-
8/11/2019 Kala-azar Control National Guideline
1/96
Learning Unit - 1
INTRODUCTION
Contents:
Background
Bangladesh situation
Target audience
Selection of different level of health facilities
Kala-azar elimination program-
1) Target
2) Objective
3) Regional strategies
Objectives: at the end of the session the participant will be
able to:
Describe global, regional and country situation of
Kala-azar.
Mention the target audience of their guideline
Identify different level of health facilities in public and
private sector
for elimination of Kala-azar.
Define target, objectives and regional strategy of Kala-azar
elimination program.
-
8/11/2019 Kala-azar Control National Guideline
2/96
1.1 Background
Kala-azar or is one of the clinical form of leishmaniasis and is
caused by the
protozoa Leishmania donovani. In the Indian sub-continent it is
transmitted by the
sand fly named Phlebotomus argentipes. The disease presents as
fever of long
duration with splenomegaly, anaemia, weight loss and darkening
of complexion. In
endemic areas, children and young adults are its principal
victims. Kala-azar is fatal
if not treated timely. Kala-azar HIV or TB co-infection has
emerged as a health
problem in recent years. The disease is seen in several
countries of the world with
about 500,000 cases annually. India, Sudan, Nepal, Bangladesh
and Brazil account
for 90% of the total global cases. It affects largely the
socially marginalized and the
poorest communities.
1.2 Kala-azar situation in Bangladesh
Kala-azar is one of the major public health problems in
Bangladesh and the disease
is endemic for many
decades. During the
Malaria Eradication
Programme blanket DDT
spraying controlled kala-
azar transmission. In the late
1970s Kala-azar re-emerged
sporadically. During 1981-
85 only 8 upazilas (Sub-
district) reported Kala-azar,
which increased to 105
upazilas in 2004. During the
last few years the Kala-azar
situation has assumed
epidemic proportion with the
-
8/11/2019 Kala-azar Control National Guideline
3/96
number of reported cases increasing from 3978 in 1993 to 8505 in
2005. Present
surveillance is weak and the current estimated total cases are
about 45,000.
Annually @ 10,000 cases are treated by the control programme but
the cases
treated by the private clinics and practitioners are not
reported.
Under the current surveillance system the Upazila Health
Complexes (UHCs),
District Hospitals and other specialized hospitals report cases
to the Malaria &
Parasitic Disease Control Unit in DGHS. This is however is a
gross under
reporting because the private sector clinics and hospitals, and
the cases treated by
private practitioners are not included. At present only Inj. SAG
is used for
treatment, which is supplied, free of charges and passive
surveillance only works
when drugs are available in the hospitals.
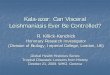
The bar chart below shows the number of Kala-azar cases reported
during 1994-
2005. It signifies the trend of the disease @ of 8,000-10,000
cases annually. The
highest case fatality rate recorded from research on known
Kala-azar patients in
Mymensingh district has been 6.4% (Desjeux P. 1991). The
prevalence rate in
some selected villages in the same district has been found be as
high as 6% of the
total population (unpublished report, 1993). However, definite
data on morbidity
and deaths due to Kala-azar are not available from the current
reporting system.
Age and sex segregated data is not available with the control
programme at
present.
Yearly Kala-azar Cases and Deaths (1999-2009)
5799
7640
4283
8110
61135920
6892
9379
4932 4840
4294
23 24
6
36
27
23
16
23
17 17
14
0
1000
2000
3000
4000
5000
6000
7000
8000
9000
10000
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Year
Cases
0
10
20
30
40
50
Deaths
Case Death
-
8/11/2019 Kala-azar Control National Guideline
4/96
Cases are usually clustered in the villages having environmental
and related factors
for the vectors to grow and proliferate. There is no marked
seasonal variation but
the pre and post-monsoon rise in number of cases indicates two
picks of
transmission. Areas in the old Brahmaputra and the Ganges basin
show the highest
prevalence of the disease.
1.3 Target audience for the guidelines
These guidelines will be useful to the-
Programme managers- national/divisional/district/upazila
level.
Doctors and health care providers
Supervisors at all levels
Supervisors and health workers engaged in supervising the
spraying
squads
The health care providers and volunteers responsible for
behaviour
change communication (BCC) can use the guidelines to (a) promote
early
care seeking if Kala-azar is suspected, (b) convince the
patients suffering
from Kala-azar to complete the treatment and (c) undertake
advocacy
with the community for participation in ensuring complete and
uniform
coverage of their households with insecticides.
This guidelines and SOPs are adopted according to the SEARO, WHO
guidelines.
Whenever translation is needed for training of grass root level
workers, volunteers,
NGO workers for providing training on particular areas of their
involvement in
Kala-azar elimination programme, local managers are encouraged
to translate it in
Bangla.
-
8/11/2019 Kala-azar Control National Guideline
5/96
Table 1 Level of health facilities in Bangladesh
Level 1 Level 2 Level 3
Public sector
-Upazila Health Complex
(UHC)-Community clinic
- Union Health Facilities
(Health & Family Welfare
Centre-H&FWC; Rural
Dispensary-RD; Sub-centre-
SC)
Private sector
-Qualified private
practitioners-Non qualified health care
providers including health
volunteers
-NGOs; private hospitals;
private clinics; and private
laboratories.
Public sector
-District Hospitals
Private sector
-Qualified private
practitioners;
NGOs; private
hospitals; private
clinics; and private
laboratories.
Public sector
-Medical college
Hospitals.-Specialized hospitals
Private sector
-Medical College
Hospitals
-Qualified private
practitioners;
-
NGOs; private hospitals;
private clinics; andprivate laboratories
N.B-Treatment wi l l be given in upazil a health complex in case
of level I and
other pri vate and public sector of L evel I wil l r efer the
patient to upazil la health
complex.
For the success of the programme it is important to develop
linkages between the
three levels and establish ongoing communication with the
private sector. The
district focal point should be responsible for sustaining the
linkages. The details of
collaboration between the public and private sector need to be
worked out with the
objective of obtaining uniform standards of practices.
1.4 Kala-azar elimination programme
Kala-azar can be eliminated from the Indian Subcontinent because
there is no
intermediate host for transmission of the disease. The Indoor
residual spray has been
very effective. As a collateral benefit of malaria Kala-azar was
almost eliminated.
The disease can be easily recognized and effective treatment for
Kala-azar is
available.
-
8/11/2019 Kala-azar Control National Guideline
6/96
1.4.1 Target
The target of Kala-azar elimination is to reduce the incidence
of the disease to less
than 1 case per 10,000 populations at the upazila level in
Bangladesh by the year
2015.
1.4.2 Objectives
The impact objective is to reduce the incidence of Kala-azar to
less than 1 case of
Kala-azar and Post Kala-azar Dermal Leishmaniasis per 10,000
population at
district (in Nepal) or sub district/upazila level (in Bangladesh
and India) by:
Reducing the incidence Kala-azar in the endemic communities
including the
poor, vulnerable and un-reached populations.
Reducing case fatality rates from Kala-azar.
Treatment of Post Kala-azar Dermal Leishmaniasis (PKDL) to
reduce the
parasite reservoir.
Prevention and treatment of Kala-azar-HIV-TB co-infections.
1.4.3 Elimination strategy
A regional strategy for elimination of Kala-azar has been
endorsed by the Regional
Technical Advisory Group (RTAG). It comprises of the following
components:
(a) Early diagnosis and complete treatment:All suspected cases
of Kala-azar and
PKDL would have access to recommended diagnosis and
treatment.
(b) Integrated vector management: The mainstay of vector control
is indoor
residual spray (IRS) with suitable insecticides. Improvements in
housing and
personal preventive methods would be promoted through
community
involvement.
(c) Effective disease surveillance: A revamped surveillance
system should
strengthen diagnosis treatment and reporting both in the public
and the
private sector.
-
8/11/2019 Kala-azar Control National Guideline
7/96
(d) Social mobilization and partnerships: Behavioral Change
Communication
(BCC) would aim at achieving early diagnosis and complete
treatment,
participation of the community in IRS, and adoption of personal
preventive
methods and micro-environmental management. Partnerships within
and
outside the health sector are to be forged to promote the goals
of Kala-azar
elimination.
(e) Operational research: Operational research to monitor the
drug and
insecticide resistance, quality of drugs, treatment compliance,
pharmaco-
vigilance, ITNs use etc.would be undertaken.
-
8/11/2019 Kala-azar Control National Guideline
8/96
Learning Unit - 2
DIAGNOSIS OF KALA-AZAR and PKDL
Objectives: at the end of the session the participant
will be able to-
describe lifecycle of L donovani, pathogenesisand
patho-physiology of KA and PKDL
mention the clinical feature of KA and PKDL
list the complications of KA
define a case of KA and PKDL
measure the spleen
perform skin sensation test (PKDL)
perform the rK-39 test aspirate hone marrow/spleen
(Optional)
prepare slides for microscopy (Optional)
Contents:
Lifecycle, Pathogenesis and Patho-physiology
Clinical Diagnosis of KA and PKDL:Clinical features of KA and
PKDL
Complications of KA and PKDL
Laboratory diagnosis of KA
Direct evidence: Microscopy, PCR, Culture
Indirect evidence: Immunological
Others: Haematological, Biochemical
Laboratory diagnosis of PKDL:
Differential diagnosis
Case definition: KA, PKDL, KATF
-
8/11/2019 Kala-azar Control National Guideline
9/96
2.1 Lifecycle, Pathogenesis and Patho-physiology
Life cycle of Leishmania donovani
Mode of transmission :
The natural transmission of Leishmania donovani from man to man
is carried out
by a certain species of sand fly of the genera Phlebotomus. The
infected female
sand fly transmits LD bodies to the susceptible human through
their bite.
