Embed Size (px)
Citation preview

Kala-azar Outbreak Management Guideline
August 2016
National Kala-azar Elimination Program
Bangladesh

Published by : National Kala-azar Elimination Program (NKEP) Communicable Disease Control (CDC) Disease Control Unit Directorate General of Health Services (DGHS) Ministry of Health and Family Welfare (MoHFW) Government of the People’s Republic of Bangladesh
Technical support : icddr,b
Financial support : UKAID, KalaCORE

Page | 1
Messages
From the Desk of Director General
Kala-azar, a vector borne disease is a public health problem for hundred years. Sand fly is the
responsible vector for this disease. Bangladesh, India, Nepal, Bhutan and Thailand signed a
memorandum of understanding initiated by World Health Organization to eliminate the disease
and are working together to achieve the elimination goal. Bangladesh is very near to the
elimination target as achieved the target in 98 among the 100 endemic Upazilas. The
elimination target is to keep the number of cases below 1 per 10,000 populations at Upazila
level. Strong monitoring, supervision and active involvement at field level is required to retain
achievement made by the government. Kala-azar Outbreak Management Guideline will assist
the programme related people who are working at field level as well as central level to direct
them while responding to any outbreak takes place. I appreciate the initiative of National Kala-
azar Elimination Programme under Communicable Disease Control Unit.
Professor Dr. Deen Mohd. Noorul Huq
Director General
Directorate General of Health Services Ministry of Health & Family Welfare

Page | 2
From the Desk of Director
Visceral Leishmaniasis, also called Kala‐azar, was first identified in 1824 in Jessore District of
Bangladesh. In 1903, a Scottish Physician Professor William Leishman and an Irish Physician
Professor Charles Donovan worked independently in India and identified the causative
organism of Kala‐azar from splenic aspirates. This parasite later came to known as Leishmenia
donavani and causing many deaths in the Indian subcontinent. Since then different drugs like
113 years old Injection Brahmanchari , recently included injection Liposomal Amphotericin B or
oral Miltefosine have been used for treatment of Kala-azar patients. Indoor Residual Spray
(IRS), environmental improvement at community level, social mobilization and new research
activities are being conducted to control the vector sandfly which are responsible for
transmitting the disease. National Kala-azar Elimination Programme (NKEP) made a great
success in achieving the control programme as 98 out of 100 Upazilas already accomplished the
elimination target which is the number of cases below 1 per 10,000 populations at Upazila
level. This downward leaning of the cases expose the programme to a new risk of case
emerging in areas that were previously considered non-endemic as previous history of Kala-
azar back the supposition. The Kala-azar Outbreak Management Guideline will strengthen the
programme people to response in such occurrence where programme can take proper strategic
plan accordingly. I anticipate this guideline will be admissible to all stakeholders who will work
in response to outbreak of Kala-azar.
Professor Dr. Abul Khair Mohammad Shamsuzzaman
Director Disease Control & Line Director, CDC
Directorate General of Health services Ministry of Health & Family Welfare

Page | 3
From the Desk of the Deputy Program Manager
In Bangladesh, Kala-azar is a public health problem for decades. It is assumed that Kala-azar
return back to the endemic areas in every 8 – 10 years. In 60s, Kala-azar was effectively
controlled due to DDT spray under malaria control programme. But in early 80s, Kala-azar
caused sporadic outbreak and in 90s it became endemic in Bangladesh, India and Nepal. In year
2005 these three countries agreed for working together to eliminate Kala-azar. The elimination
target was set as reduction of cases less than 01 per 10,000 populations every year in a defined
geographic region (for Bangladesh, Upazila). In Bangladesh the 98 out of 100 endemic Upazila
achieved the target within year 2015 which should be emulate by others. Now the elimination
target extended upto 2017 to complete the goal. To attain the goal and to retain the
achievement, early detection of Kala-azar and PKDL cases, social mobilization to control the
disease and Indoor Residual spray (IRS) for vector control should be emphasized. To keep the
success it is essential to root out any new source of infection. As history shows it is inevitable
that outbreak will occur in areas which were previously taken as non-endemic. For responding
to the threat, the Kala-azar Outbreak Management Guideline will act as a savior for the
programme people who are working in field level as well as in central level. National Kala-azar
Elimination Programme is appreciative to responsible persons who work together to develop
this guideline.
Dr. A. F. M. Akhtar Hossain
Deputy Program Manager, KEP, CDC
Directorate General of Health services Ministry of Health & Family Welfare

Page | 4
List of Contributor
Sl Name Address
1. Prof. Dr. Abul Khair Mohammad Shamsuzzaman
Director, Disease Control & Line Director, Communicable Disease Control (CDC), Directorate General of Health Services (DGHS)
2. Dr. Md. Abdus Sabur Deputy Director, CDC, DGHS
3. Dr. Md. Abdur Rakib Deputy Director (In-Charge), M&PDC, DGHS
4. Dr. AFM Akhtar Hossain DPM, Kala-azar, CDC, DGHS
5. Dr. FHM Nurunnabi Chaudhury Sr. Entomologist, CDC, DGHS
6. Md. Rezaul Karim Khan Sr. Entomologist (In-charge), CDC, DGHS
7. Md. Altab Hossain Entomologist, CDC, DGHS.
8. Narayan Prashad Maheswary Sr. Entomologist (Ret.) CDC, DGHS
9. Dr. AKM Abdul Kayum Technical Consultant, Kala-azar Elimination Program, CDC, DGHS
10. Ms. Fahima Yeasmin Lira Data Manager, Kala-azar Elimination Program, CDC, DGHS
11. Md. Mohabbat Hossain Khan Chief Health Superintendent, CDC, DGHS.
12. Md. Giash Uddin Health Superintendent, CDC, DGHS.
13. Ms. Rawshanara Health Superintendent, CDC, DGHS.
14. Ms. Shahanara Begum Health Superintendent, CDC, DGHS.
15. Dr. M. G. Mostofa Technical Advisor, Kala-azar Elimination Program, CDC, DGHS
16. Dr. Sabera Sultana National Professional Officer, NTD, WHO-Bangladesh
17. Dr. Mizanur Rahman National Consultant, Kala-azar, WHO-Bangladesh
18. Mr. Rajib Chowdhury Country Program Manager, KalaCORE-Bangladesh
19. Dr. Md. Ashraful Alam Principal Scientific Officer (Parasitology), IEDCR
20. Md. Saiful Islam Assistant Scientist, Infectious Disease Division (IDD), icddr,b
21. Dr. Muhammad Waliur Rahman Research Investigator, IDD, icddr,b
22. Dr. Dinesh Mondal Sr. Scientist, Nutrition and Clinical Services Division (NCSD), icddr,b
23. M. Mamun Huda Deputy Project Coordinator, NCSD, icddr,b
24. Dr. Sohel Shomik Deputy Project Coordinator, NCSD, icddr,b
25. Debashis Ghosh Assistant Coordination Manager, NCSD, icddr,b
26. Md. Shakhwat Hossain Assistant Coordination Manager, NCSD, icddr,b
27. Mr. Md. Sakhawat Hossain Data Management Supervisor, NCSD, icddr,b
28. Md. Shahadot Hossain Manager-Monitoring & Evaluation, NCSD, icddr,b
29. Md. Mahmudur Rahman M&E Officer, NCSD, icddr,b
30. Md. Abdul Alim Sr. Data Management Assistant, IDD, icddr,b

Page | 5
Executive Summary
Visceral Leishmaniasis (VL) or kala-azar (KA) victimizes Indian sub-continent including Bangladesh over the centuries since its first outbreak in 1824 in the territory of Jessore of Bangladesh. That outbreak turned into endemic and killed about 75,000 people. KA disappeared from Bangladesh as a collateral benefit of malaria eradication program. However in the early eighties it started to come back again and peaked in 2006 and victimized more than 100,000 people. These experiences tells us that if we could have a outbreak management activity following a standard guideline we could save many lives and could protect hundreds of people from disease as well. The current guideline on kala-azar outbreak management aims to fill up this gap in the National kala-azar Elimination Program of Bangladesh.
The guideline includes definition of kala-azar outbreak, its aim and steps. It describes the composition of kala-azar outbreak management teams and their responsibilities at different kevel of the health system to identify and investigate suspected outbreak(s). Adequate early and long term responses to an established outbreak are the pillars to prevent further transmission of the disease in the communities and hence save life and suffers of the people. The guideline describes in details about the early and long term responses to kala-azar outbreak. The guideline also underline important of communication with partners, stakeholders and media in relation to outbreak and how to declare end and report end of an our break.
We hope that the guideline will be useful for all who is involved in management of kala-azar situation in Bangladesh at all level of the public health system and for private partners, stakeholders and national and international policymakers as well.
This is the first version of kala-azar outbreak guideline so far. We invite you for your contribution to improving it further by telling us where improvements can be made as you use this Guideline.

