Embed Size (px)
DESCRIPTION
bedah saraf
Citation preview

Scandinavian Journal of Surgery 99: 235–239, 2010
Temporal paTTerns of deaTh afTer Trauma: evaluaTion of circadian, diurnal, periodical and seasonal Trends in 260 faTal injuries
K. søreide1, 2 1 Department of Surgery, Stavanger University Hospital, Stavanger, Norway 2 Department of Surgical Sciences, University of Bergen, Bergen, Norway
aBsTracT
Background: Temporal patterns of trauma deaths may indicate potential for prevention or systems improvement, but have been poorly investigated in the scandinavian trauma population. This study examines patterns in trauma deaths to the occurrence in hour and time of the day, day and time in the week, and month and season.
Materials and Methods: investigation of the temporal patterns of death in 260 fatalities undergoing autopsy. Time of death were explored according to time of the day (hour; day/night), time of the week (day of week; weekday/weekend) and time of the year (month; season) and analyzed for difference in gender, age, injury type and severity, and mechanisms of injury and death.
Results: a total of 260 trauma deaths were included, of which 125 (48%) died in hos-pital and 194 (75%) were male. no particular peak-hour of the day when deaths occurred was found. one-third of deaths occurred during weekends. for inhospital deaths during weekends, significantly more patients had respiratory distress (rr > 20 or < 16 in 72.5% for weekends and 47.0% for weekdays; p = 0.008) and hypotension (sBp < 90mmhg in 61% vs 40%; p = 0.048) during weekends. deaths occurred with some monthly variance demonstrated with two monthly peaks in february/march and july/august, respectively. overall, no statistically different seasonal differences in the occurrence of traumatic deaths, nor any differences in cause of death, type or severity of injury, nor in physio-logical parameters was found. however, a higher number of inhospital deaths presented with reduced consciousness level (Gcs < 8) and severe head injuries (ais-head ≥ 4) dur-ing spring and summer (p = 0.045, chi-square for trend) compared to winter and fall.
Conclusions: Trauma deaths in a scandinavian population did not demonstrate statis-tically significant differences in overall circadian, weekly or seasonal patterns of trauma death occurrence. however, the impact of fatal head injuries during spring and summer warrants further investigation.
Key words: Trauma; death; injury; circadian; diurnal; periodical; week; month; season
Correspondence:Kjetil Søreide, M.D.Department of Surgery, Stavanger University HospitalPOB 8100 N - 4068 Stavanger, Norway Email: [email protected]

236 K. Søreide
INTRODUCTION
Major injury is a leading cause of death and disability around the world (1). For both sexes, one in every ten deaths is the result of injury. Globally, unintentional injuries are ranked as the sixth leading cause of death and the fifth leading cause of moderate and severe disability. Road traffic accidents (RTA) alone cause 1.3 million deaths each year. For those under 35 years of age, injury is the leading cause of death, and males aged 15–24 years are responsible for the greatest share of injury burden (1).
While some studies have investigated and demon-strated temporal differences in the occurrence and death in various surgical and non-surgical diseases – such as ruptured abdominal aortic aneurysms, acute myocardial infarction, sudden cardiac death, stroke, and pulmonary embolism (2–4) – similar tem-poral relationships have been less well investigated for trauma patients (5,6). The past decades have fo-cused on the ”trimodal temporal death distribution” after trauma – from early hours exanguination, to fatal centralnervous system injuries within days and, multiorgan failure deaths occurring weeks or months after injury. Some recent reports have demonstrated diverging results as to the validity of the trimodal death pattern (7–10), as the model depends on choice of method for verification (11). Also, an overall litera-ture summary demonstrates a reduction in the rates of exsanguinating trauma patients (12), possibly due to improved diagnostics and implementation of stan-dardized treatment algorithms. Further, the introduc-tion of working-time restrictions in both North Amer-ica and European training systems have raised con-cerns for maintenance of overall patient safety and continuity of care (13). Added to this concern is the theoretical effect of annually rotas within the training system, providing for periods with more inexperi-enced trainees involved in patient care, termed the “July phenomenon” (14, 15). While several of these issues may or may not truly influence on mortality for patients with surgical diseases, such as trauma, before investigating any causal relationships it is im-portant to analyze the temporal trends to detect any statistically significant or clinically important differ-ences, if present, in the first place. Thus, this study was undertaken to investigate the temporal trends of trauma deaths in a previously described Norwegian cohort of trauma fatalities (10), recognizing the Scan-dinavian 40-hour working hour system. The aim was to investigate if there were any particular clustering of deaths according to hour of the day, day of the week, month or season.
