keefe GJ, Scott AM (2006)Lack of correlation of hypoxic cell fraction and angiogenesis withglucose metabolic rate in non-small cell lung cancer assessed by18F-Fluoromisonidazole and 18F-FDG PET. J Nucl Med47:1921–1926
50. Rajendran JG, Mankoff DA, O, Sullivan F, Peterson LM,Schwartz DL, Conrad EU, Spence AM, Muzi M, Farwell DG,Krohn KA (2004) Hypoxia and glucose metabolism in malignanttumors: evaluation by [18F]fluoromisonidazole and [18F]fluoro-deoxyglucose positron emission tomography imaging. ClinCancer Res 10:2245–2252
51. KaelinWG Jr (2007) The von Hippel-Lindau tumor suppressor proteinand clear cell renal carcinoma. Clin Cancer Res 13:680s–684s
52. Trastour C, Benizri E, Ettore F, Ramaioli A, Chamorey E,Pouyssegur J, Berra E (2007) HIF-1alpha and CA IX staining ininvasive breast carcinomas: prognosis and treatment outcome. IntJ Cancer 120:1451–1458
53. Van den Eynden GG, Van der Auwera I, Van Laere SJ, ColpaertCG, Turley H, Harris AL, van Dam P, Dirix LY, Vermeulen PB,Van Marck EA (2005) Angiogenesis and hypoxia in lymph nodemetastases is predicted by the angiogenesis and hypoxia in theprimary tumour in patients with breast cancer. Br J Cancer93:1128–1136
54. Hussain SA, Ganesan R, Reynolds G, Gross L, Stevens A,Pastorek J, Murray PG, Perunovic B, Anwar MS, Billingham L,James ND, Spooner D, Poole CJ, Rea DW, Palmer DH (2007)Hypoxia-regulated carbonic anhydrase IX expression is associatedwith poor survival in patients with invasive breast cancer. Br JCancer 96:104–109
55. Tan EY, Campo L, Han C, Turley H, Pezzella F, Gatter KC, HarrisAL, Fox SB (2007) BNIP3 as a progression marker in primaryhuman breast cancer; opposing functions in in situ versus invasivecancer. Clin Cancer Res 13:467–474
56. Giatromanolaki A, Koukourakis MI, Sowter HM, Sivridis E,Gibson S, Gatter KC, Harris AL (2004) BNIP3 expression islinked with hypoxia-regulated protein expression and with poorprognosis in non-small cell lung cancer. Clin Cancer Res10:5566–5571
57. Verheul HM, Pinedo HM (2007) Possible molecular mechanismsinvolved in the toxicity of angiogenesis inhibition. Nat RevCancer 7:475–485
58. Melillo G (2007) Targeting hypoxia cell signaling for cancertherapy. Cancer Metastasis Rev 26:341–352
59. Pelicano H, Martin DS, Xu RH, Huang P (2006) Glycolysisinhibition for anticancer treatment. Oncogene 25:4633–4646
60. Thiry A, Dogne JM, Masereel B, Supuran CT (2006) Targetingtumor-associated carbonic anhydrase IX in cancer therapy. TrendsPharmacol Sci 27:566–573
61. Izumi H, Torigoe T, Ishiguchi H, Uramoto H, Yoshida Y, TanabeM, Ise T, Murakami T, Yoshida T, Nomoto M, Kohno K (2003)Cellular pH regulators: potentially promising molecular targets forcancer chemotherapy. Cancer Treat Rev 29:541–459
62. Gerweck LE, Vijayappa S, Kozin S (2006) Tumor pH controls thein vivo efficacy of weak acid and base chemotherapeutics. MolCancer Ther 5:1275–1279
J Mol Med (2007) 85:1301–1307 1307

REVIEW
Keeping the engine primed: HIF factors as key regulatorsof cardiac metabolism and angiogenesis during ischemia
Ralph V. Shohet & Joseph A. Garcia
Received: 1 October 2007 /Revised: 22 October 2007 /Accepted: 23 October 2007 / Published online: 20 November 2007# Springer-Verlag 2007
Abstract Myocardial ischemia, the most common cause ofcardiac hypoxia in clinical medicine, occurs when oxygendelivery cannot meet myocardial metabolic requirements inthe heart. This deficiency can result from either a reducedsupply of oxygen (decreased coronary bloodflow) or anincreased myocardial demand for oxygen (increased wallstress or afterload). Patients with stable coronary arterydisease as well as patients experiencing acute myocardialinfarction can experience episodes of severe ischemia.Although hypoxia is an obligatory component, it is notthe sole environmental stress experienced by the ischemicheart. Reperfusion after ischemia is associated with in-creased oxidative stress as the heart reverts to aerobicrespiration and thereby generates toxic levels of reactiveoxygen species (ROS). During mild ischemia, mitochon-drial function is partially compromised and substratepreferences adapt to sustain adequate ATP generation. Withsevere ischemia, mitochondrial function is markedly com-promised and anaerobic metabolism must provide energyno matter what the cost in generation of toxic ROS adducts.Ischemia produces a variety of environmental stresses thatimpair cardiovascular function. As a result, multiplesignaling pathways are activated in mammalian cells during
ischemia/reperfusion injury in an attempt to minimize cellularinjury and maintain cardiac output. Amongst the transcrip-tional regulators activated are members of the hypoxiainducible factor (HIF) transcription factor family. HIF factorsregulate a variety of genes that affect a myriad of cellularprocesses including metabolism, angiogenesis, cell survival,and oxygen delivery, all of which are important in the heart. Inthis review, we will focus on the metabolic and angiogenicaspects of HIF biology as they relate to the heart duringischemia. We will review the metabolic requirements of theheart under normal as well as hypoxic conditions, the effectsof preconditioning and its regulation as it pertains to HIFbiology, the apparent roles of HIF-1 and HIF-2 in intermediarymetabolism, and translational applications of HIF-1 and HIF-2biology to cardiac angiogenesis. Increased understanding ofthe role of HIFs in cardiac ischemia will ultimately influenceclinical cardiovascular practice.
Keywords HIF. Hypoxia . Heart . Ischemia .
Angiogenesis . Metabolism
Myocardial fuel choice and oxygen supply
A remarkable feature of the heart, one of the mostmetabolically active organs in the body, is its ability touse a wide variety of fuel substrates in aerobic respirationfor energy production. Oxygen, delivered in blood throughthe coronary arteries, is efficiently extracted by the heart forgeneration of reducing equivalents by mitochondria, focalpoints for fatty acid or pyruvate oxidation, and for ketonebody utilization [1]. Fuel choice in the adult heart is nothomogenous under all conditions, but instead is highlydependent upon substrate availability as well as tissueoxygenation [2]. The adult heart preferentially uses fatty
J Mol Med (2007) 85:1309–1315DOI 10.1007/s00109-007-0279-x
R. V. ShohetJohn A. Burns School of Medicine,Center for Cardiovascular Research, University of Hawaii,651 Ilalo St.,Honolulu, HI 96813, USAe-mail: [email protected]
J. A. Garcia (*)Department of Internal Medicine, Molecular Cardiology Division,University of Texas Southwestern Medical Center at Dallas,5323 Harry Hines Blvd.,Dallas, TX 75390-8573, USAe-mail: [email protected]

acids during times of adequate oxygen availability [2, 3].This preference changes to glucose utilization via pyruvateoxidation in mild ischemia, if glucose is available, and toglycolysis during severe ischemia.
Aerobic respiration is an efficient means for generatingenergy, but it comes at a price. Reactive oxygen species(ROS) are generated under physiological conditions withthe primary source being the mitochondrial electrontransport chain. If left unchecked, elevated ROS lead tocumulative cellular damage induced by oxidative stress. ROSlevels are markedly elevated during ischemia/reperfusioninjury and perhaps during ischemia or hypoxia itself [4].Following reperfusion, a naive heart experiences a profoundincrease in oxidative stress [5] and reduced aerobic energyproduction [6]. The mitochondria are both the major source[7] and the most affected subcellular component of ROSgenerated during ischemia/reperfusion [8, 9]. However, ROSalso have a role in normal physiological processes, includingcell growth and differentiation, vascular tone, and cardiacgrowth, due to signal transduction pathways activated byROS [10, 11]. Hence, ROS homeostasis is essential forproper functioning of cardiac myocytes and other cells typesin the basal as well as stressed state.
Ischemia/reperfusion and preconditioning
A protective response by the heart and other organs tosublethal levels of hypoxia or ischemia, known as pre-conditioning, results in the induction of adaptive physio-logical processes. This process is relevant not only tocoronary artery patients experiencing repetitive ischemiadue to coronary artery vasospasm or subocclusions, but alsoto diabetic patients with microvascular heart disease as wellas to hypertensive and cardiomyopathic heart diseasepatients with increased myocardial wall stress and conse-quently greater oxygen demand. Ischemic preconditioninghas an immediate as well as a delayed component [12, 13].The immediate preconditioning response occurs withinminutes to hours [14] and is mediated by ion channels aswell as by signaling molecules produced during ischemia[15]. The delayed preconditioning response, a transcrip-tional response lasting from hours to days, is conferred byde novo synthesized cellular factors [16].
The protective cellular processes induced by delayedpreconditioning have been well studied and are aimed atoptimizing oxygen delivery, intermediary metabolism, andpreserving mitochondrial function. However, less is knownabout the regulatory network that confers delayed precon-ditioning [17]. With reperfusion or reoxygenation, as occursduring preconditioning, ROS levels increase and redox-sensitive transcription factors are activated. Being redox-
sensitive transcription factors, HIF members are poised toexert significant control over the protective cellular re-sponse generated during delayed preconditioning. Oneprotective response induced during the initial phase ofdelayed preconditioning is a shift from aerobic to glycolyticmetabolism. For the severely ischemic heart, this isbeneficial in the short-term, but is insufficient to meet itslong-term needs.
To meet the long-term challenges during prolongedischemia, the heart induces several protective effects aimedat restoring aerobic respiration. These effects includeincreased angiogenesis in an attempt to restore blooddelivery to the ischemic heart as well as augmentation ofmitochondrial respiration and mitochondrial biogenesis tomaximize energy production from the available oxygencontent [12]. Perhaps in anticipation of successfullyrestoring oxygen delivery to the hypoxic tissue, theischemic heart also induces expression of endogenouscytoprotective cellular factors including antioxidantenzymes (AOE) that eliminate ROS in the mitochondriaand other subcellular compartments [18]. Hence, a keytarget for preconditioning is the mitochondria [19], a centralorganelle with multiple biological roles in addition toenergy generation [20]. Regulatory factors implicated inmitochondrial biogenesis have been identified [21]. As willbe discussed, HIF members have been implicated inregulating the angiogenic and metabolic response tochronic ischemia. By contrast, the transcriptional regulationof the endogenous cytoprotective response remains poorlyunderstood, although it is plausible that HIF members arelikewise involved in regulation of this protective response.
Preconditioning and transcriptional regulationof intermediary metabolism
Changes in cardiac fuel substrate preference during ische-mia have been delineated, but our knowledge of howsubstrate utilization is determined at the transcriptionallevel during chronic ischemia is sparse. The most well-studied regulator of cardiac intermediary metabolism isPPARα, the transcriptional factor controlling expression ofproteins involved in fatty acid uptake, transport, derivation,and oxidation [22]. PPARα signaling is impaired duringhypoxia in neonatal cardiomyocytes as well as in hearts[23, 24], consistent with the observation that substratepreference shifts from fatty acid to glucose utilizationduring myocardial ischemia [25]. With respect to othermitochondrial substrates, our understanding of the regula-tion of factors involved in ketone body utilization islimited, despite its use during nutrient stress. Control ofglucose use during oxygen availability is also not under-stood. By contrast, the transcriptional regulator of anaerobic
1310 J Mol Med (2007) 85:1309–1315

glycolytic metabolism has been identified as HIF-1, aheterodimer comprised of HIF-1 alpha (HIF-1α) conferringbiological specificity and HIF-1 beta (HIF-1β) required forbiological activity [26]. HIF members are transcriptionalregulators of genes involved in hypoxic and other stressresponses (Fig. 1) [27, 28]. With completion of the humangenome project, a second HIF alpha member closely relatedto HIF-1α in composition and regulation was identified,Endothelial PAS domain protein 1 (EPAS1), encoding HIF-2α [29]. Although a wealth of data has been generatedabout HIF-1 over the past decade, the founding member ofthe HIF family, less is known about HIF-2. Nevertheless,distinct and, in some cases, complementary roles areemerging with respect to HIF-1 and HIF-2.
Biological roles for HIF-1 and HIF-2 in intermediarymetabolism
The role of HIF-1 appears to be the most important in theearly phase after exposure to stress where a transition fromaerobic to anaerobic metabolism is essential for cellsurvival. HIF-1 controls expression of cellular factorsinvolved in glucose metabolism which allows cells to shiftfrom aerobic metabolism to anaerobic glycolysis [30], arole analogous to PPARα and its control of fatty acidmetabolism. Elimination of HIF-1α results in a mutedglycolytic response to hypoxia [30], whereas the loss ofHIF-2α has no effect on glycolysis [31], consistent with aselective role for HIF-1α in control of glycolytic enzymegene expression. HIF-1 also affects mitochondrial-dependentmetabolism by at least three mechanisms. First, HIF-1 induces
Pdk1 encoding pyruvate dehydrogenase kinase 1 [32, 33], anegative regulator of the pyruvate dehydrogenase complex(PDH). PDH is the nexus for pyruvate entry into themitochondrial oxidation pathway. Thus, increases in Pdk1levels results in inhibition of PDH activity, reduced entry ofpyruvate into mitochondria, and a subsequent reduction ofmitochondrial respiration. Second, HIF-1 inhibits mitochon-drial respiration by altering composition of the cytochromeoxidase complex [34]. HIF-1 induces expression of COX4–2and LON, with the net result being more efficient mitochon-drial respiration during times of oxygen deficit. Third, HIF-1acts in conjunction with c-myc to induce expression of HKII[35], a glycolytic enzyme that shifts glucose away frommitochondrial utilization and also has antioxidant effects[36].
HIF-2 appears to regulate processes that are important inmore long-term adaptive or anticipatory responses. Thelatter include the desired, but potentially perilous, transitionback to an oxygenated state. HIF-2 functions to maintainmitochondrial homeostasis by regulating production ofcellular factors that alleviate oxidative stress [37, 38].HIF-2α null mice exhibit multiple organ pathology resem-bling a mitochondrial disease state as well as abnormal livermitochondrial function [37, 38]. The biochemical basis forthe HIF-2α null phenotype in liver involves increasedoxidative stress due to reduced expression of antioxidantenzyme (AOE) genes including Sod2 [38], encoding anessential modulator of mitochondrial oxidative stress [39,40], and Frataxin [37], encoding the oxidative stress-regulated chaperone protein for mitochondrial aconitase.Thus, whereas HIF-1 is a pathway regulator of genesencoding glycolytic enzymes, HIF-2 regulates productionof factors important for maintaining mitochondrial homeo-stasis. Whether these findings for HIF-2α in the liver holdtrue for the heart is unknown.
Biological roles for HIF-1 and HIF-2 in cardiacangiogenesis
Hypoxia and HIF factors have been implicated as masterregulators of cardiovascular development [41, 42]. Al-though HIF-1 and HIF-2 may have overlapping transcrip-tional regulation of proangiogenic genes, transgenic mousestudies support specific activities for HIF-1 and HIF-2 invascular development that includes stage-, cell-, and tissue-specific roles. Global HIF-1α knockout mice have abnor-mal vascular as well as cardiac development [43, 44]. Incomparison, global HIF-2α knockout embryos have moresubtle vascular defects [45]. A dominant negative form ofHIF-1α that interferes with both HIF-1 and HIF-2 signalingimpairs vascular development in the embryo whenexpressed in vascular endothelial cells [46]. Cardiomyocyte-
Fig. 1 Alignment of HIF-1α, HIF-2α, and HIF-3α. Homology(percent identity) comparisons of the conserved basic helix-loop-helix(bHLH) and PAS-A,B repeats located within the PAS domain (PAS).Also indicated are the conserved amino-terminal activation domain(NTAD) located within the oxygen-dependent degradation domain(ODD) and the carboxy-terminal activation domain (CTAD) region.HIF-1α and HIF-2α have similar structural and regulatory featureswhereas spliced variants of HIF-3α contain none or one (not shown)of the activation domains. The unique regions (UR) may conferspecific determinants of HIF-1α and HIF-2α activation
J Mol Med (2007) 85:1309–1315 1311

specific HIF-1α knockout mice have lower capillarydensities and reduced expression of proangiogenic factors[47]; it has not been reported whether endothelial cell-specific HIF-1α knockout mice have any cardiac vascularphenotype [48]. Restoration of HIF-2α expression inendothelial cells of global HIF-2α knockout mice does notfully rescue the HIF-2α null vascular phenotype [49],suggesting that HIF-2α expression in other cell types maybe required for normal vascular development.
Translational experiments support potential therapeuticroles for HIF-1 and HIF-2 in cardiac angiogenesis. In cellculture models, HIF-1α or HIF-2α over-expression resultsin increased gene expression of a variety of proangiogenicfactors in macrophages [50], cardiomyocytes [51], andvascular endothelial cells [52–55], cell types relevant to theischemic and infarcted myocardium. Transgenic mice over-expressing HIF-1α in the heart and subjected to myocardialinfarction have increased capillary density in the infarct andperi-infarct zones [56]. Gene delivery of constitutivelyactive HIF-1α in a rat myocardial infarct model reducesinfarct size and increases neoangiogenesis in the peri-infarctzone [57]. Knockout mice lacking the gene encoding theHIF prolyl hydroxylase PHD2, the enzyme targeting HIFalpha proteins for degradation during normoxia, haveelevated levels of HIF-1α, increased number of maturemedium-sized vessels, and enlarged capillaries in thesubendocardial region [58]. A potential role for HIF-1 incardiac vessel formation in human hearts is supported bythe finding that a HIF-1α polymorphism is associated withreduced coronary artery collateral formation, although themechanism behind this observation remains to be determined[59].
Relevance of HIF factors to cardiac ischemia/reperfusion injury
Environmental conditions present in ischemia/reperfusionare of direct relevance to HIF biology. HIF proteins areactivated by oxidative stress [60–63]. HIF proteins areincreased in the peri-infarct area after myocardial infarctionin rats [64] and humans [65–67] with HIF-2α expressionoccurring in remote areas from the infarct [64] suggesting abroader role for HIF-2 in ischemia/reperfusion biology.HIF-2α has several unique aspects pertinent to oxidativestress and ischemia/reperfusion biology. DNA bindingactivity of HIF-2α, but not HIF-1α, may be differentiallyregulated by redox conditions [68]. As mentioned previ-ously, HIF-2α in vivo regulates major AOE and Frataxingene expression in the liver [37, 38], cellular factorsintimately involved in ROS and mitochondrial homeostasisin the heart [69]. More recently, studies with a HIF-2αknockdown model identified a role for HIF-2 in protection
against ischemia/reperfusion injury in the kidney ascribedto HIF-2 regulation of major AOE gene expression [70],confirming the earlier findings of HIF-2 regulation of AOEgene expression.
Although it has been recognized for a decade that HIFtranscription factors are activated by environmental stress,the role of HIF members in cardiac ischemic injury remainsunknown. Stabilization of HIF members by proteins thatmodulate HIF stability [71] or by siRNA directed againstPHD2 [72] provides protection against ischemia-induceddamage. Over-expression of constitutively active HIF-1 inrat cardiomyocytes confers resistance against ischemia/reperfusion injury in a cell culture model [73]. HIF-1over-expression in mice reduces infarct size and results inimproved cardiac function after myocardial infarction [56].Yet whether endogenous HIF member(s) confer thisprotective response during preconditioning is unknown.Mice partially deficient in HIF-1 have increased suscepti-bility to cardiac ischemia/reperfusion injury after wholeanimal hypoxia exposure [74], but this has been attributedto impaired induction of renal erythropoietin. Additionalresearch will be needed to identify which HIF member(s)are important in the cardiac preconditioning response andwhether HIF factors play an active role locally in the heart.
Conclusion and future perspectives
Cardiovascular diseases are leading causes of morbidity andmortality in the USA and western world. In the USA, acuteand chronic treatments of cardiovascular disease statesaccounts for a substantial portion of USA healthcareexpenditures. While conditions leading to myocardialinjury have been well studied, endogenous protectiveresponses that preserve cellular and organelle function,particularly mitochondria, during ischemia are poorlyunderstood and thus are not targeted in current therapeuticstrategies. The roles for HIF-1 and HIF-2 in myocardialischemia are currently a largely undefined area of HIFbiology. HIF-1 likely regulates glucose utilization in theheart during oxygen deprivation and may play a critical rolein regulation of the angiogenic response after myocardialinjury. HIF-2 has a complementary role to HIF-1 inregulation of intermediary metabolism in the liver, althoughits role in the heart remains to be defined, and may also beimportant in the angiogenic response of the heart. A clearerpicture of the roles of HIF-1 and HIF-2 in cardiac biologywill emerge with active investigation. If HIF factors proveto be essential factors that orchestrate protective cellularresponses to cardiac ischemia, then studies of HIF signalingin the heart may lead to improved prevention or treatmentof cardiovascular diseases using focused drug discoveryapproaches.
1312 J Mol Med (2007) 85:1309–1315

Acknowledgement We gratefully acknowledge funding supportfrom Amgen, United Mitochondrial Disease Foundation, March ofDimes (6-FY06–319), American Heart Association/Texas Affiliate(0465047Y), and National Institutes of Health (HL080532, HL073449,RR16453, AR050597–01A1, 1P50MH66172).
References
1. Taegtmeyer H (2000) Metabolism–the lost child of cardiology. JAm Coll Cardiol 36:1386–1388
2. Neely JR, Rovetto MJ, Oram JF (1972) Myocardial utilization ofcarbohydrate and lipids. Prog Cardiovasc Dis 15:289–329
3. Nieth H, Schollmeyer P (1966) Substrate-utilization of the humankidney. Nature 209:1244–1245
4. Goswami SK, Maulik N, Das DK (2007) Ischemia-reperfusionand cardioprotection: a delicate balance between reactive oxygenspecies generation and redox homeostasis. Ann Med 39:275–289
5. Ferrari R, Alfieri O, Curello S, Ceconi C, Cargnoni A, Marzollo P,Pardini A, Caradonna E, Visioli O (1990) Occurrence of oxidativestress during reperfusion of the human heart. Circulation 81:201–211
6. Ferreira R, Llesuy S, Milei J, Scordo D, Hourquebie H, MolteniL, de Palma C, Boveris A (1988) Assessment of myocardialoxidative stress in patients after myocardial revascularization. AmHeart J 115:307–312
7. Das DK, George A, Liu XK, Rao PS (1989) Detection ofhydroxyl radical in the mitochondria of ischemic-reperfusedmyocardium by trapping with salicylate. Biochem Biophys ResCommun 165:1004–1009
8. Sadek HA, Nulton-Persson AC, Szweda PA, Szweda LI (2003)Cardiac ischemia/reperfusion, aging, and redox-dependent alter-ations in mitochondrial function. Arch Biochem Biophys420:201–208
9. Ambrosio G, Zweier JL, Flaherty JT (1991) The relationshipbetween oxygen radical generation and impairment of myocardialenergy metabolism following post-ischemic reperfusion. J MolCell Cardiol 23:1359–1374
10. Soberman RJ (2003) The expanding network of redox signaling:new observations, complexities, and perspectives. J Clin Invest111:571–574
11. Sen CK, Packer L (1996) Antioxidant and redox regulation ofgene transcription. Faseb J 10:709–720
12. McLeod CJ, Pagel I, Sack MN (2005) The mitochondrialbiogenesis regulatory program in cardiac adaptation to ischemia–aputative target for therapeutic intervention. Trends Cardiovasc Med15:118–123
13. Arstall MA, Zhao YZ, Hornberger L, Kennedy SP, Buchholz RA,Osathanondh R, Kelly RA (1998) Human ventricular myocytes invitro exhibit both early and delayed preconditioning responses tosimulated ischemia. J Mol Cell Cardiol 30:1019–1025
14. Yellon DM, Baxter GF (1995) A “second window of protection”or delayed preconditioning phenomenon: future horizons formyocardial protection? J Mol Cell Cardiol 27:1023–1034
15. Murry CE, Jennings RB, Reimer KA (1986) Preconditioning withischemia: a delay of lethal cell injury in ischemic myocardium.Circulation 74:1124–1136
16. Das DK, Moraru II, Maulik N, Engelman RM (1994) Geneexpression during myocardial adaptation to ischemia and reperfu-sion. Ann N Y Acad Sci 723:292–307
17. Kodde IF, van der Stok J, Smolenski RT, de Jong JW (2007)Metabolic and genetic regulation of cardiac energy substratepreference. Comp Biochem Physiol AMol Integr Physiol 146:26–39
18. Marczin N, El-Habashi N, Hoare GS, Bundy RE, Yacoub M(2003) Antioxidants in myocardial ischemia-reperfusion injury:
therapeutic potential and basic mechanisms. Arch BiochemBiophys 420:222–236
19. Halestrap AP, Clarke SJ, Khaliulin I (2007) The role ofmitochondria in protection of the heart by preconditioning.Biochim Biophys Acta 1767:1007–1031
20. Marin-Garcia J, Goldenthal MJ (2004) Heart mitochondriasignaling pathways: appraisal of an emerging field. J Mol Med82:565–578
21. Das DK, Maulik N, Sato M, Ray PS (1999) Reactive oxygenspecies function as second messenger during ischemic precondi-tioning of heart. Mol Cell Biochem 196:59–67
22. Watanabe K, Fujii H, Takahashi T, Kodama M, Aizawa Y, Ohta Y,Ono T, Hasegawa G, Naito M, Nakajima T, Kamijo Y, GonzalezFJ, Aoyama T (2000) Constitutive regulation of cardiac fatty acidmetabolism through peroxisome proliferator-activated receptoralpha associated with age-dependent cardiac toxicity. J Biol Chem275:22293–22299
23. Huss JM, Levy FH, Kelly DP (2001) Hypoxia inhibits theperoxisome proliferator-activated receptor alpha/retinoid X recep-tor gene regulatory pathway in cardiac myocytes: a mechanism forO2-dependent modulation of mitochondrial fatty acid oxidation. JBiol Chem 276:27605–27612
24. Razeghi P, Young ME, Abbasi S, Taegtmeyer H (2001) Hypoxiain vivo decreases peroxisome proliferator-activated receptoralpha-regulated gene expression in rat heart. Biochem BiophysRes Commun 287:5–10
25. Bolukoglu H, Goodwin GW, Guthrie PH, Carmical SG, ChenTM, Taegtmeyer H (1996) Metabolic fate of glucose in reversiblelow-flow ischemia of the isolated working rat heart. Am J Physiol270:H817–H826
26. Wang GL, Jiang BH, Rue EA, Semenza GL (1995) Hypoxia-inducible factor 1 is a basic-helix-loop-helix-PAS heterodimerregulated by cellular O2 tension. Proc Natl Acad Sci USA92:5510–5514
27. Semenza GL (2001) Hypoxia-inducible factor 1: oxygen homeo-stasis and disease pathophysiology. Trends in Molecular Medicine7:345–350
28. Semenza GL (2000) HIF-1 and human disease: one highlyinvolved factor. Genes & Development 14:1983–1991
29. Tian SL, McKnight SL, Russell DW (1997) Endothelial PASdomain protein 1 (EPAS1), a transcription factor selectivelyexpressed in endothelial cells. Genes Dev 11:72–82
30. Seagroves TN, Ryan HE, Lu H, Wouters BG, Knapp M, ThibaultP, Laderoute K, Johnson RS (2001) Transcription factor HIF-1 is anecessary mediator of the pasteur effect in mammalian cells. MolCell Biol 21:3436–3444
31. Hu CJ, Wang LY, Chodosh LA, Keith B, Simon MC (2003) Dif-ferential roles of hypoxia-inducible factor 1alpha (HIF-1alpha) andHIF-2alpha in hypoxic gene regulation. Mol Cell Biol 23:9361–9374
32. Kim JW, Tchernyshyov I, Semenza GL, Dang CV (2006) HIF-1-mediated expression of pyruvate dehydrogenase kinase: a meta-bolic switch required for cellular adaptation to hypoxia. CellMetab 3:177–185
33. Papandreou I, Cairns RA, Fontana L, Lim AL, Denko NC (2006)HIF-1 mediates adaptation to hypoxia by actively downregulatingmitochondrial oxygen consumption. Cell Metab 3:187–197
34. Fukuda R, Zhang H, Kim JW, Shimoda L, Dang CV, Semenza GL(2007) HIF-1 regulates cytochrome oxidase subunits to optimizeefficiency of respiration in hypoxic cells. Cell 129:111–122
35. Kim JW, Gao P, Liu YC, Semenza GL, Dang CV (2007) HIF-1and dysregulated c-Myc cooperatively induces VEGF andmetabolic switches, HK2 and PDK1. Mol Cell Biol 27:7381–7393
36. Ahmad A, Ahmad S, Schneider BK, Allen CB, Chang LY, WhiteCW (2002) Elevated expression of hexokinase II protects humanlung epithelial-like A549 cells against oxidative injury. Am JPhysiol Lung Cell Mol Physiol 283:L573–L584
J Mol Med (2007) 85:1309–1315 1313

37. Oktay Y, Dioum E, Matsuzaki S, Ding K, Yan LJ, Haller RG,Szweda LI, Garcia JA (2007) Hypoxia-inducible factor 2alpharegulates expression of the mitochondrial aconitase chaperoneprotein frataxin. J Biol Chem 282:11750–11756
38. Scortegagna M, Ding K, Oktay Y, Gaur A, Thurmond F, Yan LJ,Marck BT, Matsumoto AM, Shelton JM, Richardson RA, BennettMJ, Garcia JA (2003) Multiple organ pathology, metabolicabnormalities and impaired homeostasis of reactive oxygenspecies in Epas1-/- mice. Nat Genet 35:331–340
39. Harris ED (1992) Regulation of antioxidant enzymes. Faseb J6:2675–2683
40. Rabilloud T, Heller M, Rigobello MP, Bindoli A, Aebersold CW,Lunardi J (2001) The mitochondrial antioxidant defence systemand its response to oxidative stress. Proteomics 1:1105–1110
41. Lee YM, Jeong CH, Koo SY, Son MJ, Song HS, Bae SK, RaleighJA, Chung HY, Yoo MA, Kim KW (2001) Determination ofhypoxic region by hypoxia marker in developing mouse embryosin vivo: a possible signal for vessel development. Dev Dyn220:175–186
42. Wikenheiser J, Doughman YQ, Fisher SA, Watanabe M (2006)Differential levels of tissue hypoxia in the developing chickenheart. Dev Dyn 235:115–123
43. Iyer NV, Kotch LE, Agani F, Leung SW, Laughner E, WengerRH, Gassmann M, Gearhart JD, Lawler AM, Yu AY, Semenza GL(1998) Cellular and developmental control of O2 homeostasis byhypoxia-inducible factor 1 alpha. Genes Dev 12:149–162
44. Compernolle V, Brusselmans K, Franco D, Moorman A, DewerchinM, Collen D, Carmeliet P (2003) Cardia bifida, defective heartdevelopment and abnormal neural crest migration in embryos lackinghypoxia-inducible factor-1alpha. Cardiovasc Res 60:569–579
45. Peng J, Zhang L, Drysdale L, Fong GH (2000) The transcriptionfactor EPAS-1/hypoxia-inducible factor 2alpha plays an importantrole in vascular remodeling. Proc Natl Acad Sci USA 97:8386–8391
46. Licht AH, Muller-Holtkamp F, Flamme I, Breier G (2006) Inhibitionof hypoxia-inducible factor activity in endothelial cells disruptsembryonic cardiovascular development. Blood 107:584–590
47. Huang Y, Hickey RP, Yeh JL, Liu D, Dadak A, Young LH, JohnsonRS, Giordano FJ (2004) Cardiac myocyte-specific HIF-1alphadeletion alters vascularization, energy availability, calcium flux, andcontractility in the normoxic heart. Faseb J 18:1138–1140
48. Tang N, Wang L, Esko J, Giordano FJ, Huang Y, Gerber HP,Ferrara N, Johnson RS (2004) Loss of HIF-1alpha in endothelialcells disrupts a hypoxia-driven VEGF autocrine loop necessary fortumorigenesis. Cancer Cell 6:485–495
49. Duan LJ, Zhang-Benoit Y, Fong GH (2005) Endothelium-intrinsicrequirement for Hif-2alpha during vascular development. Circulation111:2227–2232
50. White JR, Harris RA, Lee SR, Craigon MH, Binley K, Price T,Beard JL, Mundy CR, Naylor S (2004) Genetic amplification ofthe transcriptional response to hypoxia as a novel means ofidentifying regulators of angiogenesis. Genomics 83:1–8
51. Jiang C, Lu H, Vincent KA, Shankara S, Belanger AJ, Cheng SH,Akita GY, Kelly RA, Goldberg AM, Gregory RJ (2002) Geneexpression profiles in human cardiac cells subjected to hypoxia orexpressing a hybrid form of HIF-1 alpha. Physiol Genomics 8:23–32
52. Takeda N, Maemura K, Imai Y, Harada T, Kawanami D, Nojiri T,Manabe I, Nagai R (2004) Endothelial PAS domain protein 1 genepromotes angiogenesis through the transactivation of bothvascular endothelial growth factor and its receptor, Flt-1. CircRes 95:146–153
53. Kelly BD, Hackett SF, Hirota K, Oshima Y, Cai Z, Berg-Dixon S,Rowan A, Yan Z, Campochiaro ZA, Semenza GL (2003) Celltype-specific regulation of angiogenic growth factor gene expres-sion and induction of angiogenesis in nonischemic tissue by a
constitutively active form of hypoxia-inducible factor 1. Circ Res93:1074–1081
54. Manalo DJ, Rowan A, Lavoie T, Natarajan L, Kelly BD, Ye SQ,Garcia JG, Semenza GL (2005) Transcriptional regulation ofvascular endothelial cell responses to hypoxia by HIF-1. Blood105:659–669
55. Yamakawa M, Liu LX, Date T, Belanger AJ, Vincent KA, AkitaGY, Kuriyama T, Cheng SH, Gregory RJ, Jiang C (2003)Hypoxia-inducible factor-1 mediates activation of cultured vascularendothelial cells by inducing multiple angiogenic factors. Circ Res93:664–673
56. Kido M, Du L, Sullivan CC, Li X, Deutsch R, Jamieson SW,Thistlethwaite PA (2005) Hypoxia-inducible factor 1-alphareduces infarction and attenuates progression of cardiac dysfunc-tion after myocardial infarction in the mouse. J Am Coll Cardiol46:2116–2124
57. Shyu KG, Wang MT, Wang BW, Chang CC, Leu JG, Kuan P,Chang H (2002) Intramyocardial injection of naked DNAencoding HIF-1alpha/VP16 hybrid to enhance angiogenesis inan acute myocardial infarction model in the rat. Cardiovasc Res54:576–583
58. Takeda K, Cowan A, Fong GH (2007) Essential role for prolylhydroxylase domain protein 2 in oxygen homeostasis of the adultvascular system. Circulation 116:774–781
59. Resar JR, Roguin A, Voner J, Nasir K, Hennebry TA, Miller JM,Ingersoll R, Kasch LM, Semenza GL (2005) Hypoxia-induciblefactor 1alpha polymorphism and coronary collaterals in patientswith ischemic heart disease. Chest 128:787–791
60. Chandel NS, McClintock DS, Feliciano CE, Wood TM, MelendezJA, Rodriguez AM, Schumacker PT (2000) Reactive oxygenspecies generated at mitochondrial complex III stabilize hypoxia-inducible factor-1alpha during hypoxia: a mechanism of O2sensing. J Biol Chem 275:25130–25138
61. Haddad JJ, Land SC (2001) A non-hypoxic, ROS-sensitivepathway mediates TNF-alpha-dependent regulation of HIF-1alpha.FEBS Lett 505:269–274
62. Huang LE, Arany Z, Livingston DM, Bunn HF (1996) Activationof hypoxia-inducible transcription factor depends primarily uponredox-sensitive stabilization of its alpha subunit. J Biol Chem271:32253–32259
63. Wang GL, Jiang BH, Semenza GL (1995) Effect of altered redoxstates on expression and DNA-binding activity of hypoxia-inducible factor 1. Biochem Biophys Res Commun 212:550–556
64. Jurgensen JS, Rosenberger S, Wiesener MS, Warnecke C,Horstrup JH, Grafe M, Philipp S, Griethe W, Maxwell PH, FreiU, Bachmann S, Willenbrock R, Eckardt KU (2004) Persistentinduction of HIF-1alpha and -2alpha in cardiomyocytes andstromal cells of ischemic myocardium. Faseb J 18:1415–1417
65. Blanco Pampin J, Garcia Rivero SA, Otero Cepeda XL, VazquezBoquete A, Forteza Vila J, Hinojal Fonseca R (2006) Immuno-histochemical expression of HIF-1alpha in response to earlymyocardial ischemia. J Forensic Sci 51:120–124
66. Lee SH, Wolf PL, Escudero R, Deutsch R, Jamieson SW,Thistlethwaite PA (2000) Early expression of angiogenesis factorsin acute myocardial ischemia and infarction. N Engl J Med342:626–633
67. Parisi Q, Biondi-Zoccai GG, Abbate A, Santini D, Vasaturo F,Scarpa S, Bussani R, Leone AM, Petrolini A, Silvestri F, BiasucciLM, Baldi A (2005) Hypoxia inducible factor-1 expressionmediates myocardial response to ischemia late after acutemyocardial infarction. Int J Cardiol 99:337–339
68. Lando D, Pongratz I, Poellinger L, Whitelaw ML (2000) A redoxmechanism controls differential DNA binding activities ofhypoxia-inducible factor (HIF) 1alpha and the HIF-like factor. JBiol Chem 275:4618–4627
1314 J Mol Med (2007) 85:1309–1315

69. Venardos KM, Kaye DM (2007) Myocardial ischemia-reperfusioninjury, antioxidant enzyme systems, and selenium: a review. CurrMed Chem 14:1539–1549
70. Kojima I, Tanaka T, Inagi R, Kato H, Yamashita T, Sakiyama A,Ohneda O, Takeda N, Sata M, Miyata T, Fujita T, Nangaku M(2007) Protective role of hypoxia-inducible factor-2alpha againstischemic damage and oxidative stress in the kidney. J Am SocNephrol 18:1218–1226
71. Muinck ED, Nagy N, Tirziu D, Murakami M, Gurusamy N,Goswami SK, Ghatpande S, Engelman RM, Simons M, Das DK(2007) Protection against myocardial ischemia-reperfusion injuryby the angiogenic Masterswitch protein PR 39 gene therapy: theroles of HIF1alpha stabilization and FGFR1 signaling. AntioxidRedox Signal 9:437–445
72. Natarajan R, Salloum FN, Fisher BJ, Kukreja RC, Fowler AA3rd (2006) Hypoxia inducible factor-1 activation by prolyl 4-hydroxylase-2 gene silencing attenuates myocardial ischemiareperfusion injury. Circ Res 98:133–140
73. Date T, Mochizuki S, Belanger AJ, Yamakawa M, Luo Z,Vincent KA, Cheng SH, Gregory RJ, Jiang C (2005) Expres-sion of constitutively stable hybrid hypoxia-inducible factor-1alpha protects cultured rat cardiomyocytes against simulatedischemia-reperfusion injury. Am J Physiol Cell Physiol 288:C314–C320
74. Cai Z, Manalo DJ, Wei G, Rodriguez ER, Fox-Talbot K, Lu H,Zweier JL, Semenza GL (2003) Hearts from rodents exposed tointermittent hypoxia or erythropoietin are protected againstischemia-reperfusion injury. Circulation 108:79–85
J Mol Med (2007) 85:1309–1315 1315

REVIEW
Hypoxia and chronic lung disease
Rubin M. Tuder & Jeong H. Yun & Anil Bhunia &
Iwona Fijalkowska
Received: 1 October 2007 /Revised: 23 October 2007 /Accepted: 24 October 2007 / Published online: 27 November 2007# Springer-Verlag 2007
Abstract The lung is both the conduit for oxygen uptakeand is also affected by hypoxia and hypoxia signaling.Decreased ventilatory drive, airway obstructive processes,intra-alveolar exudates, septal thickening by edema, inflam-mation, fibrosis, or damage to alveolar capillaries will allinterpose a significant and potentially life-threateningbarrier to proper oxygenation, therefore enhancing thealveolar/arterial pO2 gradient. These processes result indecreased blood and tissue oxygenation. This reviewaddresses the relationship of hypoxia with lung develop-ment and with lung diseases. We particularly focus onmolecular mechanisms underlying hypoxia-driven physio-logical and pathophysiological lung processes, specificallyin the infant lung, pulmonary hypertension, and chronicobstructive pulmonary disease.
Keywords Hypoxia . Lung . Pathology . HIF
Air, containing oxygen at approximately 21% partialpressure at sea level (140–150 mmHg), travels through upto 20 generations of airways by mass flow and then diffusesinto the gas exchange units (alveoli) in the lung with a partialpressure of approximately 105–110 mmHg. The human lungcontains approximately 480 million alveoli, which represent64% of total lung structure. These alveoli are elegantlypacked in only 1.3–2.6 L of total lung volume, providing asurface area of 120–150 m2, equivalent to the dimensions ofa “tennis court” dedicated for gas exchange. Although themolecular determinants of lung size are not known, oxygendiffusion constant and gas exchange surface area are roughlyproportional to body weight and oxygen consumption indifferent species [1]. Physical hyperactivity and exposure toa cold environment or high altitude lead to increased oxygendiffusion capacity, in proportion to enhanced oxygenconsumption [1].
Decreased ventilatory drive, airway obstructive processes,intraalveolar exudates, septal thickening by edema, inflam-mation, fibrosis, or damage to alveolar capillaries will allinterpose a significant and potentially life-threatening barrierto proper oxygenation, therefore enhancing the alveolar/arterial pO2 gradient. This review addresses the contributionof hypoxia to lung diseases and the potential molecularmechanisms involved in hypoxia-driven physiological andpathophysiological lung processes (Fig. 1), particularly inthe infant lung, pulmonary hypertension, and chronicobstructive pulmonary disease. The fundamental conceptsunderlying hypoxia-induced gene expression and the molec-ular regulation of HIF(s) also apply to the lung, and they willbe cited in relation to their demonstrated role in lungphysiology or pathophysiology.
J Mol Med (2007) 85:1317–1324DOI 10.1007/s00109-007-0280-4
R. M. Tuder (*) : J. H. Yun :A. Bhunia : I. FijalkowskaDivision of Cardiopulmonary Pathology,Department of Pathology,Johns Hopkins University School of Medicine,720 Rutland Avenue, Ross Research Building, Room 519,Baltimore, MD 21205, USAe-mail: [email protected]
J. H. Yune-mail: [email protected]
A. Bhuniae-mail: [email protected]
I. Fijalkowskae-mail: [email protected]
R. M. TuderDivision of Pulmonary and Critical Care Medicine,Department of Medicine,Johns Hopkins University School of Medicine,Baltimore, MD, USA

Hypoxia signaling in the lung
Hypoxia-inducible factor-HIF-1α and HIF-2α probablyregulate the expression of most of hypoxia-dependentand many hypoxia-independent genes involved lunghomeostasis and disease. Hypoxia triggers several addi-tional signaling mechanisms, many of which interfacewith HIF-dependent signaling. Under hypoxia, the reduc-tion of energy production has a major negative impact onthe translational rate of proteins, as hypoxia and HIF-1αinhibit mTOR signaling, a critical signaling pathwayinvolved in the induction of cell growth and proteinsynthesis [2].
Recent evidence indicates that hypoxia induces thesynthesis of microRNAs (MIRs), which add additional levelsof complexity in the regulation of gene expression underhypoxia [3, 4]. MIRs, a group of small RNAs withapproximately 22 nucleotides in length, have important rolesin the regulation of gene expression. MIRs posttranscrip-tionally regulate gene expression by forming perfect basepairing with sequences in the 3′ untranslated region (3′UTR)of genes, resulting in enhanced mRNA degradation, whileimperfect matching may lead to repressed or inefficientmRNA translation. More than 500 MIRs have beenidentified in the mammalian genome so far. In a recentsurvey of MIRs induced or downregulated by hypoxia,several of hypoxia MIRs shared HIF-binding sequences inregulatory regions [4]. Of note, some of these MIRs protectagainst apoptosis [4]. A set of MIRs modulate the hypoxicexpression of vascular endothelial growth factor (VEGF)expression and other angiogenic factors [5]. Other studieshave shown that hypoxia-responsive transcription factorssuch as NF-kB and p53 induce MIRs [6]. Although theinvestigation of hypoxic MIRs has been restricted to screen-ings in cell cultures and in silico comparison with tumor datasets [4], the list of MIRs present in the hypoxic lung has notbeen compiled thus far. Nevertheless, the first evidence thatMIRs may participate in lung diseases was provided by the
report that MIR-155 might regulate inflammatory cellresponses, such as in asthma [7].
During hypoxia, EGR-1, a zinc-finger transcriptionfactor expressed in monocytes, leads to the production oftissue factor and fibrin deposition in the pulmonaryvasculature [8]. In mice lung subjected to hypoxia, EGR-1and tissue factor are coproduced in bronchial and vascularsmooth muscle cells and alveolar macrophages [9]. Thus,hypoxia-induced EGR-1 activity accelerates pulmonaryvascular thrombosis.
Hypoxia, lung development and growth, and respiratorydistress syndrome
The lung develops in relative hypoxic conditions in utero asthe fetus is exposed to approximately 25% of ambientoxygen levels [10]. In line with the evidence that the hypoxicfetal environment stimulates embryonic development [11],organogenesis, and organ-specific vascularization [12], theeffect of hypoxia on lung development seems to reside onthe stimulation of branching morphogenesis and the coordi-nated growth and development of a closely integratedpulmonary arterial blood supply. In vitro studies have shownthat fetal oxygen tension enhances epithelial and vascularbranching of mouse lung and maintains lung morphogenesisin rats [13]. Terminal branching of trachea is regulated bylocal oxygen tension, as hypoxia stimulates Bnl FGF, agrowth factor that induces tracheal sprouting, while highoxygen tension suppresses terminal branching [14].
The expression of VEGF, a potent inducer of vasculogenesisin the lung, relies largely on HIF-1/2α [15]. Indeed, humanfetal lung explants cultured at physiological oxygen tensionlevels (i.e., about 40 mmHg) have increased VEGF comparedwith explants cultured at normoxic condition [16, 17]. FetalVEGF is involved in lung development, as inhibition ofVEGF receptor signaling impairs airway and blood vesselbranching in lung explants [18].
Loss of function experiments in rodents highlighted thecritical role of molecular control of hypoxia and particularlyof HIF in lung growth and maturation. Deletion of HIF-1αdecreases branching morphogenesis and vascularization[19]. Deletion of HIF-2α delays lung maturation in aVEGF-dependent manner, leading to pulmonary distressand fatality in knockdown pups. Both the alveolar epithelialand vascular systems show signs of significant immaturity,which resembles the lung complications of prematurity inhumans [20].
Proper lung development requires a tight regulation ofexpression levels of HIF(s) and hypoxia-inducible genes,such as VEGF. Chemical stabilization of HIF-1α due toprolyl-4-hydroxylase (PHD) inhibition with CoCl2 ordexferrioxamine interrupts airway and vascular branching
Fig. 1 Summary of effects of hypoxia and/or HIF-1/2α in lunghomeostasis and disease (box)
1318 J Mol Med (2007) 85:1317–1324

in cultured fetal lung explants or causes hypervascularitywith the nonspecific PHD inhibition with dimethyloxalyl-glycine [18]. Moreover, lung overexpression of VEGFthrough fetal development also leads to a hypervascularlung [21].
As a corollary of these data, HIF-1α may also regulatefetal to neonatal transition and postnatal lung growth andrepair as suggested by the fact that, in the absence ofhypoxia, normal postnatal and post-pneumectomized re-generative lungs have increased HIF-1α expression formonths after surgery [22].
Impairment of lung growth is a major factor limitingsurvival of preterm babies. Immature pulmonary surfactantprotein predisposes preterm babies to develop respiratorydistress syndrome (RDS), characterized by decreased lungcompliance and impaired gas exchange leading to hypoxia.Oxygen therapy to treat RDS exposes these infants tooxidative injury, which may impair the expression of growthfactors (i.e., VEGF) involved in vascular and alveolardevelopment, therefore leading to bronchopulmonary dys-plasia (BPD) [23]. The potential role of the HIF/VEGF axisin fetal lung maturation lung was demonstrated in HIF-2αknockout mice that are born with lung immaturity and showa phenotype similar to respiratory distress syndrome (RDS).RDS predisposes to BPD, whose pathogenesis resembles,to some extent, that of retinopathy of prematurity, in whichhigh oxygen levels lead to disruption of VEGF-maintenanceof blood vessels and endothelial cell apoptosis, resulting inorgan damage. In fact, the expression of HIF-1α, HIF-2α,and downstream angiogenic growth factors (VEGF,PECAM-1, Flt-1, and Tie-2) are decreased in animal modelsof RDS or BPD [24–27]. Several of adolescent and adultBPD patients exhibit an emphysematous phenotype, poten-tially related to disruption of alveolar maintenance (seeemphysema, below). The findings that PHDs control HIFdegradation under normoxia and PHD activity is increasedwith increased oxygen availability [28] have offered newopportunities to develop therapies for BPD, as HIF-1αstabilization with PHD inhibitors improves lung growth andoxygenation [29].
Hypoxia, pulmonary circulation, and pulmonaryhypertension
Overall, the pulmonary vasculature comprises approximatelyone-third of estimated total number of 1 to 6×1013
endothelial cells in the human body (covering an areaequivalent to 1,200–2,500 m2). The pulmonary endotheliumactively participates in hypoxia-induced responses, integrat-ing sensing and effector functions that transmit changes inblood flow and vascular pressure. Injury or dysfunction ofendothelium induced by hypoxia leads to increased perme-
ability, heightened vascular smooth muscle tone, enhancedthrombotic state, and cell proliferation, all of whichparticipate in the process of tissue remodeling.
Acute decreases in inspired (alveolar) oxygen to levelsbelow 12% of normal (approximately equivalent to analtitude of 18,000 ft) induce reversible constriction ofvascular pulmonary smooth muscle cells (PASMCs), aunique property of pre-acinar pulmonary arteries presentacross most mammals, reptiles, birds, and fish [30–32].This contraction constitutes hypoxic pulmonary vasocon-striction (HPV), i.e., a rise of 4–8 mmHg in pulmonaryarterial pressures with decreased inspired oxygen. Experi-mentally, hypoxia triggers a biphasic pressure response, anearly one followed by vasorelaxation and a persistentsecond wave of contraction; this second stage may representthe true basis of HPV. Teleologically, HPV serves to allowfor matching between ventilation and perfusion, divertingblood flow from hypoxic to better aerated alveoli. Themultidetector-row computer tomography (MR-CT) has per-mitted functional lung studies, such as the documentation ofHPV in real time by imaging regional pulmonary bloodflow and ventilation [33]. Interestingly, bacterial infectionor lipopolysaccharide inhibit HPV, which can be visualizedand documented by MR-CT (Fig. 2, based on [33]).Oxygen sensing in PASMCs has been attributed to:(1) mitochondrial respiration, (2) mitochondria-dependentdecreases in reactive oxygen species (ROS), (3) mitochondria-dependent increases in ROS, (4) mitochondria membranedepolarization, (5) decreased ATP levels with generation ofcyclic ADP-ribose, (6) NADPH oxidase, (7) small GTPaseRhoA-mediated sensitization to intracellular Ca+2, and (8)cytochrome P450-mediated activation of hemoxygenase-2[32].
High altitude pulmonary edema (HAPE) is characterizedby shortness of breath that increases with altitude ascentwithout a period of acclimatization. It occurs in 0.1–15%individuals, pending individual susceptibility and preexistingcardiovascular diseases [34]. HAPE is associated withmarked increases of pulmonary artery pressures caused byHPV, in excess of 35 to 40 mmHg. However, HPV is notuniform in the lung. Alveolar fluid leak with the potentialcomplication of alveolar hemorrhage may result from afocally reduced HPV, leading to increased blood flow anddisruption of the alveolar–capillary barrier. The mainhypotheses to explain HAPE lie on excessive vasoconstric-tion, excessive inflammation due to hypoxia, or down-regulation of alveolar cell ion pumps that move sodium andfluid from alveoli into the blood stream [34]. As miceexposed to chronic hypoxia develop lung inflammation [35],it is conceivable that acute hypoxia may trigger acute lunginflammation. However, acute inflammation and HPV maynot coexist, as inflammation caused by lipopolysaccharideprevents HPV (Fig. 2) [36].
J Mol Med (2007) 85:1317–1324 1319

Chronic hypoxia causes pulmonary hypertension (PH),which consists of an increase in mean pulmonary arterypressures in excess of 25 mmHg at rest or 30 mmHg onexercise [37]. Hypoxia-induced PH is usually mild (i.e.,less than 45 mmHg) and potentially reversible uponnormalization of inspired oxygen levels. PH associated
with several lung diseases, particularly with sleep apneaand potentially with chronic obstructive pulmonary diseases(COPD), has been linked to chronic hypoxia. The experi-mental model of hypoxia-induced PH is based on exposureof rodents to 50% reduced oxygen levels for more than2 weeks. This model is characterized by vascular cell
Fig. 2 Documentation of HPV by multidetector-row CT. a Saline-injured dog lung (in supine position, with nondependent areas at12 o’clock and dependent regions at 6 o’clock) showing lung edemaand atelectasis in the dependent areas (whitened areas in the left upperpanel), with reduced aeration (digital quantification expressed as bluepixels in upper middle panel). This poorly aerated dependent regionalso shows markedly decreased blood flow (i.e., more blue/green
pixels in upper right panel) due to HPV. Normally, these dependentareas should receive most of the pulmonary blood flow. b LPSinstillation causes loss of HPV, when the poorly aerated dependentflooded areas (blue pixels in lower middle panel) have preferentialpulmonary blood flow (red pixels in lower right panel) (based on [33],reprinted under permission)
Fig. 3 Hypoxic pulmonary vascular remodeling. Images are from ratsexposed to normoxia or chronic hypoxia (equivalent to 17,000 ftaltitude above sea level) for 3 weeks. a Pulmonary artery of a ratunder normoxia conditions. Note that there is a loss of medial smoothmuscle cells in arteries less than approximately 30 um in diameter(arrowheads), located in alveolar tissue distal to terminal bronchioles.The vascular media represents approximately 5–8% of the vesseldiameter. b Immunofluorescence of a normal pulmonary artery stainedwith anti-smooth muscle cell α-actin antibody. c Large pulmonary
artery of rats exposed to chronic hypoxia, showing prominent mediallayer. d Extension of medial muscular layer towards the lungperiphery of a pulmonary artery sectioned longitudinally. e Immuno-fluorescence with an anti-smooth muscle α-actin antibody highlightsincreased medial thickness of a chronically hypoxic pulmonary artery.f Hydroxyprobe-based detection of cellular hypoxia, showing stainingof endothelial cells in pulmonary arteries (arrowhead) and of type IIepithelial cells (arrow) in lungs exposed to chronic hypoxia
1320 J Mol Med (2007) 85:1317–1324

proliferation, involving initially endothelial cells, followedby PASMCs, and then adventitial fibroblasts [38]. Increasedmedial thickness becomes apparent with 2 weeks of chronichypoxia exposure (Fig. 3). Hypoxia stimulates a wide arrayof potential mediators of PASMC growth, includingplatelet-derived growth factor, transforming growth factorβ, and NADP oxidase subunit 4. Although there is noevidence that humans living in high altitude or sufferingfrom lung diseases associated with chronic hypoxia are atincreased risk of severe PH (i.e., pulmonary artery pressuresin excess of 45 mmHg), investigation of the underlyingmechanisms involving hypoxia sensing have offered newinsights in the pathogenesis of the human disease.
Pulmonary endothelial cell dysfunction, a leading con-cept of the pathogenesis of PH [39], may account forexcessive pulmonary vascular cell growth and/or decreasedcell death [40]. An extension of this paradigm is theevidence that the pulmonary vascular remodeling in severePH involves elements of abnormal angiogenesis [40], and itresembles that seen in neoplastic cells [41]. HIF-1αcontrols several features involved in angiogenesis andcancer cell growth, including mitochondria function, whichhave been validated recently in studies of experimental PH[42]. Mitochondria of PASMCs are different from theirsystemic counterpart, as they have lower respiratory rates,are more depolarized, have more manganese superoxidedismutase (MnSOD), and produce more hydrogen peroxide[43]. Under normoxic conditions, the electron transport inmitochondria results in a small production of superoxideradicals, in proportion to alveolar oxygen pressure. Super-oxide, a potentially toxic reactive oxygen species (ROS), isconverted to a hydrogen peroxide that acts as diffusiblesecond messenger and subsequently regulates activity ofredox-sensitive transcription factors, including HIF-1α, andthe activation and expression of voltage-gated Kv
+ channels(e.g., Kv
+ 1.5). There has been an intense debate whetherhypoxic pulmonary vascular cells have increased ordecreased oxidative stress. However, one view predicatesthat, within seconds of exposure to hypoxia, mitochondrialROS production decreases, which inhibits oxygen-sensitiveKv
+ channels and causes membrane depolarization, activa-tion of voltage-gated L-type calcium channels, and calciuminflux, thereby initiating HPV [44]. If this redox oxygensensor is impaired, disrupted mitochondria create a false“hypoxic signal”, chronically activating HIF-1α undernormoxic conditions. HIF-1α activation downregulatesoxygen-sensitive Kv
+ channels (Kv+1.5) and initiates a
cascade that causes PH. This mechanism has beenpostulated to lead not only to enhanced vasoconstriction,but also to resistance to cell death via hyperpolarization ofmitochondria and enhanced survivin expression [45].
The involvement of HIF-1α in PH was documented bythe finding that heterozygous mice when exposed to
hypoxia (10% O2 for 1 to 6 weeks) developed lesspolycythemia, right ventricular hypertrophy, pulmonaryhypertension, pulmonary vascular remodeling, and weightloss than wild-type mice [46]. HIF-2α, which is abundantlyexpressed in the lung, is also involved in PH, in thatheterozygous mice are fully protected against PH and rightventricular hypertrophy caused by chronic hypoxia [47].HIF-1α regulates PASMC Kv
+ capacitance, K+ currentdensity, and membrane depolarization, which are decreasedin HIF-1α-+/−cells [48]. After exposure to chronic hypoxia,wild-type PASMCs increase the expression and activity ofNa+/H+ exchanger (NHE), which results in increasedintracellular pH and cell growth [49]. Recent reportsindicate that hypoxic PASMCs have increased expressionof canonical transient receptor potential (TRPC) channels 1and 6 in a HIF-1α-dependent manner [50].
There is experimental and clinical data that implicateserotonin in PH and lung hypoxic responses. Serotonin(5-HT) could affect pulmonary vascular remodeling, as itpromotes vasoconstriction and vascular smooth muscle cellgrowth [51]. Hypoxia modifies plasma levels of serotonin,serotonin transporter activity, and expression of 5-HT1B and5-HR2B receptors [52]. However, rather than 5-HT trans-porters, serotonin receptors might instead mediate hypoxicPH as demonstrated by the protection against hypoxic PHdocumented in mice lacking 5-HT2B receptors [53].
Under physiological conditions, endothelial cells remainquiescent and slow growing with only 1 dividing cell per10,000 cells at any given time, which translates into a rateof one cellular division every 2 weeks. In severe pulmonaryarterial hypertension (PAH), there is a unique and charac-teristic presence of plexiform lesions in the lumens ofmedium and small precapillary pulmonary arteries. Theselesions show enhanced expression of VEGF, VEGFreceptor, HIF-1α, and HIF-1β, which suggests that lesionsmay develop by a process of disordered angiogenesis [54].Similar results were recently obtained with culturedendothelial cells isolated form patients with IPAH. Thesecells have greater proliferation rate and decreased apopto-sis, higher level of phosphorylated STAT3 and increasedexpression of its downstream prosurvival target, Mcl-1[55]. Moreover, endothelial cells from idiopathic PAHlungs have decreased mitochondria and use preferentiallythe glycolytic pathway to generate energy, properties incommon to cancer cells [56]. Although the involvement ofHIF in this phenotype and in disease severity has not yetbeen formally tested, it is conceivable that vascular cellshave an altered hypoxia-sensing mechanism, predisposingthem to increased growth potential and even genomicinstability. In a model of severe PH in the rat, chronichypoxia in association with chronic VEGF receptorinhibition with SU5416 may be critically involved in theinitial endothelial cell death and selection of apoptosis-
J Mol Med (2007) 85:1317–1324 1321

resistant proliferating cells, which obliterate the pulmonaryarteries [57].
Mutations of bone morphogenetic protein receptor 2(BMPR-2) are involved in approximately 60% of thefamilial cases of familial PAH. Up to the present day, it isnot clear how the germ line mutation in a single copy of thegene causes IPAH. There is evidence that either a state ofhaploinsufficiency or dominant negative effects leads toenhanced growth of cultured IPAH PASMCs. AlthoughBMPR-2 heterozygous mice have normal lungs andpulmonary circulation at baseline, they develop morepronounced PH (though of mild severity) under inflamma-tory conditions or under hypoxia [58].
Hypoxia and chronic obstructive pulmonary diseases
COPD is the fourth leading cause of morbidity andmortality in the United States alone [59]. This syndromeis mostly caused by chronic cigarette smoke inhalation andexposure to environmental pollutants. In COPD, progres-sive airflow limitation and destruction of the alveolarcapillary network may lead to decreased oxygen transportand alveolar hypoxia.
The finding that blockade of VEGF receptor signalingcauses rodent emphysema led to several studies thatdocumented decreased VEGF and VEGF receptor expres-sion in emphysematous lungs [60]. Whether the expressionof HIF and other signaling molecules involved in hypoxiasensing is abnormal in emphysema remains unknown.There is recent evidence that cigarette smoke impairsHIF-1α expression in ischemic limbs of mice, causingdecreased revascularization [61]. Moreover, we found thatRTP-801 or Redd-1, a negative regulator of mTORsignaling and hypoxia-responsive gene product, is inducedby cigarette smoke. RTP801 knockout mice were signifi-cantly resistant to cigarette smoke-induced inflammationand emphysema [62]. About 60% of patients with COPDsuffer from mild PH. Up to 5% of COPD patients havesevere levels of PH with pulmonary artery pressures similarto that found in the systemic circulation [63]. PH in COPDis not fully explained by hypoxia alone, as it occurs in non-hypoxic patients and long-term oxygen therapy or nitricoxide inhalation do not reverse the pulmonary vascularchanges. A direct toxic effect of cigarette smoke onpulmonary vasculature has been suggested to act in concertwith a potential hypoxic effect observed in COPD [63].
Conclusions
Cellular signaling involved in hypoxia sensing participatesin several physiological and pathophysiological processes
in the lung. Several of these effects can be traced toavailability of oxygen itself, as long-term oxygen therapy isthe only proven effective therapy that increases long-termsurvival for patients in COPD [64]. Hypoxia itself orhypoxia-induced signaling may underlie the pathogenesisof several life-threatening lung diseases, as it regulates theexpression of several critical genes. Lessons learned in therole of hypoxia in tumor growth and organ biology willcertainly apply to fundamental aspects of lung repair, cellinjury, or inflammation. We are just the beginning of thesystematic exploration of this paradigm in pulmonarydiseases. These efforts will translate in a better understand-ing of hypoxia-driven cell signaling and of suitability oftherapeutic targets aimed at several lung diseases, includinglung immaturity, pulmonary hypertension, and COPD.
Acknowledgements The authors thank Shehzin Mozammel andReda Girgis for providing the immunofluorescence images and Dr.Brett Simon for the documentation of MR-CT, Ms. Amy Richter forthe hydroxyprobe staining, and Mrs. Kathleen Wolfe for the secretarialsupport.
Grant support This work has been supported by the CMREFCenter for Tissue Processing Center of the Pulmonary HypertensionBreakthrough Initiative, P150 HL 084946-01 (Pathology Core andProject 5), and HL 66554.
References
1. Weibel ER (1980) Design and structure of human lung inPulmonary diseases and disorders. McGrow-Hill Book Company,New York
2. Liu L, Cash TP, Jones RG, Keith B, Thompson CB, Simon MC(2006) Hypoxia-induced energy stress regulates mRNA transla-tion and cell growth. Mol Cell 4:521–531
3. Kulshreshtha R, Ferracin M, Negrini M, Calin GA, Davuluri RV,Ivan M (2007) Regulation of microRNA expression: the hypoxiccomponent. Cell Cycle 12:1426–1431
4. Kulshreshtha R, Ferracin M, Wojcik SE, Garzon R, Alder H,gosto-Perez FJ, Davuluri R, Liu CG, Croce CM, Negrini M, CalinGA, Ivan M (2007) A microRNA signature of hypoxia. Mol CellBiol 5:1859–1867
5. Arbiser JL, Klauber N, Rohan RM, van Leeuwen R, Huang MT,Fisher C, Flynn E, Byers HR (1998) Curcumin is an in vivoinhibitor of angiogenesis. Mol Med 6:376
6. Kent OA, Mendell JT (2006) A small piece in the cancer puzzle:microRNAs as tumor suppressors and oncogenes. Oncogene46:6188–6196
7. Rodriguez A, Vigorito E, Clare S,WarrenMV, Couttet P, Soond DR,van DS, Grocock RJ, Das PP, Miska EA, Vetrie D, Okkenhaug K,Enright AJ, Dougan G, Turner M, Bradley A (2007) Requirement ofbic/microRNA-155 for normal immune function. Science 5824:608–611
8. Yan SF, Zou YS, Gao Y, Zhai C, Mackman N, Lee SL, Mibrandt J,Pinsky D, Kisiel W, Stern D (1998) Tissue factor transcriptiondriven by Egr-1 is a critical mechanism of murine pulmonary fibrindeposition in hypoxia. Proc Natl Acad Sci USA 14:8298
9. Lawson CA, Yan SD, Yan SF, Liao H, Zhou YS, Sobel J, Kisiel W,Stern DM, Pinsky DJ (1997) Monocytes and tissue factor promote
1322 J Mol Med (2007) 85:1317–1324

thrombosis in a murine model of oxygen deprivation. J Clin Invest7:1729–1738
10. van Tuyl M, Liu J, Wang J, Kuliszewski M, Tibboel D, Post M(2005) Role of oxygen and vascular development in epithelialbranching morphogenesis of the developing mouse lung. Am JPhysiol Lung Cell Mol Physiol 1:L167–L178
11. Maltepe E, Simon MC (1998) Oxygen, genes, and development:an analysis of the role of hypoxic gene regulation during murinevascular development. J Mol Med 6:391–401
12. Tufro-McReddie A, Norwood VF, Aylor KW, Botkin SJ, Carey RM,Gomez RA (1997) Oxygen regulates vascular endothelial growthfactor-mediated vasculogenesis and tubulogenesis. Dev Biol2:139–149
13. Gebb SA, Jones PL (2003) Hypoxia and lung branchingmorphogenesis. Adv Exp Med Biol 28:133–137
14. Jarecki J, Johnson E, Krasnow MA (1999) Oxygen regulation ofairway branching in Drosophila is mediated by branchless FGF.Cell 2:211–220
15. Minchenko A, Bauer T, Salceda S, Caro J (1994) Hypoxicstimulation of vascular endothelial growth factor expression invitro and in vivo. Lab Invest 3:374–379
16. Jakkula M, Le Cras TD, Gebb S, Hirth KP, Tuder RM, Voelkel NF,Abman SH (2000) Inhibition of angiogenesis decreasesalveolarization in the developing rat lung. Am J Physiol,Lung Cell Mol Physiol 3:L600–L607
17. Acarregui MJ, Snyder JM, Mendelson CR (1993) Oxygenmodulates the differentiation of human fetal lung in vitro and itsresponsiveness to cAMP. Am J Physiol Lung Cell Mol Physiol 5:L465–L474
18. Groenman FA, Rutter M, Wang J, Caniggia I, Tibboel D, Post M(2007) Effect of chemical stabilizers of hypoxia-inducible factorson early lung development. Am J Physiol Lung Cell Mol Physiol3:L557–L567
19. van Tuyl M, Liu J, Wang J, Kuliszewski M, Tibboel D, Post M(2005) Role of oxygen and vascular development in epithelialbranching morphogenesis of the developing mouse lung. Am JPhysiol Lung Cell Mol Physiol 1:L167–L178
20. Compernolle V, Brusselmans K, Acker T, Hoet P, Tjwa M, Beck H,Plaisance S, Dor Y, Keshet E, Lupu F, Nemery B, Dewerchin M,Van Veldhoven P, Plate K, Moons L, Collen D, Carmeliet P (2002)Loss of HIF-2alpha and inhibition of VEGF impair fetal lungmaturation, whereas treatment with VEGF prevents fatal respiratorydistress in premature mice. Nat Med 7:702–710
21. Zeng X, Wert SE, Federici R, Peters KG, Whitsett JA (1998)VEGF enhances pulmonary vasculogenesis and disrupts lungmorphogenesis. Dev Dyn 211:215–227
22. Zhang Q, Moe OW, Garcia JA, Hsia CCW (2006) Regulatedexpression of hypoxia-inducible factors during postnatal andpostpneumonectomy lung growth. Am J Physiol Lung Cell MolPhysiol 5:L880–L889
23. Asikainen TM, White CW (2005) Antioxidant defenses in thepreterm lung: role for hypoxia-inducible factors in BPD. ToxicolAppl Pharmacol 2:177–188
24. Grover TR, Asikainen TM, Kinsella JP, Abman SH, White CW(2007) Hypoxia-inducible factors HIF-1alpha and HIF-2alpha aredecreased in an experimental model of severe respiratory distresssyndrome in preterm lambs. Am J Physiol Lung Cell Mol Physiol6:L1345–L1351
25. Lassus P, Turanlahti M, Heikkila P, Andersson LC, Nupponen I,Sarnesto A, Andersson S (2001) Pulmonary vascular endothelialgrowth factor and Flt-1 in fetuses, in acute and chronic lungdisease, and in persistent pulmonary hypertension of the newborn.Am J Respir Crit Care Med 10 Pt 1:1981–1987
26. Bhatt AJ, Pryhuber GS, Huyck H, Watkins RH, Metlay LA,Maniscalco WM (2001) Disrupted pulmonary vasculature anddecreased vascular endothelial growth factor, Flt-1, and TIE-2 in
human infants dying with bronchopulmonary dysplasia. Am JRespir Crit Care Med 10 Pt 1:1971–1980
27. Maniscalco WM, Watkins RH, Pryhuber GS, Bhatt A, Shea C,Huyck H (2002) Angiogenic factors and alveolar vasculature:development and alterations by injury in very premature baboons.Am J Physiol Lung Cell Mol Physiol 4:L811–L823
28. Asikainen TM, Ahmad A, Schneider BK, Ho WB, Arend M,Brenner M, Gunzler V, White CW (2005) Stimulation of HIF-1alpha, HIF-2alpha, and VEGF by prolyl 4-hydroxylase inhibitionin human lung endothelial and epithelial cells. Free Radic BiolMed 8:1002–1013
29. Asikainen TM, Chang LY, Coalson JJ, Schneider BK, Waleh NS,IkegamiM, Shannon JM,Winter VT, Grubb P, Clyman RI, Yoder BA,Crapo JD, White CW (2006) Improved lung growth and functionthrough hypoxia-inducible factor in primate chronic lung disease ofprematurity. FASEB J 10:1698–1700
30. von Euler US, Liljsjestrand G (1946) Observations of thepulmonary arterial blood pressure on the cat. Acta Physiol Scand12:301–320
31. Weissmann N, Sommer N, Schermuly RT, Ghofrani HA, Seeger W,Grimminger F (2006) Oxygen sensors in hypoxic pulmonaryvasoconstriction. Cardiovasc Res 4:620–629
32. Ghofrani HA, Voswinckel R, Reichenberger F, Weissmann N,Schermuly RT, Seeger W, Grimminger F (2006) Hypoxia- andnon-hypoxia-related pulmonary hypertension—established andnew therapies. Cardiovasc Res 1:30–40
33. Easley RB, Fuld MK, Fernandez-Bustamante A, Hoffman EA,Simon BA (2006) Mechanism of hypoxemia in acute lunginjury evaluated by multidetector-row CT. Acad Radiol 7:916–921
34. Swenson ER (2006) Hypoxic lung whiteout: further clearing butmore questions from on high. Ann Intern Med 7:550–552
35. Minamino T, Christou H, Hsieh CM, Li Y, Dhawan V, Abraham NJ,Perrella MA, Mitsialis SA, Kourembanas S (2001) Targetedexpression of hemeoxygenase-1 prevents the pulmonary inflamma-tory and vascular responses to hypoxia. Proc Natl Acad Sci USA15:8798–8803
36. Hoffman EA, Simon BA, McLennan G (2006) State of the art. Astructural and functional assessment of the lung via multidetector-row computed tomography: phenotyping chronic obstructivepulmonary disease. Proc Am Thorac Soc 6:519–532
37. Voelkel NF, Tuder RM (2000) Hypoxia-induced pulmonaryvascular remodeling—a model for what human disease. J ClinInvest 6:733–738
38. Meyrick B, Reid L (1979) Hypoxia and incorporation of 3H-thymidine by cells of the rat pulmonary arteries and alveolar wall.Am J Pathol 1:51–70
39. Budhiraja R, Tuder RM, Hassoun PM (2004) Endothelialdysfunction in pulmonary hypertension. Circulation 2:159–165
40. Zaiman A, Fijalkowska I, Hassoun PM, Tuder RM (2005) Onehundred years of research in the pathogenesis of pulmonaryhypertension. Am J Respir Cell Mol Biol 5:425–431
41. Voelkel NF, Cool CD, Lee SD, Wright L, Geraci MW, Tuder RM(1999) Primary pulmonary hypertension between inflammationand cancer. Chest Suppl 3:225S–230S
42. Bonnet S, Michelakis ED, Porter CJ, Andrade-Navarro MA,Thebaud B, Bonnet S, Haromy A, Harry G, Moudgil R,McMurtry MS, Weir EK, Archer SL (2006) An abnormalmitochondrial-hypoxia inducible factor-1alpha-Kv channel path-way disrupts oxygen sensing and triggers pulmonary arterialhypertension in fawn hooded rats: similarities to human pulmo-nary arterial hypertension. Circulation 22:2630–2641
43. Michelakis ED, Hampl V, Nsair A, Wu X, Harry G, Haromy A,Gurtu R, Archer SL (2002) Diversity in mitochondrial functionexplains differences in vascular oxygen sensing. CirculationResearch 12:1307–1315
J Mol Med (2007) 85:1317–1324 1323

