Embed Size (px)
Citation preview
JSLS
Laparoscopic Exploration in the Management ofRetroperitoneal Masses
Arieh L. Shalhav MD, Steve W.H. Chan, MD, Eduardo Bercowsky MD,Abdelhamid M. Elbahnassy, MD, Elspeth M. McDougall, MD, Ralph V. Clayman, MD
ABSTRACT
Background and Objectives: The isolated finding of aretroperitoneal mass (RM) often represents a diagnosticchallenge. Image-guided biopsy is frequently inadequatefor diagnosis. With increasing experience, the use oflaparoscopy for exploration of an indeterminate RM mayprovide a minimally invasive alternative to open explo-ration. Herein, we present a retrospective review of ourinitial four laparoscopic explorations, comparing ourexperience to four contemporary open explorations foran RM.
Patients and Methods: From July 1995 to January 1998,four patients, aged 50 to 62 years old, with an RM ofundetermined etiology underwent laparoscopic explo-ration. Another four patients underwent open explo-ration at the same hospital. The medical records of thesepatients were reviewed.
Results: The tumors were smaller in the laparoscopicgroup, averaging 3.7 cm (range 2-6 cm) vs 6.5 cm (range1-10 cm) in the open group. A definitive diagnosis wasobtained for all eight patients. Postoperative complica-tions were observed in one of the laparoscopic explo-rations, and in three of the open explorations; there wasno operative mortality. The blood loss (90 vs 440 ml),fall in hematocrit (5.1 vs 7.8%), time to resumption of aregular diet (3 vs 5 days), amount of morphine sulfateequivalents required for analgesia (128 mg vs 161 mg),time to ambulation (2.3 vs 6 days) and hospital stay (4.8vs 6 days) were all less among the laparoscopy patients.However, the operative time was longer for the laparo-scopic procedure; this time included stent placement andpatient repositioning in addition to the time for laparo-scopic excision of the mass (7.8 vs 4.3 hours).
Conclusion: Laparoscopic exploration appears to be aviable alternative to open exploration in patients pre-senting with a retroperitoneal mass. It is as effective as
Department of Surgery, Division of Urology, Washington University School ofMedicine, St. Louis, Missouri.
Address reprint request to: A.L. Shalhav, MD, Division of Urology, WashingtonUniversity, 4960 Children's Place, Saint Louis, MO 63110, USA.
an open procedure and provides benefits with regard topatient morbidity and convalescence. However, opera-tive time for this laparoscopic procedure is lengthy.
Key Words: Surgical procedures, Laparoscopic,Retroperitoneal neoplasms.
INTRODUCTION
The isolated finding of a retroperitoneal mass (RM) oftenrepresents a diagnostic challenge. Even when possible,an image-guided biopsy frequently provides an inade-quate specimen for diagnostic purposes. Open retroperi-toneal exploration is often the only option capable ofobtaining sufficient tissue for diagnosis; however, thisnecessitates a major operation.
With increasing experience in laparoscopic retroperi-toneal surgery,1,2 the use of laparoscopy for explorationof an indeterminate retroperitoneal mass may provide aminimally invasive alternative to open exploration.Herein, we report our experience with four laparoscop-ic explorations for RM and compare our results with fourcontemporary open explorations for RM.
PATIENTS AND METHODS
From July 1995 to January 1998, four consecutivepatients, aged 50 to 62 years old, with computed tomo-graphic findings of a retroperitoneal mass underwentlaparoscopic exploration by one surgeon (RVC).Another four consecutive patients underwent openexploration by other surgeons at the same hospital. Themedical records of these patients were reviewed.
Preoperative evaluation included computed tomographyof the abdomen and chest radiography. In each case, theonly finding was a retroperitoneal mass (Figure 1). Inthe laparoscopic group, all patients had either preopera-tive biopsy of the mass or a biopsy of an enlargedperipheral lymph node.