Cycle in man:
Flagellated Promastigotes enter the body through infected
sandfly bite and
subsequent events are as follows:
Parasites enter the skin
Engulfed by resident macrophages
Promastigotes develop into Amastigotes (L-D bodies) in cells of
MPS
Amastigotes multiply and R.E. cells are packed with parasites,
enlarged, distended
& eventually burst (50 to 200 parasites present in single
cell) to release theparasites.
Free parasites pass to different organs of the body and are
engulfed by new
reticuloendothelial( RE) cells where they multiply & the
cycle is repeated.
In this way the entire Reticulo-Endothelial system becomes
progressively infected.
A blood-sucking sandfly draws Amastigotes (L-D bodies) during
its blood-meal
-
8/11/2019 Kala-azar Control National Guideline
10/96
Cycle in sandfly:
Amastigotes (L-D bodies) are taken with blood meal and develop
into
promastigote forms in the midgut of sandfly on the third day
after blood meal.
Promastigotes multiply by binary fission into enormous
number
Multiplication takes place and on the 5th
day the promastigotes gather around the
proventricular end of the gut
Multiplication and forward progression continues till 7th
day
Solid mass of flagellates fill up extending up to the
pharynx
A heavy pharyngeal infection of the sandfly is usually observed
between 6th
and
9th
day of its infected blood meal
In certain sandflies heavy infection blocks the oesophagus. Such
sandflies, at the
time of their next sucking blood cause regurgitation of
promastigotes from their
buccal cavity in the puncture wound through proboscis (biting
organ) and infection
results
Annex l:Life cycle of Leishmania donovani
-
8/11/2019 Kala-azar Control National Guideline
11/96
2.2 Pathogenesis of Kala-azar
Promastigotes are inoculated into the punctured site by the
feeding sandfly.
The entry of organism attracts mononuclear phagocytes
(macrophages) and
other white cells to the area. Certain macrophages can directly
kill the
parasite whereas others require prior stimulation before
attaining the
capability to destroy these parasites. Only resident (local)
unstimulated
macrophages are suitable for the establishment of the infection.
To avoid
being killed within the macrophages, the promastigotes
transform
themselves to amastigotes.
Leishmania donovani is a species, which tends to visceralize in
vertebrate
hosts. The infection is carried to the viscera through infected
macrophages
circulating in the blood or lymph. The spleen, liver and bone
marrow
become heavily infected. The skin may also get infected as a
sequel of
Kala-azar.
2.3 Pathophysiology of Kala-azar
The pathology of visceral leishmaniasis is due to blockage and
destruction
of the RE system with the most marked effects, being seen in the
spleen,
liver, lymph glands, bone marrow and intestines.
In active visceral leishmaniasis there is lack of a
cell-mediated immune
response to leishmanial antigens and therefore the parasites
multiply
rapidly. Humoral response with production of large amounts of
polyclonal
non-specific immunoglobulin especially IgG are found and also
specific
anti-leishmanial antibody are produced. Patients who have
recovered from
visceral leishmaniasis are immune from re-infection but relapses
can occur.
-
8/11/2019 Kala-azar Control National Guideline
12/96
2.4 Pathophysiology of Post Kala-azar Dermal Leishmaniasis
(PKDL)
In PKDL the epidermis shows several pathological changes in
different
combinations. These include hyperkeratosis, parakeratosis,
acanthosis,
follicular plugging and liquefaction degeneration of the basal
layer. The
latter is associated with incontinence of pigment and the
presence of many
melanin- containing macrophages in the upper dermis. Damage to
the
melanocytes is the cause of hypopigmentation.
The dermis shows varying intensities of inflammation with scanty
parasite,
which are best seen in slit smears of lesions. The infiltrate
may be
perivascular and band-like in the upper dermis.
Electron microscopy reveals ineffective stimulation of the
macrophage to
eliminate completely all the parasites. Neuritis involving the
small
cutaneous nerves in the dermis has been described in PKDL. This
may
suggest leprosy but lack of involvement of the superficial
nerves and other
cardinal signs of leprosy help to distinguish the two conditions
from one
another. Parasites can be demonstrated in only 20% of cases.
Epidemiology
Incubation period: Usually 3-6 months, which may range from 10
days to 2 years.
2.5 Clinical Presentation of Kala-azarA. Classical
Presentation
Fever-usually insidious onset and intermittent& may be
associated
with chills & rigor. Fever intensity decreases over time and
patient
may become afebrile for weeks to months followed by relapse
of
fever.
Weight loss
-
8/11/2019 Kala-azar Control National Guideline
13/96
Swelling of upper abdomen, specially left side.
Increased pigmentation- a feature of advanced disease.
B. Features of complication
Bleeding manifestation e.g Gum bleeding. Epistaxis and rarely
GIT
bleeding. This occurs as a result of thrombocytopenia &
hepatic
dysfunction.
Features of secondary infection.
C. Atypical presentation
Sub clinical- No fever.
Signs
A. General Examination
Raised temperature.
Anaemia- moderate to severe; may result from bone marrow
infiltration, hypersplenism, autoimmune haemolysis &
bleeding.
Gum bleeding & epistaxis
Lymphadenopathy- more common in Africa, less in Indian
Subcontinent
B. Abdominal Examination
Splenomegaly - in 100% cases. Develops quickly in the first
few
weeks and become massive as the disease progress.
Hepatomegaly
Ascites, oedema, asnasarca- in progressive disease, caused
by
hypoalbuminaemia
Cardinal Clinical feature
-
8/11/2019 Kala-azar Control National Guideline
14/96
H/O fever more than 2 weeks
Residing/traveling in endemic area
Splenomegaly
Weight loss
Anaemia
Clinical Presentation of PKDL
PKDL usually develops months to years following an attack of
untreated or
incompletely treated visceral leishmaniasis. However, 15% of
PKDL cases occur
without the preceding history of Kala-azar. They have only skin
lesions that are
varied. The lesions may be macular, papular, nodular or mixed.
Sometimes the
lesions of PKDL are extensive.
Overlapping, of 3 stages (Macular, papular and nodular) can
occur in an individual
simultaneously. In PKDL cases sensation over the lesions is
preserved in
contrast to leprosy where similar lesions have no sensations or
less sensation .
The skin lesions of PKDL do not ulcerate and self healing of the
lesions is not
reported. Though PKDL is a rare condition (I in 50-100 cases of
Kala-azar) it is
epidemiologically important because they act as the main
reservoir of infection. In
PKDL cases the parasite concentrates in the skin lesion and is
readily available to
the insect (Phlebotornus)vector when it bites the patient.
The clinical manifestations of these dermal lesions may be of
three types:
Macular lesion: These are the earliest dermal lesions. The usual
sites of
distribution of these macules are the trunk and extremities; the
face is less
commonly affected. The loss of pigmentation is not complete.
Papular lesion: These are also early lesions, which appear on
the nose,
cheeks and chin, often having a butterfly distribution
("butterfly erythema").
-
8/11/2019 Kala-azar Control National Guideline
15/96
They are very photosensitive, becoming prominent towards the
middle of
the day.
Nodular lesion:These replace the earlier lesions and
occasionally appear
from the very beginning. The nodules are generally found on the
skin and
rarely on the mucous membrane of the tongue and eyes. They
appear
mostly on the face but may appear on any part of the body. The
absence of
ulceration of the nodules is a characteristic feature of
PKDL.
2.6 Complications of Kala-azar:
1. Secondary infections:
Pneumonia
Pulmonary Tuberculosis
Amoebic or bacillary dysentery
Gastroenteritis
Herpes zoster
Chicken pox
Skin infection: boils, cellulitis, scabies
Cancrum oris
Septicaeemia
Otitis media
2. Bleeding manifestation- from gum, nose, GIT, retina, etc.
3. Post Kala-azar Dermal Leishmaniasis (PKDL)
4. Post Kala-azar laryngitis and colitis.
5. Post Kala-azar splenomegaly
6. Renal:
Glomerulonephritis
Nephrotic syndrome
-
8/11/2019 Kala-azar Control National Guideline
16/96
7. Cirrhosis of liver
2.7 Complications of PKDL:
PKDL occasionally coexist with VL; other post Kala-azar
manifestations such as
post Kala-azar mucosal leishmaniasis, uveitis, conjunctivitis,
and blepharitis may
be seen simultaneously in the same patient. Similarly,
involvement of the mucosal
surfaces, in particular in the mouth and the larynx, as well as
eye involvement such
as keratitis has also been described.
2.8 Laboratory Diagnosis of Kala-azar (annexure-2)
Diagnosis of Kala-azar may be possible by the following:
A. Indirect evidence or serological test (annexure 4)
B. Direct evidence or parasitological diagnosis
C. Others: Haernatological and Biochemical changes in blood
Laboratory Diagnosis of Kala azar
-
8/11/2019 Kala-azar Control National Guideline
17/96
A. Indirect evidence
1. Rapid dipstick rK-39 test (ICT for Kala-azar)
The rapid dipstick 'rK-39'test is the mainstay in the
serological diagnosis of
Kala-azar. It is recommended for identifying the case of
Kala-azar. (rK-39 test
may remain positive for 2 years after completion of Kala-azar
treatment)
1. a. How to perform the 'rK-39'test
Remove the test strip from the pouch or the vial
With a Fresh lancet, prick the fingertip of the patient
suspected to be
suffering from Kalaazar. Lancets; should not be reused because
of the risk
of transmitting HIV and Hepatitis B and C.