Page | 6
Table of Content
1. Background ........................................................................................................................................... 9
2. Aim of this Guideline ........................................................................................................................... 10
3. Epidemiology ....................................................................................................................................... 10
3.1. Mode of Transmission ...................................................................................................................... 10
3.2. Clinical Features ............................................................................................................................... 11
3.3. Risk Factor ........................................................................................................................................ 11
4. National Kala-azar Elimination Program ............................................................................................. 12
5. Outbreak ............................................................................................................................................. 12
5.1. Introduction ..................................................................................................................................... 12
5.2. Steps in Outbreak Management ...................................................................................................... 13
5.3. Outbreak Management Team .......................................................................................................... 13
5.3.1. Member of the Management Team ......................................................................................... 13
5.3.2. Roles of the Management Team ............................................................................................... 13
5.4. Identifications of an Outbreak ......................................................................................................... 13
5.4.1 Outbreak Detection ................................................................................................................... 13
5.4.2. Declaration of an Outbreak....................................................................................................... 16
5.5. Outbreak Investigation .................................................................................................................... 16
5.6. Outbreak Response .......................................................................................................................... 18
5.6.1. Early Control Measure .............................................................................................................. 18
5.6.2. Long Term Specific Prevention and Control Measure .............................................................. 18
5.7. Communication ................................................................................................................................ 19
6. End of Outbreak .................................................................................................................................. 19
6.1. Declaration of the Outbreak Over ................................................................................................... 19
6.2. Outbreak Report .............................................................................................................................. 19
7. Outbreak Evaluation ........................................................................................................................... 20
8. References .......................................................................................................................................... 20
9. Important Documents/links ................................................................................................................ 21
10. Annexes ........................................................................................................................................... 22
Annex-A: Forms ....................................................................................................................................... 22
Form-1: Suspected VL Outbreak Reporting Form ............................................................................... 22
Page | 7
Form-2: Suspected VL Outbreak Reporting Log .................................................................................. 23
Form-3: Index Case/Cluster Identification Form................................................................................. 24
Form-4: Index Case/Cases Interview Form ......................................................................................... 25
Form-5: Sand fly Collection Record Form ........................................................................................... 27
Form-6: Household Screening ............................................................................................................. 28
Form-7: IRS Record and Focal Search Register Form .......................................................................... 29
Form-8: VL/PKDL Case referral Form .................................................................................................. 30
Annex-B: Checklists, SOPs and Others .................................................................................................... 31
Checklist-1: Duties of Chairperson of OMT ......................................................................................... 31
Checklist-2: for OMT task ................................................................................................................... 31
SOP-1: for No Kala-azar Transmission Activity ................................................................................... 32
SOP-2: for organizing ACD-Camp at villages level ............................................................................... 35
Terms of Reference: Outbreak Management Team (OMT) ............................................................... 39
Reporting format: Kala-azar Outbreak ............................................................................................... 40
List of past Kala-azar endemic areas in Bangladesh ........................................................................... 42

Page | 8
Acronyms
ACD Active Case Detection ACSM Advocacy Communication and Social Mobilization AHI Assistant Health Inspector BCC Behavioral change and communication CDC Communicable Disease Control CS Civil Surgeon DC Disease Control DDT Dichlorodiphenyltrichloroethane DGHS Directorate General of Health Services DNA Deoxyribonucleic acid DPM Deputy Program Manager HA Health Assistant HH Household HI Health Inspector icddr,b International Centre for Diarrhoeal Disease Research, Bangladesh IEC Information, education and communication IEDCR Institute of Epidemiology, Disease Control and Research IRS Indoor Residual Spraying ITN Insecticide Treated Net KA Kala-azar KEP Kala-azar Elimination Program LD Leishmania donovani M&PDC Malaria & Parasitic Disease Control MEP Malaria Eradication Program MIS Management Information System MO Medical Officer MoU Memorandum of Understanding MT Medical Technologist NGO Non Government Organization NKA New Kala-azar NKEP National Kala-azar Elimination Program NKTA No Kala-azar Transmission Activity OMT Outbreak Management Team PKDL Post Kala azar Dermal Leishmaniasis SACMO Sub-Assistant Community Medical Officer SSN Senior Staff Nurse ToR Terms of Reference UH & FPO Upazila Health and Family Planning Officer UHC Upazilla Health Complex UKAID United Kingdom AID UKC Upazila Kala-azar Coordinator VL Visceral Leishmaniasis WHO World Health Organization
Page | 9
1. Background
Visceral leishmaniasis (VL), generally known as Kala-azar (KA) is a major public health problem in Bangladesh with an estimated incidence 12400-24990 cases in per year [1]. Historically the origin of the first recorded outbreak in the Indian sub-continent belongs to the territory of Bangladesh and was in 1824 in Jessore district. In that outbreak 75,000 people died and several thousands of people left their houses to escape from the disease. It is believed that since then the periodic outbreak of VL continued to happen in the territory of present Bangladesh [2]. The disease almost disappeared as a collateral benefit of the malaria eradication programme with indoor residual spraying (IRS) with DDT. However, when DDT spray was ceased in 1970, VL started to come back again in the early eighties, peaking in the new millennium. VL can be eliminated from the Indian sub-continent as a public health problem due to its unique epidemiological features. The features are characterized by: Leishmania donovani being the only causative agent, the human is the only reservoir, female sand fly P. argentipes is the only vector, it is limited to certain geographic areas, it can be diagnosed at the household level with a rapid test and effective oral and injectable (single dose) drugs for treatment of VL are now available. All these preconditions encouraged WHO to initiate a VL elimination program in the Indian sub-continent and the Government of Bangladesh, India and Nepal signed a Memorandum of Understanding (MoU) to eliminate VL from these three countries by 2015. The elimination target is to reduce VL cases < 1 per 10,000 people at sub-district, block and district level respectively in Bangladesh, India and Nepal by 2015 [3]. Recently the elimination target time is extended up to 2017 and two new countries (Bhutan and Thailand) joined in this initiative (see section-4). The NKEP under the DGHS has made remarkable progress in the last 7 years and achieved the target of elimination in 98% of upazilas with its limited resources and logistics. As a result the disease burden has come down dramatically. Despite focused interventions, as time progresses there will remain sporadic cases and clusters of cases in areas where there were previously no cases, or have not been cases for substantial periods. Recent data shows VL cases are re-emerging from sub-districts where cases with PKDL are left unrecognized and untreated and where program activities have stopped. In 2015, there were 420 new cases of VL reported in the country; this gradual decline means that the program needs to be alert and responsive to a spike in new cases in previously highly endemic areas where there have been a gradual and consistent fall, and also to new cases emerging in areas that were previously considered non-endemic[4]. Although poorly defined, there is no formal strategy in the national guideline to define or deal with this ‘outbreak’ that can pose a threat to sustaining the VL elimination target in the future. Considering the objective of the consolidation phase of the elimination program, it will be crucial to develop definition of VL outbreak in Bangladesh and prepare the management guideline accordingly. Therefore, this guideline for VL outbreak management has been developed by CDC, DGHS in collaboration with icddr,b through the financial support from

Page | 10
KalaCORE project funded by UKAID. The document was developed through organizing several workshops where multi-disciplinary experts were included (see the boxes 1 & 2 below). The objective of this document is to provide operational guidance for the management of outbreaks of Kala-azar in Bangladesh.
2. Aim of this Guideline
This guideline aims to ensure an effective and coordinated approach for Kala-azar outbreak, from initial detection to formal closure of the outbreak. It promotes a consistent approach from Upazila to central level of the elimination program which includes a set of standards for Kala-azar outbreak management in Bangladesh.
3. Epidemiology
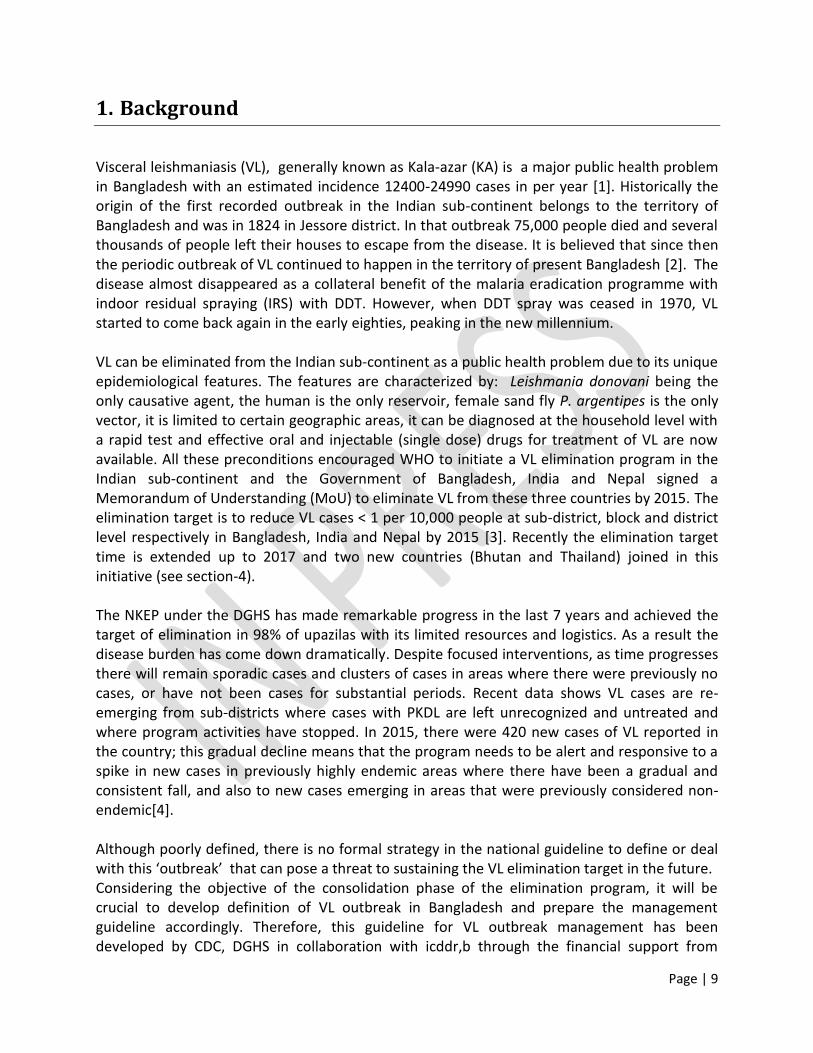
VL is a re-emerging infectious parasitic disease and its history in British Bengal revealed that the epidemic peaks were recorded in the 1820s, 1860s, 1920s and 1940s [5]. As it said earlier, the disease was disappeared from this sub-continent as a collateral benefit of Malaria eradication program during 1950-60; however, it re-emerged again in early eighty. The sporadic VL cases reported in the 1970s and an outbreak occurred in Pabna district in 1980 [5]. Since then VL has been reported every year and till than more than one lac cases were reported. Recent WHO estimate showed that the annual VL incidence ranges from 12 400 to 24 900 cases in Bangladesh [1]. The disease was prevalent in about 45 districts out of 64 in Bangladesh. However as a benefit of the program interventions, the VL incidence has been decreasing dramatically, and currently about 100 Upazilas from 26 districts are endemic. The disease is highly clustered in nature and most the cases report from Mymensingh District. The figure- 3.1 is showing the total number of Kala-azar cases reported during 2000 to 2015 depicts static decline of Kala-azar cases in overall Bangladesh [3]. According to passive surveillance report from 2000-04, the VL case fatality rate was about 1.5% [1]. In a recent study showed that VL mortality was about 6% and in Mymensingh it was about 1% where the programme activities are very much strong. However definite data on morbidity and mortality due to Kala-azar are not adequate in the current reporting system as most of the deaths in Bangladesh occur at home and those are not reported to Upazila health complexes [5].
3.1. Mode of Transmission Sand Flies (Phlebotomine) are responsible vector for Leishmania infection. Sandfly is very small, about one-third the size of a typical mosquito. Female sandflies only bite as they require blood for the maturity of their eggs. Sandflies are infected with the parasite when it bites an infected human, rodent, dog or any other host. A part of life cycle completed in the sandfly gut and the parasite is transmitted to human or to other host when it bites them. Other modes of