For laparoscopic exploration, all patients underwentplacement of a ureteral stent and Foley catheter. The
JSLS (1999)3:209-214 209
Laparoscopic Exploration in the Management of Retroperitoneal Masses, Shalhav AL et al.
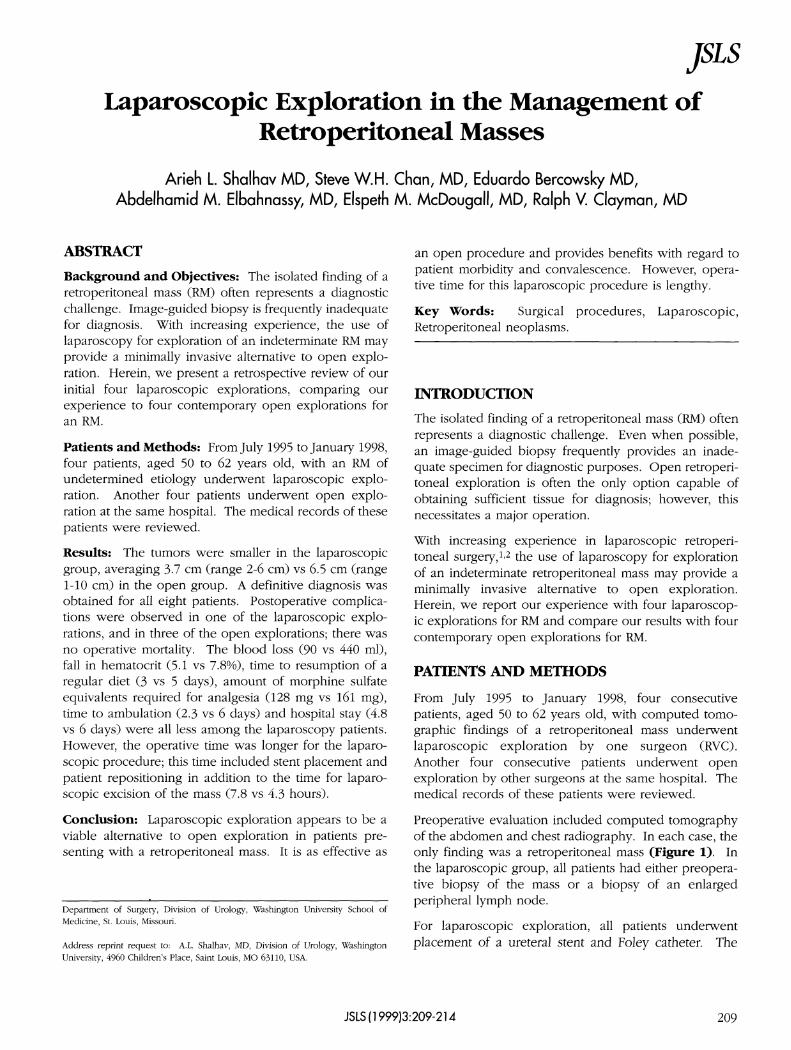
Figure 1. A, B. Preoperative CT of patient #3 showing a 4 cmleft retroperitoneal mass located posterior to the renal hilum andlateral to the aorta; renal vessels are displaced anterior.