Let the blood come out on its own. Do not use pressure or
squeezing for
obtaining blood. Place one drop of blood on the absorbent pad of
the strip
bottom.
Place the test strip into a test tube so that the end of the
strip is facing
downwards. This would encourage the blood to migrate upwards
by
capillary action..
Add 2-3 drops of buffer solution provided with the kit to the
pad.
Read the results at 10 minutes. Please do not read the result
after 10
minutes.
1. b How to interpret the results
Positive result
A red line appears in the control area and another red line
appears in test area
where the blood has migrated through capillary action. There
should be two red
lines for the test to be positive. A faint red line also is to
be considered positive.
-
8/11/2019 Kala-azar Control National Guideline
18/96
Negative result
There is a red line in control area but there is no red line in
test area where the
blood has migrated by capillary action at 10 minutes.
Invalid test
There is no red line in control area or in the test area where
the blood is to migrate
by capillary action. The test is also invalid if there is a red
line in the test area but
no red line in the control area where the blood was initially
placed.
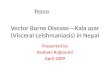
Table 2 If the test is invalid it should be repeated following
the correct
procedure.
Control area (C) Test area (T) Interpretation
Red line Red line Positive
Red line No line Negative
No line Red line Invalid test
No line No line Invalid test
Fig: 2 rK-39 test with positive and negative results
-
8/11/2019 Kala-azar Control National Guideline
19/96
1. c. Storage and supply of rK-39 test strips
The test strips should be stored safely at room temperature
between 20-30 degrees
Celsius. Temperature in excess of 30 degrees can reduce the
quality of the test.
The buffer solution should be stored at 20-8
0c. The test strips and the buffer should
not be frozen since freezing deteriorates the quality of the
reagent. The strip and
the buffer should be taken out from the vial or the pouch only
at the time of
performing the rK-39 test. The strip should only be used within
one hour of
taking out from the vial or the pouch.
It is not advisable to store large quantities of rK-39 in the
peripheral locations
where the temperature can not be properly maintained as required
in the
specifications. The districts locations (level II) should serve
as the supply points
for the peripheral units from where supplies can be made once in
a- month or when
the workers come for a review meeting.
1.d. Where should rK-39 test be done.
For the success of the elimination programme, it is necessary
that rK-39 test is
available to the poor people in the locality/area. The programme
manager should
map the various facilities in the public and private sector and
identify the locations
where the test is to be provided based on the followings:
(a) The health workers can detect enlarged spleen;
(b) The facilities where treatment of Kala-azar is
available;
(c) The distance of the facility from the community.
The test may be made available at the upazilla health complex
(level-I) in the
Government facilities. The programme manager in the district can
decide about
private and the NGO sectors where similar facilities are
available. The facilities in
the private sector that should be considered are hospitals and
private laboratories.Facilities where there is willingness and
interest in participating in the programme
-
8/11/2019 Kala-azar Control National Guideline
20/96
should be selected as the sites for testing with rK-39. MOU may
be signed with
the private sectors and NGOs. In the beginning of the programme,
a few facilities
should be selected. After ensuring that the services provided
are reliable, more
facilities may be included.
1. e. Advantages and limitations of IrK-391 test
The pros and cons of rk39 test in the diagnosis of Kala-azar are
summarized intable.
Table 3 Pros and cons of rK-39 test in the diagnosis of
Kala-azar
Pros Cons Test can be performed with one
drop of blood drawn from a finger
tip.
The result is obtained within 10
minutes
The test can be performed in anysetting by a trained health
worker
rK-39 test is reliable andcompares well with confirmatorytests
Therefore there is no need to
perform confirmatory tests in all
cases of Kala-azar
The test is also positive in cases of
PKDL
The rapid test rK-39 is positive in95-100% patients of
Kala-azar.
Early cases can be detected.( the
test become positive after twoweeks)
The test strips have to be stored at
recommended temperature and
humidity to maintain its reliability.
The test will lose its quality if
stored at temperature less than 20
and more than 30 degrees Celsius
for a long time (several months)
It is not recommended in patients
who have HIV-Kala-azar co
infections
The test remains positive even after
cure of Kala-azar, so the test cannot
be used in patients who have a
relapse or a reinfection
At present rK-39 test is notrecommended to decide about the
cure from kala azar since the test
continues to be positive even after
the patient has clinically recoveredfrom the disease.
-
8/11/2019 Kala-azar Control National Guideline
21/96
-
8/11/2019 Kala-azar Control National Guideline
22/96
be responsible for cross checking a proportion of positive and
negative tests with
standard.
2.11 Rapid Diagnosis of Kala-azar:
The rK-39 test for kala-azar is very reliable test for diagnosis
of Kala-azar in the
field situation and quick mass sero survey. Its sensitivity is
-100% and specificity
(92.3% - 95%) is also comparable to ELISA. So this test is
considered for
diagnosis of a Kala-azar at field situation. However, as with
all diagnostic tests
result must be correlated with other clinical information
available to the physician.
2.12 Diagnosis of PKDL by rK-39 test:
Suspected patients of PKDL should be screened by 'rK-39' test.
In cases of PKDL
with only macular lesions, the rK-39 test may be negative. These
cases should be
referred to a facility where detection of the presence of the
parasite can be done.
The confirmatory diagnosis of PKDL can be made by demonstration
of the
parasite (L.D.bodies) in the skin lesions by slit skin smear.
The nodular, papular or
the macular lesion is slit and tissue fluid is then placed on a
slide. The slide 1 then
stained (annexure 7) the same way as the bone marrow or splenic
puncture
aspirate. It is then examined for LD bodies under the
microscope. If smear is
negative or inconclusive, then skin puncli biopsy should be done
to detect the
parasite. If the above procedures fail to detect the parasite,
then the patient should
be tested by PCR for identification of parasite. It is
important. to observe all safety
precautions to prevent HIV/AIDS, Hepatitis B and C and other
blood borne
infections while doing the scraping of the skin for the
test.)
rK-39 Slit skin smear Skin punch biopsy PCR (annexure 9)
2. The other following serological tests are in current
practice.
Enzyme-Linked Immunosorbent Assay (ELISA)
Indirect Fluorescent Antibody Test (IFAT)
-
8/11/2019 Kala-azar Control National Guideline
23/96
Counter-Immunoelectrophoresis (CIE)
Latex Agglutition Test (LAT)
3. Hematological change:
Anaemia
Raised erythrocyte sedimentation rate (ESR)
Leucopenia: Neutropenia with relative lymphocytosis &
monocytosis.
Thrombocytopenia
4. Biochemical investigation (According to need)
Serum Bilirubin SGOT, SGPT
Serum Albumin
Serum Globulin
Urea, Creatinine
B. Direct evidence
a) Demonstration of parasites is the most conclusive evidence in
the diagnosis
of Kala-azar and PKDL, Parasites are detected by microscopic
examination
of smear prepared from:
Bone marrow
Splenic aspirates
Buffy coat
Liver biopsy
Lymph node biopsy
Skin lesions
b) Culture of the biopsy material in different media like N.N.N
media, Eagles
media etc. for isolation of parasite.
-
8/11/2019 Kala-azar Control National Guideline
24/96
c) PCR for DNA detection of L.D from the peripheral blood and
tissue
2.13 Bone marrow examination for amastigote of L.D bodies
(annex-5)
2.14 Splenic aspiration for amastigote of L.D bodies
(annex-6)
2.15 Diagnosis of Kala-azar in special situations
The diagnosis of kala-azar can be difficult in special
situations. These include the
following:
Kala -azar HIV co-infection
Kala-azar in pregnancy
PKDL with macular lesions
In cases of Kala-azar HIV co-infections and in cases of PKDL
with only macular
lesions the 'rK39'test may be negative. In Kala-azar HIV co-
infection the
diagnosis can be confirmed by bone marrow examination or splenic
aspiration in
Level III facilities. If both tests are negative or
inconclusive, then patient should be
sent to specialized laboratory for PCR identification. In PKDL
with macular
lesion, the diagnosis is made from the slit skin smear or a skin
punch biopsy in
level III facilities. If the slit skin or biopsy is negative or
inconclusive, the patient
should be tested for PCR identification. Patients with Kala-azar
in special
situations should be referred to the required level of facility
as appropriate.
Kala-azar HIV co-infection:rK-39 Bone marrow / Splenic aspirate
PCR
Kala-azar in pregnancy:
rK-39 PCR
PKDL with macular lesions only:
Slit skin smear Skin punch biopsy PCR
-
8/11/2019 Kala-azar Control National Guideline
25/96
2.16 Clinical Case Definitions of Kala-azar & PKDL:
There are three case definitions: Kala-azar (KA), Kala-azar
Treatment Failure
(KATF) and Post Kala-azar Dermal Leishmaniasis (PKDL)
Kala-azar (KA)
Fever or history of fever for two weeks or more: pattern of
fever
1. Irregular pattern of fever
And
Splenomegaly
And
2. High index of suspicion based on residing/ traveling in
endemic area
And
3. Absence of convincing evidence of any other febrile
illness
And
rK-39 test positive
A Case of kala -azar:
An individual in an endemic area who has fever for more than two
weeks,
splenomegaly and rK-39 test is positive should be diagnosed as a
case of
Kala-azar.
