Embed Size (px)
DESCRIPTION
good
Citation preview

217ISSN: 2171-4703© 2013 SECOIRSociedad Española de Cirugía Ocular Implanto-Refractiva
Combined phacoemulsification and viscogoniosynechialysis in primary angle-closure glaucoma
M. Reza Razeghinejad, MD 1
ABSTRACT: The treatment of primary angle-closure glaucoma (PACG) at an early stage prevents a proportion of PACG-related blindness. Several techniques are available with different degrees of success. Trabeculectomy augmented by antifibrotic agents represents the mainstay of glaucoma surgery, but safety and efficacy are suboptimal; phacotrabeculectomy is associated with more postoperative complications; and cataract surgery alone has been shown to reduce IOP, but does nothing with peripheral anterior synechia (PAS). Goniosynechialysis is a procedure designed to break PAS and restore trabecular filtration, but several complications have been reported. In viscogoniosynechialysis (VGS), a viscoelastic agent is used to break the synechia. VGS, when compared to surgical goniosynechialysis is relatively atraumatic procedure that does not require specific surgical instruments, and can be performed at the time of routine phacoemulsification. Combined phacoemulsification and VGS opens the angle and breaks the synechia, leading to IOP reduction. We review the procedure, indications and considerations of VGS and phaco-VGS in the treatment of PACG.
J Emmetropia. 2013; 4: 217-223
Primary angle-closure glaucoma (PACG) may account for half of the subjects with primary glaucoma worldwide. PACG has a high population-attributable risk percentage, which means that if treated at an early stage a significant proportion of PACG-related blindness is preventable1. The risk of visual impairment and blindness is higher in PACG than in primary open-angle glaucoma. It is estimated that PACG blinds five times more people than primary open-angle glaucoma in absolute terms1. The need for innovative advances in the treatment of a particular disease correlates with the prevalence and morbidity of the disease, its economic and social impact, and the efficacy and safety of its current treatments. Accordingly, there is a significant need for newer surgical approaches in the management of PACG.
PACG is mainly attributed to anatomic factors, which finally result in blockage of the trabecular meshwork by the peripheral iris. The anterior chamber
UPDATE/REVIEW
1Poostchi Ophthalmology Research Center, Shiraz University of Medical Sciences, Shiraz, Iran.
Financial disclosure: The authors have no commercial or proprietary interest in the products mentioned herein.
Corresponding Author: M Reza RazeghinejadDept. of Ophthalmology. Khalili Hospital. Shiraz, IranE-mail: [email protected]
is shallower and of smaller volume and the lens is usually thicker than normal and is located in a more anterior position2. A large lens may hinder the access of aqueous humor to the drainage angle and may play a more predominant role in causing elevation of intraocular pressure (IOP) in eyes with a shallow anterior chamber. The continuous increase in the anterior-posterior diameter of the crystalline lens throughout life results in a gradual decrease in anterior chamber depth and volume.
The predisposed patients may present with acute angle-closure (AAC) and chronic angle-closure glaucoma (CACG). In both conditions, conventional management usually starts with a laser iridotomy (LI) and medical therapy. Incisional surgery may be needed if medical or laser treatments do not work. The concurrent existence of cataract and glaucoma is a common finding in the aging population and this trend is likely to increase worldwide as the population ages. Surgical management of patients with coexisting cataract and glaucoma is difficult. The surgeon has three options: performing glaucoma surgery alone followed by later cataract surgery, combined cataract and glaucoma surgery, or cataract surgery alone.