MATERIAl AND METHODS
All trauma deaths occurring in the greater Stavanger area (population of approx. 300,000) during 1996–2004 and who were subject to autopsy were eligible for inclusion in this study. The study population has been described previously (5, 10). The study population consists of over 95% of all trauma deaths occurring in the defined area during the study period (10). Burns and isolated fractures (i.e. hip frac-
ture) are not included in the study population. Briefly, the Stavanger University Hospital (SUH) is the primary trauma hospital for about 300,000 inhabitants, with referrals re-ceived from a wider population of about 500,000 (16, 17). The SUH has a designated trauma team consisting of gen-eral surgeons, orthopaedic surgeons, anaesthesiologists and any required subspecialty care, as required. In the desig-nated region, prehospital and inhospital trauma deaths are undergoing autopsy at a very high frequency due to coop-erative agreements between law enforcements and the de-partment of pathology at SUH. The regional ethic commit-tee recognized the study as quality assurance.
DEMOGRAPHICS, INJURy DESCRIPTION AND SEvERITy
Age and gender, type and mechanism of injury, and cause of death were recorded. Injury severity scoring was per-formed by a registrar (K.S.) trained and certified in the methods by AAAM using the Abbreviated Injury Score (AIS-90, 1998 update; (ref. 18)), for calculation of the Injury Severity Score (ISS) and New Injury Severity Score (NISS) (19). For inhospital deaths, systolic blood pressure (SBP), respiratory rate (RR), and Glasgow Coma Scale (GCS) were recorded on arrival in the emergency department, were applicable. To avoid missing values in physiological pa-rameters, SBP, GCS, and RR were categorized on a five-point scale according to the Revised Trauma Score coded values. ‘Respiratory distress’ was defined as any value not indicating a RR of 16–20; ‘hypotension’ was defined as any SBP value < 90 mmHg, and ‘severely reduced consciousness level’ as GCS < 8.
TEMPORAl TREND RECORDS
Time of injury and death, if documented, were recorded to any full hour (from 0 to 23) of the day. Diurnal variation was investigated for ‘Daytime’ (07:00 hrs to 18:59 hrs) and ‘Nighttime’ (19:00 hrs to 06:59 hrs). Day of the week (Mon-day through Sunday) were recorded with “Weekdays” des-ignated as Monday through Thursday and “Weekends” as Friday through Sunday. Month of death was recorded, and Season designated as Winter (December through February), Spring (March through May), Summer (June through Au-gust) and Fall (September through November), as previ-ously reported (5, 20).
STATISTICS
Statistical analysis was performed using SPSS version 16.0 (SPSS Inc., Chicago, USA). Data are reported as mean ± standard deviation (SD) or median and ranges, were in-dicated. Comparison between continuous variables was performed with non-parametric Mann-Whitney U test. The Chi-square or Fischer’s exact test was used for comparison of categorical data. All statistical tests are two-tailed, and the statistical significance level set at P < 0.05.
RESUlTS
A total of 260 deaths underwent a full autopsy (either regular or forensic) after sustaining fatal injury and were included, of which 125 (48%) were inhospital deaths and 194 (75%) were males. The distribution in age, gender and injury profile has been reported pre-viously (10). Briefly, the mean age was 45.6 ± 25.1 years, and the mean ISS 43 ± 23 and NISS 54 ± 20, in-dicating a severely injured study population.

237Temporal patterns of trauma deaths
CIRCADIAN AND DIURNAl PATTERNS OF DEATH AFTER INJURy
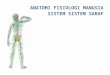
Exact time of death was only present in about half the patients (n = 123), largely due to lack of exact record-ing in prehospital cases (missing in 70%), but present in two-thirds of the inhospital deaths. For those with available records, there was no particular peak-hour of the day when deaths occurred. However, for parts of the day, there was considerable higher number for the hours 20:00 p.m. to 01:59 a.m. accounting for about one-third (32.6%) of all deaths, and the hours 16:00 to18:59 p.m. accounting for about one fifth of all deaths (19.5%). The hours 03:00 to 06:59 a.m. had the least number of deaths (< 10% for both pre- and in-hospital deaths). However, the largest share of deaths occurred during ‘daytime’ (Fig. 1A).
For inhospital deaths alone, no statistically signifi-cant diurnal differences in the injury severity (ISS and NISS) or cause of death could be detected. Neither was there any significant difference in the numbers of severe head, thoracic or abdominal injuries, nor in the numbers of patients presenting in respiratory dis-tress, with hypotension, or with decreased conscious-ness level comparing daytime with nighttime deaths.
DAy OF THE WEEK, WEEKDAyS vS WEEKENDS
No particular clustering of deaths during any day of the week was found with any statistically significant difference (Monday through Sunday; Fig. 1B). Of the 260 deaths, 32.9% (n = 102) occurred during week-ends. No significant differences were found in gen-der, age, injury type or severity, or cause of death. For inhospital deaths during weekends, significantly more patients had respiratory distress (72.5% for
weekends and 47.0% for weekdays; p = 0.008) and hypotension (61% vs 40%; p = 0.048) during week-ends.