-
8/11/2019 Kala-azar Control National Guideline
26/96
Kala-azar Treatment Failure (KATF)
1. Earlier:diagnosed as Kala-azar
And
2. Took complete treatment
And
3. Again features of Kala-azar
And
4. Any positive lab evidence: Bone Marrow (BM)/ Splenic
aspiration (SP)
And
5. Period: wthin one year
Post Kala-azar Dermal Leishmaniasis (PKDL)
1. Multiple hypo pigmented areas on skin without loss of
sensation
With any one or combination of the following
a) macule
b) papule
c) nodule
d) history of Kala-azar
And
2. High index of suspicion based on residing/traveling in
endemic area.
And
3. rK-39 test positive
N:B: Clinically Suspected PKDL with rk39 negative cases need
tissue diagnosis.
-
8/11/2019 Kala-azar Control National Guideline
27/96
2.17 Case Definitions for Reporting:
1. Suspected Kala-azar:Patients with fever (of more than 2
weeks) from an
endemic area who has one or more of the features -1)
splenomegaly, 2)
anaemia and 3) weight loss
2. Confirmed Kala-azar:When the suspected case is confirmed by
positive
rk39 test or demonstration of parasite in the tissue (BM/SP) or
by PCR.
3. Kala-azar Treatment failure (KATF)
4. PKDL
When reporting the 'reporting case definition' term will be
added as a prefix to the
'clinical case definition' term of Kala-azar categorized as per
national guidelines.
Example:
A case is found to be KA as per clinical case definition.
For
reporting purpose this will be labeled as Suspected KA. If
rK-39
test is found positive or if parasite is demonstrable in any
tissue
exam test e.g BM, SP then the case will be labeled as
'Confirmed
KA
-
8/11/2019 Kala-azar Control National Guideline
28/96
2.18 Differential diagnosis
The following common differential diagnosis should be ruled out
considering their
frequency in Bangladesh. The indicators of differential
diagnosis are mainly:
prolong fever, splenomegaly, hepatomegaly, progressive weight
loss, emaciation,
skin changes and opportunistic infection.
1. Malaria
2. Leukemia
3.
Lymphoma
4. CLD
5.
Carcinoma of liver
6. Portal hypertension
7. CCF
8. Hemolytic anemia
9. Tuberculosis
10.Leprosy (for PKDL)
11.
Storage disease
Locations where diagnosis of Kala-azar and PKDL should be
offered:
As mentioned earlier, the programme should map out the
facilities in the district to
make the locations- where the diagnosis is available and it
should be known to the
people through behaviour change communication.
-
8/11/2019 Kala-azar Control National Guideline
29/96
Table 4 Location for Kala-azar and PKDL diagnosis
A) Level 1
In endemic areas in (union subcentre,community clinic or
others)1. Identify cases of fever of more than 2 weeks duration
2. Identify cases who have macular, papular or nodular skin
lesions but no other signs
3. Refer the patients with above problems to Upazilla health
complex for evaluation,
testing and treatment for Kala-azar or PKDL.
In endemic areas in upazilla health complex1. Check patients
with fever of more than 2 weeks associated with splenomegaly
2. Check patients with macular, nodular or mixed lesions without
loss of sensation.
Perform rK-39 test :(a) On all patients with fever of more than
2 weeks and have splenomegaly
(b) Patients with macular, papular or nodular or mixed lesions
and no loss of sensation.
3.Treat patients of kala-azar with first line drugs4. Refer PKDL
cases who need tisue biopsy and unresponsive cases of Kala azar to
level
III facility.
B) Level II
1. Check patients with fever of more than 2 weeks associated
with splenomegaly.
2. Check patients with macular, nodular or mixed lesions without
loss of sensation.
Perform rK-39 test :(a) On all patients with fever of more than
2 weeks and have splenomegaly
(b) Patients with macular or nodular or mixed lesions and no
loss of sensation.3. Treat patients of kala-azar with first line
drugs
4. Refer PKDL cases to who need tisue biopsy and unresponsive
cases of Kala azar to
level III facility.
C) Level III
1. Treat unresponsive Kala azar or KATF cases and refer back of
PKDL cases to level
I and II for treatment after tissue diagnosis.
2. Perform the slit skin smear/biopsy in suspected cases of PKDL
that are rK-39testnegative
3. Perform bone marrow /splenic aspiration in patients where
these are indicated, as a
part of drug monitoring studies or as a part of quality
assessment4. Treat any complications associated with bone
marrow/splenic aspirate
D) Level IV (specialized laboratories)
1. Perform PCR test for establishing the diagnosis of PKDL in
cases that are suspected
to have the disease but rK-39test is negative2. Diagnosis of
HIV-Kala-azar coinfection may be done by bone marrow/splenic
aspirate
-
8/11/2019 Kala-azar Control National Guideline
30/96
Learning unit - 3
TREATMENT OF KALA-AZAR and PKDL
Objective: at the end of the session the participant
will be able to-
mention the Treatment of KA and PKDL
identify the AE of treatment
mention the treatment of adverse events
recognize the patient to refer
describe the management at different levels
enumerate pharmaco-vigilance
illustrate the treatment flowchart
Content:
Treatment: KA
1st line treatment
2nd line treatmentTreatment in special situations: Pregnancy, Co
morbidity (Pneumonia, HIV,
Tuberculosis)
Treatment of complications:
Treatment of PKDL
Brief description on individual drug with adverse events
Management at different levels
Terms/ Criteria for referral, referral format
Management of adverse events
Pharmaco-vigilance
Treatment flowsheet/chart
-
8/11/2019 Kala-azar Control National Guideline
31/96
TREATMENT OF KALA-AZAR and PKDL
The objective of treatment for Kala-azar is to cure the patient,
prevent the
complications of the disease and minimize side effects of
medicines, contain drug
resistance and reduce the risk of spread of disease.
This can be achieved by complete treatment and monitoring.
Other
symptoms/diseases in patients of Kala-azar should also be
diagnosed and treated.
Appropriate drug with recommended dose and duration should be
given to a
patient of Kala-azar.
3.1 Drug treatment of Kala-azar: (annexure 10 &11)
3.1.1)
1st' line of treatment for Kala-azar patients
Drug of choice-
Miltefosine
Alternate choice- (Depending on availability in our country)
1. Paromomycin
2. Liposomal Amphotericin B
2nd line of treatment for Kala-azar patients:
1. Sodium Stibogluconate (SSG)
2. Amphotericin B deoxycolate
3.2 Miltefosine:
Miltefosine is a relatively safe oral drug for the treatment of
Kala-azar. It is now
recommended for use in Bangladesh. Miltefosine, a
membrane-active alkyl
phospholipid developed as an antineoplastic agent and now also
used topically in
breast cancer skin metastases has been shown to be active
against Leishmania in
various animal and human models. It is an oral antiprotozoal
agent, which has
-
8/11/2019 Kala-azar Control National Guideline
32/96
marked direct antiLeishmanial activity both in vitro and in
vivo. Though the mode
of action of Miltefosine is not clearly known, it may act
through inhibition of
phospholipid metabolism.
Miltefosine is well absorbed from the gastrointestinal tract and
is widely
distributed in the human body. The plasma concentrations were
roughly
proportional to the dose in the range of 50-150 mg/day. The
maximum serum
concentration ranges from 24-82 g/ml with tmax of 23 days. No
relevant sex
difference of the pharmacokinetic parameters have been observed.
Miltefosine
does not show oxidative metabolism by the cytochrome P45o enzyme
system.
3.2.1 When to avoid the use of miltefosine:
Miltefosine is the preferred first line of drug in all patients
of Kala-azar in the
elimination program except in the following situations:
Pregnancy
Married women of child bearing age who are not using
contraceptives
regularly and are at risk of becoming pregnant
Women who are breast feeding.
Children less than 2 yrs of age
3.2.2 Miltefosine may not be the ideal drug for patients of
Kala-azar
with severe under nutrition
severe anaernia and
patients with known history of kidney or liver disease
3.2.3 Recommended dose schedule:
-
8/11/2019 Kala-azar Control National Guideline
33/96
Dose: 2.5mg/kg body weight, in two divided dose by mouth in the
morning
and evening after meal for 28 days.
In case of missed doses, the scheduled 28 doses may be taken
within a period of 35
days. The daily dose should never exceed the recommended
amount.
The doses should be calculated as follows:
i) >12 years and weighing ~25kg: 100 mg. (cap 50 mg in
morning and 50 mg in
evening with meals)
ii) >12 years but weighing
-
8/11/2019 Kala-azar Control National Guideline
34/96
-
8/11/2019 Kala-azar Control National Guideline
35/96
separate ampoule. Any drug left over from open ampoules should
be
discarded immediately.DO NOT REUSE.
Routeof administration: intramuscular (I/M)
Site: Gluteus muscle (alternative buttock cheeks). If additional
sites are
required,administer in Vastus lateralis muscle in the
anterolateral
thigh, alternating thighs daily.
Frequency:Once a day
Duration: 21 days
Preparation: Paromomycin I/M injection solution for
intramuscular
injection, sterile, aqueous solution containing 375 mg/ml of
Paromomycin.