Trabeculectomy augmented by antifibrotic agents represents the mainstay of glaucoma surgery. However, the high complication rate (in particular flat anterior chamber in PACG) and the unpredictable postoperative course and magnitude of IOP reduction led many to consider other treatment strategies3. In addition to

218
JOURNAL OF EMMETROPIA - VOL 4, OCTOBER-DECEMBER
unpredictability, safety and efficacy are suboptimal. Identically performed glaucoma filtering procedures in three different eyes may result in three vastly different outcomes. Moreover, trabeculectomy may accelerate the development and progression of cataract. The Advanced Glaucoma Intervention Study has shown that the risk of developing cataract increased by 78% five years after trabeculectomy4. Combined cataract and glaucoma surgery (phacotrabeculectomy) may achieve greater IOP reduction, but is associated with more postoperative complications than phacoemulsification alone and visual rehabilitation may take longer. Although a combined procedure might be less successful in terms of IOP reduction than trabeculectomy alone, the risk of postoperative hypotony after phacotrabeculectomy may be high for PACG eyes that only need lens extraction but not a glaucoma procedure5. The last option, cataract surgery alone, has been shown to reduce IOP in PACG better than other types of glaucoma. Accumulating evidence indicates that a large and anteriorly positioned lens is responsible for residual angle closure and elevated IOP in post iridotomy eyes. Considering the role the lens plays in angle closure and the fact that cataract extraction yields IOP reduction in PACG, it is likely that widening of the drainage angle contributes to the reduction in postoperative IOP.
Cataract extraction opens the angle, but does nothing with peripheral anterior synechia (PAS). Goniosynechialysis is a procedure designed to break PAS and restore trabecular filtration. Conventionally this has been described using surgical instruments under direct gonioscopic visualization or by Nd:YAG laser6,7. However, complications reported with goniosynechialysis include mild-to-severe hyphema, fibrin exudation, choroidal hemorrhage, choroidal detachment, shallow anterior chamber, and transient elevation of IOP in the immediate postoperative period8. In viscogoniosynechialysis (VGS) an ophthalmic viscoelastic agent is used as a substitute for a surgical instrument to break the synechia9,10. VGS when compared to surgical goniosynechialysis is a quick, relatively atraumatic procedure that does not require specific surgical instruments and can be performed at the time of routine phacoemulsification. Combined phacoemulsification and VGS not only opens the angle but also breaks the synechia and leads to IOP reduction. Finally, preserving the conjunctiva, by using a clear-corneal approach, facilitates any subsequent filtration procedures that may be required.
SURGICAL TECHNIQUE
Performing phacoemulsification in the context of PACG warrants a number of considerations to minimize the risk of complications and adverse events.
Pre-operative considerations
In order to reduce intraoperative complications like choroidal hemorrhage, the IOP should be reduced preoperatively using osmotic agents. This also shrinks the vitreous and may help having a slightly deeper anterior chamber intraoperatively. Placing the patient in a slight reverse-Trendelenburg position on the operating table and using the minimal amount of tension on the lid speculum will also help to reduce posterior positive pressure.
Intraoperative considerations
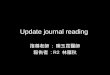
Angle closure glaucoma has some difficult ocular situations for surgery, such as a shallow anterior chamber, the lens often bulky, and the pupil is frequently small from miotic treatment or ischemic iris atrophy. The presence of posterior synechiae, sometimes over the whole 360 degree of the pupillary margin, and a relatively small pupil, which are not unusual findings in patients with CACG, pose daunting difficulties. When necessary, the pupil is dilated with sphincterotomies, stretching the iris with Sinski hooks bimanually, or iris retraction hooks (Figure 1, panels A and B). These may result in an atonic and atrophied iris, which not only has a tendency to plug any surgical wounds and increase the possibility of postoperative uveitis, but also is more prone to further PAS formation. The iris must be dealt with gently to avoid excessive postoperative uveitis.
In those patients that phacoemulsification is not possible because of reduced working space due to crowded anterior chamber, a vitreous tap (a limited pars plana dry vitrectomy) can deepen anterior chamber. In clear cornea temporal phacoemulsification, the entrance into the vitreous cavity can be 3.5 mm posterior to limbus at supero- or inferotemporal quadrants. After performing a dry vitrectomy by vitrectomy machine the anterior chamber is filled with a viscoelastic agent and phacoemulsification is performed. Using a 25-gauge vitrector have the following benefits, easy to perform during anterior segment surgery, the sclerotomy wound requires no sutures, and the minimal conjunctival damage does not hamper future filtration surgery. However, potential complications associated with vitrectomy including retinal detachment and vitreous hemorrhage, should be addressed.