44. Reeve HL, Archer SL, Weir EK (1997) Ion channels in thepulmonary vasculature. Pulm Pharmacol Ther 10:243–252
45. McMurtry MS, Archer SL, Altieri DC, Bonnet S, Haromy A,Harry G, Bonnet S, Puttagunta L, Michelakis ED (2005) Genetherapy targeting survivin selectively induces pulmonary vascularapoptosis and reverses pulmonary arterial hypertension. J ClinInvest 6:1479–1491
46. Yu AY, Shimoda LA, Iyer NV, Huso DL, Sun X, McWilliams R,Beaty T, Sham JS, Wiener CM, Sylvester JT, Semenza GL (1999)Impaired physiological responses to chronic hypoxia in micepartially deficient for hypoxia-inducible factor 1 alpha. J ClinInvest 5:691–696
47. Brusselmans K, Compernolle V, TjwaM,WiesenerMS,Maxwell PH,Collen D, Carmeliet P (2003) Heterozygous deficiency of hypoxia-inducible factor-2alpha protects mice against pulmonary hypertensionand right ventricular dysfunction during prolonged hypoxia. J ClinInvest 10:1519–1527
48. Shimoda LA, Manalo DJ, Sham JSK, Semenza GL, Sylvester JT(2001) Partial HIF-1{alpha} deficiency impairs pulmonary arterialmyocyte electrophysiological responses to hypoxia. Am J Physiol,Lung Cell Mol Physiol 1:L202–L208
49. Shimoda LA, Fallon M, Pisarcik S, Wang J, Semenza GL (2006)HIF-1 regulates hypoxic induction of NHE1 expression andalkalinization of intracellular pH in pulmonary arterial myocytes.Am J Physiol, Lung Cell Mol Physiol 5:L941–L949
50. Wang J, Weigand L, Lu W, Sylvester JT, Semenza L, Shimoda LA(2006) Hypoxia inducible factor 1 mediates hypoxia-inducedTRPC expression and elevated intracellular Ca2+ in pulmonaryarterial smooth muscle cells. Circ Res 12:1528–1537
51. Fanburg BL, Lee SL (2000) A role for the serotonin transporter inhypoxia-induced pulmonary hypertension. J Clin Invest 11:1521–1523
52. Eddahibi S, Hanoun N, Lanfumey L, Lesch KP, Raffestin B,Hamon M, Adnot S (2000) Attenuated hypoxic pulmonaryhypertension in mice lacking the 5-hydroxytryptamine transportergene. J Clin Invest 11:1555–1562
53. Launay JM, Herve P, Peoc'h K, Tournois C, Callebert J, Nebigil CG,Etienne N, Drouet L, Humbert M, Simonneau G, Maroteaux L(2002) Function of the serotonin 5-hydroxytryptamine 2B receptorin pulmonary hypertension. Nat Med 10:1129–1135
54. Tuder RM, Chacon M, Alger L, Wang J, Taraseviciene-Stewart L,Kasahara Y, Cool CD, Bishop AE, Geraci M, Semenza GL,Yacoub M, Polak JM, Voelkel NF (2001) Expression ofangiogenesis-related molecules in plexiform lesions in severe
pulmonary hypertension: evidence for a process of disorderedangiogenesis. J Pathol 3:367–374
55. Masri FA, Xu W, Comhair SAA, Asosingh K, Koo M, Vasanji A,Drazba J, Anand-Apte B, Erzurum SC (2007) Hyperproliferativeapoptosis-resistant endothelial cells in idiopathic pulmonary arterialhypertension. Am J Physiol, Lung Cell Mol Physiol 3:L548–L554
56. Xu W, Koeck T, Lara AR, Neumann D, DiFilippo FP, Koo M,Janocha AJ, Masri FA, Arroliga AC, Jennings C, Dweik RA,Tuder RM, Stuehr DJ, Erzurum SC (2007) Alterations of cellularbioenergetics in pulmonary artery endothelial cells. Proc NatlAcad Sci USA 4:1342–1347
57. Taraseviciene-Stewart L, Kasahara Y, Alger L, Hirth P,McMahonGG,Waltenberger J, Voelkel NF, Tuder RM (2001) Inhibition of the VEGFreceptor 2 combined with chronic hypoxia causes cell death-dependentpulmonary endothelial cell proliferation and severe pulmonaryhypertension. Faseb J 2:427–438
58. Beppu H, Ichinose F, Kawai N, Jones RC, Yu PB, Zapol WM,Miyazono K, Li E, Bloch KD (2004) BMPR-II heterozygous micehave mild pulmonary hypertension and an impaired pulmonaryvascular remodeling response to prolonged hypoxia. Amer JPhysiol -Lung Cell M PH 6:L1241–L1247
59. Yoshida T, Tuder RM (2007) Pathobiology of cigarette smoke-induced chronic obstructive pulmonary disease. Physiol Rev3:1047–1082
60. Voelkel NF, Vandivier RW, Tuder RM (2006) Vascular endothelialgrowth factor in the lung. Am J Physiol Lung Cell Mol Physiol 2:L209–L221
61. Michaud SE, Menard C, Guy LG, Gennaro G, Rivard A (2003)Inhibition of hypoxia-induced angiogenesis by cigarette smokeexposure: impairment of the HIF-1alpha/VEGF pathway. Faseb J9:1150–1152
62. Yoshida T, Rangasamy T, Biswal S, Petrache I, Mett I, Feinstein E,Tuder RM (2006) Role of RTP801, a suppressor of the mTORpathway, in cigarette smoke-induced pulmonary injury in mice.Proc Am Thorac Soc 6:551a–552a
63. Wright JL, Levy RD, Churg A (2005) Pulmonary hypertension inchronic obstructive pulmonary disease: current theories of patho-genesis and their implications for treatment. Thorax 7:605–609
64. Croxton TL, Bailey WC, for the NHLBI Working Group on Long-term Oxygen Treatment in COPD (2006) Long-term oxygentreatment in chronic obstructive pulmonary disease: recommen-dations for future research: An NHLBI Workshop Report. Am JRespir Crit Care Med 4(373–378)
1324 J Mol Med (2007) 85:1317–1324

REVIEW
Hypoxia and the HIF system in kidney disease
Masaomi Nangaku & Kai-Uwe Eckardt
Received: 8 October 2007 /Revised: 23 October 2007 /Accepted: 23 October 2007 / Published online: 20 November 2007# Springer-Verlag 2007
Abstract The kidney is sensitive to changes in oxygendelivery. This sensitivity has the merit of facilitating thekidneys in their adjustment of erythropoietin (EPO) produc-tion to changes in oxygen supply. The main determinant ofEPO synthesis is the transcriptional activity of its gene inkidneys, which is related to local oxygen tensions. Regula-tion of EPO production is mediated by hypoxia-induciblefactor (HIF). When local oxygen tension decreases, accu-mulated HIF binds to the key sequence of the EPO gene, thehypoxia-responsive element (HRE), and activates transcrip-tion of EPO. HIF consists of a constitutive β-subunit and oneof alternative oxygen-regulated HIF α-subunits (HIF-1α,HIF-2α, and HIF-3α), and HIF-2α is responsible forerythropoietin production. However, the high sensitivity tochanges in oxygen tension also makes the kidney prone tohypoxic injury. Severe energy depletion and subsequentactivation of a number of critical alterations in metabolismoccurs under hypoxic conditions. Hypoxia is also a profi-brogenic stimulus. In addition to ischemic acute renal failure,hypoxia can also play a crucial role in the development ofnephrotoxic acute kidney injury, radiocontrast nephropathy,and acute glomerulonephritis. Furthermore, accumulating
evidence suggests that chronic hypoxia is a final commonpathway to end-stage kidney failure in chronic kidneydisease. Given that renal hypoxia has pivotal roles on thedevelopment and progression of both acute and chronickidney disease, hypoxia can be a valid therapeutic target forchronic kidney disease. Activation of HIF leads to expres-sion of a variety of adaptive genes in a coordinated manner.Studies utilizing HIF-stimulating agents proved efficacy invarious kidney disease models, suggesting that HIF activa-tion is an ideal target of future therapeutic approaches.
Keywords HIF. Acute kidney injury .
Chronic kidney disease . Erythropoietin . Hypoxia
Oxygenation of the kidney
Although blood flow to the kidney is high, accountingfor 20% of cardiac output, the presence of oxygen shuntdiffusion between arterial and venous vessels that run inclose parallel contact keeps renal tissue oxygen tensionscomparatively low. Most of the blood supply is directed tothe renal cortex, and oxygen tension in the renal cortex isaround 30 to 50 mmHg, although this decreases dramati-cally in accordance with changes in renal perfusion. Incontrast, oxygen tension in the renal medulla does not riseabove 10 to 25 mmHg because of countercurrent oxygenexchange, resulting in borderline chronic oxygen depriva-tion. Furthermore, the cells in the S3 segment of the prox-imal tubule and the medullary thick ascending limbs areparticularly vulnerable to oxygen deprivation because of thehigh metabolic activity, principally owing to the activity ofthe basolateral Na/K-ATPase. As a consequence, the kidney
J Mol Med (2007) 85:1325–1330DOI 10.1007/s00109-007-0278-y
M. Nangaku (*)Division of Nephrology and Endocrinology,University of Tokyo School of Medicine,7-3-1 Hongo, Bunkyo-ku,Tokyo, Japane-mail: [email protected]
K.-U. EckardtDepartment of Nephrology and Hypertension,Friedrich-Alexander-University Erlangen–Nuremberg,Erlangen, Germany

is very sensitive to changes in oxygen delivery. While thissensitivity has the merit of facilitating the kidneys in theiradjustment of erythropoietin (EPO) production to changesin oxygen supply, it also renders them prone to hypoxicinjury.
Mechanisms of renal erythropoietin production
Anemia is a common complication in patients with chronickidney disease (CKD). Anemia impairs oxygen deliveryto tissues, and the kidney senses hypoxia and stimulateserythropoiesis as a compensatory response. While mecha-nisms involved in the pathogenesis of renal anemia includechronic inflammation, iron deficiency, and shortened half-lifeof erythrocytes, the primary cause is insufficient production ofEPO [1].
Circulating EPO in normal adults is mainly produced bythe peritubular fibroblast-like interstitial cells of the kidney.When hematocrit is in the normal range, the kidney pro-duces a low level of EPO, with EPO expression limited to asmall number of these fibroblasts in the deep cortex andsuperficial outer medulla [2–4]. The increased productionof EPO under anemic circumstances involves progressiverecruitment of additional interstitial fibroblasts in a patternthat spreads outward from the deep cortex toward the capsuleand the inner medulla. However, even at maximal stimulation,less than 20% of cortical fibroblast-like cells express EPO,and thus, it is likely that only a yet-unidentified subgroup ofspecialized interstitial cells produces the hormone.
The main determinant of EPO synthesis is the transcrip-tional activity of its gene in kidneys, which is related tolocal oxygen tensions. EPO production is inversely relatedto oxygen availability, so that an effective feedback loopis established, which controls erythropoiesis. More thana decade ago, a sequence in the 3′-flanking region of theEPO gene that is required for EPO gene’s upregulationby hypoxia was discovered [5]. Using large quantities oflysates from cultured Chinese hamster ovary cells exposedto a hypoxia mimetic, a heterodimeric complex of proteinsthat bind to this specific deoxyribonucleic acid (DNA)element to regulate hypoxia gene expression was thenidentified [6, 7]. The complex was designated as hypoxia-inducible factor (HIF). HIF consists of a constitutive β-subunit and one of alternative oxygen-regulated HIFαsubunits (HIF-1α, HIF-2α, and HIF-3α). Under hypoxia,accumulated HIF binds to the key sequence among severalregulatory DNA sequences in the neighborhood of the EPOgene, the hypoxia-responsive element (HRE), and activatestranscription of EPO.
While most cell types express HIF-1α and HIF-1β, HIF-2α (also called EPAS or HIF-1α-like factor) shows a more
restricted pattern of expression [8]. Localization and bio-logical functions of HIF-3α remains relatively unknown,but a splice variant of HIF-3α serves as an inhibitor of theHIF pathway in the cornea [9]. A predominant role of HIF-2α in regulation of EPO expression was confirmed bystudies employing ribonucleic acid (RNA) interference todetermine the contribution of HIF-1α vs HIF-2α to thehypoxic gene induction [10]. While most genes tested wereresponsive only to the HIF-1α small interfering RNA, EPOshowed responsiveness only to HIF-2α knockdown. High-amplification immunohistochemical analyses revealed theexpression of HIF-2 in peritubular fibroblasts [11], whichis consistent with its role in EPO regulation. Recent anal-ysis of HIF-2α knockdown mice revealed that EPO geneexpression was significantly affected, in parallel with HIF-2α expression [12]. Conditional knockout of HIF-2α afterbirth demonstrated that HIF-2α plays a critical role in adulterythropoiesis [13]. In addition, studies using mice withconditional knockout of HIF-1α and/or HIF-2α in hepato-cytes revealed that the hypoxic induction of liver EPO inanemic mice was also HIF-2α dependent [14].
Furthermore, HIF activation influences genes that playimportant roles in iron metabolism, including transferrin[15], ferroportin [16], and possibly hepcidin [16]. Thus, inaddition to increased EPO expression, HIF regulatesvarious pathways leading to efficient erythropoiesis [16].
Hypoxia in the pathogenesis of kidney disease
Aerobic respiration requires oxygen to generate energy andproduces 36–38 mol adenosine triphosphate (ATP) per 1 molglucose. In contrast, anaerobic respiration can produce only2 mol ATP out of 1 mol glucose. Therefore, it is no wonderthat severe energy depletion and subsequent activation of anumber of critical alterations in metabolism occurs underhypoxic conditions [17]. Cytoskeletal disruption leads to de-rangements and mislocation of various polarized proteinssuch as integrins and Na/K-ATPase. ATP depletion activatesharmful proteases and phospholipases. Induction of adhesionmolecules by hypoxia initiates inflammatory reactions.
In a long term, renal tubular cells subjected to hypoxiadevelop functional deficits in their mitochondria, which ag-gravate energy deficits, subsequently causing them to undergoapoptosis [18]. Hypoxia is also a profibrogenic stimulus fortubular cells, interstitial fibroblasts, and renal microvascularendothelial cells. Tubular cells under hypoxic conditionsundergo epithelial–mesenchymal transdifferentiation to be-come myofibroblasts [19]. Hypoxia can also activate fibro-blasts and change the extracellular matrix metabolism ofresident renal cells [20, 21].
1326 J Mol Med (2007) 85:1325–1330

pH is another factor that is implicated in cell injury underhypoxia. Under anaerobic conditions, cellular metabolism isshifted to the production of acidic metabolites such as lactatewith subsequent development of acidosis. However, it is con-troversial how acidic pH affects cell status. Regulation of HIFtarget genes are also inconsistent despite slight induction ofHIF protein levels under acidosis, suggesting additional, yetunidentified pH-sensitive regulatory factors [22].
Acute kidney injury
Acute renal failure (ARF) is a clinical syndrome denotedby an abrupt decline in glomerular filtration rate. Impairedrenal perfusion with a resultant fall in glomerular capillaryfiltration pressure is a common cause of ARF and can leadto acute tubular necrosis. Apart from acute ischemia, severaldistinct renal insults including nephrotoxic injury can alsocause acute tubular necrosis [23]. Prerenal azotemia, whichis considered a functional response to renal hypoperfusion,and ischemic acute tubular necrosis occur on a continuum ofthe same pathophysiological process and together accountfor 75% of the cases of ARF. In these cases, hypoxiabecause of hypoperfusion of the kidney plays a crucialrole in the pathogenesis. While patients with ischemic ARFtypically have low systemic perfusion, their blood pressuremay remain within the normal range. This type of ischemicARF is termed “normotensive ischemic ARF” and can occuras a result of various processes [24]. These processes involveincreased renal susceptibility to modest reductions in perfu-sion pressure and include structural changes of renal arte-rioles because of aging, hypertension, and CKD. Selectiverenal vasoconstriction plays a crucial role in some types of“normotensive ischemic ARF” including sepsis. Sepsis canact through various vasoconstrictor mediators to increaseafferent arteriolar resistance. This, in combination with directtoxic effects of sepsis on the tubules and low perfusion statesbecause of systemically reduced vascular resistance, resultsin “normotensive ischemic ARF.”
Hypoxia also plays an important role in developmentof radio-contrast nephropathy. Studies on a multi-insultrat model of ARF combining the application of contrastmedium with nitric oxide synthase and cyclooxygenase inhi-bition showed widespread induction of HIF in the outer andinner medulla that was initiated within 10 min, reached thehighest levels at 2 h, and diminished 8 h, to 24 h thereafter[25]. HIF isoforms were expressed in a cell type-specificfashion with HIF-1α in tubular and HIF-2α in interstitialand endothelial cells. The isolated perfused rat kidneysserve as a well-recognized model of hypoxic renal cellinjury when perfused with cell-free oxygenated medium.The pattern of both HIF activation and pimonidazole accu-mulation in the isolated kidneys perfused with cell-free
medium was remarkably consistent and in concordancewith the findings in the multi-insult rat model of ARF [26].
Various reagents cause nephrotoxic injury to the kidney.Cisplatin is a chemotherapeutic agent widely used for thetreatment of solid tumors but often induces nephrotoxickidney injury. Whether administration of cisplatin in ratsalso induces HIF-1 in tubular cells apparently depends onthe experimental conditions [27].
In addition to ARF, studies on acute glomerulonephritissuggested hypoxia-mediated pathomechanisms. Adminis-tration of angiotensin II combined with Habu snake venominduces acute glomerulonephritis in rats, with lesions beingrestricted to the glomeruli 2 days after the administration ofboth reagents. Immunohistochemical analysis and Westernblot analysis revealed that Habu snake venom caused ele-vated von Hippel-Lindau tumor suppressor protein (pVHL)expression in the injured glomeruli including endothelialcells and partially podocytes [28]. Administration of throm-bin as an inducer of pVHL accelerated the development ofglomerulonephritis even 1 day after treatment, demonstrat-ing a protective role of HIF in this model.
Chronic kidney disease
Close pathological analysis shows that functional impair-ment of the kidney is better correlated with the degree oftubulointerstitial damage than with that of glomerular injuryin patients with CKD, and this finding has in turn led to thebroad recognition that the final common pathway of kidneyfailure operates principally in the tubulointerstitium. Accu-mulating evidence emphasizes chronic hypoxia in the tubulo-interstitium as a final common pathway to end-stage kidneyinjury [29, 30].
A variety of methods have been successfully employedto demonstrate renal hypoxia with CKD. Pimonidazole,which binds to hypoxic cells in vivo, allowed us to demon-strate hypoxia of the kidney in association with reduction inperitubular capillary blood flow at an early stage of a modelof progressive glomerulonephritis induced by uninephrec-tomy and repeated injection of antimesangial Thy1 anti-body [31].
Pimonidazole staining also showed the existence of re-gional hypoxia in polycystic kidney disease (PKD) [32].HIF-1α and HIF-2α were upregulated in cyst epithelium andcells of cyst walls, respectively, in human PKD and in arodent PKD model. These results showed that polycystickidneys are hypoxic and that subsequent activation of HIFmay lead to EPO production and pericystic hypervascularity.
Chronic hypoxia of the diabetic kidney was demon-strated by pimonidazole [33], measurement with a micro-electrode [34], and blood-oxygen level-dependent magneticresonance imaging [35]. We established the hypoxia-
J Mol Med (2007) 85:1325–1330 1327

sensing transgenic rats expressing the HRE-driven lucifer-ase vector tagged with FLAG. With these rats, we observeddifferent patterns of renal hypoxia in rats with puromycin-induced nephritic syndrome and the remnant kidney model[36], as well as in the aging kidney [37].
Hypoxia-inducible transcription factors as a potentialtherapeutic target for prevention and treatmentof kidney disease
HIF-α mRNA expression is induced by hypoxia or ischemiain vivo to some extent. However, the amount of HIF isregulated mainly by the rate of degradation. The HIF-αsubunit interacts with proteins that regulate its degrada-tion, and this interaction is mediated by the pVHL. Theinteraction between HIFα and pVHL is triggered throughpost-translational HIFα hydroxylation catalyzed by specificHIF-prolyl hydroxylases (PHDs). The hydroxylated proteinis then recognized by pVHL, and is rapidly degraded bythe proteasome. Because HIF level is determined by itshydroxylation-induced degradation, hydroxylases involvedin this reaction may be good targets for therapy againstkidney disease.
The HIF hydroxylases belong to the Fe(II)- and 2-oxoglutarate-dependent dioxygenase superfamily, which isinvolved in a range of biosynthetic and metabolic pathways[38]. As the PHDs require iron as a cofactor to hydroxylatethe critical prolines on HIF-α, the finding that some ofthe best-established activators of HIF-1 are chelators ofiron is reasonable. Recent studies have demonstrated thatL-mimosine and ethyl-3,4-dihydroxybenzoate activate theHIF pathway primarily through iron chelation and induceangiogenesis in a sponge model, while other PHD inhib-itors can stabilize HIF independent of iron binding [10].Desferoxamine and cobalt chloride are among the mostwell-established iron chelators in the activation of HIF.More than half a century ago, oral administration of cobal-tous chloride was employed to treat anemia associated withchronic renal disease [39]. Cobalt therapy led to a signifi-cant erythropoietic response in association with improvedappetite and greater tolerance for medications necessary tocorrect electrolyte abnormalities.
Success of studies has been reported in various modelsof kidney diseases as described below. However, while ironchelators may also participate post-translationally in devas-tating oxidant production via reactions such as Fentonchemistry, iron is a necessary cofactor for a host of impor-tant cellular functions, including oxidative phosphoryla-tion and arachidonic acid signaling. Therefore, while thesestudies clearly provided rationale and promise of HIF-activating therapies in kidney diseases, potential sideeffects may hinder the therapeutic use of iron chelators.
A systematic examination of the relative efficacy of PHDinhibitors that bind iron vs those that do not is needed.
Acute kidney injury
Renoprotective effects of chemical preconditioning withcobaltous chloride were demonstrated in an ischemic modelof renal injury [40]. Administration induced upregulationof HIF-regulated genes, such as VEGF and EPO, and sub-sequently protected the kidney against the tubulointerstitialdamage induced by ischemia and reperfusion. Activationof HIF by pretreatment with either carbon monoxide orthe novel PHD inhibitor FG-4487 also ameliorated ARFinduced by ischemia/reperfusion in rats [41]. Collectively,these data proved that preconditional activation of the HIFsystem protects the kidney against acute ischemic injury.
Activation of HIF was also effective in nephrotoxic acutekidney injury. With the in vivo administration of cobalt toactivate HIF, the number of apoptotic renal tubular cellsbecame much smaller in cisplatin nephropathy [23]. Fur-thermore, induction of HIF with carbon monoxide beforeexposure of cisplatin significantly reduced histological renaldamage and tubular apoptosis in cisplatin nephropathy [42].
HIF induction therapy with cobalt chloride also ame-liorated disease manifestations of an acute rat glomerulo-nephritis model induced by coadministration of angiotensinII and Habu snake venom, which was associated with theinduction of HIF-1α in the glomeruli and renal tubules [43].
Chronic kidney disease
Given that renal hypoxia has pivotal roles on the progres-sion of renal failure, hypoxia can be a valid therapeutictarget for CKD. We tested whether cobalt attenuates tubulo-interstitial injury secondary to chronic hypoxia, using amodel of progressive glomerulonephritis induced by unin-ephrectomy and repeated injection of antimesangial Thy1antibodies. Activation of HIF by cobalt exerted renopro-tective roles in this model, and cobalt treatment had addi-tive, positive effects to the standard therapy of renal diseasenamely, the blockade of the renin–angiotensin system in thehypoxic tubulointerstitium [44]. We also treated rats withthe remnant kidney model, classically characterized bychronic renal failure with glomerular sclerosis and hyper-tension. Cobalt treatment mediated improvement in thetubulointerstitial injury as well as preservation of glomer-ular and peritubular capillary networks with no evidence ofvascular leakage [45]. On the other hand, activation of theHIF system in podocytes induced by VHL knockout wasrecently reported to result activation and proliferation ofpodocytes and resulted in a pathology resembling rapidprogressive glomerulonephritis [46]. Moreover, there isevidence that HIF may also promote renal fibrosis [47] and
1328 J Mol Med (2007) 85:1325–1330

thus the net balance of beneficial and potential adverseeffects of HIF activation may have to be carefully estab-lished under conditions of long-term intervention.
Conclusion
The kidney is sensitive to changes in oxygen delivery.While this sensitivity makes the kidney an appropriateorgan to produce EPO on demand for oxygen supply, it alsorenders the kidney prone to hypoxic injury. Hypoxia plays acrucial role in the pathogenesis of both acute and CKD andis a good target of therapeutic approaches. HIF, the masterswitch of hypoxic adaptation responses, is an apparentlyideal target for future therapies aiming at improving oxygensupply and hypoxia tolerance of the kidney. On the otherhand, continuous activation of the HIF system in tumorspromotes their growth and some other diseases in whichhypervascularity plays a devastating role, however, andtherapeutic utilization of HIF activation may require thepharmacological optimization.
Acknowledgement This work was supported in part by researchgrants from Grant-in-Aid for Scientific Research from Japan Societyfor the Promotion of Science (Grants 19390228).
References
1. Nangaku M, Eckardt KU (2006) Pathogenesis of renal anemia.Semin Nephrol 26:261–268
2. Koury ST, Koury MJ, Bondurant MC, Caro J, Graber SE (1989)Quantitation of erythropoietin-producing cells in kidneys of miceby in situ hybridization: Correlation with hematocrit, renalerythropoietin mRNA and serum erythropoietin concentration.Blood 74:645
3. Bachmann S, Le Hir M, Eckardt KU (1993) Co-localization oferythropoietin mRNA and ecto-5′-nucleotidase immunoreactivityin peritubular cells of rat renal cortex indicates that fibroblastsproduce erythropoietin. J Histochem Cytochem 41:335
4. Maxwell PH, Osmond MK, Pugh CW, Heryet A, Nicholls LG,Tan CC, Doe BG, Ferguson DJ, Johnson MH, Ratcliffe PJ (1993)Identification of the renal erythropoietin-producing cells usingtransgenic mice. Kidney Int 44:1149
5. Semenza GL, Wang GL (1992) A nuclear factor induced byhypoxia via de novo protein synthesis binds to the humanerythropoietin gene enhancer at a site required for transcriptionalactivation. Mol Cell Biol 12:5447
6. Wang GL, Semenza GL (1993) Characterization of hypoxia-inducible factor 1 and regulation of DNA binding activity byhypoxia. J Biol Chem 268:21513
7. Beck I, Weinmann R, Caro J (1993) Characterization of hypoxia-responsive enhancer in the human erythropoietin gene showspresence of hypoxia-inducible 120-kD nuclear DNA-bindingprotein in erythropoietin-producing and nonproducing cells.Blood 82:704
8. Wiesener MS, Jurgensen JS, Rosenberger C, Scholze CK,Horstrup JH, Warnecke C, Mandriota S, Bechmann I, Frei UA,Pugh CW, Ratcliffe PJ, Bachmann S, Maxwell PH, Eckardt KU
(2003) Widespread hypoxia-inducible expression of HIF-2alphain distinct cell populations of different organs. FASEB J 17:271
9. Makino Y, Cao R, Svensson K, Bertilsson G, Asman M, TanakaH, Cao Y, Berkenstam A, Poellinger L (2001) Inhibitory PASdomain protein is a negative regulator of hypoxia-inducible geneexpression. Nature 414:550
10. Warnecke C, Griethe W, Weidemann A, Jurgensen JS, Willam C,Bachmann S, Ivashchenko Y, Wagner I, Frei U, Wiesener M,Eckardt KU (2003) Activation of the hypoxia-inducible factor-pathway and stimulation of angiogenesis by application of prolylhydroxylase inhibitors. FASEB J 17:1186
11. Rosenberger C, Mandriota S, Jurgensen JS, Wiesener MS,Horstrup JH, Frei U, Ratcliffe PJ, Maxwell PH, Bachmann S,Eckardt KU (2002) Expression of hypoxia-inducible factor-1alphaand -2alpha in hypoxic and ischemic rat kidneys. J Am SocNephrol 13:1721
12. Morita M, Ohneda O, Yamashita T, Takahashi S, Suzuki N,Nakajima O, Kawauchi S, Ema M, Shibahara S, Udono T, TomitaK, Tamai M, Sogawa K, Yamamoto M, Fujii-Kuriyama Y (2003)HLF/HIF-2alpha is a key factor in retinopathy of prematurity inassociation with erythropoietin. EMBO J 22:1134
13. Gruber M, Hu CJ, Johnson RS, Brown EJ, Keith B, Simon MC(2006) Acute postnatal ablation of Hif-2alpha results in anemia.Proc Natl Acad Sci USA 104:2301
14. Rankin EB, Biju MP, Liu Q, Unger TL, Rha J, Johnson RS,Simon MC, Keith B, Haase VH (2007) Hypoxia-inducible factor-2 (HIF-2) regulates hepatic erythropoietin in vivo. J Clin Invest117:1068
15. Rolfs A, Kvietikova I, Gassmann M, Wenger RH (1997) Oxygen-regulated transferrin expression is mediated by hypoxia-induciblefactor-1. J Biol Chem 272:20055
16. Peyssonnaux C, Zinkernagel AS, Schuepbach RA, Rankin E,Vaulont S, Haase VH, Nizet V, Johnson RS (2007) Regulation ofiron homeostasis by the hypoxia-inducible transcription factors(HIFs). J Clin Invest 117:1926
17. Devarajan P (2006) Update on mechanisms of ischemic acutekidney injury. J Am Soc Nephrol 17:1503
18. Tanaka T, Miyata T, Inagi R, Kurokawa K, Adler S, Fujita T,Nangaku M (2003) Hypoxia-induced apoptosis in culturedglomerular endothelial cells: involvement of mitochondrial path-ways. Kidney Int 64:2020
19. Manotham K, Tanaka T, Matsumoto M, Ohse T, Inagi R, MiyataT, Kurokawa K, Fujita T, Ingelfinger JR, Nangaku M (2004)Transdifferentiation of cultured tubular cells induced by hypoxia.Kidney Int 65:871
20. Norman JT, Clark IM, Garcia PL (2000) Hypoxia promotesfibrogenesis in human renal fibroblasts. Kidney Int 58:2351
21. Norman JT, Orphanides C, Garcia P, Fine LG (1999) Hypoxia-induced changes in extracellular matrix metabolism in renal cells.Exp Nephrol 7:463
22. Willam C, Warnecke C, Schefold JC, Kugler J, Koehne P, Frei U,Wiesener M, Eckardt KU (2006) Inconsistent effects of acidosison HIF-alpha protein and its target genes. Pflugers Arch 451:534
23. Lameire N, Van Biesen W, Vanholder R (2005) Acute renalfailure. Lancet 365:417
24. Abuelo JG (2007) Normotensive ischemic acute renal failure. NEngl J Med 357:797
25. Rosenberger C, Heyman SN, Rosen S, Shina A, Goldfarb M,Griethe W, Frei U, Reinke P, Bachmann S, Eckardt KU (2005)Up-regulation of HIF in experimental acute renal failure: evidencefor a protective transcriptional response to hypoxia. Kidney Int67:531
26. Rosenberger C, Rosen S, Shina A, Bernhardt W, Wiesener MS,Frei U, Eckardt KU, Heyman SN (2006) Hypoxia-induciblefactors and tubular cell survival in isolated perfused kidneys.Kidney Int 70:60
J Mol Med (2007) 85:1325–1330 1329

27. Tanaka T, Kojima I, Ohse T, Inagi R, Miyata T, Ingelfinger JR,Fujita T, Nangaku M (2005) Hypoxia-inducible factor modulatestubular cell survival in cisplatin nephrotoxicity. Am J PhysiolRenal Physiol 289:F1123
28. Kudo Y, Kakinuma Y, Iguchi M, Sato T, Sugiura T, Furihata M,Shuin T (2007) Modification in the von Hippel-Lindau protein isinvolved in the progression of experimentally induced ratglomerulonephritis. Nephron Exp Nephrol 106:e97
29. Nangaku M (2006) Chronic hypoxia and tubulointerstitial injury:a final common pathway to end-stage renal failure. J Am SocNephrol 17:17
30. Eckardt KU, Bernhardt WM, Weidemann A, Warnecke C,Rosenberger C, Wiesener MS, Willam C (2005) Role of hypoxiain the pathogenesis of renal disease. Kidney Int 99(Suppl):S46
31. Matsumoto M, Tanaka T, Yamamoto T, Noiri E, Miyata T, InagiR, Fujita T, Nangaku M (2004) Hypoperfusion of peritubularcapillaries induced chronic hypoxia prior to progression oftubulointerstitial injury in a progressive model of rat glomerulo-nephritis. J Am Soc Nephrol 15:1574
32. Bernhardt WM, Wiesener MS, Weidemann A, Schmitt R, WeichertW, Lechler P, Campean V, Ong AC, Willam C, Gretz N, EckardtKU (2007) Involvement of hypoxia-inducible transcription factorsin polycystic kidney disease. Am J Pathol 170:830
33. Izuhara Y, Nangaku M, Inagi R, Tominaga N, Aizawa T,Kurokawa K, van Ypersele de Strihou C, Miyata T (2005)Renoprotective properties of angiotensin receptor blockers beyondblood pressure lowering. J Am Soc Nephrol 16:3631
34. Palm F, Cederberg J, Hansell P, Liss P, Carlsson PO (2003)Reactive oxygen species cause diabetes-induced decrease in renaloxygen tension. Diabetologia 46:1153
35. Ries M, Basseau F, Tyndal B, Jones R, Deminiere C, Catargi B,Combe C, Moonen CW, Grenier N (2003) Renal diffusion andBOLD MRI in experimental diabetic nephropathy. Blood oxygenlevel-dependent. J Magn Reson Imaging 17:104
36. Tanaka T, Miyata T, Inagi R, Fujita T, Nangaku M (2004)Hypoxia in renal disease with proteinuria and/or glomerularhypertension. Am J Pathol 165:1979
37. Tanaka T, Kato H, Kojima I, Ohse T, Son D, Kawakami T,Yatagawa T, Inagi R, Fujita T, Nangaku M (2006) Hypoxia and
expression of hypoxia-inducible factor in the aging kidney. JGerontol A Biol Sci Med Sci 61A:795
38. Schofield CJ, Ratcliffe PJ (2004) Oxygen sensing by HIFhydroxylases. Nat Rev Mol Cell Biol 5:343
39. Gardner HF (1953) The use of cobaltous chloride in the anemiaassociated with chronic renal disease. J Lab Clin Med 41:56
40. Matsumoto M, Makino Y, Tanaka T, Tanaka H, Ishizaka N, NoiriE, Fujita T, Nangaku M (2003) Induction of renoprotective geneexpression by cobalt ameliorates ischemic injury of the kidney inrats. J Am Soc Nephrol 14:1825
41. Bernhardt WM, Campean V, Kany S, Juergensen J-S, WeidemannA, Warnecke C, Arend M, Klaus S, Gunzler V, Amann K, WillamC, Wiesener MS, Eckardt K-U (2006) Preconditional activation ofhypoxia-inducible factors ameliorates ischemic acute renal failure.J Am Soc Nephrol 17:1970
42. Weidemann A, Bernhardt WM, Klanke B, Daniel C, Buchholz B,Campean V, Amann K, Warnecke C, Wiesener MS, Eckardt KU,Willam C (2007) HIF-activation protects from cisplatin-inducedacute toxic kidney injury. J Am Soc Nephrol (in press)
43. Kudo Y, Kakinuma Y, Mori Y, Morimoto N, Karashima T,Furihata M, Sato T, Shuin T, Sugiura T (2005) Hypoxia-induciblefactor-1alpha is involved in the attenuation of experimentallyinduced rat glomerulonephritis. Nephron Exp Nephrol 100:95
44. Tanaka T, Matsumoto M, Inagi R, Miyata T, Kojima I, Ohse T,Fujita T, Nangaku M (2005) Induction of protective genes bycobalt ameliorates tubulointerstitial injury in the progressive Thy1nephritis. Kidney Int 68:2714
45. Tanaka T, Kojima I, Ohse T, Ingelfinger JR, Adler S, Fujita T,Nangaku M (2005) Cobalt promotes angiogenesis via hypoxia-inducible factor and protects tubulointerstitium in the remnantkidney model. Lab Invest 85:1292
46. Ding M, Cui S, Li C, Jothy S, Haase V, Steer BM, Marsden PA,Pippin J, Shankland S, Rastaldi MP, Cohen CD, Kretzler M,Quaggin SE (2006) Loss of the tumor suppressor Vhlh leads toupregulation of Cxcr4 and rapidly progressive glomerulonephritisin mice. Nat Med 12:1081
47. Higgins DF, Biju MP, Akai Y, Wutz A, Johnson RS, Haase VH(2004) Hypoxic induction of Ctgf is directly mediated by Hif-1.Am J Physiol Renal Physiol 287:F1223
1330 J Mol Med (2007) 85:1325–1330

REVIEW
Harnessing hypoxic adaptation to prevent, treat,and repair stroke
Rajiv R. Ratan & Ambreena Siddiq & Natalya Smirnova &
Ksenia Karpisheva & Renee Haskew-Layton &
Stephen McConoughey & Brett Langley &
Alvaro Estevez & Patricio T. Huerta & Bruce Volpe &
Sashwati Roy & Chandan K. Sen & Irina Gazaryan &
Sunghee Cho & Matthew Fink & Joseph LaManna
Received: 9 October 2007 /Revised: 25 October 2007 /Accepted: 29 October 2007 / Published online: 28 November 2007# The Author(s) 2007
Abstract The brain demands oxygen and glucose to fulfillits roles as the master regulator of body functions as diverseas bladder control and creative thinking. Chemical andelectrical transmission in the nervous system is rapidlydisrupted in stroke as a result of hypoxia and hypoglyce-mia. Despite being highly evolved in its architecture, thehuman brain appears to utilize phylogenetically conservedhomeostatic strategies to combat hypoxia and ischemia.Specifically, several converging lines of inquiry havedemonstrated that the transcription factor hypoxia-inducible
factor-1 (HIF1-1) mediates the activation of a large cassetteof genes involved in adaptation to hypoxia in survivingneurons after stroke. Accordingly, pharmacological ormolecular approaches that engage hypoxic adaptation atthe point of one of its sensors (e.g., inhibition of HIF prolyl4 hydroxylases) leads to profound sparing of brain tissueand enhanced recovery of function. In this review, wediscuss the potential mechanisms that could subserveprotective and restorative effects of augmenting hypoxicadaptation in the brain. The strategy appears to involveHIF-dependent and HIF-independent pathways and morethan 70 genes and proteins activated transcriptionally andpost-transcriptionally that can act at cellular, local, andsystem levels to compensate for oxygen insufficiency. Thebreadth and depth of this homeostatic program offers ahopeful alternative to the current pessimism towards stroketherapeutics.
Keywords Brain . Stroke . Hypoxia . HIF .
HIF prolyl hydroxylase . Therapeutics
Stroke is defined as injury to the brain accruing from avascular etiology. Strikingly, it has emerged as the thirdleading cause of death and the leading cause of disability inthe USA. Accordingly, the estimated financial costs ofstroke are more than 50 billion dollars a year in the USAalone. These financial costs do not begin to tell the story ofthe personal suffering that amasses from the silent epidemicof stroke disability—over 5 million Americans face thechallenges of handicaps from stroke each day. Therecognition of stroke as a leading age-associated publichealth issue has led the government and the pharmaceuticalindustry to expend enormous resources on developing
J Mol Med (2007) 85:1331–1338DOI 10.1007/s00109-007-0283-1
R. R. Ratan :A. Siddiq :N. Smirnova :K. Karpisheva :R. Haskew-Layton : S. McConoughey :B. Langley :A. Estevez :P. T. Huerta : B. Volpe : I. Gazaryan : S. ChoWinifred Masterson Burke Medical Research Institute,White Plains, NY 10605, USA
R. R. Ratan :A. Siddiq :N. Smirnova :K. Karpisheva :R. Haskew-Layton : S. McConoughey :B. Langley :A. Estevez :P. T. Huerta : B. Volpe : I. Gazaryan : S. Cho :M. FinkDepartment of Neurology and Neuroscience,Weill Medical College of Cornell University,New York, NY 10016, USA
S. Roy : C. K. SenDepartment of Surgery, Ohio State University Medical Center,512 Davis Heart and Lung Research Institute,Columbus, OH 43210, USA
J. LaMannaDepartment of Neurology, Case Western Reserve University,Cleveland, OH 44106-4938, USA
R. R. Ratan (*)Burke-Cornell Medical Research Institute,785 Mamaroneck Avenue,White Plains, NY 10605, USAe-mail: [email protected]

interventions in the form of drugs that minimize braindamage associated with stroke. Despite their promise, theseefforts have been disappointing and have left a nearlyindelible sense of frustration on the biomedical researchcommunity [1]. In this chapter, we will discuss thepathophysiology of stroke with particular attention to oneof its primary mediators, hypoxia, and attempt to revive asense of optimism and enthusiasm for stroke therapeuticsmoving forward.
Ischemia is a process in which perfusion to tissue iscritically reduced creating a deficit in necessary brain fuels.The brain is highly vulnerable to ischemia because theeloquent functions it is assigned to carry out, in thepluralistic society of organ functions, depend integrally onenergy—specifically adenosine triphosphate (ATP). Thebrain comprises only 2% of body weight, but it utilizesnearly 20% of cardiac output to achieve its supply ofessential nutrients including oxygen and glucose. Abnormalcentral nervous system (CNS) symptoms begin to manifestat 40–50% of normal resting hemispheric cerebral bloodflow resulting in slowing of the EEG, attenuation of evokedpotentials, and reduction in the membrane potential inindividual cortical neurons [2]. The resting membranepotential must be maintained to allow proper neuronalfunction, including synaptic activity and axonal conduction.Once the neuronal membrane potential begins to dissipate,
neuronal function ceases. It is important to note that ATPlevels at this point may be normal or only slightly reduced[3]. The reason for this inordinate sensitivity is not entirelyclear but is likely related to the Km of neurotransmittersystems for ATP or their exquisite sensitivity to tissueacidosis [4]. Gross deterioration and damage requires evenmore severe reductions in blood flow to 20–30% of normalresting hemispheric cerebral blood flow (Fig. 1). With thislevel of ischemia, a deterioration of ionic membranegradients ensues, and the tissue begins to accumulatehydrogen ions (acidosis) [5]. Changes in ionic fluxes likelyaccrue directly from a reduction of intracellular ATP, afailure of the Na+/K+ATPase activity, and increases inintracellular Na+ and extracellular K+. The failure of ionichomeostasis reflects loss of activity of multiple transportersthat normally maintain the electrochemical gradients nec-essary for normal neuronal signal transduction [6, 7].Among the ions deregulated, intracellular calcium appearsto play a critical role in further ion dyshomeostasis via thecalmodulin-dependent activation of neuronal nitric oxidesynthase (nNOS) [8–10]. Increased nNOS activity leads toincrease in the ambient levels of neuronal nitric oxide (NO)[11]. Changes in NO coupled with ischemia-associatedincreases in cytosolic and mitochondrially derived super-oxide, combine to form toxic peroxynitrite. Peroxynitritecan trigger cell death pathways via DNA damage, poly
Fig. 1 Neuronal hypoxia leads to calcium overload and production offree radicals. Stroke is associated with a decrease in cerebral bloodflow to the brain. The consequent loss of metabolic fuels leads tofailure of sodium pumps leading to an intracellular accumulation ofsodium and calcium, depolarization, and activation of voltagesensitive and ligand gated [N-methyl-D-aspartate (NMDA)] ionchannels. Increased in calcium in microdomains near the NMDAreceptor leads to activation of neuronal nitric oxide synthase. Globaldysregulation of calcium in the neuron leads to mitochondrialoverload and superoxide production. Nitric oxide and superoxide
combine to form peroxynitrite. Peroxynitrite can damage DNAleading to PARP activation and consumption of NAD+. It can alsoactivate TRPM2/7 channels leading to further calcium dysregulation.Hypoxia is sensed by decreased activity of HIF prolyl 4 hydroxylasesthat can lead to activation genetic responses capable of compensatingfor the sentinel metabolic stress (decreased cerebral blood flow).Decrease HIF PHD activity can also prevent death via HIF-independent pathways. Acidosis and ROS can also combine withHIF regulated prodeath proteins to trigger cell death
1332 J Mol Med (2007) 85:1331–1338

(ADP-ribose)polymerase (PARP) activation, liberation ofapoptosis-inducing factor (AIF) from the mitochondria, andactivation of death signaling pathways leading to apoptosis[12, 13]; alternatively, non-selective cation channels such asTRPM2 and TRPM7 can be activated to ensure sustainedcalcium overload and death [14]. Extracellular acidosis isalso postulated to activate acid sensing ion channels, whichalso contribute to destruction of the normal ionic environ-ment [15]. As one can appreciate from a partial descriptionof the sequence of events after stroke that occur in theneuron alone, targeting a single molecule in the complexparallel and serial pathways of acute hypoxia-ischemia willnot maintain neuronal survival (Fig. 2). It is also unlikely toenhance the ability of energy-thirsty neurons to carry outtheir sophisticated roles in maintaining posture, movement,sequencing language, or making critical executive deci-
sions. Therefore, how might we move forward? One of themost important advances in the treatment of complexmedical problems has been the discovery that multimodaltherapies can greatly enhance therapeutic efficiency. Treat-ment of cancer, HIV infection, and tuberculosis withmultimodal therapies yields results that are not obtainedwith the application of single therapeutic agents.
As stroke does not represent a single homogeneouscategory of injury, it is also a poor candidate for a singleapproach to treatment [16]. Challenges involved in promot-ing recovery from stroke involve reducing the extent ofdamage that occurs in acute injury. Moreover, many differentkinds of damage are found in individuals with stroke rangingfrom necrotic, apoptotic, or parthanatotic death of neurons[17, 18], demyelination of otherwise functional axons [19],and transection of axons and subsequent loss of criticalneuronal populations [20]. Acute injury itself is extremelycomplex, including waves of cell death, inflammatoryresponses, edema, and scarring. Indeed, experimental studieshave continued to demonstrate that interventions that targetsingle aspects of the complex cascade, including blockingion gradients, scavenging free radicals, or enhancing growthfactors on their own are insufficient to overcome theconsiderable barriers to protection against hypoxia andischemia in acute stroke [21].
Instructive data from the experimental paradigm ofischemic preconditioning has pointed the way towardsnovel strategies that can address the heterogeneity andcomplexity inherent in stroke pathophysiology [22]. Ani-mals subjected to a non-lethal exposure to hypoxia arefound to be more resistant to a host of subsequent lethalstresses, including cerebral ischemia. The mechanism bywhich a sublethal exposure to hypoxia can render the brainresistant to cerebral ischemia and a host of other insults is atopic of active investigation and debate. However, onepoint appears irrefutable: The tolerance that develops after ashort duration of hypoxia involves not only the activationor inactivation of pre-existing proteins but also de novogene expression [23, 24]. These transcriptional and post-transcriptional mechanisms reflect a cassette of genes andproteins that work collectively at the cellular, local, andsystemic levels to compensate for a discrepancy in oxygensupply and demand. The findings suggest that underconditions where adaptive homeostatic mechanisms areappropriately engaged, damage to the brain can besubstantially lessened or even prevented (Fig. 3). Strokeis, almost by definition, a failure of homeostasis. Accord-ingly, identification of small molecules that augmentendogenous adaptive strategies provides a mechanism totilt the balance away from cell damage and death andtoward cell survival and repair (Fig. 3).
Examination of adaptive responses to hypoxia in thecentral nervous system has affirmed that the family of
Fig. 2 Contribution of neurons and astrocytes in mediating excito-toxic neuronal death. 1 Loss of ATP in ischemia leads to inhibition ofthe Na+/K+ATPase and subsequent collapse of normal ionic gradients.2 In turn, neuronal membrane depolarization activates voltagesensitive Ca2+ channels, which increase intracellular Ca2+ andstimulate vesicular glutamate release. Severe loss of ionic gradientsfound in certain ischemic regions may also lead to the reversal of 3neuronal specific and 4 astrocyte specific glutamate transporters,which in the reverse mode act to release glutamate into theextracellular space. 5 Cell swelling in cerebral ischemia, which ismainly localized to astrocytes, likely activates swelling sensitive anionchannels, referred to as volume regulated anion channels (VRACs).VRACs, which are permeable to organic osmolytes, contribute toglutamate release predominantly in the ischemic penumbra. 6Glutamate regulated NMDA receptors (NMDA-R) are activated by(1) extracellular glutamate and (2) release of Mg2+ from its pore aftermembrane depolarization (in part due to activation of glutamateregulated AMPA receptors, not shown). 7 NMDA-Rs are permeable toCa2+ and as such, overabundant NMDA-R activation leads to anintracellular Ca2+ overload. This increase in intracellular Ca2+ thencontributes to neuronal death via several mechanisms
J Mol Med (2007) 85:1331–1338 1333

transcriptional regulators known as the hypoxia-induciblefactors are central players [25–27]. HIF-1 was purified andcloned as a result of a search for proteins that regulate theexpression of genes involved in hypoxic adaptation, such aserythropoietin, vascular endothelial growth factor, and
glycolytic enzymes [27]. HIF is a heterodimeric transcrip-tional activator composed of an inducible HIF-1α subunitand a constitutively expressed HIF-1β subunit [28, 29].HIF-1α stability is regulated via the activity of a class ofoxygen, 2-oxoglutarate, and iron dependent enzymesknown as the HIF prolyl-4 hydroxylases (HIF PHDs,Fig. 4) [30]. As intracellular oxygen levels drop below acritical threshold, these enzymes fail to hydroxylate HIF-1α. As hydroxylation is required for the recruitment of theconstitutively active E3 Ubiquitin Ligase, Von HippelLindau protein, HIF-1α becomes stabilized. HIF-1α canpartner with its constitutively expressed but induced partnerHIF-1β and translocate to the nucleus to regulate theexpression of a host of genes involved in hypoxicadaptation [31]. Consistent with this model, several groupshave shown that HIF-1α immunoreactivity increases inareas of the cortex that become hypoxic due to stroke [25,32] An unanswered question has been whether HIF is alsoupregulated in areas connected to but remote from the siteof ischemia. Indeed, neurons projecting to an area ofinfarction are at risk for cell death due to a loss of trophicsupport from their damaged targets. Moreover, neuronsprojecting from an area of damage are at risk for cell deathdue to a loss of trophic excitatory input from their targets.An elegant recent study in non-human primates demon-strated a dramatic increase in neuronal immunoreactivityfor HIF-1α and one of its target genes in the infarct andperi-infarct region [33, 34]. Indeed, the neuronal immuno-reactivity for HIF-1α increased from less than 5% to nearly90% in both regions. Interestingly, areas remote to the areaof hypoxia and ischemia also experience increased HIF andvascular endothelial growth factor (VEGF) levels but to aquantitatively much smaller extent. Together, the publishedrodent and primate histochemical studies support thehypothesis that increased HIF protein levels resulting fromdirect hypoxia and non-hypoxic mediators such as IGF-1are a marker for surviving and regenerating neurons afterischemia [32].
Pharmacological and molecular studies have providedadditional support for the notion that stabilization of HIF-1after ischemia is associated with enhanced survival ofneurons. Small molecule hypoxia mimics, deferoxamine,and cobalt chloride, were found to stabilize HIF-1α levels,increase DNA binding to a cognate hypoxia responseelement, and increase the expression of HIF target genesin vitro cultured neurons (Zaman et al. [31]) and in vivo inthe intact brain (Fig. 4; [35]). Pretreatment or post-treatment with desferrioxamine or cobalt chloride resultedin reduced cell loss in models of focal or global ischemia invitro and in vivo [25, 31, 36–39]. Subsequent studies haveconfirmed that hypoxia, iron chelation, or cobalt chlorideappear to confer protective effects on neurons via theirability to inhibit HIF PHDs [35]. Emerging data indicate
Fig. 3 Drugs that augment endogenous homeostatic mechanisms willmore effectively neutralize the heterogeneity inherent in strokepathophysiology. As these pathways are already used by the body,their activation can occur with decreased threat of toxicity. The term“homeostasis” was coined by Walter Canon in the early twentiethcentury. It refers to the innate tendency of organisms to mobilizeadaptive responses physiological and pathological perturbations thatultimately return the system to a set point that is consistent withsurvival. a The experimental paradigm of “ischemic preconditioning”has shown that a short, sublethal exposure to hypoxia, or hypoxia-ischemia induces homeostatic responses that make the organism“immune” or “tolerant” to a lethal ischemic insult. Mechanisticstudies have revealed that tolerance is the consequence of activationof pre-existing proteins and de novo gene expression. b According tothis model, stroke can be conceptualized as a failure of homeostasis.Consequently, neurons die and the brain is permanently damaged.c By extension, small molecules that engage homeostatic mechanismsdesigned to alleviate hypoxia/ischemia early or enhance theiractivation should tip the balance away from cell death and towardsurvival and repair. Such small molecules are currently beingdeveloped and represent a new generation of stroke therapies
1334 J Mol Med (2007) 85:1331–1338

that inhibition of each of the three of the HIF PHD isoforms(1–3) may lead to cell survival in the nervous system. Ofnote, inhibition of each isoform may enhance survival viadistinct but mutually supportive pathways.
Our studies demonstrate that pharmacological inhibition ofPHDs, in vitro, leads to inhibition of oxidative stress-induceddeath, an established mediator of neural injury and death instroke [35]. More recent studies indicate that molecularsuppression of HIF PHD 1 alone can mimic this effect(Siddiq et al., unpublished observations). Interestingly, whileHIF-1, HIF-2, and cAMP response element-binding proteinare stabilized by PHD inhibition in neurons or astrocytes, themolecular deletion or inhibition of each of these threetranscription factors fails to abrogate the protective effectsof PHD inhibition suggesting that other, as yet unidentified,pathways are important in protection (Siddiq et al., unpub-lished observations). Studies are underway to clarify whethermolecular deletion of PHD1 selectively in the CNS confersresistance to stroke in a HIF-independent manner.
In contrast to PHD1, PHD2 appears to be the isoformmost important for tagging HIF for degradation. Deletion ofPHD2 but not PHD1 or PHD3 results in increased HIF andVEGF protein and consequent angiogenesis in multipleorgans including the brain [40]. Underscoring PHD2’simportant role in HIF signaling, the expression level ofthis isoform is significantly higher as compared to itsbrethren [41]. Ischemia-induced PHD2 inhibition stabilizesHIF and enhances expression of genes that mediate cellular(e.g., glycolytic enzymes), local (vascular endothelialgrowth factor), and systemic (erythropoietin, Epo) adaptiveresponses to hypoxia or hypoxia-ischemia [42]. While Epois best known as a hematopoietic growth factor that canenhance oxygen carrying capacity to tissue, it also hasorgan-autonomous roles in the nervous system. Epo isproduced in astrocytes in response to hypoxia or ischemiaand mediates a number of responses critical to strokeprevention and recovery [43, 44]. Epo can inhibit neuronaldeath due to excitotoxicity or growth factor deprivation[45–49]. It can also stimulate the proliferation of neuralprogenitors in the germinal zones of the brain and enhance
Fig. 4 HIF prolyl 4 hydroxylases sense hypoxia and transduce acritical insufficiency in oxygen in the brain into transcriptional andpost-transcriptional signal changes that mediate protection and repair.Hypoxia regulates the activity of HIF PHDs via direct or indirectmechanisms; production of peroxide via reduction in mitochondrialATP production and electron transport chain (ETC) impairment (1, 2);accumulation of the tricarboxylic cycle (TCA) intermediates succinateand fumarate (3); or direct inhibition of the activity of PHDs due tolack of oxygen (4). Accumulation of hydrogen peroxide, succinate orfumarate can inhibits the activity of PHDs by competing with 2-oxoglutarate or by oxidizing the active site iron (5). Among itsnumerous downstream effects, inhibition of HIF PHD activity leads tostabilization of HIF-1α. Stabilized HIF-1α dimerizes with HIF-1β inthe nucleus and increases gene transcription (6)
�
J Mol Med (2007) 85:1331–1338 1335

their migration to sites of injury [50, 51]. The concomitantHIF-dependent increase in VEGF expression provides,among other things, the appropriate angiogenic niche forneural progenitors to survive [52]. New neurons could mediaterecovery responses via paracrine effects or due to direct par-ticipation in functional circuits. A recent study affirmed therequisite role for HIF transcription factors in mediating someof the salutary effects of low molecular weight PHDinhibitors given after cerebral ischemia [53]. Availableevidence suggests that these inhibitors are likely targetingPHD2 to induce HIF and its gene targets in the CNS.
Inhibition of the third isoform of PHDs (PHD3) byhypoxia or hypoxia mimetics has also been linked toneuronal survival [54]. Freeman and colleagues firstidentified PHD3 (then known as SM-20) as a messageand protein that is highly upregulated in sympatheticneurons after growth factor deprivation. Subsequent studieshave shown that pharmacological or molecular deletion ofHIF PHD3 prevents apoptosis associated with trophic lossin neurons and that the protection is HIF independent [55].As target (post-synaptic) derived trophic factors appear tobe lost after stroke and result in cell death remote from theinfarct site, HIF PHD3 inhibition may be a rational strategyfor maintaining the viability of these neurons in evolving orstable stroke.
From the above discussion, a model begins to emergewhereby inhibition of HIF PHD1, 2, or 3 by hypoxia orconsequences of hypoxia can mediate HIF-dependent andHIF-independent compensatory responses via distinct butclearly reinforcing mechanisms. How does one reconcilethis model with observations from several laboratories,including our own, that HIF PHD inhibition or HIFactivation leads to the upregulation of prodeath, Bcl-2family proteins such as Puma, Bnip3, and NIX [56]?Moreover, constitutive HIF activation has been associatedwith potentiation and suppression of death [56]. Thesefindings appear to make perfect sense if one considersapoptosis as an adaptive response to stress. After stroke,oxygen may fall below a critical level rendering the prolylhydroxylases inactive. Accordingly, HIF is stabilized and ittranslocates to the nucleus to upregulate genes involved inpreventing and executing death. The anthropomorphizedcell can be visualized stepping to the edge of a steep cliff inresponse to a potentially lethal stress (Fig. 5). If adequatecompensation for hypoxia occurs, prodeath proteins are notactivated and the cell survives as a functional component ofa complex neural network—the cell moves away from thecliff to survival promoting, terra firma. By contrast, ifoxidative stress, hypoxia, and acidosis dominate, indicatingthat compensatory mechanisms have failed, then proapop-
Fig. 5 Adaptation to hypoxia-cell fate and beyond. Expression of HIF inneurons leads to the constitutive expression of proteins associated withcell death (BNIP3, NIX, and PUMA) and cell survival (VEGF, glycolyticenzymes, Epo, and p21 waf1/cip1). Similar prodeath gene expression isfound in neurons exposed to hypoxia or hypoxia mimetics despite theabsence of cell death. It appears the oxygen “starved” neurons havestepped to the edge of the cliff. If during the ensuing hours to days theneuron becomes acidotic or oxidized, then prodeath proteins such as
BNIP3 undergo a conformational change, insertion into the mitochon-drial membrane, release of apoptotic effectors, and death. By contrast, ifthe survival genes are effective in neutralizing the hypoxic stress (e.g., noacidosis or oxidative stress), then the death genes never get activated. Ourstudies indicate that antioxidants, short interfering RNAs to BNIP3 orinhibitors of the HIF prolyl 4 hydroxylases tip the balance towardsurvival (away from the cliff)
1336 J Mol Med (2007) 85:1331–1338

totic proteins such as BNIP3 undergo a conformationalchange, insertion into the mitochondrial membrane andactivation of permeabilization transition and release ofapoptotic effectors [57–59]. In the latter scenario, the celljumps off the cliff to preserve limiting resources for itsneighbors. The model suggests that state changes in the cell(e.g., redox and pH) that follow the initial ischemic insultwill determine the fate of the tissue and potential forrecovery (Fig. 5). Of note, low molecular weight or peptideinhibitors of the PHDs, antioxidants, and a small interferingRNA to BNIP3 prevent the prodeath effects of HIF (Aminoet al., personal communication). These findings suggest thatengaging the adaptive response at an upstream point wherestress is detected by the cell (the stress sensor) is going tobe more effective in stemming cell loss and facilitatingrepair than at the point of the transcription factor (HIF). It isour hypothesis that engaging the adaptive response at anupstream point in the pathway results in post-transcriptionalchanges essential for the homeostatic response. Thesechanges in concert with transcriptional changes optimallyalleviate the discrepancy between oxygen supply anddemand.
The model has some clear predictions. First, lowmolecular weight global inhibitors of the HIF prolyl 4hydroxylases will be more effective at preventing injuryand repairing damage after stroke than selective isoforminhibitors. These inhibitors will engage HIF-dependent andHIF-independent pathways at cellular, local, and systemiclevels and ultimately alleviate the discrepancy in nutrientsupply and demand. They can also (via mechanisms that areonly beginning to be defined) divert HIF away from itstendencies as a prodeath transcription factor. The ability ofsingle “drugs” to target an oligopoly of proteins (HIFPHD1–3) to affect a concerted program of neuroprotectioninvolving more than 70 genes and larger number of proteinssuggests a strategy for overcoming the heterogeneityinherent in stroke pathophysiology in the short term. Whilea significant amount of work needs to be done toadequately assess the viability of this strategy for humantherapeutics, the notion of augmenting endogenous adap-tive programs via HIF PHDs to thwart disease continues togain currency.
Acknowledgements The authors wish to thank Gregg Semenza forreagents and intellectual input on all of the studies related to hypoxiain our laboratory. This work was supported by a New York StateCenter of Research Excellence, NIH RO1 (NS 40591, NS46239, andNS37060) and the Adelson Foundation for Neurorehabilitation andRepair.
Open Access This article is distributed under the terms of theCreative Commons Attribution Noncommercial License which per-mits any noncommercial use, distribution, and reproduction in anymedium, provided the original author(s) and source are credited.
References
1. Savitz SI, FisherM (2007) Future of neuroprotection for acute stroke:in the aftermath of the SAINT trials. Ann Neurol 61:396–402
2. Sharbrough FW, Messick JM Jr., Sundt TM Jr. (1973)Correlation of continuous electroencephalograms with cerebralblood flow measurements during carotid endarterectomy. Stroke4:674–683
3. Naritomi H, Sasaki M, Kanashiro M, Kitani M, Sawada T (1988)Flow thresholds for cerebral energy disturbance and Na+ pumpfailure as studied by in vivo 31P and 23Na nuclear magneticresonance spectroscopy. J Cereb Blood Flow Metab 8:16–23
4. Gibson GE, Pulsinelli W, Blass JP, Duffy TE (1981) Braindysfunction in mild to moderate hypoxia. Am JMed 70:1247–1254
5. Hossmann KA, Ophoff BG, Csiba L, Paschen W (1988) RegionalpH and electrolyte homeostasis of cat brain after prolongedischemia. Neurochem Pathol 9:127–137
6. Astrup J, Nordstrom CH, Rehncrona S (1977) Rate of rise inextracellular potassium in the ischemic rat brain and the effect ofpreischemic metabolic rate: evidence for a specific effect ofPhenobarbital. Acta Neurol Scand Suppl 64:148–149
7. Harris RJ, Symon L (1984) Extracellular pH, potassium, andcalcium activities in progressive ischaemia of rat cortex. J CerebBlood Flow Metab 4:178–186
8. Choi DW (1988) Calcium-mediated neurotoxicity: relationship tospecific channel types and role in ischemic damage. TrendsNeurosci 11:465–469
9. Iadecola C, Yang G, Ebner TJ, Chen G (1997) Local andpropagated vascular responses evoked by focal synaptic activityin cerebellar cortex. J Neurophysiol 78:651–659
10. Siesjo BK (1988) Historical overview. Calcium, ischemia, anddeath of brain cells. Ann NY Acad Sci 522:638–661
11. Dawson VL, Dawson TM, London ED, Bredt DS, Snyder SH(1991) Nitric oxide mediates glutamate neurotoxicity in primarycortical cultures. Proc Natl Acad Sci U S A 88:6368–6371
12. Pacher P, Beckman JS, Liaudet L (2007) Nitric oxide andperoxynitrite in health and disease. Physiol Rev 87:315–424
13. Yu SW, Wang H, Poitras MF et al (2002) Mediation of poly(ADP-ribose) polymerase-1-dependent cell death by apoptosis-inducingfactor. Science 297:259–263
14. Aarts MM, Tymianski M (2005) TRPMs and neuronal cell death.Pflugers Arch 451:243–249
15. Xiong ZG, Chu XP, Simon RP (2007) Acid sensing ion channels—novel therapeutic targets for ischemic brain injury. Front Biosci12:1376–1386
16. Lyden P, Wahlgren NG (2000) Mechanisms of action of neuro-protectants in stroke. J Stroke Cerebrovasc Dis 9:9–14
17. Ito N, DeMarco RA, Mailliard RB et al (2007) Cytolytic cells induceHMGB1 release from melanoma cell lines. J Leukoc Biol 81:75–83
18. MacManus JP, Buchan AM (2000) Apoptosis after experimentalstroke: fact or fashion? J Neurotrauma 17:899–914
19. Goldberg JL (2003) How does an axon grow? Genes Dev 17:941–95820. Coleman MP, Perry VH (2002) Axon pathology in neurological
disease: a neglected therapeutic target. Trends Neurosci 25:532–53721. Fisher M, Ratan R (2003) New perspectives on developing acute
stroke therapy. Ann Neurol 53:10–2022. Cho S, Park EM, Zhou P, Frys K, Ross ME, Iadecola C (2005)
Obligatory role of inducible nitric oxide synthase in ischemicpreconditioning. J Cereb Blood Flow Metab 25:493–501
23. Stenzel-Poore MP, Stevens SL, Xiong Z et al (2003) Effect ofischaemic preconditioning on genomic response to cerebralischaemia: similarity to neuroprotective strategies in hibernationand hypoxia-tolerant states. Lancet 362:1028–1037
24. Tang Y, Pacary E, Freret T et al (2006) Effect of hypoxicpreconditioning on brain genomic response before and following
J Mol Med (2007) 85:1331–1338 1337

ischemia in the adult mouse: identification of potential neuro-protective candidates for stroke. Neurobiol Dis 21:18–28
25. Bergeron M, Gidday JM, Yu AY, Semenza GL, Ferriero DM,Sharp FR (2000) Role of hypoxia-inducible factor-1 in hypoxia-induced ischemic tolerance in neonatal rat brain. Ann Neurol48:285–296
26. Semenza GL (2000) Chairman’s summary: mechanisms of oxygenhomeostasis, circa 1999. Adv Exp Med Biol 475:303–310
27. Wang GL, Semenza GL (1993) Characterization of hypoxia-inducible factor 1 and regulation of DNA binding activity byhypoxia. J Biol Chem 268:21513–21518
28. WangGL, Jiang BH, Rue EA, Semenza GL (1995) Hypoxia-induciblefactor 1 is a basic-helix-loop-helix-PAS heterodimer regulated bycellular O2 tension. Proc Natl Acad Sci U S A 92:5510–5514
29. Wang GL, Semenza GL (1995) Purification and characterizationof hypoxia-inducible factor 1. J Biol Chem 270:1230–1237
30. Kaelin WG (2005) The von Hippel-Lindau tumor suppressorprotein: roles in cancer and oxygen sensing. Cold Spring HarbSymp Quant Biol 70:159–166
31. Zaman K, Ryu H, Hall D et al (1999) Protection from oxidativestress-induced apoptosis in cortical neuronal cultures by ironchelators is associated with enhanced DNA binding of hypoxia-inducible factor-1 and ATF-1/CREB and increased expression ofglycolytic enzymes, p21(waf1/cip1), and erythropoietin. J Neuro-sci 19:9821–9830
32. Chavez JC, LaManna JC (2002) Activation of hypoxia-induciblefactor-1 in the rat cerebral cortex after transient global ischemia:potential role of insulin-like growth factor-1. J Neurosci 22:8922–8931
33. Stowe AM, Plautz EJ, Nguyen P, et al. (2007) Neuronal HIF-1alpha protein and VEGFR-2 immunoreactivity in functionallyrelated motor areas following a focal M1 infarct. J Cereb BloodFlow Metab (in press). DOI 10.1038/sj.jcbfm.9600560
34. Stowe AM, Plautz EJ, Eisner-Janowicz I et al (2007) VEGFprotein associates to neurons in remote regions following corticalinfarct. J Cereb Blood Flow Metab 27:76–85
35. Siddiq A, Ayoub IA, Chavez JC et al (2005) Hypoxia-induciblefactor prolyl 4-hydroxylase inhibition. A target for neuroprotec-tion in the central nervous system. J Biol Chem 280:41732–41743
36. Demougeot C, Van Hoecke M, Bertrand N et al (2004)Cytoprotective efficacy and mechanisms of the liposoluble ironchelator 2,2′-dipyridyl in the rat photothrombotic ischemic strokemodel. J Pharmacol Exp Ther 311:1080–1087
37. Demougeot C, Bobillier-Chaumont S, Mossiat C, Marie C,Berthelot A (2004) Effect of diets with different magnesiumcontent in ischemic stroke rats. Neurosci Lett 362:17–20
38. Hamrick SE, McQuillen PS, Jiang X, Mu D, Madan A, FerrieroDM (2005) A role for hypoxia-inducible factor-1alpha indesferoxamine neuroprotection. Neurosci Lett 379:96–100
39. Sorond FA, Ratan RR (2000) Ironing-out mechanisms of neuronalinjury under hypoxic-ischemic conditions and potential role ofiron chelators as neuroprotective agents. Antioxid Redox Signal2:421–436
40. Takeda K, Fong GH (2007) Prolyl hydroxylase domain 2 proteinsuppresses hypoxia-induced endothelial cell proliferation. Hyper-tension 49:178–184
41. Appelhoff RJ, Tian YM, Raval RR et al (2004) Differentialfunction of the prolyl hydroxylases PHD1, PHD2, and PHD3 inthe regulation of hypoxia-inducible factor. J Biol Chem279:38458–38465
42. Natarajan J, Berrar D, Dubitzky W et al (2006) Text mining of full-text journal articles combinedwith gene expression analysis reveals a
relationship between sphingosine-1-phosphate and invasiveness of aglioblastoma cell line. BMC Bioinformatics 7:373
43. Chavez JC, Baranova O, Lin J, Pichiule P (2006) The transcrip-tional activator hypoxia inducible factor 2 (HIF-2/EPAS-1)regulates the oxygen-dependent expression of erythropoietin incortical astrocytes. J Neurosci 26:9471–9481
44. Yeo EJ, Cho YS, Kim MS, Park JW (2007) Contribution of HIF-1alpha or HIF-2alpha to erythropoietin expression: in vivoevidence based on chromatin immunoprecipitation. Ann Hematol87:11–17
45. Cerami A, Brines ML, Ghezzi P, Cerami CJ (2001) Effects ofepoetin alfa on the central nervous system. Semin Oncol 28:66–70
46. Ehrenreich H, Hasselblatt M, Dembowski C et al (2002)Erythropoietin therapy for acute stroke is both safe and beneficial.Mol Med 8:495–505
47. Liu R, Suzuki A, Guo Z, Mizuno Y, Urabe T (2006) Intrinsic andextrinsic erythropoietin enhances neuroprotection against ischemiaand reperfusion injury in vitro. J Neurochem 96:1101–1110
48. Prass K, Scharff A, Ruscher K et al (2003) Hypoxia-inducedstroke tolerance in the mouse is mediated by erythropoietin.Stroke 34:1981–1986
49. Wei L, Han BH, Li Y, Keogh CL, Holtzman DM, Yu SP (2006)Cell death mechanism and protective effect of erythropoietin afterfocal ischemia in the whisker-barrel cortex of neonatal rats. JPharmacol Exp Ther 317:109–116
50. Shingo T, Sorokan ST, Shimazaki T, Weiss S (2001) Erythropoi-etin regulates the in vitro and in vivo production of neuronalprogenitors by mammalian forebrain neural stem cells. J Neurosci21:9733–9743
51. Tsai MS, Hwang SM, Tsai YL, Cheng FC, Lee JL, Chang YJ(2006) Clonal amniotic fluid-derived stem cells express character-istics of both mesenchymal and neural stem cells. Biol Reprod74:545–551
52. Goldman CK, Kendall RL, Cabrera G et al (1998) Paracrineexpression of a native soluble vascular endothelial growth factorreceptor inhibits tumor growth, metastasis, and mortality rate.Proc Natl Acad Sci U S A 95:8795–8800
53. Baranova O, Miranda LF, Pichiule P, Dragatsis I, Johnson RS,Chavez JC (2007) Neuron-specific inactivation of the hypoxiainducible factor 1 alpha increases brain injury in a mouse modelof transient focal cerebral ischemia. J Neurosci 27:6320–6332
54. Lomb DJ, Straub JA, Freeman RS (2007) Prolyl hydroxylaseinhibitors delay neuronal cell death caused by trophic factordeprivation. J Neurochem 103:1897–1906
55. Lee S, Nakamura E, Yang H et al (2005) Neuronal apoptosislinked to EglN3 prolyl hydroxylase and familial pheochromocy-toma genes: developmental culling and cancer. Cancer Cell8:155–167
56. Aminova LR, Chavez JC, Lee J et al (2005) Prosurvival andprodeath effects of hypoxia-inducible factor-1alpha stabilization ina murine hippocampal cell line. J Biol Chem 280:3996–4003
57. Bruick RK (2000) Expression of the gene encoding the proapop-totic Nip3 protein is induced by hypoxia. Proc Natl Acad Sci U SA 97:9082–9087
58. Frazier DP, Wilson A, Graham RM, Thompson JW, BishopricNH, Webster KA (2006) Acidosis regulates the stability, hydro-phobicity, and activity of the BH3-only protein Bnip3. AntioxidRedox Signal 8:1625–1634
59. Kubasiak LA, Hernandez OM, Bishopric NH, Webster KA (2002)Hypoxia and acidosis activate cardiac myocyte death through the Bcl-2 family protein BNIP3. Proc Natl Acad Sci U S A 99:12825–12830
1338 J Mol Med (2007) 85:1331–1338