Prepare daily under supervision of doctors or trained health
care workers.
Each dose to be taken from a separate ampoule. Any drug left
over from
open ampoules should be discarded immediately. The recommended
dose is
15 mg/kg/day to be given IM for 21 days.
The total estimated cost per treatment of the drug is about 10
US Dollars.
The medicine is safe with minimal ototoxicity or nephrotoxicity.
In the
recommended dose, the ototoxicity is reversible.
Paromomycin should be avoided in patients with severe anaemia
with
hemoglobin
-
8/11/2019 Kala-azar Control National Guideline
36/96
3.3.2 Liposomal amphotericin B (LAB):
To improve the tolerance and widen the narrow therapeutic
window, a lipid
formulation of Amphotericin B is formulated. Amongst the
three
formulations liposomal Amphotericin B has the best safety
profile.
Liposomal amphotericin B is given IV in a total dose of 10-15
mg/kg
divided into 3 to 5 doses given either daily or on alternate
days.
It is one of the safest drug in both immunocompetent and
immunocompromised individual and also drug of choice in
special
situations( e.g. HIV and Pregnancy)
Liposomal amphotericin B should be administered by
intravenous
infusion (dextrose 5% infusion 100 to 300 ml) over a 30- 60 min
period
3.4 Treatment for kala azar treatment failure(KATF)
1. When a patient is diagnosed as a case of KATF after treatment
with a
particular 1st line agent, another alternative 1st line agents
should be
used.
2. If alternative 1st line agent is not available, then a
2nd
line agent should be
used.
3.5 Second line treatment for Kala-azar:
Indications:
1. When the first line drugs are not available
2. KATF cases when alternative 1stline drugs can not be used or
not available.
3.5.1 Sodium Stibo Gluconate (SSG):
SSG is an effective and widely used drug for KA and KATF. But
the drug
is pushed to second line because of its cardiac toxicity and is
recommended
by WHO to be phased out gradually.
SSG should be given at a dosage of 20mg/kg body weight, daily
IM
injection for 30 days.
-
8/11/2019 Kala-azar Control National Guideline
37/96
It is essential to weigh the patient before starting treatment.
Clinical Cardiac
monitoring should be done throughout the treatment period.
Route of Administration of SSG:
The preferred route of administration recommended is by deep
intramuscular (IM)
injection. It is better not to give the drug intravenously
(I/V)to avoid the risk of
cardiovascular collapse. After each injection the patient should
be kept in lying on
the bed under observation for at least half an hour because of
the risk of
hypotension and syncope. Unused reconstituted drug should be
discarded within
24 hours of preparation.
Adverse events of Sodium Stibogluconate Gluconate treatment:
In clinical practice of therapy with SSG, minor side effects are
common, moderate
side effects are common and severe side effects very rare. The
commonest
adverse events arepain at the injection site, muscle pain
(myalgia), joint pain
(arthralgia), loss of appetite, nausea and increased
transaminase level. These
symptoms are relatively mild and myalgia & arthralgia may be
controlled byparacetamol. QT segment changes (prolong QTc> 0.5
msec, T inversion) may
occur on the ECG, and therefore in ideal circumstances ECG
monitoring before
treatment and weekly during treatment should be performed.
Clinically important
arrhythmias (ventricular ectopics, ventricular Tachy cardia,
Torsades, de points,
ventricular fibrillation) or heart failure are very unusual, but
if occur may cause
sudden death. In ideal circumstances weekly monitoring of
hepatic and renal
function and estimation of amylase should be undertaken, though
these rarely give
rise to symptomatic illness.
There is no absolute contra-indication to SSG treatment, and
even severely ill
patients respond to treatment. SSG is not generally safe in
pregnancy and only
administered in pregnancy if benefits outweigh the potential
risks. If underlying
cardiac, renal or hepatic diseases are present, the patient
should be carefully
monitored during treatment.
-
8/11/2019 Kala-azar Control National Guideline
38/96
Since alternate relatively safe drugs are now available, SSG
should be phased
out from the national programme.
3.5.2 Amphotericin-B deoxycholate:
Recommended second line drug for treatment of Kala-azar and KATF
is
Amphotericin Bdeoxycholate.
Amphotericin B:
Amphotericin B deoxycholate is also an effective drug. But it
has high
toxicity profile and thus pushed to second line.
Amphotericin B deoxycholate 1 mg/kg daily or alternate day
is
recommended in the form of infusion (in 5% Dextrose solution 500
ml) for
15 doses having a cure rate of >90%. A test dose should be
given before
administration of Amphotericin B.
After preparating solution 5 drops /min for 30 min, then 10
drops/min for
another 30 min and if there is no reaction occurs, then the
infusion should
be given slowly over a period of 4-6 hours.
Adverse eventsof Amphotericin-B deoxycholate:
In some cases, there may be infusion releted side effects like
fever with chills
and rigors and thrombophlebitis. Generally these can be
controlled by
paracetamol and anti histaminics. Rarely hydrocortisone may be
required.
Rarely there may be severe adverse events like renal or hepatic
toxicity
hypokalaernia, and myocarditis and thrombocytopenia.
Amphotericin B should be administered by admitting a patient in
a hospital
during the entire period of treatment for close supervision and
monitoring of
side effects.
-
8/11/2019 Kala-azar Control National Guideline
39/96
3.6 Treatment for PKDL
Sodium Stibo Gluconate (SSG)
SSG should be given at a dosage of 20-mg/kg/day in intramuscular
route. It is
essential to weight the patient every time, before starting a
new cycle. Total 6
cycles of treatment should be given. Each cycle consists of 20
days of treatment
and there should be an interval of 10 days in between two
cycles.
Other treatment options of PKDL cases
Other treatment options of PKDL cases are Miltefosine,
AmphotericinB, liposomal
Amphotericin
Amphotericin-B
Dose: I mg/kg body wt daily or alternative IV (in 5%Dextrose
solution)
for 15 doses. Sixcycles with 10 days interval in between
cycles.
Route: IV
Amphotericin B (Liposomal):
Dose: 3mg/kg/day
Route: IV
Duration: Five(5) days in a cycle, sixcycles with 10 days
interval in
between cycles.
Miltefosine
Longer duration of Miltefosine are being used for treatment of
PKDL in
India. Dose and duration are yet to be standardized.
3.7 Complete Treatment of Kala-azar:
Patients of Kala-azar must complete treatment in the right dose
without any
interruption if a cure to be achieved. All efforts should be
made to ensure the
complete treatment. The followi measures are recommended to
complete the
treatment:
-
8/11/2019 Kala-azar Control National Guideline
40/96
Counsel the patient so that the patient/family fully understands
why it is
important to t complete treatment. Explain the consequences if
the treatment
is not taken as advised.
It is important to tell the patient, the family and the
community that the
premat discontinuation of the treatment would be the reason for
continued
risk of spread of t disease to others.
All treatment is provided free of cost. So economic constraints
should not
be a reason discontinuation of treatment and
Each patient should have a separate treatment box that contains
the full 28
days
Miltefosine) treatment. The treatment box should have the name
and
individu identification of the patient.
It is advisable to give the medicine supplies for a period of 3
days initially
so that if t patient has any problems a check up is done in the
health
center/hospital and treatment provided for the side effects if
required.
Use treatment card with a unique identification number. The card
shows the
number of d' the treatment has been taken by the patient.
The treatment of Kala-azar should be done under observation of
the health
care provider, any side effects or compliance or reinforcement
can be
ensured.
There should be coordination amongst the public sector and
private
providers and a foll up plan should be developed for each
patient so thatthere is no interruption of treatment.
The patient usually begins to feel better after a few days of
starting the
treatment but should be told that cure would occur only when
full treatment
has been taken..
The patient may discontinue the treatment because of the side
effects of the
medicine. The patient should be advised to contact the health
worker as
soon as a problem is detected. Tile health worker should treat
the side
-
8/11/2019 Kala-azar Control National Guideline
41/96
effects and reassure the patient so that the treatment is not
discontinued. If
improvement does not occur, the patient should be referred to
the hospital
(Upzilla health complex at level I or level II)
3.8 Pharmaco-vigilance:
Pharmaco vigilance is important to ensure the safety of the
medicines used in the
treatment of Kalaazar. It should be the responsibility of the
national programme to
ensure pharmacovogilance. The programme can provide very useful
information
but unless protocols are appropriate and the supervision is
strong the quality of
information may be compromised.
Each medicine used in the programme has some side effects. These
may be looked
for in the form of signs and symptoms. Laboratory tests can help
to recognize the
occurrence of the side effects early, Although tests like
haemogram, liver and
kidney function tests, electrolytes and ECG are recommended to
monitor the
patient, the inclusion of these tests in the programme is
difficult. This information
can be complemented by regular reporting of major and minor
adverse events. The
following measures will help to recognize early the occurrence
of adverse events.
Monitor the patient regularly for signs and symptoms (indicative
of adverse
events of drugs). These signs and symptoms should be classified
as major
and minor.
Perform the tests if possible in treatment sites and monitor the
results. This
can help to take timely measures even before the signs
appear.
Periodic meetings should be organized to review the reports of
major and
minor adverse events obtained from the different levels. This
will help
guide the prograrnme in recommending the tests that should be
done to
monitor the patients on treatment.