Viscogoniosynechialysis
OVDs have been developed and used primarily for cataract surgery, simply because so many more cataract operations are done, when compared to anything else. Before discussing the use of OVDs for glaucoma
COMBINED PHACO AND VGS IN PACG
JOURNAL OF EMMETROPIA - VOL 4, OCTOBER-DECEMBER
219
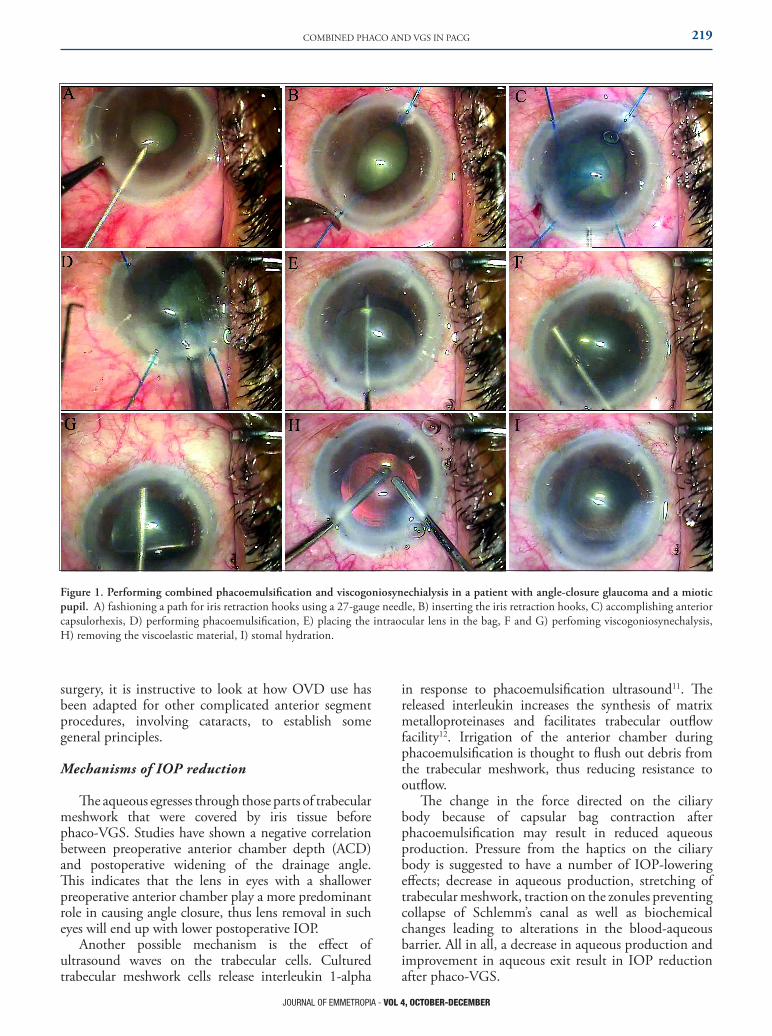
Figure 1. Performing combined phacoemulsification and viscogoniosynechialysis in a patient with angle-closure glaucoma and a miotic pupil. A) fashioning a path for iris retraction hooks using a 27-gauge needle, B) inserting the iris retraction hooks, C) accomplishing anterior capsulorhexis, D) performing phacoemulsification, E) placing the intraocular lens in the bag, F and G) perfoming viscogoniosynechalysis, H) removing the viscoelastic material, I) stomal hydration.
surgery, it is instructive to look at how OVD use has been adapted for other complicated anterior segment procedures, involving cataracts, to establish some general principles.
Mechanisms of IOP reduction
The aqueous egresses through those parts of trabecular meshwork that were covered by iris tissue before phaco-VGS. Studies have shown a negative correlation between preoperative anterior chamber depth (ACD) and postoperative widening of the drainage angle. This indicates that the lens in eyes with a shallower preoperative anterior chamber play a more predominant role in causing angle closure, thus lens removal in such eyes will end up with lower postoperative IOP.