REVIEW
Hypoxia inducible factor (HIF) function in innate immunityand infection
Annelies S. Zinkernagel & Randall S. Johnson &
Victor Nizet
Received: 14 October 2007 /Revised: 25 October 2007 /Accepted: 26 October 2007 / Published online: 21 November 2007# Springer-Verlag 2007
Abstract The hypoxia-inducible transcription factor (HIF-1α) is a major regulator of energy homeostasis and cellularadaptation to low oxygen stress. Recently, HIF-1α has beendiscovered to function as a global regulator of macrophageand neutrophil inflammatory and innate immune functions,as befits these specialized phagocytic cells who mustoperate effectively in the hypoxic microenvironments ofinfected tissues. This review summarizes current knowl-edge of the role of HIF-1α in mammalian innate immunity,emphasizing insight gained from conditional gene targetingof the transcription factor in the myeloid cell lineage.Dynamic changes in HIF-1α expression in the course ofbacterial, viral, or parasitic infections are outlined andinferences drawn regarding the consequences for pathogenand host. A better understanding of HIF-1α function mayprovide novel and rational approaches for boosting innateimmune function in the therapy of certain complicatedinfectious disease conditions.
Keywords HIF-1 . Hypoxia . Innate Immunity . Phagocyte .
Neutrophil . Macrophage
Introduction
Microorganisms are omnipresent, colonizing the exteriorand interior epithelial surfaces of the human host. Thisconstant interaction leads to many host benefits, forexample vitamin production, but also significant disadvan-tages, such as the risk of infection. To control this fragilebalance, the host has evolved a broad arsenal of innatedefense mechanisms, including physical barrier functions,soluble effectors such as complement and antimicrobialpeptides, and phagocytic cells. The critical role of phag-ocytes in host defense lies in their rapid mobilization andability to recognize and inactivate pathogens independentof prior encounter as required by adaptive immunity.
The principal phagocytes of mammalian innate immuni-ty are cells of the myeloid lineage, monocyte/macrophagesand neutrophils. These short-lived cells are recruited inresponse to alterations in tissue integrity, whether thebyproduct of chemical or physical injury or the spread ofinfectious microorganisms. In concert with vasodilation andincreased vascular permeability, the activated phagocytescontribute to local inflammation. Tissue foci of inflamma-tion are characterized by low levels of oxygen and glucose,together with high concentrations of lactate and reductivemetabolites, including free oxygen radicals [1, 2]. Tomaintain energy homeostasis and carry out their biologicalactivities in these specialized environments, phagocytic celltypes must generate ATP via glycolysis. Because upregu-lation of virtually every enzyme in the glycolytic pathwayis mediated almost exclusively by the hypoxia-induciblefactor-1α (HIF-1α) [3], a role for this transcription factor in
J Mol Med (2007) 85:1339–1346DOI 10.1007/s00109-007-0282-2
DO00282; No of Pages
A. S. Zinkernagel :V. Nizet (*)Division of Pediatric Pharmacology & Drug Discovery,University of California, San Diego School of Medicine,Cellular and Molecular Medicine East, Room 1066,9500 Gilman Drive, MC 0687,La Jolla, CA 92093-0687, USAe-mail: [email protected]
R. S. JohnsonDivision of Biological Sciences, University of California,San Diego,La Jolla, CA 92093, USA
V. NizetSkaggs School of Pharmacy & Pharmaceutical Sciences,University of California, San Diego,La Jolla, CA 92093, USA

supporting phagocyte function during inflammation wasintuitive. In the last few years, genetic tools provided notonly experimental validation of this concept, but uncoveredprofound implications of the HIF-1α control pathway in theoverall regulation of mammalian innate immunity.
HIF-1α and myeloid cell inflammation
HIF-1 is a heterodimeric helix-loop-helix transcription factorwhose expression is regulated by oxygen at the protein level.Protein stability of the α subunit (HIF-1α) is regulated by afamily of oxygen- and iron-dependent prolyl hydroxylases,whose action directs HIF-1α for degradation by theubiquitin–proteasome pathway in a process dependent uponinteraction with von Hippel–Lindau tumor-suppressor pro-tein (vHL). Under hypoxia, prolyl hydroxylase activity isinhibited, HIF-1α accumulates and translocates into thenucleus, where it binds the constitutively expressed HIF-1β(aka ARNT). The resultant heterodimer HIF-1 binds tohypoxic response elements (HREs) of target gene regulatorysequences. Classical HIF-1 target genes include the glyco-lytic enzymes, glucose transporters, erythropoietin, and theangiogenic factor VEGF.
Gene targeting provides invaluable evidence about thefunction of specific mammalian proteins, but globalelimination of HIF-1α in the mouse produced lethalembryonic defects in vascularization and morphologicdevelopment [4–6]. The advent of conditional gene target-ing methodologies allowed tissue-specific deletion offloxed HIF-1α or vHL alleles in the myeloid lineage(macrophages and neutrophils) by crosses into a back-ground of cre recombinase expression driven by thelysozyme M (lysM) promoter. The resultant mice, witheither deficient or exaggerated HIF-1α expression in theirphagocytes, are phenotypically normal at baseline butdisplay marked abnormalities when examined in classicalmodels of inflammation [7]. Compared to wild-type mice,HIF-1α myeloid-null animals have less skin redness andedema after irritation with detergent solution, and greatlydiminished joint swelling and cartilage destruction in apassive serum-induced arthritis model [7]. A role for HIF-1α in chronic inflammatory diseases such as rheumatoidarthritis and atherosclerosis is further corroborated byelevated levels of the transcription factor in biopsies ofprimary lesions of patients [8–11].
HIF-1α: a master regulator of innate immunity
The contribution of HIF-1α to myeloid cell-mediatedinflammatory pathologies prompted immediate consider-ation of the capability of the transcription factor to mediatecentral functions of macrophages and neutrophils in innatehost defense. Whereas in healthy tissues, oxygen tension is
17.5–63 mm Hg (i.e., 2.5–9% oxygen), much lower levels(<1% oxygen) are present in wounds and tissue foci ofinfection. Many bacterial pathogens survive well andproliferate under anaerobic conditions, thus phagocytesmust be adapted to function effectively in microbialeradication in the same microenvironments. Genetic experi-ments in which mouse phagocyte HIF-1α levels weremanipulated revealed the pivotal role of the transcriptionalcontrol pathway in phagocyte bactericidal activity.
Macrophages from mice deficient in HIF-1α showdiminished capacity to kill Gram-negative and Gram-positive bacteria when compared to macrophages fromwild-type littermates [7, 12], and HIF-1α deficient animalswere more susceptible to invasive skin infection producedby Streptococcus pyogenes. While HIF-1α deletion (oroverexpression through vHL elimination) did not alterphagocyte production of reactive oxygen species throughthe respiratory burst, the expression of a number of othermolecular effectors of host innate defense was significantlycorrelated to HIF-1α levels. These included cathelicidinantimicrobial peptides, the granule proteases cathepsin Gand elastase, tumor necrosis factor-α (TNFα), and nitricoxide (NO) produced by the inducible NO synthetase(iNOS) [12]. In addition to its microbicidal properties, NOis known to stabilize HIF-1α by redistributing intracellularoxygen and inhibit prolyl hydroxylase activity [13], therebysetting up an autocrine feedback loop to amplify myeloidcell inflammatory activation.
A paradoxical result of these findings is that, due to HIF-1α activation, macrophages actually phagocytose and killbacteria better under hypoxic conditions than they do undernormoxic conditions [12, 14]. Even more striking, bacterialexposure is a stronger stimulus for HIF-1α stabilizationthan is hypoxia itself, and bacterial-induced HIF-1αstabilization is readily demonstrated even at normoxia[12]. HIF-1 induces leukocyte β2 integrin expression andthereby can promote neutrophils binding to epithelium [15],and inhibits neutrophil apoptosis via NF-κB activity[16, 17], thereby prolonging the effective window for thesecells to participate in phagocytic killing. Upregulation ofHIF-1α has also been demonstrated during the differenti-ation of monocytes circulating in the blood to tissue boundmacrophages [18].
Because circulating phagocytes serve a unique biologicalrole, and must pass through radically different micro-environments upon their rapid mobilization to infectedtissues, the HIF-1α pathway represents an elegant controlmechanism for the specialized functions of these cells(Fig. 1). Phagocyte bactericidal and proinflammatorycapacities can be maintained in an “off” state while themyeloid cells circulate in the oxygen-rich bloodstream; andthen be rapidly activated in response to the decliningoxygen gradient encountered upon diapedesis and entry of
1340 J Mol Med (2007) 85:1339–1346

the cells into the infected tissues. The primed phagocytethen encounters a further potent stimulation of the HIF-1αtranscriptonal pathway by direct encounter with thebacteria, as potentiated by the NO-mediated amplificationloop. This regulatory mechanism underlying HIF-1αcontrol of target genes involved in microbial killing ensuresthat the corresponding inflammatory mediators areexpressed preferentially in tissue foci of infection but notin healthy tissues where inflammatory damage mightotherwise harm host cells.
New evidence indicates that HIF-1α control of geneswith innate immune functions may not be limited tophagocytic cell types, as conditional gene targeting andRNAi inhibition of HIF-1α in skin keratinocytes decreasedtheir production of antimicrobial peptides and intrinsiccapability to control bacterial proliferation [19]. HIF-1αtranscriptional regulation also appears to modulate theproduction of proinflammatory cytokines in CD4+ andCD8+ T lymphocytes, but in contrast to findings inmacrophage and neutrophil lineages, the effect may besuppressive. After T-cell receptor activation, the release ofTNFα and interferon γ (IFNγ) was increased in T cells
with targeted deletion of the HIF-1α gene compared towild-type T cells [20]. The release of T cells from HIF-1αsuppression enhances their proliferation and allows them tocontribute proinflammatory cytokine production and restrictbacterial proliferation in a cecal ligation puncture model[21].
Finally, it has recently been discovered that HIF-1αtranscriptional regulation mediates allelle expression phe-notypes for the innate defense factor SLC11A1 (akaNRAMP1) through differential binding and activation ofZ-DNA forming microsatellite polymorphisms in theSLC11A1 promotor [22]. Since these polymorphismsinfluence human susceptibility to tuberculosis, rheumatoidarthritis, Crohn’s disease and other disorders, HIF-1α mayinfluence heritable variation in innate resistance to infectionand inflammation within and between populations [22].
HIF-1α activities during bacterial infection
Explorations of HIF-1α function in activating neutrophil andmacrophage bactericidal activities demonstrated increasedlevels of the transcription factor were stimulated in response
Fig. 1 Model for HIF-1α transcriptional regulation of phagocyteinnate immune functions. Phagocytic cells such as neutrophils andmacrophages have low HIF-1α levels when circulating in the oxygen-rich bloodstream. When recruited to tissue foci of inflammation, theyencounter a declining oxygen gradient which increases cellular HIF-1α levels and initiates activation of proinflammatory and bactericidaleffector genes bearing HREs. Maximum activation is achieved onbacterial encounter, where HIF-1α expression is further stimulatedthrough pattern recognition receptors (e.g., TLR-4) and cell signalingpathways (e.g., NFκB, MAPK) just beginning to be elucidated. HIF-
1α promotes increased phagocytosis and the release of antimicrobialpeptides (e.g., cathelidicins) and granule proteases with direct micro-bicidal activities. Increased VEGF production and elaboration ofproinflammatory cytokines facilitate recruitment and activation ofadditional immune effector cells. Activation of inducible nitric oxide(NO) synthetase generates a molecule (NO) with not only directantimicrobial properties, but also the ability to further stabilize HIF-1αand rapidly amplify the innate defense pathway in the phagocyte(modified and updated from [11])
J Mol Med (2007) 85:1339–1346 1341

to a variety of bacterial species including Streptococcuspyogenes, Streptococcus agalactiae, Staphylococcus aureus,Salmonella typhimurium and Pseudomonas aeruginosa [7,12, 22, 23], suggesting it subserves a general role inbacterial/host interactions. Loss of myeloid cell HIF-1αrenders mice more susceptible to invasive S. pyogenesinfection [12], and decreases phagocyte killing of Gram-negative and Gram-positive bacteria in vitro [7, 12, 23],suggesting that the HIF-1α response pathway is broadlyadaptive in host defense. In select additional research studies,the interplay between a specific bacterial infection and HIF-1α expression has been pursued in more detail.
One clear demonstration of HIF-1α induction by abacterial pathogen was provided in studies of Bartonellahenselae, a facultative intracellular bacterium that causescat-scratch disease and, in immunocompromised patients,the angioproliferative disorder known as bacillary angio-matosis (BA). Using HeLa as a model host cell line, B.henselae infection was found to induce HIF-1α by Westernblot and electrophoretic mobility shift assays, and immuno-flourescence studies of BA lesions from human patientsshowed high levels of HIF-1α expression [24]. Mutantstudies suggest that pilus appendages on the B. henselaesurface contribute to HIF-1α activation, VEGF secretionand initiation of a proangiogenic program that characterizesBA tissue pathology [24]. Another intracellular pathogen,Chlamydia pneumoniae, appears to have evolved a uniquemechanism to counteract HIF-1α stabilization, therebyblunting innate immune function and promoting its ownsurvival within host cells. During the later phase ofintracellular chlamydial replication (48–72 h), secretion ofthe chlamydial protease-like activity factor into the host cellcytoplasm degraded accumulated HIF-1α, and this proteo-lytic activity was shown to play an essential role in C.pneumoniae replication during hypoxia [25].
Finally, the opportunistic pathogen P. aeruginosa hasevolved mechanisms to sense alterations in host immunefunction and activation, and respond in a fashion thatincreases its virulence phenotypes, including expression ofthe PA-1 lectin/adhesin, a protein capable of inducingdefects in host epithelial barrier function [26]. HIF-1α isupregulated in intestinal epithelial cells exposed to hypoxia,and stimulates the release of adenosine, which normallyexerts a cytoprotective function. P. aeruginosa is able tometabolize adenosine to inosine via adenosine deaminase,and both adenosine and inosine upregulate PA-1 lectin/adhesin expression by the bacterium in a dose-dependentfashion [27]. In this sense, the pathogen senses HIF-1αdependent changes in host cell function and subverts innatedefense by virulence factor upregulation and metabolicelimination of a cytoprotective factor.
Since the mechanism of HIF-1α turnover involves iron-dependent prolyl hydroxylase activity, it is conceivable that
bacterial sequestration of iron could have the effect of HIF-1α stabilization. Preliminary data have emerged that thisphenomenon may operate in the Peyer’s patches of theintestine. Pathogens including Yersinia enterocolitica,Salmonella enterica or Enterobacter aerogenes induceHIF-1α expression in Peyer’s patches, and this inductioncan be replicated by application of purified siderophores(iron-binding proteins) from each species [28]. In contrast,siderophore-deficient bacterial mutants fail to induce HIF-1α activation. The disease potential of Y. enterocolitica isenhanced in mice deficient in intestinal HIF-1α expression,suggesting this activation pathway contributes to hostinnate defense [28].
HIF-1α dynamics in viral infection
Activation of HIF-1α pathway during the life cycle of viralpathogens has been the subject of increasing investigation,revealing a diversity of functional outcomes in diseaseprogression and critical linkages to viral oncogenesis. Viralinfection is generally appreciated to induce stabilization ofHIF-1α in target cells, which consequently contributes tolocal inflammation. For example, the common upperrespiratory tract pathogen respiratory syncytial virus(RSV) induces HIF-1α in primary human bronchialepithelial cells via a NO-dependent pathway [29]. IncreasedHIF-1α levels stimulates VEGF production, enhancingmonolayer permeability, which may play a role in theairway edema of acute RSV infection.
In some cases, HIF-1α may help coordinate a hostdefense program to limit cell damage secondary to viralinfection. This scenario might particularly apply to viruseswhich exert an acute cytolytic effect, such as the vesicularstomatitis virus (VSV). Several years ago, it was noticedthat hypoxia (2% O2, 14 mmHg) reduced the cytopathoge-nicity and replication of VSV, with measured antiviraleffects of interferons α and γ potentiated under the lowoxygen conditions [30]. Interferons in turn have beenshown to upregulate the expression of HIF-1α [31]. Thesignificance of HIF in the antiviral response to VSV wasrecently established by a pharmacological approach –inhibition of HIF activity by a small molecule antagonist(chemotin) or RNA interference enhanced VSV cytotox-icity and replication, whereas the treatment with thehypoxia mimetic cobalt chloride promoted cellular resis-tance to infection [32]. Furthermore, expression profilingshowed HIF enhancement of interferon β and otherantiviral genes during VSV infection [32].
For a number of persistent viral infections, wheninduction of HIF-1α is insufficient to effect eradication,the accompanying proangiogenic program can contribute tooncogenesis. For example, chronic infections with thehepatitis B and C viruses (HBV and HCV) are epidemio-
1342 J Mol Med (2007) 85:1339–1346

logically associated with development of hepatocellularcarcinoma (HCC), a highly vascularized solid tumor. The Xprotein of HBV (HBx) is felt to play an important role inangiogenesis and metastasis of HCC [33]. HIF-1α levelsand nuclear translocation are increased in cultured livercells by expression of HBx via p42/p44 mitogen-activatedprotein kinase (MAPK) pathways, leading to transcriptionalactivation of HIF-1α target genes including VEGF, afinding corroborated in vivo in the livers of HBx transgenicmice [34]. Immunohistochemical studies in these micereveal increased microvessels in dysplastic areas of liverwhere HIF-1α, VEGF, and HBx co-localize [35]. HBx wasfound to interact directly with the bHLH/PAS domain ofHIF-1α, blocking its association with vHL and thuspreventing its ubiquitin-mediated degradation [35]. More-over, HIF-1α activation induced by HBx was found toincrease the multi-drug resistance 1 (MDR1) transporteractivity in a hepatoma cell line, thereby contributing toincreased resistance of the cancer cells to chemotherapeuticagents [36]. Recently, HCV infection has also been found tostabilize HIF-1α with contributions from MAPK and othercellular activation pathways (NF-kB, STAT-3, PI3-K/AkT),stimulating VEGF production and neovascularization in achick chorioallantioic membrane surrogate assay system [37].
Another example linking viral activation of HIF-1α toproangiongenesis and tumor development can be found inthe case of human papillomavirus-16 (HPV-16), an etio-logic agent of cervical interstitial neoplasia that, undetected,can progress to cervical carcinoma. In advanced cervicalcancer lesions, many of which are hypoxic, increased HIF-1α levels can be correlated to poor prognosis [38, 39].Transgenic mice expressing HPV-16 in cervical epitheliumunder control of the K14 promotor can develop locallyinvasive cervical cancers; the size of these lesions isincreased 70-fold when double transgenic mice are createdwith both HPV-16 and HIF-1α expression driven by K14[40]. Transfection of human cervical cancer cell lines withHPV-16 oncoproteins E6 and E7 can induce VEGFexpression and capillary formation in vitro; however, thisproangiogenic effect is abolished when the cells are co-transfected with siRNA targeting HIF-1α [41]. Together,these new studies suggest a synergism of HIF-1α with viralongogenes in premalignant lesions to promote geneactivation programs favoring neovascularization and cancerdevelopment.
HIF-1α activation is apparent during other viral infec-tions associated with risk of neoplastic transformation. Theretrovirus human T-cell leukemia virus type 1 (HTLV-1)causes adult T-cell leukemia. Increased HIF-1α proteinlevels and VEGF expression are detected in T-cell linesinfected with HTLV-1, via a process involving activation ofPI3K/Akt signaling by the HTLV-1 protein Tax [42]. Theherpesvirus Epstein Barr virus (EBV) is linked to develop-
ment of nasopharyngeal carcinoma in specific populations.The major oncoprotein of EBV, latent membrane protein 1(LMP1), increases HIF-1α levels and stimulates VEGFexpression in nasopharyngeal epithelial cells through amechanism dependant both upon H2O2 production and p42/p44 MAPK activity [43]. Recent co-immunoprecipationstudies indicate EBV LMP1 enhances the stability of Siah1E3 ubiquitin ligase, inducing proteasomal degradation ofPHD-1 and PHD-3 that normally tag HIF-1α for degrada-tion. LMP1 thus prevents formation of the VHL/HIF-1αcomplex, providing a mechanism for HIF-1α stabilizationduring EBV nasopharyngeal cell infection [44].
A fascinating crosstalk between viral genes and the HIF-1α pathway has recently been elucidated for the humanherpesvirus 8 (HHV-8). Latent infection with HHV-8 isassociated with the endothelial tumor Kaposi’s sarcoma(KS) in AIDS patients and others with lowered immunity,and KS lesions in vivo are associated with high levels ofboth the HIF-1α and HIF-2α protein [45]. HHV-8 infectionof endothelial cells in vitro leads to increased stabilizationof the two HIF α subunits and increased HIF-responsivegene expression [45]. The HHV-8 latency-associatednuclear antigen (LANA), which plays a critical role inmodulating viral and target cell gene expression, increasesHIF-1α mRNA levels, and also physically interacts withthe transcription factor to enhance its promoter activities[46]. HIF-1α induction and co-activation during HHV-8 infection can then lead to activation of target genes in thegenome of the virus itself, including that encoding Rta,which is involved in transition of the virus from latency to alytic replication phase. Several putative HREs are identifiedin the essential Rta promoter, and HIF-1α-dependentbinding of a LANA protein complex to such HREs canbe demonstrated by electromobility shift assays [46]. Inanother potential example of viral-HIF crosstalk, replicationof parvovirus B19, a cause of erythema infectiousum or“fifth disease”, is enhanced under hypoxic conditions. HIF-1α binding to an HRE located in the B19 promoter regioncan be demonstrated; however, the full implications of thisfinding for viral pathogenesis remain unclear [47].
HIF-1α modulation in parasitic infection
Though much less well studied, induction of HIF-1α alsoappears to occur in the context of infection with protozoanparasites. For example, cutaneous lesions can be generated inBALB/c mice by infection with Leishmania amazonensis,and in the later stages of infection, HIF-1α induction in thecytoplasm and parasitophorous vacuoles of macrophagesrecruited to the microenvironment can be clearly demon-strated [48]. An interesting comparative microarray analysisof transcriptional activation patterns in human fibroblastsinfected with the obligate intracellular parasites Toxoplasma
J Mol Med (2007) 85:1339–1346 1343

gondii and Trypanosoma cruzi has identified an importantrole for HIF-1α in the life cycle of the former. T. gondii, acause of opportunistic infections in fetuses and theimmunocompromised, induced transcripts for glycolyticenzymes, glucose transporters, transferrin receptor andVEGF, a transcriptome signature for HIF-1α activation[49, 50], whereas parallel fibroblast infection studies withT. cruzi produced minimal changes in expression profile[51]. Further investigation showed T. gondii infectionrapidly induced levels of HIF-1α and activated reportergene expression in infected fibroblasts [52]. Under hypoxicconditions (3% oxygen) present in the tissues (brain,muscle, retina) in which the parasite produces seriousdisease, T. gondii cell division and organelle maintenancewas severely impaired in host cells where HIF-1α functionwas deleted. The T. gondii parasite may have evolved toinduce HIF-1α because a target gene is essential to parasitegrowth, or alternatively because HIF-1α activation isnecessary to preserve the health of the host cell in whichthe parasite has become established [52].
HIF-1α and sepsis
Sepsis reflects a maladaptive and potentially lethal hostresponse to infection, in which bacteria or lipopolysaccha-ride (LPS) act as potent activators of uncontrolled proin-flammatory cytokine release from immune cells includingmonocytes and macrophages. LPS raises levels of HIF-1αin macrophages through activities of the p42/44 MAPK andNfkB signal transduction pathways [53] and in hepatocytesby JNK signaling and c-Jun activation [54]. Recently, it hasbeen shown that LPS increases HIF-1α and decreasesprolyl hydroxylase mRNA production through a processthat depends upon LPS pattern recognition by Toll-likereceptor 4 (TLR-4) [55]. Studies of LPS challenge in micewith conditional gene targeting of HIF-1α in the myeloidlineage reveal HIF-1α to be a critical determinant of thesepsis phenotype, promoting high level production ofinflammatory cytokines TNF-α, interleukin-1 (IL-1), IL-6,and IL-12. HIF-1α deletion in the macrophage lineage isprotective against LPS-induced mortality and blocks devel-opment of clinical indicators of sepsis including hypother-mia, tachycardia, and hypotension [55].
HIF-1α: a therapeutic target for infectious diseases?
We have summarized above an evolving view of HIF-1α asa master regulator of the innate immune function ofphagocytes [12, 56, 57]. Since pharmacological approachesfor manipulating HIF-1α levels have been consideredextensively in the context of cancer therapy and angiogen-esis [58, 59], the possibility is raised of a novel approach totherapy of infectious disease conditions, namely boosting
the bactericidal capacity of phagocytes [60]. Conceptualsupport for this concept was provided by in vitro studieswhere genetic augmentation of macrophage HIF-1α levels(through vHL deletion) or addition of a series of pharma-cological agonists of HIF-1α (hypoxia mimetics thatrestrict prolyl hydroxylase access to iron), each enhancedmurine macrophage bactericidal activity [12]. Similarly,dose-dependent enhancement of the bactericidal activity ofhuman whole blood, neutrophils, and macrophage cell lineU937 against the pathogen Staphylcococcus aureus wasachieved using the HIF-1α agonist L-mimosine [23]. Localtreatment with L-mimosine also significantly delayed theprogression of S. aureus skin abscesses in a murinechallenge model [23].
The proof-of-principle experiments described suggestfurther exploration of HIF-1α augmentation to boost innatedefense function. This may be of interest as a therapeuticstrategy in infectious disease conditions complicated byantibiotic resistance or compromised host immunity (e.g.AIDS, cancer chemotherapy). An advantage of targetinghost molecules that enhance phagocyte recruitment oractivate array of phagocyte bactericidal mechanisms is lackof selective pressure for resistance – the bacterial pathogencannot evolve to combat a drug that targets the host andeffectively deploys a multifaceted combination therapy ofnatural antimicrobial molecules [61]. Coincidently, HIF-1αagonist therapy may benefit the anemia that can accompanychronic infection, since it functions in the liver to suppressproduction of the peptide hepcidin, promoting iron absorp-tion and mobilization, and stimulates red blood cellsynthesis by increasing EPO production [62]. Finally,strategies to inhibit HIF-1α in therapy of chronic inflam-matory disorder such as rheumatoid arthritis may provide asafer therapeutic margin than high-dose steroids or cyto-toxic agents, since rapid posttranslational regulation of HIF-1α levels could allow rapid restoration of innate immunefunction of phagocytes upon drug withdrawal in the eventof opportunistic infection.
Acknowledgment The author’s own research contributions in thearea of HIF-1α and innate immunity have been supported by NIHgrant AI060840 (to RSJ and VN) and Swiss National FoundationFellowship PASMA-117303 (to ASZ).
Conflict of interest statement The authors declare no conflict ofinterest.
References
1. Saadi S, Wrenshall LE, Platt JL (2002) Regional manifestationsand control of the immune system. FASEB J 16:849–856
2. Schor H, Vaday GG, Lider O (2000) Modulation of leukocytebehavior by an inflamed extracellular matrix. Dev Immunol7:227–238
1344 J Mol Med (2007) 85:1339–1346

3. Semenza GL, Roth PH, Fang HM, Wang GL (1994) Transcrip-tional regulation of genes encoding glycolytic enzymes byhypoxia-inducible factor 1. J Biol Chem 269:23757–23763
4. Iyer NV, Kotch LE, Agani F, Leung SW, Laughner E, Wenger RH,Gassmann M, Gearhart JD, Lawler AM, Yu AY, Semenza GL(1998) Cellular and developmental control of O2 homeostasis byhypoxia-inducible factor 1α. Genes Dev 12:149–162
5. Ryan HE, Lo J, Johnson RS (1998) HIF-1α is required for solidtumor formation and embryonic vascularization. EMBO J17:3005–3015
6. Kotch LE, Iyer NV, Laughner E, Semenza GL (1999) Defectivevascularization of HIF-1α-null embryos is not associated withVEGF deficiency but with mesenchymal cell death. Dev Biol209:254–267
7. Cramer T, Yamanishi Y, Clausen BE, Forster I, Pawlinski R,Mackman N, Haase VH, Jaenisch R, Corr M, Nizet V, Firestein GS,Gerber HP, Ferrara N, Johnson RS (2003) HIF-1α is essential formyeloid cell-mediated inflammation. Cell 112:645–657
8. Westra J, Brouwer E, Bos R, Posthumus MD, Doornbos-van derMeer B, Kallenberg CG, Limburg PC (2007) Regulation ofcytokine-induced HIF-1α expression in rheumatoid synovialfibroblasts. Ann N Y Acad Sci 1108:340–348
9. Gaber T, Dziurla R, Tripmacher R, Burmester GR, Buttgereit F(2005) Hypoxia inducible factor (HIF) in rheumatology: low O2!See what HIF can do. Ann Rheum Dis 64:971–980
10. Hollander AP, Corke KP, Freemont AJ, Lewis CE (2001)Expression of hypoxia-inducible factor 1α by macrophages inthe rheumatoid synovium: implications for targeting of therapeuticgenes to the inflamed joint. Arthritis Rheum 44:1540–1544
11. Vink A, Schoneveld AH, Lamers D, Houben AJ, van der Groep P,van Diest PJ, Pasterkamp G (2007) HIF-1a expression isassociated with an atheromatous inflammatory plaque phenotypeand upregulated in activated macrophages. Atherosclerosis(in press)
12. Peyssonnaux C, Datta V, Cramer T, Doedens A, Theodorakis EA,Gallo RL, Hurtado-Ziola N, Nizet V, Johnson RS (2005) HIF-1alpha expression regulates the bactericidal capacity of phago-cytes. J Clin Invest 115:1806–1815
13. Hagen T, Taylor CT, Lam F, Moncada S (2003) Redistribution ofintracellular oxygen in hypoxia by nitric oxide: effect on HIF1α.Science 302:1975–1978
14. Anand RJ, Gribar SC, Li J, Kohler JW, Branca MC, Dubowski T,Sodhi CP, Hackam DJ (2007) Hypoxia causes an increase inphagocytosis by macrophages in a HIF-1a-dependent manner.J Leuk Biol 82:1257–1265
15. Kong T, Eltzschig HK, Karhausen J, Colgan SP, Shelley CS(2004) Leukocyte adhesion during hypoxia is mediated by HIF-1-dependent induction of β2 integrin gene expression. Proc NatlAcad Sci USA 101:10440–10445
16. Walmsley SR, Print C, Farahi N, Peyssonnaux C, Johnson RS,Cramer T, Sobolewski A, Condliffe AM, Cowburn AS, Johnson N,Chilvers ER (2005) Hypoxia-induced neutrophil survival ismediated by HIF-1α-dependent NF-κB activity. J Exp Med201:105–115
17. Walmsley SR, Cowburn AS, ClatworthyMR,Morrell NW, Roper EC,Singleton V, Maxwell P, Whyte MK, Chilvers ER (2006)Neutrophils from patients with heterozygous germline mutationsin the von Hippel Lindau protein (VHL) display delayed apoptosisand enhanced bacterial phagocytosis. Blood 108:3176–3178
18. Oda T, Hirota K, Nishi K, Takabuchi S, Oda S, Yamada H, Arai T,Fukuda K, Kita T, Adachi T, Semenza GL, Nohara R (2006)Activation of hypoxia-inducible factor 1 during macrophagedifferentiation. Am J Physiol 291:C104–113
19. Peyssonnaux C, Boutin A, Zinkernagel AS, Datta V, Nizet V,Johnson RS (2007) Critical role of HIF-1a in keratinocyte defenseagainst bacterial infection. J Invest Derm (in press)
20. Lukashev D, Klebanov B, Kojima H, Grinberg A, Ohta A,Berenfeld L, Wenger RH, Ohta A, Sitkovsky M (2006) Cuttingedge: hypoxia-inducible factor 1α and its activation-inducibleshort isoform I.1 negatively regulate functions of CD4+ and CD8+T lymphocytes. J Immunol 177:4962–4965
21. Thiel M, Caldwell CC, Kreth S, Kuboki S, Chen P, Smith P, Ohta A,Lentsch AB, Lukashev D, Sitkovsky MV (2007) Targeted deletionof HIF-1α gene in T cells prevents their inhibition in hypoxicinflamed tissues and improves septic mice survival. PLoS ONE 2:e853
22. Bayele HK, Peyssonnaux C, Giatromanolaki A, Arrais-Silva WW,Mohamed HS, Collins H, Giorgio S, Koukourakis M, JohnsonRS, Blackwell JM, Nizet V, Srai SK (2007) HIF-1 regulatesheritable variation and allele expression phenotypes of themacrophage immune response gene SLC11A1 from a Z-DNAforming microsatellite. Blood 110:3039–3048
23. Zinkernagel AS, Peyssonnaux C, Johnson RS, Nizet V (2007)Pharmacologic augmentation of HIF-1a with mimosine boosts thebactericidal capacity of phagocytes. J Infect Dis (in press)
24. Kempf VA, Lebiedziejewski M, Alitalo K, Walzlein JH, Ehehalt U,Fiebig J, Huber S, Schutt B, Sander CA, Muller S, Grassl G,Yazdi AS, Brehm B, Autenrieth IB (2005) Activation ofhypoxia-inducible factor-1 in bacillary angiomatosis: evidencefor a role of hypoxia-inducible factor-1 in bacterial infections.Circulation 111:1054–1062
25. Rupp J, Gieffers J, Klinger M, van Zandbergen G, Wrase R,Maass M, Solbach W, Deiwick J, Hellwig-Burgel T (2007)Chlamydia pneumoniae directly interferes with HIF-1a stabiliza-tion in human host cells. Cell Microbiol 9:2181–2191
26. Wu L, Estrada O, Zaborina O, Bains M, Shen L, Kohler JE, Patel N,Musch MW, Chang EB, Fu YX, Jacobs MA, Nishimura MI,Hancock RE, Turner JR, Alverdy JC (2005) Recognition of hostimmune activation by Pseudomonas aeruginosa. Science309:774–777
27. Patel NJ, Zaborina O, Wu L, Wang Y, Wolfgeher DJ, Valuckaite V,Ciancio MJ, Kohler JE, Shevchenko O, Colgan SP, Chang EB,Turner JR, Alverdy JC (2007) Recognition of intestinal epithelialHIF-1alpha activation by Pseudomonas aeruginosa. Am J PhysiolGastrointest Liver Physiol 292:G134–142
28. Werth N, Hartmann H, Wurz H, Amr A, Kempf VA (2006) Roleof HIF-1 in bacterial infections. Acta Physiologica 188:P23
29. Kilani MM, Mohammed KA, Nasreen N, Tepper RS, Antony VB(2004) RSV causes HIF-1alpha stabilization via NO release inprimary bronchial epithelial cells. Inflammation 28:245–251
30. Naldini A, Carraro F, Fleischmann WR Jr., Bocci V (1993)Hypoxia enhances the antiviral activity of interferons. J InterferonRes 13:127–132
31. de Veer MJ, Holko M, Frevel M, Walker E, Der S, Paranjape JM,Silverman RH, Williams BR (2001) Functional classification ofinterferon-stimulated genes identified using microarrays. J LeukBiol 69:912–920
32. Hwang II, Watson IR, Der SD, Ohh M (2006) Loss of VHLconfers hypoxia-inducible factor (HIF)-dependent resistance tovesicular stomatitis virus: role of HIF in antiviral response. J Virol80:10712–10723
33. Wang XW, Forrester K, Yeh H, Feitelson MA, Gu JR, Harris CC(1994) Hepatitis B virus X protein inhibits p53 sequence-specificDNA binding, transcriptional activity, and association with transcrip-tion factor ERCC3. Proc Natl Acad Sci USA 91:2230–2234
34. Yoo YG, Oh SH, Park ES, Cho H, Lee N, Park H, Kim DK, Yu DY,Seong JK, Lee MO (2003) Hepatitis B virus X protein enhancestranscriptional activity of hypoxia-inducible factor-1α throughactivation of mitogen-activated protein kinase pathway. J BiolChem 278:39076–39084
35. Moon EJ, Jeong CH, Jeong JW, Kim KR, Yu DY, Murakami S,Kim CW, Kim KW (2004) Hepatitis B virus X protein induces
J Mol Med (2007) 85:1339–1346 1345

angiogenesis by stabilizing hypoxia-inducible factor-1α. FASEB J18:382–384
36. Han HK, Han CY, Cheon EP, Lee J, Kang KW (2007) Role ofhypoxia-inducible factor-1α in hepatitis-B-virus X protein-mediatedMDR1 activation. Biochem Biophys Res Commun 357:567–573
37. Nasimuzzaman M, Waris G, Mikolon D, Stupack DG, Siddiqui A(2007) Hepatitis C virus stabilizes hypoxia-inducible factor-1α(HIF-1α) and stimulates the synthesis of vascular endothelialgrowth factor (VEGF). J Virol 81:10249–10257
38. Hockel M, Schlenger K, Aral B, Mitze M, Schaffer U, Vaupel P(1996) Association between tumor hypoxia and malignantprogression in advanced cancer of the uterine cervix. CancerRes 56:4509–4515
39. Birner P, Schindl M, Obermair A, Plank C, Breitenecker G,Oberhuber G (2000) Overexpression of hypoxia-inducible factor1α is a marker for an unfavorable prognosis in early-stageinvasive cervical cancer. Cancer Res 60:4693–4696
40. Lu ZH, Wright JD, Belt B, Cardiff RD, Arbeit JM (2007) Hypoxia-inducible factor-1 facilitates cervical cancer progression in humanpapillomavirus type 16 transgenic mice. Am J Pathol 171:667–681
41. Tang X, Zhang Q, Nishitani J, Brown J, Shi S, Le AD (2007)Overexpression of human papillomavirus type 16 oncoproteinsenhances hypoxia-inducible factor 1α protein accumulation andvascular endothelial growth factor expression in human cervicalcarcinoma cells. Clin Cancer Res 13:2568–2576
42. Tomita M, Semenza GL, Michiels C, Matsuda T, Uchihara JN,Okudaira T, Tanaka Y, Taira N, Ohshiro K, Mori N (2007)Activation of hypoxia-inducible factor 1 in human T-cellleukaemia virus type 1-infected cell lines and primary adult T-cell leukaemia cells. Biochem J 406:317–323
43. Wakisaka N, Kondo S, Yoshizaki T, Murono S, Furukawa M,Pagano JS (2004) Epstein-Barr virus latent membrane protein 1induces synthesis of hypoxia-inducible factor 1α. Mol Cell Biol24:5223–5234
44. Kondo S, Seo SY, Yoshizaki T, Wakisaka N, Furukawa M, Joab I,Jang KL, Pagano JS (2006) EBV latent membrane protein 1 up-regulates hypoxia-inducible factor 1α through Siah1-mediateddown-regulation of prolyl hydroxylases 1 and 3 in nasopharyngealepithelial cells. Cancer Res 66:9870–9877
45. Carroll PA, Kenerson HL, Yeung RS, Lagunoff M (2006) LatentKaposi’s sarcoma-associated herpesvirus infection of endothelialcells activates hypoxia-induced factors. J Virol 80:10802–10812
46. Cai Q, Lan K, Verma SC, Si H, Lin D, Robertson ES (2006) Kaposi’ssarcoma-associated herpesvirus latent protein LANA interacts withHIF-1α to upregulate RTA expression during hypoxia: Latencycontrol under low oxygen conditions. J Virol 80:7965–7975
47. Pillet S, Le Guyader N, Hofer T, NguyenKhac F, KokenM, Aubin JT,Fichelson S, Gassmann M, Morinet F (2004) Hypoxia enhances
human B19 erythrovirus gene expression in primary erythroid cells.Virology 327:1–7
48. Arrais-Silva WW, Paffaro VA Jr., Yamada AT, Giorgio S (2005)Expression of hypoxia-inducible factor-1α in the cutaneouslesions of BALB/c mice infected with Leishmania amazonensis.Exp Mol Pathol 78:49–54
49. Gail M, Gross U, Bohne W (2001) Transcriptional profile ofToxoplasma gondii-infected human fibroblasts as revealed bygene-array hybridization. Mol Genet Genomics 265:905–912
50. Blader IJ, Manger ID, Boothroyd JC (2001) Microarray analysisreveals previously unknown changes in Toxoplasma gondii-infected human cells. J Biol Chem 276:24223–24231
51. Vaena de Avalos S, Blader IJ, Fisher M, Boothroyd JC, Burleigh BA(2002) Immediate/early response to Trypanosoma cruzi infectioninvolves minimal modulation of host cell transcription. J Biol Chem277:639–644
52. Spear W, Chan D, Coppens I, Johnson RS, Giaccia A, Blader IJ(2006) The host cell transcription factor hypoxia-inducible factor1 is required for Toxoplasma gondii growth and survival atphysiological oxygen levels. Cell Microbiol 8:339–352
53. Frede S, Stockmann C, Freitag P, Fandrey J (2006) Bacteriallipopolysaccharide induces HIF-1 activation in human monocytesvia p44/42 MAPK and NF-κB. Biochem J 396:517–527
54. Kim HY, Kim YH, Nam BH, Kong HJ, Kim HH, Kim YJ, AnWG, Cheong J (2007) HIF-1α expression in response to lip-opolysaccaride mediates induction of hepatic inflammatorycytokine TNFα. Exp Cell Res 313:1866–1876
55. Peyssonnaux C, Cejudo-Martin P, Doedens A, Zinkernagel AS,Johnson RS, Nizet V (2007) Cutting edge: Essential role ofhypoxia inducible factor-1α in development of lipopolysaccha-ride-induced sepsis. J Immunol 178:7516–7519
56. Cramer T, Johnson RS (2003) A novel role for the hypoxiainducible transcription factor HIF-1a: critical regulation ofinflammatory cell function. Cell Cycle 2:192–193
57. Strieter RM (2003) Mastering innate immunity. Nat Med 9:512–51358. Semenza GL (2003) Targeting HIF-1 for cancer therapy. Nat Rev
Cancer 3:721–73259. Semenza GL (2006) Development of novel therapeutic strategies
that target HIF-1. Exp Opin Therapeut Targets 10:267–28060. Zarember KA, Malech HL (2005) HIF-1α: a master regulator of
innate host defenses. J Clin Invest 115:1702–170461. Nizet V (2007) Understanding how leading bacterial pathogens
subvert innate immunity to reveal novel therapeutic targets. JAllergy Clin Immunol 120:13–22
62. Peyssonnaux C, Zinkernagel AS, Scheupbach RA, Rankin E,Vaulont S, Haase VH, Nizet V, Johnson RS (2007) Regulation ofiron homeostasis by the hypoxia inducible transcription factors(HIF). J Clin Invest 117:1926–1932
1346 J Mol Med (2007) 85:1339–1346

CLINICAL IMPLICATION
The “brain–skin connection”: nerve growth factor-dependentpathways for stress-induced skin disorders
Emmanouil Zoumakis & Sophia N. Kalantaridou &
George P. Chrousos
Received: 20 September 2007 /Accepted: 20 September 2007 / Published online: 16 October 2007# Springer-Verlag 2007
Keywords CNS . NGF. CRF.Mast cells
Stress can precipitate or exacerbate certain neuroinflamma-tory manifestations in peripheral tissues, including the skin.Indeed, stress may trigger or aggravate skin diseases, such asatopic dermatitis, psoriasis, urticaria, and alopecia areata ortotalis. The precise mechanisms leading to stress-induced or -aggravated skin disorders have just begun to be understood.Thus, recent experimental evidence reveals that distinctneuroendocrine pathways of the brain and the skin areintricately intertwined. This so-called “brain–skin connec-tion” represents an exciting new area of investigation [5].Mouse models are now available for the detailed mechanisticinvestigation of the effects of stress on skin diseases.
The stress system in the brain and the periphery includesthe hypothalamic–pituitary–adrenal (HPA) axis and thearousal and sympathetic systems (Fig. 1). When activatedby stress, the stress system leads to several behavioral, neu-roendocrine, autonomic, and immune changes that are part ofthe adaptive response [1]. Besides the classic stress-relatedneurohormones of the stress system [corticotropin-releasinghormone (CRH), arginine-vasopressin, adrenocorticotropic
hormone, glucocorticoids and the catecholamines norepi-nephrine and epinephrine], additional mediators, such asnerve growth factor (NGF) and several cytokines, havebeen identified as important players of the stress response.Circulating NGF levels are increased in patients withinflammatory skin diseases, such as psoriasis [7].
Mast cells are involved in the development of allergicand late-phase inflammation reactions [2]. They are alsoimplicated in nonallergic inflammation, as they releaseseveral proinflammatory cytokines, such as tumor necrosisfactor and other inflammatory mediators (Table 1). Mastcells are located perivascularly in close proximity toperipheral neuron terminals, including both those ofpostganglionic sympathetic and sensory [dorsal root ganglia(DRG) neurons] neurons originating in the sympathetic andDRG, respectively (Fig. 1). Skin mast cells produce CRHand express CRH receptors type 1 [4, 6]. They can beactivated by many neuropeptides secreted by postganglion-ic sympathetic and sensory neurons, especially peripheralCRH, substance P (SP), and calcitonin gene-related peptide(CGRP), in response to stress, or by inflammatorymediators. Stress-induced or -aggravated neuroinflamma-tory skin conditions have been associated with mast cellactivation and degranulation. Similarly, we have previouslyshown that stress induces intracranial mast cell activation,through the sequential action of CRH and sensory neuro-peptides [9], and that CRH degranulates skin mast cells andincreases vascular permeability [8].
In a murine model of stress involving exposure ofC57BL/6 mice to sound stress, Joachim et al. [3] in thisissue of the Journal provide evidence that stress, orintracutaneous injection of recombinant NGF mimickingthe skin’s response to stress, up-regulate the percentage ofSP+ or CGRP+ sensory neurons in skin-innervating DRG
J Mol Med (2007) 85:1347–1349DOI 10.1007/s00109-007-0270-6
E. Zoumakis :G. P. Chrousos (*)First Department of Pediatrics, Choremeio Research Laboratory,University of Athens Medical School,Athens, Greecee-mail: [email protected]
S. N. KalantaridouDivision of Reproductive Endocrinology,Department of Obstetrics and Gynecology,University of Ioannina Medical School,Ioannina, Greece

neurons. They also show that the number of SP+ or CGRP+
sensory nerve fibers in the dermis of stressed C57BL/6mice is significantly increased. This means that increasedsecretion of neuropeptides would be expected, withresultant enhanced local mast cell degranulation and
immune cell activation and, hence, inflammation. Further-more, they demonstrate that neutralization of NGF activityabrogates stress-induced effects on the percentage of SP+
and CGRP+ sensory neurons in skin-innervating DRGneurons, as well as on dermal sensory nerve fibers. Thissuggests that NGF plays a major role in the neurogeniccomponent of inflammation and that it is a major mediatorof the effects of stress in the skin.
No target-specific pharmacologic interventions are cur-rently available for the management of stress-triggered or -aggravated skin disorders. The findings by Joachim et al. [3]provide a useful model to conceptualize and generate moreeffective therapies for these disorders. Thus, abrogation ofmast-cell activation, degranulation and local cytokine secre-tion by blockade of DRG neuron products appears to be apossible area of further investigation for the treatment ofstress-related skin disorders. Another possible approach maybe the inhibition of the principal stress regulator CRH andperipheral CRH by using CRH receptor type 1 antagonists,such as antalarmin [10]. This small molecular CRHantagonist was previously shown to block CRH-inducedmast cell degranulation [9]. Finally, blockade of other stress-related DRG neuron-produced and mast cell-regulatingneuropeptides, such as SP, CGRP, or NGF, could bepromising areas of research in this direction.
Table 1 Mediators synthesized and secreted during mast cellactivation
Mediator
CGRPCRHCysteinyl leukotrienes (cysLTs)HistamineInteleukins (ILs)NGFNitric oxide (NO)Pituitary adenylate cyclase-activating polypeptide (PACAP)Prostaglandin D2 (PGD2)Stem cell factor (SCF)SPTransforming growth factor-β (TGF-β)Tumor necrosis factorUrocortin (Ucn)Vascular endothelial growth factor (VEGF)Vasoactive intestinal peptide (VIP)
Fig. 1 The stressed brain (CNS) exerts its effects on the skin throughthe stress and sensory afferent systems through endocrine and neuralpathways. The first includes effects of the circulating hormones of theHPA axis and sympathetic system, respectively, cortisol (F, cortico-sterone in rodents) and the catecholamines norepinephrine (NE) andepinephrine (E) on skin cells including mast cells and otherimmunocytes. The stress system also influences skin targets through
the terminals of the postganglionic neurons (PGN) emanating from thesympathetic ganglia secreting norepinephrine and a variety of othermediators, including several neuropeptides, such as CRH. The sensoryafferent system influences the skin through peripheral nerve fibersemanating from the dorsal root ganglia (DRG), also secreting a varietyof mediators such as substance P (SP)
1348 J Mol Med (2007) 85:1347–1349

The results reported by Joachim et al. may shed light onthe pathophysiology of neuroimmune skin disorders, whichare clearly triggered or exacerbated by stress and provide atool to investigate new treatment strategies for the manage-ment of such disorders.
References
1. Chrousos GP (1995) The hypothalamic–pituitary–adrenal axis andimmune-mediated inflammation. N Engl J Med 332:1351–1362
2. Elenkov IJ, Chrousos GP (2006) Stress system—organization,physiology and immunoregulation. Neuroimmunomodulation13:257–267
3. Joachim RA, Kuhlmei A, Dinh QT, Handjiski B, Fischer T, PetersEM, Klapp BF, Paus R, Arck PC (2007) Neuronal plasticity of the“brain–skin-connection”: stress-triggered up-regulation of neuro-peptides in dorsal root ganglia and skin via nerve growth factor-dependent pathways. J Mol Med DOI 10.1007/s00109-007-0262-6
4. Kempuraj D, Papadopoulou NG, Lytinas M, Huang M, Kandere-Grzybowska K, Madhappan B, Boucher W, Christodoulou S,Athanassiou A, Theoharides TC (2004) Corticotropin-releasing
hormone and its structurally related urocortin are synthesized andsecreted by human mast cells. Endocrinology 145:43–48
5. Paus R, Theoharides TC, Arck PC (2006) Neuroimmunoendo-crine circuitry of the ‘brain–skin connection’. Trends Immunol27:32–39
6. Pisarchik A, Slominski AT (2001) Alternative splicing of CRH-R1 receptors in human and mouse skin: identification of newvariants and their differential expression. FASEB J 15:2754–2756
7. Schulte-Herbruggen O, Folster-Holst R, von Elstermann M,Augustin M, Hellweg R (2007) Clinical relevance of nervegrowth factor serum levels in patients with atopic dermatitis andpsoriasis. Int Arch Allergy Immunol 144:211–216
8. Theoharides TC, Singh LK, Boucher W, Pang X, Letourneau R,Webster E, Chrousos G (1998) Corticotropin-releasing hormoneinduces skin mast cell degranulation and increased vascularpermeability, a possible explanation for its proinflammatoryeffects. Endocrinology 139:403–413
9. Theoharides TC, Spanos C, Pang X, Alferes L, Ligris K, LetourneauR, Rozniecki JJ, Webster E, Chrousos GP (1995) Stress-inducedintracranial mast cell degranulation: a corticotropin-releasing hormone-mediated effect. Endocrinology 136:5745–5750
10. Zoumakis E, Rice KC, Gold PW, Chrousos GP (2006) Potentialuses of corticotropin-releasing hormone antagonists. Ann N YAcad Sci 1083:239–251
J Mol Med (2007) 85:1347–1349 1349

REVIEW
IDO expression in the brain: a double-edged sword
Erik Kwidzinski & Ingo Bechmann
Received: 22 January 2007 /Revised: 6 April 2007 /Accepted: 11 May 2007 / Published online: 27 June 2007# Springer-Verlag 2007
Abstract The tryptophan-catabolizing enzyme indole-amine-2,3-dioxygenase (IDO) initiates the first and rate-limiting step of the kynurenine pathway. It is induced byproinflammatory cytokines such as interferon-β and inter-feron-γ and has established effects in the control ofintracellular parasites. The recent detection of its decisivefunction in immune tolerance at the maternal–fetal interfacestimulated various studies unraveling its regulatory effecton T cells in many pathologies. In the brain, IDO can beinduced in microglia by interferon-γ-producing T helper(Th) 1 cells, thereby initiating a negative feedback loopwhich downmodulates neuroinflammation in experimentalautoimmune encephalomyelitis (EAE), the animal model ofmultiple sclerosis (MS). This protective effect could to becounteracted by the production of neurotoxic metabolites ofthe kynurenine pathway such as quinolinic acid, which areproduced upon IDO induction. Some metabolites of thekynurenine pathway can pass the blood–brain barrier andthus could act as neurotoxins, e.g., during systemicinfection. In this paper, we give a brief overview onestablished immune regulatory functions of IDO, reviewrecent data on IDO expression in the brain, and proposethat autoimmune neuroinflammation and the increasinglyappreciated neuronal damage in MS are linked by Th1-mediated IDO induction through subsequent synthesis oftoxic metabolites of tryptophan.
Keywords Indoleamine-2 . 3-dioxygenase . Interferon .
Tryptophan
Introduction
Mammals have two different oxygenases for the degrada-tion of the essential amino acid tryptophan (Trp). Thetryptophan dioxygenase (TDO), which is primarily
J Mol Med (2007) 85:1351–1359DOI 10.1007/s00109-007-0229-7
E. KwidzinskiInstitute of Cell Biology and Neurobiology, Charite,Berlin, Germany
I. Bechmann (*)Institute of Clinical Neuroanatomy, Senckenbergische Anatomie,J.W. Goethe-University,Theodor-Stern Kai 7,60590 Frankfurt, Germanye-mail: [email protected]
ERIK KWIDZINSKI
received his Ph.D. in neuroim-munology from the Charité,Berlin, Germany. Currently heworks as a post doc, at theInstitute of Cell Biology andNeurobiology, Center for Anat-omy at Charité. His researchdeals with the regulation ofimmune processes within CNSafter trauma and autoimmuneinflammation.
INGO BECHMANN
received his M.D. and habilita-tion at Charité, Berlin, where hebecame junior professor in 2002and professor in 2004. Since2006, he works at the Institute ofClinical Neuroanatomy, JohannWolfgang Goethe-University,Frankfurt. He is interested in themechanisms maintainingimmune privilege in the brainand how they are related tohuman disorders such as multiplesclerosis, Alzheimer’s disease,and Parkinson’s disease.

expressed within the liver, catabolizes the main part ofdietary Trp for the maintenance of serum levels. The secondenzyme is the indoleamine 2,3-dioxygenase (IDO), whichrepresents the first and rate-limiting enzyme of thekynurenine pathway in extrahepatic tissues. This enzymewas first described by Higuchi et al. [1]. IDO is a heme-containing enzyme that catalyzes the oxidative cleavage ofthe Trp pyrrol ring, thereby producing N-formyl-kynurenine,which is then further degraded along the kynureninepathway (Fig. 1).
IDO expression is inducible by the proinflammatorycytokine interferon-γ (IFN-γ) and to a lower extent byinterferon-β (IFN-β) in several cell types including macro-phages, dendritic cells (DC), and fibroblasts [2–5]. In thebrain, murine and human microglia have been shown toexpress IDO upon treatment with IFN-γ [6, 7]. Inperipheral tissues, IDO expression is a common mechanismto suppress the proliferation of infectious parasites such asChlamydia trachomatis [8] and Toxoplasma gondii [9, 10]through Trp depletion. Moreover, metabolites of thekynurenine pathway also exhibit immune modulatoryfunctions, e.g., during tumor maintenance [11] and allograftacceptance/rejection [12, 13].
During experimental autoimmune encephalomyelitis(EAE), IDO induction has been shown to downmodulateneuroinflammation [14–16]. However, the induction of
IDO in the central nervous system (CNS) is delicatebecause several metabolites of the kynurenine pathwayhave well-established neurotoxic effects [17]. Given thatmultiple sclerosis (MS) is characterized by the massiveinflux of activated T helper (Th) 1 cells and loss of neurons,an increasingly appreciated hallmark of this disease [18,19], we propose that neuroinflammation and neurodegen-eration are linked by IFN-γ-mediated IDO induction andthe accompanying production of toxic Trp metabolites.
IDO in infection
Over the last decades, many studies with human cellsshowed that IFN-γ-induced IDO expression represents animportant mechanism of antimicrobial resistance to para-sites [9, 20, 21] and bacteria [8, 22, 23]. In all these cases,the functional expression of IDO and the subsequentdegradation of Trp were identified as the effector mecha-nisms of microbial suppression. Induction of the kynureninepathway was recently shown to be involved in down-modulation of a fungal infection of the gastrointestinal tractwith Candida albicans [24]. In vivo, inhibition of IDOexacerbated the infection and its associated inflammatorypathology. In extension of previous studies, Montagnoli et al.[25] demonstrated a reduced number of CD4+ CD25+regu-latory T cells (Tregs) in C. albicans-infected animals afterIDO inhibition. This cell type is capable of downmodulatinginflammatory and antifungal Th1 immunity in C. albicans-infected mice. In fact, the strain of C. albicans used in theseexperiments was Trp prototrophic. Therefore, the antifungaleffect of IDO expression is likely to be mediated through themodification of the host’s T cell.
Recent data demonstrate that IDO also plays a role inviral infections. The replication of cytomegalovirus andherpes simplex type I and II has been shown to be restrictedby IFN-γ-induced IDO expression [26–28]. Oppositeeffects have been observed in the course of CNS infectionwith the human immunodeficiency virus (HIV). IDOactivity is also increased in response to this virus [29], butIDO inhibition by 1-methyl Trp does not increase but ratherdecrease the viral burden. Remarkably, IDO inhibitionamplified the number of HIV-specific cytotoxic T cells inHIV-infected severe combined immunodeficiency mice[30]. The HIV virus-infected cells seem to protect them-selves from killer cell-mediated lysis by immunomodula-tion, thereby providing a niche hiding the virus from theimmune system. Thus, during infection, IDO induction canexert divergent effects: On the one hand, it limits growth ofinfectious agents but also the strength of the immuneresponse. The latter may be important to limit loss ofinfected cells in organs of poor regenerative capacity at theprize of viral persistence [31, 32].
Fig. 1 The kynurenine pathway. Enzymatic degradation of tryptophanto kynurenic acid or quinolinic acid via the kynurenine pathway.Neurotoxic metabolites are labeled in italics
1352 J Mol Med (2007) 85:1351–1359