Page | 11
transmission (through blood transfusions, contaminated needles, from pregnant mother to her baby) are very rare. In Bangladesh, The female Phlebotomas argentipes is the only vector; humans are the only reservoir, there is no intermediate host and Leishmania donovani is the only species responsible for VL [6, 7].
Figure-3.1: Kala-azar cases and deaths in Bangladesh, 2000-2015
Sources: National guideline for Kala-azar case management 2015
3.2. Clinical Features Fever is the most recognizable feature of VL. Any person, who is living or has been exposed to the endemic region recently, has more than 2 weeks of fever with enlarged spleen and liver is a classical phenomenon of VL. Weakness, malaise, anorexia, anaemia and weight loss are the other orthodox features of VL. rk39 strip test is the most effective laboratory tool for diagnosing VL, though clinical diagnosis is the most important aspect till date. Other methods are the spleenic aspiration cytology, different molecular tests, DAT etc. The disease is fatal if not treated. Even with treatment the mortality rate is high (~10%) [6, 7]. About 17% of persons treated for VL in Bangladesh develop Post–Kala-azar Dermal Leishmaniasis (PKDL) within 5 years after apparent cure of VL [8].
3.3. Risk Factor
As per WHO, socio-economic conditions, malnutrition, population mobility, environmental changes and climate changes are the risk factor for Kala-zar in the endemic countries. In Bangladesh there are few studies reported risk factor of Kala-azar which includes, proximity to the previous Kala-azar case in same household, mud house, sleeping on floor etc. [9]

Page | 12
4. National Kala-azar Elimination Program Vision: Kala-azar Free Bangladesh by 2020. Goal: The goal is to contribute in improving the health status of vulnerable groups and at-risk population living in Kala-azar endemic areas of Bangladesh by the elimination of Kala-azar. Target: The target of Kala-azar elimination programme in Bangladesh is to reduce the incidence rate of the disease to less than 1 case per 10000 populations at the upazila level in Bangladesh by the year 2017. Elimination strategies: A regional strategic framework for elimination of Kala-azar of WHO/SEARO 2011-2015 has been endorsed by the Regional Technical Advisory Group. It comprises of the following components:
1. Early diagnosis and complete treatment: All suspected cases of Kala-azar and PKDL should have access to recommended diagnosis and treatment.
2. Integrated vector management (IVM): The IVM strategy aims to prevent and decrease vector (sandfly) spread within the community and reduce human-vector-pathogen contact, and is done by controlling vector through IRS in households and distributing LLIN within the kala-azar patients.
3. Effective disease surveillance: An effective surveillance system should be strengthen to ensure early diagnosis, provide prompt treatment, undertake active case detection, and report kala-azar cases from the public and private sector.
4. Social mobilization and building partnerships: For community participation and social mobilization for behavioural change communication (BCC) at community level; and partnership building would help to achieve the goal of Kala-azar elimination program.
5. Operational research: Operational research aims to explore strategies, interventions, tools and knowledge that can monitor the quality, coverage, effectiveness and performance of the kala-azar elimination program activities and evaluate the drug efficacy, insecticide resistance, quality of drugs, treatment compliance, pharmaco-vigilance and LLIN use.
5. Outbreak
5.1. Introduction An outbreak is defined as an episode in which two or more people, thought to have a common exposure, experience a similar illness or proven infection [10]. Outbreak investigation aims to control the outbreak, prevent additional cases of the disease, identify the source and learn lessons for the future. In Bangladesh, Kala-azar surveillance includes both active and passive surveillance system. Passive surveillance is usually conducted by Upazila Health Complexes (UHC) whereas active surveillance is jointly conducted by the NKEP at central level and UHC
Page | 13
level. Based on recent surveillance data it revealed that Kala-azar outbreak is remerging from some non-endemic areas where no Kala-azar case was reported in last 3-5 years. Total 17 Upazilas from 15 districts reported about 47 cases in the year of 2014, where no Kala-azar was reported in the mentioned time period [3]. Kala-azar outbreaks can occur in the community setting, across geographical and political boundaries. An early, rapid response to an outbreak through the Outbreak Management Team (OMT) (see 5.3) is the key to its effective control and prevention. This section includes details on Kala-azar outbreak investigation and response strategies in Bangladesh.
5.2. Steps in Outbreak Management Managing outbreak involves a logical series of steps to identify risk factors and put control measures in place. Standards for managing Kala-azar outbreaks are developed following the steps used elsewhere [11] and the summarized in the figure-5.2.1 below.
5.3. Outbreak Management Team The Kala-azar outbreak management team (OMT) is a multi-disciplinary group which will work together to manage an outbreak. The team will be chaired by Director, CDC, DGHS. There are two different levels of group in this management team in NKEP which are central level team and Upazila level team. The central level team is considered as a core team which mostly includes staffs from central level program, respective Civil Surgeon (CS) at District level and relevant collaborative partners (IEDCR, WHO, icddr,b etc). Upazila level team will be based on the program staffs at the Upazila Health Complex.
5.3.1. Member of the Management Team
The outbreak management team composition are given in the table-5.3.1
5.3.2. Roles of the Management Team
The OMT will be leaded by the chair of the team, Director, CDC, DGHS. Both the central and Upazila level team will closely work with the Kala-azar surveillance team to suspect/detect Kala-azar outbreak in Bangladesh. The core team is responsible for planning and coordinating the investigation. Upazila level team will work with the central level team in their respective Upazila for outbreak detection, investigation and response. Brief terms and reference (ToR) of the OMT are noted in Annex-B.
5.4. Identifications of an Outbreak
5.4.1 Outbreak Detection
Outbreak management begins with the timely identification of an outbreak. Establish an operational definition of Kala-azar outbreak is an important to suspect a Kala-azar outbreak. The definition of Kala-azar outbreak is noted below (see table-5.4.1) which has been developed

Page | 14
based on VL expert opinion from the workshop held in February, 2016 at Dhaka, Bangladesh on development of “Kala-azar Outbreak Management Guideline in Bangladesh (2016)”. Currently Kala-azar surveillance is being operated in 100 endemic Upazilas through the web based surveillance system hosted by MIS, DGHS. Central level outbreak team will jointly work with surveillance team to suspect any Kala-azar outbreak based on the surveillance data. At the same time the team will check the MIS aggregated diseases surveillance data for others areas where the VL specific web based surveillance system is not in placed. The central level team also will build communication with other District hospitals and UHCs which are not under web based surveillance system to suspect any Kala-azar outbreak in other geographic areas in Bangladesh. Similar to central level team, Upazila level team also works with Upazila level surveillance team and other partners to suspect Kala-azar outbreak. When Upazila level team will suspect any Kala-azar outbreak in their respective Upazila then they should report it to the national level team as soon as possible using Form-1 (see Annex-A) for further assessment to detect the existence of Kala-azar outbreak. The central level team will maintain the suspected Kala-azar outbreak reporting log using Form-2 (see Annex-A). Table-5.3.1: Composition of Kala-azar outbreak management team
OMT at Central level [No.] OMT at Upazila level [No] 1. Director, DC and Line Director, CDC, DGHS (
Chair) [01] 2. Deputy Director, M&PDC [01] 3. Assistant Director, CDC [01] 4. Civil Surgeon of respective District [01] 5. Deputy Program Manager (Kala-azar) (Focal
Person) [01] 6. Entomologist [01] 7. Ento-Technician [03] 8. Medical Technologist (Lab) [01]
1. Upazila Health & Family Planning Officer (UH&FPO) (Lead, Upazila level) [01]
2. Medical Officer (DC)/Medical Officer (MO)/ Sub-Assistant Community Medical Officer (SACMO) (Focal Person, Upazila level) [01]
3. Sr. Staff Nurse (SSN) [01] 4. Medical Technologist (Lab) [01] 5. Store Keeper [01] 6. Statistician [01] 7. Health Inspector (In charge) [01] 8. Assistant Health Inspector-Corresponding
Union 9. Health Assistant-Corresponding Village 10. IRS Team [06]
Collaborative Institute/Organization
1. Technical Advisor, NKEP, CDC, DGHS [01] 2. National Consultant, Kala-azar, WHO
Bangladesh [01] 3. Medical Officer, NKEP, WHO Bangladesh [01] 4. Data Manager, NKEP, WHO Bangladesh [01] 5. Microbiologist [01], IEDCR / icddr,b 6. Epidemiologist [01] , IEDCR / icddr,b 7. Social Scientist/Anthropologist [01], IEDCR /
icddr,b 8. Bio-statistician [01], IEDCR / icddr,b
Collaborative Institute/Organization
1. As required at Upazila/Union/Village level 2. Upazila Kala-azar Co-ordinator (UKC) from
KalaCORE
The following steps should be followed jointly by the central and Upazila level team to detect if a real Kala-azar outbreak exists: Identify the location of index case (s) (first reported case (s)) by the HI/AHI at the
corresponding UHC by using Form-3 (see annex-A)