Another possible mechanism is the effect of ultrasound waves on the trabecular cells. Cultured trabecular meshwork cells release interleukin 1-alpha
in response to phacoemulsification ultrasound11. The released interleukin increases the synthesis of matrix metalloproteinases and facilitates trabecular outflow facility12. Irrigation of the anterior chamber during phacoemulsification is thought to flush out debris from the trabecular meshwork, thus reducing resistance to outflow.
The change in the force directed on the ciliary body because of capsular bag contraction after phacoemulsification may result in reduced aqueous production. Pressure from the haptics on the ciliary body is suggested to have a number of IOP-lowering effects; decrease in aqueous production, stretching of trabecular meshwork, traction on the zonules preventing collapse of Schlemm’s canal as well as biochemical changes leading to alterations in the blood-aqueous barrier. All in all, a decrease in aqueous production and improvement in aqueous exit result in IOP reduction after phaco-VGS.
COMBINED PHACO AND VGS IN PACG

220
JOURNAL OF EMMETROPIA - VOL 4, OCTOBER-DECEMBER
Phaco or Phacoviscogoniosynechailysis
Lens extraction alone and its replacement by a much thinner artificial intraocular lens will increase the ACD, but this increase of the ACD is by no means the same as reopening of the closed anterior angle as the angle may remain closed by the PAS. Although cataract extraction in PACG has been shown to be relatively effective in lowering pressure it has also been shown that in glaucoma associated with extensive PAS, removal of lens alone may be insufficient. Lai et al. reported the result of phacoemulsification with posterior chamber intraocular lens implantation and goniosynechialysis followed by diode laser peripheral iridoplasty to the inferior half of the angle in seven patients with CACG and concurrent total synechial angle closure. Postoperative ultrasound biomicroscopy showed that the superior angle, where no goniosynechialysis performed, remained closed. In contrast, the inferior angle in all patients, however, was opened up by the goniosynechialysis13. This confirms the necessity of goniosynechialysis in patients with PACG during cataract surgery. Synechialysis at the end of phacoemulsification compared to phacoemulsification alone in a randomized study revealed greater IOP reduction with less anti-glaucoma medications in the synechialysis group14.
Preoperative evaluation and contraindications
All ocular examinations including visual acuity, IOP, indentation gonioscopy, fundoscopy for evaluating optic nerve and macula, and paraclinical tests such as visual field and optic nerve head imaging are performed to determine the severity of glaucoma. Gonioscopic examination is still the sole means of detecting PAS in the anterior chamber angle. Indentation gonioscopy using lenses with a diameter less than the corneal diameter (i.e. Sussman, Zeiss, Posner) differentiate appositional iridotrabecular contact from PAS. Generally, it is suggested to do phaco-VGS in patients with PAS up to 270 degree9, 10, 14. In other words, at least 90 degree of the angle should be free of PAS and have appositional angle closure. Goniosynechialysis has been described to be effective in patients with PAS that has been present for fewer than 6 to 12 months. However, it is difficult to estimate the duration of PAS, especially in patients with CACG without a history of glaucoma attack. VGS has been reported to be effective in releasing the synechia and reducing IOP disregarding the duration of PAS10,
14, 15. PAS secondary to neovascular glaucoma is a contraindication for phaco-VGS, because of bleeding risk and lack of its effect on releasing the PAS.
Indications
Acute angle-closure
Acute angle-closure is a potentially blinding ocular condition and is regarded as an ocular emergency. As soon as IOP is controlled and sufficient corneal clarity is reestablished, laser iridotomy has been the next step in treatment, with the aim of preventing recurrence of the acute attack, and to prevent progression to CACG. Then, if medical therapy is not effective, laser iridoplasty (Argon or Diode laser; power 200 mw, spot size 500 µm, and duration 0.5 seconds) can be used. Laser iridoplasty mechanically open up the angle in medically resistant AAC. Treatment of only 180 degree of the peripheral iris with iridoplasty may be sufficient to reduce IOP in the majority of AAC cases. In some cases, permanent PAS develop and, when greater than 180 degree of the angle is closed, the IOP rises despite medical therapy or a patent iridotomy. Despite initial medical and laser treatment successes, 38% to 58% of patients may have persistently raised IOP subsequently16, 17.