Possible mechanisms of IDO-mediated toleranceinduction
In contrast to the liver, Trp degradation is restricted topathologic conditions in all other organs. The functionalexpression of IDO initiates the kynurenine pathway duringwhich the degradation progresses along several enzymaticreactions (Fig. 1). Intermediates such as kynurenic acid(KA), quinolinic acid (QUIN) and 3-hydroxyanthranilicacid (3-HAA) have strong effects on many cell typesincluding lymphocytes and antigen-presenting cells (APC).Munn et al. [33] were the first to demonstrate that blockingthe IDO during pregnancy in mice causes tolerancebreakdown and fetus rejection. Since then, several studieshave confirmed a major role of IDO in the maintenance ofimmune tolerance [16, 34]. Two mechanisms have beenproposed to explain the downmodulatory effect of IDOactivation on T cells:
1) Munn et al. [33] hypothesized that in analogy of itsfunction during infection, IDO activity creates a Trp-depleted microenvironment limiting the proliferation ofT cells.
2) Fallarino et al. [4] showed that Trp degradationproducts enhance the susceptibility of T cell toapoptosis.
In fact, IDO activity depletes Trp from the culturemedium of human macrophages and activated T cellscultured in such medium arrest in a late G1 phase [35].This Trp starvation-mediated arrest has been shown to becaused in part by the stress-activated GCN2 kinase [36].However, T cells not only stop proliferation when they arekept under Trp-depleted conditions, they also becomehighly sensitive to CD95L (FasL)-induced apoptosis [37].CD95L-mediated deletion of activated T cells is a commonmechanism of self-limitation of inflammation [38] andimportant to minimize inflammation-mediated damage insensitive tissues such as the brain and the eye [39].
While IDO is inducible in many cell types, its regulationin DC turns out to be decisive for shifting the balancebetween tolerance and immunity. DC are professional APC.The type of DC presenting an antigen determines the T cell-polarizing signals and thus the T cell differentiation intoTh1, Th2, or Treg. In the case of tolerance induction, thecytotoxic T lymphocyte-associated antigen 4 (CTLA-4)plays a crucial role. CTLA-4 blocks the CD28-B7 costimu-latory signaling, which is essential for functional T cellactivation [40]. CTLA-4 immonoglobulin (CTLA-4-Ig)induces IFN-γ expression in DC and thereby an auto- orparacrine induction of IDO expression in the local micro-environment, providing the conditions for long-term sur-vival of allogeneic islet transplants [41]. In cell cultures, DC
expressing B220 or CD8α upregulate IDO expression whenthey are cocultured with CTLA-4-expressing T cells [42].
IDO-expressing DC inhibit T cell proliferation in vitroeven when Trp is still available in the medium [43]. Thiseffect is caused by kynurenine, 3-hydroxyanthranilin, and3-HAA, which are all Trp metabolites produced down-stream of the kynurenine pathway [44]. Moreover, 3-HAAand QUIN induce CD95L-independent apoptosis viacaspase 8 in activated Th1 but not Th2 cells [4]. Thiseffect can be increased by lowering Trp concentrations incell cultures [43]. The restriction of these effects to Th1cells may represent an IDO-dependent mechanism ofimmune deviation during inflammation.
Interestingly, in CD123+DC, IDO expression is inducedby interleukine 10 (IL-10), an anti-inflammatory cytokineexpressed by Treg cells [45]. While in most investigated invitro models, IFN-γ is the main inducer of IDO inmacrophages, DC, fibroblasts, and microglia [2–5, 46], itsexpression can also be triggered by lipopolysaccharide(LPS) through an IFN-γ-independent mechanism [47]. Theinduction of IDO expression without IFN-γ signaling is notdependent on signal transducer and activator of transcription1α and interferon regulatory factor-1 but requires p38mitogen-activated protein kinase and nuclear factor-κB[48]. Thus, IDO induction is not restricted to Th1 cellssecreting INF-γ but alternate triggers involving IL-10 andLPS. This is in line with the observation that Th2-mediatedexperimental asthma is also abrogated by functionalexpression of IDO [49].
An undesirable case of tolerance induction is themanifestation of tumors. The first recognition of tumorantigens by T cells occurs in the tumor draining lymphnodes. Within such lymph nodes, there is a population ofplasmocytoid DC (PDC) expressing B220, CD11c, andCD19. These PDC induce T cell anergy and immunosup-pression in vivo by the constitutive expression of IDO [50].CD19+PDC are also found in neighboring lymph nodes andspleen, but in contrast to the PDC from tumor drainingsentinal lymph nodes, they do not express IDO constitu-tively. The tumor itself is therefore likely to trigger IDOexpression in draining lymph nodes by an as yet unknownmechanism. One possible way of induction could be thebinding of CTLA-4 expressed by Tregs, which have beenshown to induce IDO expression in DC in vitro [44, 51].The adoptive transfer of IDO expressing PDC in vivoinduces not only a systemic unresponsiveness to antigens[52] but also antigen-specific anergy of T cells withinlymph nodes [50].
Tolerogenic mechanisms are not only active in sentinallymph nodes but were also found within the tumor itself,and IDO expression may represent one of such mechanisms[34]. In fact, the tumor cell line P815 becomes resistantagainst immunological deletion when the cells were trans-
J Mol Med (2007) 85:1351–1359 1353

fected for constitutive IDO expression. In ovarian andcolorectal cancer, IDO expression within the tumorscorrelates to malignancy [53]. In support of this concept,colorectal tumors exhibiting a high IDO activity have asignificantly reduced number of CD3+ infiltrating T cellsand show an increased frequency of metastases [54]. Thus,determining IDO expression in tumors may be used forclinical prognostic in the future. Moreover, IDO inhibitorscould increase the success of antitumor treatment [11].
The kynurenine-pathway and neurotoxic metabolitesin the brain
Two Trp degradation products, QUIN and 3-HAA,exhibit neurotoxic properties. QUIN is an endogen N-methyl-D-aspartate (NMDA) receptor agonist [55]. Atmicromolar concentrations, the excitotoxic effect of QUINcan be mimicked in primary cortical neuronal cell cultures[56]. The same effect is found in vivo where intracerebralinjection of QUIN induces excitotoxic lesions [17]. Thesecond neurotoxic Trp metabolite is 3-HAA, which isunstable under physiological conditions. Upon spontane-ous auto-oxidation, 3-HAA produces reactive radicalspecies, which in turn induce oxidative stress andapoptosis in neurons [57–59].
In a dead end side branch of the kynurenine pathway,KA is synthesized by kynurenine aminotransferases(KATs). KA is known as a noncompetitive NMDA receptorantagonist [60]. Therefore, KA might counteract theneurotoxic effect of QUIN. Indeed, blocking of thekynurenine pathway at the kynurenine hydroxylase stagereduced the neuronal damage after cerebral ischemia in vivo[61] and postischemic neuronal death in slice cultures [62].
As anticipated, such treatment forced Trp degradation tothe KA branch [59, 63]. To analyze the biological role ofKA, Yu et al. [64] created a knockout mouse deficient forKAT2 expression. KAT2 is the aminotransferase substan-tially contributing to the KA formation in the CNS [65].These mice exhibit a decreased KA formation within theCNS for the first 3 weeks of life, which afterward returnsto control levels as seen in wild-type mice. No significantdifferences in the production of QUIN or 3-HAA wereobserved at any age [64]. The delayed compensation wasassumed to be caused by the alternative KAT1 enzyme orby other enzymes that exhibit KAT activity. To analyze aneuroprotective effect of endogenous KA in vivo, Sapko et al.[66] induced excitotoxic lesions by the injection of QUIN in14-day-old KAT2−/− mice. In comparison to wild-type mice,the lesion volumes were significantly increased in theknockout. If the same experiment was performed in 2-month-old mice, the lesion volumes were similar in
knockout and wild-type animals. This suggests that theCNS-specific synthesis of KA by KATs represents a neuro-protective mechanism, which at least in part counteracts theneurotoxic effects of QUIN.
The neurotoxic effects caused by chronical induction ofthe kynurenine pathway have been analyzed in severaldiseases. Mackay et al. [67] reported an increased Trpkatabolism to kynurenine but not to QUIN in the serumfrom patients with brain injuries even several years afterinjury. They proposed that this might be a result ofincreased activity of IDO and/or TDO. QUIN accumulateswithin the cerebrospinal fluid (CSF) of humans aftertraumatic brain injuries [68] and is increased in the CNSbut not in the blood of gerbils after cerebral ischemia [69].It is therefore tempting to speculate that trauma-inducedIDO activation induces secondary neuronal damage viaaccumulation of neurotoxic metabolites. First evidence forthis hypothesis derives from studies of spinal cord injury.Inhibition of 3-HAA oxygenase attenuated QUIN accu-mulation after spinal cord injury and reduced the severityof injury-related functional deficits [70, 71]. A similarmechanism may also be active in HIV encephalopathy.HIV-infected macrophages within the CNS express IDO.The way of its induction by the virus is currently not clear,but it is plausible that IFN-γ or even virus particles them-selves trigger it [72]. However, HIV-1 is known to persistwithin the CNS [73], and as discussed above, its persistenceseems to involve IDO-mediated immune deviation [30].Thus, the chronic production of neurotoxic substances suchas QUIN may cause part of the damage leading to HIVdementia [74].
Increasing data show the involvement of the kynureninepathway in several neurodegenerative diseases such asParkinson’s, Huntington’s, and Alzheimer’s disease, epi-lepsy, and amyotrophic lateral sclerosis and in mentaldisorders such as schizophrenia and depression [75]. It isremarkable that even an acute injury of the brain induceslong-lasting alterations in Trp degradation with a shifttoward detrimental metabolites [67]. The respectiveenzymes thus are promising therapeutic targets for thefuture. However, it is noteworthy that many human cellsrespond to stimulation with IFN-γ, Tumor necrosis factor-α(TNF-α), and LPS by much higher IDO activities than theirmurine counterparts. On the other hand, only the lattersynthesize high amounts of reactive nitrogen species viainducible nitric oxide synthase induction in response tostimulation [76] rendering it difficult to transfer results fromanimal models to the human situation.
While the detrimental effects of QUIN and 3-HAA toneurons are well described, the cell types producingthese metabolites under pathologic conditions are illdefined. In primary cell cultures, microglia, astrocytes,
1354 J Mol Med (2007) 85:1351–1359

and neurons have been shown to express IDO uponIFN-γ stimulation. Mass spectrometry of QUIN in thesecultures revealed its degradation by astrocytes andneurons, suggesting that they do not contribute toneurotoxicity but to neuroprotection. On the other hand,stimulated microglia synthesize high amounts of QUIN[46]. This in vitro observation is in line with the immunehistological identification of IDO-positive microglia/mac-rophages in EAE and viral encephalitis [15, 72].Unfortunately, no marker exists to differentiate betweenintrinsic microglia and recruited macrophages. In activatedmacrophages, the kynurenine pathway is much moreeffective than in activated microglia [6, 46], and therefore,macrophages may provide significantly more harm forneurons.
Under physiological conditions, most Trp metabolites ofthe brain are primarily produced outside of the CNS. Thefirst substrate for the kynurenine pathway, Trp, is trans-ported into the CNS by large neutral amino acid trans-porters [77]. However, in the absence of local inflammatorysignals, the vast majority of Trp is not degradative toneurotoxic substances [78]. L-Kynurenine is also importedinto the CNS by large neutral amino acid transporters andsubsequently taken up by astrocytes and maybe microglia[79]. 3-Hydroxykynurenine is incorporated in the same wayas L-kynurenine. Both substrates are then degradativedepending on the distribution of downstream enzymes andthe glial subtype.
Activated microglia secrete high amounts of neurotoxic3-HAA and QUIN, while astrocytes synthesize but do notrelease significant quantities of QUIN [46]. In cell culture ofhuman astrocytes, IFN-γ induces not only the degradation ofneurotoxic 3-HAA and QUIN but also enhances theproduction of neuroprotective KA. [46]. Thus, astrocytesmight counteract the production of neurotoxins by microglia.
In the CNS of gerbils, 85% of extracellular QUIN isimported from the blood into the brain under normalconditions, while almost all (96%) QUIN is producedwithin the CNS after intracerebral LPS stimulation. Aftersystemic immune activation, almost all QUIN within theCNS is imported from the blood raising the intriguingquestion of whether peripheral QUIN production, e.g.,during infection, may provide harm to the brain [78].
In summary, kynurenines produced in the periphery canenter the CNS through the blood–brain barrier, where theycan be taken up and degraded by glial cells in an IDO-independent way. It is currently unclear whether thiscapacity of glial cells can fully protect neurons under allconditions of peripheral pathology. In case of local damage,astrocytes seem to eliminate neurotoxins produced bymicroglia. If this delicate balance is deranged by infiltratingmacrophages remains to be evaluated.
The kynurenine pathway in EAE and MS
Like many autoimmune diseases, MS is characterized bywaxing and waning inflammation in the target organ. Whatinitiates the onset of individual attacks is poorly under-stood, but there is some insight from animal models intowhat drives their termination and what cause tissue damage.In EAE, the animal model for MS, autoimmunity to myelinepitopes is induced by immunization with myelin epitopesor transfer of myelin-specific Th1 cells. Subsequently,leukocytes accumulate in perivascular cuffs around brainblood vessels. Many of these cells are Th1 lymphocytes,but there is also a high percentage (depending on themodel, approx. 50%) of macrophages [80]. As a result ofthis inflammation, myelin is phagocytosed by macrophagesand activated microglia. In addition, there is a significantdegeneration of axons and neurons, which for long hasbeen neglected [18, 19].
During the acute phase of EAE, tissue levels of theneurotoxin QUIN are increased in the lumbar and sacralparts of the spinal cord. Interestingly, the clinical diseaseseverity and the QUIN concentration in the cervicolumbarspinal cord correlate well [81]. Immunohistochemicalstudies have shown that enzymes of the kynureninepathway such as the IDO and kynurenine 3-mono-xygenaseare mainly expressed by infiltrating macrophages/activatedmicroglia in the perivascular/juxtavascular area during theacute phase of EAE [15, 56]. IDO expression and activity isincreased in the acute and remission phase of EAE. Themain inducer of IDO, the proinflammatory cytokine IFN-γ,is the key cytokine of encephalitogenic Th1 cells. TNF-α isalso secreted by these Th1 cells and acts synergistically
Fig. 2 The dual role of IDO: immune regulation and bystanderdamage. Immune regulation (left side): Infiltrating Th1 cells (T)secrete high amounts of interferon-γ inducing IDO expression inmicroglia (MG). Through the subsequent Trp depletion and productionof toxic metabolites, T cell growth is inhibited, and apoptosis issupported. This negative feedback loop may underlie the self-limitation of inflammation not only in MS. Bystander damage (rightside): IDO induction causes enhanced production of neurotoxins suchas QUIN and 3-HAA. Excessive production during neuroinflamma-tion is likely to contribute to neurodegeneration
J Mol Med (2007) 85:1351–1359 1355

with IFN-γ on the induction of IDO in macrophages andmicroglia [2, 6].
In analogy to the experiments by Munn et al. [33] in theplacenta, the net effect of IDO induction during neuro-inflammation has been tested by in vivo inhibition experi-ments. Daily application of the IDO inhibitor 1-methyl-Trpclearly exacerbated disease development and reduced theclinical recovery [14, 15]. The effects of IDO inhibitionwere similar when the treatment started in the preclinicalphase [14] or at the onset of the acute phase of disease [15].This observation suggests that the inhibition of IDO in theperiphery is not crucial for disease development. Conse-quently, the local induction of the kynurenine pathway andthe accompanying synthesis of Trp metabolites appear todownmodulate autoimmune CNS inflammation.
Recently, the anti-inflammatory effect of the kynureninepathway reaction products was shown by intraperitoneallyinjection of 3-HAA and oral administration of its synthesizedderivate N-3,4-dimethoxycinnamoyl anthranilic acid (DAA).Both substances significantly reduced the relapse phase inimmunized SJL mice [16]. Splenocytes from animals thathad been treated with 3-HAA or 2,4-DAA showed decreasedproliferation of T cells and expression of IFN-γ and TNF-α.Moreover, treatment of immunized mice with 3-HAA or 3,4-DAA also shifted inflammatory lymph node cells to apotentially regulatory cell type with a decreased IFN-γsecretion and an increased production of IL-10 [16].
From all these studies in EAE, one can interpret IDOinduction by IFN-γ-secreting Th1 cells as a protectivenegative feedback loop eventually terminating neuroin-flammation [15]. However, this interpretation by no meansexcludes significant bystander damage through toxic Trpmetabolites as the downside of such self-limitation (Fig. 2).Conversely, the apparent tight control over IDO expressionin the brain supports this view. Currently, little is known as tothe induction of IDO and the subsequent synthesis ofbioactive kynurenines within the CNS duringMS. Kepplingeret al. [82] described an increase in KA in the CSF of MSpatients during relapse, and Barans et al. [83] described lowactivities of the KA synthesizing enzymes KAT I and KAT IIin postmortem MS brains. The latter results were supportedby the analysis of CSF probes from MS patients where adecrease in KA was found in the relapse phases [84].However, changes in the synthesis of KA do not necessarilylead to an alteration in the synthesis of QUIN or 3-HAA.Consequently, modulation of the kynurenine pathway inhuman MS remains to be further investigated.
The overall beneficial effects of IFN-β treatment inMS are poorly understood but often explained by a shiftfrom Th1 to Th2-mediated immune responses. Interest-ingly, IFN-β induces the kynurenine pathway and thesynthesis of QUIN in human macrophages, although to alesser extent than IFN-γ [5]. This is in line with the
observation that treatment with IFN-β increased therelative IDO activity in blood serum samples (Kyn/Trp)from MS patients [85]. However, increased IDO activitywas not found in specimens deriving from patients whoreceived long-term treatment with IFN-β. This is of note, asQUIN and 3-HAA induce secondary degeneration of neuronsand potentially of oligodendrocytes [86]. This must be takeninto account when testing therapeutical strategies targeting thekynurenine pathway in MS. Moreover, the contribution ofTrp metabolites to the increasingly appreciated axonal andneuronal damage in MS [19] must be further explored.
References
1. Higuchi K, Kuno S, Hayaishi O (1963) Enzymic formation ofD-kynurenine. Fed Proc 22:243
2. Carlin JM, Borden EC, Sondel PM, Byrne GI (1989) Interferon-induced indoleamine 2,3- dioxygenase activity in human mono-nuclear phagocytes. J Leukoc Biol 45:29–34
3. Currier AR, Ziegler MH, Riley MM, Babcock TA, Telbis VP,Carlin JM (2000) Tumor necrosis factor-alpha an lipopolysaccha-ride enhances interferon-induced antichlamydial indoleamine diox-ygenase activity independently. J Interferon Cytokine Res 20:369–376
4. Fallarino F, Grohmann U, Vacca C, Bianchi C, Orabona C, SprecaA, Fioretti MC, Lucetti P (2002) T cell apoptosis by tryptophancatabolism. Cell Death Differ 9:1069–1077
5. Guillemin GJ, Kerr SJ, Pemberton LA, Smith DG, Smythe GA,Armati PJ, Brew BJ (2001) IFN-beta1b induces kynureninepathway metabolism in human macrophages: potential implica-tions for multiple sclerosis treatment. J Interferon Cytokine Res21:1097–1010
6. Alberati-Giani D, Ricciardi-Castagnoli P, Kohler C, Cesura AM(1996) Regulation of the kynurenine metabolic pathway byinterferon-gamma in murine cloned macrophages and microglialcells. J Neurochem 66:996–1004
7. Heyes MP, Achim CL, Wiley CA, Major EO, Saito K, Markey SP(1996) Human microglia convert L-tryptophan into the neurotoxinquinolinic acid. Biochem J 320:595–597
8. Nettelnbreker E, Zeidler H, Bartels H, Dreses-Werringloer U,Daubener W, Holtmann H, Kohler L (1998) Studies ofpersistent infection by Chlamydia trachomatis serovar K inTPA-differentiated U937 cells and the role of IFN-gamma. JMed Microbiol 47:141–149
9. Pfefferkorn ER (1984) Interferon gamma blocks the growth ofToxoplasma gondii in human fibroblasts by inducing the host cellto degrade tryptophan. Proc Natl Acad Sci 81:908–912
10. Daubener W, MacKenzie CR (1999) IFN-gamma activatedindoleamine 2,3- dioxygenase activty in human cells is anantiparasitic and an antibacterial effector mechanism. Adv ExpMed Biol 467:517–524
11. Muller AJ, Prendergast GC (2005) Marrying immunotherapy withchemotherapy: why say IDO? Cancer Res 65:8065–8068
12. Bauer TM, Jiga LP, Chuang JJ, Randozzo M, Opelz G, Terness P(2005) Studying the immunosuppressive role of indoleamine 2,3-dioxygenase: tryptophan metabolites suppress rat allogeneicT-cell responses in vitro and in vivo. Transpl Int 18:95–100
13. Li Y, Tredget EE, Ghaffari A, Lin X, Kilani RT, Ghahary A (2006)Local expression of indoleamine 2,3-dioxygenase protects engraft-ment of xenogeneic skin substitute. J Invest Dermatol 126:128–136
1356 J Mol Med (2007) 85:1351–1359

14. Sakurai K, Zou JP, Tschetter JR, Ward JM, Shearer GM (2002)Effect of indoleamine 2,3-dioxygenase on induction of experi-mental autoimmune encephalomyelitis. J Neuroimmunol129:186–196
15. Kwidzinski E, Bunse J, Aktas O, Richter D, Mutlu L, Zipp F,Nitsch R, Bechmann I (2005) Indoleamine 2,3-dioxygenase isexpressed in the CNS and down-regulates autoimmune inflam-mation. FASEB J 19:1347–1349
16. Platten M, Ho PP, Youssef S, Fontoura P, Garren H, Hur EM,Gupta R, Lee LY, Kidd BA, Robinson WH, Sobel RA, Selly ML,Steinmann L (2005) Treatment of autoimmune neuroinflammationwith a synthetic tryptophan metabolite. Science 310:850–855
17. Schwarcz R, Whetsell WO Jr, Mangano RM (1983) Quinolinicacid: an endogenous metabolite that produces axon-sparinglesions in rat brain. Science 219:316–318
18. Aktas O, Smordochenko A, Brocke S, Infante-Duarte C, TopphoffUS, Vogt J, Prozorovski T, Meier S, Osmanova V, Pohl E,Bechmann I, Nitsch R, Zipp F (2005) Neuronal damage inautoimmune neuroinflammation mediated by the death ligandTRAIL. Neuron 46:421–432
19. Zipp F, Aktas O (2006) The brain as a target of inflammation:common pathways link inflammatory and neurodegenerativediseases. Trends Neurosci 29:518–527
20. Sanni LA, Thomas SR, Tattam BN, Moore DE, Chaudhri G,Stocker R, Hunt NH (1998) Dramatic changes in oxidativetryptophan metabolism along the kynurenine pathway in experi-mental cerebral and noncerebral malaria. Am J Pathol 152:611–619
21. Silva NM, Rodrigues CV, Santoro MM, Reis LF, Alvarez-Leite JI,Gazzinelli RT (2002) Expression of indoleamine 2,3-dioxygenase,tryptophan degradation and kynurenine formation during in vivoinfection with Toxoplasma gondii: induction by endogenousgamma interferon and requirement of interferon regulatory factor1. Infect Immun 70:859–868
22. Beatty WL, Belanger TA, Desai AA, Morrison RP, Byrne GI(1994) Tryptophan depletion as a mechanism of gamma interfer-on-mediated chlamydial persistence. Infect Immun 62:3705–3711
23. MacKenzie CR, Hadding U, Daubener W (1998) Interferon-gamma-induced activation of indoleamine 2,3-dioxygenase incord blood monocyte-derived macrophages inhibits the growthof group B streptococci. J Infect Dis 178:875–878
24. Bozza S, Fallarino F, Pitzurra L, Zelante T, Montagnoli C,Bellochio S, Mosci P, Vacca C, Pucetti P, Romani L (2005) Acrucial role for tryptophan catabolism at the host/Candidaalbicans interface. J Immunol 174:2910–2918
25. Montagnoli C, Bacci A, Bozza S, Gaziano R, Mosci P, SharpeAH, Romani L (2002) B7/CD28-dependent CD4+CD25+ regula-tory T cells are essential components of the memory-protectiveimmunity to Candida albicans. J Immunol 169: 6298–6308
26. Bodaghi B, Goureau O, Zipeto D, Laurent L, Virelizier JL,Michelson S (1999) Role of IFN-gamma-induced indoleamine 2,3dioxygenase and inducible nitric oxide synthase in the replicationof human cytomegalovirus in retinal pigment epithelial cells. JImmunol 162:957–964
27. Adams O, Besken K, Oberdörfer C, MacKenzie CR, Rüßing D,Däubener W (2004) Inhibition of human herpes simplex virustype 2 by interferon γ and tumor necrosis factor a is mediated byindoleamine 2,3-dioxygenase. Microbes and Infection 6:806–812
28. Adams O, Besken K, Oberdörfer C, MacKenzie CR, Takikawa O,Däubener W (2004) Role of indoleamine-2,3-dioxygenase inalpha/beta and gamma interferon-mediated antiviral effects againstherpes simplex virus infections. J Virol 78:2632–2636
29. Sardar AM, Reynolds GP (1995) Frontal cortex indoleamine-2,3-dioxygenase activity is increased in HIV-1-associated dementia.Neurosci Lett 187:9–12
30. Potula R, Poluektova L, Knipe B, Chrastil J, Heilman D, Dou H,Takikawa O, Munn DH, Gendelman HE, Persidsky Y (2005)Inhibition of indoleamine 2,3-dioxygenase (IDO) enhances elim-ination of virus-infected macrophages in an animal model of HIV-1 encephalitis. Blood 106:2382–2390
31. Kwidzinski E, Mutlu LK, Kovac AD, Bunse J, Goldmann J,Mahlo J, Aktas O, Zipp F, Kamradt T, Nitsch R, Bechmann I(2003) Self-tolerance in the immune privileged CNS: lessons fromthe entorhinal cortex lesion model. J Neural Transm Suppl 65:29–49
32. Bechmann I (2005) Failed central nervous system regeneration: adownside of immune privilege? Neuromolecular Med 7:217–228
33. Munn DH, Zhou M, Attwood JT, Bondarev I, Conway SJ,Marshall B, Brown C, Mellor AL (1998) Prevention of allogeneicfetal rejection by tryptophan catabolism. Science 281:1122–1124
34. Uyttenhove C, Pilotte L, Theate I, Stroobant V, Colau D,Parmentier N, Boon T, Van den Eynde BJ (2003) Evidence for atumoral immune resistance mechanism based on tryptophandegradation by indoleamine 2,3-dioxygenase. Nat Med 9:1269–1274
35. Munn DH, Shafizadeh E, Attwood JT, Bondarev I, Pashine A,Mellor AL (1999) Inhibition of T cell proliferation by macrophagetryptophan catabolism. J Exp Med 189:1363–1372
36. Munn DH, Sharma MD, Baban B, Harding HP, Thang Y, Ron D,Mellor AL (2005) GCN2 kinase in T cells mediates proliferativearrest and anergy induction in response to indoleamine 2,3-dioxygenase. Immunity 22:633–642
37. Lee GK, Park HJ, Macleod M, Chandler P, Munn DH, Mellor AL(2002) Tryptophan deprivation sensitizes activated T cells toapoptosis prior to cell division. Immunology 107:452–460
38. Dehin J, Walczak H, Baumler C, Debatin KM, Kramer PH (1995)Autocrine T cell suicide mediated by APO-1 (Fas/CD95). Nature373:441
39. Bechmann I, Mor G, Nilsen J, Eliza M, Nitsch R, Naftolin F(1999) FasL (CD95L, Apo1L) is expressed in the normal rat andhuman brain: evidence for the existence of an immunologicalbrain barrier. Glia 27:62–74
40. De Jong EC, Smits HH, Kapsenberg ML (2005) Dendritic cell-mediated T cell polarization. Semin Immun 26:289–307
41. Grohmann U, Orabona C, Fallarino F, Vacca C, Calcinaro F,Falorni A, Candeloro P, Belladonna ML, Bianchi R, Fioretti MC,Pucetti P (2002) CTLA-4-Ig regulates tryptophan catabolism invivo. Nat Immunol 3:1097–1101
42. Mellor AL, Chandler P, Baban B, Hansen AM, Marshall B,Phikala J, Waldmann H, Cobbold S, Adams E, Munn DH (2004)Specific subsets of murine dendritic cells acquire potent T cellregulatory functions following CTLA4-mediated induction ofindoleamine 2,3 dioxygenase. Int Immunol 16:1391–1401
43. Frumento G, Rotondo R, Tonetti M, Damonte G, Benatti U, FerraraGB (2002) Tryptophan-derived catabolites are responsible forinhibition of T and natural killer cell proliferation induced byindoleamine 2,3-dioxygenase. J Exp Med 196:459–468
44. Terness P, Bauer TM, Rose L, Dufter C, Watzlik A, Simon H,Opelz G (2002) Inhibition of allogeneic T cell proliferation byindoleamine 2,3-dioxygenase-expressing dendritic cells: media-tion of suppression by tryptophan metabolites. J Exp Med196:447–457
45. Munn DH, Sharma MD, Lee JR, Jhaver KG, Johnson TS, KeskinDB, Marshall B, Chandler P, Antonia SJ, Burgess R, Slingluff CLJr, Mellor AL (2002) Potential regulatory function of humandendritic cells expressing indoleamine 2,3-dioxygenase. Science297:1867–1870
46. Guillemin GJ, Smythe G, Takikawa O, Brew BJ (2005)Expression of indoleamine 2,3-dioxygenase and production ofquinolinic acid by human microglia, astrocytes and neurons. Glia49:15–23
J Mol Med (2007) 85:1351–1359 1357

47. Fujigaki S, Saito K, Sekikawa K, Tone S, Takikawa O, Fujii H,Wada H, Noma A, Seishima M (2001) Lipopolysaccharideinduction of indoleamine 2,3-dioxygenase is mediated dominantlyby an IFN-gamma-independent mechanism. Eur J Immunol31:2313–2318
48. Fujigaki H, Saito K, Fujigaki S, Takemura M, Sudo K, IshiguroH, Seishima M (2006) The signal transducer and activator oftranscription 1alpha and interferon regulatory factor 1 are notessential for the induction of indoleamine 2,3-dioxygenase bylipopolysaccharide: involvement of p38 mitogen-activated proteinkinase and nuclear factor-kappaB pathways, and synergistic effectof several proinflammatory cytokines. J Biochem 139:655–662
49. Hayashi T, Beck L, Rossetto C, Gong X, Takikawa O,Takabayashi K, Broide DH, Carson DA, Raz E (2004) Inhibitionof experimental asthma by indoleamine 2,3-dioxygenase. J ClinInvest 114:270–279
50. Munn DH, Sharma MD, Hou D, Baban B, Lee JR, Antonia SJ,Messina JL, Chandler P, Koni PA, Mellor AL (2004) Expressionof indoleamine 2,3-dioxygenase by plasmacytoid dendritic cells intumor-draining lymph nodes. J Clin Invest 114:280–290
51. Fallarino F, Grohmann U, Hwang KW, Orabona C, Vacca C,Bianchi R, Belladonna ML, Fioretti MC, Alegre ML, Lucetti P(2003) Modulation of tryptophan catabolism by regulatory T cells.Nat Immunol 4:1206–1212
52. Grohmann U, Fallarino F, Silla S, Bianchi R, Belladonna ML,Vacca C, Micheletti A, Fioretti MC, Pucetti P (2001) CD40ligation ablates the tolerogenic potential of lymphoid dendriticcells. J Immunol 166:277–283
53. Okamoto A, Nikaido T, Ochiai K, Takakura S, Saito M, Aoki Y,Ishii N, Yanaihara N, Yamada K, Takikawa O, Kawaguchi R,Isonishi S, Tanaka T, Urashima M (2005) Indoleamine 2,3-dioxygenase serves as a marker of poor prognosis in geneexpression profiles of serous ovarian cancer cells. Clin CancerRes 11:6030–6039
54. Brandacher, G, Perathoner A, Ladurner R, Schneeberger S, ObristP, Winkler C, Werner ER, Werner-Felmayer G, Weiss HG, GöbelG, Margreiter R, Königsrainer A, Fuchs D, Amberger A (2006)Prognostic value of indoleamine 2,3-dioxygenase expression incolorectal cancer: effect on tumor-infiltrating T cells. Clin CancerRes 12:1144–1151
55. Stone TW, Perkins MN (1981) Quinolinic acid: a potentendogenous excitant at amino acid receptors in CNS. Eur JPharmacol 72:411–412
56. Chiarugi A, Meli E, Moroni F (2001) Similarities and differencesin the neuronal death processes activated by 3OH-kynurenine andquinolinic acid. J Neurochem 77:1310–1318
57. Eastman CL, Guilarte TR (1990) The role of hydrogen peroxide inthe in vitro cytotoxicity of 3-hydroxykynurenine. Neurochem Res15:1101–1107
58. Okuda S, Nishiyama N, Saito H, Katsuki H (1996) Hydrogenperoxide-mediated neuronal cell death induced by an endogenousneurotoxin, 3-hydroxykynurenine. Proc Natl Acad Sci USA93:12553–12558
59. Chiarugi A, Cozzi A, Ballerini C, Massacesi L, Moroni F(2001) Kynurenine 3-mono-oxygenase activity and neurotoxickynurenine metabolites increase in the spinal cord of rats withexperimental allergic encephalomyelitis. Neuroscience 102:687–695
60. Perkins MN, Stone TW (1982) An iontophoretic investigationof the actions of convulsant kynurenines and their interactionwith the endogenous excitant quinolinic acid. Brain Res 247:184–187
61. Cozzi A, Carpendeo R, Moroni F (1999) Kynurenine hydroxylaseinhibitors reduce ischemic brain damage: studies with(m-nitrobenzoyl)-alanine (mNBA) and 3,4-dimethoxy-[-N-4-(nitrophenyl)thiazol-2yl]-benzenesulfonamide (Ro 61–8048) in
models of focal or global brain ischemia. J Cereb Blood FlowMetab 19:771–777
62. Carpenedo R, Meli E, Peruginelli F, Pellegrini-Giampietro DE,Morini F (2002) Kynurenine 3-mono-oxygenase inhibitors attenuatepost-ischemic neuronal death in organotypic hippocampal slicecultures. J Neurochem 82:1465–1471
63. Moroni F, Russi P, Gallo-Mezo MA, Moneti G, Pellicari R (1991)Modulation of quinolinic and kynurenic acid content in the ratbrain: effects of endotoxins and nicotinylalanine. J Neurochem57:1630–1635
64. Yu P, Di Prospero NA, Sapko MT, Cai T, Chen A, Melendez-Ferro M, Du F, Whetsell WO Jr, Guidetti P, Schwarcz R, TagleDA (2004) Biochemical and phenotypic abnormalities inkynurenine aminotransferase II-deficient mice. Mol Cell Biol24:6919–6930
65. Guidetti P, Okuno E, Schwarcz R (1997) Characterization of ratbrain kynurenine aminotransferases I and II. J Neurosci Res50:457–465
66. Sapko MT, Guidetti P, Yu P, Tagle DA, Pellicari R, Schwarcz R(2006) Endogenous kynurenate controls the vulnerability ofstriatal neurons to quinolinate: Implications for Huntington’sdisease. Exp Neurol 197:31–40
67. Mackay GM, Forrest CM, Stoy N, Christofides J, Egerton M,Stone TW, Darlington LG (2006) Tryptophan metabolism andoxidative stress in patients with chronic brain injury. Eur J Neurol13:30–42
68. Sinz EH, Kochanek PM, Heyes MP, Wisniewski SR, Bell MJ,Clarks RS, DeKosky ST, Blight AR, Marion DW (1998)Quinolinic acid is increased in CSF and associated with mortalityafter traumatic brain injury in humans. J Cereb Blood Flow Metab18:610–615
69. Saito K, Nowak TS Jr, Markey SP, Heyes MP (1993) Mechanismof delayed increases in kynurenine pathway metabolism indamaged brain regions following transient cerebral ischemia. JNeurochem 60:180–192
70. Blight AR, Cohen TI, Saito K, Heyes MO (1995) Quinolinic acidand functional deficits following experimental spinal cord injuriy.Brain 118:735–752
71. Yates JR, Heyes MP, Blight AR (2006) 4-chloro-3-hydroxyanthrani-late reduces local quinolinic acid synthesis, improves functionalrecovery and preserves white matter after spinal cord injury. JNeurotrauma 23:866–881
72. Depboylu C, Reinhardt TA, Takikawa O, Imai Y, Maeda H,Mitsuya H, Rausch D, Eiden LE, Weihe E (2004) Brain virusburden and indoleamine-2,3-dioxygenase expression duringlentiviral infection of rhesus monkey are concomitantlylowered by 6-chloro-2′,3′-dideoxyguanosine. Eur J Neurosci19:2997–3005
73. An SF, Groves M, Gray F, Scaravilli F (1999) Early entry andwidespread cellular involvement of HIV-1 DNA in brains of HIV-1 positive asymptomatic individuals. J Neuropathol Exp Neurol58:1156–1162
74. Lawrence DM, Major EO (2002) HIV-1 and the brain: connectionsbetween HIV-1-associated dementia, neuropathology and neuro-immunology. Microbes Infect 4:301–308
75. Nemeth H, Toldi J, Vecsei J (2006) Kynurenines, Parkinson’sdisease and other neurodegenerative disorders: preclinical andclinical studies. J Neural Transm Suppl 70:285–304
76. Roshick C, Wood H, Caldwell HD, McClarty G (2006)Comparison of gamma interferon-mediated antichlamydial de-fense mechanisms in human and mouse cells. Infect Immun74:225–238
77. Boado RJ, Li JY, Nagaya M, Zhang C, Pardridge WM (1999)Selective expression of the large neutral amino acid transporterat the blood-brain barrier. Proc Natl Acad Sci USA 96:12079–1284
1358 J Mol Med (2007) 85:1351–1359

78. Beagles KE, Morrison PF, Heyes MP (1998) Quinolinic acid invivo synthesis rates, extracellular concentrations and intercom-partmental distributions in normal and immune-activated brain asdetermined by multiple-isotope microdialysis. J Neurochem70:281–291
79. Fukui S, Schwarcz R, Rapoport SI, Takada Y, Smith QR (1991)Blood–brain barrier transport of kynurenines: implications forbrain synthesis and metabolism. J Neurochem 56:2007–2017
80. Raine CS (1991) Multiple sclerosis: a pivotal role for the T cell inlesion development. Neuropathol Appl Neurobiol 17:265–274
81. Flanagan EM, Erickson JB, Viveros OH, Chang SY, Reinhard JFJr (1995) Neurotoxin quinolinic acid is selectively elevated inspinal cords of rats with experimental allergic encephalomyelitis. JNeurochem 64:1192–1196
82. Kepplinger B, Baran H, Kainz A, Newcombe J, Nohl H (2001)Altered kynureninc acid levels in CSF and serum of patients
with multiple sclerosis. ECTRIMS’2001. Mult Scler Abstr 118(Suppl 1)
83. Baran H, Kepplinger B, Newcombe J, Stolze K, Kainz A, Nohl H(2000) Lowered kynurenine aminotransferase activities in CNS ofMS Patients. Society for Neuroscience 30th Annual Meeting,Abstract no. 1302
84. Rejdak K, Bartosik-Psujek H, Dobosz B, Grieb P, Giovannoni G,Turski WA, Stemasiak Z (2002) Decreased level of kynurenic acidin cerebrospinal fluid of relapsing-onset multiple sclerosispatients. Neurosci Lett 331:63–65
85. Amirkhani A, Rajda C, Arvidsson B, Bencsik K, Bodak K, SeresE, Markides KE, Vecsej L, Bergquist J (2005) Interferon-betaaffects the tryptophan metabolism in multiple sclerosis patients.Eur J Neurol 12:625–631
86. Cammer W (2001) Oligodendrocyte killing by quinolinic acid invitro. Brain Res 896:157–160
J Mol Med (2007) 85:1351–1359 1359

REVIEW ARTICLE
Primary immune surveillance: some like it hot
Joseph J. Skitzki & Qing Chen & W. C. Wang &
Sharon S. Evans
Received: 17 April 2007 /Revised: 11 June 2007 /Accepted: 29 June 2007 / Published online: 18 August 2007# Springer-Verlag 2007
Abstract The thermal element of fever has been found tobe beneficial in models of infectious disease. The con-tributions of fever-range temperatures to the efficacy of theadaptive immune response have only begun to be delineat-ed. There is accumulating evidence that fever-range thermalstress bolsters primary immune surveillance of lymph nodesand Peyer patches by augmenting lymphocyte extravasationacross specialized vessels termed high endothelial venules.Molecular mechanisms have recently come to light bywhich the thermal component of fever alone may promotelymphocyte trafficking, and thereby the probability ofmounting a defense against microbial infection. Acquiredknowledge of the molecular changes associated withthermal stress may allow for the development of noveltherapies for a variety of disease processes.
Keywords Hyperthermia . Lymphocyte trafficking .
Primary immune surveillance . IL-6
Introduction
Fever is one of the most common but least understood of thebiological processes associated with inflammation [1].Debate continues over both the potential harms andbenefits afforded by this physiologic function. In terms ofevolution, fever is highly conserved despite the associatedincrease in metabolic demands. Evidence for the benefits offever is noted in both homeothermic (warm-blooded) and
poikilothermic (cold-blooded) animals. Experiments havedemonstrated the ability of poikilotherms to alter theirbehavior during infection and migrate to warmer environ-ments, thereby elevating their core body temperatures [2,3]. This heat-seeking behavior has been linked to improvedsurvival [2, 4, 5] and could be abrogated with the use ofantipyretics [6]. Homeothermic mammals also demonstrateimproved survival with fever in models of infection.Multiple studies in mice, rabbits, and dogs have shownsimilar findings of increased survival even when body
J Mol Med (2007) 85:1361–1367DOI 10.1007/s00109-007-0245-7
J. J. Skitzki :Q. Chen :W. C. Wang : S. S. Evans (*)Department of Immunology, Roswell Park Cancer Institute,Elm & Carlton Streets,Buffalo, NY 14263, USAe-mail: [email protected]
JOSEPH SKITZKIreceived his M.D. from thePennsylvania State UniversityCollege of Medicine in Hershey,PA, USA. He is presently aclinical surgical oncology fellowat Roswell Park Cancer Institutewith an active interest inresearch. His area of researchinvestigates lymphocyte traf-ficking mechanisms in adoptiveimmunotherapy of cancer.
SHARON EVANS
received her Ph.D. from theUniversity of Buffalo in Buffalo,NY, USA. She is currently aProfessor of Oncology in theDepartment of Immunology, atRoswell Park Cancer Institute,Buffalo, NY, USA. Her researchfocuses on the intersectionbetween cytokine signal trans-duction pathways and the in-flammatory mechanismsgoverning lymphocyte traffickingin health and disease.

temperatures are artificially increased to the range ofnatural fever [3, 7, 8]. However, fever may be detrimentalto the severely ill who cannot afford the increasedmetabolic demands [7, 9, 10]. Given this paradigm, fevermay be viewed as a beneficial adaptive response that haspersisted over millions of years. The role of the thermalcomponent of fever in regulating the immune system hasonly begun to be elucidated. The following review willdetail the potential contributions of the thermal element offever to primary immune surveillance.
Fever and hyperthermia in the context of disease
Before discussing temperature and its effect on the immunesystem, it is necessary to distinguish between the termsfever and hyperthermia. Fever is defined as a state ofelevated core temperature as a defensive response of a hostto pathogenic stimuli. In fever, elevation of the set point ofbody temperature increases core temperature via thermoef-fectors such as prostaglandins or cytokines [11]. Thisresponse is accompanied by a complex interplay ofcytokine networks and hemodynamic parameters such asvasodilatation and blood flow. Elevations in body temper-ature not associated with a change in the set point orthermoeffectors is called hyperthermia. Hyperthermia canbe induced by increasing the heat load and/or inactivatingheat dissipation by a variety of methods [11]. Fever is acomplex state that presents difficulty in dissecting thebiological changes associated with its thermal component.Given this complexity, a reductionist approach has beentaken in a number of studies to investigate the biologicaleffects of the thermal component of fever [7, 12]. Thus,experimentally induced hyperthermia differs from fevergeneration in organisms and avoids any confoundingvariables associated with natural fever such as endotox-emia, inflammatory cytokine elaboration, and/or neurohor-monal axis changes. Accordingly, induced hyperthermiacan be a useful tool to dissect the role of heat as one aspectof fever and its influence upon the immune system,specifically immune surveillance.
Immune surveillance by T and B lymphocytes of theadaptive immune system allows for a range of effectorresponses as well as the generation of memory topathogenic stimuli. Primary immune surveillance refers tothe ability of antigen-presenting cells and naïve lympho-cytes to colocalize in the unique environment of peripherallymph nodes (PLNs), which function as the first line ofdefense against microbial invaders entering the skin [13].For the purposes of this review, the gut interface consistingof Peyer patches (PPs) and mesenteric lymph nodes(MLNs) as sentinels of pathogens will also be consideredas components of primary immune surveillance. Dendritic
cells that function as professional antigen-presenting cellsenter lymph nodes via afferent lymphatics. Concurrently,naïve T cells continually enter through high endothelialvenules (HEVs) of lymph nodes in an attempt to enhancethe incredibly small chance that a particular cognate antigenwill be encountered by numerically rare T cells that expressan appropriate T cell receptor [14]. Upon presentation of anappropriate antigen, antigen-specific naïve T cells canundergo activation, expansion, and differentiation intomemory or effector phenotypes [13]. Given the grosslyabundant number of potential pathogens in the externalenvironment, the extensive recirculation of a diverse butfinite number of naïve lymphocytes into the lymph nodeshas evolved into a highly efficient and necessary compo-nent of the adaptive immune response. Notably, themechanisms of lymphocyte entry into lymph nodes viaHEVs are pivotal for the efficiency of this system in bothnormothermic and hyperthermic states.
Process of lymphocyte entry into lymph nodes
Lymphocyte entry into lymph nodes is a highly regulatedprocess orchestrated by adhesion molecules on both lym-phocytes and vascular endothelium. The high shear forceexerted on lymphocytes traveling through the bloodstreammakes their arrest and eventual extravasation into tissues atruly remarkable process. The multistep scheme of lympho-cyte trafficking involves four consecutive interdependentsteps consisting of tethering/rolling, chemokine activation,firm adhesion, and transendothelial migration [14, 15]. Theability of lymphocytes to roll along the endothelium andslow their velocity is mediated by the presence of selectin-homing receptors. In the case of blood-borne lymphocytesentering PLNs via HEVs, lymphocyte expression of L-selectin is required for initial tethering and rolling. L-selectinpresent on the cell surface of lymphocytes interacts with theglycoprotein complex known as PLN addressin (PNAd)displayed on the lumenal border of HEVs [16]. In the case ofMLNs or PPs of the gut, α4β7 integrin expressed onlymphocytes interacts with mucosal addressin cell adhesionmolecule-1 (MAdCAM-1) to generate rolling.
Transient rolling interactions allow the lymphocyte to“sample” the endothelium for factors that can promote firmarrest. Activation of lymphocytes to induce firm arrest ismediated by tissue-specific chemokines displayed onendothelial surfaces [17]. In mice, HEVs have the abilityto produce and display CCL21, the chemokine primarilyassociated with naïve lymphocyte activation [18, 19]. In atruly restricted fashion, CCL21 has the ability to onlyinteract with its specific receptor namely, CCR7, which isuniformly found on naïve and central memory T cells.Engagement of CCR7 leads to a rapid change in the affinity
1362 J Mol Med (2007) 85:1361–1367

and/or avidity of lymphocyte integrins for endothelialreceptors that mediate firm adhesion. The β2-integrin,lymphocyte function-associated antigen-1 (LFA-1), onlymphocytes binds strongly with the intercellular adhesionmolecule 1 or 2 (ICAM-1, ICAM-2) endothelial receptorsexpressed on HEVs. Upon integrin binding and firm arrestof the lymphocyte, extravasation into the lymphoid tissueoccurs, which is also thought to involve ICAM-1 [20].
The elegant cascade of aforementioned events that leadto colocalization of lymphocytes and antigen-presentingcells in the compartmentalized environment of the lymphnode is crucial for a successful adaptive immune response.Once in the lymph node, T and B cells migrate to theirrespective zones and interactions between the two popula-tions are believed to be chemokine mediated. T cellactivation by antigen-presenting cells that enter via afferentlymphatics subsequently occurs with the generation of apotent T and B cell response.
Enhanced lymphocyte–endothelial interactionswith hyperthermia
As a nontoxic treatment, whole-body hyperthermia (WBH)maintains an elevation of core body temperature byisolating an organism in a contained, temperature-controlled environment, thereby mimicking the thermalcomponent of fever [12, 21, 22]. As previously stated,elevated core body temperatures in the febrile range havebeen associated with improved survival in homeothermsand poikilotherms; however, alterations in the immunesystem during thermal stress were largely undefined. Fever-range thermal stress has previously been shown to increaselymphocyte priming, proliferation, and cytotoxicity [2, 21,23]. WBH also shortens the time to generate an immuneresponse by stimulating the migration of skin-deriveddendritic cells (i.e., Langerhans cells) to lymph nodeswhere they colocalize with arriving T lymphocytes [21, 24].Recently, lymphocyte recruitment to lymph nodes and PPs,a key component of primary immune surveillance, has beendemonstrated to improve with the application of fever-range WBH [25, 26].
Augmentation of primary immune surveillance by fever-range thermal stress is mediated by changes found both inthe lymphocyte as well as the endothelium (Fig. 1). In vivoexperiments in both mice and humans demonstrated aredistribution of lymphocytes after exposure to 6 h of WBHin the febrile range (39.5±0.5°C) with a transient decreasein the peripheral blood pool [26, 27]. Further utilizing themurine model, lymphocytes expressing either L-selectin orα4β7 integrin decreased in the peripheral blood andconcomitantly increased in PLNs and PPs. To determine ifthis redistribution was causally related to improved inter-
actions with HEVs, splenocytes taken from mice receivingWBH were examined in adhesion assays utilizing cryosec-tions of lymphoid tissue containing HEVs, i.e., Stamper–Woodruff assay [28]. A significant increase was noted inthe ability of splenocytes derived from WBH-treatedanimals to adhere to HEVs in frozen sections compared tosplenocytes from normothermic control mice.
The improved adhesion noted in PLN and PP HEVs wasdue to L-selectin/PNAd and α4β7/MAdCAM-1-mediatedprimary tethering and rolling interactions, respectively,which could be abrogated with the use of adhesion-blocking antibodies [26]. It is interesting to note that theimproved interactions were not due to a change in thesurface density of either L-selectin or α4β7 integrin, butrather an enhanced affinity and/or avidity, suggestive ofstructural changes of these molecules [29–31]. These invitro findings were further supported by in vivo lymphocytehoming studies. Hyperthermia treatment of L-selectin orα4β7 integrin-expressing lymphocytes in culture, beforeadoptive transfer into mice, yielded an approximate twofoldincrease in adoptively transferred cells found in PLNs orPPs, respectively [26, 29]. Notably, thermal treatment didnot override the intrinsic specificity of homing molecules asevidenced by the restricted entry of α4β7 integrin+/L-selectin− cells only in PPs and not PLNs [26].
Fever-range thermal stress has also been shown to actindependently upon HEVs to increase their adhesiveproperties as observed in multiple murine strains [25, 26].In vitro Stamper–Woodruff assays using PLNs or PPs ofmice treated with WBH (39.5±0.5°C for 6 h) demonstratedimproved ability of HEVs to support lymphocyte adhesioncompared to normothermic controls. Importantly, increasedadhesion was only noted in the plump, near-cuboidal,
Fig. 1 Effects of fever-range hyperthermia on lymphocyte-endothelialadhesion. A, Hyperthermia increases the affinity of L-selectinexpressed on lymphocytes, allowing for greater interaction with PNAdand improved tethering/rolling. B, Hyperthermia increases the displayof CCL21 on the HEV lumenal surface to augment activation oflymphocytes via CCR7 for eventual arrest. C, ICAM-1 expression onHEVs is upregulated by hyperthermia to promote firm adhesion andsubsequent extravasation of LFA-1-expressing lymphocytes
J Mol Med (2007) 85:1361–1367 1363

differentiated HEVs of LNs and PPs but not in thesquamous endothelium of nonlymphoid tissues [26]. Invivo homing studies also demonstrated a twofold increasein trafficking of normothermic lymphocytes to PLNs, PPs,and MLNs in mice receiving WBH. Paralleling the resultsof frozen section adherence assays, heat effects on homingwere site specific, supported by the lack of an increase inhoming to sites with normal squamous endothelial vascu-lature such as the liver or pancreas [25, 26, 32].
To further pinpoint the specific adhesive mechanismsthat occur in cells lining HEVs, intravital microscopystudies were performed. Interactions between fluorescent-tagged lymphocytes and vascular substrates in PLNs ofliving mice demonstrated a functional dichotomy betweenthe effects of thermal stress on higher-order HEVs andlower-order venules [25]. Although the rolling interactionsdid not manifest any change, the number of lymphocytesachieving firm arrest increased with WBH and wasrestricted to the higher-order HEVs [25]. Lymphocyteaggregates were not detected in vivo, consistent with priorobservations that heat treatment alone does not inducehomotypic adhesion in lymphocytes in vitro [31]. Tominimize the known nonspecific effects of thermal stresson hemodynamic parameters such as vasodilatation andincreased blood flow [25, 26, 32], which could have animpact on lymphocyte–endothelial interactions during theobservation period, heated mice were allowed to revert tonormothermal core temperature before adoptive transfer offluorescent-labeled lymphocytes. Given that the velocityof noninteracting lymphocytes passing through thevenular tree was similar between normothermic andhyperthermia-pretreated groups, improved lymphocyte–endothelial interactions were likely due to molecularchanges in the endothelium and not from nonspecifichemodynamic thermal effects [25]. Taken together, evi-dence that a greater number of lymphocytes can recirculatethrough lymphoid organs over a given period of time withhyperthermia suggests that increased temperatures associ-ated with fever directly benefit the process of primaryimmune surveillance.
A large range of molecules involved in the multisteptrafficking cascade was evaluated to determine the causa-tive agents of improved adhesion in HEVs [25]. Intravas-cular staining demonstrated ICAM-1 and CCL21 as theonly components found to be substantially increased interms of HEV lumenal expression. This increased expres-sion could be quantified by image analysis of immunoflu-orescence, which indicated a ∼2- and ∼1.5-fold increaseover baseline immunofluorescence staining for ICAM-1(Fig. 2) and CCL21, respectively, on near-cuboidal HEVsof PLNs and PPs [25]. In contrast, intravascular staining forother endothelial molecules such as ICAM-2 did notincrease with heat arguing against a non-specific hemody-
namic effect on antibody delivery during staining proce-dures. Consistent with observations in homing assays andintravital microscopy studies, increased ICAM-1 andCCL21 staining was noted only in HEVs during WBHand not in normal squamous vascular endothelium ofextralymphoid organs [25]. Upregulated CCL21 expressionduring WBH is functionally relevant to the improvedtrafficking of lymphocytes, as homing was abrogated bytreating lymphocytes with pertussis toxin, a generalinhibitor of chemokine receptor function [25]. Desensitiza-tion of CCR7 by ex vivo exposure of lymphocytes to highconcentrations of CCL21 before adoptive transfer as well asin vivo antibody blockade of CCL21 similarly abolishedthe improved homing associated with WBH. Heat-inducibleICAM-1 was also demonstrated to be crucial for theobserved increases in lymphocyte homing to lymph nodes[25] through the use of either ICAM-1 knockout mice orblocking antibodies to ICAM-1 in vivo.
Fever-range hyperthermia can be viewed as influencinglymphocytes early in the adhesion cascade (tethering/rolling) as well as the endothelium in later steps (chemo-kine activation, firm adhesion, and transendothelial migra-tion; Fig. 1). These mechanisms substantially increase theprobability of antigen-specific T cells encountering theappropriate antigen-presenting cell in lymphoid organs. In asystem where approximately one in four lymphocytesextravasate after entering HEVs under steady-state con-
Fig. 2 Fever-range hyperthermia enhances the intravascular expres-sion of ICAM-1 on PNAd+ HEVs in peripheral lymph nodes.Intravascular ICAM-1 was detected by intravenous injection ofICAM-1-specific primary antibody followed by immunofluorescencestaining. Peripheral lymph node cryosections were counterstained withMECA-79 antibody to demark the position of PNAd+ near-cuboidalHEVs. The intravascular density of ICAM-1 was substantiallyupregulated in HEVs of mice receiving whole-body hyperthermia(WBH) compared to normothermal (NT) controls. PNAd expressionwas not affected by exposure to WBH
1364 J Mol Med (2007) 85:1361–1367

ditions [14], the approximately twofold increase observedwith fever-range thermal stress represents a profoundenhancement of primary immune surveillance. An interest-ing question that remains to be addressed is whether fever-range temperatures also increase the rate of transit oflymphocytes out of the lymph nodes via the efferentlymphatics [14].
Elucidation of an IL-6 trans-signaling mechanism
The mediator of thermal effects upon lymphocytes andHEVs was revealed in a series of complementary experi-ments. In vitro studies involving thermally treated lympho-cytes implied that the hypothalamic responses associatedwith fever were not necessary for the changes seen withhyperthermia [26, 29, 30, 33]. While thermal effects onlymphocyte adhesion were shown to be mediated bysoluble factors in conditioned medium, no increase inconcentrations of fever-associated cytokines such as inter-leukin (IL) 1α, IL-1β, IL-6, IL-8, or tumor necrosis factor(TNF) were detectable. Additionally, IL-2, IL-3, IL-4, IL-10, IL-11, IL-12, IL-13, IL-15, interferon (IFN) γ, leukemiainhibitory factor, granulocyte monocyte colony-stimulatingfactor, transforming growth factor 1, and Flt3 wereundetectable in this culture medium. These data suggestedthat thermal stress likely improves the bioactivity of solublefactors locally and not their overall concentrations. Todetermine the relevant cytokines, antibody blockade experi-ments against IL-8, IFNα, IFNγ, TNF, IL-1β, and IL-6were performed. Only blockade of IL-6 was capable ofneutralizing the effects of thermal stress on adhesion inlymphocytes treated either in vitro or in vivo [33].
IL-6 signaling can be triggered by two separate path-ways [34]. In classical signaling, IL-6 influences cellularresponses by binding to a specific IL-6 cell surface receptorsubunit (IL-6Rα). In turn, the IL-6Rα/IL-6 complexinitiates homodimerization of gp130, an associated mole-cule of the IL-6 cell surface receptor. The gp130 complex isthen capable of transducing the original IL-6 signalintracellularly [35]. An alternate signaling pathway forIL-6 utilizes a soluble form of the IL-6 receptor (sIL-6Rα).When bound to IL-6, the sIL-6Rα can act to dimerizemembrane-anchored gp130 leading to signal transduction.It is interesting to note that cells that do not express themembrane form of the IL-6Rα but express gp130 arerendered responsive to the IL-6/sIL-6Rα complex. Thismode of action has been termed IL-6 trans-signaling [35].Accordingly, soluble forms of gp130 are capable ofcompetitively inhibiting IL-6 trans-signaling by binding tosIL-6Rα/IL-6 complexes, thereby eliminating their inter-action with membrane-bound gp130 [35].
In the models of hyperthermia-treated lymphocytes, theaddition of antibodies against IL-6, the IL-6 receptor(which can recognize membrane or soluble forms), orgp130 similarly inhibited the increased adhesion associatedwith heat [33]. Moreover, blockade of IL-6 trans-signalingby the receptor antagonist, recombinant soluble gp130,prevented augmented heat-induced adhesion both in vitroand in vivo [33]. The role of IL-6 trans-signaling as themediator of hyperthermia-induced lymphocyte changes wassupported by the ability of recombinant soluble gp130 toinhibit the proadhesive effects of exogenously added IL-6to lymphocyte cultures. Additionally, the level of mem-brane bound IL-6Rα expression on treated lymphocyteswas not detectable by flow cytometry [33]. Collectively,these lines of investigation support an IL-6 trans-signalingmechanism as being the prime mediator of enhancedlymphocyte adhesion during thermal stress.
Remarkably, a nonredundant requirement for IL-6 trans-signaling was also demonstrated for the thermal inductionof ICAM-1 on HEVs. By utilizing IL-6 knockout mice oradministering IL-6 blocking antibody before WBH treat-ment of wild-type mice, the typical upregulation of ICAM-1 expression on HEVs was eliminated [25]. To define theIL-6 pathway involved, recombinant soluble gp130 wasinjected into mice before WBH to selectively block IL-6trans-signaling but not the classical pathway [25]. Thistreatment prevented ICAM-1 upregulation during WBHsuggesting that IL-6 trans-signaling was the commonmediator of thermal effects seen on both HEVs andlymphocytes. The increased expression of CCL21 seenwith WBH, however, was not associated with an IL-6-dependent pathway and remains to be elucidated [25].
Clinical implications of thermal therapy dynamics
The ability of fever-range WBH to selectively alter theadhesive properties of lymphocytes and endothelium hasseveral potential clinical implications. The thermal compo-nent of fever appears beneficial to primary immunesurveillance and may be hampered by the use of antipy-retics. Subsequently, the judicious use of antipyretics isincreasingly advocated [36]. Furthermore, the circulation oflymphocytes through lymph nodes is not only importantduring infection but may also be necessary for immuneresponses to cancer [37, 38]. Improved lymphocyterecirculation across HEVs by WBH treatment of cancerpatients may allow for a more potent antitumor immuneresponse based upon recent recognition that lymphoid organsare key sites for promoting antitumor immunity [39].
Another critical site of lymphocyte entry for elaborationof antitumor immunity is within the tumor microenviron-ment itself [40, 41]. Tumor microvasculature in patient and
J Mol Med (2007) 85:1361–1367 1365

murine models is associated with low basal levels ofICAM-1 expression, which may explain poor T cellinfiltration in tumor tissues [32, 40, 42]. Recent studieshave identified endogenous IL-6 and the soluble IL-6receptor in local tumor microenvironments that wereresponsible for promoting tumor growth [43]. Paradoxical-ly, IL-6 trans-signaling present in the tumor microenviron-ment may also be an attractive therapeutic target duringsystemic thermal therapy to inhibit tumor growth throughimmune-mediated mechanisms. It remains to be determinedif hyperthermia can exploit IL-6 and the soluble IL-6receptor in the tumor microenvironment to improvevascular adhesion similar to that observed in HEVs. Inaddition to changes in tumor blood flow and oxygenationassociated with hyperthermia [44], improved vascularadhesion may theoretically enhance T lymphocyte infiltra-tion into tumor sites, as has been reported for natural killerlymphocytes [22]. T lymphocyte infiltration is critical toantitumor responses and improved patient survival [45–47].Although local hyperthermia in combination with otherlocal intratumoral therapies such as vaccination, ablation, orradiation have potential efficacy by improving lymphocyteinfiltration [48–50], the role of WBH alone as a modifier ofthe tumor microenvironment has not been established in thecontext of improving vascular adhesion. The limitedtoxicity of WBH in humans has already been borne out ininitial clinical trials [27]. The ability to actively increase thedelivery of tumor-reactive lymphocytes to the tumormicroenvironment in immunotherapy protocols representsa current area of active investigation.
A working knowledge of the molecular mechanismsassociated with the dynamic changes seen in lymphocytetrafficking during WBH may also benefit the currentunderstanding of several inflammatory disease models.For example, lymphocyte recruitment to areas of inflam-mation has been linked to an IL-6 trans-signaling mecha-nism in autoimmune states such as rheumatoid arthritis andinflammatory bowel disease [34]. It is believed that IL-6trans-signaling also triggers the transition from innateimmunity to acquired immunity by selectively regulatingchemokine and adhesion molecule-dependent recruitmentof leukocyte subsets to inflamed tissues [51]. Thus,perturbations of this system may be responsible for themaintenance of a chronic inflammatory disease state [51].Accordingly, directed and specific therapies such as IL-6blocking antibodies and exogenous soluble gp130 arebeing evaluated for clinical use in chronic inflammatorydisorders [52, 53].
Acknowledgments We thank Heinz Baumann and ElizabethRepasky for long-standing contributions to this work and MichelleAppenheimer, Daniel Fisher, Jason Muhitch, Trupti Vardam, and LeiZhou for critical review of the manuscript.
References
1. Paul WE (1999) Fundamental immunology. Lippincott-Raven,Philadelphia
2. Kluger MJ (1991) Fever: role of pyrogens and cryogens. PhysiolRev 71:93–127
3. Mackowiak PA (1994) Fever: blessing or curse? A unifyinghypothesis. Ann Intern Med 120:1037–1040
4. Mackowiak PA (2000) Physiological rationale for suppression offever. Clin Infect Dis 31(Suppl 5):S185–189
5. Covert JB, Reynolds WW (1977) Survival value of fever in fish.Nature 267:43–45
6. Bernheim HA, Kluger MJ (1976) Fever: effect of drug-inducedantipyresis on survival. Science (New York, NY) 193:237–239
7. Hasday JD, Fairchild KD, Shanholtz C (2000) The role of fever inthe infected host. Microbes Infect 2:1891–1904
8. Kluger MJ, Kozak W, Conn CA et al (1996) The adaptive value offever. Infect Dis Clin North Am 10:1–20
9. Manthous CA, Hall JB, Olson D et al (1995) Effect of cooling onoxygen consumption in febrile critically ill patients. Am J RespirCrit Care Med 151:10–14
10. Schumacker PT, Rowland J, Saltz S et al (1987) Effects ofhyperthermia and hypothermia on oxygen extraction by tissuesduring hypovolemia. J Appl Physiol 63:1246–1252
11. Schumacker PT, Rowland J, Saltz S et al (2001) Glossary of termsfor thermal physiology Third Edition revised by The Commissionfor Thermal Physiology of the International Union of PhysiologicalSciences (IUPS Thermal Commission). Jpn J Physiol 51:245–280
12. Pritchard MT, Ostberg JR, Evans SS et al (2004) Protocols forsimulating the thermal component of fever: preclinical and clinicalexperience. Methods (San Diego, Calif) 32:54–62
13. Kupper TS, Fuhlbrigge RC (2004) Immune surveillance in theskin: mechanisms and clinical consequences. Nat Rev 4:211–222
14. von Andrian UH, Mempel TR (2003) Homing and cellular trafficin lymph nodes. Nat Rev 3:867–878
15. Butcher EC, Picker LJ (1996) Lymphocyte homing and homeo-stasis. Science (New York, NY) 272:60–66
16. Rosen SD (2004) Ligands for L-selectin: homing, inflammation,and beyond. Ann Rev Immunol 22:129–156
17. Ebert LM, Schaerli P, Moser B (2005) Chemokine-mediatedcontrol of T cell traffic in lymphoid and peripheral tissues. MolImmunol 42:799–809
18. Gunn MD, Tangemann K, Tam C et al (1998) A chemokineexpressed in lymphoid high endothelial venules promotes theadhesion and chemotaxis of naive T lymphocytes. Proc Natl AcadSci USA 95:258–263
19. Stein JV, Rot A, Luo Y et al (2000) The CC chemokine thymus-derived chemotactic agent 4 (TCA-4, secondary lymphoid tissuechemokine, 6Ckine, exodus-2) triggers lymphocyte function-associated antigen 1-mediated arrest of rolling T lymphocytes inperipheral lymph node high endothelial venules. J Exp Med191:61–76
20. Carman CV, Springer TA (2004) A transmigratory cup inleukocyte diapedesis both through individual vascular endothelialcells and between them. J Cell Biol 167:377–388
21. Ostberg JR, Gellin C, Patel R et al (2001) Regulatory potential offever-range whole body hyperthermia on Langerhans cells andlymphocytes in an antigen-dependent cellular immune response. JImmunol 167:2666–2670
22. Burd R, Dziedzic TS, Xu Y et al (1998) Tumor cell apoptosis,lymphocyte recruitment and tumor vascular changes are inducedby low temperature, long duration (fever-like) whole bodyhyperthermia. J Cell Physiol 177:137–147
23. Roberts NJ Jr (1991) Impact of temperature elevation onimmunologic defenses. Rev Infect Dis 13:462–472
1366 J Mol Med (2007) 85:1361–1367

24. Ostberg JR, Repasky EA (2006) Emerging evidence indicates thatphysiologically relevant thermal stress regulates dendritic cellfunction. Cancer Immunol Immunother 55:292–298
25. Chen Q, Fisher DT, Clancy KA et al (2006) Fever-range thermalstress promotes lymphocyte trafficking across high endothelialvenules via an interleukin 6 trans-signaling mechanism. NatImmunol 7:1299–1308
26. Evans SS, Wang WC, Bain MD et al (2001) Fever-rangehyperthermia dynamically regulates lymphocyte delivery to highendothelial venules. Blood 97:2727–2733
27. Kraybill WG, Olenki T, Evans SS et al (2002) A phase I study offever-range whole body hyperthermia (FR-WBH) in patients withadvanced solid tumours: correlation with mouse models. Int JHypertherm 18:253–266
28. Stamper HB Jr, Woodruff JJ (1976) Lymphocyte homing intolymph nodes: in vitro demonstration of the selective affinity ofrecirculating lymphocytes for high-endothelial venules. J ExpMed 144:828–833
29. Wang WC, Goldman LM, Schleider DM et al (1998) Fever-rangehyperthermia enhances L-selectin-dependent adhesion of lympho-cytes to vascular endothelium. J Immunol 160:961–969
30. Evans SS, Schleider DM, Bowman LA et al (1999) Dynamicassociation of L-selectin with the lymphocyte cytoskeletal matrix.J Immunol 162:3615–3624
31. Evans SS, Bain MD, Wang WC (2000) Fever-range hyperthermiastimulates alpha4beta7 integrin-dependent lymphocyte-endothelialadhesion. Int J Hypertherm 16:45–59
32. Chen Q, Fisher DT, Kucinska SA et al (2006) Dynamic control oflymphocyte trafficking by fever-range thermal stress. CancerImmunol Immunother 55:299–311
33. Chen Q, Wang WC, Bruce R et al (2004) Central role of IL-6receptor signal-transducing chain gp130 in activation of L-selectinadhesion by fever-range thermal stress. Immunity 20:59–70
34. Jones SA, Horiuchi S, Topley N et al (2001) The solubleinterleukin 6 receptor: mechanisms of production and implicationsin disease. FASEB J 15:43–58
35. Jostock T, Mullberg J, Ozbek S et al (2001) Soluble gp130 is thenatural inhibitor of soluble interleukin-6 receptor transsignalingresponses. Eur J Biochem 268:160–167
36. Plaisance KI, Mackowiak PA (2000) Antipyretic therapy: physi-ologic rationale, diagnostic implications, and clinical consequen-ces. Arch Intern Med 160:449–456
37. Bai XF, Gao JX, Liu J et al (2001) On the site and mode of antigenpresentation for the initiation of clonal expansion of CD8 T cellsspecific for a natural tumor antigen. Cancer Res 61:6860–6867
38. van Mierlo GJ, Boonman ZF, Dumortier HM et al (2004)Activation of dendritic cells that cross-present tumor-derivedantigen licenses CD8+ CTL to cause tumor eradication. JImmunol 173:6753–6759
39. Gattinoni L, Klebanoff CA, Palmer DC et al (2005) Acquisition offull effector function in vitro paradoxically impairs the in vivo
antitumor efficacy of adoptively transferred CD8+ T cells. JClinical invest 115:1616–1626
40. Ganss R, Arnold B, Hammerling GJ (2004) Mini-review:overcoming tumor-intrinsic resistance to immune effector func-tion. Eur J Immunol 34:2635–2641
41. Skitzki J, Craig RA, Okuyama R et al (2004) Donor cell cycling,trafficking, and accumulation during adoptive immunotherapy formurine lung metastases. Cancer Res 64:2183–2191
42. Chen Q, Wang WC, Evans SS (2003) Tumor microvasculature asa barrier to antitumor immunity. Cancer Immunol Immunother52:670–679
43. Rose-John S, Scheller J, Elson G et al (2006) Interleukin-6biology is coordinated by membrane-bound and soluble receptors:role in inflammation and cancer. J Leukoc Biol 80:227–236
44. Song CW, Park HJ, Lee CK et al (2005) Implications ofincreased tumor blood flow and oxygenation caused by mildtemperature hyperthermia in tumor treatment. Int J Hypertherm21:761–767
45. thor Straten P, Becker JC, Guldberg P et al (1999) In situ T cells inmelanoma. Cancer Immunol Immunother 48:386–395
46. Hiraoka K, Miyamoto M, Cho Y et al (2006) Concurrentinfiltration by CD8+ T cells and CD4+ T cells is a favourableprognostic factor in non-small-cell lung carcinoma. Br J Cancer94:275–280
47. Galon J, Costes A, Sanchez-Cabo F et al (2006) Type, density, andlocation of immune cells within human colorectal tumors predictclinical outcome. Science (New York, NY) 313:1960–1964
48. Guo J, Zhu J, Sheng X et al (2007) Intratumoral injection ofdendritic cells in combination with local hyperthermia inducessystemic antitumor effect in patients with advanced melanoma. IntJ Cancer 120:2418–2425
49. Morita M, Kuwano H, Araki K et al (2001) Prognosticsignificance of lymphocyte infiltration following preoperativechemoradiotherapy and hyperthermia for esophageal cancer. Int JRadiat Oncol Biol Phys 49:1259–1266
50. Nakayama J, Kokuba H, Kobayashi J et al (1997) Experimentalapproaches for the treatment of murine B16 melanomas of varioussizes. I: Local injection of ethanol with a combination ofinterleukin-2 or microwaval hyperthermia for B16 melanomaswith a size of less than 7 mm in diameter. J Dermatol Sci 15:75–81
51. Jones SA (2005) Directing transition from innate to acquiredimmunity: defining a role for IL-6. J Immunol 175:3463–3468
52. Paul-Pletzer K (2006) Tocilizumab: blockade of interleukin-6signaling pathway as a therapeutic strategy for inflammatorydisorders. Drugs Today (Barc) 42:559–576
53. Nowell MA, Richards PJ, Horiuchi S et al (2003) Soluble IL-6receptor governs IL-6 activity in experimental arthritis: blockadeof arthritis severity by soluble glycoprotein 130. J Immunol171:3202–3209
J Mol Med (2007) 85:1361–1367 1367