Regularly report the adverse events on the reporting formats to
higher levels
once in a month for a review and feedback
-
8/11/2019 Kala-azar Control National Guideline
42/96
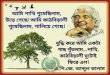
Figure 3
PeripheralPeripheral BloodBlood//UrineUrinerk39k39 KAtexKAtex
PCRPCR
65% 8765% 87--100% 72100% 72--100%100%
POSITIVE
TREATMENT
NEGATIVE
BM/BM/SpleenSpleen AspirateAspirate
MIC CULTMIC CULT PCRPCR
6767--94% 5094% 50--100% 82100% 82--100%100%
VL NEGATIVE
NEGATIVE
DiagnosticDiagnostic atat primeattackprimeattack inin
LeishmaniaLeishmania--HIVHIV coco--infectioninfection
Table 5 Adverse events and laboratory test used
Medicine Side effects Laboratory tests
Miltefosine Vomiting, Diarrhoea, Abdominal
pain (minor)
Persistent vomiting, Dehydration
(major)
Oedema, decreased urine, jaundice
(major)
Fatal nephro/hepato toxicity in
about 1% cases
Complete blood
counts
Electrolytes
Liver and kidney
function tests
Paromomycin Ototoxicity or nephrotoxicity Kidney function
tests,
Audiometry
Liposomal
Amphotericin B
Rare, Less toxic
Amphotericin B
Deoxycholate
Fever with chills and rigors (major)
Severe vomiting, dehydration
(major)
Electrolytes
Kidney function tests
ECG
-
8/11/2019 Kala-azar Control National Guideline
43/96
Oedema, decreased urine output
Arrhythmias (major)
SSG Arthralgia, myalgia (minor)
Arryhthmias, heart failure (major)
Oedema, decreased urine (major)
Jaundice (Major)
Electrolytes
ECG
Kidney functionstests
Liver function tests
3.9 Treatment of Kala-azar in special situations:
The treatment of Kala-azar in special situations is recommended
in centers where
appropria expertise and facilities are available. The following
conditions can beconsidered as special situations:
Pregnancy
Married women of reproductive age who are not using
contraceptives
regularly
Women who are breast feeding their babies
Children less than 2 yrs of age
Kal-azar with severe anaemia (Haemoglobiri less than 5 g/dl)
Kala-azar with TB
Kala-azar HIV coinfection or kala azar and AIDS
Kala-azar in a patient suffering from another serious
disease
3.9.1 Kala-azar in Pregnancy:
Vertical transmission of Kala-azar is possible and the
instituation of treatment is
imperative in cases of pregnant women with Kala-azar.
Amphotericin B is
recommended as the drug of first choice. It is reasonably safe
in the mother and
foetus. US Food and Drug Administration consider liposonial
Amphotericin B in
pregnancy category B. Miltefosine is contra-indicated. Antimoy
containing drugs
-
8/11/2019 Kala-azar Control National Guideline
44/96
have reproductive toxicity and mutagenic and oncogenic
potential, though the risk
is low.
Treatment of Kala-azar In Pregnancy:
1.
The best option in pregnancy with Kala-azar is Liposomal
Amphotericin B
2. When Liposomal Amphotericin B is not available, then
Amphotericin B
Deoxycolate or Paromomycin can be used.
3. When none of the safe drug is available,and benefit
outweights risk, then inj
SSG should be used in 2nd
and 3rd
trimester of pregnancy
3.9.2. Kala-azar in women who are breast feeding their
babies:
The choice is between amphotericin B and liposomal amphotericin
B. Miltefosine
is contraindicated.
3.9.3. Kala-azar in married women in reproductive age not on
contraceptives:
Miltfosine can be used in these patients but before initiating
miltefosine, a long
acting contraceptive should be given. The contraceptive should
be effective in
averting pregnancy for at least 2 months after completion of
treatment.
3.9.4. Kala-azar in children less than 2 yrs of age:
1.The best option in in children less than 2 yrs of age with
Kala-azar is Liposomal
Amphotericin B.
2. When Liposomal Amphotericin B is not available, then
Amphotericin B
Deoxycolate or Paromomycin can be used.
3. When none of the safe drug is available,and then inj SSG
should be used
3.9.5. Kala-azar with severe anaemia:
Anemia should be corrected by blood transfusion and /or
supplementation of iron
and folic acid before specific treatment started. If this seems
to delay the treatment
and the patient has severe Kala-azar then it is advisable to
treat the patient with
amphotericin B or liposomal amphotericin B. Similarly
nutritional status of the
-
8/11/2019 Kala-azar Control National Guideline
45/96
patient should be improved before administration of specific
treatment. This
treatment is available in level 11 and level III facilities.
3.9.6. Kala-azar HIV co-infection:
Level 11 facilities cannot check the HIV status. However, level
II facilities can
suspect the nfection based.on the risk profile of the patient
(FSW, MSM or an
IDU). It is also possible to the opportunistic infections
related to HIV and treat
Kala-azar in level 11 facilities. If HIV is suspectedbecause of
the risk profile or
HIV status is known the patient should be referred to a facility
where the HIV
status can be checked and facilities are available to provide
ART. Since the 'rK-39'
test may not be positive in patients who have HIV it is
necessary to refer such
patients with coinfection to a facility where the
parasitological diagnosis can be
made.
Guidelines for treatment and care are to be provided jointly by
National
programmes for Kala-azar elimination and the national AIDS
control programme.
These programmes should have collaboration to effectively deal
with the Kala-azar
HIV confection. The key steps in the diagnosi and treatment of
HIV Kala-azar
coinfection are summarized in the diagram. The details are
outsid the scope of
these guidelines. Response to SSG, Amphotericin B is far from
satisfactory.
Miltefosine has been found to be promising.
Kala-azar in special situation (In HIV co-infection)
1. The best option is Liposomal Amphotericin B
2. The other agents can be given if liposomal amphotricin B is
not available
3.9.7. Kala-azar TB co-infection:
The treatment of this co-infection requires treatment of TB with
DOTS and of
Kala-azar as per the national guidelines. If there are any
complications then the
treatment may have to be done in level III or specialized
facilities.
-
8/11/2019 Kala-azar Control National Guideline
46/96
3.10 Treatment of Kala-azar and KATF at different levels of
health facilities
The facilities referred to in the table can be in the government
sector, private sector
or NGOs.
Table 6: Kala-azar and PKDL treatment in different health
facilities
Level I at union level: Suspect cases of Kala-azar and PKDL and
refer them for diagnosis and treatment
to upazilia Health complex
Educate and convince the patient to complete the treatment as
advised
Follow up the cases of Kala-azar
Observe for vomiting, diarrhea or abdominal pain and for any
other severe sign
like jaundice, oedema or decline in the volume of urine passed.
If any of these are
detected, stop the treatment immediately. Refer cases e.g.
severe vomiting, severe
diarrhea, jaundice, oedema or decline in the volume of urine
immediately
Treat vomiting/diarrhea with ORS or home available fluids. Refer
patients to level
I upazilla health complex who do not improve.
Level I at Upazilla health complex:
Treat cases with Miltefosine. Ensure availability of effective
contraceptives for
three months to women at child bearing age that could get
miltefosine. Refer cases
who cannot be treated with miltefosine to level II
facilities.
Registrar and fill treatment cards and update them
Prepare the patient for treatment by treating anaernia and give
nutiritonal guidance
for undernutrition. Treat dehydration before the patient is
started on specific
medicines for Kalaazar
Provide written guidance to the health worker for follow up and
observation.
Advise patients on treatment to report as soon as any side
effects are observed.
Refer the PKDL cases who need tissue diagnosis to level III
Treat PKDL cases who are diagnosed clinically and rk39 test
positive and also
those cases who are referred back from Level III after tissue
diagnosis.
Report to level II facilities on kala azar patients once in a
month
Level II District and equivalent hospital: Treat cases with
Miltefosine. Ensure availability of effective contraceptives
for
three months to women at child bearing age that could get
miltefosine. Refer cases
who cannot be treated with miltefosine or other alternate 1st
line drug to level III
facilities.
Until miltefosine is available treat cases of Kala-azar with
other alternate 1st line
drug.
Patients on Miltefosine who are referred from government or
private facilities forside effects should be hospitalized for
treatment.
Refer cases to level III if Miltefosine or other alternate 1st
line drug is not
available. Non responsive Kala-aza patients and patients of KA
who have an
associated disease that can not be managed at level II
facilities should also be
referred..
All cases of PKDL who need tissue diagnosis and kala azar &
PKDL cases
suspected to be suffering from HIV coinfection should be
referred to level III
facility.
Supervise the staff working in level I facilities Report once a
month all
information (include reports from all level I facilities) to the
level III
-
8/11/2019 Kala-azar Control National Guideline
47/96
Level III
Treat cases of Kala-azar referred from level II facilities with
alternative
drugs. These includ pregnant women, married women in child
bearing age
who are not taking regular contraceptives, patients who do not
respond to
medicines given in level II facilities patients with severe
disease (severe
anaemia, severe under nutrition, kidney or liver disease) an
patients with
complications and side effects of medicine.
Parasitological diagnosis is recommended before starting the
treatment if
the patient require admission.
Treat Kala-azar cases who need to be treated with Amphotericin B
or
Liposomal amphotericin B.
Treat uncomplicated cases of Kala-azar who are self referred
withMiltefosine or other alternate 1st line drug..
Treat cases of PKDL who need tissue diagnoisis and Complicated
cases.
PKDL cases may be referred back to level I/ II for treatment
aftert tissue
diagnosis
Treat cases of Kala-azar HIV coinfections.