A treatment dilemma that occurs in patients with AAC is how to treat persistent elevation of IOP despite maximal medical therapy after iridotomy and iridoplasty. Further therapeutic options for these patients include anterior chamber paracentesis, filtering surgery, and/or cataract removal. The presence of two risk factors for cataractogenesis (the acute attack and subsequent trabeculectomy) would suggest that a good proportion of these eyes will eventually require cataract surgery, perhaps placing further trabeculectomy at risk of failure. Phacoemulsification has been shown as an effective and the first procedure in AAC and in patients unresponsive to medical and laser therapies9, 18. Because these patients develop PAS, performing VGS at the end of phacoemulsification will release the synechia. The optimal timing for performing phaco-VGS in AAC is yet unclear. Conceptually, it would be optimal to have the phaco-VGS done after the eye has become quiet. Approximately 1 month after the abortion of the AAC may be a good time.
Chronic angle-closure glaucoma
Chronic angle-closure glaucoma is characterized by increased IOP, PAS, and glaucomatous optic neuropathy. In a patient with CACG and cataract the surgical options include phacotrabeculectomy, phacoemulsification alone, trabeculectomy followed by phacoemulsification, and phaco-VGS. Comparing phacoemulsification alone with phacotrabeculectomy in patients with medically controlled CACG revealed no statistically significant differences between the two treatment groups in terms of visual acuity, progression of glaucomatous optic neuropathy, or visual field loss. Additionally, in the phacotrabeculectomy group more postoperative complications were observed. Although
COMBINED PHACO AND VGS IN PACG

JOURNAL OF EMMETROPIA - VOL 4, OCTOBER-DECEMBER
221
the complications were mostly not serious and did not lead to worse clinical outcomes, these complications resulted in more surgical interventions postoperatively, more clinic visits, and delayed rehabilitation5. In another study comparing phacoemulsification alone with phacotrabeculectomy in patients with medically uncontrolled CACG, IOP and number of medications were lower in the phacotrabeculectomy group. However, phacotrabeculectomy was associated with more postoperative complications and more progression of optic neuropathy19. Phacoemulsification has been shown to result in greater opening of drainage angle and deepening of anterior chamber than combined phaco-trabeculectomy20. A possible explanation may be the shallow anterior chamber after phacotrabeculectomy, due to the drainage of aqueous from anterior chamber by trabeculectomy. The shallow anterior chamber may also aggravate the extent of PAS. Gunning and Greve advocated cataract extraction with IOL implantation alone for subacute or CACG, because cataract extraction reduced IOP to the same extent as filtering surgery, but with fewer complications21.
Postoperative care
Postoperatively, a topical antibiotic and steroid are started and based on the amount of ocular inflammation the steroid dosage is titrated. All anti-glaucoma medications can be discontinued and resumed at the follow-up as necessary to control the IOP according to its level. The other option is starting acetazolamide tablet for the first two postoperative days to combat the IOP spike secondary to the remaining viscoelastic agent. The second option seems to be a safe modality, especially in patients with severe glaucomatous optic neuropathy. The IOP should be checked regularly because the studies reveled that there is not a clear correlation of the IOP with the extent of angle closure. Some eyes with only 90 degree angle closure after cataract extraction may require anti-glaucoma medications to control the IOP but some eyes with more than 270 degree angle closure may not22.