ORIGINAL ARTICLE
Neuronal plasticity of the “brain–skin connection”:stress-triggered up-regulation of neuropeptides in dorsal rootganglia and skin via nerve growth factor-dependent pathways
Ricarda A. Joachim & Arne Kuhlmei & Q. Thai Dinh &
Bori Handjiski & Tanja Fischer & Eva M. J. Peters &
Burghard F. Klapp & Ralf Paus & Petra C. Arck
Received: 7 February 2007 /Revised: 30 April 2007 /Accepted: 29 May 2007 / Published online: 17 July 2007# Springer-Verlag 2007
Abstract Emerging research indicates that central-nervousstress perception is translated to peripheral tissues such asthe skin not only via classical stress hormones but also vianeurotrophins and neuropeptides. This can result in neuro-genic inflammation, which is likely to contribute to thetriggering and/aggravation of immunodermatoses. Al-though the existence of such a “brain–skin connection” issupported by steadily increasing experimental evidence, itremains unclear to which extent perceived stress affects thesensory “hardwiring” between skin and its afferent neuronsin the corresponding dorsal root ganglia (DRG). In thispaper, we provide experimental evidence in a murine modelof stress (exposure of C57BL/6 mice to sound stress) thatstress exposure, or intracutaneous injection of recombinantnerve growth factor (NGF) to mimic the skin’s response tostress, up-regulate the percentage of substance P (SP)+ orcalcitonin gene-related peptide (CGRP)+ sensory neurons in
skin-innervating DRG. Further, we show that the number ofSP+ or CGRP+ sensory nerve fibers in the dermis ofstressed C57BL/6 mice is significantly increased. Finally,we document that neutralization of NGF activity abrogates
J Mol Med (2007) 85:1369–1378DOI 10.1007/s00109-007-0236-8
R. A. Joachim :Q. T. Dinh :B. Handjiski : T. Fischer :E. M. J. Peters :B. F. Klapp : P. C. ArckCenter of Internal Medicine and Dermatology,Charité, University Medicine Berlin, Campus Virchow,Berlin, Germany
A. KuhlmeiUniversity of Ulm,Ulm, Germany
R. PausDepartment of Dermatology, University of Schleswig Hostein,University of Luebeck,Lübeck, Germany
P. C. Arck (*)Universitätsmedizin Berlin, Biomedizinisches Forschungszentrum,R. 2.0549, Augustenburger Platz 1,13353 Berlin, Germanye-mail: [email protected]
RICARDA JOACHIMreceived her medical training atthe University of Berlin,Germany and the CatholicUniversity of Córdoba,Argentina. She continued herpostgraduate training at thepsycho-neuro-immunologicalresearch laboratory at theCharité, Universitaetsmedizin,Berlin, where she now leads aresearch group. Her researchinterests include the neuroim-munological interaction inhealth and disease, focusing onbronchial asthma.
PETRA ARCK
began to develop her scientificinterest on the effects of stresson the neuroimmunoligicalhemostasis in health and diseasewhile receiving her medicaltraining at the University ofTuebingen, Germany. Afterpostdoctoral fellowships at theMcMaster University inHamilton and the University ofToronto, Canada, she is nowhead of the psycho-neuro-immunological researchlab at the Charité, UniversityMedicine Berlin. Further, she isan international associate of theBrain Body Institute in Hamilton,Canada.

stress-induced effects on the percentage of SP+ and CGRP+
sensory neurons in skin-innervating DRG as well as ondermal sensory nerve fibers. These data suggest that highstress perception results in an intense cross talk between theskin and skin-innervating DRG, which increases thelikelihood of NGF-dependent neurogenic skin inflamma-tion by enhancing sensory skin innervation.
Keywords Brain–skin connection . Dorsal root ganglia .
Nerve growth factor-dependent pathways . Stress .
Atopic dermatitis . Hair loss
Introduction
Emerging research indicates that the central stressperception is translated to the body via stress mediatorssuch as neurotrophins and neuropeptides—besides thetraditional notion of a stress-triggered activation of thehypothalamic pituitary adrenal (HPA) axis. In general,such stress-response pathways may be considered as aphysiological process of adaptation to the demands of theenvironment; however, an exceeding stress response hasbeen shown to aggravate or trigger chronic diseases inselected individuals, such as exacerbations of inflamma-tory bowel disease, atopic diseases, or pregnancy compli-cations [1–5]. High perception of stress influences skinimmune homeostasis and may contribute to trigger and/oraggravate immune dermatoses such as atopic dermatitis,psoriasis, alopecia areata (AA), or chronic urticaria [6–8].Further, stress perception has been suggested as a cause oraggravating factor of telogen effluvium [9, 10].
Based on published evidence indicating a link betweenstress perception and skin diseases [6, 7], we previouslypostulated the existence of the “brain–skin connection”through which the central stress response and peripheralmediators of stress response execution challenge the skin’scell homeostasis and neuro-endocrine-immune equilibrium[11]. The stress-induced increased expression of substanceP (SP) in skin nerve fibers and of cutaneous nerve growthfactor (NGF) consequently lead to the development of neu-rogenic skin inflammation, recognized by its classicalfeatures of mast cell degranulation, vasodilatation, andplasma extravasation [12, 13]. Both SP and NGF are nowwidely acknowledged as cardinal immunomodulators andprevailing stress markers in different settings [4, 14–16].NGF, an essential trophic factor for axon sprouting ofpeptidergic and sympathetic neurons, promotes cross-talkbetween neuronal cells, glia, and immune cells and facil-itates monocyte/macrophage migration through vascularendothelium [17]. During inflammation, NGF is markedlyup-regulated in nerves associated with the inflamed area
[18], and NGF levels are increased in inflammatory skindiseases such as psoriasis [19].
Today, established mouse models are on hand to investi-gate stress effects on skin diseases. Sound stress, which iswidely used in neuro-endocrine-immunological research [3,5, 20, 21], has been demonstrated to induce neurogenic skininflammation in mice [4, 22] and the premature terminationof murine hair growth [2, 4]. Blockade of the neurokinin-1receptor [2], for which SP has the highest affinity, as well asneutralization of NGF abrogate stress-induced neurogenicinflammation [4]. Interestingly, Aoki and Kawana [23], whoemployed a mouse model of intermittent foot shock stress,independently supported the existence of a stress-associatedbrain–skin connection by observing a retardation of hairfollicle cycling in stressed mice.
In the skin, sensory nerves derive from the dorsal rootganglion (DRG) and represent the initial somatic portion ofthe afferent sensory pathway. This cutaneous sensorynervous system comprises a network of fine C-fibers whichinnervate multiple target structures and play an essentialrole in inflammation. SP is synthesized in DRG andtransported to the terminals of C-fibers located in thedorsal horn of the spinal cord and in the skin [24], where itcan be released from sensory nerve fiber endings, e.g., inresponse to NGF [25]. In-depth analysis of the intricate skininnervation further revealed that—besides SP—the neuro-peptide calcitonin gene-related peptide (CGRP) is localizedin primary afferent sensory neurons in bundles as well assingle nerve fibers, with distinct distribution patterns andmajor hair-cycle-associated changes [26, 27]. In theepidermis and around the distal hair follicle and the arrectorpili muscle, CGRP+ nerve fibers can be detected, whereasSP+ nerve fibers are largely restricted to the dermis andsubcutis. Compared to telogen skin, the number of CGRP+
and SP+ single nerve fibers is increased during anagen inskin regions such as the bulge region [27], where theepithelial stem cells of the hair follicle are located. CGRP isa potent vasodilator, mediates weal and flare reaction, andhence contributes to the perpetuation of neurogenicinflammation [28]. Like SP, CGRP can be released inresponse to peripheral stimuli or by inflammatory mediatorslike interleukin (IL)-1 or prostaglandins [12]. Peptidergiccutaneous innervation, which is subject to lifelong plastic-ity, is altered in response to stress, as reflected by an in-creased number of SP+ nerve fibers and an increasedexpression of NGF [2, 22]. However, to date, no insightsare available on cutaneous CGRP expression in response tostress. Further, it remains to be elucidated whether or notNGF-dependent skin inflammation orchestrates neuropep-tide expression in DRG and if stress-triggered plasticity ofSP+ and CGRP+ DRG neurons and skin nerve fibers islargely dependent on NGF.
1370 J Mol Med (2007) 85:1369–1378

By employing the technique of retrograde tracing [29],skin-innervating neurons in cervical and thoracic DRG canbe identified and allow their phenotypic evaluation. Thismethod, fundamental to map connectivity in the nervoussystem, may provide insights if and how stress-induced andNGF-dependent skin inflammation orchestrates neuropep-tide expression in DRG by altering the relative expressionof neuropeptides among traced neurons.
Thus, in the present study, we aimed to investigate
1. whether stress exposure or subcutaneous (s.c.) injectionof recombinant NGF (to mimic stress in the absence ofsonic stress) affects the percentage of SP+ and/orCGRP+ sensory neurons in skin-innervating thoracicand cervical DRG in mice.
2. whether an increase in intracutaneous NGF (either as askin response to stress or as a result of s.c. NGFinjection) alters the number of immunohistochemicallydetectable SP+ and/or CGRP+ sensory nerve fibers inthe dermis.
3. whether neutralization of NGF mitigates or abro-gates stress-induced effects on the percentage of SP+
or CGRP+ sensory neurons in skin-innervating DRGand/or on SP+ /CGRP+ sensory dermal nerve fibers.
Materials and methods
Animals
Six- to 8-week-old female C57BL/6 mice were purchasedfrom Charles River (Sulzfeld, Germany) as mice at this ageshow the most reliable and profound stress response and arein the telogen stage of the hair cycle. The animals werehoused in community cages with 12-h light periods andwere fed water and mouse chow ad libitum. Animal careand experimental procedures were followed according toguidelines of the respective institutions and conformed tothe requirements of the state authority for animal researchconduct.
Anagen induction
Anagen was experimentally induced by depilation, aspreviously published [30]. Briefly, mice were anesthetizedwith intramuscular injection of ketamine hydrochloride(Ketanest, Parke-Davis, Freiburg, Germany, 10 mg/kg bodyweight) and xylazine hydrochloride (Rompun, Bayer,Leverkusen, Germany, 10 mg/kg). Then, a wax/rosin mix-ture was applied to the dorsal skin of mice with all hairfollicles in telogen, as evidenced by the pink back skincolor. Peeling off the wax/rosin mixture removes all hair
shafts and immediately induces a highly synchronized hairgrowth.
Retrograde Tracing of DRG
Mice were anesthetized 9 days post-depilation (p.d.), and aFluoroGold-like tracer (hydroxystilbamidine; Biotium) wasapplied in five s.c. injections with a total volume of 20 μl ata concentration of 1.25% (100 mg/800 μl distilled H2O) inthe dorsal skin tissue right below the scapula, covering atotal tissue area of about 1 cm2. All animals recoveredundisturbed for a postoperative period of 5 days, until day14 p.d. [4].
Application of stress
For each experimental setting, a group of C57BL/6 mice(n=4) was exposed to sonic stress for the duration of 24 hstarting on day 14 p.d., when all back skin hair follicleswere in late anagen. The time point of stress application inthe model of induced anagen was chosen based on earlierexperiments, where stress effects on hair cycle andneurogenic inflammation in the skin were examined [2,4]. In this paper, we aimed to extend the knowledge aboutstress effects to the level of skin-innervating neurons andinfluence on neuronal and peripheral CGRP expression.The sonic stress was emitted by a rodent repellent device(Conrad Electronics, Berlin, Germany) at a frequency of300 Hertz in intervals of 15 s. The stress device was placedinto the mouse cage so that the mice could not escapesound perception.
Application of NGF
A subgroup of nonstressed mice (n=4) was injectedsubcutaneously on day 14 in the dorsal skin with murineNGF (7S; Roche, Mannheim, Germany) with 10 μl/mouseat a concentration of 100 μg/ml phosphate-buffered saline(PBS). The NGF concentration has been selected consider-ing a publication with local NGF application to murineairways [31]. We included this subcutaneous application ofNGF to mimic stress-triggered increase in skin NGF.Another subgroup of mice was injected with PBS aloneand served as a nonstressed control (n=4).
Application of anti-NGF
Intraperitoneal application of 200 μl polyclonal rabbitantimouse NGF antibody (Sigma-Aldrich, Munich, Ger-many) at a dilution of 1:1,500 in PBS was performed in tworespective groups of nonstressed control (n=4) or stressedmice (n=4) on days 14 and 15 p.d. According to the
J Mol Med (2007) 85:1369–1378 1371

manufacturer, a 1:4,000 dilution of this antibody blocksbioactivity of 5 ng/ml NGF.
Tissue preparation
On day 16 p.d., at the time when control mice are just aboutto spontaneously enter the anagen/catagen transformation oftheir depilation-induced hair cycle [32], all mice were killed.The animals were perfusion-fixed retrogradely through theleft ventricle with freshly prepared Zamboni’s solution (2%paraformaldehyde, 15% picrinic acid, 0.1 mol/l PBS,pH 7.4) for 5 min. Dissection of the Zamboni-fixed cervicaland thoracic DRG (C4 to Th10) was performed by rinses in0.1 mol/l phosphate buffer (pH 7.4) and cryoprotection with18% sucrose in 0.1 mol/l phosphate buffer overnight. Onaverage, 30 DRGs were harvested per mouse and screenedfor traced neurons by preparing cryosections of each DRG.Traced DRG could predominantly be identified from C5 toTh3, thus, on average, 14 traced DRG/mouse wereavailable for the preparation of serial sections, andapproximately 40 consecutive slides were cut per DRG.
Skin specimens from the neck region of the murine backwere harvested parallel to the vertebral line, snap-frozen inliquid nitrogen, and then covered with embeddingmedium, asdescribed in detail in by Müller-Röver et al. [30]. Cryosec-tions were then processed for immunohistochemistry.
Fluorescence immunohistochemistry of SP and CGRPin ganglia and skin tissue
Ganglion (7 μm) and skin (14 μm) sections were air driedfor 30 min and incubated overnight with the correspond-ing primary antibody at a dilution of 1:400 with a mono-clonal rat antimouse SP antibody (Chemicon) and at adilution of 1:200 with monoclonal rabbit antimouse CGRPantibody (Chemicon). Several washing steps were fol-lowed by an incubation of 1 h at 37°C with rhodamine-conjugated F(ab)2 fragments of goat antimouse IgG orgoat antirabbit IgG (Jackson ImmunoResearch), respec-tively, at a Tris-buffered saline (TBS) dilution of 1:200 in2% mouse normal serum. All sections were mounted andstored at −20°C until further analysis.
Quantitative histomorphometry and statistical analysis
A fluorescence microscope (Axioplan; Zeiss, Jena,Germany) with appropriate excitation emission filtersystem for fluorescence induced by rhodamine was usedto analyze fluorescence immunohistochemistry (FIH)-labeled sections. FluoroGold-positive neurons were iden-tified through a wide-band UV filter. To avoid doublecounting of neurons, only neurons with an apparent
nucleus were counted. Expression of neuropeptides inganglion sections is indicated as percentage of retrogradetraced neurons. Analysis and photo documentation wasperformed by a digital image analysis system (Spotadvanced software, version 3.5.2; Visitron Systems;Puchheim, Germany). Quantification of single dermalnerve fibers was performed by histomorphometry as pre-viously described [33]. From each mouse, two to fourdifferent sections were used to analyze at least ten adjacentmicroscopic fields. This number was raised up to 100 mi-croscopic fields per mouse if there were microscopic fieldswith no positive nerve-fiber profiles detectable. The datawere pooled per mouse and the mean and standard errorcalculated per group. Nonparametric tests were used becauseof nonnormal distribution of the results (Kolmogorov–Smirnov). Significance of differences between groups wasdetermined using the nonparametric Kruskal–Wallis testfollowed by the Mann–Whitney U test to compare twogroups. Differences were judged as significant if the p valuewas <0.05.
Results
Stress and cutaneous injection of NGF up-regulatethe percentage of SP+ and CGRP+ sensory neuronsin skin-innervating DRG
The percentage of SP+ and CGRP+ sensory neurons in skin-innervating DRG was determined among the total numberof neurons which could be traced by retrograde labeling. Asalready shown in pilot experiments in one of our earlierpublications [4], the percentage of SP+ sensory neurons inskin-innervating DRG was significantly increased in ani-mals exposed to sonic stress compared to nonstressedcontrol animals (p<0.05; Fig. 1a; representative photo-graphs are shown in Fig. 2a–d). S.c. injection of recombi-nant murine NGF in the dorsal skin mimicked the effect ofstress on neuronal plasticity in DRG, as the percentage ofSP+ sensory neurons in skin-innervating DRG was signif-icantly increased in these animals compared to nonstressedcontrol animals (p<0.05; Fig. 1a).
Similar results were obtained with respect to CGRP+
sensory neurons in skin-innervating DRG. In the presentstudy, stress exposure resulted in a significantly higherpercentage of CGRP+ neurons among the skin-innervatingneurons localized in spinal DRG compared to nonstressedcontrol mice (p<0.05). Further, s.c. injection of NGF intothe dorsal skin also caused an increase in the relative CGRPexpression among the traced neurons, akin to stressexposure (p<0.05; Fig. 1b, representative photographs areshown in Fig. 2e–h).
1372 J Mol Med (2007) 85:1369–1378

Increased numbers of SP+ and CGRP+ sensory nerve fibersin the dermis
Besides the effect of stress and/or cutaneous NGF onneuronal plasticity of DRG, we wished to identify the effectof stress exposure or s.c. NGF injection in the dorsal skinon the expression of neuropeptides in the skin. In thispaper, we confirmed our pilot data [2] by showing thatstress exposure resulted in an increased number of SP+
nerve fibers in the skin, compared to nonstressed mice (p<0.01). In addition, we now provide experimental evidencethat local injection of NGF in the dorsal skin led to anincreased expression of SP+ nerve fibers in the skin,although levels of significance could not be reached whencompared to nonstressed control mice (Fig. 3a, representa-tive photographs are shown in Fig. 2i and j).
Stress exposure resulted in an increased number ofCGRP+ nerve fibers in the skin compared to nonstressedmice (p<0.05). Further, local injection of recombinant NGFin the dorsal skin led to a significantly increased number ofCGRP+ nerve fibers in the skin when compared tononstressed control mice (p<0.05; Fig. 3b; representativephotographs are shown in Fig. 2k and l).
Neutralization of NGF abrogates stress induced effectson the percentage of SP+ and CGRP+ sensory neuronsin skin-innervating DRG
In a second set of experiments, we determined the role ofNGF in stress-induced neuronal plasticity of SP+ and
CGRP + neurons in retrograde traced neurons of the DRGand nerve fibers in the skin, respectively, by neutralizingNGF in mice, employing an established method of injectingmice with a neutralizing antibody to NGF [4, 34]. Thisshowed that neutralization of NGF significantly abrogatedthe effect of stress on the increased percentage of SP+
neurons in DRG (p<0.05; Fig. 4a). Similarly, neutralizationof NGF also diminished the stress-triggered increasedpercentage of CGRP+ neurons in DRG (p<0.05; Fig. 4b).
Neutralization of NGF abrogates stress induced effectson numbers of SP+ and CGRP+ sensory nerve fibersin the dermis
Next, we analyzed the effect of NGF neutralization on SP+
and CGRP+ sensory nerve fibers in the dermis andobserved that both the stress-triggered increase in SP+
(Fig. 5a) as well as CGRP+ nerve fibers in skin (Fig. 5b)were significantly abrogated upon NGF neutralization.
Discussion
With the present work, we provide experimental evidencethat stress exposure and cutaneous NGF modulate thepercentage of SP+ and CGRP+ neurons in skin-innervatingDRG. We further show that stress exposure or s.c. injectionof NGF up-regulate the number of CGRP+ and SP+ skinnerve fibers. Lastly, we provide substantiation that the crosstalk between neuropeptide expression in skin and DRG is
Fig. 1 a Percentage of sub-stance P-positive neurons fromtotal number of retrogradetraced neurons in dorsal rootganglia from nonstressed con-trols, stressed mice, and non-stressed mice subcutaneouslyinjected with NGF. Columnsrepresent mean and SEM pergroup. b Percentage of CGRP-positive neurons from totalnumber of retrograde tracedneurons in dorsal root gangliafrom nonstressed controls,stressed mice, and nonstressedmice subcutaneously injectedwith NGF. Columns representmean and SEM per group
J Mol Med (2007) 85:1369–1378 1373

dependent on NGF, as systemic neutralization of NGFprevented stress-triggered alterations of CGRP+ and SP+
skin nerve fibers and skin-innervating DRG neurons.
Stress exposure up-regulates the number of CGRP+
and SP+ skin nerve fibers via NGF-dependent pathways
In the skin, neuropeptides comprise a large family ofregulatory molecules including tachykinins, CGRP, vasoac-tive intestinal peptide (VIP), pituitary adenylate cyclase-activating polypeptide (PACAP), and others. Their importantrole in skin health and disease has been investigatedintensively (latest reviews [35, 36]). In this context, awealth of published data is now available on the role ofcutaneous SP. Once released into the skin, the tachykininSP induces inflammation and vasodilatation and activatesmast cells [16, 37]. Increased numbers of SP+ nerve fibershave been observed in inflammatory skin diseases likeatopic dermatitis and psoriasis, as well as in AA and telogeneffluvium (recently reviewed in [38]). SP induces adhesionmolecule expression (P-selectin, E-selectin, VCAM-1) onskin-isolated human endothelial cells and promotes infiltra-tion with neutrophil and eosinophil granulocytes [39].
Further, emerging research indicates that cutaneousCGRP is released by sensory neurons and modulatesvasodilatation, plasma extravasation, as well as severalbiological functions of epidermal and dermal cells [37].There is some evidence that immunocompetent cells likemacrophages, lymphocytes, neutrophils, mast cells, andLangerhans cells express CGRP receptors indicating theimmunomodulating potential for CGRP [40–44]. In theskin, like SP, CGRP exerts vasoactive effects [12].Clearly, the skin is a crucial barrier protecting the bodyagainst external harmful influences [45], which is largelymediated by the skin’s immune system, whereas an im-paired barrier function is characteristic in immune derma-toses such as atopic dermatitis and psoriasis vulgaris [46,47]. Thus, an increased release of SP or CGRP in responseto stress, as identified in the present study by employing amouse model, may trigger or aggravate such immunedermatoses and/or AA by challenging skin immunehomeostasis and skin barrier function. This notion issupported by studies in humans suggesting that CGRP isinvolved in the pathophysiogenesis of AA. Hordinsky et al.[48] reported increased neuronal CGRP immunoreactivityaround eccrine glands of AA patients, while Meyronet et al.[49] found decreased immunoreactivity of skin and hairfollicles in the areas of lesions compared to biopsies fromhealthy scalp regions. Lower levels of CGRP were detectedwhen comparing biopsies from AA patients with those fromhealthy controls [50]. Other mediators like the neuropeptideneurotensin [51] or the corticotropin-releasing hormone(CRH) [52] via induction of mast cell degranulation might
Fig. 2 Representative examples of flourogold-traced dorsal rootganglia from nonstressed (a) and stressed mice (c). b Correspondingarea to a using the rhodamine filter to identify substance P (SP)-positive neurons. d Corresponding area to c using the rhodamine filterto identify SP-positive neurons. Arrows indicate SP-positive neurons.Representative examples of flourogold-traced dorsal root ganglia fromnonstressed (e) and stressed mice (g). f Corresponding area to e usingthe rhodamine filter to identify CGRP-positive neurons. h Correspondingarea to g using the rhodamine filter to identify CGRP-positive neurons.Arrows indicate CGRP-positive neurons. Immunoreactivity for SP (i, j)and CGRP (k, l). Representative dermis sections from nonstressedcontrols (i, k) and stressed mice (j, l). Magnification 200×
1374 J Mol Med (2007) 85:1369–1378

be involved in the pathogenesis of inflammatory skindisorders, especially those exacerbated by stress effects.Future research is needed to identify whether alterations ofskin neuropeptide expression in humans may be identified inresponse to high stress perception.
Stress-triggered cross talk between neuropeptidesexpression in skin and DRG is dependent on NGF
Neuropeptides are synthesized in the neuronal cell bodylocated in DRG and are transported to the peripheral nerveending and released under certain conditions like local
mechanical or thermical stimulation [53, 54]. As neuro-peptides located in cutaneous nerve fibers originate fromsensory neurons, we aimed to investigate their neuronalexpression. It is well established that increases in theneuropeptides SP and CGRP in the innervating DRG occurafter target-tissue damage like inflammation [18] orwounding [55]. In this paper, we were able to show thatsonic stress, a stimulus processed and transmitted from thecentral nervous system, induces neuronal plasticity in skin-innervating sensory neurons.
Second aim of the study was to dissect the role of NGFin stress-induced neuropeptide expression in DRG neurons.
Fig. 3 a Number of substanceP-positive nerve fibers per visu-al field in the dermis from non-stressed controls, stressed mice,and nonstressed mice subcuta-neously injected with NGF.Columns represent mean andSEM per group. b Number ofCGRP-positive nerve fibers pervisual field in the dermis fromnonstressed controls, stressedmice, and nonstressed micesubcutaneously injected withNGF. Columns represent meanand SEM per group
Fig. 4 a Percentage of sub-stance P-positive neurons fromtotal number of retrogradetraced neurons in dorsal rootganglia from nonstressed con-trols, stressed mice, and non-stressed mice and the respectivegroups subcutaneously injectedwith anti-NGF. Columns repre-sent mean and SEM per group.b Percentage of CGRP-positiveneurons from total number ofretrograde traced neurons indorsal root ganglia from non-stressed controls, stressed mice,and nonstressed mice and therespective groups subcutaneous-ly injected with anti-NGF.Columns represent meanand SEM per group
J Mol Med (2007) 85:1369–1378 1375

In the recent years, NGF and its ability to induce tachykininand other neuropeptide expression in DRG have beeninvestigated intensively in animal models in vivo and invitro. More than 20 years ago, Kessler and Black [25]showed for the first time that neonatal NGF applicationdramatically increased SP content in DRGs 2 days afterapplication. Similar results were reported by Otten et al.[24] the same year; however, administration of anti-NGFreduced SP content in sensory neurons and nerve fibers inthe skin. Local NGF injection into paws or ear skin led toincreased preprotachykinin and prepro CGRP mRNAexpression in the corresponding DRG and increased SPand CGRP immunoreactivity in corresponding afferentneurons [56]. In the present study, we were able to prove
that neuronal plasticity of DRG is under the influence ofstress, as the percentages of CGRP+ and SP+ skin-innervating neurons significantly increased, and highernumbers of nerve fibers localized in the skin showedneuropeptide positivity. Such stress-triggered ganglionicand peripheral neuropeptide expression is clearly regulatedby NGF, as neutralization of NGF abrogates the stresseffects. Further, s.c. application of recombinant NGFmimicked the increase in neuronal neuropeptide expressionin DRG. In this paper, no effect of s.c. NGF applicationcould be identified with respect to the number of SP+
cutaneous nerve fibers, which may be attributable to of theexperimental approach we chose, such as an impairedbioactivity of NGF by local degradation. However, NGF
Fig. 5 a Number of substanceP-positive nerve fibers per visu-al field in the dermis from non-stressed controls, stressed mice,and the respective groups sub-cutaneously injected with anti-NGF. Columns represent meanand SEM per group. b Numberof CGRP-positive nerve fibersper visual field in the dermisfrom nonstressed controls,stressed mice, and the respectivegroups subcutaneously injectedwith anti-NGF. Columns repre-sent mean and SEM per group
Fig. 6 Hypothetical scenario. After stress or exogenous NGFapplication, SP and CGRP are up-regulated in skin-innervatingneurons located in DRG. This neuronal increase is associated withlocal neuropeptide increase in skin nerve fibers. Release of theseneuropeptides leads to increased neurogenic inflammation, which
might not only interfere with hair follicle cycling, subsequentlyleading to telogen effluvium or an aggravation of alopecia areata, butalso deteriorate immune-driven dermatoses such as psoriasis or atopicdermatitis
1376 J Mol Med (2007) 85:1369–1378

application increased the number of CGRP+ cutaneousnerve fibers. This result is in line with findings from Alberset al. [57] who found increased sensory innervation in theskin of NGF-overexpressing mice.
Together with the finding that anti-NGF applicationabrogated stress-induced effects on neuropeptide expressionin retrograde traced neurons and local nerve fibers, our datastrongly suggest a stress-mediating role for NGF. Probably,stress through the demonstrated neuropeptide release andneurogenic inflammation might impair the skin barrierfunction by increasing vascular permeability and/or influ-encing local immunocompetent cell populations like den-dritic cells. This question has to be investigated in thefuture.
Finally, a hypothetical scenario based on our recentfindings is drawn in Fig. 6. After stress or exogenous NGFapplication, SP and CGRP are up-regulated in skin-innervating neurons located in DRG. This neuronal increaseis associated with local neuropeptide increase in skin nervefibers. Release of these neuropeptides leads to increasedneurogenic inflammation, which might not only interferewith hair follicle cycling, subsequently leading to telogeneffluvium or an aggravation of AA, but also deteriorateimmune-driven dermatoses such as psoriasis or atopicdermatitis.
Acknowledgments This work was supported by grants from theGerman Research Foundation (Deutsche Forschungsgemeinschaft;Ar 232/14-2; Pa 345/11-2) and the Charité (UFF 99-648). We thankR. Pliet, E. Hagen, P. Moschansky, and P. Busse for their excellenttechnical assistance.
References
1. Levenstein S, Prantera C, Varvo V, Scribano ML, Berto E,Andreoli A, Luzi C (1994) Psychological stress and diseaseactivity in ulcerative colitis: a multidimensional cross-sectionalstudy. Am J Gastroenterol 89:1219–1225
2. Arck PC, Handjiski B, Peters EMJ, Peter AS, Hagen E, Fischer A,Klapp BF, Paus R (2003) Stress inhibits hair growth in mice byinduction of premature catagen development and deleteriousperifollicular inflammatory events via neuropeptide substance P-dependent pathways. Am J Pathol 162:803–814
3. Joachim RA, Quarcoo D, Arck PC, Herz U, Renz H, Klapp BF(2003) Stress enhances airway reactivity and airway inflammationin an animal model of allergic bronchial asthma. Psychosom Med65:811–815
4. Peters EMJ, Handjiski B, Kuhlmei A, Hagen E, Bielas H, Braun A,Klapp BF, Paus R, Arck PC (2004) Neurogenic inflammation instress-induced termination of murine hair growth is promoted bynerve growth factor. Am J Pathol 165:259–271
5. Blois SM, Joachim R, Kandil J, Margni R, Tometten M, Klapp BF,Arck PC (2004) Depletion of CD8+ cells abolishes the pregnancyprotective effect of progesterone substitution with dydrogesteronein mice by altering the Th1/Th2 cytokine profile. J Immunol172:5893–5899
6. Wright RJ, Cohen RT, Cohen S (2005) The impact of stress on thedevelopment and expression of atopy. Curr Opin Allergy ClinImmunol 5:23–29
7. Al’Abadie MS, Kent GG, Gawkrodger DJ (1994) The relationshipbetween stress and the onset and exacerbation of psoriasis andother skin conditions. Br J Dermatol 130:199–203
8. Katsarou-Katsari A, Singh LK, Theoharides TC (2001) Alopeciaareata and affected skin CRH receptor upregulation induced byacute emotional stress. Dermatology 203:157–161
9. Panconesi E, Hautmann G (1996) Psychophysiology of stress indermatology. The psychobiologic pattern of psychosomatics.Dermatol Clin 14:399–421
10. Botchkarev VA (2003) Stress and the Hair Follicle: Exploring theConnections. Am J Pathol 162:709–712
11. Paus R, Theoharides TC, Arck PC (2006) Neuroimmunoendocrinecircuitry of the ‘brain–skin connection’. Trends Immunol 27:32–39
12. Holzer P (1998) Neurogenic vasodilatation and plasma leakage inthe skin. Gen Pharmacol 30:5–11
13. Kiernan JA (1972) The involvement of mast cells in vasodilata-tion due to axon reflexes in injured skin. Q J Exp Physiol CognMed Sci 57:311–317
14. Aloe L, Bracci Laudiero L, Alleva E, Lambiase A, Micera A,Tirassa P (1994) Emotional stress induced by parachute jumpingenhances blood nerve growth factor levels and the distribution ofnerve growth factor receptors in lymphocytes. Proc Natl Acad SciU S A 91:10440–10444
15. Tometten M, Klapp BF, Joachim R, Fest S, Zenclussen AC,Peters EM, Hertwig K, Arck PC (2004) Nerve growth factor andits functional receptor TrkA are up-regulated in murine decidualtissue of stress-triggered and substance P-mediated abortion. Am JReprod Immunol 51:86–93, DOI 10.1046/j.8755-8920.2003.00123
16. Singh LK, Pang X, Alexacos N, Letourneau R, Theoharides TC(1999) Acute immobilization stress triggers skin mast celldegranulation via corticotropin releasing hormone, neurotensin,and substance P: A link to neurogenic skin disorders. Brain BehavImmun 13:225–239
17. Levi-Montalcini R, Skaper SD, Dal Toso R, Petrelli L, Leon A(1996) Nerve growth factor: from neurotrophin to neurokine.Trends Neurosci 19:514–520
18. Donnerer J, Schuligoi R, Stein C (1992) Increased content andtransport of substance P and calcitonin gene-related peptide insensory nerves innervating inflamed tissue: evidence for aregulatory function of nerve growth factor in vivo. Neuroscience49:693–698
19. Bracci-Laudiero L, Pincelli C (1995) Nerve growth factor isincreased in psoriatic skin. J Invest Dermatol 105:854–855
20. Qiu BS, Vallance BA, Blennerhassett PA, Collins SM (1999)The role of CD4+ lymphocytes in the susceptibility of mice tostress-induced reactivation of experimental colitis. Nat Med 5:1178–1182
21. Pincus-Knackstedt MK, Joachim RA, Blois SM, Douglas AJ,Orsal AS, Klapp BF, Wahn U, Hamelmann E, Arck PC (2006)Prenatal stress enhances susceptibility of murine adult offspringtoward airway inflammation. J Immunol 177:8484–8492
22. Peters EMJ, Kuhlmei A, Tobin DJ, Muller-Rover S, Klapp BF,Arck PC (2005) Stress exposure modulates peptidergic innerva-tion and degranulates mast cells in murine skin. Brain BehavImmun 19:252–262
23. Aoki E ST, Kawana S. (2003) Intermittent foot shock stressprolongs the telogen stage in the hair cycle of mice. Exp Dermatol12:371–377
24. Otten U, Goedert M, Mayer N, Lembeck F (1980) Requirement ofnerve growth factor for development of substance P-containingsensory neurones. Nature 287:158–159
J Mol Med (2007) 85:1369–1378 1377

25. Kessler JA, Black IB (1980) Nerve growth factor stimulates thedevelopment of substance P in sensory ganglia. Proc Natl AcadSci U S A 77:649–652
26. Botchkarev VA, Eichmuller S, Peters EM, Pietsch P, Johansson O,Maurer M, Paus R (1997) A simple immunofluorescencetechnique for simultaneous visualization of mast cells and nervefibers reveals selectivity and hair cycle-dependent changes in mastcell-nerve fiber contacts in murine skin. Arch Dermatol Res289:292–302
27. Peters EMJ, Botchkarev VA, Botchkareva NV, Tobin DJ, Paus R(2001) Hair-cycle-associated remodeling of the peptidergic inner-vation of murine skin, and hair growth modulation by neuro-peptides. J Invest Dermatol 116:236–245
28. Wallengren J, Hakanson R (1987) Effects of substance P, neuro-kinin A and calcitonin gene-related peptide in human skin andtheir involvement in sensory nerve-mediated responses. Eur JPharmacol 143:267–273
29. Dinh QT, Groneberg DA,Mingomataj E, Peiser C, Heppt W, Dinh S,Arck PC, Klapp BF, Fischer A (2003) Expression of substance P andvanilloid receptor (VR1) in trigeminal sensory neurons projecting tothe mouse nasal mucosa. Neuropeptides 37:245–250
30. Muller-Rover S, Handjiski B, van der Veen C, Eichmuller S,Foitzik K, McKay IA, Stenn KS, Paus R (2001) A comprehensiveguide for the accurate classification of murine hair follicles indistinct hair cycle stages. J Invest Dermatol 117:3–15
31. Braun A, Quarcoo D, Schulte-Herbrüggen O, Lommatzsch M,Hoyle G, Renz H (2001) Nerve Growth Factor Induces AirwayHyperresponsiveness inMice. Int ArchAllergy Immunol 124:205–207
32. Stenn KS, Paus R (2001) Controls of hair follicle cycling. PhysiolRev 81:449–494
33. Botchkarev VA, Eichmüller S, Johansson O, Paus R (1997) Haircycle-dependent plasticity of skin and hair follicle innervation innormal murine skin. J Comp Neurol 386:379–395
34. Tometten M, Blois S, Kuhlmei A, Stretz A, Klapp BF, Arck PC(2006) Nerve growth factor translates stress response andsubsequent murine abortion via adhesion molecule-dependentpathways. Biol Reprod 74:674–683
35. Roosterman D, Goerge T, Schneider SW, Bunnett NW, Steinhoff M(2006) Neuronal control of skin function: the skin as a neuro-immunoendocrine organ. Physiol Rev 86:1309–1379
36. Hendrix S, Peters E (2007) Neuronal plasticity and neuroregenera-tion in the skin—The role of inflammation. J Neuroimmunol184:113–126
37. Scholzen TE, Steinhoff M, Bonaccorsi P, Klein R, Amadesi S,Geppetti P, Lu B, Gerard NP, Olerud JE, Luger TA, Bunnett NW,Grady EF, Armstrong CA, Ansel JC (2001) Neutral endopeptidaseterminates substance P-induced inflammation in allergic contactdermatitis. J Immunol 166:1285–1291
38. Steinhoff M, Stander S, Seeliger S, Ansel JC, Schmelz M, Luger T(2003) Modern aspects of cutaneous neurogenic inflammation.Arch Dermatol 139:1479–1488
39. Smith C, Barker J, Morris R, MacDonald D, Lee T (1993)Neuropeptides induce rapid expression of endothelial cell adhe-sion molecules and elicit granulocytic infiltration in human skin. JImmunol 151:3274–3282
40. Wang F, Millet I, Bottomly K, Vignery A (1992) Calcitonin gene-related peptide inhibits interleukin 2 production by murine Tlymphocytes. J Biol Chem 267:21052–21057
41. McGillis J, Humphreys S, Reid S (1991) Characterization offunctional calcitonin gene-related peptide receptors on rat lym-phocytes. J Immunol 147:3482–3489
42. Vignery A, Wang F, Ganz MB (1991) Macrophages expressfunctional receptors for calcitonin-gene-related peptide. J CellPhysiol 149:301–306
43. Kitabatake Y, Kawamura S, Yamashita M, Okuyama K,Takayanagi M, Ohno I (2004) The expression of mRNA forcalcitonin gene-related peptide receptors in a mucosal type mastcell line, RBL-2H3. Biol Pharm Bull 27:896–898
44. Hosoi J, Murphy GF, Egan CL, Lerner EA, Grabbe S, Asahina A,Granstein RD (1993) Regulation of Langerhans cell function by nervescontaining calcitonin gene-related peptide. Nature 363:159–163
45. Elias PM, Wood LC, Feingold KR (1999) Epidermal patho-genesis of inflammatory dermatoses. Am J Contact Dermat 10:119–126
46. Chamlin SL, Kao J, Frieden IJ, Sheu MY, Fowler AJ, Fluhr JW,Williams ML, Elias PM (2002) Ceramide-dominant barrier repairlipids alleviate childhood atopic dermatitis: Changes in barrierfunction provide a sensitive indicator of disease activity. J AmAcad Dermatol 47:198–208
47. Ghadially R, Reed JT, Elias PM (1996) Stratum corneum structureand function correlates with phenotype in psoriasis. J InvestigDermatol 107:558–564
48. Hordinsky M, Kennedy W, Wendelschafer-Crabb G, Lewis S(1995) Structure and function of cutaneous nerves in alopeciaareata. J Invest Dermatol 104:28S–29S
49. Meyronet D, Jaber K, Gentil-Perret A, Cambazard F, Misery L(2003) Decreased CGRP staining in alopecia areata. Brit JDermatol 149:422–424
50. Rossi R, Del Bianco E, Isolani D, Baccari MC, Cappugi P (1997)Possible involvement of neuropeptidergic sensory nerves inalopecia areata. Neuroreport 8:1135–8
51. Donelan J, Boucher W, Papadopoulou N, Lytinas M, Papaliodis D,Dobner P, Theoharides TC (2006) Corticotropin-releasing hormoneinduces skin vascular permeability through a neurotensin-dependentprocess. Proc Natl Acad Sci 103:7759–7764
52. Theoharides TC, Singh LK, Boucher W, Pang X, Letourneau R,Webster E, Chrousos G (1998) Corticotropin-releasing hormoneinduces skin mast cell degranulation and increased vascularpermeability, a possible explanation for its proinflammatoryeffects. Endocrinology 139:403–413
53. Lu C-L, Pasricha PJ, Hsieh J-C, Lu R-H, Lai C-R, Wu L-L,Chang F-Y, Lee S-D (2005) Changes of the neuropeptides contentand gene expression in spinal cord and dorsal root ganglion afternoxious colorectal distension. Regul Pept 131:66–73
54. Siney L, Brain SD (1996) Involvement of sensory neuropeptidesin the development of plasma extravasation in rat dorsal skinfollowing thermal injury. Br J Pharmacol 117:1065–1070
55. Cruise BA, Xu P, Hall AK (2004) Wounds increase activin in skinand a vasoactive neuropeptide in sensory ganglia. Dev Biol 271:1–10
56. Amann R, Sirinathsinghji DJS, Donnerer J, Liebmann I, Schuligoi R(1996) Stimulation by nerve growth factor of neuropeptide synthesisin the adult rat in vivo: bilateral response to unilateral intraplantarinjections. Neurosci Lett 203:171–174
57. Albers K, Wright D, Davis B (1994) Overexpression of nervegrowth factor in epidermis of transgenic mice causes hypertrophyof the peripheral nervous system. J Neurosci 14:1422–1432
1378 J Mol Med (2007) 85:1369–1378

ORIGINAL ARTICLE
Cannabinoid CB1 receptor stimulation affordsneuroprotection in MPTP-induced neurotoxicityby attenuating S100B up-regulation in vitro
Teresa Iuvone & Giuseppe Esposito & Daniele De Filippis &
Tiziana Bisogno & Stefania Petrosino & Caterina Scuderi &Vincenzo Di Marzo & Luca Steardo &
Endocannabinoid Research Group
Received: 1 December 2006 /Revised: 30 March 2007 /Accepted: 22 May 2007 / Published online: 17 July 2007# Springer-Verlag 2007
Abstract In this study, we investigated the mechanism ofS100B neurotoxicity and the effect of cannabinoids, in C6cells treated with 1-methyl-4-phenyl 1,2,3,6 tetrahydropyr-idine (MPTP) and co-cultured with differentiated PC12 cells.MPTP concentration- and time-dependently increasedS100B density in C6 cells. This effect was followed byincreased C6 cell proliferation and decreased cell viability ofco-cultured PC12 cells. An antibody against S100B, given toPC12 cells before co-culture, led to their survival. Treatmentwith arachidonyl-2-chloroethylamide, a CB1 agonist, sig-nificantly inhibited MPTP-induced S100B density in C6cells and protected co-cultured PC12 cells from cell death.Because MPTP selectively increased the levels of ananda-mide in C6 cells, the involvement of the endocannabinoidsystem was investigated by using selective inhibitors ofendocannabinoid inactivation (cellular re-uptake or enzy-matic hydrolysis) and selective cannabinoid CB1 and CB2
receptor antagonists and by silencing the CB1 receptor. Ourdata suggest that selective activation of CB1 receptors byeither exogenous or endogenous cannabinoids might affordneuroprotection in MPTP-induced neurotoxicity also bycontrolling S100B up-regulation in activated glial cells.
Keywords Cannabinoid .MPTP. Neurotoxicity
J Mol Med (2007) 85:1379–1392DOI 10.1007/s00109-007-0233-y
Teresa Iuvone, Daniele De Filippis, Tiziana Bisogno, StefaniaPetrosino and Vincenzo Di Marzo are collaborated with theEndocannabinoid Research Group.
T. Iuvone (*) :D. De FilippisDepartment of Experimental Pharmacology, Faculty of Pharmacy,University of Naples “Federico II”,Via D. Montesano, 49,80131 Naples, Italye-mail: [email protected]
G. Esposito :C. Scuderi : L. SteardoDepartment of Human Physiology and Pharmacology “V.Erspamer”, University of Rome “La Sapienza”,Rome, Italy
T. Bisogno : S. Petrosino :V. Di MarzoInstitute of Biomolecular Chemistry,CNR, Pozzuoli,Naples, Italy
TERESA IUVONEgraduated in Pharmacy in 1985.She received her M.S. in Ex-perimental Pharmacology andher Ph.D. in Chemistry of Nat-ural Drugs from the Universityof Naples Federico II, Italy. Sheis presently associate professorin Pharmacology at the Facultyof Pharmacy of the same Uni-versity. Her research interestsregard the molecular mecha-nisms at the basis of the in-flammatory process, includingthe neuroinflammation and thepharmacology of cannabinoidsand endocannabinoid system.
LUCA STEARDOreceived his M.D. degree fromthe University of Naples“Federico II.” He is presentlyfull professor of Pharmacologyand Pharmacotherapy at theUniversity of Rome “LaSapienza.” At present, hisresearch interests includecellular and molecular mecha-nisms involved in neuroinflam-matory/neurodegenerativeprocesses and the possibleinvolvement of cannabinoidsystem in the neurobiology ofdrug abuse and eating disorders.

Introduction
The neurotoxin 1-methyl-4-phenyl 1,2,3,6 tetrahydropyr-idine (MPTP) induces in primates and in rodents neurolog-ical and pathological changes comparable to those observedin Parkinson’s disease (PD) [1]. MPTP neurotoxicity hasbeen demonstrated to involve energy depletion and freeradicals production [2]. Its detrimental action is initiated by1-methyl -4 phenylpyridinium (MPP+), a noxious metabo-lite generated by the monoamino-oxidase B, an enzymelocated in the brain mostly in astrocytes. MPP+, taken upinto dopaminergic neurons [3], is then accumulated into themitochondria, where it disrupts oxidative phosphorylation,thereby leading to adenosine triphosphate productionimpairment, intracellular calcium enhancement and overtincrease in free radical production.
Reactive gliosis represents a common response of thebrain to a neuronal injury [4]. It is characterized byactivation of either microglia or astroglia, both able torespond to insults and to participate to the pathologicalprocess. The glial reaction observed in PD experimentalmodels has been believed to contribute significantly toneuronal degeneration [5, 6] because activated astrocytesand microglia express a broad array of neurotoxic molecules,including pro-inflammatory cytokines and chemokines, inaddiction to reactive oxygen and nitrogen species. In thereactive gliosis secondary to MPTP exposure, it has beenreported that astrocyte activation parallels the time courseof neuronal cell death and lasts long after most neuronshave died as a consequence of MPTP toxicity. Althoughevidence suggests that astroglial activation may be crucialfor MPTP-induced neuronal loss [7], the precise role ofreactive astrogliosis in the cascade of deleterious eventsultimately leading to neuronal death remains still not clearlyelucidated.
S100B is a calcium/zinc-binding protein produced andsecreted by astrocytes; it is expressed throughout the brainand is observed primarily in the cytoplasm of astrocytes [8].The role of S100B is still under debate. In fact, on the onehand, it was believed that S100B is neuroprotective becauseit may decrease neuronal injury and/or contribute to repairafter traumatic brain injury [9]; on the other hand, earlyinvestigations have shown that exaggerated expression ofS100B can result in neuronal damage [10]. Consistentwith the latter observations, evidence has been providedsuggesting that S100B up-regulation behaves as a worsen-ing factor in some neurodegenerative pathologies, such asDown’s syndrome and Alzheimer’s disease [11]. It isinteresting to note that more recent studies have demon-strated that S100B-positive cells may be involved inMPTP-induced neuronal death [12], although the informa-tion regarding the precise relationship between S100B over-expression and MPTP-caused neurodegeneration is still
very limited. Therefore, further investigations are needed tobetter understand the exact mechanism of the role ofastrocyte S100B over-production in MPTP neurotoxiceffects.
Activation of the cannabinoid system has been proposedto act ‘on demand’ to limit neuronal damage during toxicevents and to be neuroprotective in different experimentalmodels [13, 14]. Cannabinoids can modulate inflammatoryresponse [15], and it has been reported that they can affectastroglial functions [16]. Astrocytes have been observed topossess a functional endocannabinoid system (ECS) be-cause (a) they express cannabinoid receptors, termed CB1
and CB2, (b) they produce the endogenous ligands of thesereceptors, anandamide (AEA) [17] and 2-arachydonoylglycerol (2-AG) [15] and (c) they also contain themolecular machinery to inactivate these compounds bycellular uptake and degradation [18] either by fatty acidamide hydrolase [19] or monoacylglycerol lipase [20]. Thisclose relationship between the ECS and glial cells hasattracted much attention in the attempt to identify newmolecular targets aimed to attenuating or even haltingreactive gliosis. Therefore, based on the above background,the major purpose of the present study was to elucidate (1)the involvement of S100B in MPTP-induced neurotoxicity,(2) the molecular mechanism of S100B neurotoxicity and(3) the role of CBs and the ECS in the control of S100Btoxicity, in MPTP-exposed C6 rat glioma cells co-culturedwith rat pheochromocytoma PC12 cells differentiated intoneurons.
Materials and methods
All materials for cell culture were purchased from Bio-Whittaker (Caravaggio, BG, Italy). Foetal calf serum andhorse serum (HS) were from HyClone (Logan, UT). MPTP,nerve growth factor, FURA-2 and all the material unlessotherwise stated were from Sigma-Aldrich (St.Louis, MO).Anti-S100B antibody was from AbCam (Cambridge, UK),anti-CB1 antibody was from Affinity BioReagent (Golden,CO) and anti-CB2 antibody was from Cayman (Ann Arbor,MI); AEA, arachidonyl-2-chloroethylamide (ACEA), JWH-015 were from Tocris (Cookson, Bristol, UK), SR141716Aand SR144528 were a gift from Dr. Madaleine Mosse(SANOFI-Reserche, Montpellier, France) and VDM-11 andarachydonoylserotonin (AA-5-HT) were synthesized in thelaboratory of prof. Vincenzo Di Marzo (CNR-Pozzuoli,Italy).
Rat C6 glioma cell culture and treatments
C6 rat glioma cells (American Type Tissue Collection CCL-107) were cultured in 10-cm Petri dishes in Dulbecco’s
1380 J Mol Med (2007) 85:1379–1392

Modified Eagle’s Medium (DMEM) supplemented with 5%foetal bovine serum (FBS), 2 mM glutamine, 100 U/mLpenicillin and 100 μg/mL streptomycin at 37°C in 5% CO2/95% air. Confluent cells were washed three times withphosphate-buffered saline (PBS), detached with tripsyn/ethyl-enediamine tetraacetic acid, plated and left to adhere for 24 hat 37°C. Thereafter, confluent C6 cells were treated withdifferent concentration of MPTP (ranging up from 1 to100 μM) for different time points according to the experi-mental protocol and in presence or absence of the followingsubstances: a selective CB1 agonist, ACEA (10−8−10−6 M), aselective CB2 agonist, JWH015 (10−8−10−6 M), the endo-cannabinoid AEA (10−8−10−6 M), the inhibitor of AEAenzymatic hydrolysis AA-5-HT (10−8−10−6 M) [21], addedto C6 cells 15 min before MPTP in the presence or in theabsence of selective CB1 and CB2 receptor antagonists,SR141716A (10−8−10−6 M) and SR144528 (10−6 M). In thecontrol experiments, we also tested the effect of SR141716-Aand ACEA (10−6 M) on C6 cell in absence of MPTP(100 μM). In some experiments, VDM-11 (10−7−10−6 M), asynthetic inhibitor of AEA transport across the cell membrane[22], was added 30 min before or 12 h after MPTP (100 μM)stimulation to C6 cells. In other experiments, an anti-S100B-neutralizing antibody (dilution 1:1,000–1:10,000 v/v) or anunrelated IgG (anti-tubulin) was added to cells 15 min beforeMPTP (100 μM).
Rat PC12 pheocromocytoma cell culture
In our study, we used differentiated rat pheocromocytomaPC12 cells that are currently considered a useful model forin vitro study of neuronal toxicity, as in cited references[23]. Moreover, PC12 cells can be considered as dopami-nergic-like neurons because they synthesize and releasedopamine [24]. PC12 cells (American Tissue Type Collec-tion CRL-1721) were cultured in 10-cm Petri dishes inDMEM supplemented with 5% FBS, 15% HS, 2 mMglutamine, 100 U/mL penicillin and 100 μg/mL streptomy-cin at 37°C in 5% CO2/95% air and differentiated withretinoic acid as described by Koh et al. [25]. Depending onthe experiments, PC12 cells were treated with a MPTP-conditioned C6 cell medium, with S100B protein (SigmaAldrich; 0.005–5 μM) or co-cultured with C6 cells. Insome experiments, an anti-S100B-neutralizing antibody(dilution 1:1,000 v/v) or an anti-tubulin (dilution 1:1,000v/v) antibody were added directly to PC12 cells in theexperiments with co-cultures or ‘conditioned medium.’
Experiments with co-cultures of C6/PC12 cells
In ‘co-culture’ experiments, confluent PC12 cells were seededin sterile Falcon inserts at the density of 2.5×105 cells/well. Inparallel, C6 cells (1×106 cells/well) were treated for 24 h with
MPTP (100 μM) in a six-multiwell plate with or withoutACEA (10−8−10−6 M), JWH015 (10−8−10−6 M), AEA(10−7−10−6 M) and AA-5HT (10−7−10−6 M) in the presenceor absence of SR141716A (10−6 M) given 15 min beforeMPTP. In other experiments, SR141716A (10−8−10−6 M)alone was given 15 min before MPTP. Then, the C6 cellsupernatant was removed, and cells were extensivelywashed to remove any residual MPTP or MPTP metabolitesor tested drugs. C6 cells were then supplemented with freshmedium, and PC12 cells were inserted in the six-multiwellplate. PC12 and C6 cells were than co-cultured for a further24 h at 37°C (Scheme 1). After this time, the inserts wereremoved, and PC12 cell viability was measured by the3-(4,5-dimethyltiazol-2yl)-2,5 diphenyltetrazolium bromide(MTT)–formazan conversion assay (see below).
Experiments with PC12 cells and the conditioned mediumfrom MPTP-treated C6 cells
PC12 cells were incubated for different time periods withthe ‘conditioned medium,’ deriving from C6 cells previ-ously treated with MPTP (100 μM) for 24 h, to measure[Ca2+]i levels and caspase-3 activity. In some experiments,an S100B-neutralizing antibody (1:1,000 v/v dilution) wasadded to the PC12 cell medium 15 min before theirexposure to the C6 cell ‘conditioned medium.’
Preparation of cytosolic fractions from C6 and PC12 cellsand Western blot analysis for S100B
Extracts of C6 and PC12 cells treated as described abovewere prepared as previously reported [26]. Briefly, harvested
Scheme 1 General procedure for the ‘co-culture’ experiments (seeexperimental procedures)
J Mol Med (2007) 85:1379–1392 1381

cells (1×106) were washed two times with ice-cold PBSand centrifuged at 180×g for 10 min at 4°C. The cell pelletwas resuspended in 100 μL of ice-cold hypotonic lysisbuffer (10 mM 4-(2-hydroxyethyl)-1-piperazineethanesul-fonic acid [HEPES], 1.5 mM MgCl2, 10 mM KCl, 0.5 mMphenylmethylsulphonylfluoride, 1.5 μg/mL soybean trypsininhibitor, 7 μg/mL pepstatin A, 5 μg/mL leupeptin, 0.1 mMbenzamidine, 0.5 mM dithiothreitol) and incubated on icefor 15 min. The cells were lysed by rapid passage through asyringe needle for five to six times, and the cytoplasmicfraction was then obtained by centrifugation for 1 min at13,000×g. Cytosolic fraction proteins were mixed withnon-reducing gel-loading buffer (50 mM Tris/10% sodiumdodecyl sulphate [SDS]/10% glycerol/10%/2 mg of bro-mophenol per mL) in a ratio of 1:1, boiled for 3 min andcentrifuged at 10,000×g for 10 min. Cytosolic fractionproteins were mixed with gel-loading buffer (50 mM Tris/10% SDS/10% glycerol/10%/2-mercaptoethanol /2 mg ofbromophenol per mL) in a ratio of 1:1, boiled for 3 min andcentrifuged at 10,000×g for 10 min. Protein concentrationwas determined, and equivalent amounts (100 μg) of eachsample were electrophoresed in a 15% discontinuouspolyacrylamide mini-gel. The proteins were transferredonto nitro-cellulose membranes, according to the manufac-turer’s instructions (Bio-Rad). The membranes weresaturated by incubation at 4°C overnight with 10% non-fat dry milk in PBS and then incubated with 1:1,000 v/vanti-mouse S100B antibody, 1:250 v/v anti-rabbit CB1
(Affinity SpioBio), 1:250 v/v anti-rabbit CB2 (Cayman) or1:1,000 v/v anti-mouse tubulin antibody. The membraneswere washed three times with 1% Triton 100-X in PBS andthen incubated with anti-mouse or anti-rabbit immunoglob-ulins coupled to peroxidase (1:2000 v/v). The immuno-complexes were visualised by the ECL chemiluminescencemethod (Amersham, Buckinghamshire, UK). Subsequently,the relative density of S100B protein in the cytosolicfraction was quantified by densitometric scanning of theX-ray films with a GS 700 Imaging Densitometer (Bio-Rad,Hercules, CA) and a computer programme (MolecularAnalyst, IBM).
MTT–formazan assay
Cell viability was measured both on C6 and on PC12 cellsusing the MTT assay, as previously described [26]. MTT(5 mg/mL in DMEM) was added to the cells treated asabove described, and cells were incubated for additional 3 hat 37°C. After this time interval, cells were lysed, and darkblue crystals were solubilized with a solution containing50% (v/v) N,N′-dimethyl formamide, 20% (w/v) SDS withan adjusted pH of 4.5. The optical density (OD) of eachwell was measured with a microplate spectrophotometer(Titertek Multiskan MCC/340) equipped with a 620-nm
filter. The cell viability was thus calculated as percent ofcell viability=(OD treated/OD control)×100.
Determination of [Ca+2]i levels in C6 cells and in PC12cells
Intracellular calcium [Ca+2]i levels were measured, atdifferent time points, both in C6 and in PC12 cells byusing the fluorescent probe FURA-2AM as described byGrynkiewicz et al. [27]. Both cell types, after the specifictreatment described, were incubated at the density of 2.5×105 cells in Hanks Balanced Salt Solution (HBSS; 137 mMNaCl, 5.4 mM KCl, 0.49 mM MgCl2, 0.44 mM KH2PO4,0.64 mM Na2HPO4, 3 mM NaHCO3, 5.5 mM glucose,1.26 mM CaCl2 and 20 mM HEPES, pH 7.4) buffercontaining 4 μL (5 μM) FURA-2 probe at 37°C for 1 h.Afterwards, cells were centrifuged at 1,200 rpm for 5 minand washed with fresh HBSS buffer, and a volume of200 μL of cells (5×103) were subjected to 340/380 nm dualwavelength measurement using a spectrofluorometer withan LS55 luminescence spectrometer (Perkin Elmer). Calci-um influx was so expressed as percent of increase in basal.
ELISA assay
Nunc Maxisorp 96-well microtiter plates (Gibco, Paisley,UK) were coated overnight at 4°C with 1 μg/well ofmonoclonal anti-S100B antibody, diluted in 0.5 M Na2CO3.The wells were washed three times and then blocked withPBS containing 0.05% (v/v) Tween 20 and 0.3% FBS(enzyme-linked immunosorbent assay [ELISA] buffer) for30 min at room temperature. The standards and sampleswere added in a 100-μL volume and incubated at 37°C for1.5 h. The standard curve was generated using 0.1 ng to1 μg/well of purified S100B, diluted in ELISA buffer.Supernatant from C6 cells, treated with MPTP (100 μM) inthe presence or absence of ACEA (10−8−10−6) or JWH-015, was diluted (1:100) in ELISA buffer, and 100 μL wasassayed in triplicate. After four washes in ELISA buffer,monoclonal anti-S100B antibodies were diluted 1:500 andadded to the wells for 1 h. The wells were washed fourmore times and then incubated with the secondaryantibody: anti-mouse Ig, biotinylated species-specific F(ab8)2 fragment from the donkey (Amersham), diluted1:1,000, for 1 h. After a further four washes, the wells wereincubated with 100 μL of streptavidinbiotinylated horse-radish peroxidase complex (Amersham) diluted 1:1,000 inELISA buffer for 1 h. After a final six washes in ELISAbuffer, 200 μL of a 0.4 mg/mL solution of o-phenylenedi-amine dihydrochloride (Sigma) in a 0.05-M phosphatecitrate buffer was added to each well, and colour wasallowed to develop for up to 10 min. The colour reaction wasstopped by the addition of HCl, and ODs at 490 nm were
1382 J Mol Med (2007) 85:1379–1392

measured using a microplate reader. The absorbance valueswere corrected by subtracting background readings of wellsin which the antigen was omitted. The sensitivity of the assaywas 0.1 ng/mL purified S100B. All data were read from thelinear portion of the standard curve (1–100 ng/mL).
RNA Interference
Transfection of 25-nucleotide small interfering RNA(siRNA) duplexes (Santa Cruz Biotechnology) for targetingendogenous genes was carried out using OligofectAMINE(Invitrogen) and 70 pmol siRNA for each transfectionaccording to manufacturing instructions (Santa Cruz Bio-technology) Transfected C6 cells were serum starved andassayed 3 days after transfection.
The sequence of the siRNA used for rat CB1 receptorwas: ACGTGGGCTCGAATGACATTCAGTA accessionnumber U40395. Specific silencing of targeted genes wasconfirmed by Western blot analysis for CB1 receptor.Transfected C6 cells were then treated for 24 h with MPTP(1–100 μM).
Quantification of endocannabinoids in MPTP-treated rat C6glioma cells
After stimulation, media plus cells were treated with 2 volof cold methanol and transferred to 50-mL Falcon tubes. Atthis point, 100 pmol of d8-AEA, d4-palmitoylethanolamideand d5-2-AG were added as internal standards. The mixturewas then extracted three times with 4 vol of chloroform by30-s sonication. The three organic phases were then pooled,lyophilised and pre-purified by open-bed chromatographyon silica gel, eluted with chloroform/methanol (9:1 v/v).The eluate was then lyophilised and analysed by isotopedilution–liquid chromatography–atmospheric pressurechemical ionization–mass spectrometry (MS) using con-ditions described in Marsicano et al. [28] and allowing theseparation of 2-AG and AEA. MS detection was carried outin the selected ion monitoring mode using m/z values of356.0 and 348.0 (molecular ions +1 for deuterated andundeuterated AEA), 384.35 and 379.35 (molecular ions +1for deuterated and undeuterated 2-AG) and 304.0 and 300.0(molecular ions +1 for deuterated and undeuterated palmi-toylethanolamide). The area ratios between signals ofdeuterated and undeuterated AEA varied linearly withvarying amounts of undeuterated AEA (30 fmol–100 pmol).The same applied to the area ratios between signals ofdeuterated and undeuterated 2-AG in the 100 pmol–20 nmolinterval. AEA and 2-AG levels in unknown samples weretherefore calculated on the basis of their area ratios with theinternal deuterated standard signal areas. The amounts ofendocannabinoids are expressed as pmoles per milligram oflipid extract.
Results
Effect of MPTP on S100B protein density
The density of S100B protein in C6 cells treated with MPTPwas evaluated, in two different sets of experiments, byWestern blot analysis and the band corresponding to proteinmolecular weight was quantified by densitometry. In thefirst set of experiments, incubation with MPTP (1–100 μM)for 24 h resulted in a significant and concentration-dependent increase in S100B protein density in C6 cellswith respect to basal levels (unstimulated cells). In a secondset of experiments, C6 cells were treated for 24 h withMPTP (100 μM) and extensively washed, and S100Bprotein density was evaluated after further 24 h. Underthese conditions, S100B protein density in C6 cells was stillsignificantly increased with respect to basal levels (Fig. 1).
Effect of MPTP on [Ca+2]i levels in C6 cells
Because S100B is a calcium-binding protein, we tested thehypothesis that an increase in intracellular calcium ([Ca+2]i)levels after MPTP administration may be a trigger signalfor S100B up-regulation. Therefore, we measured [Ca+2]ilevels in MPTP-treated C6 cells after different intervals oftime.
Fig. 1 Effect of MPTP (1–100 μM) on S100B protein density in C6cells. a Western blot analysis of S100B protein at 24 and 48 h.b Relative densitometric analysis. Each bar shows the mean±SEM ofn=4 experiments. *P<0.05, ***P<0.001 vs control
J Mol Med (2007) 85:1379–1392 1383

When MPTP was added to C6 cells, [Ca+2]i levels weresignificantly increased starting from 20 up to 120 min,reaching a peak at 60 min, in comparison to basal levels(unstimulated cells; no Ca+2 detection by FURA-2 wasrevealed). At 60 min, moreover, MPTP (1–100 μM)concentration-dependently increased [Ca+2]i, in comparisonto basal levels (Fig. 2).
Effect of MPTP on C6 cell proliferation
Incubation of C6 cells with MPTP (1–100 μM) concentra-tion-dependently increased cell proliferation at 48 h. Theeffect of MPTP on C6 cell proliferation was significantlyand concentration-dependently inhibited by the anti-S100Bantibody given to the cells 15 min before MPTP challenge,while the unrelated anti-tubulin IgG was ineffective (Fig. 3).
Effect of MPTP-conditioned C6 cell medium on PC12[Ca+2]i levels
Because it has been described that S100B protein directlyincreases Ca+2 influx in neuronal cell lines and this isaccompanied by a pro-apoptotic effect [29], we evaluated theincrease in [Ca+2]i levels in PC12 cells treated for differenttime intervals (5–15–30–60–120 min) with the ‘conditionedmedium’ from MPTP (100 μM)-treated C6 cells.
[Ca+2]i levels increased in PC12 cells starting from 5 to120 min with respect to basal levels (unstimulated cells),reaching a peak at 30 min and progressively decreasing at120 min (Fig. 4a). When PC12 cells were treated with anti-S100B antibody (dilution 1:1,000 v/v), given 15 min beforethe MPTP-‘conditioned medium,’ this [Ca+2]i increase wassignificantly reduced at all time points (Fig. 4a). The
S100B-neutralizing antibody given alone to PC12 cells didnot modify [Ca+2]i (Fig. 4a).
Effect of MPTP on co-cultured PC12 cell viability
In co-cultured PC12 cells, we observed a reduction in cellviability in comparison to control cells (PC12 cells co-cultured with unstimulated C6 cells=100% viability). Theanti-S100B antibody (1:1,000 v/v dilution) reversed PC12 celldeath, while the unrelated anti-tubulin IgG was ineffective,suggesting that the effect was mediated, at least in part, byS100B release from MPTP-treated C6 cells (Fig. 4b).
Effect of exogenous S100B on PC12 cell-viability
Treatment with S100B protein (0.005–5 μM) significantlyand concentration dependently reduced PC12 cells viability(Fig. 4c).
Effect of the conditioned medium from 24-h MPTP-treatedC6 cells on caspase-3 activation in PC12 cells
To study whether PC12 cell death occurred because ofapoptosis, we evaluated the appearance of caspase-3 fromthe inactive precursor, pro-caspase, in cellular extracts ofPC12 cells co-cultured for 3 or 6 h with the ‘conditionedmedium’ derived from MPTP (100 μM)-treated C6 cells, inthe presence or absence of an anti-S100β antibody.
Fig. 3 Effect of MPTP (1–100 μM) on C6 cell proliferation at 48 h.Each bar shows the mean±SEM of n=5 experiments. The effect ofS100B-neutralizing antibody (1:10,000–1:1,000 dilution v/v) onMPTP (100 μM)-induced C6 cell proliferation at 48 h is also shown.Each bar shows the mean±SEM of n=5 experiments.*P<0.05, ***P<0.001 vs control.°°P<0.01, °°°P<0.001 vs MPTP (100 μM)
Fig. 2 Effect of MPTP (1–100 μM) on C6 [Ca+2]i levels. [Ca+2]i
levels were measured at 60 min, i.e. at their peak and expressed as $increase in comparison to basal level. Each bar shows the mean±SEMof n=6 experiments. **P<0.05 vs control; ***P<0.001 vs control
1384 J Mol Med (2007) 85:1379–1392