Page | 15
Conduct semi-structured interview of index cases of Kala-azar by a Medical Officer (DC)/Medical Officer/SACMO at UHC by using Form-4 (see annex-A)
Figure-5.2.1: Kala-azar outbreak management overview
Kala-azar case reported /identified (as a suspect of outbreak)
Outbreak detection (5.4.1)
Outbreak declared
Review as required OMT convene
(5.3.1)
No OMT convene
No outbreak
Actions Review as required
Early control
measure (5.6.1)
Control measure (5.6.2)
Communications (5.7)
No Kala-azar Transmission
Activity (NKTA)
Source/Mode of spread Protect persons at risk Monitor effectiveness
OMT minutes Communication
protocol Media
End of outbreak
Declare outbreak over; Constructive debrief and lessons
identified; Final outbreak report; Action lessons learnt
Epidemiological, Microbiological, Entomological,
Environmental, Veterinary & Social/Anthropological
Investigation (5.5)
Page | 16
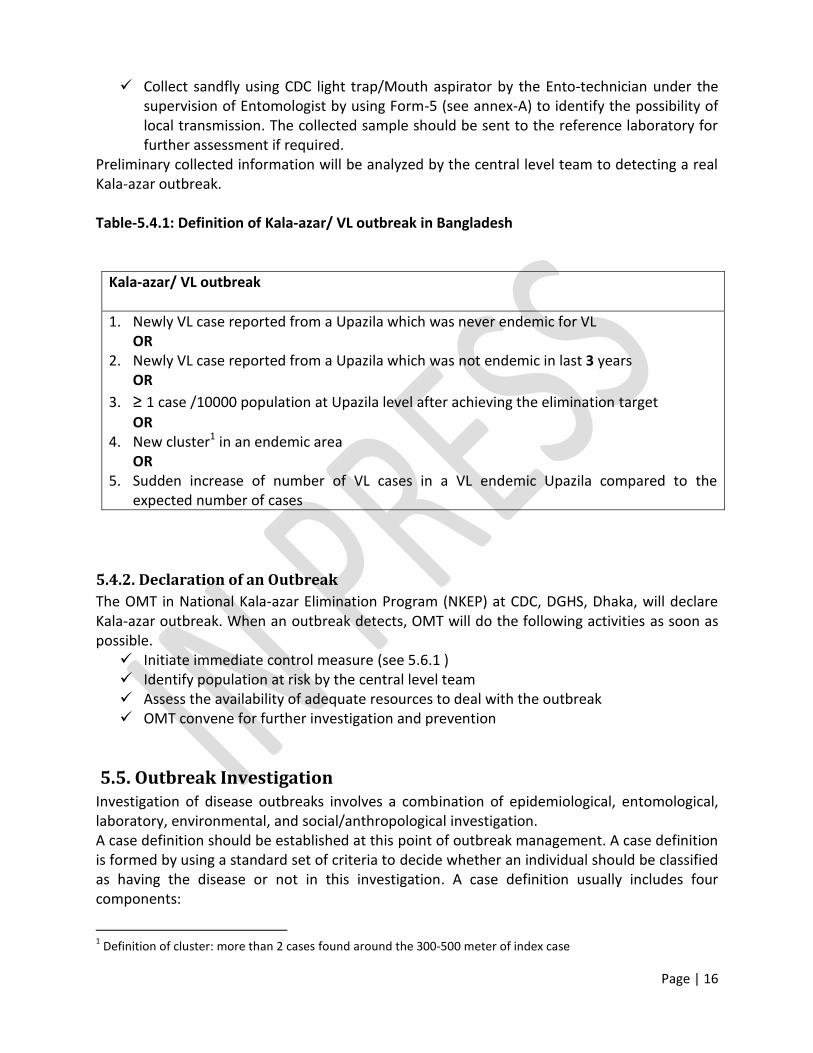
Collect sandfly using CDC light trap/Mouth aspirator by the Ento-technician under the supervision of Entomologist by using Form-5 (see annex-A) to identify the possibility of local transmission. The collected sample should be sent to the reference laboratory for further assessment if required.
Preliminary collected information will be analyzed by the central level team to detecting a real Kala-azar outbreak. Table-5.4.1: Definition of Kala-azar/ VL outbreak in Bangladesh
Kala-azar/ VL outbreak
1. Newly VL case reported from a Upazila which was never endemic for VL OR
2. Newly VL case reported from a Upazila which was not endemic in last 3 years OR
3. ≥ 1 case /10000 population at Upazila level after achieving the elimination target
OR 4. New cluster1 in an endemic area
OR 5. Sudden increase of number of VL cases in a VL endemic Upazila compared to the
expected number of cases
5.4.2. Declaration of an Outbreak
The OMT in National Kala-azar Elimination Program (NKEP) at CDC, DGHS, Dhaka, will declare Kala-azar outbreak. When an outbreak detects, OMT will do the following activities as soon as possible. Initiate immediate control measure (see 5.6.1 ) Identify population at risk by the central level team Assess the availability of adequate resources to deal with the outbreak OMT convene for further investigation and prevention
5.5. Outbreak Investigation Investigation of disease outbreaks involves a combination of epidemiological, entomological, laboratory, environmental, and social/anthropological investigation. A case definition should be established at this point of outbreak management. A case definition is formed by using a standard set of criteria to decide whether an individual should be classified as having the disease or not in this investigation. A case definition usually includes four components:
1 Definition of cluster: more than 2 cases found around the 300-500 meter of index case

Page | 17
Clinical information about the disease Characteristics about the people who are affected Information regarding the location or place Specification of time during which the outbreak occurred.
In this document Kala-azar case definition has been defined based on a study published elsewhere [3] and National Guideline for Kala-azar Case Management in Bangladesh, 2016 (table-5.4.2) [12]. Attempts should be made to identify additional persons who meet the case definition. This enables a more accurate estimate of the magnitude of the outbreak, it reduces the likelihood of bias which may occur by only focusing on cases detected early in the investigation and it increases the sample size. A structured questionnaire should be used to collect detailed information regarding cases. Information to be collected from each case includes: Identifying information History of travel/previous residence Demographic information Clinical information (date/time of onset, signs and symptoms, hospitalisation, death etc) Laboratory information Risk factor information (contact with known case, environmental exposures etc) Contact with individuals with similar symptoms.
If required, a case control study could be designed to identify the risk factor(s) of the outbreak for developing appropriate control/preventive measure against Kala-azar.
Table-5.4.2: Case definition of VL/Kala-azar
VL/ Kala-azar Case Definition
Suspected VL case Fever for more than 2 weeks Residing/ history of travelling in Kala-azar endemic areas Splenomegaly (palpable spleen) Any additional symptoms: weight loss, anaemia, darkening of skin
Probable VL case Fever for more than 2 weeks Residing/ history of travelling in Kala-azar endemic areas Splenomegaly (palpable spleen) Any additional symptoms: weight loss, anaemia, darkening of skin Positive rK39 test
Confirm VL cases Fever for more than 2 weeks Residing/ history of travelling in Kala-azar endemic areas Splenomegaly (palpable spleen) Any additional symptoms: weight loss, anaemia, darkening of skin Positive rK39 test Positive for Lesihmania Donovani (LD) in tissue / LD DNA positive
by molecular test

Page | 18
5.6. Outbreak Response Kala-azar outbreak response includes two types for control measures such as i) Early control measures and ii) Long term specific prevention and control measure. The actions of early response measure should be taken immediately after the detection of outbreak. This will prevent the transmission of the disease among the risk population. The actions related to long term specific prevention and control measures should be taken considering factors identified by all level of detailed investigation.
5.6.1. Early Control Measure
The early control measure includes “No Kala-azar Transmission Activity (NKTA)” of the program. This activity is undertaken to interrupt the transmission of the VL from recently treated case of Kala-azar (index case) to the new population in the community. This activity will be done as per National Kala-azar Guideline for Kala-azar Case Management in Bangladesh, 2016[12]. The SOP for conducing NKTA is attached in Annex B. Briefly the NKTA includes the followings activities at the community of the index case: The epidemiological team consisting of medical officer will use to investigate the index
case and conduct active searching for NKA & PKDL cases (using Form-6 in annex A) in and the around the 60-100 HH of the Index Case. Suspected case goes under observation by the Medical Doctor and MT lab at the same time. After that the case will be referred to the nearest UHC for further confirmation and management.
The Entomological team will conduct KA vector and larval survey around the index case. The team will conduct IRS in the living rooms as well as cattle shed of 60-100 households around the index household to control the vector density. The form -7 in annex A will be used to maintain the record.
At the same time the team will also indentify the suspected sand fly breeding places in and around the 60-100 households in using the larvaecide.
In addition, Advocacy Communication and Social Mobilization (ACSM) activity will be done to make community members aware of transmission.
5.6.2. Long Term Specific Prevention and Control Measure
The eventual methods for prevention and control of the disease depend highly on the findings from detailed investigation of the outbreak. The following prevention and control measures could be taken for Kala-azar outbreak:
1. IRS/Bed-net Distribution: Blanket IRS/ITN distribution to the indexed case village will be done as vector control activities. IRS/ITN distribution will be done as per Integrated Vector Management (IVM) Guideline for Kala-azar Elimination Program (KEP), Bangladesh, 2016[13]
2. ACD-Camp: Organized villages level camp to detect additional cases. Repeat the NKTA if required. ACD-Camp will be organized as per National Guideline for Kala-azar Case Management in Bangladesh, 2016 [12]
3. IEC/BCC activities: Conduct the IEC/BCC activities where the outbreak occurred to make the community people more aware about Kala-azar. Existing IEC/BCC material will be used in this activity.

