Embed Size (px)
Citation preview
Prepared by:-
KAMARUL AMIN BIN ABDULLAH @ ABU BAKAR
At the end of lesson, the student should able to:-
1. List type of mobile x-ray units.
2. Briefly explain type of generators in mobile x-ray units.
3. List the advantages and limitation of the generators.
4. Briefly explain the principle operation of mobile x-ray units.
5. List the advantages and limitation of mobile x-ray units.
6. Briefly explain the special consideration for mobile x-ray units.
7. Briefly explain the safe handling for mobile x-ray units.
3/5/2014 2Kamarul Amin (c)
What is mobile x-ray units?
Mobile radiographic units consist of awheeled cart that transports :-
1. x-ray generator
2. x-ray tube
3. tubestand
4. collimators
5. film-cassette or flat-panel detector
3/5/2014 3Kamarul Amin (c)
It is equipment which can be moved from one place to another and used at the patient’s bedside or in operation theatre.
There are TWO (2) types of mobile x-ray units:-
1. Mobile Radiography Unit
2. Mobile C-arm (II) Unit
3/5/2014 Kamarul Amin (c) 4
x-rays are produced by the
x-ray tube
collimators confines the
primary beam
capture images using a
film/screen or flat panel detector
3/5/2014 Kamarul Amin (c) 5
Where are they commonly used?
1. Patient’s rooms or wards
2. Emergency Department, Resuscitation Unit
3. ICU, CCU, HDU/W
4. Surgery and Recovery Rooms (OT)
5. Nursery and Neonatal units
3/5/2014 6Kamarul Amin (c)

MOBILE X-RAY (RADIOGRAPHY)
MOBILE C-ARM (II)
3/5/2014 7Kamarul Amin (c)
Used at patient bedsides.
Requires Radiographer’s skills and expertise.
Procedures should be performed using as standard a method as possible.
Manual technique is generally used.
Ordinary factors such as distance, grids, and technique can become a challenge.
3/5/2014 9Kamarul Amin (c)
Battery powered uses two sets of lead-acid, or nickel-cadmium batteries.
One set powers driving of the machine. One set provides power to the x-ray tube.
recharging is necessary after a number of exposures.
Capacitor discharge does not operate on batteries. It can produce x-ray from
energy stored in, then discharged from a capacitor. carries two metal plates that hold electrical charge.
High Frequency converts hf AC to DC - resulting in high voltage ripple
60Hz-500 Hz techniques are equivalent to 3Ø 12 p