Analysis of the pro-caspase/total caspase-3 ratio showedthat PC12 cells started to undergo to apoptosis 3 h after co-culture with the ‘conditioned medium,’ although a markedapoptosis was evident only 6 h after the treatment. Apoptosiswas counteracted by the anti-S100β antibody (1:1,000 v/vdilution), added to PC12 cells 15 min before the ‘conditionedmedium’ from MPTP-treated C6 cells (Fig. 4d,e).
Effect of ACEA and JWH015 on MPTP-induced S100Bprotein density in C6 rat glioma cells
The selective CB1 receptor agonist, ACEA (10−8−10−6 M)added to MPTP (100 μM)-treated C6 cells, concentration-
dependently reduced S100B protein density at 24 h. Bycontrast, the selective CB2 receptor agonist, JWH015(10−6 M), did not reverse the effect of MPTP (Fig. 5).
Effect of ACEA and JWH-015 on MPTP-induced S100Bprotein release in C6 rat glioma cells
When ACEA (10−8−10−6 M) was added to MPTP(100 μM)-treated C6 cells, it significantly and concentra-tion-dependently reduced S100B protein release in thecultured medium 24 h after treatment. By contrast, theselective CB2 receptor agonist, JWH015 (10−6 M), did notreverse the effect of MPTP (Fig. 6).
Fig. 4 a Time-dependent effect of MPTP-conditioned C6 cellmedium on PC12 [Ca+2]i levels in the presence or absence ofS100B-neutralizing antibody (1:1,000 dilution v/v). Each point showsthe mean±SEM of n=5 experiments. ***P<0.001 vs MPTP-condi-tioned C6 cell medium. b Effect of MPTP (1–100 μM)-conditionedC6 cell medium in the presence of S100B-neutralizing antibody(1:1,000 dilution v/v) given to PC12 cells on co-cultured PC12 cellviability. Each bar in panel b shows the mean±SEM of threeexperiments. *P<0.01 vs control; ***P<0.001 vs control. c Concen-tration dependent effect of S100B protein on PC12 cells viability. d
Western blot analysis showing the effect of the conditioned mediumfrom 24-h MPTP-treated C6 cells on caspase-3 activation in PC12cells, evaluated at 3 and 6 h, in the presence and absence of S100B-neutralizing antibody (1:1,000 dilution v/v). e Densitometric analysisof Pro-caspase-3/caspase-3 ratio of corresponding bands (opticaldensity). d is representative of n=3 separated experiments. Each barin e shows the mean±SEM of n=3 experiments. **P<0.05 vs control***P<0.001 vs control. °°°P<0.001 vs MPTP-conditioned C6 cellderiving medium
J Mol Med (2007) 85:1379–1392 1385

Effect of ACEA and JWH015 on MPTP-induced [Ca+2]ilevels in C6 rat glioma cells
ACEA (10−8−10−6 M) added to MPTP (100 μM)-treatedC6 cells significantly and concentration-dependently re-duced [Ca+2]i levels in the cells evaluated 60 min afterMPTP addition (Fig. 7), whereas under the same experi-mental conditions, JWH015 (10−6 M) did not show anyeffect (data not shown).
Effect of ACEA and JWH015 on MPTP-challenged C6cells and corresponding effect on PC12 cells co-culturedwith C6 cells
When PC12 cells were co-cultured for 24 h with MPTP(100 μM)-treated C6 cells, a significant and concentration-dependent reduction in cell viability was observed. Under thesame experimental conditions, ACEA (10−8−10−6 M) butnot JWH015 (10−8−10−6 M), given to C6 cells 15 minbefore MPTP, resulted in a significant and concentration-dependent inhibition of co-cultured PC12 cell death (Fig. 8).
Effect of MPTP on endocannabinoid levels in C6 ratglioma cells
Incubation with MPTP (100 μM) resulted in a significantand almost fourfold increase in AEA levels but not of thelevels of 2-AG or of other cannabimimetic fatty acidamides, such as palmitoylethanolamide (PEA), in C6 ratglioma cells (Fig. 9).
Effect of AEA, AA-5-HT and SR141716A on MPTP-induced S100B protein density in C6 cells
AEA and AA-5-HT (10−6 M), a selective inhibitor of AEAdegradation via fatty acid amide hydrolase added to MPTP(100 μM)-treated C6 cells, reduced S100B protein densityat 24 h. This effect was attenuated by the concomitanttreatment of MPTP-stimulated C6 cells with AEA plusSR141716A (10−6 M) or AA-5-HT plus SR141716A(10−6 M). Under the same experimental conditions,SR141716A (10−6 M) alone slightly, although significantly,increased MPTP (100 μM)-induced S100B protein density.
Fig. 7 Effect of ACEA and SR141716-A on MPTP induced [Ca+2]ilevels in C6 rat glioma cells. [Ca+2]i levels were measured at 60 min,i.e. at their peak and expressed as $% increase in comparison to basallevel. ACEA (10−8−10−6 M) and SR141716A (10−6M) were given15 min before MPTP (100 μM). Each bar shows the mean±SEM ofn=6 experiments. ***P<0.001 vs control; °°°P<0.001 vs MPTP. ###
°°°P<0.001 vs ACEA
Fig. 6 Effect of ACEA (10−8−10−6) and JWH-015 (10−6) on MPTP-induced S100B levels in C6 rat glioma cells medium. ELISA analysisof S100B protein levels at 24 h in MPTP (100 μM)-treated C6 cells inthe presence of ACEA (10−8−10−6 M) and JWH015 (10−6 M). Eachbar shows the mean±SEM of n=4 experiments. ***P<0.001 vscontrol. °°°P<0.001, °°P<0.05 vs MPTP
Fig. 5 Effect of ACEA, JWH015 and SR 141716-A onMPTP-inducedS100B protein expression in C6 rat glioma cells. a Western blotanalysis of S100B protein expression at 24 h in MPTP (100 μM)-treated C6 cells in the presence of ACEA (10−8−10−6 M), JWH015(10−6 M) and SR141716A (10−6 M). b Corresponding densitometricanalysis. Each bar shows the mean±SEM of n=4 experiments. ***P<0.001 vs control. °°°P<0.001, °°P<0.05 vs MPTP. ###P<0.001 vsACEA
1386 J Mol Med (2007) 85:1379–1392

However, the partial reversal of AEA and AA-5-HT effectsby SR141716A appeared to be higher than the effectexerted by SR141716A per se (Fig. 10a).
Effect of CB1 siRNA on MPTP-induced S100B density
As shown in Fig. 10d, both CB1 and CB2 receptors areexpressed in resting C6 cells. Western blot analysis showedthat in CB1 siRNA-treated C6 cells, the levels of MPTP(100 μM)-induced S100B protein were increased to ahigher extent than in non-treated C6 cells (Fig. 10d).
Effect of ACEA, AEA, AA-5-HT, SR141716Aand SR144528 on MPTP-induced C6 cell proliferation
MPTP (100 μM) increased C6 cell proliferation at 48 h.ACEA (10−8−10−6 M), AEA (10−8−10−6 M) and AA-5-HT(10−8−10−6 M) concentration-dependently reduced C6 cell
proliferation. SR141716A (10−7−10−6 M) co-administeredwith ACEA, AEA and AA5-HT to C6 cells 15 min beforeMPTP reversed their effects (Fig. 11a). Treatment withSR141716A (10−6 M) or ACEA (10−6 M) had no effect onC6 cell proliferation in the absence of MPTP (Fig. 11a).
Under the same experimental conditions, SR141716A(10−8−10−6 M) significantly and concentration-dependentlyincreased MPTP-induced C6 cell proliferation, whereasSR144528 (10−6 M) had no effect (Fig. 11b).
Effect of VDM-11 on MPTP-induced C6 cell proliferation
Experiments with an inhibitor of AEA transport across cellmembrane, VDM-11 (10−7−10−6 M), given to cells 30 minbefore MPTP (100 μM), significantly and concentration-dependently increased MPTP-induced C6 cell proliferation.Conversely, when VDM-11 (10−7−10−6 M) was given tothe cells 12 h after MPTP (100 μM), a significant reductionin MPTP-induced C6 cell proliferation was observed, andthis effect was reversed by SR141716A (10−7−10−6 M;Fig. 11c). VDM-11 had no effect on C6 cell proliferation inthe absence of MPTP (data not shown).
Effect of ACEA, AEA, AA-5-HT and SR141716A givento MPTP-treated C6 cell on co-cultured PC12 cells
When MPTP (100 μM)-treated C6 cells were extensivelywashed and placed in contact with PC12 cells for further24 h, this resulted in a significant and concentration-dependent reduction in PC12 cell viability. ACEA(10−7−10−6 M), AEA (10−7−10−6 M) and AA-5-HT(10−7−10−6 M), given to C6 cells 15 min before MPTP,increased co-cultured PC12 cell viability. SR141716A(10−6 M) co-administered with ACEA, AEA and AA-5-HTto C6 cells 15 min before MPTP abolished their effects(Fig. 12a). On the contrary, SR141716A (10−8−10−6 M)given alone significantly and concentration-dependentlydecreased PC12 co-cultured cell viability (Fig. 12b), whereasSR144528 (10−6 M) had no effect (data not shown).
Fig. 9 Effect of MPTP on endocannabinoid levels in C6 cells. Cellswere treated with MPTP (100 μM) for 24 h and endocannabinoid(AEA, 2-AG) and palmitoylethanolamide (PEA) levels, were analysed
by LC-APCI-MS. Each bar shows the mean±SEM of n=4 separateexperiments. *P<0.001 vs control
Fig. 8 Concentration dependent effect of ACEA and JWH-015 onPC12 cell viability co-cultured with C6 cells. ACEA and JWH-015(10−8−10−6M) were given to C6 cells 15 min before MPTP (100 μM),thereafter PC12 were co-cultured with C6 cells. Each bar shows themean±SEM of n=4 experiments. ***P<0.001 vs control; °°°P<0.001vs MPTP
J Mol Med (2007) 85:1379–1392 1387

Discussion
The results of the present study demonstrate that theneurotoxin MPTP is able to directly promote the densityand the release of the glial neurotrophin S100B in C6 ratglioma cells. This up-regulation was thereafter responsiblefor two opposite effects: the increased glial cell prolifera-tion and the extensive death of co-cultured PC12 neuronalcells. It is interesting to note that the neuronal injurybecause of MPTP exposure appeared closely related to theover-density and the increased release of S100B protein.Although the biochemical apparatus accounting for sucheffect remains to be fully clarified, it is reasonable toassume that the over-expression and release of S100B byreactive C6 cells plays a key role in the induction of PC12cell loss. The observation that a significant increase inintracellular Ca+2 levels in C6 cells was caused by exposureto MPTP allows us to suggest that this is one of themechanisms contributing to the increased density andrelease of S100B occurring after MPTP treatment. Asimilar increase in intracellular Ca+2 levels, with conse-quent activation of caspase-3 and reduction in PC12 cellviability, was also observed in PC12 cells exposed to the‘conditioned medium’ from C6 cells, suggesting thatreleased S100B promotes a pro-apoptotic process. Indeed,the specific S100B-blocking antibody was able to reverseCa+2 level increase, caspase-3 activation and neuronal cell
death, thus confirming the crucial role played by extracel-lular S100B under the present experimental conditions.
All the above reported findings suggest that S100B, inagreement with its dual nature, operates also under ourexperimental conditions in to two opposite ways: as anautocrine, pro-proliferative agent in C6 cells and as a paracrine,toxic agent for co-cultured PC12 cells.
We also found that a selective CB1 receptor agonist,ACEA, but not a selective CB2 receptor agonist, JWH-015,significantly inhibited intracellular Ca2+ levels in MPTP-treated C6 cells. This inhibition was accompanied by thereduction in both S100B protein density and the subsequentglial cell proliferation. As a consequence, stimulation ofCB1 receptors in C6 cells by ACEA also protected PC12cells from S100B-induced intracellular Ca2+ elevation, andthe subsequent caspase-3 release and apoptosis, which wereobserved when PC12 cells, were placed in contact with the‘conditioned medium’ from C6 cells.
Because it is well known that AEA synthesis is triggeredby increased intracellular Ca2+ levels, the role of thisendocannabinoid in a possible tonic regulation of S100Bdensity in C6 cells was also investigated. In these experi-ments, MPTP elevated AEA levels in parallel to theincrease in intracellular Ca2+ in C6 cells. It is interestingto note that MPTP-induced endocannabinoid synthesis wasselective for AEA and did not involve a cannabinoidreceptor-inactive AEA congener as PEA nor the other
Fig. 10 Effect of AEA and AA-5-HT in the presence or absence ofSR141716A and SR141716A alone on MPTP-induced S100B proteinexpression in C6 cells. a Western blot analysis of S100B protein at24 h. b Relative densitometric analysis. c Effect of silencing mRNA(siRNA) for CB1 receptor in C6 cells and d CB2 receptor expression
in C6 cells and Jurkat cells as control. e Effect of CB1 siRNA onMPTP-induced S100B density. f Relative densitometric analysis. Eachbar shows the mean±SEM of n=4 experiments. ***P<0.001 vscontrol; °°°P<0.001, °°P<0.01 and °P<0.05 vs MPTP
1388 J Mol Med (2007) 85:1379–1392

major endocannabinoid, 2-AG. This is in agreement withthe recent observation that increases in intracellular Ca2+
might not be sufficient alone and must be accompanied byactivation of phospholipase Cβ by metabotropic receptors,to cause 2-AG biosynthesis [30]. More importantly,elevation of AEA levels, either by administration ofexogenous AEA or by inhibition of AEA enzymatichydrolysis with AA-5-HT, caused here a CB1 receptor-mediated inhibition of MPTP-induced C6 cell proliferation.This effect was due again to inhibition of S100B density.Furthermore, experiments with VDM-11, a selective inhib-itor of AEA transport across the cell membrane, allowed tobetter understand the possible role played by endogenousAEA under the present experimental conditions. In fact,VDM-11 exerted opposite effects on MPTP-treated C6cells, depending on whether it was administered: simulta-
neously or after MPTP. In the latter case, it inhibitedMPTP-induced glial cell proliferation; however, whenVDM-11 was given concomitantly to MPTP, this resultedin a significant increase in glial cell proliferation. Therefore,because VDM-11 is known to inhibit both AEA release andre-uptake from cells [31], it seems likely that when thiscompound was given 12 h after MPTP (when AEA hadalready been synthesized and released from the cells), itinhibited AEA re-uptake and, subsequently, increasedextracellular AEA concentrations and CB1 activation. Inthis case, VDM-11 thus causes a very potent and significantinhibition of glial cell proliferation, similar to what wasseen with exogenous ACEA, AEA and AA-5-HT. Con-versely, when VDM-11 was given concomitantly to MPTP,it might have interfered with the release of newlysynthesized AEA from the cells, thereby reducing extracel-
Fig. 11 C6 cell proliferation at48 h. a Concentration-dependenteffect of ACEA, AEA and AA-5-HT (10−8−10−6 M) in thepresence or absence ofSR141716A (10−7−10−6 M) onMPTP (100 μM)-induced cellproliferation. Effect of ACEAand SR141716A (10−6 M) givenalone on C6 cell proliferation.Maximal concentration ofACEA, AEA and AA-5-HT(10−6 M) was used in the pres-ence of CB1 antagonist.b Effects of SR141716A andSR144528 (10−6 M) on MPTP(100 μM)-induced cell prolifer-ation. c Effect of VDM-11(10−7−10−6 M) given 30 minbefore MPTP or 12 h afterMPTP. Maximal concentrationof VDM-11 (10−6 M) was usedin the presence of CB1 antago-nist (10−7−10−6 M). Each barshows the mean±SEM of n=4experiments. ***P<0.001 vscontrol; °P<0.05, °°P<0.01,°°°P<0.001 vs MPTP; §P<0.05,§§P<0.01, §§§P<0.001 vsMPTP; #P<0.05, ##P<0.01,###P<0.001 vs MPTP. ##P<0.05and ###P<0.001 vs ACEA@@P<0.05 and @@@P<0.001vs AEA; §§P<0.05 and§§§P<0.001 vs AA-5-HT
J Mol Med (2007) 85:1379–1392 1389

lular AEA concentrations and CB1 receptor activation andfailing to control glial cell proliferation. Overall, these datasuggest that after MPTP exposure, C6 cells release not onlyS100B with an autocrine, pro-proliferative, action and aparacrine, pro-apoptotic, effect on neurons but also AEA,which counterbalances both S100B effects, via CB1
receptors. Therefore, AEA acts as an ‘on demand’ neuro-protective response to S100B over-density, similar to whatwas previously shown for kainate-induced neuronal excito-toxicity [32]. To strengthen this hypothesis, blockade ofCB1 receptors with SR141716A induced a pro-proliferativeeffect on MPTP-treated C6 cells and decreased viability ofPC12 cells co-cultured with MPTP-treated C6 cells. Thislatter finding was unlikely due to the inverse agonistproperties of SR141716A because the compound exertedno effects on C6 cells when they were not treated with
MPTP. Therefore, these data, together with our observationof increased AEA levels after MPTP exposure, stronglysuggest the existence of an AEA tonic inhibitory action onMPTP-induced S100B over-expression. This result wasfurther supported by our findings with silenced CB1
receptors in C6 cells because under these conditions, wefound an increase in MPTP-induced S100B significantlyhigher than in non-transfected C6 cells.
The results of the present study allows to suggest alsothat CB1 activation, by suppressing S100B density in glialcells, might afford a dual ‘rebound’ neuroprotection throughthe inhibition of both glial cell proliferation and S100B-induced neurotoxicity. On the basis of these results, it ispossible to assume that the tonic, negative control played byAEA and CB1 receptor activation on S100B protein densityultimately down-regulates also reactive gliosis. Intriguingly,
Fig. 12 Effect of ACEA, AEA,AA-5-HT and SR141716A giv-en to MPTP-treated C6 cell onco-cultured PC12 cell viability.a Concentration-dependenteffects of ACEA, AEA and AA-5-HT in the presence or absenceof SR141716A. Maximal con-centrations of ACEA, AEA andAA-5-HT (10−6 M) were used inthe presence of the CB1 antago-nist. b Concentration-dependenteffect of SR141716A. Each barshows the mean±SEM of n=3experiments. °°°P<0.001 vscontrol; *P<0.05, **P<0.01,***P<0.001 vs MPTP
1390 J Mol Med (2007) 85:1379–1392

S100B protein density and CB1 receptor activation seem toregulate cell activity in an opposite ways. Whilst S100Bleads to Gs protein activation, intracellular cyclic adenosinemonophosphate (cAMP) elevation and increased Ca2+
levels in glial and neuronal cells [29], CB1 receptoractivation is coupled to Gi protein activation, decreasedintracellular cAMP and inhibition of Ca2+ entry into thecells via voltage-activated Ca2+ channels in culturedneurons [33]. Therefore, it is possible that CB1 activationmight also counteract S100B neurotoxic signalling inneurons and not only its production by glial cells.
In conclusion, the above reported results point to theautocrine (pro-gliotic) and paracrine (neurotoxic) effects ofS100B as a new possible mechanism contributing toMPTP-induced neurotoxicity (Scheme 2). In this context,CB1 receptor activation by both exogenous and endogenouscannabinoids may be regarded as a putative candidate forinhibition of S100B over-production and hence as anendogenous control system over MPTP-dependent gliosisand neuronal loss. Non-psychotropic inhibitors of endocan-nabinoid metabolism, such as VDM11 and AA-5-HT, mayrepresent, by this way, a new tool to attenuate MPTP-
induced neurotoxicity and other neuropathological condi-tions where S100B plays a major role.
References
1. Richardson JR, Caudle WM, Wang M, Dean ED, Pennell KD,Miller GW (2000) Developmental exposure to the pesticidedieldrin alters the dopamine system and increases neurotoxicityin an animal model of Parkinson’s disease. FASEB J 20(10):1695–1697, Aug
2. Kil IS, Park JW (2005) Regulation of mitochondrial NADP+-dependent isocitrate dehydrogenase activity by glutathionylation.J Biol Chem 280(11):10846–10854, Mar 18
3. Russ H, Staust K, Martel F, Gliese M, Schomig E (1996) Theextraneuronal transporter for monoamine transmitters exists in cellsderived from human central nervous system glia. Eur J Neurosci8:1256–1264
4. Tripanichkul W, Sripanichkulchai K, Finkelstein DI (2006)Estrogen down-regulates glial activation in male mice following1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine intoxication. BrainRes 1084:28–37
5. Liberatore GT, Jackson-Lewis V, Vukosavic S, Mandir AS, VilaM, McAuliffe WG, Dawson VL, Dawson TM, Przedborski S(2005) Inducible nitric oxide synthase stimulates dopaminergic
Scheme 2 Anandamide and CB1 receptors as an endogenous ‘ondemand’ neuroprotective response against S100B-induced neuronaltoxicity and gliosis. Possible scenario for the neuroprotection inducedby endogenous anandamide (AEA) against the neurotoxic effects ofglial cell-derived S100B. Stimulation of glial cells with MPTP causeselevation of intracellular Ca2+, which in turns triggers S100B densityand AEA formation. S100B is then released by glial cells andstimulates their proliferation while inducing elevation of intracellularCa2+, capsase-3 activation and apoptosis in neighbouring neurons.AEA acts on CB1 receptors in glial cells to suppress S100B density.
Inhibitors of the intracellular hydrolysis of AEA to arachidonic acid(AA) and ethanolamine (EtNH2) by fatty acid amide hydrolase(FAAH), such as arachidonoylserotonin (AA-5-HT), potentiate theCB1-mediated neuroprotective action of AEA. Inhibitors of AEArelease/re-uptake, such as VDM-11, exert opposing actions on AEAstimulation of CB1 receptors and subsequent neuroprotective effects,depending on whether they are administered to glial cells concomi-tantly or after MPTP. Finally, blockage of CB1 receptors by electiveantagonists enhances the pro-proliferative (on glial cells) and toxic (onneurons) effects of S100B
J Mol Med (2007) 85:1379–1392 1391

neurodegeneration in the MPTP model of Parkinson disease. NatMed 5:1403–1409
6. Wu DC, Jackson-Lewis V, Vila M, Tieu K, Teismann P, VadsethC, Choi DK, Ischiropoulos H, Przedborski S (2005) Blockade ofmicroglial activation is neuroprotective in the 1-methyl-4-phenyl-1,2,3,6-tetrahydropyridine mouse model of Parkinsondisease. J Neurosci 22:1763–1771
7. Kurkowska-Jastrzebska I, Wronska A, Kohutnicka M, CzlonkowskiA, Czlonkowska A (1999) The inflammatory reaction following1-methyl-4-phenyl-1,2,3, 6-tetrahydropyridine intoxication inmouse. Exp Neurol 156(1):50–61
8. Van Eldik LJ, Christie-Pope B, Bolin LM, Shooter EM, WhetsellWO Jr (1991) Neurotrophic activity of S100-beta in cultures ofdorsal root ganglia from embryonic chick and fetal rat. Brain Res542:280–285
9. Kleindienst A, Ross BullockM (2006) A critical analysis of the roleof the neurotrophic protein S100B in acute brain injury. J Neuro-trauma 23(11):85–200
10. Hu J, Ferreira A, van Eldik L (1997) S100b induces neuronaldeath through nitric oxide release from astrocytes. J Neurochem69:2294–22301
11. Griffin WST, Stanley LC, Ling C, White L, MacLeod V, PerrotLJ, White CL III, Araoz C (1989) Brain interleukin-1 and S100immunoreactivity are elevated in Down Syndrome and AlzheimerDisease. Proc Natl Acad Sci USA 86:7611–7615
12. Muramatsu Y, Kurosaki R, Watanabe H, Michimata M, MatsubaraM, Imai Y, Araki T (2003) Density of S100 protein is related toneuronal damage in MPTP treated mice. Glia 42:307–313
13. Marsicano G, Moosmann B, Hermann H, Lutz B, Behl C (2002)Neuroprotective properties of cannabinoids against oxidativestress: role of the cannabinoid receptor CB1. J Neurochem 80:448–456
14. Panikashvili D, Simeonidou C, Ben-Shabat S, Hanus L, BreuerA, Mechoulam R, Shohami E (2001) An endogenous cannabi-noid (2-AG) is neuroprotective after brain injury. Nature 413:527–531
15. Walter L, Stella N (2004) Cannabinoids and neuroinflammation.Br J Pharmacol 141(5):775–785, Mar
16. Condorelli DF, Dell’Albani P, Amico C, Kaczmarek L, NicolettiF, Lukasiuk K, Stella AM (1993) Induction of primary responsegenes by excitatory amino acid receptor agonists in primaryastroglial cultures. J Neurochem 60:877–885 Links
17. Franklin A, Parmentier-Batteur S, Walter L, Greenberg DA, StellaN (1997) Palmitoylethanolamide increases after focal cerebralischemia and potentiates microglial cell motility. J Neurosci23:7767–7775
18. BeltramoM, Stella N, CalignanoA, Lin SY,Makriyannis A, PiomelliD (1997) Functional role of high-affinity anandamide transport, asrevealed by selective inhibition. Science 277:1094–1097
19. Di Marzo V, Bisogno T, De Petrocellis L (2000) Endocannabinoids:new targets for drug development. Curr Pharm Des 6:1361–1380
20. Bisogno T, Ligresti A, Marzo V (2005) The endocannabinoidsignalling system: biochemical aspects. Pharmacol BiochemBehav 81:224–238
21. Bisogno T, Melck D, De Petrocellis L, Bobrov MY, GretskayaNM, Bezuglov VV, Sitachitta N, Gerwick WH, Marzo V(1998) Arachidonoylserotonin and other novel inhibitors of fattyacid amide hydrolase. Biochem Biophys Res Commun 248:515–522
22. De Petrocellis L, Melck D, Bisogno T, Marzo V (2000)Endocannabinoids and fatty acid amides in cancer, inflammationand related disorders. Chem Phys Lipids 108:191–209
23. Nair VD, McNaught KS, Gonzalez-Maeso J, Sealfon SC, OlanowCW (2006) p53 mediates nontranscriptional cell death indopaminergic cells in response to proteasome inhibition. J BiolChem 281:39550–39560
24. Jeon HJ, Lee DH, Kang MS, Lee MO, Jung KM, Jung SY,Kim DK (2005) Dopamine release in PC12 cells is mediatedby Ca(2+)-dependent production of ceramide via sphingomyelinpathway. J Neurochem 95:811–820
25. Koh SH, Kwon H, Park KH, Ko JK, Kim JH, Hwang MS, YumYN, Kim OH, Kim J, Kim HT, Do BR, Kim KS, Kim H, Roh H,Yu HJ, Jung HK, Kim SH (2005) Protective effect of diallyldisulfide on oxidative stress-injured neuronally differentiatedPC12 cells. Brain Res Mol Brain Res 133:176–186
26. Esposito G, Izzo AA, Di Rosa M, Iuvone T (2001) Selectivecannabinoid CB1 receptor-mediated inhibition of inducible nitricoxide synthase protein density in C6 rat glioma cells. J Neuro-chem 78:835–841
27. Grynkiewicz G, Poenie M, Tsien RY (1985) A new generationof Ca2+ indicators with greatly improved fluorescence proper-ties. J Biol Chem 25(260):3440–3450
28. Marsicano G, Moosmann B, Hermann H, Lutz B, Behl C (2002)Neuroprotective properties of cannabinoids against oxidative stress:role of the cannabinoid receptor CB1. J Neurochem 80:448–456
29. Barger SW, Van Eldik LJ (1992) S100beta stimulates calciumfluxes in glial and neuronal cells. J Biol Chem 267:9689–9694
30. Hashimotodani Y, Ohno-Shosaku T, Tsubokawa H, Ogata H,Emoto K, Maejima T, Araishi K, Shin HS, Kano M (2005)Phospholipase Cbeta serves as a coincidence detector through itsCa2+ dependency for triggering retrograde endocannabinoidsignal. Neuron 45:257–268
31. Ligresti A, Morera E, Van Der Stelt M, Monory K, Lutz B, OrtarG, Di Marzo V (2004) Further evidence for the existence of aspecific process for the membrane transport of anandamide.Biochem J 380:265–272
32. Marsicano G, Goodenough S, Monory K (2003) CB1 cannabinoidreceptors and on-demand defense against excitotoxicity. Science302:84–88
33. Twitchell W, Brown S, Mackie K (1997) Cannabinoids inhibit N-and P/Q-type calcium channels in cultured rat hippocampalneurons. J Neurophysiol 78:43–50
1392 J Mol Med (2007) 85:1379–1392

ORIGINAL ARTICLE
Effects of transcription factor activator protein-1on interleukin-8 expression and enteritis in responseto Clostridium difficile toxin A
Jin Young Lee & Hye Ri Park & Yu-Kyoung Oh &
Yeong-Jeon Kim & Jeehee Youn & Joong-Soo Han &
Jung Mogg Kim
Received: 1 February 2007 /Revised: 1 June 2007 /Accepted: 12 June 2007 / Published online: 18 July 2007# Springer-Verlag 2007
Abstract Clostridium difficile toxin A causes acute colitisassociated with intense infiltration of neutrophils. AlthoughC. difficile toxin A is known to induce nuclear factor-kappaB-mediated chemokine expression in intestinal epi-thelial cells, little is known about its effect on the regulationof activator protein-1 (AP-1) by mitogen-activated proteinkinase (MAPK). In the present study, we investigatedwhether the MAPK and AP-1 signaling pathway isinvolved in interleukin (IL)-8 expression and entericinflammation in response to stimulation with toxin A.
Toxin A activated MAPK and AP-1 composed of c-Jun/c-Fos heterodimers in primary intestinal epithelial cells andHT-29 cell lines. Transfection with mutant genes for Ras,c-Jun, p38, or c-Jun N-terminal kinase (JNK) significantlyinhibited C. difficile toxin A-induced activation of AP-1and expression of IL-8 in HT-29 cell lines. Furthermore, thep38 inhibitor SB203580 attenuated toxin A-induced in-flammation in vivo in the mouse ileum, evidenced by a
J Mol Med (2007) 85:1393–1404DOI 10.1007/s00109-007-0237-7
J. Y. Lee :H. R. Park : J. M. KimDepartment of Microbiology and Institute of Biomedical Science,Hanyang University College of Medicine,Seoul 133-791, South Korea
Y.-K. OhSchool of Life Sciences and Biotechnology, Korea University,Seoul 136-701, South Korea
Y.-J. KimDepartment of Biotechnology, Joongbu University,Choongnam 312-940, South Korea
J. YounDepartment of Anatomy and Cell Biology,Hanyang University College of Medicine,Seoul 133-791, South Korea
J.-S. HanDepartment of Biochemistry and Molecular Biology,Hanyang University College of Medicine,Seoul 133-791, South Korea
J. M. Kim (*)Department of Microbiology,Hanyang University College of Medicine,17 Haengdang-dong, Sungdong-gu,Seoul 133-791, South Koreae-mail: [email protected]
JIN YOUNG LEE
received her M.S. fromHanyang University College ofMedicine in Seoul, Republic ofKorea. She is presently astudent of Ph.D. course atDepartment of Microbiology,Hanyang University College ofMedicine. Her research inter-ests include host responses toC. difficile toxin.
JUNG MOGG KIM
received his M.D. and Ph.D. inMicrobiology and Immunologyfrom Hanyang UniversityCollege of Medicine in Seoul,Republic of Korea. He workedas a research scientist at Labo-ratory of Mucosal Immunologyof University of California, SanDiego, USA. He is presently aProfessor and Chief of Depart-ment of Microbiology, HanyangUniversity College of Medicine.His research interests includemucosal immunology and host–parasite relationship.

significant decrease in neutrophil infiltration, villous de-struction, and mucosal congestion. Our results suggest thatthe Ras/MAPK cascade acts as the upstream signaling forAP-1 activation and IL-8 expression in toxin A-stimulatedintestinal epithelial cells and may be involved in thedevelopment of enteritis after infection with toxin A-producing C. difficile.
Keywords Activatorprotein-1 .Clostridium difficile toxin A .
Interleukin-8 . Epithelial cells . Mitogen-activatedprotein kinase
Introduction
Clostridium difficile causes antibiotic-associated diarrheaand pseudomembranous colitis in humans. These manifes-tations are mainly caused by two exotoxins, toxin A(308 kDa) and toxin B (269 kDa), produced by pathogenicstrains of C. difficile [1]. In animal models, toxin A causesfluid secretion, mucosal edema, and villous disruptionthrough the induction of massive acute inflammation withneutrophil infiltration [1, 2]. As the first host cells that C.difficile toxins interact with are epithelial cells in the colon[3], it has been proposed that mucosal inflammatory signalsmay be initiated from intestinal epithelial cells. Workingfrom this hypothesis, several reports have demonstrated thatintestinal epithelial cells can produce chemokines, includinginterleukin (IL)-8, growth-related oncogene-α, and mono-cyte chemotactic protein-1, in response to C. difficile toxinA [4–7]. However, the pathogenic mechanism of toxin A-induced inflammation has not been fully investigated.
Mucosal inflammation is mediated by chemokines thattrigger proinflammatory signals. Toxigenic C. difficile-infected colitis is accompanied by a massive infiltration ofneutrophils into the mucosa [1]. CXC chemokines, charac-terized by two cysteine residues separated by any otheramino acid, seem to play important roles in mobilizinginflammatory cells to areas of immune challenge [8], andIL-8 is a CXC chemokine that plays a role in recruiting andactivating neutrophils in the intestinal mucosa. This processis primarily controlled at the transcriptional level, andbinding sites for the inducible transcription factors, such asnuclear factor-kappaB (NF-κB) and activator protein-1(AP-1), are present in the promoter region of the IL-8 gene[9]. Although the importance of NF-κB in toxin A-inducedchemokine production is apparent [7, 10, 11], it remainsunclear how toxin A activates transcription factor AP-1 andinduces chemokine expression.
Mitogen-activated protein kinases (MAPKs) comprise animportant group of serine- and threonine-signaling kinasesthat transduce a variety of extracellular stimuli through acascade of protein phosphorylation, leading to the activation
of transcription factors [12–14]. Three groups of MAPKshave been identified in mammalian cells: (1) p42 and p44extracellular signal-regulated kinase (ERK), (2) p38 MAPKwith α, β, γ, and δ isoforms, and (3) p46 and p54 c-JunNH2-terminal kinase (JNK) or stress-activated proteinkinase with multiple subisoforms. All of these signalingcascades have been shown to regulate AP-1 activity and areimplicated in the control of IL-8 transcription [15].Activation of Ras is known to result in activation of theRas/Raf/MAPK cascade [16]. As activation of the Ras–Rafpathway increases the activity of transcription factors suchas c-Jun, an important component of AP-1 [17], it seemslikely that the Ras/MAPK cascade is involved in AP-1activation. Although several studies revealed that C. difficiletoxin A activates MAPK signaling in monocytes [18] andcolonocytes [19, 20], the signaling pathway in intestinalepithelial cells stimulated with C. difficile toxin A has notyet been elucidated. In the present study, we investigated therole of toxin A-induced MAPK pathways in mucosalinflammation. Our results indicate that a signaling pathwayinvolving Ras, MAPK, and AP-1 plays an important role intoxin A-induced IL-8 expression in intestinal epithelial cellsand the development of enteritis in vivo.
Materials and methods
Cell culture
HT-29 human colon epithelial cells (ATCC HTB 38)were grown in DMEM (pH 7.4, Sigma Chemical, St.Louis, MO, USA) supplemented with 10% fetal bovineserum (FBS, Gibco BRL, Grand Island, NY, USA),2 mM L-glutamine, 25 mM N-2-hydroxyethylpiperazine-N′-2-ethanesulfonic acid (HEPES), and antibiotics (100 unit/ml of penicillin and 100 μg/ml of streptomycin), asdescribed previously [21]. Human colon epithelial cellswere obtained from normal-appearing mucosa of surgicallyresected colons from individuals with colon cancer, asdescribed previously [22, 23]. Freshly isolated colonepithelial cells were cultured in 2×106/ml in Roswell ParkMemorial Institute-1640 media supplemented with 10%FBS, 2 mM L-glutamine, and antibiotics (100 unit/ml ofpenicillin and 100 μg/ml of streptomycin). Epithelial cellpreparations contained less than 5% contamination with Bcells and monocytes/macrophages, as assessed by flowcytometry using CD19/20 and CD14 as markers.
Purification of C. difficile toxin A
C. difficile toxin A was purified from a toxigenic strain(ATCC 9689) as described previously [4, 6]. Briefly,toxigenic C. difficile was cultured anaerobically at 37°C
1394 J Mol Med (2007) 85:1393–1404

in dialysis tubing, and culture filtrates were applied to athyroglobulin affinity column. Fractions showing cytotox-icity (assessed by the rounding of Vero cells) andhemagglutinating activity (determined using a 1% rabbiterythrocyte suspension) were subsequently subjected totwo sequential anion exchange chromatographic steps withQ Sepharose FF and Mono Q columns (PharmaciaBiotech, Brussels, Belgium) incorporated into a fastprotein liquid chromatography apparatus (Pharmacia Bio-tech). Finally, the purity of toxin A was monitored using acommercial monoclonal enzyme-linked immunosorbentassay (ELISA) kit for toxin A of C. difficile (TechLab C.difficile TOX A/B ELISA test kit, Blacksburg, VA, USA).To confirm the absence of contaminating toxin B, weperformed ELISA for toxin B using the TechLab C.difficile TOX A/B ELISA test kit. In addition, cytotoxicactivity against HT-29 cells was completely neutralizedwith specific anti-toxin A antibody. Buffers were preparedusing lipopolysaccharide (LPS)-free water (Baxter Health-care, Deerfield, IL, USA), and LPS activity in 1 mg/mltoxin A solutions was less than one endotoxin unit/ml(quantitative chromogenic limulus amebocyte lysate; Bio-Whittaker, Walkersville, MD, USA). Aliquots of purifiedtoxin A at concentrations of 50 to 100 μg/ml were storedat −70°C until used.
Immunoblot analyses
Confluent monolayers in six-well plates were washed withice-cold phosphate-buffered saline (PBS) and lysed in0.5 ml/well lysis buffer (150 mM NaCl, 20 mM Tris,pH 7.5, 0.1% Triton X-100, 1 mM phenylmethanesulfonylfluoride, 10 μg/ml aprotinin) as described previously [22].Protein concentrations in the lysates were determined bythe Bradford assay (Bio-Rad, Hercules, CA, USA). Fifteento 50 μg protein/lane was size-fractionated on 6% poly-acrylamide minigels (Mini-PROTEIN II; Bio-Rad) andelectrophoretically transferred to a nitrocellulose membrane(0.1-μm pore size). Specific proteins were identified withpolyclonal antibodies for pan-ERK1/2 (p44/p42), phospho-ERK1/2, pan-JNK (p54/p46), phospho-JNK, pan-p38, andphospho-p38 (all from Cell Signaling Technology, Bervery,MA, USA; Catalog # 9102, 9101, 9252, 9251, 9212, and9212, respectively). The immunoreactive proteins werevisualized using goat anti-rabbit secondary antibodiesconjugated to horseradish peroxidase (Transduction Labo-ratories, Lexington, KY, USA), followed by enhancedchemiluminescence (ECL system; Amersham Life Science,Buckinghamshire, England) and exposure to X-ray film(XAR5; Eastman Kodak Company, Rochester, NY, USA).
Ras pull-down assay was performed as described accord-ing to the manufacturer’s protocol (Upstate Biotechnology,Lake Placid, NY, USA). Briefly, toxin A-stimulated cells
were lysed in 2% Triton X-100, 100 mM HEPES, pH 7.5,200mMNaCl, 10 mMMgCl2, 2 mM sodium orthovanadate,1:50 (v/v) mammalian cell protease inhibitor mixture, andcleared by centrifugation at 15,000×g for 2 min at 4°C. Theremainder of the lysates was incubated for 90 min at 4°Cwith beads coated with a fusion protein (glutathione-S-transferase [GST]–Raf-1 rhotekin Rho-binding domain)consisting of GST fused to the Ras-binding domain of Raf-1(Upstate Biotechnology). Beads were washed three timeswith cold PBS, 5 mM MgCl2, and 0.1% Triton X-100, andbound protein was eluted for 15 min with 2× Laemmlisample buffer that had been preheated to 95°C. The activeRas was determined by immunobloting with an ant-Rasantibody (clone RAS10, Upstate Biotechnology) accordingto the manufacturer’s protocol.
Reverse transcription-PCR analysis and ELISA
Total cellular RNAwas extracted using an acid guanidinium–phenol–chloroformmethod (Trizol; Gibco BRL, Gaithersburg,MD, USA). Quantitative reverse transcription-polymerasechain reaction (RT-PCR) using an internal standard was usedto quantify chemokine messenger RNA (mRNA) levels, asdescribed previously [6]. Synthetic standard RNAs wereprovided by Dr. Kagnoff at the University of California,San Diego. PCR amplification consisted of 35 cycles of1 min denaturation at 95°C and 2.5 min annealing andextension at either 60°C (IL-8) or 72°C (β-actin).
ELISA was performed in triplicate on chemokines inculture supernatants and tissue extracts. Ileal loops wereobtained after toxin A challenge and homogenized with 0.3 mlPBS containing complete protease inhibitor mixture (Roche,Tokyo, Japan). Homogenates were centrifuged at 12,000×gfor 15 min, and the supernatants were filtered through a0.22-μm filter to remove any contaminants. The concentra-tion of human IL-8 and mouse macrophage-inflammatoryprotein (MIP)-2 was determined using Quantikine immuno-assay kits (R&D Systems, Minneapolis, MN, USA).
Electrophoretic mobility shift assay
Nuclear extracts were prepared from cells as previouslydescribed [22], and protein concentrations were determinedusing the Bradford assay (Bio-Rad). Electrophoretic mobil-ity shift assay (EMSA) for AP-1 was performed accordingto the manufacturer’s protocol (Promega, Madison, WI,USA). In brief, 5 μg nuclear extract was incubated for30 min at room temperature with a γ32P-labeled oligonu-cleotide probe (5′-CGC TTG ATG ACT CAG CCG GAA-3′) corresponding to an AP-1 binding site. After incubation,bound and free DNA was resolved on 5% native polyacryl-amide gels, as described previously [22]. For competition
J Mol Med (2007) 85:1393–1404 1395

assays, nuclear extracts were pre-incubated with AP-1oligomer, AP-1 oligomer mutant (5′-CGC TTG ATG ACTTGG CCG GAA-3′), or NF-κB oligomer (5′-AGT TGAGGG GAC TTT CCC AGG C-3′) for 1 h at 4°C. Forsupershift assays, nuclear extracts were incubated for 1 h at4°C with rabbit antibodies (1 μg/reaction) against c-Jun,c-Fos, Jun-B, Jun-D, or Fos-B (Santa Cruz Biotechnology,Santa Cruz, CA, USA) before incubation with the radio-labeled probe.
Plasmids and transfection
TAM-67 is a dominant-negative c-Jun superrepressor thatlacks the transactivation domain of c-Jun and is a potentinhibitor of AP-1-mediated transactivation [24]. TAM-67dimerizes with c-Jun or c-Fos family members and bindsDNA, resulting in the inhibition of wild-type c-Jun andc-Fos function. The TAM-67 used in the present study was agift from Dr. Andreas von Knethen at University ofErlangen, Erlangen, Germany. N-17 is a dominant-negativeRas superrepressor containing an inhibitory Ser17Argsubstitution that is present in c-Ha-ras [25]. N-17 wasprovided by Dr. Hyeyoung Kim at Yonsei University, Seoul,Korea [26]. As a control, pcDNA3 (Invitrogen, Carlsbad,CA, USA) was transfected into cells instead of the c-Jun orRas mutant genes. Recombinant adenoviruses containingdominant-negative p38α (ADV-105), and dominant-negativeJNK1 expression vectors were obtained from Cell Biolabs(San Diego, CA, USA). In the dominant-negative p38αplasmid, the TGY dual phosphorylation site has been changedto angioblastic growth factor, and in the dominant-negativeJNK1 plasmid, the dual phosphorylation site T183/Y185 hasbeen changed to A183/F185. The pIL8-luciferase, pβ-actin-luciferase, and pRSV-β-galactosidase transcriptional report-ers were provided by Dr. Kagnoff at the University ofCalifornia, San Diego [27]. The reporter plasmid containingAP-1-luciferase was purchased from BD Sciences (FranklinLakes, NJ, USA).
Cells in six-well dishes were transfected with 1.5 μgplasmid DNA using Fugene 6 (Roche, Mannheim, Ger-many), according to the manufacturer’s instructions [23], andthe transfected cells were incubated for 48 h at 37°C in a 5%CO2 incubator. Cells were then incubated with toxin A,harvested, and whole cell lysates were prepared as describedpreviously [23]. Briefly, cells were lysed at 4°C for 25 minin whole cell lysis buffer (0.1 M KPO4, 0.1 M DTT, 0.5%Triton X-100, pH 7.8). Luciferase activity was determinedand normalized relative to β-galactosidase expressionaccording to with the manufacturer’s instructions (Tropix,Bedford, MA, USA). Light release was quantitated for 10 susing a luminometer (MicroLumat Plus, Berthold, BadWildbad, Germany). β-galactosidase activity was deter-mined using the chemiluminescent substrate AMPGD (3-
(4-methoxyspiro[1,2-dioxetane-3,2′- tricylo[3.3.1.1]decan]-4-yl)phenyl-β-D-galactopyranoside; Tropix) as describedpreviously [23]. Light release was induced by the additionof 50 μl 0.2 N NaOH containing 10% Emerald enhancer(Tropix), and quantitated for 10 s in a luminometer. Non-transfected cells were used as a background control.
Small interfering RNA (siRNA) against c-Jun andnonsilencing siRNA were purchased from DharmaconResearch (Lafayette, CO, USA). Briefly, HT-29 cells werecultured in six-well plates to 50 to 80% confluence. Thecells were then transfected with Jun-specific silencingsiRNA using Fugene 6 (Roche) as transfection reagent,following the manufacturer’s instructions. Transfectionswere incubated for 48 h before assay.
Effect of p38 inhibitor SB203580 on C. difficile toxinA-induced enteritis in mice
Fasted (16 h)-specific pathogen-free mice (20–25 g,C57BL6Cr; Orient Experimental Animal, Kyounggi-do,Korea) were anesthetized by intraperitoneal injection ofsodium pentobarbital (600 μg/mouse). Ileal loops (3–4 cm)were prepared and injected with a 200-μl buffer or p38inhibitor SB203580-hydrochloride (100 μg in water, Sig-ma) as described previously [22, 23]. After 30 min, C.difficile toxin A (5 μg in PBS) was injected into the loops,and animals were killed 4 h later by pentobarbital overdose.One loop in each mouse was used in this experiment. Allprocedures of animal study were approved by the AnimalCare Committee of Hanyang University College of Medi-cine. Loops were excised weighed, and the length wasmeasured. Ileal tissue samples were fixed in formalin,paraffin embedded, and stained with hematoxylin andeosin. Tissue sections were examined by a gastrointestinalpathologist who was blinded to the study conditions andscored using the system described by Pothoulakis et al. [28]in which the severity of enteritis was graded based on thefollowing parameters: (a) epithelial damage, (b) mucosalcongestion and edema, and (c) neutrophil infiltration, with ascore of 0–3, denoting increasingly severe abnormality,assigned to each parameter. To assess AP-1 activity inmouse tissue, we used a TransAM™ AP-1 family kit(Active Motif, Carlsbad, CA, USA). Briefly, nuclearproteins from tissue extracts were obtained by using theNuclear Extract Kit (Active Motif) according to themanufacturer’s instruction. The total protein concentrationof the extracts was determined by Bradford assay. Theactivation of c-Jun was measured using the TransAM™AP-1 family kit (Active Motif) according to the manufac-turer’s instruction in which the method measures the DNA-binding activity of AP-1 by ELISA. Specific binding wasdetected by colorimetric estimation at 450 nmwith a referencewavelength of 655 nm. As a positive control for AP-1
1396 J Mol Med (2007) 85:1393–1404

activation, the K-562 (tetradecanoylphorbol-13-acetate [TPA]stimulated) nuclear extract provided with the kit was used.
Statistical analyses
Data are presented as mean±standard deviation (SD) forquantitative RT-PCR and mean±standard error of the means(SEM) for ELISA and luciferase assay. Wilcoxon’s ranksum test was used for statistical analysis. Mann–Whitney Utest was used for intergroup comparisons.
Results
C. difficile toxin A activates c-Jun/c-Fos heterodimericAP-1 DNA binding activity in human colon epithelial cells
To determine whether C. difficile toxin A activates AP-1signals in human colon epithelial cells, DNA-binding
studies were performed using nuclear extracts from cellsafter treatment with toxin A. Stimulation of HT-29 colonepithelial cell line or primary intestinal epithelial cells withtoxin A increased DNA binding activity of AP-1 (Fig. 1aand d). Binding specificity was confirmed by a competitionassay with cold probes: The addition of an AP-1 oligomerto nuclear extracts after stimulation with toxin A for 1 hsuppressed the AP-1 signal, whereas the addition of an AP-1 mutant oligomer or an NF-κB oligomer had no effect onbinding (Fig. 1b). A supershift assay was then performed toidentify the specific AP-1 subunits that comprise the AP-1signal detected in toxin A-stimulated cells. As shown inFig. 1c, AP-1 binding was inhibited by antibodies to c-Junand c-Fos. However, the addition of antibodies to Jun-B,Jun-D, or Fos-B did not affect AP-1 binding activityinduced by toxin A. Similar results were also observed inprimary human colon epithelial cells (Fig 1e). These resultsindicate that toxin A can activate DNA-binding activity ofAP-1, composed of c-Jun/c-Fos heterodimers.
a
AP-1 in HT-29
(+) (-) 0 10 30 60 120 240
Time after stimulation (min)
c
Toxin
A a
lone
Anti-c
-Jun
+ Toxin A
Anti-c
-Fos
Anti-J
un-B
Anti-J
un-D
Anti-F
os-B
AP-1
Toxin
A a
lone
Anti-c
-Jun
+ Toxin A
Anti-c
-Fos
Anti-J
un-B
Anti-J
un-D
Anti-F
os-B
b
Contr
ol
AP
-1
olig
om
er
Muta
nt A
P-1
olig
om
er
NF
-κB
olig
om
er
+ Toxin A
Toxin
A a
lone
AP-1 in
primary cells
d
Fig. 1 C. difficile toxin A acti-vates AP-1 DNA binding incolon epithelial cells. a HT-29cell lines (above) and primaryhuman colon epithelial cells(below) were stimulated withC. difficile toxin A (20 ng/ml)for the indicated periods of time.AP-1 DNA-binding activity wasassessed by EMSA. b Competi-tion assay for AP-1 specificitywas performed by addition ofeach oligomer to nuclearextracts of HT-29 cells. c and dSupershift assays were per-formed using antibodies toc-Jun, c-Fos, Jun-B, Jun-D, andFos-B and nuclear extracts fromHT-29 cells (c) or primary hu-man colon epithelial cells (d)stimulated with toxin A for 1 h.Results are representative of fiveindependent experiments
J Mol Med (2007) 85:1393–1404 1397

Luciferase activity in the HT-29 cells transfected withAP-1 promoter plasmid correlated with the concentration oftoxin A: 1 h after stimulation with 0.1, 1, 10, 50, and100 ng/ml concentrations of toxin A, the reporter geneactivity of the AP-1 construct increased 1.1±0.3, 2.8±0.6,8.3±0.9, 7.2±1.4, and 5.4±0.7-fold respectively, relative tounstimulated controls (mean value, n=3).
Having shown that toxin A activated c-Jun/c-Fosheterodimeric AP-1 in human colon epithelial cells, wenext investigated whether this AP-1 activation is associatedwith increased IL-8 expression. Transfection with c-Junsuperrepressor completely suppressed the AP-1 DNAbinding in HT-29 cells stimulated with toxin A, whereastransfection with control plasmid had no effect on binding(Fig. 2a). Treatment with toxin A also stimulated produc-tion of IL-8 (Fig. 2b). This toxin A-induced production ofIL-8 was significantly decreased in cells transfected with ac-Jun superrepressor plasmid, but not in cells transfectedwith control plasmid (Fig. 2b). Consistent with this result,stimulationwith toxinA also increased the levels of IL-8mRNAtranscript in primary colon epithelial cells, while pretreat-ment with the AP-1 inhibitor curcumin before toxin Astimulation resulted in a significant decrease in IL-8 mRNAexpression (Table 1). To confirm the inhibition of IL-8 byAP-1 inhibitor curcumin, an experiment using siRNAagainst c-Jun was performed. As a result, IL-8 expressionin toxin A-exposed HT-29 cells was significantly inhibitedby transfection with c-Jun siRNA [control, 8.3±4.2; toxinA, 196±92; toxin A + c-Jun siRNA, 73±190; toxin A +nonsilencing siRNA, 203±107; mean no of IL-8 mRNAtranscripts (×105)/μg RNA±SD, n=3]. In this experiment,β-actin mRNA levels in each group remained relativelyconstant [control, 8.6±3.4; toxin A, 9.3±5.0; toxin A + c-Jun siRNA, 9.8±6.3; toxin A + nonsilencing siRNA, 10.6±2.6; mean no of β-actin mRNA transcripts (×106) /μgRNA±SD, n=3].
C. difficile toxin A activates ERK1/2, p38, and JNK kinasesin human colon epithelial cells
As MAPKs regulate cytokine production in response to avariety of stimuli [12–14], we measured the phosphor-ylation of MAPKs in colon epithelial cells exposed to toxinA (20 ng/ml) for various time periods. As shown inFig. 3a, toxin A strongly induced phosphorylation ofERK1/2, p38, and JNK in HT-29 cells. All three MAPKpathways were activated within 5–10 min of stimulation,but the kinetics of activation were quite different: Levels ofphospho-ERK and phospho-JNK reached their maximumsafter 60 and 10 min, respectively, and subsequentlydecreased, while phospho-p38 was induced as early as5 min after stimulation and continued to increase for up to2 h (Fig. 3b).
MAPK can induce AP-1 activation and IL-8 expressionin human colon epithelial cells stimulated with C. difficiletoxin A
To further evaluate the relationship between MAPK andAP-1 activation in toxin A-stimulated epithelial cells, weexamined the effect of the following kinase inhibitors:PD98059, an inhibitor of MEK1/2, a MAPK that phos-phorylates ERK1/2; pyridinyl imidazole SB203580, whichspecifically inhibits p38; and SP600125, which inhibitsJNK. As shown in Fig. 4, pretreatment of HT-29 cells withPD98059 (>50 μM), SB203580 (>10 μM), or SP600125(>10 μM) for 30 min significantly inhibited the AP-1transcriptional activity induced by toxin A. However,
a
AP-1
dn-c
-Jun
contr
ol
pla
sm
id
None
Contr
ol
+ Toxin A
IL-8
se
cre
ted
(pg
/ml)
b
*
None
dn-c
-Jun
contr
ol
pla
sm
id
+ Toxin AC
ontr
ol
Fig. 2 The superrepressor of c-Jun decreased AP-1 DNA-bindingactivity and IL-8 secretion in HT-29 cell lines stimulated with C.difficile toxin A. HT-29 cells were transfected with a dominant-negative c-Jun expression vector (dn-c-Jun). a Forty-eight hours aftertransfection, cells were stimulated with C. difficile toxin A (20 ng/ml)for 1 h, and EMSA was performed. b Cells were stimulated with C.difficile toxin A for 24 h, and concentration of IL-8 protein wasmeasured by ELISA. Data are expressed as mean±SEM (n=7). *p<0.05 compared with toxin A alone
1398 J Mol Med (2007) 85:1393–1404

SB203580 and SP600125 had a greater inhibitory effect onAP-1 activity than PD98059 did.
To confirm the role of MAPK signaling pathways in AP-1activation by toxin A, we transfected recombinant adenovi-ruses into HT-29 cells and measured DNA-binding activityof AP-1. As shown in Fig. 5b, transfection with expressionvectors containing dominant-negative mutants of p38 orJNK significantly decreased the activation of AP-1 aftertoxin A stimulation. Concurrently, transfection with adeno-virus containing dominant-negative p38 or JNK expressionvectors significantly inhibited IL-8 mRNA expression intoxin A-stimulated HT-29 cells. Phosphorylation of p38 orJNK was suppressed in HT-29 cells infected with thecorresponding recombinant adenovirus (Fig. 5c).
A superrepressor for Ras inhibits AP-1 activationand IL-8 expression in C. difficile toxin A-stimulatedHT-29 cells
Although Ras is known to be a major regulator of MAPKand AP-1-mediated gene transcription, its role in C. difficiletoxin A stimulation remains unclear. In this study, toxin Aactivated the Ras signal in HT-29 cells, as determined byRas affinity precipitation assay (Fig. 6a). To determine
whether Ras is involved in the signaling pathway for AP-1activation and IL-8 expression in toxin A-stimulatedintestinal epithelial cells, we transfected HT-29 cells witha dominant-negative Ras superrepressor. As shown inFig. 6b, transfection with the Ras superrepressor signifi-cantly reduced the induction AP-1 transcriptional activityafter stimulation with toxin A, while transfection withcontrol plasmid had no effect. In addition, activation of theIL-8 transcriptional reporter was also inhibited in cellscotransfected with a Ras superrepressor plasmid, but not incells cotransfected with control plasmid. In this condition,transfection with the Ras superrepressor significantlyreduced the levels of phosphorylated p38 and JNK in toxinA-stimulated HT-29 cells (Fig. 6c). These results suggestthat the stimulation of intestinal epithelial cells with C.difficile toxin A activates a signaling cascade of Ras/MAPK/AP-1, resulting in expression of IL-8.
Concentration of inhibitors (µM)
Fold
-incre
ase o
f A
P-1
report
er
**
**
*
*
*
Fig. 4 Effects of MAPK inhibition on AP-1 reporter gene expression inHT-29 cells stimulated with C. difficile toxin A. HT-29 cell lines weretransfected with pAP-1-luciferase transcriptional reporter. Forty-eighthours after transfection, cells were pre-incubated with each concentrationof PD98059 (open circle), SB203580 (open square), or SP600125 (filledcircle) for 30 min and stimulated with C. difficile toxin A (20 ng/ml) foranother 1 h. Data are expressed as the mean fold induction in luciferaseactivity relative to unstimulated controls±SEM (n=7). * p<0.05compared with toxin A alone
Phospho-ERK1/2
ERK1/2
Phospho-JNK1/2
JNK1/2
Phospho-p38
p38
Actin
44 kDa42 kDa
43 kDa
43 kDa
45 kDa
Time after stimulation (min)
0 5 10 30 60 120
44 kDa42 kDa
54 kDa46 kDa
54 kDa46 kDa
Fig. 3 C. difficile toxin A activates MAPKs ERK1/2, p38, and JNK inhuman colon epithelial cells. HT-29 cell lines were stimulated with C.difficile toxin A (20 ng/ml) for the indicated periods of time.Phosphorylation of ERK1/2, p38, and JNK was measured by Westernblot analysis. Results are representative of five independent experiments
Table 1 AP-1 inhibitor curcumin reduced the levels of IL-8 mRNA transcripts in primary colon epithelial cells stimulated with C. difficile toxin A
Control Curcumin Toxin A Toxin A+curcumin
IL-8 (×105) 6.7±7.2 (1) 7.5±6.5 (1) 173±103 (26) 62±49a (9)β-actin (×106) 6.8±5.5 (1) 8.1±6.1 (1.2) 7.7±7.6 (1.1) 6.3±4.2 (0.9)
Primary colon epithelial cells were preincubated with AP-1 inhibitor curcumin (20 μM) for 30 min. Then, the cells were treated with C. difficiletoxin A (20 ng/ml) for 6 h, after which total cellular RNA was extracted. The values represent the mean numbers of mRNA transcripts±SD permicrogram of total RNA (n=5). Values in parentheses are the mean fold-induction, compared with the unstimulated control.a Values are significantly different from those for samples treated with toxin A alone (p<0.05).
J Mol Med (2007) 85:1393–1404 1399

Inhibition of p38 attenuates C. difficile toxin A-inducedenteritis in mice
The above results indicate that toxin A-induced MAPKactivation is essential for AP-1 activation and IL-8 produc-tion in vitro. To assess its pathophysiological relevance inan in vivo model, we investigated whether the p38 inhibitorSB203580 would prevent toxin A-induced enteritis in mice.SB203580 was injected into the lumen of a 3- to 4-cm ilealloop (100 μg/loop) 30 min before treatment with toxin A.Administration of toxin A alone resulted in pathologicmanifestations of enteritis, characterized by the destruction
of villi, infiltration of neutrophils, and mucosal congestion(Fig. 7), while pretreatment with SB203580 attenuatedthese manifestations (Fig. 7d). Histopathological scoresobtained by measuring neutrophil infiltration, congestion,and villous destruction showed that SB203580 reduced theseverity of enteritis by ∼75% (Fig. 8a). In this experiment,C. difficile toxin A increased the AP-1 activity and a p38inhibitor SB203580 decreased the AP-1 activity (toxin A,3.9±0.6; toxin A + SB203580; 1.4±0.3; mean of relativevalues to control±SEM, n=3), indicating that inhibition ofp38 signal in vivo reduced toxin A-related AP-1 activation.In addition, the toxin A-induced secretion of MIP-2, amouse homologue of IL-8, was significantly decreased inthe SB203580-treated mice (Fig. 8b).
Discussion
The present study demonstrated that the stimulation ofintestinal epithelial cells with C. difficile toxin A resulted inthe activation of AP-1 signals and IL-8 expression. Thepathophysiological relevance of this association wasassessed in vivo using a murine system of ileal loops. Wefound that the p38 inhibitor SB203580 significantlyinhibited the induction of both mucosal inflammation andexpression of the murine homolog of IL-8 by C. difficiletoxin A, although both were significantly increased in toxinA-treated ileal loops of control mice. Together, these dataindicate that MAPK signaling and AP-1 activation may beinvolved in inflammatory responses in a toxigenic C.difficile infection.
AP-1 functions as a transcriptional regulator by bindingto the TPA response element. AP-1 is actually a collectionof related transcription factors belonging to the Fos (c-Fos,Fos-B, Fra1, Fra2) and Jun (c-Jun, Jun-B, Jun-D) families,which dimerize in various combinations through a leucine
AP-1
Contr
ol
+ Toxin A
dn-p
38
Contr
ol
virus
Toxin
A a
lone
dn-J
NK
a
b
IL-8
actin
Contr
ol
+ Toxin Adn-p
38
Contr
ol
virus
Toxin
A a
lone
dn-J
NK
(+) (-)
c 1 2 3 5
Actin
Actin
Phospho-JNK1/2
Phospho-p38
1 2 4 5
Fig. 5 Effects of transfection with recombinant adenovirus on AP-1activation and IL-8 expression in HT-29 cell lines stimulated with C.difficile toxin A. a HT-29 cells were transfected with adenoviruscontaining dominant-negative p38 (dn-p38) or JNK (dn-JNK) expres-sion vectors. Forty-eight hours after transfection, cells were stimulatedwith C. difficile toxin A (20 ng/ml). AP-1 DNA-binding activity wasmeasured by EMSA 1 h after stimulation. The control meansuntreated HT-29 cells. b Transfected cells were stimulated with toxinA (20 ng/ml) for 6 h, and total RNA was extracted. Expression of IL-8 and β-actin mRNA was assessed by RT-PCR. Results arerepresentative of five independent experiments. Positive and negativesymbols represent positive and negative control, respectively. TotalRNA extracted from HT-29 cells stimulated with TNF-α (20 ng/ml)for 8 h was used as the positive control and products obtained by PCRreaction without cDNA was used as the negative control. cPhosphorylated p38 and JNK were detected in recombinant adenovi-rus-transfected HT-29 cells after stimulation with toxin A (20 ng/ml)for 10 min. Results are representative of five independent experi-ments. 1 control; 2 toxin A alone; 3 toxin A + dominant-negative p38;4 toxin A + dominant-negative JNK; 5 toxin A + control virus
R
1400 J Mol Med (2007) 85:1393–1404

zipper [29]. We demonstrated that C. difficile toxin Ainduced AP-1 heterodimers composed of c-Jun/c-Fos inintestinal epithelial cells. As AP-1 can be activated byvarious pathways, including protein kinase C, proteintyrosine kinase, and MAPK [29], we further investigatedhow AP-1 was activated in intestinal epithelial cells in
response to toxin A and showed that C. difficile toxin Ainduced the phosphorylation of the MAPKs ERK1/2, p38,and JNK in intestinal epithelial cells. This finding isconsistent with recent reports that toxin A can activate MAPKsignals in monocytes and intestinal epithelial cells [18–20].Moreover, inhibition of MAPK significantly decreased theactivity of AP-1 and IL-8 expression. These results indicatethat MAPK activation is directly associated with theinduction of AP-1 transcriptional activity and IL-8 geneexpression in toxin A-stimulated intestinal epithelial cells.
Ras is known to control multiple downstream effectorpathways through Raf/MAPK [30, 31]. In addition, it hasbeen reported that Ras can induce the phosphorylation andactivation of transcription factors such as c-Jun [16, 32] andthat c-Jun promotes chemokine expression in response tobacterial infection or enterotoxin stimulation [22, 26]. Thepresent study showed that C. difficile toxin A activated AP-1composed of c-Jun/c-Fos heterodimers and it is thereforelikely that Ras is involved in the activation of AP-1 by toxinA. Indeed, toxin A induced Ras activation, which seem to bethe most upstream member and thereby the staring point ofthe signaling cascade. In addition, our study showed thatinduction of AP-1 by toxin A was significantly inhibited bytransfection with a Ras superrepressor. Furthermore, trans-fection with a Ras superrepressor also inhibited phosphory-lation of p38 and JNK, leading to down-regulation of AP-1activity and decreased IL-8 expression. These results clearlyindicate that IL-8 expression induced by toxin A depends onthe activation of Ras, a MAPK cascade and c-Jun/c-Fosheterodimeric AP-1 molecules in intestinal epithelial cells.
One of molecular mechanisms of bacterial protein toxinsis glycosylation of eukaryotic target protein. In C. difficileinfection, the target proteins are known to be Rassuperfamily of small guanosine triphosphatase (GTPase),including Ras, Rho, Rab, Ran, and Arf [33]. For example,C. difficile toxins A and B transfer the glucose moiety ofUDP-glucose to members of the Rho family of smallGTPase, i.e., Rho, Rac, and Cdc42 [34]. Although the
a
GTP-Ras
0 10 30
Toxin A stimulation (min)F
old
-incre
ase o
f
AP
-1 r
eport
er
Fold
-incre
ase o
f
IL-8
report
er
b
*
*
Phospho-
JNK1/2
Phospho-p38
Actin
c+ Toxin A
None
dn-R
as
Contr
ol
pla
sm
id
Contr
ol
+ Toxin A
None
dn-R
as
Contr
ol
pla
sm
id
Contr
ol
Fig. 6 The Ras superrepressor inhibits AP-1 activation and IL-8 expression in HT-29 cell lines stimulated with C. difficile toxin A.a HT-29 cells were treated with C. difficile toxin A (20 ng/ml) for theindicated periods. The fraction of active Ras was determined byaffinity precipitation assay. Results are representative of threeindependent experiments. b HT-29 cells were transfected with pAP-1or pIL-8-luciferase transcriptional reporter together with the dominant-negative Ras superrepressor (dn-Ras) as indicated. After 48 h, the cellswere stimulated with C. difficile toxin A (20 ng/ml) for 1 h (AP-1) or6 h (IL-8), and luciferase assays were performed. Data are expressedas the mean fold induction in luciferase activity relative tounstimulated controls±SEM (n=7). *p<0.05 compared with toxin Aalone. c Phosphorylated p38 and JNK were detected in Ras super-repressor-transfected HT-29 cells after stimulation with toxin A(20 ng/ml) for 10 min. Results are representative of five independentexperiments
R
J Mol Med (2007) 85:1393–1404 1401

protein substrates of the C. difficile toxins A and B arefound in the families of the Rho and Ras GTPase [34], ithas not reported how toxin A activates Ras in intestinalepithelial cells. Therefore, further study should be neededto clarify the molecular mechanism for activating Rasmolecule in toxin A-stimulated cells.
In the present study, the inhibition of AP-1 did notcompletely suppress IL-8 expression in vitro or the manifes-tation of enteritis in vivo. This partial suppression may reflectthe activity of other pathways that activate NF-κB. IL-8 genetranscription requires the activation of a combination of thetranscription factors NF-κB and AP-1, or NF-κB and C/EBP,depending on the type of cell or stimuli [35, 36]. We foundthat C/EBP was not involved in toxin A-induced IL-8 expres-sion in HT-29 cells (as determined by EMSA, data not shown),whereas C. difficile toxin A-enhanced IL-8 transcription isdependent on NF-κB [7] and AP-1 (the present study).Furthermore, several studies demonstrated that C. difficiletoxin A induced the secretion of IL-8 through MAPK [5, 18,19] or tyrosine kinase-regulated NF-κB [7, 11]. Therefore, itis possible that both the Ras/MAPK/AP-1 pathway (in the
present study) and the IκB kinase (IKK)/NF-κB pathway [7,11], which lead to chemokine expression, may be activated inresponse to C. difficile toxin A stimulation. This hypothesis isconsistent with the observation that Ras can activate NF-κBsignaling via MAPK/extracellular signal regulated kinasekinase (MEKK). Activated MAPK/MEKK may activateIKK [37–39], which in turn mediates the phosphorylationand degradation of IκB, allowing the translocation of NF-κBto the nucleus. In addition, IKK shares structural elementswith MAPK [40]. Therefore, it is possible that the twopathways are interconnected in the upstream activationpathway of AP-1.
a
d
b
c
Fig. 7 Inhibition of p38 MAPK reduces C. difficile toxin A-inducedenteritis in murine ilea. SB203580 (100 μg/loop) was injected into thelumen of an ileal loop of specific pathogen-free C57BL6Cr mouse.After 30 min, C. difficile toxin A (5 μg/loop) was administered, andanimals were sacrificed 4 h later. Results are representative of sevenindependent experiments. a Control; b SB203580 alone; c toxin Aalone; d toxin A + SB203580. Magnifications of all figures are ×200
a
b
Severi
ty o
f en
teri
tis
Mo
use M
IP-2
(p
g/m
l)
Co
ntr
ol
To
xin
A
To
xin
A +
SB
20
35
80
SB
20
35
80
*
*
Fig. 8 Inhibition of inflammation and MIP-2 production in murineilea treated with C. difficile toxin A. The conditions of the C. difficiletoxin A-treatment of murine ilea are the same as in Fig. 7. a Severityof enteritis was measured using histological scores for epithelialdamage, congestion/edema, and neutrophil infiltration, as described inthe “Materials and methods.” b Production of murine MIP-2 wasmeasured by ELISA. Data represent the mean±SEM (seven loops pergroup). *p<0.05 compared with C. difficile toxin A alone
1402 J Mol Med (2007) 85:1393–1404