Page | 19
4. Maintaining surveillance: Initiate and maintain regular effective surveillance in affected area (as required)
These type of preventive and control activities should be maintained for next three years after declaration of the outbreak over (cases declined/end).
5.7. Communication Early, effective communication is important to control the disease during outbreak. The following point need to be considered during communication regarding VL outbreak: Ensure appropriate information is given to the public especially those at high risk Ensure accuracy and timeliness of the outbreak related activities Include all those who need to know Use media constructively Disseminate information on any lesson learnt from managing the outbreak
Chair of the OMT will be responsible to communicate with central level collaborative partners who should engage in the outbreak management activities. The chair is also responsible to maintain the communication with media effectively. UH&FPO is the responsible person regarding communication at Uapzila level. S/he will maintain communication with the community people, Upazila level collaborative partners as well as central level OMT during outbreak investigation and response.
6. End of Outbreak
6.1. Declaration of the Outbreak Over The OMT will decide when the outbreak is over and will make a statement to this effort. The decision to declare the outbreak over should be informed by on-going risk assessment and when: There is no longer a risk to the public health that requires further investigation or
management of control measures by an OMT. The number of cases has declined/end. The probable source has been identified and treated.
6.2. Outbreak Report OMT will prepare a written report while declaring that ‘outbreak is over’. OMT will decide the ‘list of sharing’ of the prepared report and will take necessary action accordingly. Final outbreak report should be completed as soon as possible of the formal closure of the outbreak. Lessons from the outbreak as well as necessary recommendations should be disseminated among the respective partners and key stakeholders. Scientific publication may be an effective way to bring out the lessons and recommendation to world for future use.
Page | 20
7. Outbreak Evaluation
A thorough evaluation of the outbreak response helps bring about continuous improvements in practice. The aim of the evaluation is to determine if the incident objectives were met and to identify positive outcomes and document areas for improvement. The following is a list of criteria that helps evaluation: Preparedness for this type of investigation (includes resources, guidelines,
questionnaires, databases, etc) Coordination of outbreak meetings, communication (including media management) Organization Record keeping (responsibility) Epidemiology Investigation processes and control initiatives implemented.
Program existing monitoring and evaluation team could engage to evaluate the outbreak management activities for its further improvement.
8. References 1. Alvar J, Velez ID, Bern C, Herrero M, Desjeux P, Cano J, Jannin J, den Boer M, Team
WHOLC: Leishmaniasis worldwide and global estimates of its incidence. PLoS One 2012, 7(5):e35671.
2. Bern C, Chowdhury R: The epidemiology of visceral leishmaniasis in Bangladesh: prospects for improved control. Indian J Med Res 2006, 123(3):275-288.
3. Mondal D, Singh SP, Kumar N, Joshi A, Sundar S, Das P, Siddhivinayak H, Kroeger A, Boelaert M: Visceral leishmaniasis elimination programme in India, Bangladesh, and Nepal: reshaping the case finding/case management strategy. PLoS Negl Trop Dis 2009, 3(1):e355.
4. National Guideline for Kala-azar Case Management, 2016. In. Edited by Program K-aE: CDC, DGHS; 2015.
5. Huda MM, Chowdhury R, Ghosh D, Dash AP, Bhattacharya SK, Mondal D: Visceral leishmaniasis-associated mortality in Bangladesh: a retrospective cross-sectional study. BMJ Open 2014, 4(7):e005408.
6. Joshi A, Narain JP, Prasittisuk C, Bhatia R, Hashim G, Jorge A, Banjara M, Kroeger A: Can visceral leishmaniasis be eliminated from Asia? J Vector Borne Dis 2008, 45(2):105-111.
7. Rahman R B, M, Kabir, H, Naher, FB, Mahboob, S: Kala-azar situation in Bangladesh. In. Dhaka, Bangladesh: CDC, DGHS, Ministry of Health and Family Welfare, Government of the Peoples Republic of Bangladesh; 2008.
8. Islam S, Kenah E, Bhuiyan MA, Rahman KM, Goodhew B, Ghalib CM, Zahid MM, Ozaki M, Rahman MW, Haque R et al: Clinical and immunological aspects of post-kala-azar dermal leishmaniasis in Bangladesh. Am J Trop Med Hyg, 89(2):345-353.

Page | 21
9. Bern C, Courtenay O, Alvar J: Of cattle, sand flies and men: a systematic review of risk factor analyses for South Asian visceral leishmaniasis and implications for elimination. PLoS Negl Trop Dis 2010, 4(2):e599.
10. National guidelines on the management of outbreaks of norovirus infection in healthcare settings In. Edited by (NDSC) NDSC. Dublin 8, Ireland; 2003.
11. Helen McAuslane DM, Caroline Hird, Lorraine Lighton, Marian McEvoy: Communicable Disease Outbreak Management: Operational guidance. In. Edited by England PH. 133-155 Waterloo Road, Wellington House, London SE1 8UG; 2014.
12. National Guideline for Kala-azar Case Management, 2016. In. Edited by (NKEP) NK-aEP: CDC, DGHS; 2016.
13. Integrated Vector Management (IVM) Guideline for Kala-azar Elimination Program (KEP), Bangladesh. In. Edited by (NKEP) NK-aEP. Dhaka: CDC, DGHS; 2016.
9. Important Documents/links
1. National Guideline for Kala-azar Case Management in Bangladesh, 2016 2. Integrated Vector Management (IVM) Guideline for Kala-azar Elimination Program (KEP),
Bangladesh, 2016 3. Web based surveillance system for Kala-azar in Bangladesh;
http://103.247.238.82:8080/dhismohfw/dhis-web-commons/security/login.action 4. Regional Strategic Framework for Elimination of Kala-azar from the South-East Asia
Region (2011-15); http://www.searo.who.int/entity/world_health_day/2014/KA_CD239.pdf
5. Indicators for monitoring and evaluation of the kala-azar elimination programme; http://www.who.int/tdr/publications/documents/kala_azar_indicators.pdf
6. Monitoring and Evaluation Toolkit for Indoor Residual Spraying (IRS) http://www.who.int/tdr/publications/documents/irs_toolkit.pdf

Page | 22
10. Annexes
Annex-A: Forms
Form-1: Suspected VL Outbreak Reporting Form
Form-1: Suspected VL Outbreak Reporting Form [For the health facility (UHC/others) who report the outbreak to the central level]
Name of reported hospital / health facility:_______________________________
Type of facility: |___|
Other, specify……………………….)
1=Community Clinic; 2=Union Health Centre; 3=Upazila health complex; 4=District hospital; 5=Tertiary hospital, 6= referral hospital/medical college/specialized institution, 8=other
Health sector: |___| 1 = public; 2 = private; 3 = NGOs
Reporting person’s name:____________________ Designation:__________________
Date of reporting (dd-mm-yyyy):____________________________
1. Type of suspected Outbreak?
Sl. Definition of Outbreak Yes/No
1. Newly VL case reported from a Upazila which was never endemic for VL
2. Newly VL case reported from a Upazila which was not endemic in last 3 years
3. ≥1 case /10000 population at Upazila level after achieving the elimination goal
4. New cluster in an endemic area
5. Sudden increase of number of VL cases in a VL endemic Upazila compared to the expected number of cases
2. List Location(s) of the Outbreak?
Sl Case/Cluster Name Address Comments
3. Brief description of the Outbreak?
………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………………
Reporting Person’s Name:_________________________
Signature:____________________________________ Date (dd-mm-yyyy):___________________

Page | 23
Form-2: Suspected VL Outbreak Reporting Log
Form-2: Suspected VL Outbreak Reporting Log [For Central level use]
Sl. Reporting
date (dd/mm/yyyy)
Reported by
(Name, Designation,
UHC)
Key message (regarding outbreak including place and
time)
Action-1 Action-2 Action-3 Action-4 Action-5
Remarks/File
location
Outbreak detection
(yes/no)
If yes, date
(dd/mm/yyyy)
OMT
convene (yes/no)
If yes, date
(dd/mm/yyyy)
Early control
measure
yes/no)
If yes, date
(dd/mm/yyyy
)
Investigation
(yes/no)
If yes, date (dd/mm/yyy
y)
Long term
Control measure (yes/no)
If yes, date
(dd/mm/yyyy)
Form-3: Index Case/Cluster Identification Form
Form-3: Index Case/Cluster Identification Form
[For UHC level to used by HI/AHI/HA/CHCP]
Name of UHC / health facility:_______________________________
1. Patient's Serial no. (1, 2, 3, ........)
2. Cluster no. (1., 2, ....... N/A)
3. Full name
4. Father's name / Husband's name
5. Guardian name
6. Date of birth
7. Age in Year
8. Gender Male Female Third gender
9. Contact number 1
10. Contact number 2
11. District
12. Upazila
13. Union
14. Mouza
15. Moholla/Para/Street No
16. Village
17. House Hold Head Name
18. Household longitude
19. Household latitude
Location visited by:____________________________
Designation:__________________________________
Signature:____________________________________ Date (dd-mm-yyyy):___________________