Uncontrolled IOP after phaco-VGS
The maximum IOP reduction after phacoemulsification in a group of patients with occludable angle was detected at week 12 after operation23. Gonioscopic findings may not truly reflect the extent of damage in the trabecular outflow pathway as there is loss of trabecular cells and irregular architecture of the trabeculum in areas away from visible PAS. Not all patients with PACG respond to phaco-VGS. If the IOP is not controlled even after addition of medical therapy, trabeculectomy may be performed as a second-stage procedure. Subsequent glaucoma surgery can be achieved safely because of the deepened
anterior chamber and intact conjunctiva. Furthermore, the fibrosed pseuophakos-capsular membrane would add stability to the anterior segment (compared with a large crystalline lens suspended from the zonule) and trabeculectomy would in theory carry a lower risk of encountering a shallow anterior chamber in the postoperative period.
Complications
Corneal endothelial cell loss seems to be more in PACG patients who undergo phacoemulsification. These eyes have characteristically shallow anterior chambers, which may render anterior chamber surgical maneuvers more difficult and risky. This provides less room for maneuvering the nucleus, and forces the phaco surgeon to apply ultrasonic power closer to the corneal endothelium. This may aggravate corneal endothelial cell loss. This is expected to be a more significant problem in eyes with previous AAC attack because endothelial cell count in these eyes may have already been reduced as a result of previous episodes of acutely raised IOP. Endothelial cell damage after AAC is well documented, with average decreases in cell density of up to 33%24. The amount of endothelial cell loss correlates closely with the duration of IOP elevation. Eyes with CACG, especially those with previous episodes of AAC, often have lower corneal endothelial cell density and are therefore more prone to intraoperative and postoperative corneal edema. The expertise of surgeon in performing a fast and precise operation is important in saving the corneal endothelial cells. To minimize corneal endothelial cell damage, it is critical to avoid an IOP spike in the early postoperative period as well25.
Anterior capsular tear secondary to posterior positive pressure intraoperatively and anterior vaulting of the lens is another potential complication. As stated in the surgical technique section, performing a dry vitrectomy to reduce IOP and deep the anterior chamber, and fashioning a smaller capsulorhexis can prevent this complication.
Transient IOP elevation after phaco-VGS is mainly due to remained viscoelastic agents. Removing the viscoelastic agent at the end of surgery can prevent this event largely.
Fibrin formation in the anterior chamber is another reported complication. In a series of patients, all patients with postoperative fibrin and reaction in the anterior chamber had been on Latanoprost eye drop preoperatively10. Viscoelastic material, intraocular lens, and disruption of blood-aqueous barrier are other suggested mechanisms. Treatments include topical steroid, intracameral streptokinase (500 - 1000 IU), recombinant tissue plasminogen activator (20 µg), subtenon steroid, and disruption of the fibrin membrane with Nd:YAG laser10, 26, 27.
COMBINED PHACO AND VGS IN PACG

222
JOURNAL OF EMMETROPIA - VOL 4, OCTOBER-DECEMBER
Cystoid macular edema may occur after cataract surgery, but seems to be more common in PACG patients who undergo phaco-VGS. The disruption of blood-aqueous barrier secondary to IOP rise and anti-glaucoma medications (mainly their preservatives) seems to be inciting factors. Latanoprost therapy enhances disruption of the blood-aqueous barrier and increases the incidence of angiographic cystoids macular edema28. The usual presentation is a drop in visual acuity after a period of having a good vision postoperatively. Optical coherent tomography of macular area is a non-invasive and sensitive tool for assessing macular edema. The suggested therapies are topical non-steroidal anti-inflammatory drugs, corticosteroid intravitreal injections and implants, and intravitreal anti-vascular endothelial growth factor29.