Report once a month to the National programme.
Specialized facilities
Ensure drug quality and maintain quality assurance of rK-39 by
PCR.
PCR testing for diagnosis in special cases.
Study and research on developing new drugs.
Report to the national programme once in a month.
-
8/11/2019 Kala-azar Control National Guideline
48/96
Learning Unit - 4
KALA-AZAR SURVEILLANCE AND REPORTING SYSTEM
Contents
Introduction
Reporting system
Reporting formatReporting- data flow
Report review and feedback
Reporting of treatment, hospitalized cases
Surveillance of Kala-azar and PKDL- passive surveillance,
Active
surveillance and sentinel surveillance
Objective: at the end of the session the participant will beable
to
describe the background and introduction
describe the reporting system for KA/PKDL
mention the reporting format
describe the data flow
mention review and feedback of Kala-azar
describe the reporting of treatment and
hospitalized cases
to enumerate passive surveillance, sentinel
surveillance,
enumerate options of surveillance, PKDL
-
8/11/2019 Kala-azar Control National Guideline
49/96
4.1 Introduction
Disease surveillance is a key component of kala-azar elimination
program. It
comprises passive and active surveillance of kala-azar cases and
vector
surveillance. Vector surveillance is described in Chapter IV.
Surveillance includes
reporting of all cases of kala-azar and PKDL. To make the
disease surveillance
effective, it is necessary to organize a system of regular
reporting, analysis, review
and feedback of information. Regular reporting and exchange
information should
be organized upwards, downwards and laterally in the system that
comprises
government, private sector, NGOs and the community as partners.
Feedback
linked to surveillance system is a critical element of the
elimination program.
Surveillance should also be used for sharing of reports
periodically to higher
authorities on a regular basis to facilitate and rationalize the
planning of
elimination program. Surveillance is useful for planning indoor
residual spray
through mapping of the areas to be sprayed and in monitoring the
trends of kala
azar.
4.2 Kala-azar Surveillance
Kala-azar surveillance will be a part of web-based national
disease surveillance
system centrally managed by IEDCR. Kala-azar elimination
program-specific
indicators will be incorporated in the reporting format. In
order to strenghten kala
azar surveillance, KA surveillance units will be set up at
district and upazila level.
Kala azar Elimination Program will have access to surveillance
data in real time.
The surveillance data will also be fed into the Management
Information System
(MIS) of DGHS.
4.2.1 Kala-azar Surveillance Units
I. Upazila Kala-azar Surveillance Unit
Head: UHFPO
Focal Person: MO (Kala-azar Elimination)
Statistical Assistant
-
8/11/2019 Kala-azar Control National Guideline
50/96
II. District Kala-azar Surveillance Unit:
Head: Civil Surgeon
Focal Person: MO (CS/DC)
Statistician
III. Government Medical College Hospitals:
Hospital Director
Focal Person: to be assigned by the Hospital Director
Statistician
4.2.2 Surveillance Reporting from UZHC
UHFPO will be responsible for implementation of KA surveillance
activities at the
upazila level and below. The activities will include:
1. Community awareness building through advocacy meetings
2. Organizing training for the health personnel
3.
Identification of suspected cases of kala-azar and PKDL at the
community
level and their referral (as per flow chart given thereof)
4. Confirmation of diagnosis by rK39 based ICT
5. Line listing of the confirmed cases at all levels using a
software which
should be compatible with the web-based disease surveillance
(software to
be provided by the program)
6. Reporting of confirmed kala-azar and PKDL cases including the
program
monitoring indicators
7. Generation of a unique identification number for each case
with
confirmation of diagnosis of KA and PKDL at all reporting
levels
-
8/11/2019 Kala-azar Control National Guideline
51/96
4.2.3 Flow Chart for KA and PKDL Detection from Community
Identification of suspected cases of KA and PKDL by First
Contact Points*(Fig. 1)
Referral of the suspected cases of KA and PKDL using prescribed
referral form
Diagnosis of the cases at UHC
Weekly reporting of incidence of KA and PKDL through the
web-based disease
surveillance system
*Health and family welfare centre
Union sub-centreCommunity clinic
NGO health clinic
Field staff of health and family welfare
Private practitioner
Informal health care providers
IPD of UHC
OPD of UHC
-
8/11/2019 Kala-azar Control National Guideline
52/96
Fig 1:Data Flowin Kala-azar Elimination Surveillance
H&FWC,
Union Sub
Centre
NGO Health Centre Private Practition
Level I:
Upazila KA Surveillance Unit
(UHC)
OPD of UHC IPD of UHC
Level II:
District KA Surveillance Unit
(Civil Surgeon Office)
Central Level:
National KA Surveillance Centre at
IEDCR
MIS
Director, DC
Focal point/PM/DPM
Kala-azar
Division
Medical College
Hospital
Sadar Hospital
OPD/IPD
Health Worker/
FP Worker
F IRST CONTACT POINT
Informal HealthCare ProvidersCommunity
Clinics
Web-based surveillance
-
8/11/2019 Kala-azar Control National Guideline
53/96
4.2.4 Reporting format for diagnosis of Kala-azar and PKDL
All suspected cases of Kala-azar and PKDL attending UZHC should
be screened
using the check list given below (Table 1 and 2). All reporting
units are expected
to enter the information using the reporting format mentioned in
Tables 3-6.
Prototype formats including the check list for identification of
cases for reporting
are summarized in the Tables below.
TABLE 8 Screening tool for diagnosis of kala-azar attending UHC
(Checklist)
Put a () mark onthe appropriate area.Items
1 History of fever for 2 weeks or more
2 Living in endemic area
3 Palpable spleen
If all of the above indicators are positive, then do rK39
test
Results of rK39 test: +ve -ve
PATIENTS WILL BE LABELLED AS A SUSPECTED KALA-AZARCASE IF THE
THREE INDICATORS MENTIONED ABOVE AREPOSITIVE.
PATIENTS WILL BE LABELLED AS PROBABLE KALA-AZAR CASEIF rK39 TEST
IS POSITIVE IN A SUSPECTED KALA-AZAR CASE. (ALL
PROBABLE KALA-AZAR CASES MUST BE TREATED ACORDING TONATIONAL
GUIDELINE)
PATIENTS WILL BE LABELLED AS CONFIRMED KALA-AZARCASES IF THEY
MEET THE CRITERIA FOR PROBABLE KALA AZARCASE AND ARE
PARASITOLOGICALLY CONFIRMED BY SPLEEN ORBONE-MARROW ASPIRATION.
ONLY THE SUSPECTED CASES AND PROBABLE CASES AREREQUIRED TO BE
REPORTED FOR THE SURVEILLANCE SYSTEM.
-
8/11/2019 Kala-azar Control National Guideline
54/96
TABLE 9 Screening tool for Suspected Cases of PKDL attending
UHC
(Check list)
Put a () mark on the appropriate area.Items
1 Previous history of kala-azar
2 Living in endemic area
3 Skin manifestations: with macule, papule or nodule without
loss of sensation
If all of the above indicators are positive, then do rK39
test
Results of rK39 test: +ve
-ve
Results of skin biopsy: +ve
-ve
PATIENTS WILL BE LABELLED AS A SUSPECTED PKDL CASEIF THE THREE
INDICATORS MENTIONED ABOVE AREPOSITIVE.
PATIENTS WILL BE LABELLED AS A PROBABLE PKDL CASEIF RK39 TEST IS
POSITIVE IN A SUSPECTED PKDL CASE.
PATIENTS WILL BE LABELLED AS CONFIRMED PKDL CASEIF SKIN BIOPSY
IS POSITIVE FOR PKDL. SKIN BIOPSY IS
RECOMMENDED WHEN THE FACILITY IS AVAILABLE OR IN
DOUBTFUL CASES.
ALL THREE CATEGORIES OF PKDL CASES SHOULD BE
REPORTED FOR THE SURVEILLANCE SYSTEM.
-
8/11/2019 Kala-azar Control National Guideline
55/96
TABLE 10 Reporting format for diagnosis of Kala-azar and
PKDL
Content
Name of the Reporting Unit
Upazila: Code:
District: Code:
Number of suspected kala-azar cases
Number of probable kala-azar cases
Number of suspected PKDL cases
Number of Probable PKDL cases
Number of confirmed PKDL cases
Table 11 Reporting format for treatment of Kala-azar
Content Level I
(Upazila)
Level II
(District)
Level III
(National)
Number of patients recruited for treatment
with Miltefosine
Number of patients completing treatment
with Miltefosine
Number of patients where treatment with
miltefosine was discontinued
Number of patients recruited for treatment withParomomycin
Number of patients completing treatment
with Paromomycin
Number of patients where treatment with
Paromomycin was discontinued
Number of patients recruited for treatment with
Amphotericin B
Number of patients completing treatment
with Amhotericin B
Number u, patients where treatment withamphotericin B was
discontinued
Number of patients recruited for treatmentwith Liposomal
amphotericin B
Number of patients completing treatment
with Liposornal amphotericin. B
Number of patients where liposornal
B was discontinued
Number of patients recruited for treatment
with SSG
Number of patients completing treatment
with SSG
Number of patients where SSG was discontinued because
of complications
Number of patients where SSG was ontinued because of
side effects of SSG
-
8/11/2019 Kala-azar Control National Guideline
56/96
-
8/11/2019 Kala-azar Control National Guideline
57/96
4.2.5 Reporting of information
The data flow for reporting of cases of kala-azar and PKDL
should follow the flow
chart shown in Fig 1. Upazila kala-azar surveillance unit should
send complete
information on kala-azar to the district focal point once in a
month before the first
Wednesday of each month. Once web-based surveillance is in
place, surveillance
data should be uploaded to the server maintained at IEDCR from
all levels. A
unique identifier should be used for each case during diagnosis
to avoid
duplication of reporting. If there are no cases then it should
be a zero report. The
data should be compiled at each level for the government,
private and facilities,
and reported mainly at Upazila and District levels in a
coordinated way. Data from
tertiary level health facilities including the medical college
hospitals may be
reported through District level or uploaded directly to
web-based surveillance
system if the facilities are available. There should be a
feedback mechanism to
make the best use of surveillance data by the government,
private and NGO
facilities for a common understanding of the problems that will
lead to
identification of possible solutions. The reports after
compilation should be
submitted to MO (Kala-azar elimination) of the UHC. The
statistical Assistant will
compile information from the reporting units from the
government, private and
NGO facilities and add their own.