Form-4: Index Case/Cases Interview Form
Form-4: Index Case/Cases Interview Form
For UHC level use by Medical Officer]
Name of the patient:_______________________________________________________________
Name of hospital / health facility patients finally treated:_________________________________
Type of facility: |___|
other (specify)
1=Community Clinic; 2=Union Health Centre; 3=Upazila health complex; 4=District hospital; 5=Tertiary hospital, 6= referral hospital/medical college/specialized institution, 8=other
Health Sector: |___| 1=public; 2=private; 3=NGOs
Patient serial no: |___| 01, 02, 03….etc Cluster/Village No. : |___||___||___| (where applicable)
Name of the respondent:______________
Patients Address: Father/Mother/Guardian name: __________________ Contact Number: ____________________
District name: _________________________________ Upazila name: _______________________
Union name: __________________________________ Mouza/Ward name: __________________
Village name: _________________________________ Moholla/Para/Street :______________
Sl Question Code
1. Age of the patients (in years)
|__| |__|
2. Sex 1=male; 2=female, 3=Third Gender
|__|
3. Marital Status 1=Currently Married, 2=Separated, 3=Deserted, 4=Divorced, 5=Widowed, 6=Never Married
|__|
4. Occupation 0=children (yrs <5), 1=Own agriculture, 2= labor; 3=Skilled worker (person who has training on his/her profession), 4=Unskilled worker, 5= Small business; 6= Big business; 7= Govt. Job; 8=Pvt. Job, 9=Work in aboard; 10= Student; 11=Housewife; 12=Others specify…………)
|__|
5. Educational qualification (00=Illiterate)
|__| |__|
6. Have you heard about Kala-azar before getting the disease? 1=yes, 2=no
|__|
6.1. If Yes, when (dd-mm-yyyy)
7. Past history of VL 1=yes, 2=no
|__|
If Yes, when (dd-mm-yyyy)
8. Past history of VL in your family? 1=yes, 2=no
|__|
8.1. If Yes, when (dd-mm-yyyy)

Page | 26
Sl Question Code
9. Has any member of your family suffering from Kala-azar? 1=yes, 2=no
|__|
9.1. If yes, who?
10. Did you travel VL endemic areas? 1=yes, 2=no
|__|
10.1. If yes, Where?
10.2. When? (dd-mm-yyyy)
10.3. How many nights did you stay there (00 for ‘no’ stay at night)
11. Did anybody travel to your home from VL endemic areas 1=yes, 2=no
|__|
11.1. Who?
11.2. From where?
11.3. When? (dd-mm-yyyy)
11.4. How many nights did he/she stay at your home (00 for ‘no’ stay at night)
12. How many days did it take between getting fever and seeking health care providers (local term)?
|__| |__| |__| days
13. How many days did it take between going to the health care providers (hospital) and knowing that you had suffered from kala-azar?
|__| |__| |__| days
14. How many days did it take to start treatment after you became aware from doctor that you had kala-azar?
|__| |__| |__| days
15. Consultations for KA treatment
1st provider
2nd provider
3rd provider
4th provider
5th provider
Provider type (1=healer/ unqualified doctor; 2= chemist; 3=health worker; 4= pvt qual dr /pvt clinic/NGO; 5=govt dr/govt Hospital; 6= Specialised hospital; 8= Other(specify__________________)
Date of visit (dd-mm-yyyy)
Test done for KA (0=no, 1=rapid diagnostic test rk39; 2=DAT; 3= bone marrow aspirate; 4= spleen aspirate; 5= clinically; 6=rk39+spleen or bone marrow; 8= other(specify________________)
Treatment given (1=SAG; 2= Amphotericin; 3=Miltefosine; 4=liposomal Amphotericin B; 5= Immunotherapy; 6= Combination; 9=don’t know; 8= other (specify________________)
Was treatment interrupted?(1=yes; 2= no)
If yes, duration of the interruption (days)
If yes, reason for the interruption (1=side effects; 2= personal problems; 3= no money to pay for treatment; 4=no money for travel; 5= no drugs available; 6= migration; 8=other (specify______________)
Comments (if any): ……………………………………………………………………………………………………………………
Name of interviewer:_________________________ Designation:___________________________
Signature:_________________________________ Date (dd-mm-yyyy):______________________

Page | 27
Form-5: Sand fly Collection Record Form
Form-5: Sand fly Collection Record Form (Using CDC Light trap/ Mouth Aspirator)
Name of the household head:__________________________ District name: ___________________
Upazila name: ______________________________________ Village name: ____________________
House hold no.: |___||___||___|
Method of collection: |___| (1=CDC Light trap, 2= Mouth Aspirator)
Time of Collection: |___| (1=1st day, 2= 2nd day) Date of collection (dd-mm-yyyy):___________
Temperature and humidity of the place of test:
Temperature (in OF): |__| |__| . |__| Humidity (in %):|__| |__| . |__|
Exposure time: |______| ( in minutes) Total sand fly collected; |___|___|
Types of sand fly
Sand fly
Males Females Total
Unfed Fed Gravid
Phlebotomas argentipes
Phlebotomas papatasi
Sergentomyia spp.
Total
Comments (if any): ……………………………………………………………………………………………………………………
Entomologist Name:_________________________
Signature:__________________________________ Date (dd-mm-yyyy):______________________

Page | 28
Form-6: Household Screening
Form-6: Household Screening
Name of household head:_________________ District name:_________________________
Upazila name: __________________________ Village name: _________________________
House hold no:|___||___||___|
Name of the respondent (preferably HH head) : ____________________________
Socio-Demographic characteristics
Sl. Name of the family members (Chronological order)
Age (in year)
Sex (1=male, 2=female, 3= transgendert)
Past kala-azar Past PKDL Currently with (1=yes, 2=no)
(1=yes, 2=no)
If yes, date (dd-mm-yyyy)
(1=yes, 2=no)
If yes, date (dd-mm-yyyy)
fever > 2weeks
Skin lesion like PKDL
1. hh head
2.
3.
4.
5.
6.
Name of interviewer:_________________________ Designation:___________________________
Signature:__________________________________ Date (dd-mm-yyyy):______________________
Verified by:_________________________ Designation:___________________________
Signature:__________________________________ Date (dd-mm-yyyy):______________________

Page | 29
Form-7: IRS Record and Focal Search Register Form
Form-7: IRS Record Form (For focal spray)
Name of intervention area (Village): __________________ Mouza name: _________________
Union name:_______________________________ Upazila name _________________
District name:______________________________
Index cases no: |__| |__| (Mention name and registration no. of the index case/cases ___________________________________________)
Time of intervention(dd/mm/yyyy): from ______________________
to_________________________
HH no. |__| |__|
HH head name
Sprayed? (1=yes, 2=no)
If yes, date (dd-mm-yyyy)
If yes, no. of
If no, why?
No. of places where
Larvicide deploy
(0,1,2...)
bed-room sprayed
Cattle shed
Other place
01
02
03
..
..
..
60
Supervisor name:_________________________ Designation:___________________________
Signature:__________________________________ Date (dd-mm-yyyy):______________________
Verified by:_________________________ Designation:___________________________
Signature:__________________________________ Date (dd-mm-yyyy):______________________

Page | 30
Form-8: VL/PKDL Case referral Form
Form-8: VL/PKDL Case referral Form
SL. No:______ Date (dd-mm-yyyy):_________________
Patient’s Name:________________________________________
Parent’s Name:________________________________________
Sex: |__| 1=male, 2=female, 3=third gender Age: |__||__||__| years
Moholla/Para/Street:_______ Village:_________________
Union:_________ Upazila: _________
District:__________________
Name of Suspected Kala-azar: |__| (1= PKA, 2= KATF, 3= Relapse KA, 4= PKDL)
Referred by: |__| (1=Kala-azar Search Volunteer, 2= HI/AHI/HA/FWA/FWI, 3=Private unqualified doctor, 4=Private qualified doctor, 5=Govt. doctor, 6=Others (specify…………………..)
Name & designation of the referee:_______________________ & __________
Signature _________________ Date: ……………………………..
Referred to :_______________________________Upazila Health Complex
Name of the Medical Officer: Dr._________________________________________
Mobile no.:_______________________________
(Note: one copy to be retained by referring person for further follow-up of the patient)
For any information/query, please contact with (central level): 1. Dr. A.F.M. Akter Hossain Deputy Programme Manager Kala-azar Elimination Programme DGHS, Mohakhali, Dhaka Mobile no.: 01672 667919
2. Dr. AKM Abdul Kayum Technical Consultant, Kala-azar Elimination Program, CDC, DGHS Mobile no.: 01797131317

Page | 31
Annex-B: Checklists, SOPs and Others
Checklist-1: Duties of Chairperson of OMT
Checklist-1: Duties of Chairperson of OMT to declare an outbreak and convene the OMT
to act as Chairperson of the OMT by leading and coordinating the response to the
outbreak
to endorse the outbreak management objectives and response strategy
if necessary, organize an outbreak control centre and appropriate support resources
where appropriate, arrange for medical examination of cases and contacts and the
taking of clinical specimens
to ensure communication strategies are developed and implemented
prepare and circulate a final report on the outbreak.
Checklist-2: for OMT task
Checklist for Outbreak Management Team (OMT) Tasks
The principal aim of the OMT is to investigate the cause of the outbreak and to implement action
to identify the source, minimise spread and prevent recurrence of the Kala-azar. The following
tasks must be undertaken to deal effectively with an outbreak.
Outbreak detection
Determine if there is a real outbreak
Collect relevant clinical (Blood PCR) or environmental specimens (Sand fly) for
laboratory analysis
Conduct unstructured, in-depth interview of index cases of VL
Identify population at risk
Initiate immediate control measure
Assess the availability of adequate resources to deal with the outbreak
Outbreak investigation

Page | 32
Establish a VL case definition (indigenous/or migrated)
Search for others VL cases
Collect and collate data from affected and unaffected persons using a standardised
questionnaire
Describe VL cases by time, place and person
Form primary hypothesis on the cause of the outbreak
Test and review hypothesis of the cause
Identify risk factors
Ascertain source and mode of spread
Outbreak response
Control the sources
Control the transmission by treating VL cases to reduce infection period
Control the transmission by larvicide; identify the cases; and vector control by ITN/IRS
Screening and monitoring of contact
Monitor control measure by continued surveillance of diseases
Declare the outbreak over
Communication
Ensure appropriate information is given to the public especially those at high risk
Ensure accuracy and timeliness of the activities taken
Include all those who need to know
Use the media constructively
Disseminate information on any lesson learnt from managing the outbreak
Evaluation of response
Evaluate the management of the outbreak and make recommendations for the future
SOP-1: for No Kala-azar Transmission Activity
SOP: No Kala-azar Transmission Activity (NKTA)
PURPOSE
To describe the procedure for “No Kala-azar Transmission Activity” as an early
response to a Kala-azar outbreak to interrupt the transmission of the disease from
recently treated case of VL/PKDL (index case) to the new population in the community.