CONCLUSION
Cataract extraction itself can reduce the IOP and open the angle in many patients with narrow/ closed angles. However, without further angle procedures to release the PAS it is unusual to get a large pressure drop. Combined phaco-VGS is a safe and an easy to do procedure. Phaco-VGS has the following advantages over phacotrabeculectomy: avoidance of trabeculectomy complications, substantial saving in operation time, reduction in the number of postoperative visits, and restoration of normal outflow by VGS. After phaco-VGS, not only is the IOP reduced, the requirement for the number of anti-glaucoma medications decreases significantly. This can help in improving the quality of life of the patients as the side effects, inconvenience, and economic burden of these medications can be avoided. Contrary to trabeculectomy that induces trabecular meshwork hypoperfusion and possibly worsen its function, phaco-VGS induces favorable changes in the anterior chamber configuration. It seems wise to do phaco-VGS as the first procedure and if IOP is not controlled with medications proceed to trabeculectomy. When filtering surgery alone is performed, functioning filtering blebs may become smaller or even vanish after later cataract surgery.
Considering the number of people affected by PACG, the role of the lens in pathogenesis, as well as ready availability of competent cataract surgeons, the physicians should not hesitate to postpone this IOP reducing procedure in a patient with uncontrolled PACG. Most ophthalmologists are able to do a relatively safe cataract surgery, whereas a minority of non-glaucoma specialists can cope with turbulences after glaucoma surgical intervention. The evidence suggests that cataract surgery combined with VGS should always be considered first in the treatment of PACG. However, the concept of primary clear lens surgery for treating
angle-closure glaucoma remains a subject of debate. The benefits of primary clear lens surgery in eyes with uncontrolled AAC and CACG should be weighed against accommodation loss, technical difficulties, and potential intra- and postoperative complications.
REFERENCES1. Thomas R, Sekhar GC, Kumar RS. Glaucoma management in
developing countries: medical, laser, and surgical options for glaucoma management in countries with limited resources. Curr Opin Ophthalmol. 2004; 15:127-31.
2. Marchini G. Biometric data and pathogenesis of angle closure glaucoma. Acta Ophthalmol Scand Suppl. 2002; 236:13-4.
3. Razeghinejad MR, Fudemberg SJ, Spaeth GL. The changing conceptual basis of trabeculectomy: a review of past and current surgical techniques. Surv Ophthalmol. 2012; 57:1 25.
4. The Advanced Glaucoma Intervention Study: 8. Risk of cataract formation after trabeculectomy. Arch Ophthalmol. 2001; 119:1771-9.
5. Tham CC, Kwong YY, Leung DY, et al. Phacoemulsification versus combined phacotrabeculectomy in medically controlled chronic angle closure glaucoma with cataract. Ophthalmology. 2008; 115:2167-2173 e2.
6. Shingleton BJ, Chang MA, Bellows AR, Thomas JV. Surgical goniosynechialysis for angle-closure glaucoma. Ophthalmology. 1990; 97:551-6.
7. Senn P, Kopp B. Nd:YAG laser synechiolysis in glaucoma due to iridocorneal angle synechiae. Klin Monbl Augenheilkd. 1990; 196:210-3.
8. Tanihara H, Negi A, Akimoto M, Nagata M. Long-term results of non-filtering surgery for the treatment of primary angle-closure glaucoma. Graefes Arch Clin Exp Ophthalmol. 1995; 233:563-7.
9. Razeghinejad MR. Combined phacoemulsification and viscogoniosynechialysis in patients with refractory acute angle-closure glaucoma. J Cataract Refract Surg. 2008; 34:827-30.
10. Razeghinejad MR, Rahat F. Combined phacoemulsification and viscogoniosynechialysis in the management of patients with chronic angle closure glaucoma. Int Ophthalmol. 2010; 30:353-9.
11. Wang N, Chintala SK, Fini ME, Schuman JS. Ultrasound activates the TM ELAM-1/IL-1/NF-kappaB response: a potential mechanism for intraocular pressure reduction after phacoemulsification. Invest Ophthalmol Vis Sci. 2003; 44:1977-81.
12. Meyer MA, Savitt ML, Kopitas E. The effect of phacoemulsification on aqueous outflow facility. Ophthalmology. 1997; 104:1221-7.
13. Lai JS, Tham CC, Chua JK, Lam DS. Efficacy and safety of inferior 180 degrees goniosynechialysis followed by diode laser peripheral iridoplasty in the treatment of chronic angle-closure glaucoma. J Glaucoma. 2000; 9:388-91.