3/5/2014 10Kamarul Amin (c)

3/5/2014 Kamarul Amin (c) 11
3/5/2014 Kamarul Amin (c) 12
12 VOLT BATTERIES
CAR BATTERY
Silver or Nickel Cadmium

3/5/2014 Kamarul Amin (c) 13

3/5/2014 Kamarul Amin (c) 14

3/5/2014 Kamarul Amin (c) 15
DIGITAL UNITS
3/5/2014 Kamarul Amin (c) 16

3/5/2014 Kamarul Amin (c) 17
Advantages:1. This machine can be used freely, provides wide
range of satisfactory kVp & mAs.2. This machine could be recharging less frequently
that the capacitor one.3. Some machine allows you to take up to 500
exposures without re-charging.
Disadvantages:1. It needs special care and maintenance.2. This machine is heavy and hard to control.
3/5/2014 18Kamarul Amin (c)
Advantages1. Lightweight, smaller and easier to maneuver.2. Require much less time to charge than battery
units.3. The production and quality is consistence.4. No battery usage.
Disadvantages1. Can’t handle thick body parts due to voltage drop
during exposure.2. Must be charged prior to each use.
3/5/2014 19Kamarul Amin (c)
3/5/2014 Kamarul Amin (c) 20
Battery Powered
Uses 9 - 10 12V batteries -(heavy)
Battery supplies power for all inst. operations
Motor Driven
Wt - +1,000 lbs