MONTH OF THE yEAR AND SEASONAl PATTERN
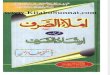
Deaths occurred with some monthly variance dem-onstrated with two monthly peaks (Fig. 2A) with the first occurring during February/March and the other during July/August.
Spread over the year, there were no statistically different seasonal differences in the occurrence of traumatic deaths (Fig. 2B), nor any differences in cause of death, type and severity of injury (Fig. 3), or physiological parameters, except for more inhospital deaths having a lower consciousness level on arrival during spring and summer (GCS < 8 in 86% and 69%) compared to winter and fall (52% and 63%, respec-tively; P = 0.045, chi-square for trend), and more pa-tients with severe head-injuries (AIS head of 4 or higher) during spring and summer (75% and 78%) compared to winter and fall (52% and 63%, respec-tively; P=0.045, chi-square for trend).
DISCUSSION
This study demonstrates temporal trends in circa-dian, diurnal, weekly, and seasonal patterns of trauma deaths occurring in a defined Norwegian population. Notably, these patterns were investigated in a non-formal trauma system depending on trauma-care de-livered by general and/or subspecialty surgeons (non-designated for trauma only), as is the present state in Norway and other Scandinavian countries (21, 22). This study demonstrates no significant circa-
Figure 1. Diurnal (A) and weekday (B) distribution of trauma deaths
Figure 2. Monthly (A) and seasonal (B) distribution of trauma deaths.
Fig. 1. Diurnal (A) and weekday (B) distribution of trauma deaths.

238 K. Søreide
Figure 1. Diurnal (A) and weekday (B) distribution of trauma deaths
Figure 2. Monthly (A) and seasonal (B) distribution of trauma deaths.
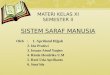
Figure 3. Distribution of injury mechanism according to time of year
RTA denotes ”road traffic accident”.
dian differences, although one third of all deaths oc-curred during evening and early night. Of notice, the staff number is usually lower with less degree of ex-perience during this time, than during day-hours. However, due to the number of missing data and the investigation of deaths only (and not survivors of trauma) these number should be interpreted with
caution before drawing firm conclusions, and prefer-ably larger cohorts of trauma patients (both survivors and non-survivors) should be investigated to firmly establish any clinically important pattern in this re-gard.
The increased number of trauma deaths presenting with severe head-injuries and reduced GCS scores on
Fig. 2. Monthly (A) and seasonal (B) distribution of trauma deaths.
Fig. 3. Distribution of injury mechanism according to time of year
RTA denotes ”road traffic accident”.

239Temporal patterns of trauma deaths
arrival in the emergency department during spring and summer are in line with previous findings dem-onstrated in children (5). These findings coincide with the higher incidence of fatalities after road traffic ac-cidents during spring and summer, as well as higher incidence of fall-related deaths during summer (Fig. 3). The role of falls as a contributor to the incidence of head injuries has been noted in a previous report from the Stavanger region (23), with falls as the most frequent contributor to head injuries in both extremes of age. However, other reports have not demonstrated any seasonal patterns in the occurrence of fatal and non-fatal falls (20).
The monthly clustering of fatal trauma during the months February/March and July/August represents the peak seasons of vacation (winter and summer, respectively) and increased activity, both in terms of more busy traffic (with increased risk for road traffic accidents) and increased leisure activities.
In Norway, there is no specific month, or time of the year, for rotation for residents in training (not for surgeons, nor for other related specialties including orthopaedic surgeons, nor anaesthesiologists). Rather, training is begun on a random basis, year-round, de-pending on vacant positions available (22). Thus, we believe that the finding of an increased number of deaths during July/August is not a reflection of train-ing and experience status of the staff involved, but may rather reflect a time of the year with peak inci-dence in accidents. This should, however, warrant further studies in the Scandinavian population. Of notice, recent reports (14, 15) from North American trauma centres have not confirmed any “July-phe-nomenon”, nor have this been found in other fields including obstetrics, intensive care, nor in neurosur-gery (24–26).
In conclusion, the patterns of trauma deaths in a Scandinavian population with a 40-hour working week pattern did not demonstrate statistically sig-nificant circadian, weekly or seasonal patterns of trauma death occurrence in an overall perspective. However, some clustering of the number of deaths was demonstrated during evening and early night-hours, more critical and fatal head injuries during weekends and particularly for spring and summer-time, and clustering of deaths during typical months of vacation (winter break and summer break). These findings should be explored in further detail, using the current trauma registries under establishment in the Scandinavian systems, to allow for future evalu-ation, planning, and possible improvements of the trauma system at hand.