A consolidated report should be sent to the district. The data
will cover
information for the preceding month. In the district, the
information from each
reporting facility should be entered on the computer and mapping
done to identify
the hot spots of Kala-azar in the district. The information flow
is summarized in
the illustration.
-
8/11/2019 Kala-azar Control National Guideline
58/96
Figure 2. Information flow
4.2.6 Report review and feedback
The focal points at all levels have the responsibility to
provide regular written
feedback to relevant stakeholders every month. Review and
feedback are
important at all levels to take appropriate action. The written
feedback from
upazila and district will have to be copied to the program.
4.2.7 Reporting of treatment
Information available from the Treatment cards provided to
patients and registers
will be used for preparing treatment report. The basic
information recorded include
Personal information about the patient including address, age,
sex,
weight, marital status, pregnancy and lactating status
Drugs used for treatment of kala-azar
Number of days treatment provided
If treatment course has been completed or not
Side effects of drugs
-
8/11/2019 Kala-azar Control National Guideline
59/96
Outcome of treatment
Treatment provider (public, private, NGO)
4.2.8 Reporting of hospitalized cases
Separate reports are needed for indoor patients of Kala-azar.
This should include
the total number of admissions, the total number of patients
admitted for
Kala-azar, the total number of deaths and the total number of
deaths due to
Kala-azar. The report should be categorized according to age
(under five, 5-14 and
15 and above) and sex. Information on pregnant women should be
included
separately in the monthly report. The outcome should be
summarized as (a) cured(b) worsened (c) died. To indicate the
number of patients who worsened and were
referred. The report should indicate the number of patients who
used the referral
services. The monthly report should indicate the number of
patients who
completed the treatment and the number of patients who are being
treated but have
not completed treatment. It is also necessary to indicate the
number of patients
who were started treatment but have dropped out.
4.2.9 Criteria for cure
The following criteria should be used to assess cure in every
patient treated for
Kala-azar.
Return of normal appetite
Remission of fever
Regression of spleen size
Improvement in anaemia and a rise in hemoglobin
The full course of treatment has been taken
Increase in body weight
-
8/11/2019 Kala-azar Control National Guideline
60/96
-
8/11/2019 Kala-azar Control National Guideline
61/96
4.3.4 Surveillance of PKDL
The surveillance of PKDL is as important as surveillance of
kala-azar since cases
of PKDL serve as a reservoir for disease transmission during the
inter epidemic
period. The program should do passive and active surveillance of
PKDL.
-
8/11/2019 Kala-azar Control National Guideline
62/96
Learning Unit - 5
INTEGRATED VECTOR MANAGEMENT (IVM)
Contents:
Vector behaviour and bionomics
Integreted Vector Management (IVM)
Indoor Residual Spraying (IRS)
Spray Programme
Monitoring and evaluation
Informing and involving the community
Personal protection
Environmental management (EVM)
Objectives: at the end of the session the participant will be
able
to
describe kala-azar vector (sand fly) behaviour and
bionomics
describe the components of integrated vector management
(IVM)
describe planning and implementation of indoor residual
spraying (IRS)
enumerate surveillance, monitoring and evaluation of
vector control measures
take measures on personal protection
learn about environmental management (EVM)-household
and surrounding conditions
-
8/11/2019 Kala-azar Control National Guideline
63/96
5.1. Vector behaviour and bionomics
Sand flies are small, dark grey, hairy insects measuring about
1.5- 2.5 mm in
length. Phlebotomus argentipes is probably the only species
amongst about 50
phlebotomine species that transmits kala-azar to humans in the
Indian subcontinent
(Bangladesh, India and Nepal). It thrives best in alluvial soil,
in areas with
relatively even/warm temperature, high humidity and abundance of
cattle
population. Eggs and larvae of sand fly can withstand immersion
in water for a
period of 5 days and fourth instar larvae for 14 days. Thus they
can survive even
flooding. Breeding places are found within a radius of about
20-50 meters from a
dwelling in dark, humid soil protected from the sunlight . In
cattle sheds, the
favorite breeding places are floor periphery with moisture and
organic debris.
Troughs found in and around cattle sheds are other important
breeding sites.
Immature stages are also often found in loose soil, cracks and
crevices in and
around dwelling houses, moist plinth and cattle sheds. Mud
houses are the main
resting site but also found in old brick built houses. Adult
sand fly takes rest in
cracks and crevices of both indoor and out doors of households.
Only the females
suck blood and they prefer cattle to human blood. Transmission
can occur after a
heavy build up of sand fly population because then the sand fly
shifts from cattle
to human because of scarcity of blood.
Adult sand fly is active after dark while during the day they
escape into their
resting shelters. Since the habitat of P. argentipes is mainly
indoor, it has
implications on the effectiveness of control measures. The sand
fly is a poor flier
and it can hop only short distances. It usually do not reach
above a height of 2
meter (6 feet). P. argentipes is a wet zone species. The highest
risk of disease
transmission in Bangladesh is therefore observed from the month
of April to
September, the months when the humidity is high (75-85%).
Susceptibility test so
far conducted by M&PDC unit of DGHS have shown that sand fly
is susceptible to
insecticides like Malathion, Permethrin, Deltamethrin and
Fenitrothion.
The vector behaviour and bionomics that make interruption of
kala-azar
transmission achievable inBangladesh include the following
factors:
-
8/11/2019 Kala-azar Control National Guideline
64/96
So far there is one species of sandfly,Phlebotomus
argentipesthat transmit
kala-azar in Bangladesh (Ref. M&PDC unit of DGHS)
The vector is sensitive to insecticides mentioned above
The insecticide spraying can be done with economy since the
spraying is
required up to a height of about 2 meters only and the
operations may be
confined to only indoors of households and cattle sheds and some
specific
outdoor sites. This entails a saving of about half the costs
when compared to
IRS for malaria eradication programme (MEP)
There is a historical evidence of interruption of transmission
as a collateral
benefit of MEP when kala-azar was virtually eliminated from
the
subcontinent as a result of insecticide spraying
The operation of IRS is to be limited to geographical area
affecting only the
endemic districts in Bangladesh
Cross border collaboration in IRS operations can interrupt the
transmission
of the disease in the border areas.
5.2 Integrated vector management (IVM)
IVM may be defined as a decision-making process for the
management of vector
population, so as to reduce or interrupt transmission of vector
borne diseases.
It deals with combination of two or more approaches along with
community
participation to achieve maximum benefit at a reasonable and
minimal cost. IVM
is recommended as a part of public health policy since this
strategy uses the
followings
decision making procedures based on the knowledge of vector
biology and
disease transmission
targeting of multiple vector control methods
planning and application of targeted interventions often in
combination and
synergistically
rational use of insecticides
use of cost-effective interventions
-
8/11/2019 Kala-azar Control National Guideline
65/96
multi-sectoral partnerships
involvement of communities including planning and decision
making at the
lowest possible administrative levels
measurable impact on disease transmission risks
use of effective public health regulation and legislation.
5.2.1 Components of IVM
Prevention of kala-azar and reduction of transmission are the
major strategies in
the elimination of the disease. The standards and standard
operating procedures for
prevention of kala-azar require application of the right mix of
interventions based
on vector behaviour and vector bionomics. IVM for elimination of
kala-azar
comprises of the following options:
Indoor Residual Spraying (IRS),
Personal protection to prevent human vector contact including
use of long
lasting insecticidal nets (LNs),
Environment management (EVM)
5.3 Indoor residual spraying (IRS)
At present IRS is the mainstay of vector control of kala-azar
elimination
programme. To maximize the impact, IRS and case search should be
synchronized.
The objective of IRS is to ensure safe and correct application
(uniform and
complete) of a residual insecticide up to the height of 2 meter
(6 feet) on indoor
surfaces of houses and animal shelters and also other important
outdoor resting
sites, e.g. cattle troughs, outdoor base (plinth) of houses,
chicken houses, pigeon
holes etc. This will help in achieving a marked reduction in the
populations of
vector sand fly and consequently a sharp reduction of kala-azar
transmission in the
target areas.
5.3.1 Timing of IRS
The build up in the population of the vector P. argentipes
starts in Bangladeshfrom April onward. The effectiveness of
insecticide deltamethrin deposits lasts for
-
8/11/2019 Kala-azar Control National Guideline
66/96