Treatment of cultured intestinal epithelial cells with C.difficile toxin A was shown to cause mitochondrial damage,cytochrome c release, oxidative stress, and ultimatelyapoptosis and necrosis of those cells [4, 5, 41, 42]. Inaddition, activation of epithelial cell NF-κB has significantanti-apoptotic function in toxin A-treated mice [11]. Consid-ering these reports, it is possible that early activated signalsuch as MAPK, NF-κB, or AP-1 may be involved inepithelial damage. Although we demonstrated that MAPKand AP-1 signaling may be associated with toxin A-induceddamage, it is not clear whether this signaling pathway canregulate apoptotic processes. Recently, a study demonstratedthat signaling pathway for colonocyte apoptosis after toxin Aexposure involves p38-dependent activation of p53 andsubsequent induction of p21 (WAF1/CIP1), resulting incytochrome c release and caspase-3 activation through Bakinduction [20]. In addition, inhibition of JNK activityreduced epithelial cell apoptosis in colitis model [43]. Thesefindings may support a hypothesis that MPAK signalsinduced by toxin A stimulation may be involved in apoptoticprocess. Therefore, further study is needed to clarify therelationship between MAPK and apoptosis in toxin A-stimulated epithelial cells.
In summary, this study demonstrates that the exposure ofintestinal epithelial cells to C. difficile toxin A results in therapid activation of MAPK signaling pathways, leading toAP-1 activation and IL-8 gene expression. Notably, theactivation of AP-1 seems to mediate intestinal inflammationand mucosal damage induced by toxin A. Based on thesefindings, we suggest that MAPK signaling and AP-1activation contribute to the biological effects of toxin Aproduced by toxigenic C. difficile and that specific targetingof AP-1 activation may therefore be effective in theprevention or treatment of inflammation associated withinfection by toxigenic C. difficile.
Acknowledgement We thank Dr. Martin F. Kagnoff, Dr. Joseph A.DiDonato, Dr. Andreas von Knethen, and Dr. Hyeyoung Kim forseveral plasmids, Dr. Kyoung-Ho Kim for histolopathologic exami-nations, and Han-Jin Lee for the excellent technical help. This studywas supported by a grant of Seoul R&BD Program.
References
1. Kelly CP, LaMont JT (1998) Clostridium difficile infection. AnnuRev Med 49:375–390
2. Burakoff R, Zhao L, Celifarco AJ, Rose KL, Donovan V, Pot-houlakis C, PercyWH (1995) Effects of purifiedClostridium difficiletoxin A on rabbit distal colon. Gastroenterology 109:348–354
3. Just I, Selzer J, von Eichel-Streiber C, Aktories K (1995) The lowmolecular mass GTP-binding protein Rho is affected by toxin Afrom Clostridium difficile. J Clin Invest 95:1026–1031
4. Mahida YR, Makh S, Hyde S, Gray T, Borriello SP (1996) Effectof Clostridium difficile toxin A on human intestinal epithelial
cells: induction of interleukin 8 production and apoptosis after celldetachment. Gut 38:337–347
5. He D, Sougioultzis S, Hagen S, Liu J, eates S, Keates AC,Pothoulakis C, Lamont JT (2002) Clostridium difficile toxin Atriggers human colonocyte IL-8 release via mitochondrial oxygenradical generation. Gastroenterology 122:1048–1057
6. Kim JM, Kim JS, Jun HC, Oh YK, Song IS, Kim CY (2002)Differential expression and polarized secretion of CXC and CCchemokines by human intestinal epithelial cancer cell lines in responseto Clostridium difficile toxin A. Microbiol Immunol 46:333–342
7. Kim JM, Lee JY, Yoon YM, Oh YK, Youn J, Kim YJ (2006) NF-kappa B activation pathway is essential for the chemokineexpression in intestinal epithelial cells stimulated with Clostridiumdifficile toxin A. Scand J Immunol 63:453–460
8. Rollins BJ (1997) Chemokines. Blood 90:909–9289. Roebuck KA (1999) Oxidant stress regulation of IL-8 and ICAM-
1 gene expression: differential activation and binding of thetranscription factors AP-1 and NF-κB. Int J Mol Med 4:223–230
10. Jefferson KK, Smith MF Jr, Bobak DA (1999) Roles ofintracellular calcium and NF-kappa B in the Clostridium difficiletoxin A-induced up-regulation and secretion of IL-8 from humanmonocytes. J Immunol 163:5183–5191
11. Chae S, Eckmann L, Miyamoto Y, Pothoulakis C, Karin M,Kagnoff MF (2006) Epithelial cell IkappaB-kinase beta has animportant protective role in Clostridium difficile toxin A-inducedmucosal injury. J Immunol 177:1214–1220
12. Ip YT, Davis RJ (1998) Signal transduction by the c-Jun N-terminal kinase (JNK) from inflammation to development. CurrOpin Cell Biol 10:205–219
13. Karin M, Liu Z, Zandi E (1997) AP-1 function and regulation.Curr Opin Cell Biol 9:240–246
14. Kyriakis JM, Avruch J (2001) Mammalian mitogen-activatedprotein kinase signal transduction pathways activated by stressand inflammation. Physiol Rev 81:807–869
15. Whitmarsh AJ, Davis RJ (1996) Transcription factor AP-1regulation by mitogen-activated protein kinase signal transductionpathways. J Mol Med 74:589–607
16. Garrington TP, Johnson GL (1999) Organization and regulation ofmitogen-activated protein kinase signaling pathways. Curr OpinCell Biol 11:211–218
17. Binetruy B, Smeal T, Karin M (1991) Ha-Ras augments c-Junactivity and stimulates phosphorylation of its activation domain.Nature 351:122–127
18. Warny M, Keates AC, Keates S, Castagliuolo I, Zacks JK,Aboudola S, Qamar A, Pothoulakis C, LaMont JT, Kelly CP(2000) p38 MAP kinase activation by Clostridium difficile toxinA mediates monocyte necrosis, IL-8 production, and enteritis.J Clin Invest 105:1147–1156
19. Chen X, Kokkotou EG, Mustafa N, Bhaskar KR, Sougioultzis S,O’Brien M, Pothoulakis C, Kelly CP (2006) Saccharomycesboulardii inhibits ERK1/2 mitogen-activated protein kinaseactivation both in vitro and in vivo and protects againstClostridium difficile toxin A-induced enteritis. J Biol Chem281:24449–24454
20. Kim H, Kokkotou E, Na X, Rhee SH, Moyer MP, Pothoulakis C,Lamont JT (2005) Clostridium difficile toxin A-induced colono-cyte apoptosis involves p53-dependent p21(WAF1/CIP1) induc-tion via p38 mitogen-activated protein kinase. Gastroenterology129:1875–1888
21. Kim JM, Eckmann L, Savidge TC, Lowe DC, Witthoeft T,Kagnoff MF (1998) Apoptosis of human intestinal epithelial cellsafter bacterial invasion. J Clin Invest 102:1815–1823
22. Kim JM, Jung HY, Lee JY, Youn J, Lee CH, Kim KH (2005)Mitogen-activated protein kinase and activator protein-1 depen-dent signals are essential for Bacteroides fragilis enterotoxin-induced enteritis. Eur J Immunol 35:2648–2657
J Mol Med (2007) 85:1393–1404 1403

23. Kim JM, Lee JY, Yoon YM, Oh YK, Kang JS, Kim YJ, Kim KH(2006) Bacteroides fragilis enterotoxin induces cyclooxygenase-2and fluid secretion in intestinal epithelial cells through NF-kappaBactivation. Eur J Immunol 36:2446–2456
24. Brown PH, Alani R, Preis LH, Szabo E, Birrer MJ (1993)Suppression of oncogene-induced transformation by a deletionmutant of c-Jun. Oncogene 8:877–886
25. Cai H, Szeberenyi J, Cooper GM (1990) Effect of a dominantinhibitory Ha-ras mutation on mitogenic signal transduction inNIH 3T3 cells. Mol Cell Biol 10:5314–5323
26. Seo JH, Lim JW, Kim H, Kim KH (2004) Helicobacter pylori in aKorean isolate activates mitogen-activated protein kinases, AP-1,and NF-kappaB and induces chemokine expression in gastricepithelial AGS cells. Lab Invest 84:49–62
27. Elewaut D, DiDonato JA, Kim JM, Truong F, Eckmann L,Kagnoff MF (1999) NF-kappaB is a central regulator of theintestinal epithelial cell innate immune response induced byinfection with enteroinvasive bacteria. J Immunol 163:1457–1466
28. Pothoulakis C, Castagliuolo I, LaMont JT, Jaffer A, O’Keane JC,Snider RM, Leeman SE (1994) CP-96,345, a substance P antagonist,inhibits rat intestinal responses to Clostridium difficile toxin A butnot cholera toxin. Proc Natl Acad Sci USA 91:947–951
29. Barnes PJ (2006) Transcription factors in airway diseases. LabInvest 86:867–872
30. Boguski MS, McCormick F (1993) Proteins regulating Ras and itsrelatives. Nature 366:643–654
31. Lowy DR, Willumsen BM (1993) Function and regulation of ras.Annu Rev Biochem 62:851–891
32. Joneson T, Bar-Sagi D (1997) Ras effectors and their role inmitogenesis and oncogenesis. J Mol Med 75:587–593
33. Wennerberg K, Rossman KL, Der CJ (2005) The Ras superfamilyat a glance. J Cell Sci 118:843–846
34. Schirmer J, Aktories K (2004) Large clostridial cytotoxins: cellularbiology of Rho/Ras-glucosylating toxins. Biochim Biophys Acta1673:66–74
35. Matsusaka T, Fujikawa K, Nishio Y, Mukaida N, Matsushima K,Kishimoto T, Akira S (1993) Transcripton factors NF-IL-6 andNF-κB synergistically activate transcription of the inflammatorycytokines, interleukin 6 and interleukin 8. Proc Natl Acad SciUSA 90:10193–10197
36. Mukaida N, Mahe Y, Matsushima K (1990) Cooperative interac-tion of nuclear factor κB- and cis-regulatory enhancer bindingprotein-like factor binding elements in activating the interleukin-8 gene by proinflammatory cytokines. J Biol Chem 265:21128–21133
37. Lange-Carter CA, Johnson GL (1994) Ras-dependent growthfactor regulation of MEK kinase in PC12 cells. Science265:1458–1461
38. Lange-Carter CA, Pleiman CM, Gardner AM, Blumer KJ,Johnson GL (1993) A divergence in the MAP kinase regulatorynetwork defined by MEK kinase and Raf. Science 260:315–319
39. Russell M, Lange-Carter CA, Johnson GL (1995) Direct interac-tion between Ras and the kinase domain of mitogen-activatedprotein kinase kinase kinase (MEKK1). J Biol Chem 270:11757–11760
40. Nemoto S, DiDonato JA, Lin A (1998) Coordinate regulation ofIκB kinases by mitogen-activated protein kinase kinase kinase 1and NF-κB inducing kinase. Mol Cell Biol 18:7336–7343
41. Pothoulakis C, Lamont LT (2001) Microbes and microbial toxins:paradigms for microbial-mucosal interactions. II. The integratedresponse of the intestine to Clostridium difficile toxins. Am JPhysiol 280:G178–G183
42. Brito GA, Fujji J, Carneiro-Filho BA, Lima AA, Obrig T,Guerrant RL (2002) Mechanism of Clostridium difficile toxin A-induced apoptosis in T84 cells. J Infect Dis 186:1438–1447
43. Assi K, Pillai R, Gomez–Munoz A, Owen D, Salh B (2006) Thespecific JNK inhibitor SP600125 targets tumour necrosis factor-alpha production and epithelial cell apoptosis in acute murinecolitis. Immunology 118:112–121
1404 J Mol Med (2007) 85:1393–1404

ORIGINAL ARTICLE
Modulation of muscle contractionby a cell-permeable peptide
Gisela Tünnemann & Peter Karczewski &Hannelore Haase & M. Cristina Cardoso & Ingo Morano
Received: 31 March 2007 /Revised: 18 May 2007 /Accepted: 13 June 2007 / Published online: 24 August 2007# Springer-Verlag 2007
Abstract In contrast to immortal cell lines, primary cells arehardly susceptible to intracellular delivery methods such astransfection. In this study, we evaluated the direct delivery ofseveral cell-permeable peptides under noninvasive condi-tions into living primary adult rat cardiomyocytes. Wespecifically monitored the functional effects of a cell-permeable peptide containing the 15 amino acid N-terminalpeptide from human ventricular light chain-1 (VLC-1) oncontraction and intracellular Ca2+ signals after electricalstimulation in primary adult cardiomyocytes. The trans-ducible VLC-1 variant was taken up by cardiomyocyteswithin 5 min with more than 95% efficiency and localizedto sarcomeric structures. Analysis of the functional effectsof the cell-permeable VLC-1 revealed an enhancement ofthe intrinsic contractility of cardiomyocytes without affect-ing the intracellular Ca2+. Therefore, peptide transductionmediated by cell-penetrating peptides represents not only aunique strategy to enhance heart muscle function with nosecondary effect on intracellular Ca2+ but also an invaluabletool for the modulation and manipulation of proteininteractions in general and in primary cells.
Keywords Ventricular light chain-1 (VLC-1) .
Cell penetrating peptide (CPP) . Peptide transduction .
Cardiomyocytes . Drug delivery
Introduction
Therapeutical delivery of protein or peptides into livingprimary cells is hampered by the lack of a suitable andefficient method for the introduction of macromolecules.Most commonly used transfections methods work in immor-talized cells but mostly fail in primary cells or requirespecialized and time-consuming protocols, i.e., production
J Mol Med (2007) 85:1405–1412DOI 10.1007/s00109-007-0238-6
DO00238; No of Pages
M. Cristina Cardoso and Ingo Morano contributed equally.
G. Tünnemann : P. Karczewski :H. Haase :M. C. Cardoso (*) :I. Morano (*)Max Delbrück Center for Molecular Medicine,Robert Rössle Str. 10,13125 Berlin, Germanye-mail: [email protected]
I. MoranoCharité Medical School, Johannes Müller Institute for Physiology,Tucholskystr. 2,10117 Berlin, Germany
INGO MORANO
received his Ph.D. in humansciences and postdoctoral Ha-bilitation in Human Physiologyfrom the Medical Faculty of theUniversity of Heidelberg. He ispresently Professor for Molecu-lar Clinical Physiology at theMedical Faculty of theHumboldt University (Charité),Berlin, and leader of the“Molecular Muscle PhysiologyGroup” at the Max-Delbrück-Center, Berlin. His researchinterests include expression,regulation, and function of con-tractile handling proteins insmooth and cardiac muscle.
GISELA TÜNNEMANN
studied chemistry at the Carlvon Ossietzky-University inOldenburg, Germany. She ispresently working in theresearch group “Molecular andCell Biology of the (Epi)genome” at theMax-Delbrück-Center forMolecular Medicine in Berlin,Germany. Her research interestsinclude peptide delivery intoliving cells, mechanisticalaspects of the translocationevent of cell-penetratingpeptides, and cell cycleregulation.
e-mail: [email protected]

of viral vectors. Moreover, the limited life span of primarycells often does not provide sufficient time for expression ofgene products and subsequent analysis of their effects.Physical methods such as microinjection and bead loadingare highly invasive procedures and are not tolerated by severalcell types. It has been known for quite some time that basicproteins like histones or poly-ornithine as well as stretches ofbasic amino acids within proteins aid the uptake of proteinsinto mammalian cells [14, 17, 20, 30]. In the 1990s,transducible peptides like penetratin-1 from the homeodo-main of Antennapedia [11] and amino acids 48–57 from thetransactivator of transcription of human immunodeficiencyvirus (HIV)-1 [14] were identified and exploited to introducedrugs or biological macromolecules into mammalian cells.Together with other native and synthetic transducingpeptides, they are referred to as cell-penetrating peptides(CPPs) [12]. However, it became evident that the invasivemethods used to analyze the transduction mediated by CPPsor effects of interconnected cargoes had led to overestimatedtransduction results and overrated effects of cargoes fused toCPPs [27]. Nevertheless, CPPs mediate the introduction offused cargoes into living cells, with cargo-dependentmechanistical differences. One uptake mechanism can bedescribed as a slow adsorptive endocytosis and is preferen-tially used by globular proteins, whereas small compoundslike peptides linked to CPPs favor a rapid membranepotential-dependent uptake with overall intracellular avail-ability of the transduced species [33]. CPP-mediated peptidetransduction has recently been used to deliver cardioprotec-tive peptides derived from protein kinase C [4, 7–9, 24], theantiapoptotic BH4 peptide derived from the apoptosisregulator protein Bcl-xL [26, 28] and a Nox2-derivedpeptide [34] into isolated cardiomyocytes or whole hearts.We have tested the feasibility of this approach to studymuscle function in living adult primary cardiomyocytes.Therefore, we targeted the interaction between actin and theessential myosin light chain (MLC-1) of cardiac type IImyosin by a peptide competition approach. Transgenicoverexpression of the N terminus of the human ventricularMLC-1 (residues 1–15; hereafter termed VLC-1), whichbinds to actin and targets actin/MLC-1 interaction, signif-icantly increased the magnitude and kinetics of the contrac-tion of isolated perfused hearts [21]. We fused the samehuman VLC-1 peptide to the TAT CPP (VLC-1-TAT) andinvestigated its uptake, intracellular distribution, and function-al consequences in primary living adult rat cardiomyocytes.
Materials and methods
Isolation of adult rat cardiomyocytes Primary cultures ofcardiomyocytes from male WKY rats aged 3 months wereperformed as described previously [1].
Peptides The peptides consisted of either L-amino acids(capital letters) or of D-amino acids (lower case letters). Incase of D-amino acid peptides, functional motifs weresynthesized as retro-all D-variants (underlined) to maintaintheir functionality. Peptides were either labeled with thefluorophore 5,6-carboxy-tetramethylrhodamine (TAMRA)or fluorescein isothiocyanate (FITC). TAT (TAMRA- orFITC-rrrqrrkkrg), PTD4 [23, 33] (TAMRA-araqraaaray),and TAT-p21 (TAMRA-rrrqrrkkrgaaAGRKRRQTSMTDFYHSKRRLIFSa-amide) [33] were labeled directly attheir N termini with the indicated fluorophores (PeptideSpeciality Laboratories, Heidelberg). In the case of VLC-1(MAPKKPEPKKSSAKA-C-TAMRA-ME-amide) andVLC-1-TAT (MAPKKPEPKDDAKAPAGRKKRRQRRR-C-TAMRA-ME-amide; Biosyntan, Berlin) the TAMRAfluorophore was coupled via an additional cysteine at theC terminus leaving the N terminus free for the interactionwith actin.
Uptake of transducible peptides and controls To analyzethe transduction ability of different compounds into livingadult ventricular cardiomyocytes, the primary cells wereplated into a laminin-coated μ-slide eight-well ibiTreat(ibidi, Martinsried) or four-well labtek (Nunc, Wiesbaden)microscopy observation chamber. The respective peptidesand controls were added directly to Hank’s balanced saltssolution buffered with 10 mM 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid at pH 7.4 (HBSS) ormedium and gently shaken to yield a final concentrationof 10 μM in case of the peptides and 5,6-TAMRA-fluorophore. Trypan blue (Sigma-Aldrich) was added to afinal concentration of 0.5% (v/v) to the HBSS buffer. Forthe experiments summarized in Fig. 1 confocal imageswere acquired 1 h after addition of the respectivecompounds to living cardiomyocytes. To study theintracellular localization of transducible peptides inFig. 3, after 15 min of peptide incubation, the mediumwas removed, and the cells were washed twice with theHBSS buffer. For subsequent confocal image collection,the cells were kept in medium or buffer. To study theeffect of the peptide on muscle contraction and intracel-lular Ca2+ (Fig. 4), cardiomyocytes were electricallystimulated (see below) to permit the access of the peptidesto all actin molecules with potential binding sites. Duringconfocal image collection, the electric stimulation wastemporarily switched off.
Microscopy, image acquisition, and analysis Confocalimages were acquired with a Zeiss laser scanning micro-scope LSM510 Meta mounted on an Axiovert 200Minverted microscope using a 63× phase-contrast oil immer-sion plan-apochromat objective NA1.4 or a 100× phase-contrast oil immersion plan-neofluar objective NA1.3. For
1406 J Mol Med (2007) 85:1405–1412

all settings, the main beam splitter was HFT UV/488/543/633, and the specific parameters for the single fluorophoreswere: FITC, excited at 488 nm light, detected with a 500–530-nm bandpass filter; TAMRA or rhodamine excited at543 nm, detected with 565–615 bandpass filter; and trypanblue, excited with 633 nm, detected with 650 longpassfilter. Phase-contrast images were recorded with excitationat 488 nm and detection in the transmission channel. Laserpower for observation was typically 1–5% (488 nm,25 mW) and 50–60% (543 nm, 1 mW) unless otherwiseindicated. Settings were adjusted in a way that image pixelswere not over- or underexposed with the range indicatorfunction in the Zeiss LSM image acquisition and examinersoftware version 3.2.
Measurement of cardiomyocyte shortening and Ca2+
transients Attached cardiomyocytes were washed with
HBSS. Cells were loaded with Fura-2-AM for 30 min atroom temperature in the dark. The dye solution was removed,and cells were left on HBSS for another 15 min. Onlycardiomyocytes of optically intact rod-shaped morphologywith clear cross-striation were analyzed. Cardiomyocyteswere electrically stimulated until a stable steady-statecontraction and Fura-2 signal could be monitored.
Cell shortening and Fura-2 signals were simultaneouslymeasured at 30°C on an Ionoptix Contractility andFluorescence System (Ionoptix). Cardiomyocytes wereelectrically stimulated with bipolar pulses of 5 ms durationat 1 Hz. Cell shortening, expressed as percentage of restingcell length, was measured using the video-edge technique ata sampling rate of 240 per second. Ca2+ transients weremonitored as ratio of fluorescence emission at 510 nm wasobtained by alternate excitation at 340 and 380 nm (340/
Fig. 1 Peptide uptake and in-tracellular distribution in livingadult cardiomyocytes. To studythe uptake capacity of differentcompounds into primary ratcardiomyocytes, different fluo-rescent compounds were direct-ly added for 1 h to the mediumor buffer of freshly isolatedcardiomyocytes. After the incu-bation period, confocal imagesof the cells were taken withoutexchange of the medium andafter removal of the fluorescentsolution and exchange againstthe fresh medium. Internaliza-tion into healthy adult cardio-myocytes occurred afterapplication of 10 μM of thetransducible peptides FITC-TATshown at low (a) and highmagnification (b) and TAMRA-TAT-p21 shown at low (c) andhigh magnification (d) but notwith application of 10 μM of abasic control peptide PTD4 (e).Moreover, 0.5% of the vital dyetrypan blue (f) or 10 μM of theTAMRA-fluorophore (g) itselfwere not able to enter healthycardiomyocytes (rod-shapedcells in culture). Scale bar,10 μm. Stars indicate the nucleiand arrowheads the nucleoli (N)in the higher magnificationimages. PC Phase contrast, NPnucleoplasm
J Mol Med (2007) 85:1405–1412 1407

380 ratio). Data files from 15 consecutive beats recorded atintervals were averaged for analysis. Subsequently, thecardiomyocytes were incubated with the peptides for15 min without electrical stimulation. The peptide was thenremoved by replacing the peptide-containing HBSS bufferwith normal HBSS buffer without the peptide. Thecardiomyocytes were subsequently electrically stimulated,and both the shortening and Fura-2 signals were simulta-neously recorded. The effect of the peptide on shorteningamplitude and the Fura-2 signal was expressed in percentchange compared to the steady-state signals obtained in thepreincubation period.
Results and discussion
We recently demonstrated by live-cell confocal microscopythat the TAT CPP was able to shuttle fused peptides intoprimary blood cells and subsequently modulated theirfunctional properties [10]. In this study, we tested whetherTAT CPP could penetrate and if a peptide derived from theN terminus of VLC-1 fused to TAT is able to modulate thecontractile function of primary adult cardiomyocytes.
Different basic peptides were incubated with freshlyprepared cultures of cardiomyocytes, and peptide internal-ization was analyzed live by laser-scanning confocalmicroscopy. The fluorescently labeled minimal transductiondomain TAT CPP of the transactivator of transcription fromHIV-1 was readily taken up into cardiomyocytes anddisplayed a strong affinity to the nuclear compartment(Fig. 1a). It could also be visualized in a punctate patternthroughout the entire cardiomyocyte (Fig. 1a). To determinewhether the TAT CPP is able to shuttle an attached peptideinto cardiomyocytes, we used the TAMRA-labeled TAT-p21WAF/CIP (TAT-p21) fusion peptide [33], which inaddition to the transducing moiety contains 26 amino acidsderived from the C terminus of human p21WAF/CIP protein.The uptake of this cargo peptide (assessed by appearance innucleoli) occurred on a timescale of 5 to 10 min afterpeptide application. Its pattern of localization inside thecardiomyocytes was similar than that seen for TAT alone(Fig. 1c). Basic amino acid residues are a prerequisite forthe transduction ability of CPPs [13, 25, 35], and peptidescontaining a minimum of six basic amino acids have beenshown to traverse biological membranes [5, 18]. As anontransducing control peptide, we chose the TAMRA-labeled peptide PTD4, which contains three arginines intotal [23, 33]. More than 1 h after application of this peptideto the cardiomyocyte culture, none of the healthy intactcardiomyocytes took up the fluorescent peptide (Fig. 1e).Similar results were obtained for the vital dye trypan blue(Fig. 1f) and the TAMRA fluorophore (Fig. 1g). Approx-imately 5% of cardiomyocytes in the cultures were dead or
Fig. 2 Molecular hypothesis for the enhancement of cardiomyocytecontractility by the cell-permeable VLC-1 peptide. a Primarysequence of VLC-1-TAT peptide color-coded orange for the VLC-1-and yellow for the TAT-moiety. b Schematic sliding filament modeldisplaying actin in violet and the MHC in red. The highermagnification shows the catalytic domain (CD) and the neck domain(ND) of one molecule of the MHC. MLC proteins are colored greenwith the N-terminal SE inside the essential MLC-1 protein highlightedin red. Upon intramolecular conformational changes in the CD ofMHC, the ND swings out, exposing the SE of MLC-1 to an actinmolecule in direction to the Z-line. Treatment of cardiomyocytes withthe transducible TAT peptide (yellow ball) fused to the SE-peptide(orange) blocks potential binding sites of the native MLC-1 Nterminus. After the MHC rearrangement, the MLC-1 protein can nolonger interact with actin and downregulate the myosin motor activity.The scheme is based on the pre- and postpower stroke model [19]developed with respect to crystallographic data on the Dicytosteliummyosin motor domain [15, 32]
1408 J Mol Med (2007) 85:1405–1412

harmed (visible in the phase-contrast images as not rodshaped and with no striations). These cells were floodedwith both the CPPs as well as any other control dyes(Fig. 1c,e–g). The cell-permeable TAT-derived peptidesdisplayed a similar enrichment in the nuclear compartmentwith strong accumulation inside nucleoli (arrowheads) ascan be seen in the higher magnification images (Fig. 1b,d).This intranuclear distribution is basically determined by theTAT moiety, which includes a nuclear localization sequence[22, 29, 33].
Having shown that CPP TAT was able to shuttle fusedpeptides into living cardiomyocytes, we designed a trans-ducible peptide comprising the actin-binding element of theventricular isoform of human MLC-1 (VLC-1), i.e., the N-terminal residues 1–15 (VLC-1 peptide) connected to TAT,termed VLC-1-TAT (Fig. 2). The hearts of transgenicanimals harboring minigenes encoding for the VLC-1peptide revealed enhanced myosin motor activity andpositive inotropic effects [21]. A possible molecularmechanism for the increase in myosin motor activity and
contractility is illustrated in the scheme in Fig. 2. MLC-1isoforms of vertebrate striated muscle play a regulatory rolein myosin motor function: The N-terminal part of MLC-1contains a sticky element (SE), which consists of severalpositively charged amino acids that bind to the C terminusof actin [3, 6, 16, 31]. The 46 N-terminal amino acids ofMLC-1 have previously been modeled on the basis ofcontemporary crystallographic data [2]. Interactions be-tween the sticky MLC-1 element and actin serve as anegative modulator and decrease the activity of the myosinmotor domain. Intracellular delivery of a synthetic stickyMLC-1 element by TAT-mediated transduction thereforewould antagonize MLC-1/actin interaction. We predict thiswould increase myosin motor activity and enhance theshortening amplitude without change of the systolic freeCa2+ activation level of intact cardiomyocytes.
To first test whether the VLC-1 peptide itself might betaken up by isolated cardiomyocytes because of its basiccharge, VLC-1 and VLC-1-TAT were applied for 15 min tofreshly isolated cardiomyocytes under resting conditions or,
Fig. 3 Transduction and intracellular localization of VLC-1-TAT inisolated adult cardiomyocytes. a Scheme for the application of theVLC-1-derived peptides and confocal imaging. Peptides were appliedat a concentration of 1 μM, incubated for 15 min to freshly isolatedcardiomyocytes. After removal of the peptide solution, the cells werewashed twice and kept in buffer or medium for direct live-cellconfocal imaging microscopy. Subsequently, the transduced cardio-myocytes were electrically stimulated with 1 Hz for maximally 1 h. bThe negative control peptide TAMRA-labeled VLC-1 stained onlydead cardiomyocytes (low magnification, upper panel) but failed to
get internalized into healthy cardiomyocytes even when 100% laserpower was used to detect potentially weak signals (lower panel). cApplication of TAT-VLC-1 to living cardiomyocytes led to rapidinternalization of the peptide (upper panel). The lower panel showstransduced VLC-1-TAT at higher magnification in an overlay of thephase contrast and the TAMRA-fluorescence. The arrow indicates thedirection of the intensity profile of gray and red intensities in the linescan for the localization analysis of VLC-1-TAT, which was present atsarcomeric structures with enrichment at the actin-containing I-bands(light bands in phase-contrast image)
J Mol Med (2007) 85:1405–1412 1409

in another set of experiments, constant electric stimulation(1 Hz, 20 V). After the fluorescent peptides were washedaway, the cells were analyzed live by confocal laser-scanning microscopy (Fig. 3a). VLC-1 alone was notinternalized into healthy cardiomyocytes and stained only
compromised cells (upper panel, Fig. 3b). To ensure thatlow concentrations of intracellular VLC-1 were not missed,the laser intensity was increased to its maximum, and stillno fluorescent signals were measured (lower panel,Fig. 3b). In contrast, VLC-1-TAT reached the intracellular
Fig. 4 Functional effects of cellpermeable VLC-1-TAT in livingadult cardiomyocytes. a Originalregistration of cell length (top)and cytosolic Ca2+ signals(Fura-2 signal, expressed as ra-tio R between 340 and 380excitation; bottom) of electrical-ly paced adult rat cardiomyo-cytes before (basal) and afterincubation with 1 μM VLC-1-TAT or 1 μM TAT as control.b Statistical evaluation of theeffects of different concentra-tions of transducible peptides(0.5, 1 μM) on fractional short-ening (FS; given in percent ofbasal contraction obtained be-fore incubation with the pep-tide), maximal rate of FS (+dFS/dtmax), and maximal relaxationrate (-dFS/dtmax; both given inpercent of basal values obtainedbefore peptide incubation) ofcontrol peptide (TAT) and VLC-1-TAT. c Statistical evaluation ofthe effects of different concen-trations of transducible peptides(0.5, 1 μM) on peak Fura-2fluorescence signal (expressedas ratio R between 340 and 380excitation, given in percent ofbasal R340/380 obtained beforeincubation with the peptide),maximal rate of R340/380(+dR340/380/dtmax), and maxi-mal rate of fluorescence decline(-dR340/380/dtmax; both givenin percent of basal valuesobtained before peptide incuba-tion) of control peptide (TAT)and VLC-1-TAT. Values aremeans±SEM, n=6–9 differentcardiomyocytes at each peptideconcentration used. Double as-terisk, p<0.01; triple asterisk,p<0.001 (t test for pairedvalues)
1410 J Mol Med (2007) 85:1405–1412

compartments of more than 95% of adult cardiomyocytes(Fig. 3c).
Unlike the localization of the TAT and TAT-p21 peptides(Fig. 1), the VLC-1-TAT was not detected in the cellnucleus. Detailed analysis of the intracellular distribution oftransduced VLC-1-TAT and correlation of the fluorescentsignals with the phase contrast images (merge image, lowerpanel, Fig. 3c) demonstrated that the peptide associateswith sarcomeric structures. It showed strong enrichment atthe I-bands representing the nonoverlapping zones of thethin actin filaments with the thick myosin filaments(linescan, lower panel, Fig. 3c). After transduction, theVLC-1-TAT peptide remained inside the sarcomeric compart-ments of the cardiomyocytes for at least 1 h after transferringthe loaded cardiomyocytes into the peptide-free buffersolution.
Using the same incubation protocol, we studied theeffects of the cell-permeable VLC-1 peptide on musclefunction by simultaneously monitoring the shorteningamplitude and the systolic and diastolic cytoplasmic Ca2+
fluctuations (measured by Fura-2 fluorescence) of pacedadult rat cardiomyocytes (Fig. 4a). As shown in Figs. 4band c, 1 μM, but not 0.5 μM, of VLC-1-TAT significantlyincreased the shortening amplitude of adult cardiomyocyte,while the cytosolic Ca2+ signal remained unchanged. Thesame concentrations of control TAT peptide alone did notchange the contractile state or the Fura-2 signals ifcompared to the basal state during the preincubation period.Higher concentrations of both control and test peptidesinduced deleterious effects on the cardiomyocyte contrac-tion. It is interesting to note that not only the maximalamplitude of shortening rose but also the maximal rate ofshortening and the maximal relaxation velocity increasedsignificantly. Because the Fura-2 signal remained un-changed, the selective effect of the VLC-1-TAT peptideon the contraction parameters suggests a selective anddirect effect on the function of the myosin cross-bridges.The Ca2+-sensitizing effect of the VLC-1-TAT peptidecould be predicted from the mechanism of action, as theinhibition of the MLC-1/actin interaction may rise selec-tively myosin motor activity and therefore muscle contrac-tion at a given activating free Ca2+ concentration, i.e., aninotropic effect without additional recruitment of Ca2+. Itshould be noted that the VLC-1-TAT peptide left theintracellular Ca2+-handling system unchanged, as seen bythe fact that the kinetic parameters of the Fura-2 fluores-cence signals remained normal (Fig. 4c).
In summary, we demonstrate by live-cell microscopythat CPPs and CPPs fused to peptides were taken up byadult cardiomyocytes with high efficiency and localize totheir targets inside the cytoplasm and/or nucleus. The cell-permeable peptide VLC-1-TAT accumulated in the actin-containing I-band of the sarcomeres and was able to
enhance the contractility of isolated adult cardiomyocyteswithout changing the myoplasmic Ca2+ levels. Importantly,the fact that VLC-1-TAT did not affect intracellular Ca2+
concentration and that it only has targets in striated musclecells makes this peptide uniquely suited as a novel potentialtherapeutic tool to modulate heart function. VLC-1-TAT is apowerful new drug candidate to improve the contractilestate of the failing heart.
Acknowledgments We thank W.-P. Schlegel and P. Pierschalek fortechnical assistance, R.M. Martin for invaluable help with confocalmicroscopy, and Jeff Stear for comments. G.T. was supported by theEuropean Union (ESF Program). This work was funded in part bygrants of the Deutsche Forschungsgemeinschaft and the VolkswagenFoundation to M.C.C and Deutsche Forschungsgemeinschaft to I.M.
References
1. Alvarez J, Hamplova J, Hohaus A, Morano I, Haase H, Vassort G(2004) Calcium current in rat cardiomyocytes is modulated bythe carboxyl-terminal ahnak domain. J Biol Chem 279:12456–12461
2. Aydt EM, Wolff G, Morano I (2007) Molecular modeling of themyosin-S1(A1) isoform. J Struct Biol. 159:158–163
3. Bottinelli R, Betto R, Schiaffino S, Reggiani C (1994) Unloadedshortening velocity and myosin heavy chain and alkali light chainisoform composition in rat skeletal muscle fibres. J Physiol 478(Pt2):341–349
4. Brandman R, Disatnik MH, Churchill E, Mochly-Rosen D (2007)Peptides derived from the C2 domain of protein kinase C epsilon(epsilon PKC) modulate epsilon PKC activity and identifypotential protein-protein interaction surfaces. J Biol Chem282:4113–4123
5. Cardoso MC, Leonhardt H (2002) Protein transduction: a noveltool for tissue regeneration. Biol Chem 383:1593–1599
6. Chalovich JM, Stein LA, Greene LE, Eisenberg E (1984)Interaction of isozymes of myosin subfragment 1 with actin:effect of ionic strength and nucleotide. Biochemistry 23:4885–4889
7. Chen L, Hahn H, Wu G, Chen CH, Liron T, Schechtman D,Cavallaro G, Banci L, Guo Y, Bolli R, Dorn GW 2nd, Mochly-Rosen D (2001) Opposing cardioprotective actions and parallelhypertrophic effects of delta PKC and epsilon PKC. Proc NatlAcad Sci USA 98:11114–11119
8. Chen L, Wright LR, Chen CH, Oliver SF, Wender PA, Mochly-Rosen D (2001) Molecular transporters for peptides: delivery of acardioprotective epsilonPKC agonist peptide into cells and intactischemic heart using a transport system, R(7). Chem Biol 8:1123–1129
9. Chen M, Won DJ, Krajewski S, Gottlieb RA (2002) Calpain andmitochondria in ischemia/reperfusion injury. J Biol Chem277:29181–29186
10. Choi M, Rolle S, Wellner M, Cardoso MC, Scheidereit C, Luft FC,Kettritz R (2003) Inhibition of NF-kappaB by a TAT-NEMO-binding domain peptide accelerates constitutive apoptosis andabrogates LPS-delayed neutrophil apoptosis. Blood 102:2259–2267
11. Derossi D, Chassaing G, Prochiantz A (1998) Trojan peptides: thepenetrating system for intracellular delivery. Trends Cell Biol 8:84–87
12. Dietz GP, Bahr M (2004) Delivery of bioactive molecules into thecell: the Trojan horse approach. Mol Cell Neurosci 27:85–131
J Mol Med (2007) 85:1405–1412 1411

13. Dom G, Shaw-Jackson C, Matis C, Bouffioux O, Picard JJ,Prochiantz A, Mingeot-Leclercq MP, Brasseur R, Rezsohazy R(2003) Cellular uptake of Antennapedia Penetratin peptides is atwo-step process in which phase transfer precedes a tryptophan-dependent translocation. Nucleic Acids Res 31:556–561
14. Fawell S, Seery J, Daikh Y, Moore C, Chen LL, Pepinsky B,Barsoum J (1994) Tat-mediated delivery of heterologous proteinsinto cells. Proc Natl Acad Sci USA 91:664–668
15. Fisher AJ, Smith CA, Thoden JB, Smith R, Sutoh K, Holden HM,Rayment I (1995) X-ray structures of the myosin motor domain ofDictyostelium discoideum complexed with MgADP.BeFx andMgADP.AlF4. Biochemistry 34:8960–8972
16. Fodor WL, Darras B, Seharaseyon J, Falkenthal S, Francke U,Vanin EF (1989) Human ventricular/slow twitch myosin alkalilight chain gene characterization, sequence, and chromosomallocation. J Biol Chem 264:2143–2149
17. Frankel AD, Pabo CO (1988) Cellular uptake of the tat proteinfrom human immunodeficiency virus. Cell 55:1189–1193
18. Futaki S, Suzuki T, Ohashi W, Yagami T, Tanaka S, Ueda K,Sugiura Y (2001) Arginine-rich peptides. An abundant source ofmembrane-permeable peptides having potential as carriers forintracellular protein delivery. J Biol Chem 276:5836–5840
19. Geeves MA, Holmes KC (1999) Structural mechanism of musclecontraction. Annu Rev Biochem 68:687–728
20. Green M, Loewenstein PM (1988) Autonomous functionaldomains of chemically synthesized human immunodeficiencyvirus tat trans-activator protein. Cell 55:1179–1188
21. Haase H, Dobbernack G, Tunnemann G, Karczewski P, CardosoC, Petzhold D, Schlegel WP, Lutter S, Pierschalek P, Behlke J,Morano I (2006) Minigenes encoding N-terminal domains ofhuman cardiac myosin light chain-1 improve heart function oftransgenic rats. FASEB J 20:865–873
22. Hauber J, Malim MH, Cullen BR (1989) Mutational analysis ofthe conserved basic domain of human immunodeficiency virus tatprotein. J Virol 63:1181–1187
23. Ho A, Schwarze SR, Mermelstein SJ, Waksman G, Dowdy SF(2001) Synthetic protein transduction domains: enhancedtransduction potential in vitro and in vivo. Cancer Res61:474–477
24. Inagaki K, Hahn HS, Dorn GW 2nd, Mochly-Rosen D (2003)Additive protection of the ischemic heart ex vivo by combinedtreatment with delta-protein kinase C inhibitor and epsilon-proteinkinase C activator. Circulation 108:869–875
25. Mai JC, Shen H, Watkins SC, Cheng T, Robbins PD (2002)Efficiency of protein transduction is cell type-dependent and isenhanced by dextran sulfate. J Biol Chem 277:30208–30218
26. Ono M, Sawa Y, Ryugo M, Alechine AN, Shimizu S, Sugioka R,Tsujimoto Y, Matsuda H (2005) BH4 peptide derivative from Bcl-xL attenuates ischemia/reperfusion injury thorough anti-apoptoticmechanism in rat hearts. Eur J Cardiothorac Surg 27:117–121
27. Richard JP, Melikov K, Vives E, Ramos C, Verbeure B, Gait MJ,Chernomordik LV, Lebleu B (2003) Cell-penetrating peptides. Areevaluation of the mechanism of cellular uptake. J Biol Chem278:585–590
28. Rohrbach S, Muller-Werdan U, Werdan K, Koch S, Gellerich NF,Holtz J (2005) Apoptosis-modulating interaction of the neuregu-lin/erbB pathway with anthracyclines in regulating Bcl-xS andBcl-xL in cardiomyocytes. J Mol Cell Cardiol 38:485–493
29. Ruben S, Perkins A, Purcell R, Joung K, Sia R, Burghoff R,Haseltine WA, Rosen CA (1989) Structural and functionalcharacterization of human immunodeficiency virus tat protein. JVirol 63:1–8
30. Ryser HJ, Hancock R (1965) Histones and basic polyamino acidsstimulate the uptake of albumin by tumor cells in culture. Science150:501–503
31. Seharaseyon J, Bober E, Hsieh CL, Fodor WL, Francke U, ArnoldHH, Vanin EF (1990) Human embryonic/atrial myosin alkali lightchain gene: characterization, sequence, and chromosomal loca-tion. Genomics 7:289–293
32. Smith CA, Rayment I (1996) X-ray structure of the magnesium(II).ADP.vanadate complex of the Dictyostelium discoideummyosin motor domain to 1.9 A resolution. Biochemistry35:5404–5417
33. Tunnemann G, Martin RM, Haupt S, Patsch C, Edenhofer F,Cardoso MC (2006) Cargo-dependent mode of uptake andbioavailability of TAT-containing proteins and peptides in livingcells. FASEB J 20:1775–1784
34. Zhang M, Kho AL, Anilkumar N, Chibber R, Pagano PJ, ShahAM, Cave AC (2006) Glycated proteins stimulate reactive oxygenspecies production in cardiac myocytes: involvement of Nox2(gp91phox)-containing NADPH oxidase. Circulation 113:1235–1243
35. Ziegler A, Blatter XL, Seelig A, Seelig J (2003) Proteintransduction domains of HIV-1 and SIV TAT interact with chargedlipid vesicles. Binding mechanism and thermodynamic analysis.Biochemistry 42:9185–9194
1412 J Mol Med (2007) 85:1405–1412

ORIGINAL ARTICLE
Accumulation of dietary glycotoxins in the reproductivesystem of normal female rats
Evanthia Diamanti-Kandarakis & Christina Piperi &Penelope Korkolopoulou & Eleni Kandaraki &Georgia Levidou & Apostolos Papalois &
Efstratios Patsouris & Athanasios G. Papavassiliou
Received: 21 May 2007 /Revised: 10 July 2007 /Accepted: 13 July 2007 / Published online: 11 August 2007# Springer-Verlag 2007
Abstract The aim of the present study was to investigatewhether dietary advanced glycation end-products (AGEs)can be detected in the ovarian tissue of normal female ratsand whether they can affect their metabolic or hormonalprofile. Sixty normal rats (20 animals in each group) wererandomly assigned to regular diet, either high (H-AGE) orlow (L-AGE) in AGE content for 6 months. H-AGE ratsdemonstrated higher levels of fasting glucose (P<0.001),insulin (P<0.069), and serum AGEs (P<0.001) thancontrol and L-AGE rats. Additionally, the H-AGE groupshowed increased AGE localization in the theca internacells of the ovarian tissue compared to control/L-AGE rats(P=0.003). Furthermore, increased receptor for AGE(RAGE) staining was also observed in granulosa cellscompared to control/L-AGE samples (P=0.038). In the H-AGE group, plasma testosterone was higher than in controlrats (P<0.001) and in the L-AGE group (P<0.001).However, H-AGE rats did not exhibit higher body weight
compared with normal (P=0.118) and L-AGE-fed rats (P=0.35). These results demonstrate for the first time thatadministration of high AGE diet in female rats for aprolonged period is associated with increased deposition ofAGEs in the theca cells and of RAGE in the granulosa andtheca interna cells of the ovarian tissue compared with thecorresponding ovarian compartments of the control and
J Mol Med (2007) 85:1413–1420DOI 10.1007/s00109-007-0246-6
E. Diamanti-KandarakisFirst Department of Internal Medicine, Endocrine section,Medical School, University of Athens,Athens, Greece
C. Piperi : E. Kandaraki :A. G. Papavassiliou (*)Department of Biological Chemistry, Medical School,University of Athens,75, M. Asias Street,11527 Athens, Greecee-mail: [email protected]
P. Korkolopoulou :G. Levidou : E. PatsourisDepartment of Pathology, Medical School, University of Athens,Athens, Greece
A. PapaloisELPEN S.A, Experimental Research Center,Athens, Greece
EVANTHIA DIAMANTI-KANDARAKIS
received her M.D. from AthensMedical School, Greece andher Ph.D. in experimental en-docrinology on the effects ofandrogens in female hypophy-sectomised rats from the sameUniversity. She is presentlyAssociate Professor of Endo-crinology and Metabolism andChief of the Endocrine sectionat the 1st Department of Med-icine, Athens University. Herresearch interests include mo-lecular and environmentalstudies on insulin action onPCOS.
ATHANASIOS G. PAPAVASSILIOUM.D., Ph.D. is presently Professorof Biochemistry and Head of theDepartment of Biological Chem-istry at Athens University Medi-cal School, Greece. He receivedhis Ph.D. in biochemistry andmolecular biophysics from theCollege of Physicians & Surgeonsof Columbia University in NewYork, USA. His research interestsinclude the study of signal trans-duction to transcription factors intumourigenesis and certain endo-crine pathologies.

L-AGE-fed animals. The metabolic alterations in conjuc-tion with the increased deposition in ovarian tissues ofdietary glycotoxins and elevated levels of testosterone in H-AGE-fed animals compared to the controls suggest animpact of environmental factors on ovarian tissue and thesefindings need further exploration.
Keywords AGEs . Insulin . Ovaries . RAGE . Testosterone
Introduction
In the modern world, it has been demonstrated thatpopulations adopting a Western lifestyle and diet indepen-dently of their genetic background exhibit alterations intheir metabolic profile. However, the impact of Westerndiets on the reproductive system in humans and animals hasstarted to attract major scientific interest.
Advanced glycation end-products (AGEs) are highlyreactive molecules, formed by nonenzymatic glycation ofproteins, lipids, and nucleic acids, which may inducestructural and vascular changes [1, 2]. The mechanismsby which AGE leads to these injuries in multicellularstructures remain largely unknown; however, the formationof insoluble cross-links, the induction of oxidative stress,and cell activation play a significant role. Interaction ofAGE with specific cellular receptors (RAGE) leads to cellactivation, release of cytokines, and growth factors, whichcontribute to abnormal cell/ matrix proliferation, such asseen in diabetic renal lesions and atheromas [3–5]. AGE-modified proteins are continuously formed in the body fromthe reaction of reducing sugars, but they can also beproduced from exogenous sources during contemporarymethods of cooking (precooked fast food meals heated inhigh temperatures) [6–9]. There is evidence that AGEabsorption from food is associated with the protein and fatingredients [9]. Recent reports have confirmed oral absorp-tion and tissue incorporation of end-products originatingfrom mixed foods [10]. Human studies confirmed thatabout 10% of exogenous AGEs are absorbed and correlatewith circulating and tissue AGEs levels, exceeding theirendogenous production [11]. Data in humans and experi-mental animals favor that exogenous food-ingested AGEsresult in elevated serum levels and increased tissuedeposition [12, 13]. Specifically, ingestion of a meal richin AGEs has led to increased serum levels of AGEs indiabetic patients, which were compared with controls, andtissue deposition was enhanced when the AGE meals wererich in fat [11].
Furthermore, normal mice fed high-fat diets rich inAGE content for 6 months displayed markedly impairedglucose and insulin responses during glucose tolerancetests and altered pancreatic islet structure and function
compared with those of control mice fed with a low-AGE-content diet [14].
While the mechanisms linking AGEs and the relateddeleterious metabolic effects are likely to be complex, theevidence indicates that lowering AGE content in fatty foodsmight be a mode of intervention to control metabolicsequelae. Dietary AGE restriction has been shown to resultin significant reduction in circulating AGE levels anddisease progression in animal models of atherosclerosis[13] and diabetes [15] and in diabetic patients with orwithout renal impairment [16]. These findings suggest thatdietary AGEs represent a significant source of circulatingand tissue-deposed AGEs, possibly manifesting similarpathogenic properties to their endogenous counterparts,and they may further constitute a chronic environmentalrisk factor for tissue injury.
Recently, AGEs levels were found to be elevated in serumof young normoglycemic women with polycystic ovarysyndrome (PCOS) [17]. In addition, increased immuno-staining of AGE and RAGE was observed in the differentcompartments of the ovarian tissue in polycystic ovaries[18]. Furthermore, young women with PCOS demonstratedincreased serum levels of AGEs after receiving a high-AGEdiet [19]. The source of these glycosylated end-products innormoglycemic women with PCOS has not been deter-mined and could be either endogenous or exogenous.
In the present study, the deposition of food glycotoxinson the ovarian tissue of normal female rats is investigatedfor the first time. It was postulated that female ratssubjected to long-term feeding on high- or low-AGE dietcontent could be detected on the ovarian tissue. Further-more, measurements of plasma testosterone were performedin parallel with estimation of glucose and insulin levels.
Materials and methods
Animals and diets
Wistar rats (60 animals total; female, 12 weeks old) werehoused at ELPEN S.A, Experimental Research Center,Athens, Greece. Animal care and experimental proceduresconformed with the “Guide for the Care and Use ofLaboratory Animals” (Department of Health, Educationand Welfare, Athens, Greece) and were approved by theInstitutional Animal Care and Use Committee.
The diets used were derived from a single standard ratchow (AIN-93G) purchased from Bioserve (Frenchtown, NJ),consisting of 18% protein, 58% carbohydrate, 7.5% fat, and3.73 kcal/g. Regular AIN-93G chow is normally prepared byheating at 100°C for 20 s and at 125°C for 30 min [20, 21].
Analysis of the AGE content of rat chow after heatingwas performed in collaboration with Dr. Henle’s Laborato-
1414 J Mol Med (2007) 85:1413–1420

ry, Institute of Food Chemistry, Technische UniversitätDresden, Dresden, Germany. This preparation contained76.0±15.3 mg carboxymethyllysine (CML)/100 g sample(or 436.9±88.1 mg CML/100 g protein), 205.32±22.25 mgfructoselysine/100 g sample (or 1,179.98±127.90 mgfructoselysine/100 g protein), and 52.68±5.71 mg furo-sine/100 g sample (or 302.78±32.82 mg furosine/100 gprotein) and was used as a high-in-AGE diet (H-AGE). Thesame rodent mix was also prepared by heating at 100°C for20 s only; this preparation was of equivalent macro- andmicronutrient and energy content but contained 1.3±0.4 mgCML/100 g sample (or 7.7±2.2 mg CML/100 g protein),104.58±3.08 mg fructoselysine/100 g sample (or 601.01±17.7 mg fructoselysine/100 g protein), and 26.83±0.79 mgfurosine/100 g sample (or 154.22±4.54 mg furosine/100 gprotein) and was considered as a low-in-AGE diet (L-AGE)(Table 1).
Analysis for total nitrogen and protein content wascarried out according to Kjeldahl’s method. For calculationof the protein content (nitrogen content multiplied with aspecific Protein factor), the factor F=6.25 for unknownproteins was used. Measurements of CML were carried outvia gas chromatography–mass spectroscopy after derivati-zation to the trifluor-acetic acid-methylesters. N-Carbox-ymethylornithine served as an internal standard. CML was
released from the protein by acid hydrolysis with 6 N HClat 110°C for 23 h.
Calculation of fructoselysine was carried out accordingto Krause et al. [22] by multiplying the molar amount offurosine with a conversion factor of 3.1. Measurements offurosine were carried out via high-performance liquidchromatography with UV detection at 280 nm accordingto Resmini et al. [23] after acid hydrolysis with 6 N HCl at110°C for 23 h. Results related to 100 g protein are basedon a protein content of 17.4%.
Control rats were given a standard rat chow containing23.4% protein, 4.5% fat, 5.3% crude fiber, 6.9% ash, 0.95%calcium, and 0.67% phosphorus.
Experimental design
At 12 weeks of age, animals (20 animals in each group)were randomly assigned to the diets for 6 months. Ratswere given pelleted food and water ad libitum in a specificpathogen-free environment at the animal laboratory. Bodyweight, serum glucose, and insulin and testosteroneconcentrations were monitored every 3 months. At theend of the 6 months, rats were killed for blood collectionand ovarian tissue retrieval.
Immunohistochemistry
Paraffin-embedded sections of formalin-fixed ovarian tissuewere deparaffinized by xylene and dehydrated in gradedethanol. Sections were treated in 3% hydrogen peroxide inphosphate-buffered saline (PBS) for 15 min and then rinsedin PBS. To increase the immunoreactivity of AGEs, thesections were placed in 500 ml of 0.01 M citric acid-buffered solution (pH 7.0) and microwaved at 500 W for5 min. After thorough washing, the sections were incubatedwith normal rabbit serum for 20 min at room temperature toavoid nonspecific binding of the antibodies. The sectionswere then incubated overnight at 4°C with the anti-AGEmonoclonal antibody, 6D12 (0.25 mg/ml stock, dilution1:50; Research Diagnostics, Concord, MA) or goat mono-clonal anti-RAGE antibody (0.25 ml, dilution 1:400; RDI-RAGEabG, Research Diagnostics) in PBS containing 1%bovine serum albumin. Immunoreactivity was detected bythe streptavidin–biotin–peroxidase method according to themanufacturer’s protocol. The final reaction product wasvisualized with 3,3′-diaminobenzidine tetrahydrochloride(LSAB detection kit; Dako, Carpinteria, CA). Lung tissuesections from diabetic rats were used as positive controlsfor AGE and RAGE antibodies. Negative controls (e.g.,ovarian tissue in which the primary antibody was substi-tuted with nonimmune mouse or goat serum) were alsostained in each run. Fourteen sections of control and L-AGE rat ovaries were evaluated along with 19 sections of
Table 1 Characteristics of dietary formulas with H-AGE and L-AGEglycotoxin content
H-AGE L-AGE
AssaysCML (mg/100 g protein) 436.9±88.1 7.7±2.2Fructoselysine (mg/100 g protein) 1179.98±127.90 601.01±17.7Furosine (mg/100 g protein) 302.78±32.82 154.22±4.54Nutrients (%)Protein 18.4 18.4Lipids 7.2 7.2Carbohydrate 58.6 58.6Other (fiber, moisture) 15.8 15.8Total calories (kcal/g) 3.9 3.9Micronutrients (kg)Biotin 0.2 mg 0.2 mgFolate 2 mg 2 mgNiacin 30 mg 30 mgPyridoxine (B6) 6 mg 6 mgRiboflavin 6 mg 6 mgThiamin 5 mg 5 mgVitamin A 4,000 IU 4,000 IUVitamin B-12 25 μg 25 μgVitamin E 75 IU 75 IUVitamin D3 1,000 IU 1,000 IU
Nutrients and micronutrients content were obtained from the study ofLin et al. [21]
J Mol Med (2007) 85:1413–1420 1415

H-AGE rat ovaries. The percentage of positive cells wasestimated using light microscopy. The evaluation of theimmunostained slides was performed blindly and indepen-dently by two pathologists. AGE and RAGE expressionwere categorized in four levels according to the percentageof positive cells, as follows: minimum (staining 1–10% ofcells), low (staining 11–30% of cells), moderate (31–60%of cells), and extensive (more than 60% of cells) immu-nostaining. The staining intensity was also assessed in fourlevels: 1, very weak; 2, weak; 3, moderate; and 4, strong.
Assays
Serum fasting glucose concentrations (mg/dl) were measuredwith the glucose oxidase technique (Linear Diagnostics, Spain).Serum insulin levels (μIU/ml) were evaluated with an enzymeimmunoassay (Insulin enzyme-linked immunosorbent assay[ELISA] kit, Mercodia AB, Uppsala, Sweden). Serum testos-terone levels (ng/ml) were estimated using the commerciallyavailable immunoassay kit from IBL Immunoassays, Germany.
Serum AGE levels (U/ml) were measured by AGE-specific competitive ELISA as described previously [17].
Statistical analysis
All data are given as mean±SE. Differences of means wereanalyzed by analysis of variance, which was followed bypost-hoc analysis using Bonferroni correction for multiplecomparisons. When comparing the differences in the AGEand RAGE expression levels, animals receiving the normaldiet were assigned in the same group with those receivingL-AGE diet because they displayed a similar distributionregarding AGE and RAGE staining. The respective differ-ences in the AGE and RAGE expression levels betweenthis group (controls/L-AGE) and the group of animalsreceiving H-AGE diet were tested employing logisticregression analysis for case–control studies (using thevariable denoting which animal is the H-AGE fed and
which one the L-AGE/control as a dependent variable) aswell as Fisher’s exact test. Statistically significant differ-ence was defined as a P value less than 0.05. All reported Pvalues are based on two-sided tests. All data analyses wereperformed using the SPSS 14.0 for windows.
Results
Effect of dietary glycotoxins in ovarian weights, in serumAGEs, and glucose levels
Body weights (grams) were similar before the initiation ofthe experiment and did not show a statistically significantchange after the experiment within the control, H-AGE, andL-AGE-fed rats (P=not significant, Table 2). However,post-treatment weight in the H-AGE group was significant-ly lower than in the L-AGE group (P=0.015, Table 2).
Ovarian tissue weight (grams) was increased in H-AGErats compared to controls (P<0.001) as well as between H-AGE rats and L-AGE (P=0.005).
Significant correlations were obtained between bodyweight and ovarian tissue weight after the 6-monthtreatment period (r=−0.422, P=0.018).
Fasting blood glucose (mg/dl) was higher in H-AGE ratscompared to controls (P<0.001) as well as compared toL-AGE rats (P<0.001).
Fasting glucose levels were negatively correlated withbody weights (r=−0.386, P=0.032) after the 6-monthtreatment period.
Fasting serum AGE levels (U/ml) were significantlyhigher in the H-AGE-fed compared with the L-AGE-fedrats (P=0.001; Table 2) as well as with controls (P<0.001).
AGE levels correlated negatively with body weights(r=−0.557, P=0.001) and positively with ovarian tissueweight (r=0.433, P=0.012), fasting glucose (r=0.374,P=0.027), and serum testosterone levels (r=0.463, P=0.035) after the 6-month treatment period.
Table 2 Anthropometric, metabolic and hormonal parameters of the three study groups
Variable Control(N=20)
L-AGE(N=20)
H-AGE(N=20)
P value, controlvs L-AGE
P value, controlvs H-AGE
P value, L-AGEvs H-AGE
Rat weight (g) 242.5±14.24 262.14±10.79 215.27±8.4 0.350 0.118 0.015Ovarian weight (g) 0.53±0.1 0.577±0.1 1.12±0.079 0.77 <0.001 0.005Fasting glucose (mg/dl) 109.87±6.64 87.6±4.42 149.5±6.06 0.015 <0.001 <0.001Fasting insulin (μIU/ml) 0.418±0.189 0.36±0.167 0.78±0.094 0.822 0.069 0.03Testosterone (ng/ml) 0.06±0.01 0.054±0.02 0.139±0.009 0.754 <0.001 <0.001Serum AGEs (U/ml) 5.06±0.06 4.35±0.3 9.88±1.07 0.055 <0.001 0.001
Data are given as means±SEM, P<0.05 statistically significant. Post-hoc tests were used to derive the respective P values because of the fact thatall the overall tests were proved to be statistically significant.
1416 J Mol Med (2007) 85:1413–1420

Effect of dietary glycotoxins in insulin and testosteronelevels
H-AGE rats demonstrated higher levels of fasting insulin(μIU/ml) than control (P=0.069) and L-AGE rats (P=0.03).
In addition, the H-AGE group presented higher plasmatestosterone levels (ng/ml) compared to control rats (P<0.001) and to the L-AGE group (P<0.001).
Testosterone levels correlated positively with ovariantissue weight (r=0.615, P=0.005), fasting glucose levels(r=0.641, P=0.002), and AGE levels (r=0.463, P=0.035)after the 6-month treatment period.
Immunohistochemical localization of AGEs in ovariantissue of control, L-AGE and H-AGE-fed rats
Control and L-AGE ovarian tissue samples presented asimilar distribution regarding AGE staining and, as men-
tioned earlier, were considered as one group. Statisticalanalysis was therefore performed in two groups namely,control/L-AGE (N=14) and H-AGE (N=19). The results ofboth logistic regression analysis and Fisher’s exact test forthe comparison of the two groups are reported in Table 3.The two methods, as expected, yielded similar results.
AGE expression was detected in all cases of control/L-AGE (14/14) and H-AGE (19/19) ovarian tissue, but it wasmore extensive in the ovaries of H-AGE-fed rats comparedto controls/L-AGE (logistic regression analysis, P=0.003).In addition, H-AGE rats ovaries displayed a higher intensityof AGE staining compared to control/L-AGE (logisticregression analysis, P=0.007).
AGE immunoreactivity was detected in granulosa, theca,and luteinized cells as well as in the ovarian stroma.However, the H-AGE group presented higher AGE expres-sion levels in the theca interna cells when compared tocontrols (logistic regression analysis, P=0.003, Fig. 1),
Table 3 Immunohistochemistry data of AGE and RAGE staining in ovarian tissue and uterine tubes of control, L-AGE (N=14), and H-AGE rats (N=19)
AGE RAGE
Control+L-AGE(numberof cases)
H-AGE(numberof cases)
P value,logisticregressionanalysis
P value,Fisher’sexact test
Control +L-AGE(# ofcases)
H-AGE(# ofcases)
P valueLogisticregressionanalysis
P valueFisher’sexact test
Expression 0.003* 0.001* Expression 0.042* 0.042*Minimum 6 0 Minimum/Low 2 0Low 6 5 Moderate 4 1Moderate 2 8 Extensive 8 17Extensive 0 6Intensity 0.007* 0.007* Intensity 0.010* 0.018*Very weak 5 1 Very Weak/Weak 2 0Weak 8 7 Moderate 7 3Moderate 1 10 Strong 5 15Strong 0 1Granulosa cells 0.292 0.424 Granulosa cells 0.038* 0.034*No 1 0 Low expression 4 1Yes 13 19 High expression 5 16Theca cells 0.003* 0.001* Theca cells 0.052 0.047*No 12 4 Low expression 12 4Yes 2 12 High expression 2 12Luteinizing cells 0.386 -a Luteinizing cells 0.481 –a
No 0 0 Low expression 0 0Yes 14 19 High expression 14 18Stroma cells 0.277 0.183 Stroma cells 0.706 0.492No 2 0 Low expression 0 2Yes 12 18 High expression 13 15Uterine tubes 0.313 0.44 Uterine tubes 0.435 –a
No 7 7 No 0 0Yes 4 9 Yes 11 15
Results of logistic regression analysis and Fisher’s exact test*P<0.05 statistically significanta Not applicable
J Mol Med (2007) 85:1413–1420 1417

whereas the respective differences for the granulosa celllayer and luteinizing cells did not achieve statisticalsignificance (logistic regression analysis, P=0.292 and P=0.277, respectively). Furthermore, there was no differencein the AGE stroma deposition between H-AGE and control/L-AGE samples (logistic regression analysis, P=0.386).
AGE staining was also observed in uterine tubes of bothH-AGE and control/L-AGE animals, displaying a similarpattern and extension of staining in both groups (logisticregression analysis, P=0.313).
Fig. 1 Immunohistochemical localization of AGE expression incontrol (a, 100× magnification), L-AGE-fed rat ovary (b, 100×magnification), and H-AGE-fed rat ovary (c, 200× magnification).AGE staining is observed in follicular cell layers and stroma cells;however, AGE staining is stronger in theca interna cells of H-AGE-fedrats compared to control and L-AGE
Fig. 2 Immunohistochemical localization of RAGE expression incontrol (a, 200× magnification), L-AGE-fed rat ovary (b, 200×magnification), and H-AGE-fed rat ovary (c, 200× magnification).RAGE immunoreactivity is observed in granulosa cells, theca internacells, as well as endothelial and stromal cells. RAGE staining infollicular cells revealed both cytoplasmic and nuclear localization.Significant difference in RAGE staining is observed between thegranulosa cell layer and theca interna of H-AGE-fed rats and controls
1418 J Mol Med (2007) 85:1413–1420

Immunohistochemical localization of RAGE in ovariantissue of control, L-AGE-fed, and H-AGE-fed rats
All but two samples (12 in 14 control/L-AGE and 19/19 H-AGE cases) exhibited a significant (moderate or high)RAGE immunoreactivity, although it seemed to be higherin H-AGE tissues (P=0.042). In addition, RAGE-stainingintensity was also higher in H-AGE ovarian tissue (P=0.01).Data are shown in Table 3.
Granulosa and theca cells displayed a cytoplasmic andnuclear RAGE immunoreactivity, whereas in luteinizing andstroma cells, RAGE staining was only cytoplasmic, in alltissue samples. RAGE expression in granulosa and theca celllayers was significantly higher in H-AGE-fed rats whencompared to the control/L-AGE (logistic regression analysis,P=0.038 and P=0.052, respectively, Fig. 2). A high RAGEexpression was also present in stroma and luteinizing cells,showing the same distribution in both groups (logisticregression analysis, P=0.706 and P=0.481, respectively).
RAGE staining was also observed in uterine tubes of bothH-AGE and control/L-AGE ovaries, without any significantdifferences (logistic regression analysis, P=0.435) in theextension or the localization of immunoreactivity betweenthe two groups.
Discussion
The present study demonstrates for the first time that normalfemale rats exposed to the H-AGE diet for 6 months presentincreased serum AGE levels as well as higher AGE andRAGE deposition in their ovarian tissue compared to L-AGE-fed animals and controls. More specifically, AGE expressionwas stronger in the ovaries of H-AGE-fed rats compared tocontrols and those animals that received the L-AGE diet andin particular in the theca interna cell layer. RAGE stainingwas increased in both granulosa and theca interna cells of H-AGE-fed rats compared to control/L-AGE rats.
It was also found that fasting glucose and insulin levels,as well as the weight of the ovaries, were increased in H-AGE-fed animals compared to the control and L-AGE,despite the fact that there was no increase in their bodyweight, suggesting that this impact is likely to beindependent of the degree of obesity.
The present findings of AGEs deposition in the ovariantissue in conjunction with altered metabolic profile andelevated testosterone levels provide evidence for dual effectof dietary glycotoxins, in reproductive and metabolicaspects of the female rat.
Similarities with the above findings are suggested whenelevated serum AGEs with increased RAGE expression weredemonstrated in women with PCOS, a female syndrome withmetabolic and reproductive abnormalities [17].
Furthermore, in women with PCOS receiving a high-AGE fast food meal, serum AGE levels were increasedpostmeal [19]. Noticeably, AGE levels were positivelycorrelated with insulin resistance indices and hyperandro-genemia in women with PCOS [17, 19, 24]. Similarly, inthe present study, in H-AGE-fed rats, testosterone levelswere positively correlated with the AGE levels and ovarianweight. These findings are also in accordance with theincreased distribution of AGEs and RAGE in theca cells inthe same group of animals compared with the control andL-AGE-fed animals. It is known that theca cells areresponsible for the androgen production in the ovariantissue, and therefore a functional link between the increaseddeposition of AGE and RAGE in theca cells of H-AGE-fedanimals and the increased levels of serum testosteronecannot be excluded.
The immunohistochemistry data of the study indicatethat AGEs appear to be differentially distributed in theovarian tissue. Previous observations have shown increasedAGE deposition in granulosa cells from human polycysticovarian tissue compared to controls [18], whereas in thepresent study, AGEs seem to localize in theca interna cellsof H-AGE-fed normal female rats. It is likely that thesource of AGEs, being either endogenous or exogenous,may play a role in localization of AGEs in the ovarian aswell as in other tissues, as in the previous immunochem-istry study of ovarian tissue, the source of these moleculescould not be defined and the type of diet was not known inPCOS patients from which the ovarian tissue was obtained.
In conclusion, it is demonstrated that excess dietaryglycotoxins in experimental animals appeared to beaccumulated in the ovarian tissues and are also associatedwith metabolic and hormonal alterations. Although it isalways hard to extrapolate from animal studies to humans,these findings in conjunction with human observationalstudies in women with PCOS provide a scientific basis forfurther exploration of the role of dietary glycotoxins onstructural as well as functional alterations in femalereproductive system.
Acknowledgments We thank Christos Adamopoulos and Stelios A.Kandarakis for technical assistance at various stages of this work.
References
1. Vlassara H, Palace MR (2002) Diabetes and advanced glycationendproducts. J Intern Med 251:87–101
2. Baynes JW (2002) The Maillard hypothesis on aging: time tofocus on DNA. Ann NY Acad Sci 959:360–367
3. Vlassara H, Bucala R, Striker L (1994) Pathogenic effects ofadvanced glycosylation: biochemical, biologic, and clinicalimplications for diabetes and aging. Lab Invest 70:138–151
J Mol Med (2007) 85:1413–1420 1419