Page | 33
POLICY/SCOPE
The SOP is applicable to new patients screening and vector control activities to be used
in as an early response to a Kala-azar outbreak. This approach is to be implemented in
the areas where Kala-azar outbreak will be detected and declared.
GENERAL RESPONSIBILITIES
The Focal Person of OMT at the central as well as the sub-district/upazila is responsible
for implementing the activity.
MATERIALS REQUIRED
Work diary
Diagnostic kits and its associated materials, Record keeping form
Insecticide for IRS and its associated materials, Record keeping form
Larveceide for treating suspected sand fly breeding places
PROCEDURES
1. At the beginning team for NKTA at central and upazila level has to be formed under
OMT.
2. Under the activity MO (DC), MOs, SSNs, MTs (Lab), HI, AHI, Team leader and Spray
man would be trained on NKTA. All the members of the team would be trained
under the activity. Team member’s responsibility will be shared.
3. MO (DC), MOs, SSNs, MTs (Lab), HI, AHI will act as epidemiological team and
Entomologist, Ento-technician, Team leader and Spray man will act as
entomological team.
4. When outbreak will be detected and declared, then the team will conduct NKTA at
the community where outbreak detected. Activity flowchart of the NKTA is given
below in the figure- A.
5. Before the activities the focal person has to be informed to recruit team leader and
Spray man and to assign other field support like SSNs, MT (Lab), AHI, HI and MOs.
6. During implementation of the activity, epidemiological team will do investigation
of the index case and active searching of NKA & PKDL cases. Around or
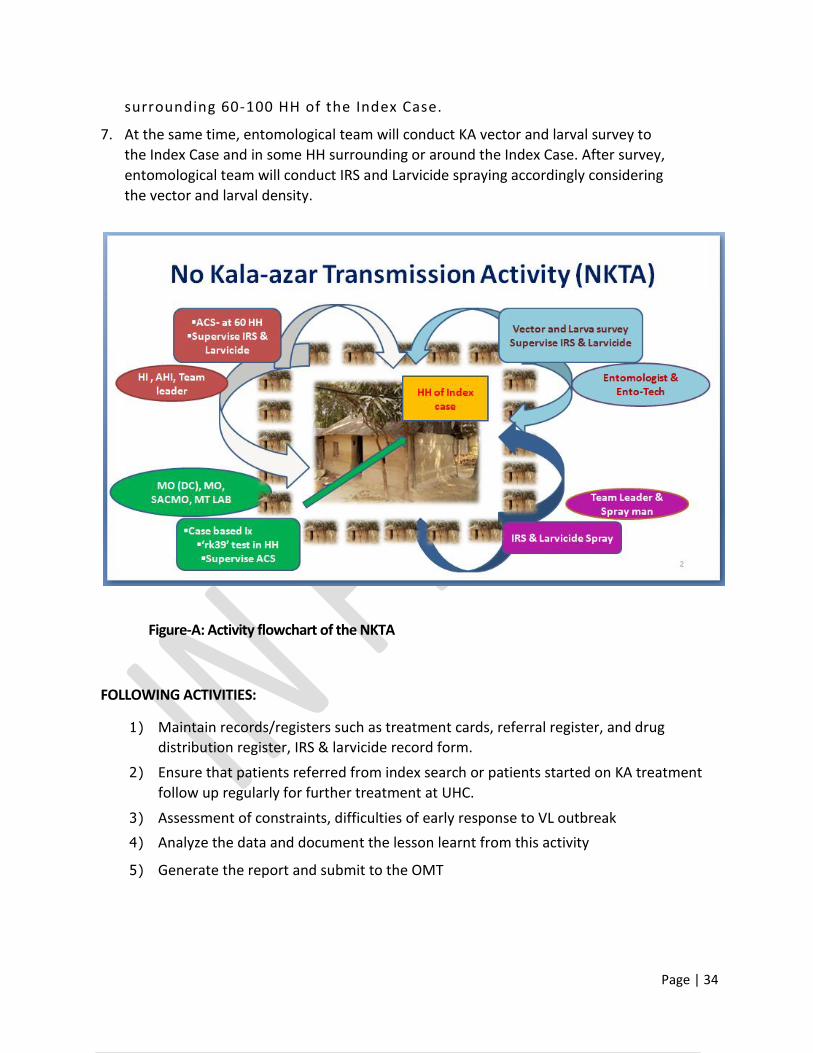
Page | 34
surrounding 60-100 HH of the Index Case.
7. At the same time, entomological team will conduct KA vector and larval survey to
the Index Case and in some HH surrounding or around the Index Case. After survey,
entomological team will conduct IRS and Larvicide spraying accordingly considering
the vector and larval density.
Figure-A: Activity flowchart of the NKTA
FOLLOWING ACTIVITIES:
1) Maintain records/registers such as treatment cards, referral register, and drug
distribution register, IRS & larvicide record form.
2) Ensure that patients referred from index search or patients started on KA treatment
follow up regularly for further treatment at UHC.
3) Assessment of constraints, difficulties of early response to VL outbreak
4) Analyze the data and document the lesson learnt from this activity
5) Generate the report and submit to the OMT

Page | 35
SOP-2: for organizing ACD-Camp at villages level
SOP: Camp Based Approach for Active Case Detection
PURPOSE
To describe the procedures for active case detection of new KA cases using camp approach.
POLICY/SCOPE
The SOP is applicable to screening procedures for NKA and PKDL to be used in the camp
approach. The camp approach is to be implemented in high & moderate KA endemic areas (to
be defined by KEP, Bangladesh). The camp approach ideally is to be implemented twice a year.
GENERAL RESPONSIBILITIES
The Program Manager of the KA elimination program at central level and UHFPO/ MO (DC) at
the sub district/upazila designee is responsible for implementing the camp detection
strategies.
MATERIALS REQUIRED
1. rK39 kits in a cool box for transport
2. Lancet & Lancet disposal box
3. Cotton
4. Spirit
5. Gloves
6. General medicines– anti-pyretic, antibiotics, anti-diarrheal, anti-malarial drugs etc.
7. Patient referral form
8. Lab investigation form
9. Patient register (Register book)
10. Photo album of PKDL
11. KA/PKDL patient registration form

Page | 36
12. IEC materials, banners, posters, pamphlets (local language), pictures of PKDL skin lesions
13. Mikes
14. BP apparatus
15. Thermometer
16. Stethoscope
17. Disposable syringes, IV infusion sets etc. (optional)
18. Transport boxes for drugs and supplies
19. Emergency drugs – cortisone, anti-histamines, IV fluids, adrenaline
20. Bio-waste disposal containers
21. Equipment for starting treatment (optional in areas where treatment will be started in the camp)
Preparatory activities (Central / district level)
1. List the upazila name with high and moderate KA incidence (New cases reported).
2. Conduct a meeting with Director, DC and LD, CDC, DGHS,
3. DD, AD, WHO personnel’s etc. at central/ headquarter level to prepare a micro action plan at least 15 days to 1 month before initiation of camps.
4. Prepare a time schedule for camps– decide number of camps, timings, duration of each camp, list name of villages where camps are to be held etc.
5. Prepare logistics plan– estimate requirement of drugs, rk39 test kits, lancets, gloves, fund requirements, IEC material etc. at upazila level and supply them accordingly.
6. Prepare supervision and monitoring plan for camps– identify supervision team, supervision schedule etc. (on a sample basis).
7. Finalize the micro plan and send a letter for start the implementation of the Camp approach.
8. Define reporting system from sub district/upazila to district/central level.
Pre-camp preparatory activities (sub district/upazila level)
1. List the union/ villages with high KA incidence (new cases reported).
2. Conduct a meeting with MO and staff of Union health centres and UHC to prepare a micro-action plan at least 15 days before initiation of camps.
3. Prepare a time schedule for camps– decide number of camps, timings, duration of each camp, list name of villages where camps are to be held etc.
4. Prepare logistics plan– estimate requirement of drugs, rk39 test kits, lancets, gloves,

Page | 37
fund requirements, IEC material etc. and send the indent letter to central level
5. Prepare supervision and monitoring plan for camps – identify supervision team, supervision schedule etc. (on a sample basis).
6. Identify the members of the Camp team (Medical Officer, Nurse, lab technician, Health inspector, AHI, etc.) which will conduct/ coordinate camp activities
7. Define duration of camp (usually one day camp)
8. Confirm venue for camp and determine its suitability for conducting camp.
9. Provide for refreshments for camp team on the day of camp
10. Vehicle requirement
11. Identify and coordinate with village level functionaries/ leaders
Pre-camp preparatory activities (village /union level)
1. One union level staff (nurse, lab technician, health inspectors or other) conducts coordination meeting at least 1 week before camp with Village Head/ Union Chairman and other formal and informal village leaders to inform and solicit community involvement in publicity and conduct of camp activities.
2. Identify venue for camp and determine its suitability for conducting camp. Identify, train and assign roles to village functionaries/ volunteers/ religious leaders/ school teachers for camp publicity activities.
3. Publicity activities to include milking, public announcement through mosques (in Bangladesh), distribution of pamphlets, putting up of banners/ posters (at least 4) in public places, mouth publicity of camps by health workers etc.
4. Publicity activities to be conducted at least one day prior to camp and on the day of camp.
5. List and procure locally camp furniture (tables, chairs, bench, examination table, bedside screens), drinking water provision etc.
6. Set up camp one day prior or early morning of the camp day (e.g. through local volunteers).
Camp day activities
1) Camp Team: one MO, one lab technician, one nurse/ field staff/ community
volunteers etc.
2) Organize flow of camp activities
3) Patient registration (name, address, age and sex)
4) Examination of patient for fever ≥ 2 weeks by MO, past history of kala azar, spleen
examination, general examination, examination for skin lesions.