patient was then turned from a supine to a full lateralposition. A pneumoperitoneum was created with aVeress needle inserted 3 cm above and medial to theanterior superior iliac spine; a 12 mm port was placed.Additional 12 mm ports were placed in the mid-clavicu-lar line subcostally and just above and lateral to theumbilicus. The colon was mobilized medially by incis-ing the line of Toldt. Another 5 mm port was placed inthe posterior axillary line subcostally for placement of a5 mm retractor. The colonic mesentery was further sep-arated from Gerota's fascia; the mass was identified and
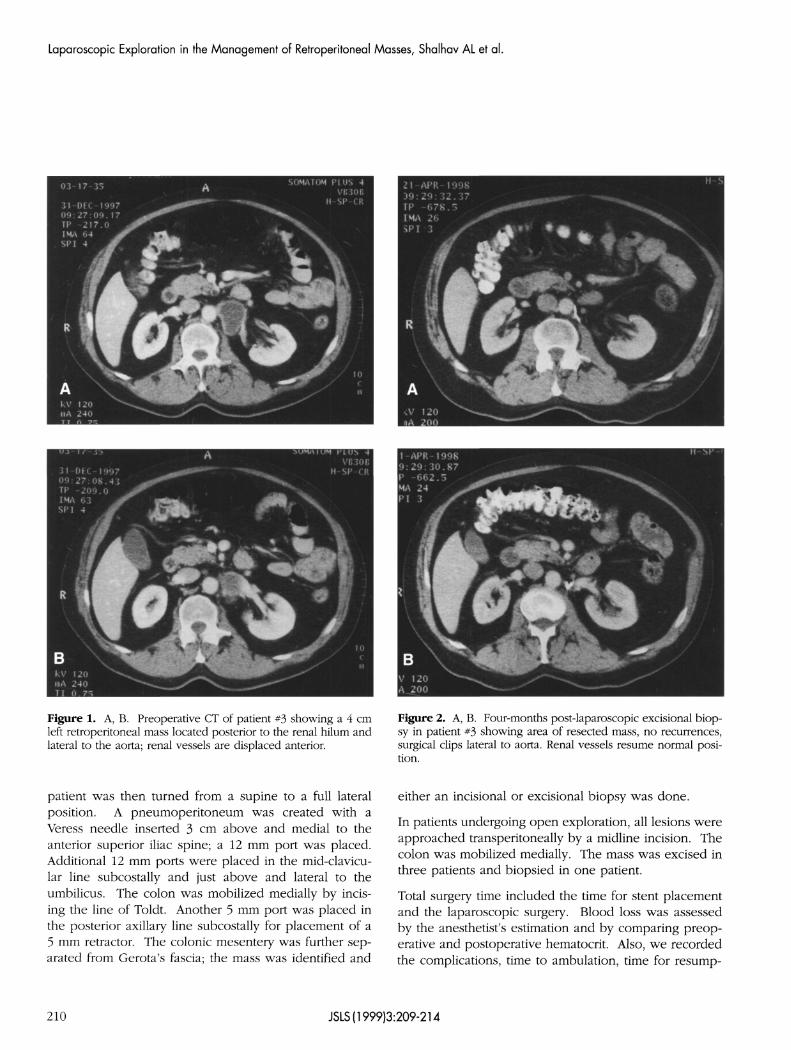
Figure 2. A, B. Four-months post-laparoscopic excisional biop-sy in patient #3 showing area of resected mass, no recurrences,surgical clips lateral to aorta. Renal vessels resume normal posi-tion.
either an incisional or excisional biopsy was done.
In patients undergoing open exploration, all lesions wereapproached transperitoneally by a midline incision. Thecolon was mobilized medially. The mass was excised inthree patients and biopsied in one patient.