4. Makino H, Shikata K, Hironaka K (1995) Ultrastructure ofnonenzymatically glycated mesangial matrix in diabetic nephrop-athy. Kidney Int 48:517–526
5. McCance DR, Dyer DG, Dunn JA (1993) Maillard reactionproducts and their relation to complications in insulin-dependentdiabetes mellitus. J Clin Invest 91:2470–2478
6. O’Brien J (1989) Nutritional and toxicological aspects of theMaillard browning reaction in foods. Crit Rev Food Sci Nutr28:211–248
7. Lee T-C, Kimiagar M, Pintauro SJ, Chichester CO (1981)Physiological and safetyaspects of Maillard browning of foods.Prog Food Nutr Sci 5:243–256
8. Cai W, Cao Q, Zhu L, Peppa M, He CJ, Vlassara H (2002)Oxidative stress-inducingcarbonyl compounds from commonfoods: novel mediators of cellular dysfunction. Mol Med 8:337–346
9. Goldberg T, Cai W, Peppa M, Dardaine V, Uribarri J, Vlassara H(2004) Advanced glycoxidation end products in commonlyconsumed foods. J Am Diet Assoc 104:1287–1291
10. Koschinsky T, He CJ, Mitsuhashi T, Bucala R, Liu C, Buenting C,Heitmann, K, Vlassara H (1997) Orally absorbed reactiveglycation products (glycotoxins): an environmental risk factor indiabetic nephropathy. Proc Natl Acad Sci USA 94:6474–6479
11. Lin RY, Dore AT, Ghodsi N, Fallon JT, Fisher EA, Vlassara H(2002) Lowering of dietary advanced glycation end products (AGE)reduces neointimal formation after arterial injury in geneticallyhypercholesterolemic mice. Atherosclerosis 163:303–311
12. Zheng F, He C, Cai W, Hattori M, Steffes M, Vlassara H (2002)Prevention of diabetic nephropathy in mice by a diet low inglycoxidation products. Diabetes Metab Res Rev 18:224–237
13. Vlassara H, Cai W, Crandall J (2002) Inflammatory markers areinduced by dietary glycotoxins: a pathway for acceleratedatherosclerosis in diabetes. Proc Natl Acad Sci USA 99:15596–15601
14. Sandu O, Song K, Cai W, Zheng F, Uribarri J, Vlassara H (2005)Insulin resistance and type 2 diabetes in high-fat-fed mice arelinked to high glycotoxin intake. Diabetes 54:2314–2319
15. Hofmann SM, Dong HJ, Li Z (2002) Improved insulin sensitivityis associated with restricted intake of dietary glycoxidationproducts in the db/db mouse. Diabetes 51:2082–2089
16. Uribarri J, Peppa M, Cai W (2003) Restriction of dietaryglycotoxins reduces excessive advanced glycation end productsin renal failure patients. J Am Soc Nephrol 14:728–731
17. Diamanti-Kandarakis E, Piperi C, Kalofoutis A, Creatsas G(2005) Increased levels of serum advanced glycation end-productsin women with polycystic ovary syndrome. Clin Endocrinol (Oxf)62:37–43
18. Diamanti-Kandarakis E, Piperi C, Patsouris E, Korkolopoulou P,Panidis D, Pawelczyk L, Papavassiliou AG, Duleba AJ (2007)Immunohistochemical localization of advanced glycation end-products (AGEs) and their receptor (RAGE) in polycystic andnormal ovaries. Histochem Cell Biol 127:581–589
19. Diamanti-Kandarakis E, Piperi C, Alexandraki K, KatsilambrosN, Kouroupi E, Papailiou J, Lazaridis S, Koulouri E, KandarakisHA, Douzinas EE, Creatsas G, Kalofoutis A (2006) Short-termeffect of orlistat on dietary glycotoxins in healthy women andwomen with polycystic ovary syndrome. Metabolism 55:494–500
20. Zheng F, He C, Cai W, Hattori M, Steffes M, Vlassara H (2002)Prevention of diabetic nephropathy in mice by a diet low inglycoxidation products. Diabetes/Metab Res Rev 18:224–237
21. Lin R-Y, Reis ED, Dore AT, Lu M, Ghodsi N, Fallon JT (2002)Lowering of dietary advanced glycation endproducts (AGE)reduced neointimal formation after arterial injury in geneticallyhypercholesterolemic mice. Atherosclerosis 163:303–311
22. Krause R, Knoll K, Henle T (2003) Studies on the formation offurosine and pyridosine during acid hydrolysis of differentAmadori products of lysine. Eur J Food Res Technol 216:277–283
23. Resmini P, Pellegrino L, Batelli G (1990) Accurate quantificationof furosine in milk and dairy products by a direct HPLC method.Ital J Food Sci 3:173–183
24. Diamanti-Kandarakis E, Katsikis I, Piperi C, Alexandraki K,Panidis D (2007) Effect of long-term orlistat treatment on serumlevels of advanced glycation end-products in women withpolycystic ovary syndrome. Clin Endocrinol (Oxf) 66:103–109
1420 J Mol Med (2007) 85:1413–1420

ORIGINAL ARTICLE
Celastrol inhibits polyglutamine aggregation and toxicitythough induction of the heat shock response
Yu-Qian Zhang & Kevin D. Sarge
Received: 6 November 2006 /Revised: 6 July 2007 /Accepted: 19 July 2007 / Published online: 18 October 2007# Springer-Verlag 2007
Abstract Heat shock proteins (hsps) are protective againstthe harmful effects of mutant expanded polyglutamine repeatproteins that occur in diseases such as Huntington’s, prompt-ing the search for pharmacologic compounds that increase hspexpression in cells as potential treatments for this and relateddiseases. In this paper, we show that celastrol, a compoundrecently shown to up-regulate hsp gene expression, signifi-cantly decreases killing of cells expressing mutant polyglu-tamine protein. This effect requires the presence of thetranscription factor responsible for mediating inducible hspgene expression, HSF1, and is correlated with decreasedamounts and increased sodium dodecyl sulfate (SDS)solubility of polyglutamine aggregates. These results suggestthe potential of celastrol as a therapeutic agent in the treatmentof human polyglutamine expansion diseases.
Keywords Celastrol . HSF1 . Polyglutamine . Aggregates .
Heat shock proteins . hsp70
Introduction
A large number of neurodegenerative diseases, includingHuntington’s and Kennedy’s diseases, are characterized byexpanded polyglutamine repeats in certain proteins leading totheir aggregation and toxic effects on the cells expressing
them [1, 2]. A number of results suggest that polyglutamine-containing aggregates are important both for the initiationand progression of these diseases [3, 4]. Polyglutamineprotein aggregates in brains of patients and transgenicanimals have been found to contain various molecularchaperones, ubiquitin, and components of the 20S protea-some [5, 6]. This suggests that neuronal cells recognize theprotein aggregates as abnormally folded and try to disag-gregate or degrade the mutant proteins by recruiting
J Mol Med (2007) 85:1421–1428DOI 10.1007/s00109-007-0251-9
Electronic supplementary material The online version of this article(doi:10.1007/s00109-007-0251-9) contains supplementary material,which is available to authorized users.
Y.-Q. Zhang :K. D. Sarge (*)Department of Molecular and Cellular Biochemistry,University of Kentucky,741 S. Limestone Street,Lexington, KY 40536, USAe-mail: [email protected]
KEVIN SARGEreceived his Ph.D. in Bio-chemistry from North Car-olina State University inRaleigh, NC, followed by post-doctoral training at NorthwesternUniversity in Evanston, IL. He iscurrently Professor of Molecularand Cellular Biochemistry at theUniversity of Kentucky, Lexing-ton, KY. His research interestsinclude regulation of stress geneexpression, gene bookmarking,and protein sumoylation.
YU-QIAN ZHANG
received her Bachelor degree inMolecular and Cellular Biologyfrom the University of Scienceand Technology of China in2003. She is currently a Ph.D.candidate in the Department ofMolecular and Cellular Bio-chemistry at the University ofKentucky College of Medicine.Her research interests include theheat shock response in neurode-generative diseases and cancer,protein sumoylation, and tumorimmunology.

chaperones and proteasomal components [7]. Consistentwith this view, increased expression of hsp70 and other heatshock proteins (hsps) has been found to be effective inreducing the toxicity of mutant polyglutamine proteins,suggesting the potential of pharmacological up-regulation ofhsp gene regulation as a means for treating polyglutamineexpansion diseases such as Huntington’s [8–11].
Heat Shock Factor 1, HSF1, is the transcription factorresponsible for up-regulating the expression of hsp70 andother hsp genes in response to cellular stress [12, 13]. HSFactivation involves stress-induced conversion of this factorto its trimeric DNA-binding form [14–17]. The activatedtrimeric HSF1 then binds to heat shock elements in thepromoters of hsp genes to up-regulate their transcription,ultimately leading to elevated levels of cytoprotective hspsin these cells.
The function of HSF1 as a key positive regulator of hspexpression, coupled to the observed ability of hsp proteins toprotect cells from polyglutamine toxicity prompted thehypothesis that interventions that lead to activation of HSF1could provide protection for cells against this toxicity andpossibly represent agents that could be useful in treatingpolyglutamine expansion diseases such as Huntington’s [10,18]. Consistent with this hypothesis, expression in cells of aconstitutively active mutant HSF1 protein results in de-creased polyglutamine toxicity and aggregate formation inboth cell culture and animal models [19, 20]. These andother results have stimulated the search for pharmacologicalcompounds capable of up-regulating hsp gene expression, assuch compounds would theoretically have potential astreatments for these and other diseases of protein misfolding.
Recently, it was demonstrated that a compound calledcelastrol, which is found in the Celastraceae family of plantsand is already being used to treat diseases such as rheumatoidarthritis, bacterial infection, and fever [21, 22], is able toactivate HSF1 and up-regulate hsp gene expression [18].Celastrol has previously been found to inhibit the aggrega-tion of purified Q58-huntingtin 1-171 amino terminalfragment in an in vitro assay, although this study did notexamine effects of celastrol on polyglutamine aggregation incells [23]. Celastrol has also been found to inhibit thecytotoxicity of expanded polyglutamine form of huntingtinexon 1 [24] and androgen receptor [25], but these studies didnot examine the mechanism by which celastrol protects cellsfrom expanded polyglutamine protein cytotoxicity.
The results of the experiments presented in this paperdemonstrate that celastrol is effective in preventing both theaggregation and toxicity of polyglutamine expression incells and that it mediates these effects via the HSF1-mediated gene expression pathway. These results supportthe potential of this drug as a possible therapeutic agent fortreating polyglutamine expansion diseases. The results alsosuggest that other drugs that stimulate HSF1 activity
leading to hsp gene expression may also have beneficialactivity against these disease states as well as other humandiseases that are caused by protein misfolding.
Materials and methods
Plasmids, cell culture, and celastrol
The expression constructs encoding Q19-YFP, Q57-YFP, andQ81-YFP were kindly provided by Dr. James Burke (DukeUniversity). The polyglutamine-YFP (Qn-YFP) vectors wereconstructed using CAG repeats that were synthesized bypolymerase chain reaction (PCR) from human dentatorubralpallidoluysian atrophy (DRPLA) cDNAs containing differ-ent CAG repeats. HeLa cells were cultured in Dulbecco’smodified Eagle’s medium (DMEM; Cellgro) supplementedwith 10% fetal bovine serum (FBS) and 50 μg/mlgentamicin. PC12 cells were cultured in DMEM medium(Cellgro) supplemented with 5% FBS and 10% heat-inactivated horse serum (Gibco), and 100 units/ml Penicillin-Streptomycin (Gibco). HSF1+/+ and HSF1−/−mouse embryofibroblast (MEF) cells (kindly provided by Dr. Ivor Benjamin,University of Utah) were cultured in DMEM medium(Cellgro) supplemented with 10% FBS, 1× Penicillin-streptomycin (Gibco), and 1× Non-essential amino acids(Gibco). Transfection was performed using Effectenetransfection reagent (Qiagen), following the manufacturer’sprotocol. Celastrol (Calbiochem) was dissolved in dimethylsulphoxide at a stock concentration of 5.54 mM.
Trypan blue cell viability assay
Cells were collected by centrifugation at 1,000 rpm for 10 minat 4°C, and the pellet was washed twice with 1× phosphate-buffered saline (PBS). The cell pellet was then resuspended in1× PBS to a concentration of approximately 106 cells/ml. A1:1 dilution of the suspension was prepared using a solutioncontaining 0.4% trypan blue stain (Gibco), and the suspen-sion was then loaded into the counting chamber of ahemocytometer. The number of stained cells as well as thetotal number of cells was counted, and the percentage ofstained cells was taken to represent the percentage of celldeath. Experiments were repeated three times.
Fluorescence microscopy
Cells were seeded on coverslips, and 48 h after transfection,Hoechst 33342 and verapamil were added to the medium tofinal concentrations of 5 and 50 μg/ml, respectively. Afterincubation at 37°C for 30 min, the medium was removed,and the coverslips washed with 1× PBS for 5 min. Asolution containing 3.7% paraformaldehyde in 1× PBS was
1422 J Mol Med (2007) 85:1421–1428

added, and after 20 min incubation at room temperature,coverslips were washed with 1× PBS for 5 min. Coverslipswere washed briefly three times in distilled water andmounted onto a slide spotted with 15 μl Vectashield (VectorLaboratories). Excess fluid was wicked from the coverslipand the edges of the coverslip sealed with fingernail polish.The fluorescence was then visualized using a Nikonfluorescent microscope and pictures taken with a NikonSpotcam digital-imaging camera. To quantify the formationof polyglutamine aggregates, visual fields which containedsimilar numbers of cells (based on the density of nucleistained by Hoechst) were chosen under 20× objective, andthen the number of cells that contained aggregates in eachfield of vision was counted. Three different visual fieldswere quantified in each case. There were approximately300 cells in each visual field for the experiments involvingHeLa cells and PC12 cells, and approximately 100 cells inthe experiments involving MEF cells. We scored a cell aspositive if it had any visible aggregates, and the aggregatesin the majority of cells appeared to be intranuclear orperinuclear (example shown in Fig. S1).
Extract preparation and Western blot assay
Cell lysis was performed on ice for 30 min in 50 mM Tris–HCl [pH 8.0], 100 mM NaCl, 5 mM MgCl2, 0.5% NP40lysis buffer [26] containing 1× protease inhibitor cocktail(Roche), and 1 mM phenylmethanesulfonyl fluoride added.To examine hsp70 level, the cell lysate was cleared bycentrifugation at 1,000 rpm at 4°C for 10 min, and theprotein concentration of the supernatant was then deter-mined by BioRad assay. Five micrograms of protein extractwas subjected to sodium dodecyl sulfate-polyacrylamidegel electrophoresis (SDS-PAGE) and Western blot follow-ing standard procedures. The antibodies and dilutions usedto probe the Western blots were as follows. Anti-hsp70(stress-induced form; Stressgen) was used at 1:10,000, anti-β-actin antibody (Sigma) was used at 1:10,000, and theanti-green fluorescent protein (GFP) polyclonal antibody(Bethyl labs) was used at a dilution of 1:4,000. Hsp70Western blots were quantified using ImageQuant software.
Filtration assay
Cell lysis was performed on ice for 30 min in the lysisbuffer described above. The insoluble fraction was obtainedby centrifugation of the cell lysate at 14,000 rpm at 4°C for10 min. The pellet was resuspended in DNase buffer(20 mM Tris–HCl [pH 8.0], 15 mM MgCl2, and 0.5 mg/mlDNase I), followed by incubation at 37°C for 1 h. AfterDNase treatment, the protein concentration was determinedby analyzing an aliquot using the BioRad assay. Theincubation was terminated by adjusting the mixtures to
20 mM ethylenediamine tetraacetic acid (EDTA), 2%sodium dodecyl sulfate (SDS), and 50 mM dithiothreitoland boiling for 5 min. Thirty micrograms of protein wasdiluted into 200 μl 2% SDS, and this was then filteredthrough a 0.2-μm pore size cellulose acetate membrane(Schleicher & Schuell) that was equilibrated with 2% SDSusing a Dot-Blot system (Schleicher & Schuell). Filterswere washed twice with 200 μl 0.1% SDS and thensubjected to anti-GFP Western blot [27].
SDS solubility assay
To perform the SDS solubility assay, cell lysates wereprepared as described above for the filtration assay,including the 14,000 rpm centrifugation of the cell lysateand DNase treatment and protein concentration determina-tion by BioRad assay. Forty micrograms of protein wasthen adjusted to 2× SDS-PAGE sample buffer (62.5 mMTris·HCl [pH 6.8], 10% glycerol, 2% SDS, 5% β-mercaptoethanol) and boiled for 5 min after which thesample was analyzed by SDS-PAGE and Western blot withanti-GFP polyclonal antibody.
Statistical analysis
Statistical significance was determined using the Student’s ttest. A P value of <0.05 was considered to be statisticallysignificant.
Results
Celastrol protects against polyglutamine toxicity
The experimental system we chose to test for effects ofcelastrol on polyglutamine aggregation and toxicity istransfection of a Q57-YFP fusion protein into cell lines(gift of Dr. James Burke), which is an established model forthe aggregation of polyglutamine containing proteins invivo [28]. Consistent with this, the Q57-YFP protein formsclearly visible aggregates upon expression in HeLa cells,while cells transfected with Q19-YFP exhibit a diffusepattern (Fig. S1). A previous study showed that 8 h ofcelastrol treatment leads to increased levels of the hsp70protein [18]. As the studies described in this paper includecell death and aggregation assays performed at 48 h aftertransfection with the Q57-YFP construct, we wanted toensure that cells treated with celastrol treatment for longertimes also exhibit elevated hsp70 expression. As shown inFig. 1a (upper panel), celastrol treatment of HeLa cells for24 or 48 h both result in a dose-dependent increase inexpression of the hsp70 protein. Quantification of thesehsp70 Western blot results indicates that the induction of
J Mol Med (2007) 85:1421–1428 1423

hsp70 by each celastrol concentration is very similar at 24and 48 h, showing that treatment with this drug results in asustained increase in hsp70 levels (lower panel). Next, totest whether treatment with this drug confers protectionfrom polyglutamine toxicity, HeLa cells were transfectedwith the Q57-YFP construct and then incubated in mediacontaining different concentrations of celastrol. The resultsof this experiment, shown in Fig. 1b, reveal that celastrol
treatment is associated with a significant decrease in deathof these cells expressing this mutant polyglutamine protein.
Celastrol protective effect are correlated with decreasednumber of cells containing polyglutamine aggregates
To determine whether the ability of celastrol to protect cellsfrom polyQ toxicity could be mediated via effects on polyQaggregates, we then examined whether celastrol treatmentalters the number of polyQ aggregates in cells and/or theirsolubility. The results of these experiments show thattreatment with celastrol is associated both with a decreasein the number of cells containing Q57-YFP aggregates, asquantified by fluorescence microscopy (Fig. 2a), and alsowith an increase in the amount of Q57-YFP that can besolubilized from aggregates by SDS treatment (Fig. 2b).SDS solubility of aggregates is related with their toxicity,and data from previous studies suggests that molecularchaperones may ameliorate the neurodegenerative effect ofmutant polyglutamine protein, at least in part, by increasingthe solubility of these proteins [9, 29]. Together, the resultsshown in Figs. 1 and 2 indicate that celastrol treatmentdecreases the death of cells expressing mutant polyglu-tamine protein and also decreases the number of cellscontaining Q57-YFP-aggregates and the insolubility ofQ57-YFP-aggregates.
Protective effects of celastrol treatment in PC12 cells
As the deleterious effects of expression of mutant polyglu-tamine proteins in vivo are observed primarily in cells ofneuronal origin, we next sought to test the effect of celastroltreatment on polyglutamine toxicity and aggregation inPC12 cells. As shown in Fig. 3a, PC12 cells are verysensitive to killing by expression of the Q57-YFP protein,but as observed for HeLa cells in Fig. 1b above, celastroltreatment results in a significant decrease in death of thesecells. As was observed in the experiments using HeLa cells,treatment of PC12 cells with celastrol resulted in asignificant decrease in the number of polyglutamineaggregates in the cells (Fig. 3b) and an increase in theamount of Q57-YFP that can be solubilized from aggre-gates by SDS treatment (Fig. 3c). Interestingly, theconcentrations of celastrol required to achieve these effectson polyglutamine toxicity and number and solubilityproperties of aggregates in PC12 cells were significantlylower than that needed for HeLa cells.
HSF1−/− cells exhibit increased polyglutamine aggregationand toxicity
Inducible hsp expression is thought to be important for theability of cells to decrease polyglutamine toxicity and
Fig. 1 Celastrol treatment reduces Q57-YFP cytotoxicity. a Hsp70 proteinlevel is increased by celastrol treatment. HeLa cells were treated with theindicated concentrations of celastrol for 24 or 48 h, after which cellextracts were made and subjected to Western blot using antibodies againsthsp70 or β-actin (upper panel). These results were quantified using theImageQuant program, and the values for the two treatment times, groupedby celastrol concentration, were graphed (lower panel). b HeLa cells weretransfected with Q57-YFP along with celastrol treatment at the concen-trations indicated. After 48 h, the amount of cell death was determined bytrypan blue assay. Data are shown as means ± SE (*P<0.007, **P<0.004,***P<0.0001, for each celastrol concentration treatment vs no celastrol)
1424 J Mol Med (2007) 85:1421–1428

aggregation [8–11]. Consistent with this hypothesis,HSF1−/− MEFs [30] that are transfected with Q57-YFPexhibit a higher incidence of cell death than HSF1+/+ MEFcells (Fig. 4a). The HSF1−/− MEFs also show increasedQ57-YFP aggregation, both as measured by numbers ofaggregates using fluorescence microscopy of cells (Fig. 4b)and by amount of aggregated Q57-YFP protein present incell extracts detected by filtration assay (Fig. 4c).
Protective effects of celastrol require HSF1
Based on previous results showing the ability of celastrol toactivate HSF1 leading to increased hsp gene expression[18], we hypothesized that this drug’s ability to decreasepolyglutamine toxicity and aggregation shown by the
Fig. 3 Celastrol effects on Q57-YFP toxicity and aggregates in PC12cells. PC12 cells were transfected with Q57-YFP along with celastroltreatment at the concentrations indicated. After 48 h, the amount of celldeath was determined by trypan blue assay (a), the number of cellscontaining Q57-YFP aggregates was quantified using fluorescencemicroscopy (b), and the amount of Q57-YFP monomer solubilized fromaggregates by SDS treatment visualized by Western blot using anti-GFPantibody (c). In a and b, data are shown as means ± SE [*P<0.0001and **P<0.0001 (a), *P<0.001 and **P<0.0001 (b), in each case foreach celastrol concentration treatment vs no celastrol)
Fig. 2 Celastrol treatment reduces number of cells containing Q57-YFP aggregates and increases Q57-YFP solubility. HeLa cells weretransfected with Q57-YFP along with celastrol treatment at theconcentrations indicated. a After 48 h of transfection, the formationof Q57-YFP aggregates was quantified using fluorescence microsco-py. Visual fields which contained similar numbers of cells (based onthe density of nuclei stained by Hoechst) were chosen under 20×objective, and then the number of aggregates in each field of visionwas counted. Three different visual fields were quantified in eachcase, and data are shown as means ± SE (*P<0.004, **P<0.001,***P<0.0003, for each celastrol concentration treatment vs nocelastrol). b To determine the amount of Q57-YFP monomer thatcould be solubilized from aggregates in lysates of the transfected cellsby SDS treatment, the protein concentration of the insoluble fractionof the cell lysates was determined, and then 40 μg of protein wassubjected to SDS solubilization treatment, followed by Western blotusing anti-GFP antibody
J Mol Med (2007) 85:1421–1428 1425

results of Figs. 1, 2, and 3 above could be mediated via theHSF1-regulated gene expression pathway. To test thishypothesis, we compared the effect of celastrol treatmenton polyglutamine toxicity and aggregation in the HSF1+/+vs HSF1−/− MEF cells. Celastrol does not exhibit anytoxicity in HeLa cells at 1.6 μM, but we found its optimalconcentration in MEF cells to be lower than that of HeLacells. Thus, for these experiments, we used 0.4 μMcelastrol treatment, which has no toxic effect in eitherHSF1−/− or wild-type MEFs (data not shown). First,Western blot analysis shows that the HSF1−/− cells areunable to up-regulate hsp70 protein expression in responseto celastrol treatment, demonstrating that celastrol-inducedup-regulation of hsp70 expression is mediated by theHSF1-regulated gene expression pathway (Fig. 5a).
The results shown above (Figs. 1, 2, 3, and 5a) indicate thatcelastrol treatment is effective in preventing polyglutamineaggregation and toxicity and that this drug up-regulates hsp70expression by an HSF1-dependent mechanism. These resultssuggest that celastrol treatment protects cells by stimulatingHSF1-dependent expression of hsps. However, celastrolcould also modulate other cellular activities that couldcontribute to these protective effects. Thus, to test thecontribution of HSF1-regulated pathways in these protectiveeffects, we transfected HSF1+/+ and HSF1−/− MEF cellswith Q57-YFP in combination with celastrol treatment andthen measured the amount of cell death and levels ofaggregated Q57-YFP. The results of this experiment showthat, as it did for the HeLa and PC12 cells in the experimentsof Figs. 1 and 3 above, celastrol treatment resulted indecreased death of HSF1+/+ MEF cells transfected withQ57-YFP, but treatment with this drug did not protect theHSF1−/− cells (Fig. 5b). Consistent with these results, theHSF1+/+ cells, but not the HSF1−/− cells, showed decreasedlevels of aggregated Q57-YFP upon celastrol treatment, asmeasured by the filtration assay (Fig. 5c). These resultssuggest that the HSF1 protein plays an important role in theprotective effects of celastrol against polyglutamine toxicityand aggregation.
Discussion
The results described above indicate that the drug celastrolis able to decrease polyglutamine toxicity, supporting theproposal that this drug could potentially be useful in thetreatment of Huntington’s disease and possibly other humanpolyglutamine expansion disorders. In support of thispossibility, it has been found that celastrol treatment ofmice results in elevation of hsp70 levels in neurons in thebrains of these mice [31]. The results also show that lowerconcentrations of celastrol are required for its protectiveeffects against polyglutamine toxicity in PC12 cells, cells
Fig. 4 HSF1−/− cells exhibit higher Q57-YFP aggregation and celldeath. HSF1−/− and wild-type MEF cells were transfected with Q57-YFP, and after 48 h, cell death was examined by trypan blue assay (a),and the number of cells containing Q57-YFP aggregates wasquantified using fluorescence microscopy (b), or filtration assay, inwhich 30 μg of the insoluble fraction was filtered through 0.2 μmcellulose acetate membrane, and the aggregates retained on themembrane were immunoblotted using anti-GFP antibody (c). In aand b, data are shown as means ± SE. *P<0.008 (a); *P<0.003 (b)
1426 J Mol Med (2007) 85:1421–1428

with neuronal characteristics, compared to other cell types.A particularly beneficial aspect of this drug is that it isalready being used to treat people with other disorders [21,22], and thus it could likely be adapted more quickly foruse in treating polyglutamine expansion diseases than otherdrugs not currently being used in humans.
Results presented in this paper indicate that the protec-tive effect of celastrol against polyglutamine toxicity isassociated with decreased numbers of cells containingaggregates as well as increased SDS-solubility of the
mutant polyglutamine protein. This might seem to be atodds with findings that formation of polyglutamine aggre-gates can be protective for cells expressing these mutantproteins [32–34]. However, our results are consistent withthe findings of a number of studies which indicate thatmolecular chaperones can reduce the formation of polyglu-tamine aggregates and increase the solubility of expandedpolyglutamine proteins [8–11, 19, 20]. While one studyfound that hsp40 overexpression, but not hsp70 over-expression, was associated with reduced aggregation [35],the results of a number of studies do suggest that chap-erones are able to reduce aggregation of mutant polyglu-tamine proteins. Molecular chaperones could be acting atmultiple levels to reduce polyglutamine toxicity, but onepossibility that has been proposed is that these chaperones,and by extension celastrol through its HSF1-mediated up-regulation of chaperones, may be acting at an early step toprevent formation of toxic intermediates before they canbecome part of larger aggregates [8–11, 19, 20]. This wouldexplain both how celastrol treatment protects cells frompolyglutamine toxicity and the effects we observe onpolyglutamine aggregates in the celastrol-treated cells. Analternative explanation that must be considered, in keepingwith previous studies indicating that aggregate formationcan be protective for cells [32–34], is that the results weobserve relating celastrol with the numbers of cellscontaining polyglutamine aggregates could be due, at leastin part, to a potential ability of celastrol to enhance thesurvival of cells that do not contain aggregates, whichwould then lead to a perceived decrease in the numbers ofcells containing aggregates in our experiments. Our data doindicate, however, the protective effects of celastrol withrespect to polyglutamine toxicity.
In addition to its ability to its effects on HSF1activity, celastrol has been found to affect other pathwaysin the cell, including the NF–κB pathway [18, 21, 22,36]. However, our results suggest that the beneficial effectsof celastrol treatment in decreasing polyglutamine toxicityare mediated through the action of the HSF1-regulated geneexpression pathway, based on the finding that celastrol isnot protective in Q57-YFP transfected HSF1−/− MEF cells(Fig. 5b). This finding also suggests that other drugs thatactivate HSF1 could also have potential as candidatetherapeutic agents for treating polyglutamine expansiondiseases.
Acknowledgements We would like to thank Dr. James Burke forproviding polyglutamine-YFP plasmid constructs, Dr. Ivor Benjaminfor providing the HSF1+/+ and HSF1−/− MEF cells, and Dr. DougAndres for providing PC12 cells. We also thank the other members ofour laboratory for insightful discussions during the course of thiswork. This work was supported by NIH grants GM61053 andGM64606 to K.D.S.
Fig. 5 Celastrol decreases Q57-YFP toxicity and aggregation in wild-type but not HSF1−/− MEF cells. a Celastrol treatment does notinduce hsp70 expression in HSF1−/− cells. Wild-type and HSF1−/−MEF cells were treated with no celastrol or 0.4 μM celastrol, and after12 h, cell extracts were made, and 5 μg protein was loaded into eachlane for immunoblotting with anti-hsp70 antibodies. b and c Wild-type and HSF1−/− MEF cells were transfected with Q57-YFP, withcelastrol at the indicated concentrations added at the same time. After48 h, cell death was examined by trypan blue assay (b), with datashown as means ± SE (*P<0.002 for HSF2+/+ 0.4 μM celastrol vs nocelastrol; *P<0.002 for HSF2−/− 0.4 μM celastrol vs no celastrol),and amount of aggregated Q57-YFP was determined by filtrationassay followed by anti-GFP Western blot (c)
J Mol Med (2007) 85:1421–1428 1427

References
1. Bates G (2003) Huntingtin aggregation and toxicity in Huntington’sdisease. Lancet 361:1642–1644
2. Ross CA (2002) Polyglutamine pathogenesis: emergence ofunifying mechanisms for Huntington’s disease and relateddisorders. Neuron 35:819–822
3. Davies SW, Turmaine M, Cozens BA, DiFiglia M, Sharp AH,Ross CA, Scherzinger E, Wanker EE, Mangiarini L, Bates GP(1997) Formation of neuronal intranuclear inclusions underlies theneurological dysfunction in mice transgenic for the HD mutation.Cell 90:537–548
4. Yamamoto A, Lucas JJ, Hen R (2000) Reversal of neuropathologyand motor dysfunction in a conditional model of Huntington’sdisease. Cell 101:57–66
5. Perez MK, Paulson HL, Pendse SJ, Saionz SJ, Bonini NM,Pittman RN (1998) Recruitment and the role of nuclearlocalization in polyglutamine-mediated aggregation. J Cell Biol143:1457–1470
6. Cummings CJ, Mancini MA, Antalffy B, DeFranco DB, Orr HT,Zoghbi HY (1998) Chaperone suppression of aggregation andaltered subcellular proteasome localization imply protein misfold-ing in SCA1. Nat Genet 19:148–154
7. Sittler A, Lurz R, Lueder G, Priller J, Lehrach H, Hayer-HartlMK, Hartl FU, Wanker EE (2001) Geldanamycin activates a heatshock response and inhibits huntingtin aggregation in a cellculture model of Huntington’s disease. Hum Mol Genet 10:1307–1315
8. Meriin AB, Sherman MY (2005) Role of molecular chaperones inneurodegenerative disorders. Int J Hyperthermia 21:403–419
9. Muchowski PJ, Wacker JL (2005) Modulation of neurodegenera-tion by molecular chaperones. Nat Rev Neurosci 6:11–22
10. Westerheide SD, Morimoto RI (2005) Heat shock responsemodulators as therapeutic tools for diseases of protein conforma-tion. J Biol Chem 280:33097–33100
11. Sakahira H, Breuer P, Hayer-Hartl MK, Hartl FU (2002)Molecular chaperones as modulators of polyglutamine proteinaggregation and toxicity. Proc Natl Acad Sci 99:16412–16418
12. Voellmy R (2004) On mechanisms that control heat shocktranscription factor activity in metazoan cells. Cell StressChaperones 9:122–133
13. Pirkkala L, Nykanen P, Sistonen L (2001) Roles of the heat shocktranscription factors in regulation of the heat shock response andbeyond. FASEB J 15:1118–1131
14. Rabindran SK, Haroun RI, Clos J, Wisniewski J, Wu C (1993)Regulation of heat shock factor trimer formation: role of aconserved leucine zipper. Science 259:230–234
15. Sarge KD, Murphy SP, Morimoto RI (1993) Activation of heatshock gene transcription by heat shock factor 1 involvesoligomerization, acquisition of DNA-binding activity, and nuclearlocalization and can occur in the absence of stress. Mol Cell Biol13:1392–1407
16. Baler R, Dahl G, Voellmy R (1993) Activation of human heatshock genes is accompanied by oligomerization, modification, andrapid translocation of heat shock transcription factor HSF1. MolCell Biol 13:2486–2496
17. Westwood JT, Wu C (1993) Activation of Drosophila heat shockfactor: conformational change associated with a monomer-to-trimer transition. Mol Cell Biol 13:3481–3486
18. Westerheide SD, Bosman JD, Mbadugha BN, Kawahara TL,Matsumoto G, Kim S, Gu W, Devlin JP, Silverman RB, MorimotoRI (2004) Celastrols as inducers of the heat shock response andcytoprotection. J Biol Chem 279:56010–56053
19. Rimoldi M, Servadio A, Zimarino V (2001) Analysis of heatshock transcription factor for suppression of polyglutaminetoxicity. Brain Res Bull 56:353–362
20. Fujimoto M, Takaki E, Hayashi T, Kitaura Y, Tanaka Y, Inouye S,Nakai A (2005) Active HSF1 significantly suppresses polyglut-amine aggregate formation in cellular and mouse models. J BiolChem 280:34908–34916
21. Li RL, Shu DF (1989) Investigations and Clinical Applications ofTrysterygium wilfordü hook F. China Science and TechnologyPress, Beijing, China
22. Gunatilaka AAL, Herz W, Kirby GW, Moore RE, Steglich W,Tamm C (1996) Triterpenoid quinonemethides and related com-pounds (Celastroids). Springer, Vienna
23. Wang J, Gines S, MacDonald ME, Gusella JF (2005) Reversal ofa full-length mutant huntingtin neuronal cell phenotype bychemical inhibitors of polyglutamine-mediated aggregation.BMC Neurosci 6:1–12
24. Aiken CT, Tobin AJ, Schweitzer ES (2004) A cell-based screenfor drugs to treat Huntington’s disease. Neurobiol Dis 16:546–555
25. Piccioni F, Roman BR, Fischbeck KH, Taylor JP (2004) A screenfor drugs that protect against the cytotoxicity of polyglutamine-expanded androgen receptor. Hum Mol Genet 13:437–446
26. Sittler A, Walter S, Wedemeyer N, Hasenbank R, Scherzinger E,Eickhoff H, Bates GP, Lehrach H, Wanker EE (1998) SH3GL3associates with the Huntingtin exon 1 protein and promotes theformation of polygln-containing protein aggregates. Mol Cell2:427–436
27. Wanker EE, Scherzinger E, Heiser V, Sittler A, Eickhoff H, LehrachH (1999) Membrane filter assay for detection of amyloid-likepolyglutamine-containing protein aggregates. Methods Enzymol309:375–386
28. Onodera O, Burke JR, Miller SE, Hester S, Tsuji S, Roses AD,Strittmatter WJ (1997) Oligomerization of expanded-polyglutaminedomain fluorescent fusion proteins in cultured mammalian cells.Biochem Biophys Res Commun 238:599–605
29. Chan HY, Warrick JM, Gray-Board GL, Paulson HL, Bonini NM(2000) Mechanisms of chaperone suppression of polyglutaminedisease: selectivity, synergy and modulation of protein solubility inDrosophila. Hum Mol Genet 9:2811–2820
30. McMillan DR, Xiao X, Shao L, Graves K, Benjamin IJ (1998)Targeted disruption of heat shock transcription factor 1 abolishesthermotolerance and protection against heat-inducible apoptosis. JBiol Chem 273:7523–7528
31. Cleren C, Calingasan NY, Chen J, Beal MF (2005) Celastrolprotects against MPTP- and 3-nitropropionic acid-induced neuro-toxicity. J Neurochem 94:995–1004
32. Arrasate M, Mitra S, Schweitzer ES, Segal MR, Finkbeiner S(2004) Inclusion body formation reduces levels of mutanthuntingtin and the risk of neuronal death. Nature 431:805–810
33. Ryan AB, Zeitlin SO, Scrable H (2006) Genetic interactionbetween expanded murine Hdh alleles and p53 reveal deleteriouseffects of p53 on Huntington’s disease pathogenesis. NeurobiolDis 24:419–427
34. Bodner RA, Housman DE, Kazantsev AG (2006) New directionsfor neurodegenerative disease therapy: using chemical compoundsto boost the formation of mutant protein inclusions. Cell Cycle5:1477–1480
35. Zhou H, Li SH, Li XJ (2001) Chaperone suppression of cellulartoxicity of huntingtin is independent of polyglutamine aggrega-tion. J Biol Chem 276:48417–48424
36. Lee JH, Koo TH, YoonH, Jung HS, Jin HZ, Lee K, Hong YS, Lee JJ(2006) Inhibition of NF-kappaB activation through targetingIkappaB kinase by celastrol, a quinone methide triterpenoid.Biochem Pharmacol 72:1311–1321
1428 J Mol Med (2007) 85:1421–1428

RAPID COMMUNICATION
Immunoadsorption and subsequent immunoglobulinsubstitution decreases myocardial gene expressionof desmin in dilated cardiomyopathy
Angela Kallwellis-Opara & Alexander Staudt &Christiane Trimpert & Michel Noutsias & Uwe Kühl &Matthias Pauschinger & Heinz-Peter Schultheiss &
Markus Grube & Michael Böhm & Gert Baumann &
Uwe Völker & Heyo K. Kroemer & Stephan B. Felix
Received: 21 December 2006 /Revised: 30 June 2007 /Accepted: 24 July 2007 / Published online: 9 October 2007# Springer-Verlag 2007
Abstract Cardiac autoantibodies play a pathogenic role indilated cardiomyopathy (DCM). Removal of antibodies byimmunoadsorption (IA) induces hemodynamic improve-ment in DCM patients. The present study investigated theeffects of IA on myocardial gene expression of the inter-
mediate cytoskeletal filament desmin, which is upregulatedin heart failure. RNAwas isolated from five explanted non-failing hearts and five explanted failing hearts of DCMpatients, and myocardial gene expression of desmin was es-timated by real-time polymerase chain reaction (PCR). In acase-control study in six DCM patients (LVEF < 40%,
J Mol Med (2007) 85:1429–1435DOI 10.1007/s00109-007-0263-5
A. Kallwellis-Opara :A. Staudt :C. Trimpert : S. B. FelixDepartment of Internal Medicine B, University of Greifswald,Greifswald, Germany
M. Noutsias :U. Kühl :M. Pauschinger :H.-P. SchultheissDepartment of Cardiology and Pneumology,Charité – University Medicine Berlin,Campus Benjamin Franklin,Berlin, Germany
M. Grube :H. K. KroemerDepartment of Pharmacology, University of Greifswald,Greifswald, Germany
M. BöhmDepartment of Internal Medicine III, University of Saarland,Homburg/Saar, Germany
G. BaumannDepartment of Cardiology, Angiology and Pneumology,Charité – University Medicine Berlin, Campus Mitte,Berlin, Germany
U. VölkerInterfacultary Institute for Genetics and Functional Genomics,University of Greifswald,Greifswald, Germany
S. B. Felix (*)Klinik für Innere Medizin B, University of Greifswald,Friedrich-Loeffler-Strasse 23 a,17475 Greifswald, Germanye-mail: [email protected]
STEPHAN B. FELIXis a Professor of Medicine andCardiology. He is presentlychairman of the Department ofCardiology and Internal Medi-cine B of the University ofGreifswald, Germany. His re-search interests include the mo-lecular pathogenesis of heartfailure. His current research fieldfocuses on characterization ofmyocardial molecular changes indilated cardiomyopathy, and ondevelopment of new treatmentstrategies.
ANGELA KALLWELLIS-OPARA
graduated in human biology andreceived her PhD in molecularbiology from the University ofGreifswald, Germany. Sheworked for 4 years in the De-partment of Cardiology of theUniversity of Greifswald and inthe Department of Cardiologyand Pneumology, Charité, Berlinon the molecular characterizationof dilated cardiomyopathy. She iscurrently working in a sixth formcollege of science in Berlinteaching chemistry and biology.

NYHA II-III), IA and subsequent IgG substitution wereperformed at monthly intervals until month 3. Endomyocar-dial biopsies (EMBs) were obtained before and after IA(after 3–6 months). From six DCM patients without IAtherapy (controls), EMBs were also obtained over a com-parable time interval. Expression of the desmin gene wasanalyzed in these EMBs by real-time PCR. In failing ex-planted hearts, expression of desmin was significantlyincreased (0.88±0.12 vs 0.45±0.15 in non-failing hearts,P < 0.05). After IA, myocardial gene expression of desminwas significantly decreased (from 0.26±0.05 [baseline] to0.14±0.04 [P < 0.05] vs baseline and controls). Removal ofantibodies by IA modulates myocardial gene expression ofdesmin in DCM patients.
Keywords Dilated cardiomyopathy . Immunoadsorption .
Myocardial gene expression . Desmin
Introduction
Dilated cardiomyopathy (DCM) is a chronic myocardialdisease characterized by progressive depression of myocar-dial contractile function and by ventricular dilatation [1]. It isone of the most common myocardial diseases leading toheart transplantation. Disturbances in humoral immunityplay an important role in cardiac dysfunction of DCM pa-tients. A number of autoantibodies against cardiac cell pro-teins have been identified in DCM: e.g., antibodies againstthe cardiac beta-1 adrenergic receptor, contractile proteins,mitochondrial proteins and the muscarinic acetylcholinereceptor-2 [2–7]. Experimental and clinical data indicatethat cardiac antibodies play an active role in the patho-genesis of DCM and may contribute to cardiac dysfunc-tion. Animal models have shown that DCM can betriggered by autoantibodies [8–11]. Recent clinical studiesindicate that cardiac antibodies may play an active role in thepathogenesis and progression of the disease in humans:removal of antibodies by immunoadsorption (IA) induceshemodynamic improvement and ameliorates myocardialinflammation in patients with DCM [12–17]. Elimination ofcardiodepressant antibodies may be one explanation for thebeneficial hemodynamic effects of IA in patients with DCM[15–17].
Previous data indicate that the cytoskeleton, together withcontractile proteins, is a major site of the cellular damage andimpairment of myocyte function in DCM [18–21]. Desminbelongs to the intermediate filaments and is exclusivelyexpressed in muscle cells [22]. An increase in myocardialcytoskeletal proteins, including desmin, has been describedin myocyte hypertrophy and failing hearts [18–21]. More-over, myocardial desmin expression accelerates during tran-sition from compensated ventricular hypertrophy to heart
failure in an experimental model of cardiac hypertrophy [19].In addition, there is inverse correlation between myocardialdesmin expression and left ventricular ejection fraction ofDCM patients [23].
Although the hemodynamic effects of IA have been welldescribed its influence on gene expression remains to beelucidated. To ascertain DCM-associated changes in myocar-dial gene expression, we measured expression of desmin inmyocardial samples obtained from explanted failing and non-failing human hearts. Furthermore, in a separate case-controlstudy, we measured the effects of IA on gene expression ofdesmin in endomyocardial biopsies (EMBs) of DCM patients.
Materials and methods
Myocardial tissue samples from explanted hearts
Human myocardial samples were obtained, as describedbefore, from the left ventricular free wall of five explantednon-failing hearts that were not used for cardiac transplanta-tion and of five explanted failing hearts of DCMpatients [24].The non-failing hearts were obtained from potential donorswithout evidence of heart disease in their medical histories.Echocardiography showed normal fractional shortening andno evidence of regional wall-motion abnormalities or valvedisease. Valves were taken and used for human homografts.Myocardium was used for experimental purposes. Patients diedfrom intracerebral hemorrhage or head injury. The failing heartswere obtained during heart transplantation from patientssuffering from end-stage heart failure due to DCM. In thesepatients, significant stenoses of the coronary arteries were ex-cluded by coronary angiography. Therapy of patients sufferingfrom DCM consisted of digitalis, diuretics, nitrates, β-blockers,and angiotensin-converting enzyme inhibitors. Tissue sampleswere immediately snap-frozen in liquid nitrogen.
Immunoadsorption (IA)
In a case-control study, DCM patients (n=6) were treatedwith Ig-Therasorb (PlasmaSelect, Teterow, Germany), ananti-IgG immunoadsorber, at monthly intervals untilmonth 3, as described previously [13]. After every final IAsession, the patients received 0.5 g/kg polyclonal IgG(Venimmun-N®) for safety reasons to restore IgG plasmalevels and to reduce the risk of infection after immunoglob-ulin depletion. EMBs (five to eight) were obtained from allpatients from the interventricular septum of the rightventricle at baseline before the study began (<7 days), andafter 3–6 months. From age-matched, comparable DCMpatients who were treated only conservatively with stable oralmedication for heart failure (control group, n=6), EMBswere obtained from the interventricular septum of the right
1430 J Mol Med (2007) 85:1429–1435

ventricle at the same time intervals (baseline and after3–6 months) for clinical diagnostic reasons. Patients demon-strated persistent cardiac heart-failure symptoms and dys-function despite stable heart-failure therapy.
Oral medical treatment (β-blockers, ACE inhibitors, anddiuretics) of both groups of DCM patients was comparableand stable for more than 3 months before the study andthroughout the study period. All patients demonstrated leftventricular dysfunction (LVEF < 40%, as assessed by two-dimensional echocardiography), and symptoms of chronicheart failure (New York Heart Association [NYHA] function-al classes II–III). Coronary heart disease was excluded byangiography. Patients were excluded if they had suffered fromactive infectious diseases, cancer, chronic alcoholism, or heartfailure due to known origins (e.g., primary valvular disease).Echocardiography was performed at baseline and after3 months. LVEFwas measured according to the Simpson rule.
RNA isolation
Total RNAwas isolated from human non-failing and failingheart samples and human EMBs by use of a QiagenRNAeasy micro kit (Qiagen, Hilden, Germany) accordingto the manufacturer’s protocol. DNA digestion was included.RNA quantity was determined by A260 measurement. All260/280 nm ratios were above 1.8.
cDNA synthesis and amplification
Limitation in the amount of RNA from EMBs necessitated apreamplification technique. We chose polymerase chainreaction (PCR)-based amplification using the SMART-PCRSynthesis Kit and the Advantage 2 PCR Kit (Clontech, SanJose, CA), which is known to amplify high, medium, and lowtranscripts in a representative manner, and to provide full-length cDNA [25]. Total RNAwas reverse-transcribed usingthe SMART-PCR Synthesis Kit, according to the manufac-turer’s protocol. For PCR-based cDNA amplification, wesubsequently employed an Advantage 2 PCRKit according tothe manufacturer’s protocol. To avoid saturation, we deter-mined the optimal number of PCR cycles to ensure that thecDNAwould remain in the exponential phase of amplificationby real-time PCR and by electrophoresis. The PCR conditionswere 95°C for 1 min, followed by 21 cycles with 95°C for15 s, 65°C for 30 s, and 68°C for 3 min, under the conditionsin which linearity of the amplification was confirmed. Theresulting preamplified cDNAwas purified using the QiaquickPCR Purification Kit (Qiagen, Hilden, Germany).
Relative mRNA quantitation
Using amplified 5 ng cDNA of human heart samples andEMBs, we performed quantitation by using an ABI Prism
7700 sequence detection system (TaqMan®) using the 5′-nuclease activity of TaqDNA polymerase to generate real-time DNA analysis. Amplifications were generated at 2 minat 50°C and 10 min at 95°C, followed by 40 cycles ofdenaturation at 95°C for 15 s, annealing, and synthesis(1 min, 60°C), with use of the TaqMan® universal PCRMaster Mix (Applied Biosystems, Darmstadt, Germany). AllPCR products include an intron–exon breakpoint to avoidamplification of DNA contamination. The primers (humandesmin forward 5′-CGGACGTGGATGCAGCTACT-3′, hu-man desmin reverse 5′- CCTCTTCATGCACTTTCTTAAGGAA-3′, human desmin probe TAMRA/FAM 5′- CCTGGAGCGCAGAATTGAATCTCTCAAC, and commerciallyavailable human GAPDH-primers from Applied Biosystems)were employed in a final concentration of 400 nM. The PCR-reaction products were analyzed on agarose gels stained withethidium bromide. Before the normalization of the expressionof the target gene (desmin) to an internal standard gene[glyceraldehyde-3-phosphate dehydrogenase (GAPDH)] toaccomplish comparative quantitation (ΔCT), we verified thecomparable dose-dependent linear amplification of bothgenes. The TaqMan assay was repeated three times, witheach assay containing duplicate reactions, and with eachassay including an independent amplification of the probes.
Statistics
Results are expressed by mean ± SEM. The paired Wilcoxontest was applied to detect changes in gene expression beforeand after IA. Changes in gene expression in failing hearts vsnon-failing hearts were analyzed by the Mann–Whitney Utest. Significance was assessed at the P < 0.05 level.
Ethics
Written consent was obtained from each patient, and theprotocol was approved by the local Hospital Ethics Committee.The case-control study was performed in accordance with theethical standards laid down in the 1964 Declaration of Helsinki.Furthermore, the Ethics Committee likewise approved the useof samples of explanted hearts for scientific purposes.
Results
Gene expression of desmin in explanted hearts
To study disease-associated changes in desmin gene expres-sion, RNA was isolated from five explanted non-failinghearts and five explanted failing hearts from DCM patients.Expression of desmin which was normalized to GAPDHwassignificantly elevated in failing explanted hearts [0.88±0.12vs 0.45±0.15 (non-failing hearts, P < 0.05)], (Fig. 1).
J Mol Med (2007) 85:1429–1435 1431

The effects of immunoadsorption on myocardial desmingene expression of DCM patients
In both groups at baseline, the following data were com-parable: age, gender, LVEF, oral medication at baseline, andNYHA-classification (Table 1). In the IA group, LVEF in-creased significantly from 27.67±2.71% to 34.00±2.40%(P < 0.05), whereas the LVEF of the control group did notsignificantly change (32.17±1.36% to 32.33±1.54%, n. s.).
At baseline and after 3 months, changes of desmin geneexpression were measured in EMBs of DCM patients treatedwith IA, and of DCM patients without IA treatment. Atbaseline, expression of desmin did not differ significantlybetween the control group and IA group. In the controlgroup, gene expression of desmin increased during the studyperiod (from 0.29±0.03 to 0.42±0.05 n.s. [Fig. 2a]). Incontrast, desmin expression significantly decreased in theIA group after 3–6 months [from 0.26±0.05 to 0.14±0.04,P < 0.05 vs baseline and controls (Fig. 2b)].
Discussion
The cytoskeleton is a well-organized structure whichconsists of microtubules, actin filaments, and intermediatefilaments such as desmin that is exclusively expressed inmuscle cells [22]. Changes within the cardiac cytoskeleton,including the loss of contractile filaments and increase incytoskeletal proteins—which leads to desmin disorganiza-tion and impairment of contractile function—are part of thepathological alteration occurring in heart failure and DCM[18, 20, 21, 23]. In addition to its involvement in cellularstability, the cytoskeleton is also responsible for signal trans-mission from cellular membrane to the nucleus.
The essential role of desmin for cardiac integrity hasbeen investigated in animal models with null mutations ofthe desmin gene. At birth, no anatomical defects areapparent in mice lacking desmin [22]. However, after birth,these mice develop cardiomyopathy, skeletal myopathy, andsmooth muscle dysfunction. These disorders reduce their
Table 1 Baseline characteristics of study population
Characteristics Control group(n=6)
IA group(n=6)
Age 45.3±4.2 41.5±6.3Gender (male/female) 5/1 6/0LVEF (%)a 32.17±1.36 27.67±2.71NYHA functional class (II/III) 2/4 1/5Medicationβ-blocker 6 6ACE-inhibitor 6 6Diuretics 6 6
a LVEF Left ventricular ejection fractionbNYHA New York Heart Association
nonfailing hearts failing hearts0.00
0.25
0.50
0.75
1.00
1.25 *R
elat
ive
desm
in g
ene
expr
essi
on/G
AP
DH
Fig. 1 Desmin gene expression in explanted failing and non-failinghearts. The RNA of explanted non-failing donor hearts (n=5) andDCM hearts (n=5) was isolated and reverse-transcribed. The geneexpression of desmin was quantified relative to GAPDH by real-timePCR (*P < 0.05 vs non-failing hearts)
0.26±0.05
0.14±0.04* #
b
Rel
ativ
e de
smin
gene
expr
essi
on/G
AP
DH
Rel
ativ
e de
smin
gene
expr
essi
on/G
AP
DH
0.29±0.03
0.42±0.05
a
control group control group after 3 month0.0
0.1
0.2
0.3
0.4
0.5
0.6
before IA after IA0.0
0.1
0.2
0.3
0.4
0.5
0.6
Fig. 2 Changes in desmin gene expression during IA. At baseline andafter 3 months, the RNA of endomyocardial biopsies of DCM patientswithout IA (control group, n=6; a) and with IA (IA, n=6; b) wasisolated and reverse-transcribed. The gene expression of desmin wasquantified relative to GAPDH by real-time PCR (*P < 0.05 vsbaseline, #P < 0.05 vs controls)
1432 J Mol Med (2007) 85:1429–1435

life span and make them less tolerant of exercise [22].Furthermore, in animal models, null mutation of the desmingene gives rise to ultrastructural defects in cardiac muscle[26], degeneration of cardiomyocytes, accumulation ofmacrophages, and fibrosis [27]. Mice lacking desmindevelop cardiomyocyte hypertrophy and age-dependentloss of cardiac performance, with chamber dilatation andcompromised systolic function resembling cardiomyopathy[28]. On the other hand, desmin rescue mice withcardiomyocyte-specific desmin expression display a wild-type cardiac phenotype [29]. These findings indicate thatdesmin accumulation is not the cause of myocardialdisease; on the contrary, they demonstrate the cytoprotec-tive effects of the protein and its essential role for cardiacintegrity. The important functional and structural role ofdesmin in cardiac tissue is documented by several differenthereditary desmin missense mutations in humans, resultingin restrictive cardiomyopathy [30] or DCM [31]. Thepathogenic properties of desmin-mutation were shown ina mouse model for desminopathy as well; transgenic micewith a 7-amino acid deletion (D7-des) exhibited structuraldefects of the myocardium that resembled human desmin-related cardiomyopathy with aberrant intrasarcoplasmic andelectron-dense granular filamentous aggregates that weredesmin-positive [32].
Abnormalities of the humoral immune system are presentin patients with DCM, and various antibodies have beenidentified in DCM [2–7]. Animal models further indicatethat under certain pathological conditions, DCM can betriggered by autoantibodies. A recent experimental studyprovided direct evidence that antibodies against the β1-receptor can induce DCM [9]. BALB/c mice, deficient forthe immune-regulatory PD-1 receptor, generate autoanti-bodies against a sarcolemmal protein [10], which wasidentified as cardiac troponin I [11]. These autoantibodiesinduce cardiac dysfunction resembling DCM.
Recent studies demonstrated that IA removes functionalactive antibodies from the plasma of patients with DCM.These antibodies induce a negative inotropic effect in isolatedrat cardiomyocytes through depression of calcium transients;they are furthermore detectable in the majority of DCMpatients [15, 17]. Recent in vitro data indicate that theseantibodies belong to the IgG-3 subclass [16]. Elimination ofantibodies by IA results in hemodynamic improvement anda reduction in myocardial inflammation [12–17]. The IgG,which was substituted for safety reasons after IA [13] mayadditionally influence the immune system through variousmechanisms [33]—and can possibly have beneficial effectsin patients with heart failure [34].
In this study, we investigated the effects of IA on the levelof gene expression. Our findings show that in accordancewith published data, desmin is upregulated in failing DCMhearts [18, 23]. The present study did not ascertain the
function of desmin in DCM and heart failure. Whereas thisprotein plays an essential role for cardiac integrity [22, 26–29, 32], the consequences of desmin upregulation in DCMare still unknown. However, the inverse correlation betweenthe amount of myocardial desmin and the ejection fraction inDCM patients [23] may establish desmin as a valuable myo-cardial marker for cardiac dysfunction. Our study shows forthe first time that specific immunomodulatory therapy—i.e.,removal of antibodies by immunoadsorption and subsequentIgG substitution—induces changes in myocardial gene ex-pression of DCM patients. Parallel to the increase in LVEF,expression of desmin was significantly reduced, indicatingimprovement of left ventricular function.
Medical therapy may modulate desmin gene expression aswell. As was shown recently, initiation of β-blocker therapyinduces changes in myocardial expression of various genes inpatients with DCM [35]. However, our patients had receivedstable oral medication for more than 3 months before thestudy and during the study period. Hence, the present studyexcluded the possibility that an alteration of gene expressionwas induced or modulated by medical therapy or that itreflects the natural course of disease. This conclusion issupported by the fact that patients of the control group withsimilar clinical characteristics and similar medication dem-onstrated no change in desmin transcription.
Study limitations
The present case-control study analyzed changes of myo-cardial gene expression of desmin after IA therapy. It wouldbe of interest to ascertain the influence of IA on the complexpattern of myocardial gene expression by performance ofexpression profiling for a broad spectrum of other genesknown to be involved in development of heart failure. This,however, would be out of the focus of this pilot study thatencompassed only a small number of DCM patients. Large-scale studies should be designed to evaluate changes inmyocardial gene expression on a genome-wide scale. Fur-thermore, as only a small amount of myocardial tissue wasobtained for ethical reasons, assessment of the influence ofIA on protein expression was not feasible.
Conclusions
Findings of the present study indicate that production ofcardiac autoantibodies is involved in DCM-associatedchanges in myocardial gene expression, and in turn, thatremoval of these antibodies by IA may reverse some changesin myocardial gene expression—as shown for the interme-diate cytoskeletal filament desmin. Ongoing studies willanalyze the influence of immunoadsorption on myocardialexpression of further genes.
J Mol Med (2007) 85:1429–1435 1433

Acknowledgements We thank Ms. K. Lissek for her excellent tech-nical assistance.Funding This study has been supported by the Deutsche Forschungs-gemeinschaft through Sonderforschungsbereich/Transregio 19.
References
1. Maron BJ, Towbin JA, Thiene G, Antzelevitch C, Corrado D,Arnett D, Moss AJ, Seidman CE, Young JB (2006) Contemporarydefinitions and classification of the cardiomyopathies. Circulation113:1807–1816
2. Schultheiss HP, Kuhl U, Janda I, Melzner B, Ulrich G, Morad M(1988) Antibody-mediated enhancement of calcium permeabilityin cardiac myocytes. J Exp Med 168:2105–2119
3. Caforio AL, Grazzini M, Mann JM, Keeling PJ, Bottazzo GF,McKenna WJ, Schiaffino S (1992) Identification of alpha- andbeta-cardiac myosin heavy chain isoforms as major autoantigensin dilated cardiomyopathy. Circulation 85:1734–1742
4. Fu ML, Magnusson Y, Bergh CH, Liljeqvist JA, Waagstein F,Hjalmarson A, Hoebeke J (1993) Localization of a functionalautoimmune epitope on the muscarinic acetylcholine receptor-2 inpatients with idiopathic dilated cardiomyopathy. J Clin Invest91:1964–1968
5. Wallukat G, Wollenberger A, Morwinski R, Pitschner HF (1995)Anti-beta 1-adrenoceptor autoantibodies with chronotropic activityfrom the serum of patients with dilated cardiomyopathy: mappingof epitopes in the first and second extracellular loops. J Mol CellCardiol 27:397–406
6. Matsui S, FuML, Shimizu M, Fukuoka T, Teraoka K, Takekoshi N,Murakami E, Hjalmarson A (1995) Dilated cardiomyopathydefines serum autoantibodies against G-protein-coupled cardiovas-cular receptors. Autoimmunity 21:85–88
7. Jahns R, Boivin V, Siegmund C, Inselmann G, Lohse MJ, Boege F(1999) Autoantibodies activating human beta1-adrenergic recep-tors are associated with reduced cardiac function in chronic heartfailure. Circulation 99:649–654
8. Matsui S, Fu ML, Katsuda S, Hayase M, Yamaguchi N, Teraoka K,Kurihara T, Takekoshi N, Murakami E, Hoebeke J, Hjalmarson A(1997) Peptides derived from cardiovascular G-protein-coupledreceptors induce morphological cardiomyopathic changes in immu-nized rabbits. J Mol Cell Cardiol 29:641–655
9. Jahns R, Boivin V, Hein L, Triebel S, Angermann CE, Ertl G,Lohse MJ (2004) Direct evidence for a beta 1-adrenergic receptor-directed autoimmune attack as a cause of idiopathic dilated cardio-myopathy. J Clin Invest 113:1419–1429
10. Nishimura H, Okazaki T, Tanaka Y, Nakatani K, Hara M,Matsumori A, Sasayama S, Mizoguchi A, Hiai H, Minato N,Honjo T (2001) Autoimmune dilated cardiomyopathy in PD-1receptor-deficient mice. Science 291:319–322
11. Okazaki T, Tanaka Y, Nishio R, Mitsuiye T, Mizoguchi A, Wang J,Ishida M, Hiai H, Matsumori A, Minato N, Honjo T (2003)Autoantibodies against cardiac troponin I are responsible for dilatedcardiomyopathy in PD-1-deficient mice. Nat Med 9:1477–1483
12. Dorffel WV, Felix SB, Wallukat G, Brehme S, Bestvater K,Hofmann T, Kleber FX, Baumann G, Reinke P (1997) Short-termhemodynamic effects of immunoadsorption in dilated cardiomy-opathy. Circulation 95:1994–1997
13. Felix SB, Staudt A, Dorffel WV, Stangl V, Merkel K, Pohl M,DockeWD,Morgera S, Neumayer HH,Wernecke KD, Wallukat G,Stangl K, Baumann G (2000) Hemodynamic effects of immunoad-sorption and subsequent immunoglobulin substitution in dilatedcardiomyopathy: three-month results from a randomized study.J Am Coll Cardiol 35:1590–1598
14. Staudt A, Schaper F, Stangl V, Plagemann A, Bohm M, Merkel K,Wallukat G, Wernecke KD, Stangl K, Baumann G, Felix SB(2001) Immunohistological changes in dilated cardiomyopathyinduced by immunoadsorption therapy and subsequent immuno-globulin substitution. Circulation 103:2681–2686
15. Felix SB, Staudt A, Landsberger M, Grosse Y, Stangl V,Spielhagen T, Wallukat G, Wernecke KD, Baumann G, StanglK (2002) Removal of cardiodepressant antibodies in dilatedcardiomyopathy by immunoadsorption. J Am Coll Cardiol39:646–652
16. Staudt A, Bohm M, Knebel F, Grosse Y, Bischoff C, Hummel A,Dahm JB, Borges A, Jochmann N, Wernecke KD, Wallukat G,Baumann G, Felix SB (2002) Potential role of autoantibodiesbelonging to the immunoglobulin G-3 subclass in cardiac dysfunc-tion among patients with dilated cardiomyopathy. Circulation106:2448–2453
17. Staudt A, Staudt Y, Dorr M, Bohm M, Knebel F, Hummel A,Wunderle L, Tiburcy M, Wernecke KD, Baumann G, Felix SB(2004) Potential role of humoral immunity in cardiac dysfunctionof patients suffering from dilated cardiomyopathy. J Am CollCardiol 44:829–836
18. Schaper J, Froede R, Hein S, Buck A, Hashizume H, Speiser B,Friedl A, Bleese N (1991) Impairment of the myocardial ultrastruc-ture and changes of the cytoskeleton in dilated cardiomyopathy.Circulation 83:504–514
19. Collins JF, Pawloski-Dahm C, Davis MG, Ball N, Dorn GW, WalshRA (1996) The role of the cytoskeleton in left ventricular pressureoverload hypertrophy and failure. J Mol Cell Cardiol 28:1435–1443
20. Heling A, Zimmermann R, Kostin S, Maeno Y, Hein S, DevauxB, Bauer E, Klovekorn WP, Schlepper M, Schaper W, Schaper J(2000) Increased expression of cytoskeletal, linkage, and extra-cellular proteins in failing human myocardium. Circ Res 86:846–853
21. Kostin S, Hein S, Arnon E, Scholz D, Schaper J (2000) Thecytoskeleton and related proteins in the human failing heart. HeartFail Rev 5:271–280
22. Paulin D, Li Z (2004) Desmin: a major intermediate filamentprotein essential for the structural integrity and function ofmuscle. Exp Cell Res 301:1–7
23. Di Somma S, Marotta M, Salvatore G, Cudemo G, Cuda G, DeVivo F, Di Benedetto MP, Ciaramella F, Caputo G, de Divitiis(2000) Changes in myocardial cytoskeletal intermediate filamentsand myocyte contractile dysfunction in dilated cardiomyopathy: anin vivo study in humans. Heart 84:659–667
24. Dazert P, Meissner K, Vogelgesang S, Heydrich B, Eckel L, BohmM,Warzok R, Kerb R, Brinkmann U, Schaeffeler E, Schwab M,Cascorbi I, Jedlitschky G, Kroemer HK (2003) Expression andlocalization of the multidrug resistance protein 5 (MRP5/ABCC5), acellular export pump for cyclic nucleotides, in human heart. Am JPathol 163:1567–1577
25. Endege WO, Steinmann KE, Boardman LA, Thibodeau SN,Schlegel R (1999) Representative cDNA libraries and their utilityin gene expression profiling. Biotechniques 26:542–548, 550
26. Milner DJ, Weitzer G, Tran D, Bradley A, Capetanaki Y (1996)Disruption of muscle architecture and myocardial degeneration inmice lacking desmin. J Cell Biol 134:1255–1270
27. Thornell L, Carlsson L, Li Z, Mericskay M, Paulin D (1997) Nullmutation in the desmin gene gives rise to a cardiomyopathy. J MolCell Cardiol 29:2107–2124
28. Milner DJ, Taffet GE, Wang X, Pham T, Tamura T, Hartley C,Gerdes AM, Capetanaki Y (1999) The absence of desmin leads tocardiomyocyte hypertrophy and cardiac dilation with compromisedsystolic function. J Mol Cell Cardiol 31:2063–2076
29. WeislederN, SoumakaE,Abbasi S, TaegtmeyerH,CapetanakY (2004)Cardiomyocyte-specific desmin rescue of desmin null cardiomyopathyexcludes vascular involvement. J Mol Cell Cardiol 36:121–128
1434 J Mol Med (2007) 85:1429–1435

30. Goldfarb LG, Park K-Y, Cervenáková L, Gorokhova S, Lee H-S,Vasconcelos O, Nagle JW, Semino-Mora C, Sivakumar K, DalakasMC (1998) Missense mutations in desmin associated with familialcardiac and skeletal myopathy. Nat Gen 19:402–403
31. Li D, Tapscoft T, Gonzalez O, Burch PE, QuinonesMA, ZoghbiWA,Hill R, Bachinski LL, Mann DL, Roberts R (1999) Desmin mutationresponsible for idiopathic dilated cardiomyopathy. Circulation100:461–464
32. Wang X, Osinska H, Dorn GW, Nieman M, Lorenz JN, GerdesAM, Witt S, Kimball T, Gulick J, Robbins J (2001) Mousemodel of desmin-related cardiomyopathy. Circulation 103:2402–2407
33. Dwyer JM (1992) Manipulating the immune system with immuneglobulin. N Engl J Med 326:107–116
34. Gullestad L, Aass H, Fjeld JG, Wikeby L, Andreassen AK, IhlenH, Simonsen S, Kjekshus J, Nitter-Hauge S, Ueland T, Lien E,Froland SS, Aukrust P (2001) Immunomodulating therapy withintravenous immunoglobulin in patients with chronic heart failure.Circulation 103:220–225
35. Lowes BD, Gilbert EM, Abraham WT, Minobe WA, Larrabee P,Ferguson D, Wolfel EE, Lindenfeld J, Tsvetkova T, Robertson AD,Quaife RA, Bristow MR (2002) Myocardial gene expression indilated cardiomyopathy treated with beta-blocking agents. N Engl JMed 346:1357–1365
J Mol Med (2007) 85:1429–1435 1435