Page | 38
5) rk39 test to be done by lab technician at camp if fever ≥ 2 weeks and splenomegaly
6) If rk39 test positive, Case Referral form to be filled and given to patient. Case referral
register to be completed. The patients are referred to UHC/district hospital/Referral
centre for treatment and follow up.
7) For suspected PKDL patients (PKDL-like skin lesions with rk39 test positive and past
history of kala azar treatment) will be referred to UHC/ appropriate level hospital for
confirmation of diagnosis and treatment start.
8) If rk39 test negative or for all other patients, MO advises appropriate
treatment/refers for further diagnostic tests. Particular emphasis may be given to
suspected leprosy patients
9) All patients with severe kala-azar and or other co-infections to be referred to
appropriate level hospital.
10) Proper disposal of bio-waste at the end of the camp.
Post camp activities at UHC/Union level
1. Maintain camp records– camp registers, treatment cards, referral register, drug
distribution register.
2. Manage patient specific drug box for kala-azar patients.
3. Ensure that patients referred from camp or patients started on KA treatment follow
up regularly for further treatment at UHC.
4. Assessment of camps- # of attendees, # of chronic fever cases, # of rk39 tests done,
# of rk39 test positives, # of patients started treatment for Kala azar/PKDL, # of
patients referred for KA/PKDL treatment and follow up, drug distribution.
5. Assessment of constraints, difficulties of conducting camp
6. Submit camp activity reports to district /central level on a monthly basis (web-based
reporting in Bangladesh)
7. Ensure timely payment of incentives to community volunteers or health workers for
patient follow up (if required)
Post camp activities at village level
1. Inform community volunteers/health workers of patients diagnosed and started with
KA/PKDL treatment to ensure treatment compliance or for any side effects.
Page | 39
Terms of Reference: Outbreak Management Team (OMT)
Terms of Reference: Outbreak Management Team (OMT)
A central outbreak log (refer to Form 2 Outbreak Log for an example) should be kept of all activities associated with the outbreak investigation, including minutes of meetings, delegated tasks and actions taken by team members, laboratory results and other relevant information. Terms of reference for the OMT may include the following:
1. Review the evidence and confirm or refute existence of an outbreak; decide whether further investigation is required to confirm the outbreak; immediate steps must be taken by the focal point of central level OMT in consultation with chair of the OMT.
2. Medical officer in the Upazila level team will take initiative to collect further clinical, epidemiological and laboratory information as directed by the central level OMT.
3. A case definition in this guideline will be used to verify known cases and to search for further possible cases by the Upazila level team
4. Declared the outbreak by the chair of OMT. 5. Use the proposed strategy in this guideline to investigate and control the outbreak 6. Allocate tasks to outbreak team members at different level. Engage the required
collaborative parters’ at different level. 7. Investigate the outbreak and identify the intensity, nature, and risk factor jointly by the
central and upazila level team. If required, scientific study needs to be design by the central level team to generate the evidence for policy implication.
8. Implement control measures and monitor their effectiveness in dealing with the cause of the outbreak including preventing further spread by central level team.
9. Conduct formal outbreak control meetings on a regular basis by the central level team 10. Document minutes of each OMT meeting including allocated tasks and any actions
taken or completed by the central level. 11. Ensure adequate staff and resources are available for the management of the outbreak 12. Consider potential staff training opportunities of the outbreak by the central level team. 13. Keep relevant outside agencies, the general public and media appropriately informed by
the central level team. 14. Evaluate the response to the outbreak and implement changes in outbreak
management procedures based upon lessons learnt.

Page | 40
Reporting format: Kala-azar Outbreak
Sample Reporting Format: Kala-azar Outbreak
Type of Outbreak: Kala-azar
Date Outbreak was reported to OTM, CDC, DGHS: __/__/__
Reported to (Name, designation and address):
Reported by (Name, designation and address):
Outbreak Location: …………………………… Area affected: ………………………………
Formulation of the OMT in the corresponding areas (briefly describe about the meeting and
communication to formulate the OMT for further investigation and response to this outbreak. Also
attached the list of OMT members):
……………………………………………………………………………………………………………………………………………………………
……………………………………………………………………………………………………………………………………………………………
Describe brief methods of the outbreak detection and its outcome:
……………………………………………………………………………………………………………………………………………………………
……………………………………………………………………………………………………………………………………………………………
Final outcome of outbreak detection? ………………………………………………. (Outbreak detected/ Outbreak not
detected)
Date of outbreak declaration: ………………………………………….. (if outbreak detected)
If outbreak declared,
1. List further effort in response to the outbreak (attached required documents):
……………………………………………………………………………………………………………………………………………………………
……………………………………………………………………………………………………………………………………………………………
2. Outbreak Investigation and its associated outcome (attached required documents):
……………………………………………………………………………………………………………………………………………………………
……………………………………………………………………………………………………………………………………………………………

Page | 41
3. Long term specific prevention and control measure taken (attached required documents):
……………………………………………………………………………………………………………………………………………………………
……………………………………………………………………………………………………………………………………………………………
4. Message from the evaluation report (if any):
……………………………………………………………………………………………………………………………………………………………
……………………………………………………………………………………………………………………………………………………………
Conclusion and Recommendation:
……………………………………………………………………………………………………………………………………………………………
……………………………………………………………………………………………………………………………………………………………
Report prepared by:_________________________ Designation:___________________________
Signature:__________________________________ Date (dd-mm-yyyy):______________________
Verified by:_________________________ Designation:___________________________
Signature:__________________________________ Date (dd-mm-yyyy):______________________

Page | 42
List of past Kala-azar endemic areas in Bangladesh
List of past Kala-azar endemic areas in Bangladesh
Divisions Districts Nmae of Upazilas
Barishal Bhola Lalmohon
Patuakhali Dashmina Golachipa
Dhaka Chandpur Kachua
Dhaka Dhamrai Savar
Faridpur Faridpur sadar Nagarkanda
Gazipur Gazipur sadar Kaliakoir
Sreepur
Gopalganj Gopalganj sadar Tungipara
Kishoregonj Hosanpur Pakundia
Manikganj Daulatpur Ghior
Manikgang sadar Saturia
Shibalaya Singair
Narsingdi Narsingdi sadar Raipura
Shibpur
Rajbari Pangsha Rajbari sadar
Shariatpur Vedorganj
Tangail Basail Bhuapur
Delduar Dhanbari
Ghatail Gopalpur
Kalihati Mirzapur
Modhupur Nagorpur
Shakhipur Tangail sadar
Khulna Jhenaidah Kaligonj Mohespur
Kotchandpur
Khulna Terokhada
Kustia Daulatpur Kamarkhali
Magura Magura Sadar
Mymensingh Jamalpur Jamalpur sadar Melandah
Madarganj Shorishabari
Mymensingh Bhaluka Ishwarganj
Dhobaura Muktagachcha
Fulbaria Mymensingh sadar
Fulpur Nandail
Gafargaon Trishal
Haluaghat
Rajshahi Bogra Adamdighi Nandigram
Bogra sadar Sherpur
Dhunat Shonatala

Page | 43
Dupchachia
Chapai Nawabganj Bholahat Nachol
Chapai Nawabganj Sadar Shibgonj
Gomostapur
Joypurhat Akkelpur Khetlal
Kalai Panchbibi
Naogaon Badalagachi Neyamatpur
Dhamoirhat Patnitala
Mahadebpur Porsha
Manda Sapahar
Naogaon Sadar
Natore Bagatipara Lalpur
Baraigram Natore Sadar
Gurudaspur Singra
Pabna Atgharia Ishwardi
Bera Pabna sadar Bhangura Sathia
Chatmohor Shujanagar
Faridpur
Rajshahi Bagha Godagari
Baghmara Motihar
Charghat Puthia
Durgapur Tanore
Sirajganj Belkuchi Shahajadpur
Chouhali Sirajganj Sadar
Kajipur Tarash
Kamarkhand Ullapara
Raiganj
Rangpur Dinajpur Birampur Fulbari
Birganj Ghoraghat
Chirirbandar Nababganj
Dinajpur Sadar Parbotipur
Gaibandha Gobindaganj Sadullapur
Polashbari Shaghata
Panchagar Atowari Debiganj
Boda
Rangpur Pirganj Rangpur Sadar
Thakurgaon Baliadangi Ranisankail
Haripur Thakurgaon sadar
Pirganj