Total surgery time included the time for stent placementand the laparoscopic surgery. Blood loss was assessedby the anesthetist's estimation and by comparing preop-erative and postoperative hematocrit. Also, we recordedthe complications, time to ambulation, time for resump-
210 JSLS(1999)3:209-214
JSLS
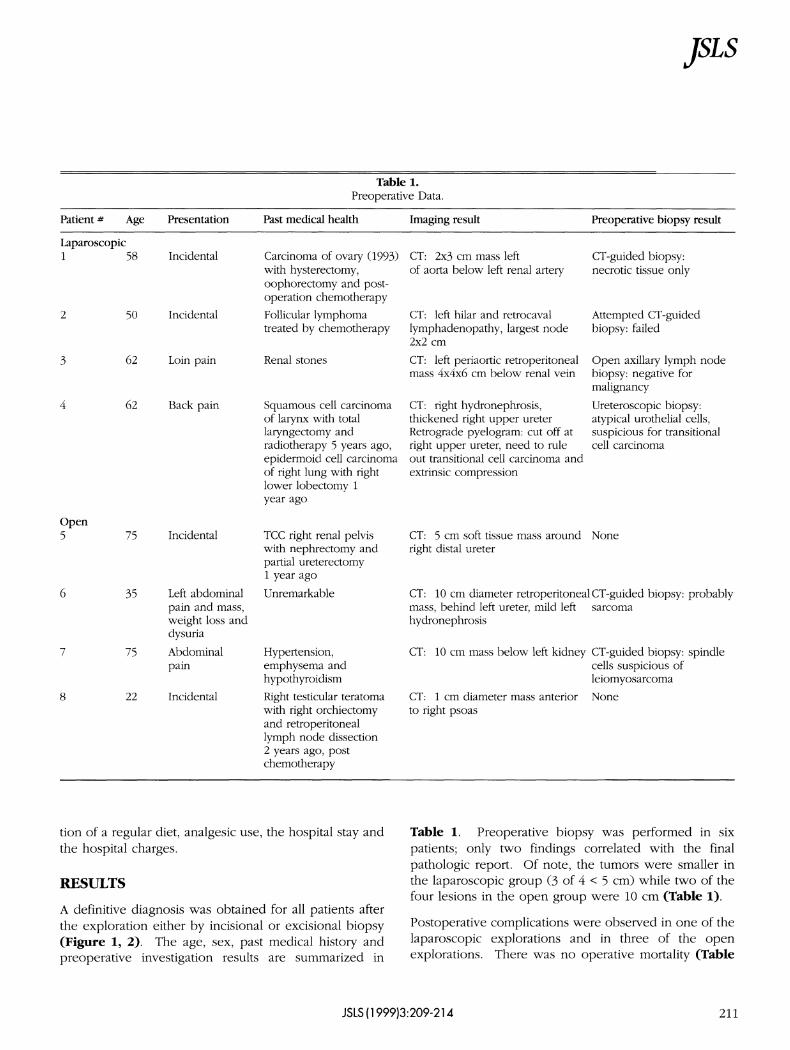
Table 1.Preoperative Data.
Patient # Age
Laparoscopic1
2
3
4
Open5
6
7
8
58
50
62
62
75
35
75
22
Presentation
Incidental
Incidental
Loin pain
Back pain
Incidental
Left abdominalpain and mass,weight loss anddysuria
Abdominalpain
Incidental
Past medical health
Carcinoma of ovary (1993)with hysterectomy,oophorectomy and post-operation chemotherapyFollicular lymphomatreated by chemotherapy
Renal stones
Squamous cell carcinomaof larynx with totallaryngectomy andradiotherapy 5 years ago,epidermoid cell carcinomaof right lung with rightlower lobectomy 1year ago
TCC right renal pelviswith nephrectomy andpartial ureterectomy1 year ago
Unremarkable
Hypertension,emphysema andhypothyroidism
Right testicular teratomawith right orchiectomyand retroperitoneallymph node dissection2 years ago, postchemotherapy
Imaging result
CT: 2x3 cm mass leftof aorta below left renal artery
CT: left hilar and retrocavallymphadenopathy, largest node2x2 cm
CT: left periaortic retroperitonealmass 4x4x6 cm below renal vein
CT: right hydronephrosis,thickened right upper ureterRetrograde pyelogram: cut off atright upper ureter, need to ruleout transitional cell carcinoma andextrinsic compression
CT: 5 cm soft tissue mass aroundright distal ureter
CT: 10 cm diameter retroperitonealmass, behind left ureter, mild lefthydronephrosis
CT: 10 cm mass below left kidney
CT: 1 cm diameter mass anteriorto right psoas
Preoperative biopsy result
CT-guided biopsy:necrotic tissue only
Attempted CT-guidedbiopsy: failed
Open axillary lymph nodebiopsy: negative formalignancy
Ureteroscopic biopsy:atypical urothelial cells,suspicious for transitionalcell carcinoma
None
CT-guided biopsy: probablysarcoma
CT-guided biopsy: spindlecells suspicious ofleiomyosarcoma
None
tion of a regular diet, analgesic use, the hospital stay andthe hospital charges.