14. Varma D, Adams W, Bunce C, Phelan P, Fraser S. Viscogonioplasty in narrow angle glaucoma: a randomized controlled trial. Clin Ophthalmol. 2010; 4:1475-9.
15. Varma D, Adams WE, Phelan PS, Fraser SG. Viscogonioplasty in patients with chronic narrow angle glaucoma. Br J Ophthalmol. 2006; 90:648-9.
16. Lam DS, Lai JS, Tham CC, Chua JK, Poon AS. Argon laser peripheral iridoplasty versus conventional systemic medical therapy in treatment of acute primary angle-closure glaucoma: a prospective, randomized, controlled trial. Ophthalmology. 2002; 109:1591-6.
COMBINED PHACO AND VGS IN PACG

JOURNAL OF EMMETROPIA - VOL 4, OCTOBER-DECEMBER
223
17. Aung T, Ang LP, Chan SP, Chew PT. Acute primary angle-closure: long-term intraocular pressure outcome in Asian eyes. Am J Ophthalmol. 2001; 131:7-12.
18. Imaizumi M, Takaki Y, Yamashita H. Phacoemulsification and intraocular lens implantation for acute angle closure not treated or previously treated by laser iridotomy. J Cataract Refract Surg 2006; 32:85-90.
19. Tham CC, Kwong YY, Leung DY, et al. Phacoemulsification versus combined phacotrabeculectomy in medically uncontrolled chronic angle closure glaucoma with cataracts. Ophthalmology. 2009; 116:725-31, 731 e1-3.
20. Tham CC, Leung DY, Kwong YY, Li FC, Lai JS, Lam DS. Effects of phacoemulsification versus combined phaco-trabeculectomy on drainage angle status in primary angle closure glaucoma (PACG). J Glaucoma. 2010; 19:119-23.
21. Gunning FP, Greve EL. Lens extraction for uncontrolled angle-closure glaucoma: long-term follow-up. J Cataract Refract Surg. 1998; 24:1347-56.
22. Lai JS, Tham CC, Chan JC. The clinical outcomes of cataract extraction by phacoemulsification in eyes with primary angle-closure glaucoma (PACG) and co-existing cataract: a prospective case series. J Glaucoma. 2006; 15:47-52.
23. Shin HC, Subrayan V, Tajunisah I. Changes in anterior chamber depth and intraocular pressure after phacoemulsification in eyes with occludable angles. J Cataract Refract Surg. 2010; 36:1289-95.
24. Markowitz SN, Morin JD. The endothelium in primary angle-closure glaucoma. Am J Ophthalmol. 1984; 98:103-4.
25. Ko YC, Liu CJ, Lau LI, Wu CW, Chou JC, Hsu WM. Factors related to corneal endothelial damage after phacoemulsification in eyes with occludable angles. J Cataract Refract Surg. 2008; 34:46-51.
26. Mullaney PB, Wheeler DT, al-Nahdi T. Dissolution of pseudophakic fibrinous exudate with intraocular streptokinase. Eye (Lond). 1996; 10:362-6.
27. Siatiri H, Beheshtnezhad AH, Asghari H, Siatiri N, Moghimi S, Piri N. Intracameral tissue plasminogen activator to prevent severe fibrinous effusion after congenital cataract surgery. Br J Ophthalmol. 2005; 89:1458-61.
28. Yeh PC, Ramanathan S. Latanoprost and clinically significant cystoid macular edema after uneventful phacoemulsification with intraocular lens implantation. J Cataract Refract Surg. 2002; 28:1814-8.
29. Yonekawa Y, Kim IK. Pseudophakic cystoid macular edema. Curr Opin Ophthalmol. 2012; 23:26-32.
First author:
M. Reza Razeghinejad, MD
Poostchi Ophthalmology Research Center, Shiraz University of Medical Sciences, Shiraz, Iran.
COMBINED PHACO AND VGS IN PACG