? Constant potential
Some have AEC
Needs recharging - holds 8 hr charge
3Ø 12pulse techniques
Can double expose +
Capacitor DC
Uses 110 outlet
Capacitors stores up charge - then exposure discharges
“Muscle Driven”
Wt - + 450 lbs
? Constant potential
Some have programmed memory
Must be plugged in to store up charge
? Not for large parts
Very Expensive - not many in use
Smaller - more compact units
High voltage transformer 1/10 the size
Minimal voltage ripple = higher efficiency
3/5/2014 Kamarul Amin (c) 21
3/5/2014 Kamarul Amin (c) 22

3/5/2014 Kamarul Amin (c) 23
MinXray high frequency
portable medical x-ray units
These models are designed
for use in nursing homes,
private homes, correctional
facilities, field clinics,
hospitals, or anywhere an x-
ray machine must be
brought to a patient.
maximum of 80 mAs
70 lbs
24
Portables can be the “ultimate test” of skill, competency and resourcefulness
Compounded with the urgency and tension of the Emergency Room , Intensive Care Unit and/or Operating Room
Patient’s inability to cooperate for positioning
Technical Considerations - varying SID, grid alignment, patient positioning
25
More acutely ill and/or unable to transport
Cardiac Monitoring Lines, tubes, ventilators and traction Pt may be conscious or unconscious
cooperative or uncooperative Show courtesy to the patient - even the
one who may not appear to be able to hear or understand* *remember Phil Ballingers’ Story
26
Before entering, park machine outside of room and go in and talk to the patient (establish rapport, check for correct patient)
Rearrange equipment/furniture if necessary - remember to put it back when done!
Radiographer’s responsibility to return all items to their original locations
Locks on bars, bed rails, etc
27
Get patient’s permission to do the exam Explain the procedure Move items that will be in the way
Overhanging TV’s and the X-ray tube can be hazardous to your head!
Don’t bump the bed or your head Place cassette in a pillowcase when possible Unconscious patients Surgery/Emergency Room/ICU
28
Watch out for:
Equipment power supplies
Oxygen tubing
Intravenous lines
Catheters, etc.
EKG wires
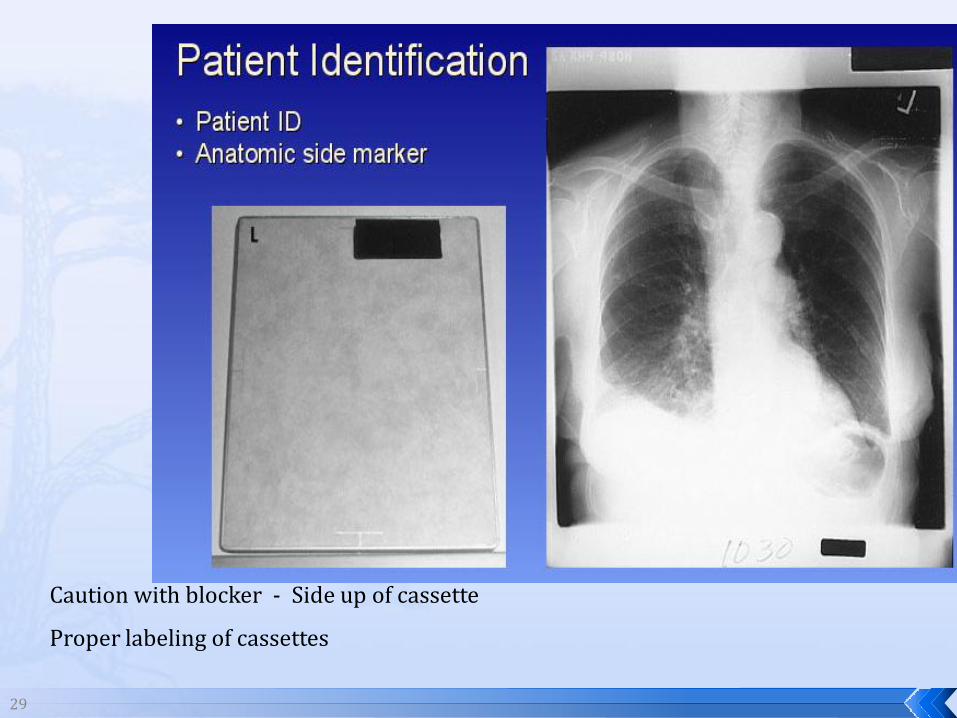
29
Caution with blocker - Side up of cassette
Proper labeling of cassettes
30
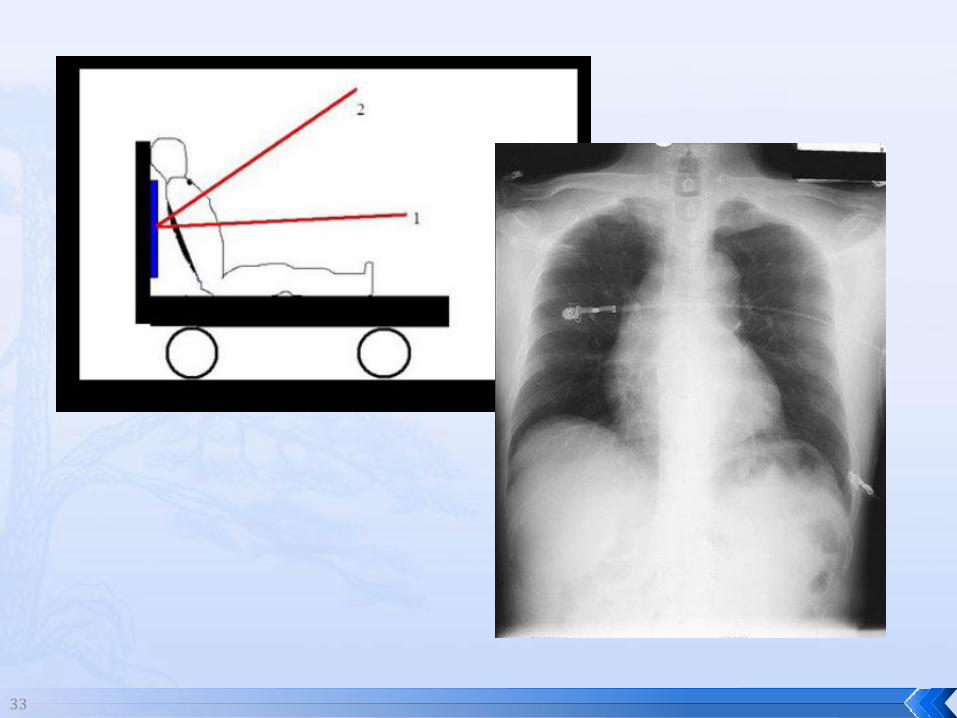