RESULTS
A definitive diagnosis was obtained for all patients afterthe exploration either by incisional or excisional biopsy(Figure 1, 2). The age, sex, past medical history andpreoperative investigation results are summarized in
Table 1. Preoperative biopsy was performed in sixpatients; only two findings correlated with the finalpathologic report. Of note, the tumors were smaller inthe laparoscopic group (3 of 4 < 5 cm) while two of thefour lesions in the open group were 10 cm (Table 1).
Postoperative complications were observed in one of thelaparoscopic explorations and in three of the openexplorations. There was no operative mortality (Table
JSLS (1999)3:209-214 211
Laparoscopic Exploration in the Management of Retroperitoneal Masses, Shalhav AL et al.
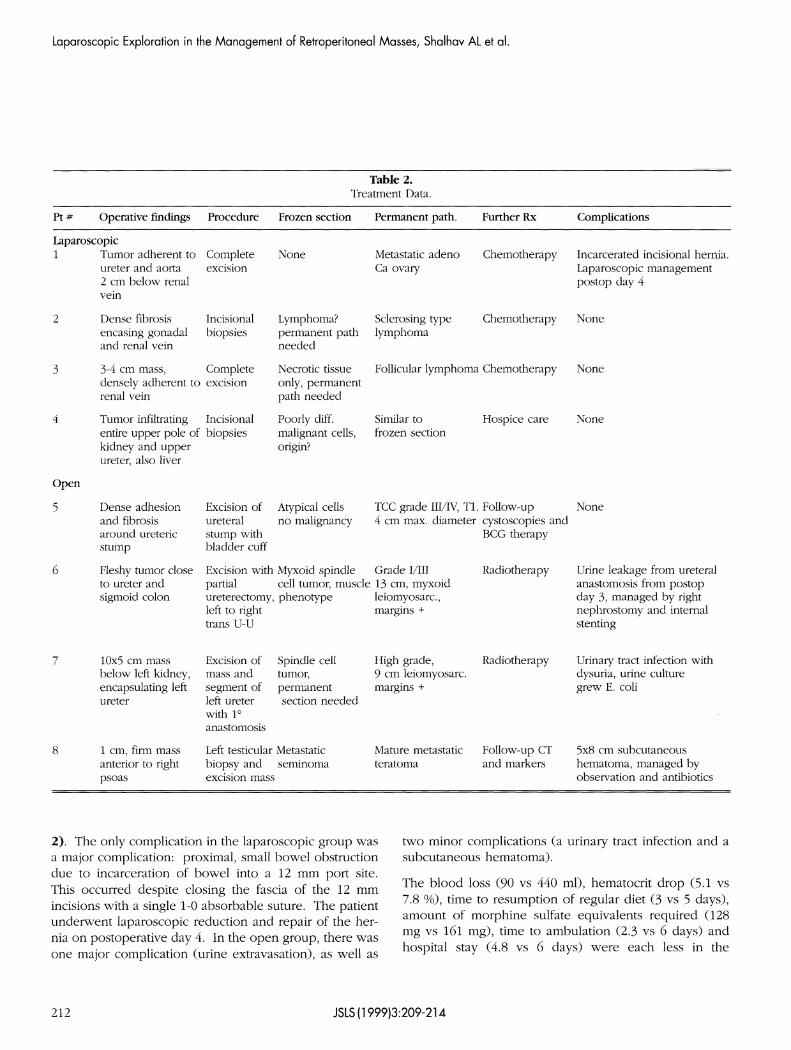
Table 2.Treatment Data.