REFERENCES
01. Søreide K: Epidemiology of major trauma. Br J Surg 2009;96(7): 697–698
02. Manfredini R, Boari B, Gallerani M, et al: Chronobiology of rupture and dissection of aortic aneurysms. J vasc Surg 2004; 40(2): 382–388
03. Bilora F, Manfredini R, Petrobelli F, et al: Chronobiology of non fatal pulmonary thromboembolism. Panminerva Med 2001; 43(1): 7–10
04. Rosenberg J, Pedersen MH, Ramsing T, Kehlet H. Circadian variation in unexpected postoperative death. Br J Surg 1992;79(12):1300–1302
05. Søreide K, Kruger AJ, Ellingsen Cl, Tjosevik KE: Pediatric trauma deaths are predominated by severe head injuries dur-ing spring and summer. Scand J Trauma Resusc Emerg Med 2009;17(1): 3
06. Morris RW, leikin JB, Eckenrode P, Boston D: The effects of time of trauma patient presentation on emergency department utilization. Prog Clin Biol Res 1990;341A:201–211
07. Pang JM, Civil I, Ng A, Adams D, Koelmeyer T: Is the tri-modal pattern of death after trauma a dated concept in the 21st century? Trauma deaths in Auckland 2004. Injury 2008;39(1): 102–106
08. de Knegt C, Meylaerts SA, leenen lP: Applicability of the trimodal distribution of trauma deaths in a level I trauma centre in the Netherlands with a population of mainly blunt trauma. Injury 2008;39(9): 993–1000
09. Demetriades D, Kimbrell B, Salim A, et al: Trauma deaths in a mature urban trauma system: is “trimodal” distribution a valid concept? J Am Coll Surg 2005;201(3): 343–348
10. Søreide K, Krüger AJ, vardal Al, et al: Epidemiology and contemporary patterns of trauma deaths: changing place, similar pace, older face. World J Surg 2007;31(11):2092–2103
11. Kruger AJ, Søreide K: Trimodal temporal distribution of fatal trauma – fact or fiction? Injury 2008;39(8): 960–961; author reply 961–962
12. Pfeifer R, Tarkin IS, Rocos B, Pape HC: Patterns of mortality and causes of death in polytrauma patients – has anything changed? Injury 2009;40(9):907–911
13. Glomsaker TB, Søreide K: Surgical training and working time restriction. Br J Surg 2009;96(4):329–330
14. Schroeppel TJ, Fischer PE, Magnotti lJ, et al: The “July phe-nomenon”: is trauma the exception? J Am Coll Surg 2009; 209(3):378–384
15. Claridge JA, Schulman AM, Sawyer RG, et al: The “July phe-nomenon” and the care of the severely injured patient: fact or fiction? Surgery 2001;130(2):346–353
16. Meling T, Harboe K, Søreide K: Incidence of traumatic long-bone fractures requiring in-hospital management: A prospec-tive age- and gender-specific analysis of 4890 fractures. Injury 2009;40(11):1212–1219
17. Søreide K, Søiland H, lossius HM, et al: Resuscitative emer-gency thoracotomy in a Scandinavian trauma hospital – is it justified? Injury 2007;38(1):34–42
18. AAAM: The Abbreviated Injury Scale (AIS) 1990 revision (Up-date 1998). Association for the Advancement of Automotive Medicine: Barrington, Illinois, 2001
19. Champion HR: Trauma scoring. Scand J Surg 2002;91(1):12–22
20. Stevens JA, Thomas KE, Sogolow ED: Seasonal patterns of fatal and nonfatal falls among older adults in the U.S. Accid Anal Prev 2007;39(6):1239–1244
21. Kristiansen T, Søreide K, Ringdal KG, et al: Trauma systems and early management of severe injuries in Scandinavia: Re-view of the current state. Injury 2009 May; 41(5):444–452
22. Søreide K, Glomsaker T, Søreide JA: Surgery in Norway: be-yond the scalpel in the 21st century. Arch Surg 2008;143(10): 1011–1016
23. Heskestad B, Baardsen R, Helseth E, et al: Incidence of hospi-tal referred head injuries in Norway: A population based sur-vey from the Stavanger region. Scand J Trauma Resusc Emerg Med 2009;17(1):6
24. Smith ER, Butler WE, Barker FG 2nd: Is there a “July phenom-enon” in pediatric neurosurgery at teaching hospitals? J Neu-rosurg 2006;105(3 Suppl):169–176
25. Myles TD: Is there an obstetric July phenomenon? Obstet Gy-necol 2003;102(5 Pt 1):1080–1084
26. Barry WA, Rosenthal GE: Is there a July phenomenon? The effect of July admission on intensive care mortality and length of stay in teaching hospitals. J Gen Intern Med 2003;18(8): 639–645
Received: October 8, 2009Accepted: March 3, 2010