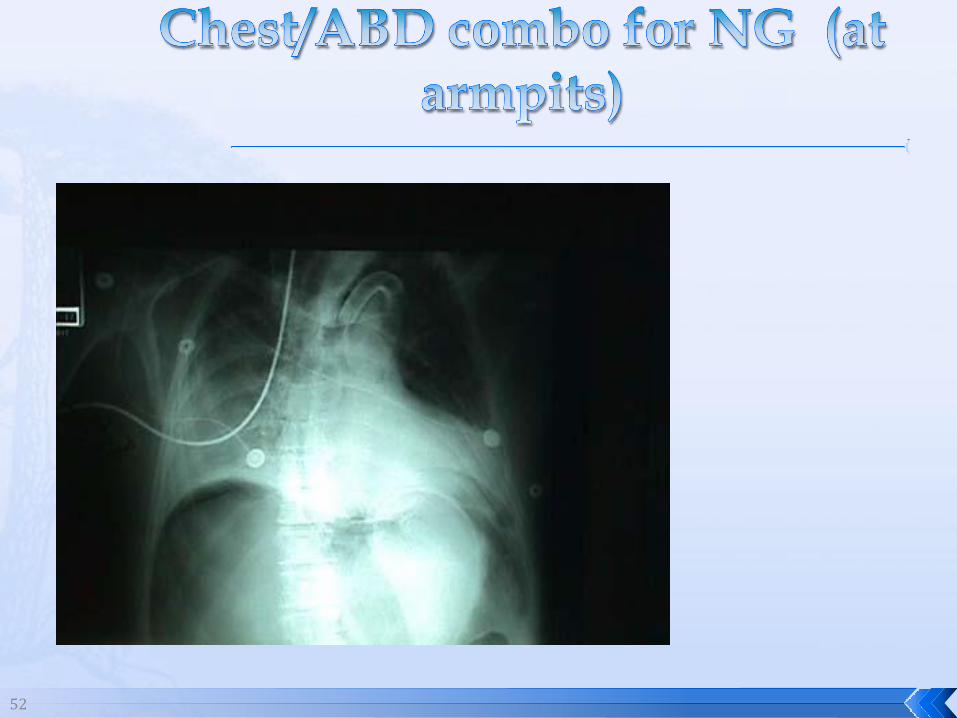
CHEST – PLACE C/R ± TO STERNUM –
or ANGLE 5° CAUDAL FROM ± TO CASSETTE
C/R TOO CEPHALIC = APICAL LORDOTIC
C/R TOO CAUDAL = CLAVICLES IN MIDDLE OF THE CHEST
CONSIDER YOUR PATIENT’S BODY HABIUTS
31
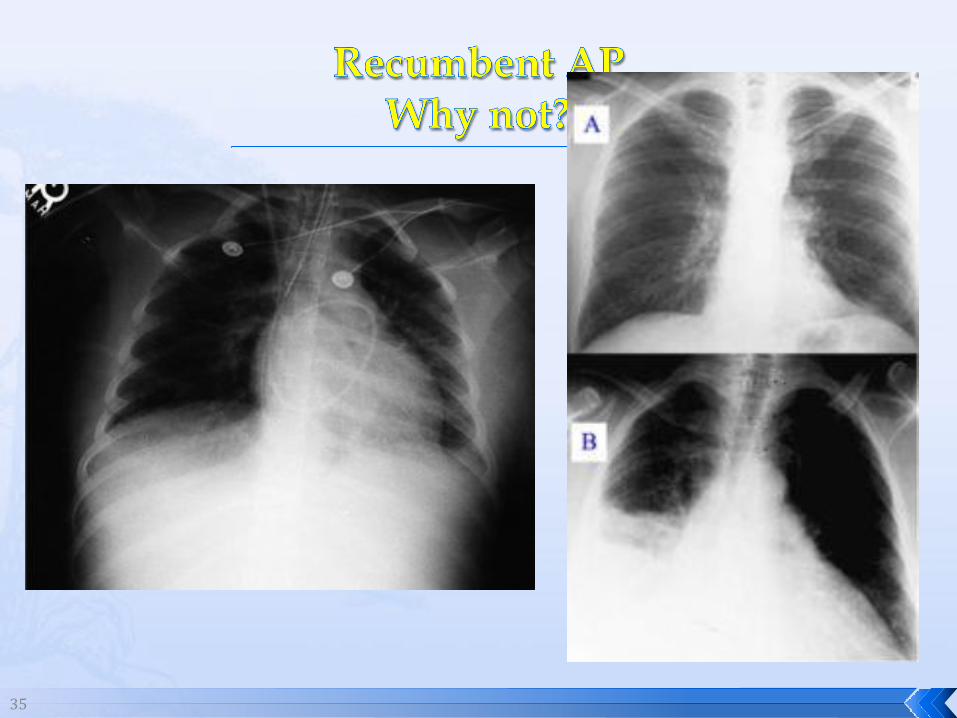
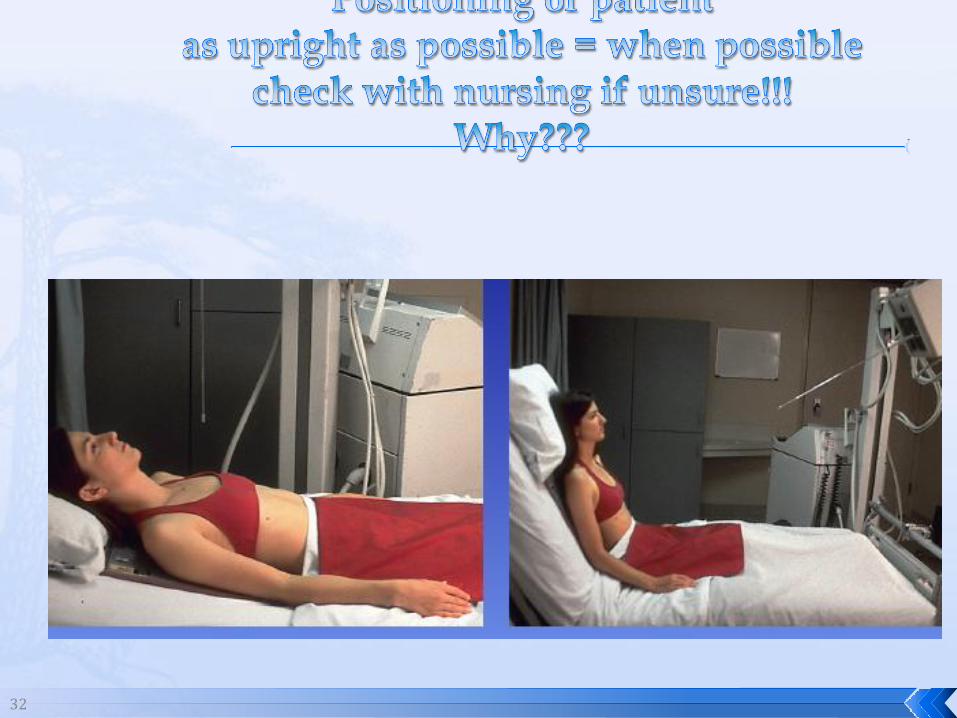
Maintain typical positioning for examinations
Perform chest radiography in semi-erect position whenever possible
Check with the nurse forCritically ill patients
32
33
34
36
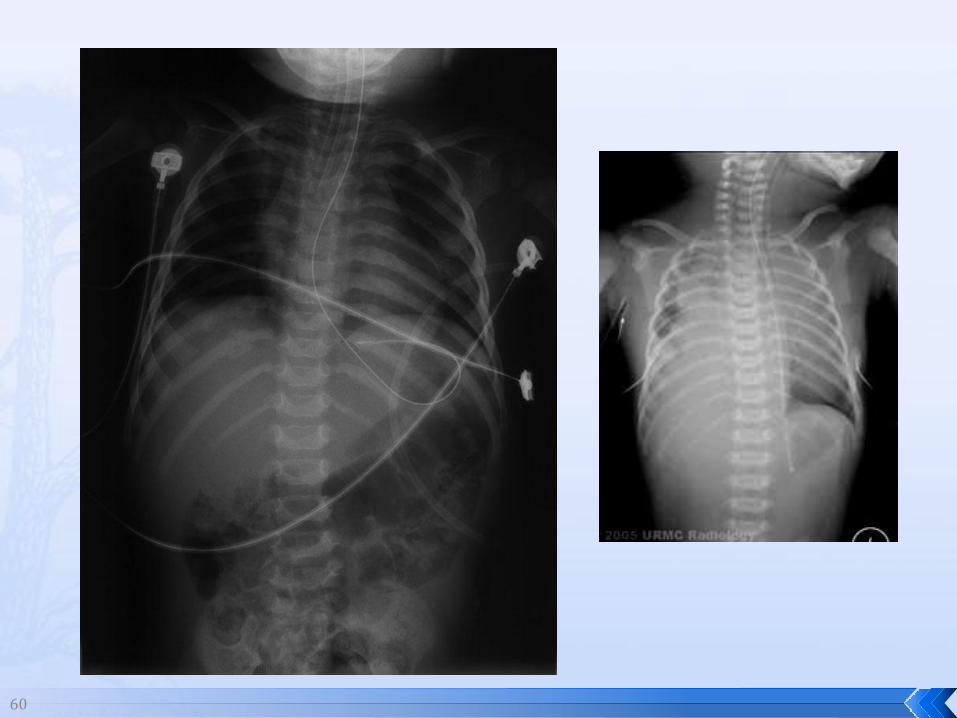
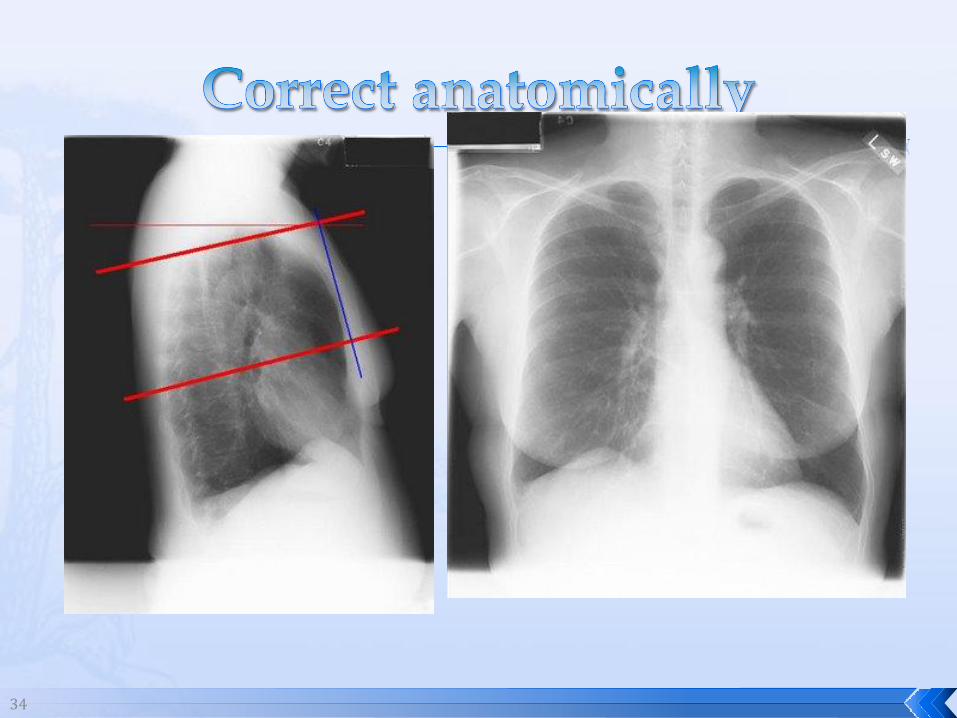
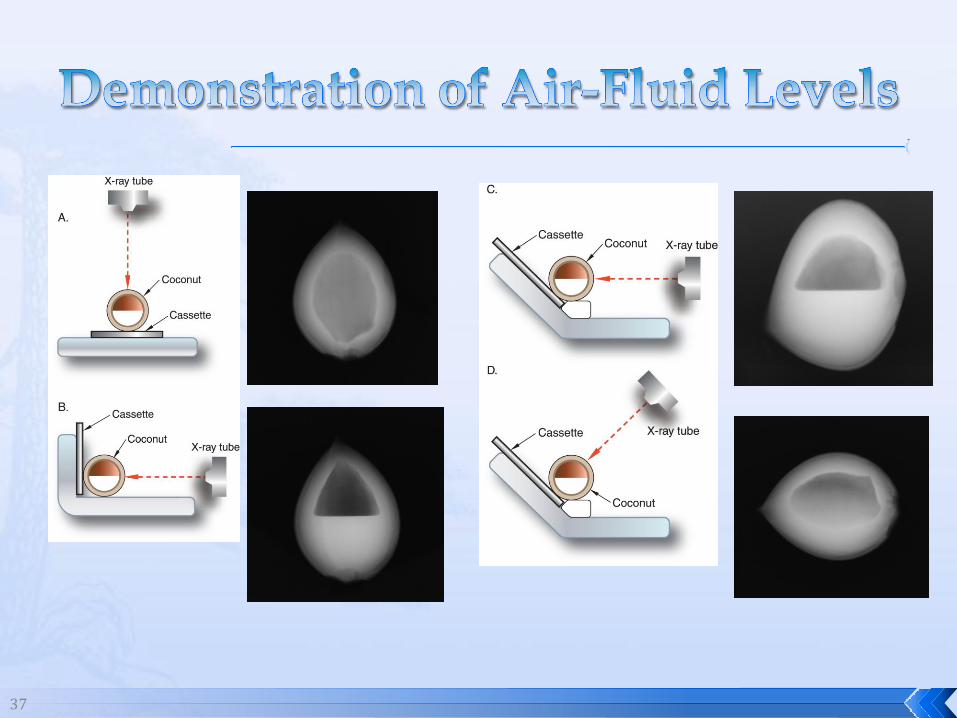
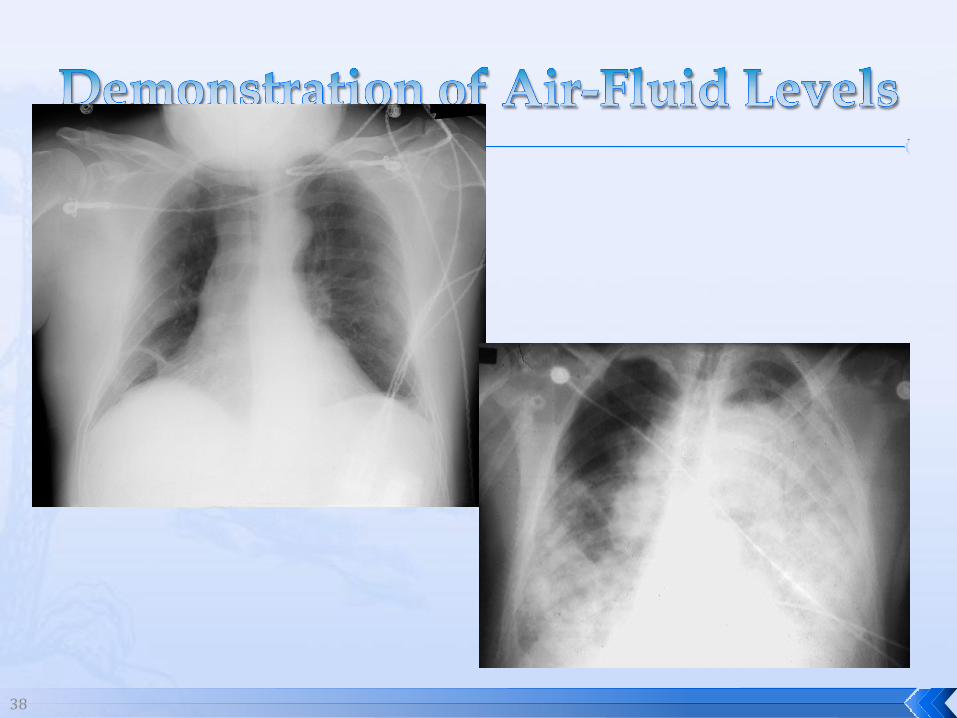
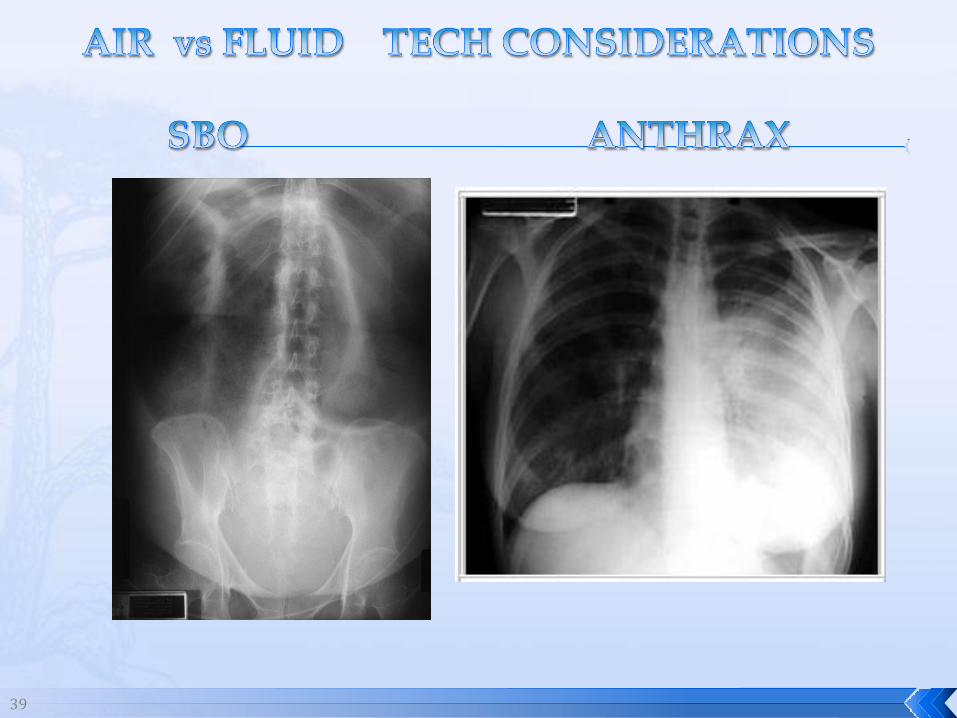
When checking for air-fluid levels : 2 exposures may be necessary
1 - horizontal beam to see level
1 - C/R ± to sternum “anatomically correct”
CHECK FOR ARTIFACTS
Grid alignment - low ratio grids used
(see coconut for fluid levels pg 525 Carltons)
37
38
39
40
Kilovoltage
Milliampere-seconds
Distance
Grids
Film/screen combinations
Other factors
41
SAME RULES APPLY AS IN RAD ROOM
AP CHEST – SCREEN OR GRID *
(REMEMBER: 4x LESS FOR SCREENS*)