Pt # Operative findings
Laparoscopic1
2
3
4
Open
5
6
7
8
Tumor adherent toureter and aorta2 cm below renalvein
Dense fibrosisencasing gonadaland renal vein
3-4 cm mass,densely adherent torenal vein
Tumor infiltratingentire upper pole ofkidney and upperureter, also liver
Dense adhesionand fibrosisaround uretericstump
Fleshy tumor closeto ureter andsigmoid colon
10x5 cm massbelow left kidney,encapsulating leftureter
1 cm, firm massanterior to rightpsoas
Procedure
Completeexcision
Incisionalbiopsies
Completeexcision
Incisionalbiopsies
Excision ofureteralstump withbladder cuff
Excision withpartialureterectomy,left to righttrans U-U
Excision ofmass andsegment ofleft ureterwith 1°anastomosis
Left testicularbiopsy andexcision mass
Frozen section
None
Lymphoma?permanent pathneeded
Necrotic tissueonly, permanentpath needed
Poorly diff.malignant cells,origin?
Atypical cellsno malignancy
Myxoid spindlecell tumor, musclephenotype
Spindle celltumor,permanentsection needed
Metastaticseminoma
Permanent path.
Metastatic adenoCa ovary
Sclerosing typelymphoma
Follicular lymphoma
Similar tofrozen section
CC grade III/IV, T1.4 cm max. diameter
Grade I/III13 cm, myxoidleiomyosarc.,margins +
High grade,9 cm leiomyosarc.margins +
Mature metastaticteratoma
Further Rx
Chemotherapy
Chemotherapy
Chemotherapy
Hospice care
Follow-upcystoscopies andBCG therapy
Radiotherapy
Radiotherapy
Follow-up CTand markers
Complications
Incarcerated incisional hernia.Laparoscopic managementpostop day 4
None
None
None
None
Urine leakage from ureteralanastomosis from postopday 3, managed by rightnephrostomy and internalstenting
Urinary tract infection withdysuria, urine culturegrew E. coli
5x8 cm subcutaneoushematoma, managed byobservation and antibiotics
2). The only complication in the laparoscopic group wasa major complication: proximal, small bowel obstructiondue to incarceration of bowel into a 12 mm port site.This occurred despite closing the fascia of the 12 mmincisions with a single 1-0 absorbable suture. The patientunderwent laparoscopic reduction and repair of the her-nia on postoperative day 4. In the open group, there wasone major complication (urine extravasation), as well as
two minor complications (a urinary tract infection and asubcutaneous hematoma).
The blood loss (90 vs 440 ml), hematocrit drop (5.1 vs7.8 %), time to resumption of regular diet (3 vs 5 days),amount of morphine sulfate equivalents required (128mg vs 161 mg), time to ambulation (2.3 vs 6 days) andhospital stay (4.8 vs 6 days) were each less in the
212 JSLS (1999)3:209-214
JSLS
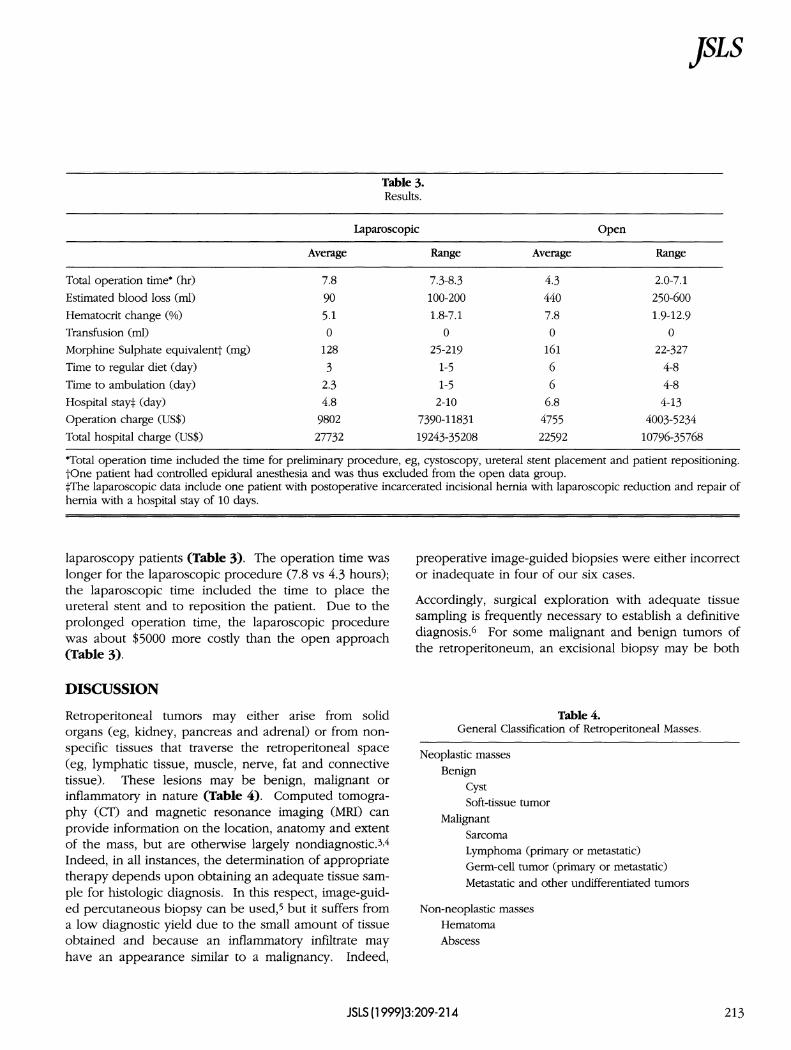
Table 3.Results.
Total operation time* (hr)
Estimated blood loss (ml)
Hematocrit change (%)
Transfusion (ml)
Morphine Sulphate equivalent† (mg)
Time to regular diet (day)
Time to ambulation (day)
Hospital stay‡ (day)
Operation charge (US$)
Total hospital charge (US$)
Laparoscopic
Average
7.8
90
5.10
128
3
2.34.8
9802
27732
Range
7.3-8.3100-200
1.8-7.10
25-219
1-51-5
2-10
7390-11831
19243-35208
Open
Average
4.34407.80
16166
6.84755
22592
Range
2.0-7.1
250-600
1.9-12.90
22-327
4-84-8
4-134003-5234
10796-35768
*Total operation time included the time for preliminary procedure, eg, cystoscopy, ureteral stent placement and patient repositioning.†One patient had controlled epidural anesthesia and was thus excluded from the open data group.‡The laparoscopic data include one patient with postoperative incarcerated incisional hernia with laparoscopic reduction and repair ofhernia with a hospital stay of 10 days.
laparoscopy patients (Table 3). The operation time waslonger for the laparoscopic procedure (7.8 vs 4.3 hours);the laparoscopic time included the time to place theureteral stent and to reposition the patient. Due to theprolonged operation time, the laparoscopic procedurewas about $5000 more costly than the open approach(Table 3).
DISCUSSION
Retroperitoneal tumors may either arise from solidorgans (eg, kidney, pancreas and adrenal) or from non-specific tissues that traverse the retroperitoneal space(eg, lymphatic tissue, muscle, nerve, fat and connectivetissue). These lesions may be benign, malignant orinflammatory in nature (Table 4). Computed tomogra-phy (CT) and magnetic resonance imaging (MRI) canprovide information on the location, anatomy and extentof the mass, but are otherwise largely nondiagnostic.3,4
Indeed, in all instances, the determination of appropriatetherapy depends upon obtaining an adequate tissue sam-ple for histologic diagnosis. In this respect, image-guid-ed percutaneous biopsy can be used,5 but it suffers froma low diagnostic yield due to the small amount of tissueobtained and because an inflammatory infiltrate mayhave an appearance similar to a malignancy. Indeed,
preoperative image-guided biopsies were either incorrector inadequate in four of our six cases.