BODY PARTS OVER 12 CM = GRID
SID – VERY IMPORTANT TO MEASURE
CHEST USUALLY DONE AT 62 – 72”
ALL OTHER DONE AT 40” * SEE MERRILLS BEGINNING AT PG 212
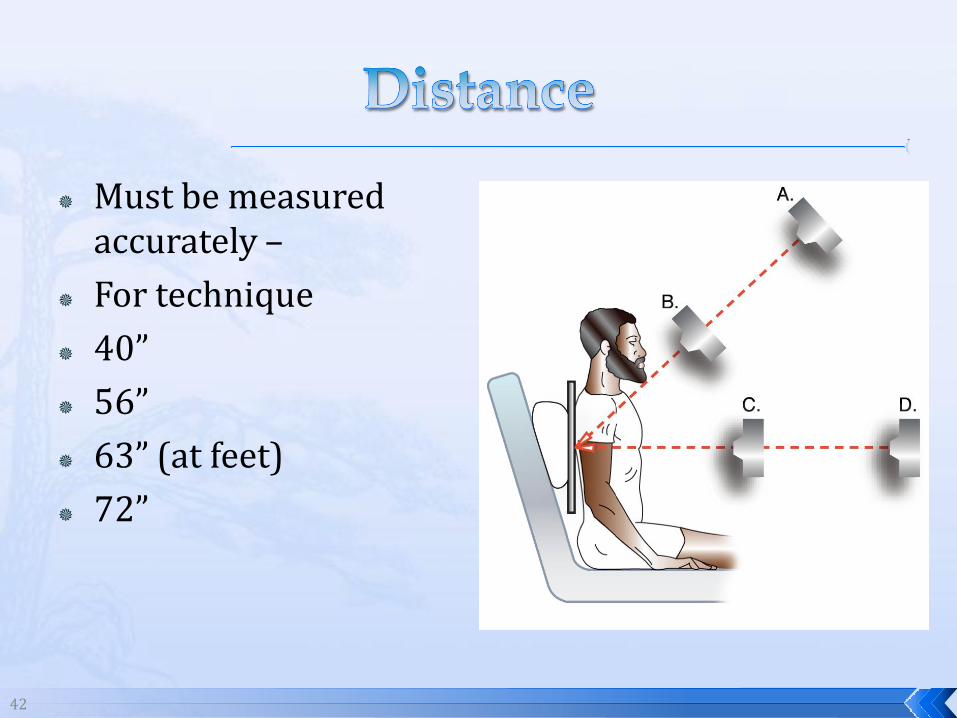
42
Must be measured accurately –
For technique
40”
56”
63” (at feet)
72”
43
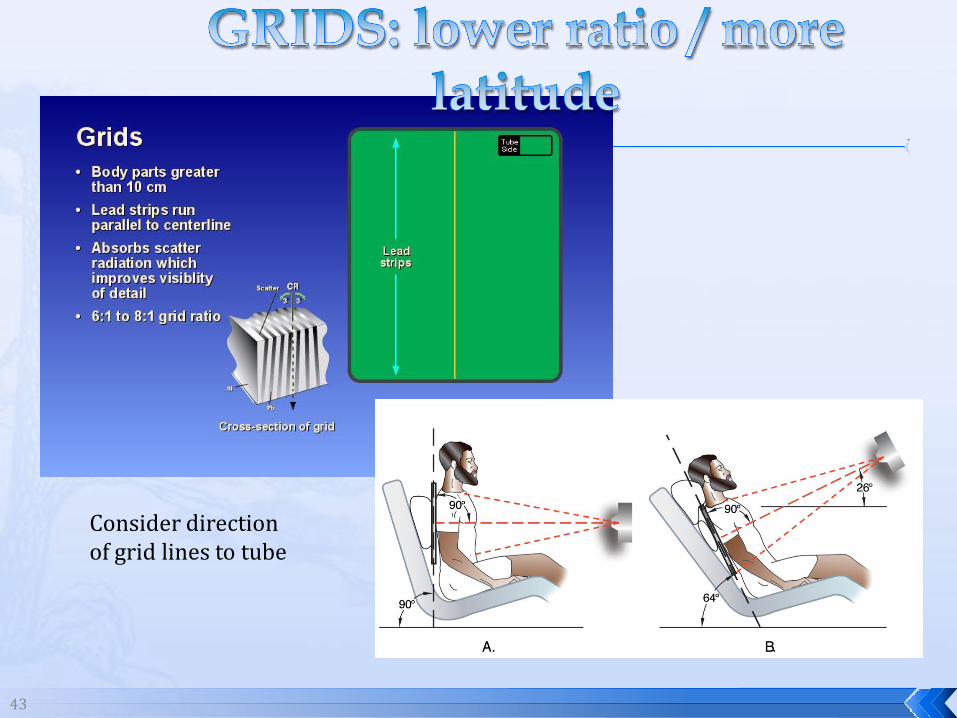
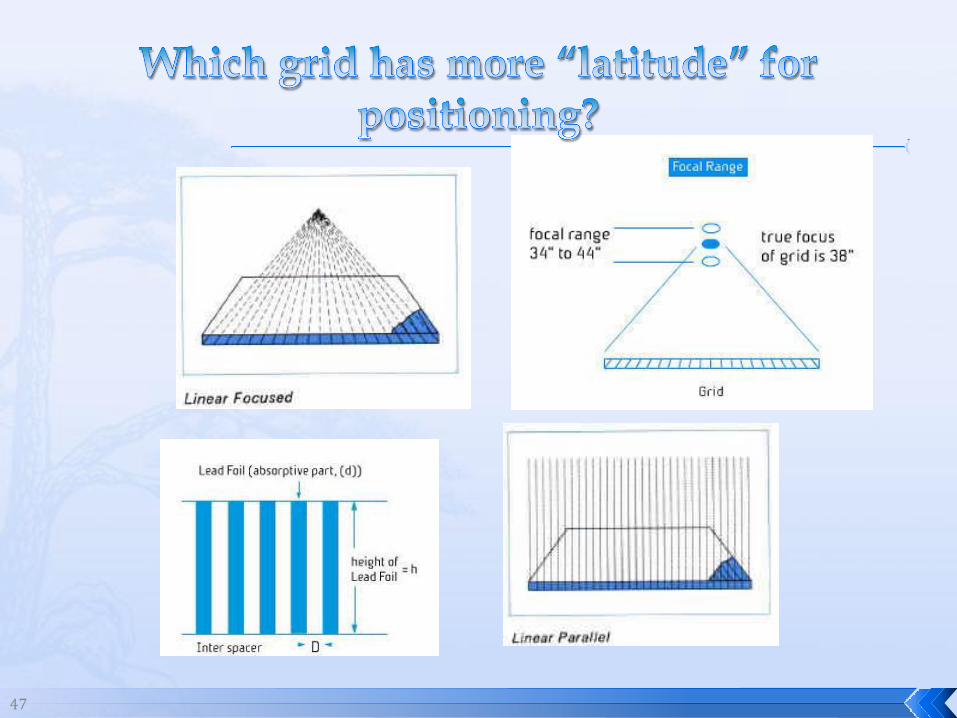
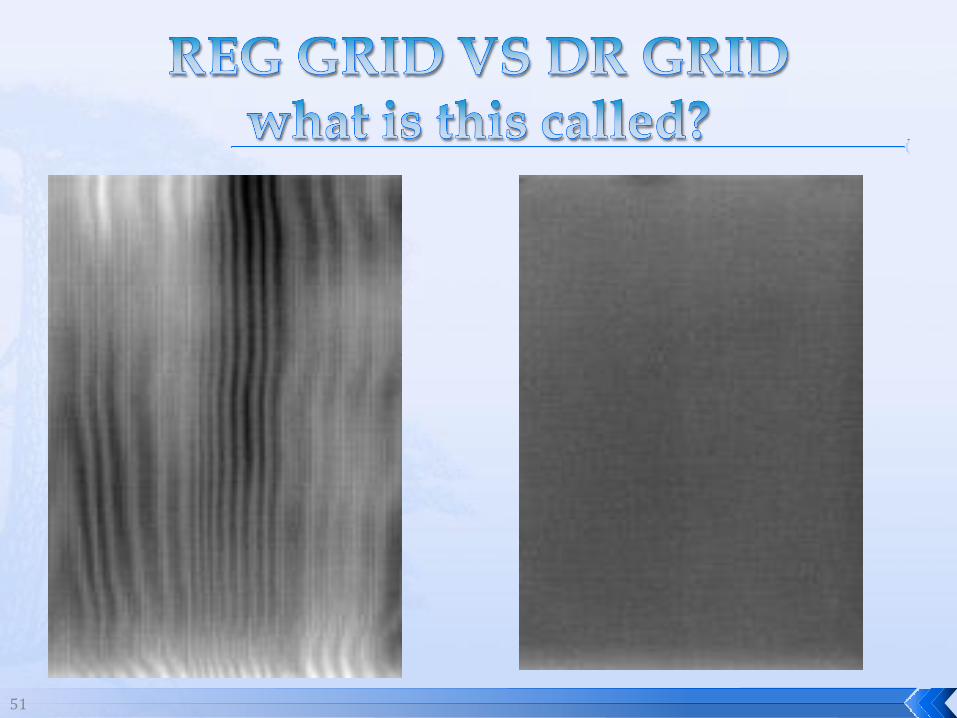
Consider direction of grid lines to tube
44
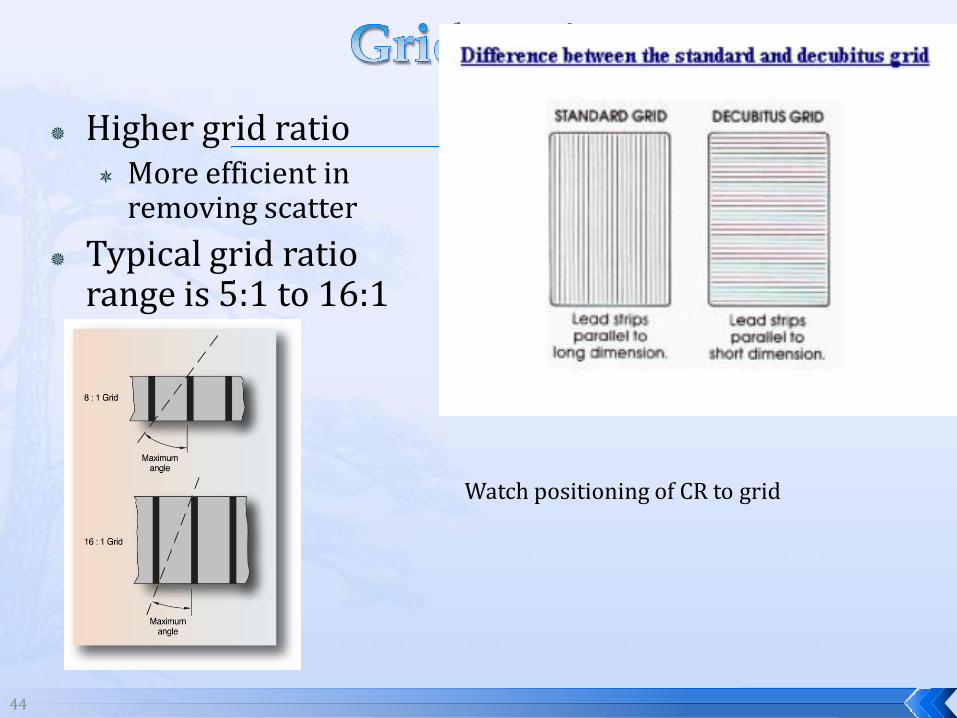
Higher grid ratio More efficient in
removing scatter
Typical grid ratio range is 5:1 to 16:1
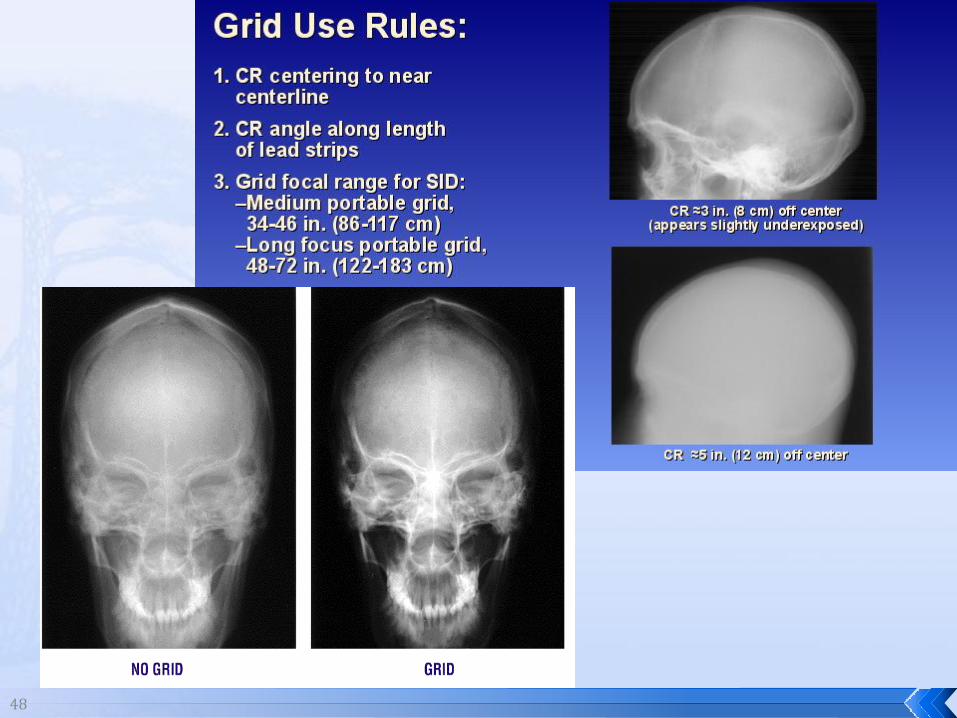
Watch positioning of CR to grid
45
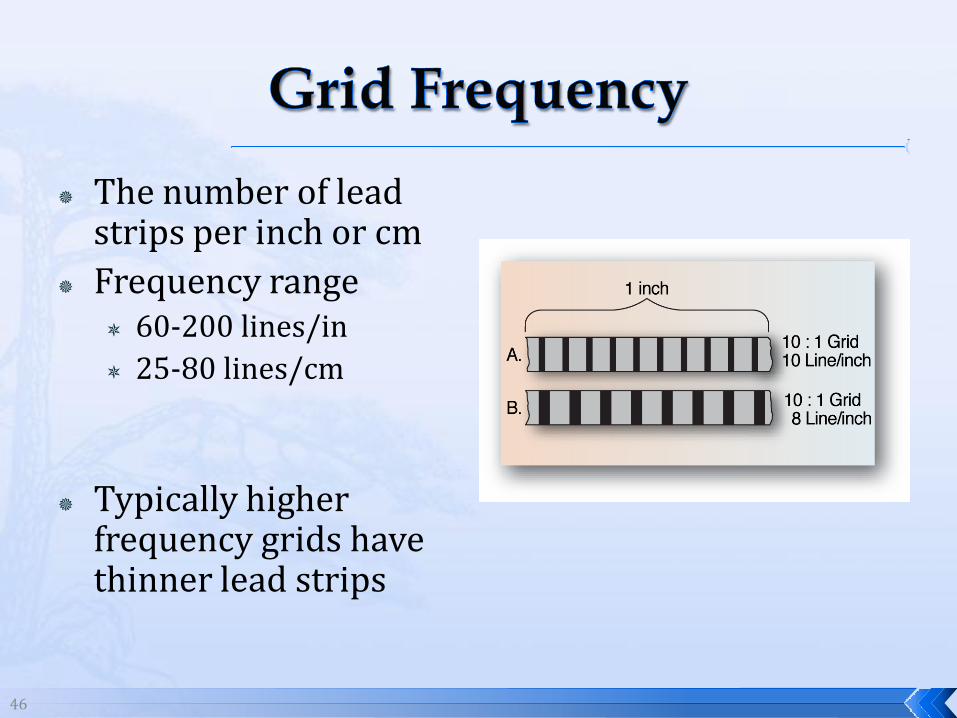
46
The number of lead strips per inch or cm
Frequency range 60-200 lines/in
25-80 lines/cm
Typically higher frequency grids have thinner lead strips
47
48
49
50
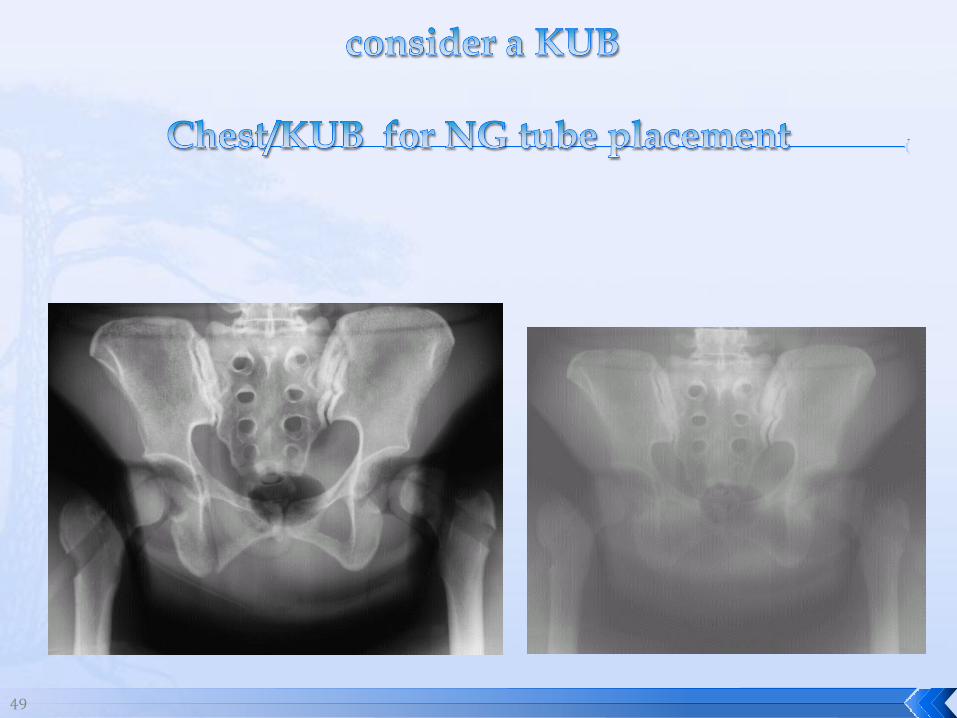
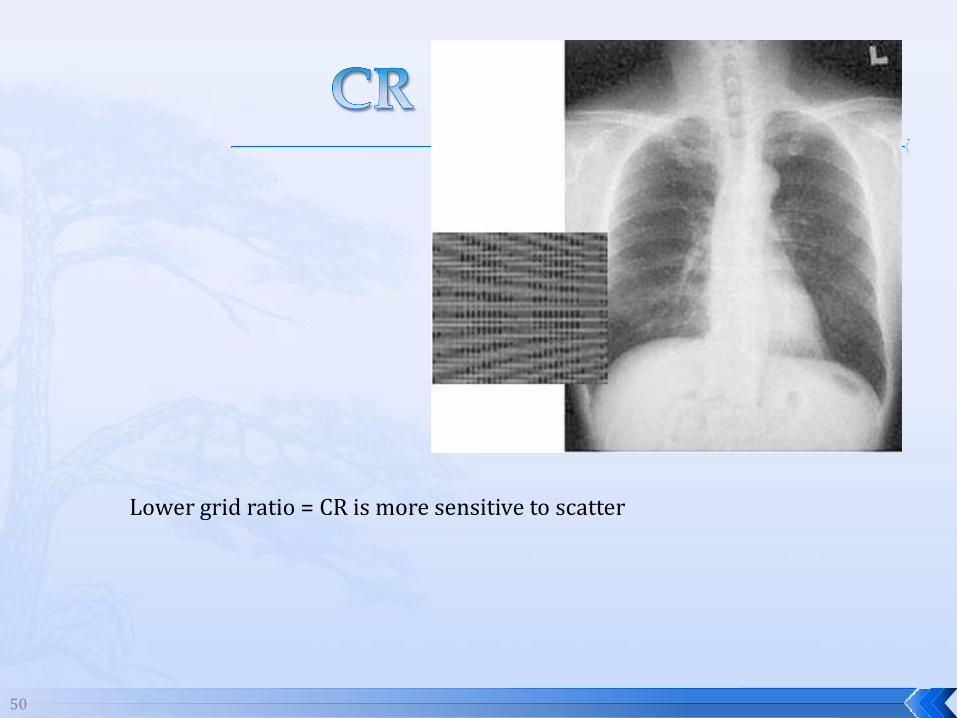
Lower grid ratio = CR is more sensitive to scatter
51
52
53
54
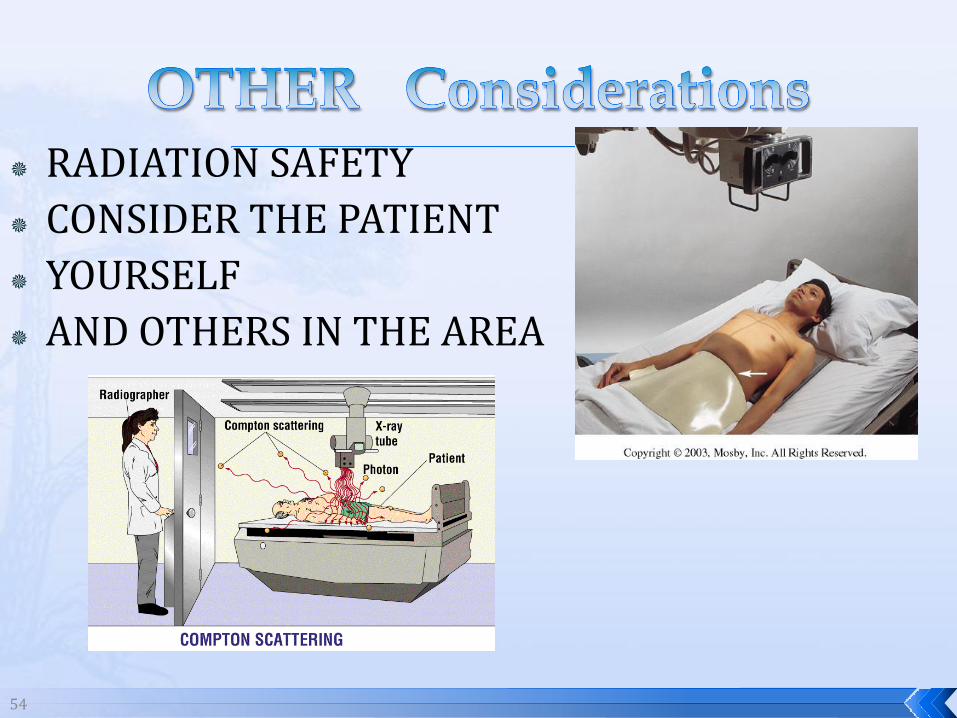
RADIATION SAFETY
CONSIDER THE PATIENT
YOURSELF
AND OTHERS IN THE AREA
55