Accordingly, surgical exploration with adequate tissuesampling is frequently necessary to establish a definitivediagnosis.6 For some malignant and benign tumors ofthe retroperitoneum, an excisional biopsy may be both
Table 4.General Classification of Retroperitoneal Masses.
Neoplastic massesBenign
CystSoft-tissue tumor
MalignantSarcomaLymphoma (primary or metastatic)Germ-cell tumor (primary or metastatic)Metastatic and other undifferentiated tumors
Non-neoplastic massesHematomaAbscess
JSLS (1999)3:209-214 213

Laparoscopic Exploration in the Management of Retroperitoneal Masses, Shalhav AL et al.
diagnostic and curative.3,7,8
Laparoscopic exploration potentially can provide a mini-mally invasive means to obtain adequate tissue for histo-logic diagnosis without the need for a major midlineabdominal or flank incision. All of our patients whounderwent laparoscopic exploration tolerated the proce-dure well and were able to ambulate and resume a fulldiet within five days. The postoperative pain was mini-mal, and the hospital stay was brief (average 4.8 days).In the laparoscopic cases, two patients had an excisionalbiopsy, and two patients had an incisional biopsy. In allfour cases, a definitive diagnosis was made, and no fur-ther surgical intervention was necessary.
In comparison with open exploration, the laparoscopicapproach was equally as effective, yielding a definitivediagnosis in all four cases. However, due to longer oper-ative time, the laparoscopic procedure was more costlyand, hence, less efficient than the open approach. Withregard to morbidity, patient recovery and hospital stay,laparoscopic exploration was more favorable.
CONCLUSIONS
In summary, we believe that laparoscopic exploration fora retroperitoneal mass of undetermined origin is a viablealternative to open exploration. The laparoscopicapproach is as effective, albeit less efficient, than an openprocedure; however, the laparoscopic approach providedbenefits with regard to patient morbidity and convales-cence. As urologic surgeons become more experiencedwith laparoscopic techniques and with the advent ofmore efficient nondisposable instrumentation, we antici-pate that the operative time and cost for more complex
laparoscopic procedures, such as retroperitoneal explo-ration, will decrease. Nonetheless, our initial experiencewith laparoscopic retroperitoneal exploration is favor-able, and we are now offering this approach as first-linetherapy in these patients.
References:
1. Gerber GS, Rukstalis DB. Laparoscopic approach toretroperitoneal lymph node dissection. Semin Surg Oncol.1996;12:121-125.
2. Janetschek G, Hobisch A, Holtl L, Bartsch G.Retroperitoneal lymphadenectomy for clinical stage I nonsemi-nomatous testicular tumor: laparoscopy versus open surgery andimpact of learning curve. J Urol. 1996;156:89-94.
3. Testini M, Catalanlo Jr., Macarini L, Paccione F. Diagnosisand surgical treatment of retroperitoneal tumors. Int Surg.1996;81:88-93.
4. Bechtold RE, Dyer RB, Zagoria RJ, Chen MYM. The perire-nal space: relationship of pathologic processes to normalretroperitoneal anatomy. Radiographics. 1996;16:841-854.
5. Fisher AJ, Paulson EK, Sheafor DH, Simmons CM, NelsonRC. Small lymph nodes of the abdomen, pelvis, and retroperi-toneum: usefulness of sonographically guided biopsy.Radiology. 1997;205:185-190.
6. Scully RE, Mark EJ, McNeely WF, Ebeling SH. Case recordsof the Massachusetts General Hospital. N Eng J Med.1996;29:650-655.
7. Klein EA, Streem SB, Novick AC. Intraoperative consultationfor the retroperitoneum and adrenal glands. Urol Clin N Am.1985;12(3):411-421.
8. Felix EL, Wood DK, Das Gupta TKD. Tumors of theretroperitoneum. Curr Probl Cancer. 1981;6:1-47.
214 JSLS(1999)3:209-214





