It’s your duty to protect the patient, yourself and others (healthcare professional, family members)
Politely ask whoever can, to leave the area
Provide aprons to those who cannot leave -always carry 2 aprons with you on the machine (for you and the patient)
Announce your intent to make an exposure and give time for others to leave (but they shouldn’t “run” away)
56
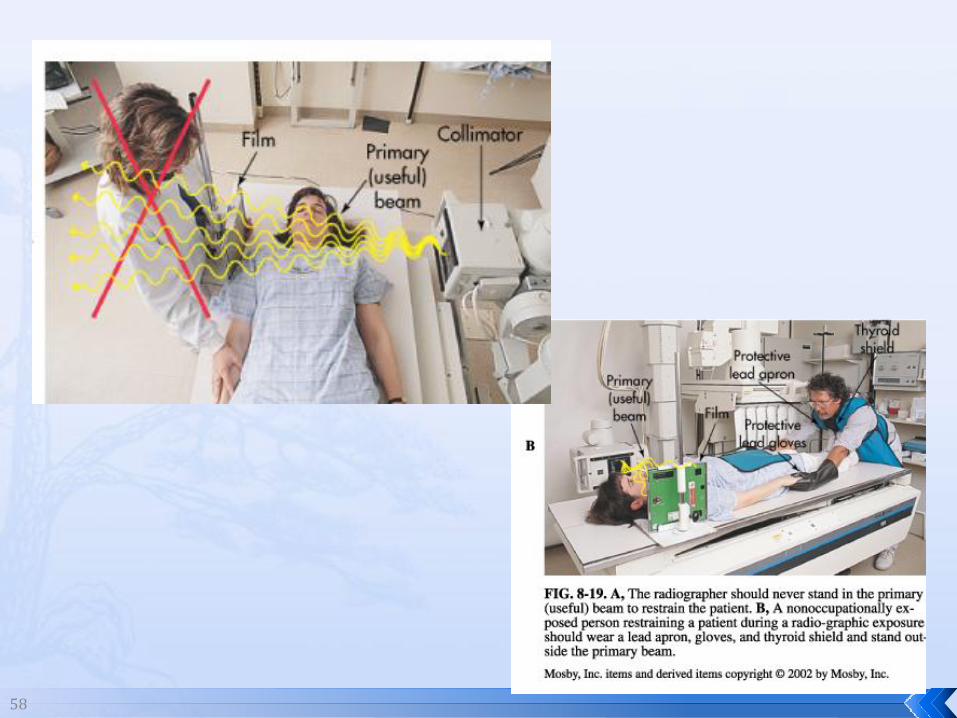
Never place your hand or other body part in primary beam
Provide gonadal protection for the patient
Achieve maximum distance from the patient and tube (stand 90° from the patient- SEE Merrills – pg 212)
Minimum 6 foot exposure cord for radiography
Label and handle cassettes carefully
57
58
59
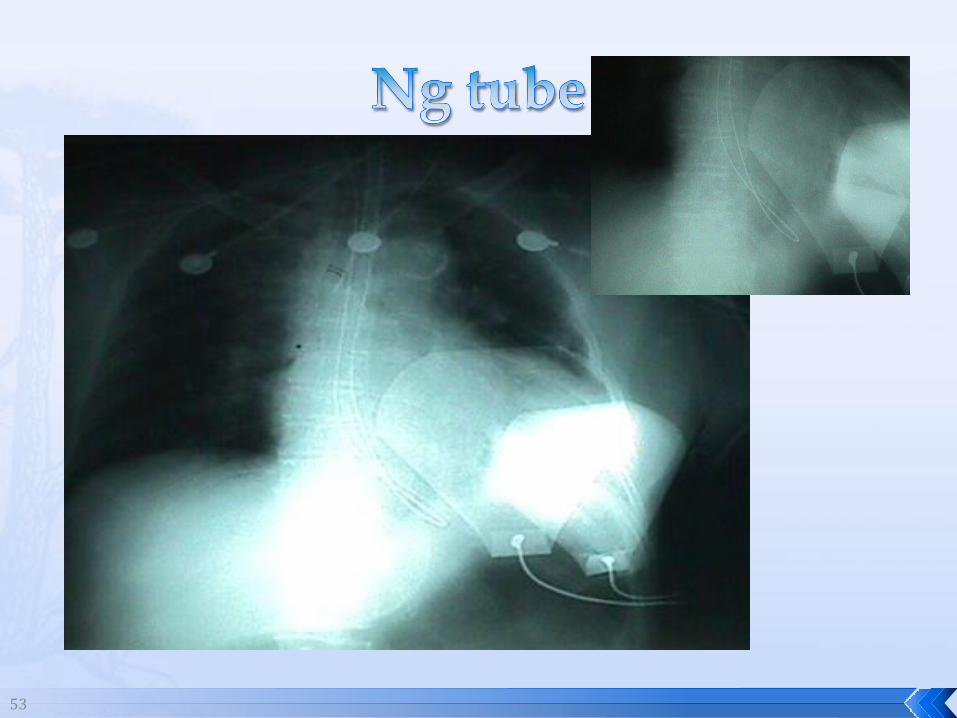
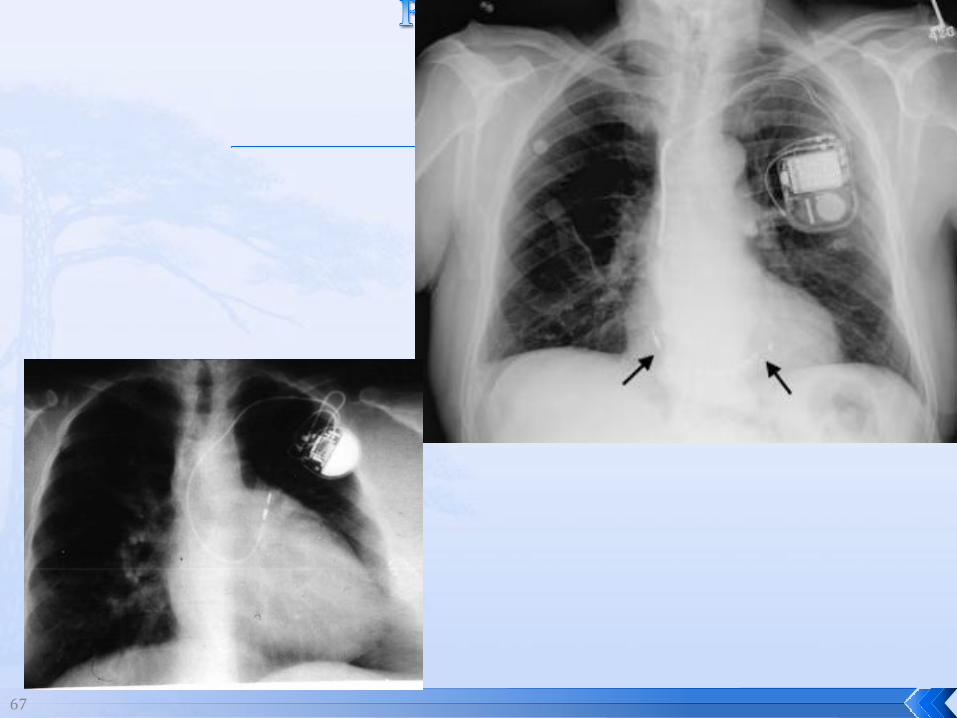
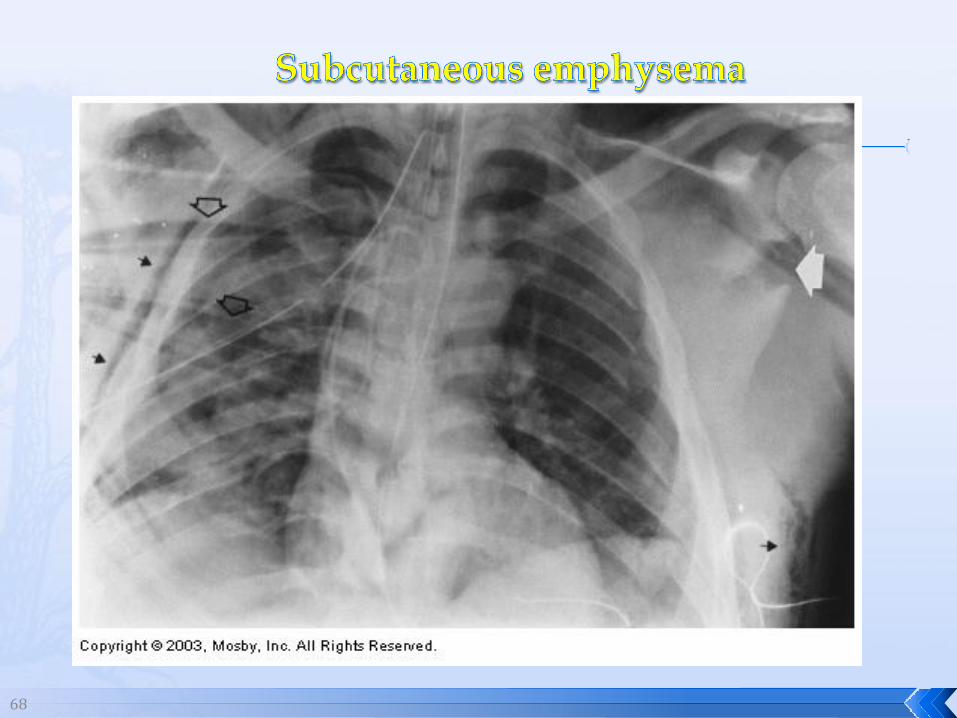
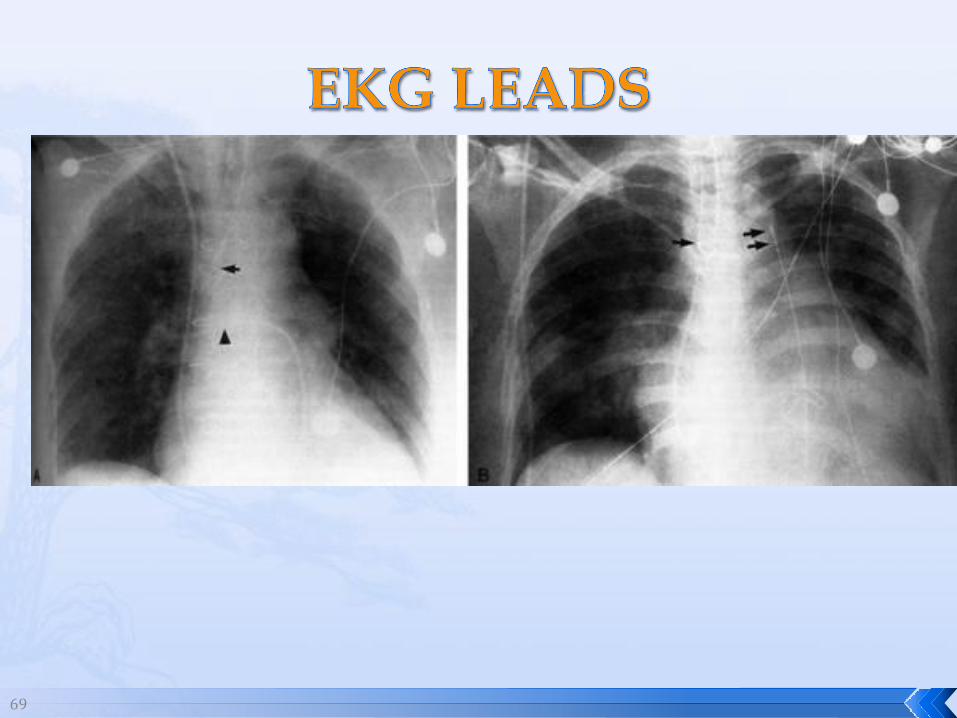
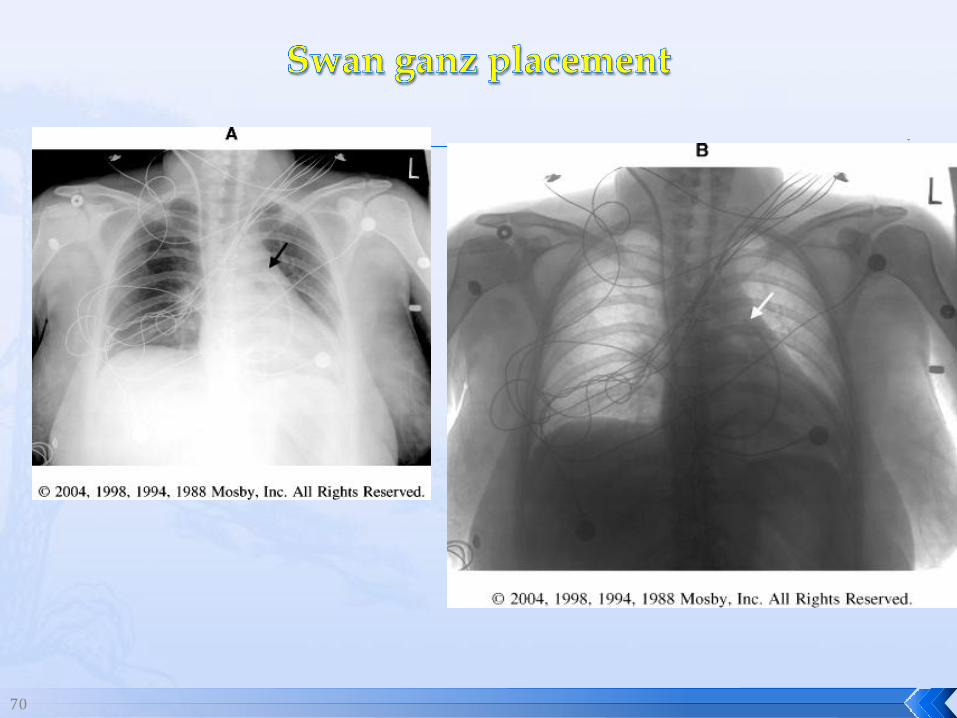
Increased possibility of artifacts
Remove all radiopaque objects
Move lines from imaging field if possible
Limit coverings to single, smoothed layer
61
62
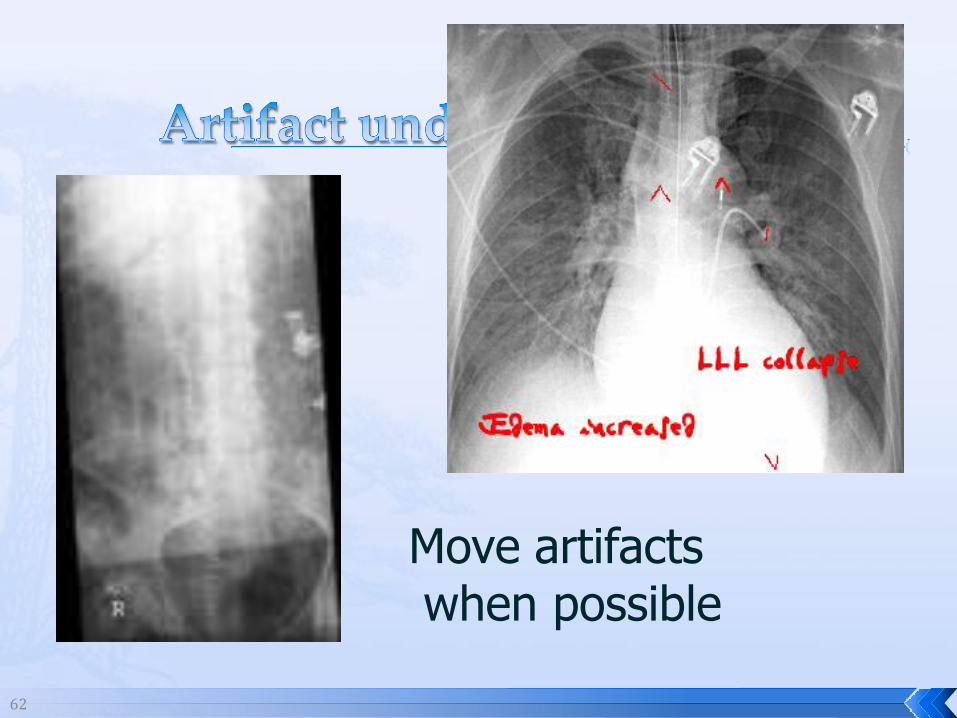
Move artifactswhen possible
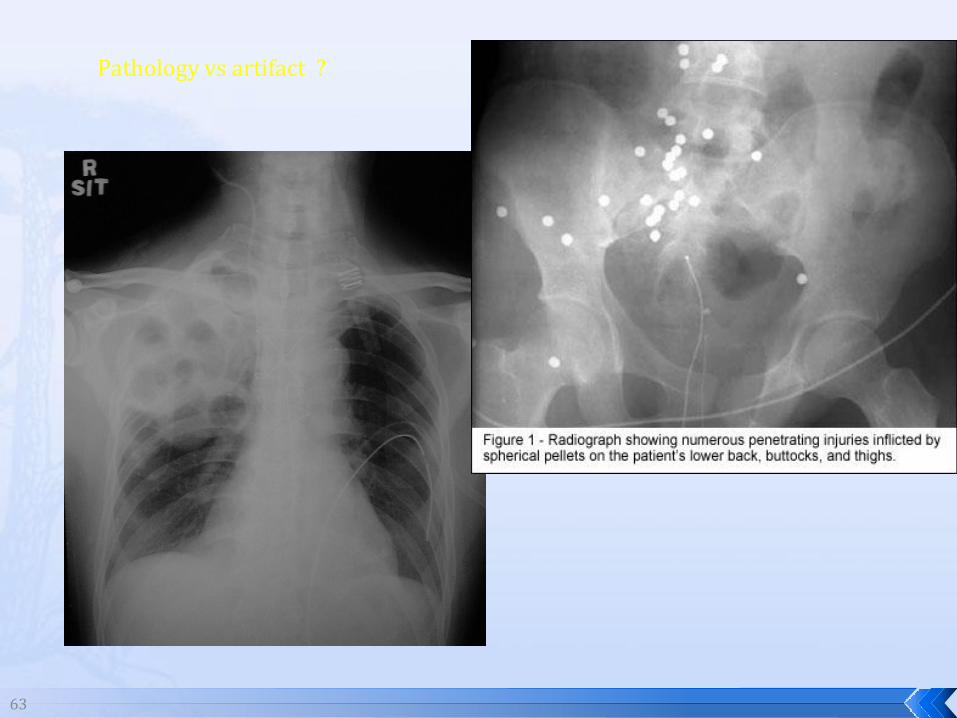
63
Pathology vs artifact ?
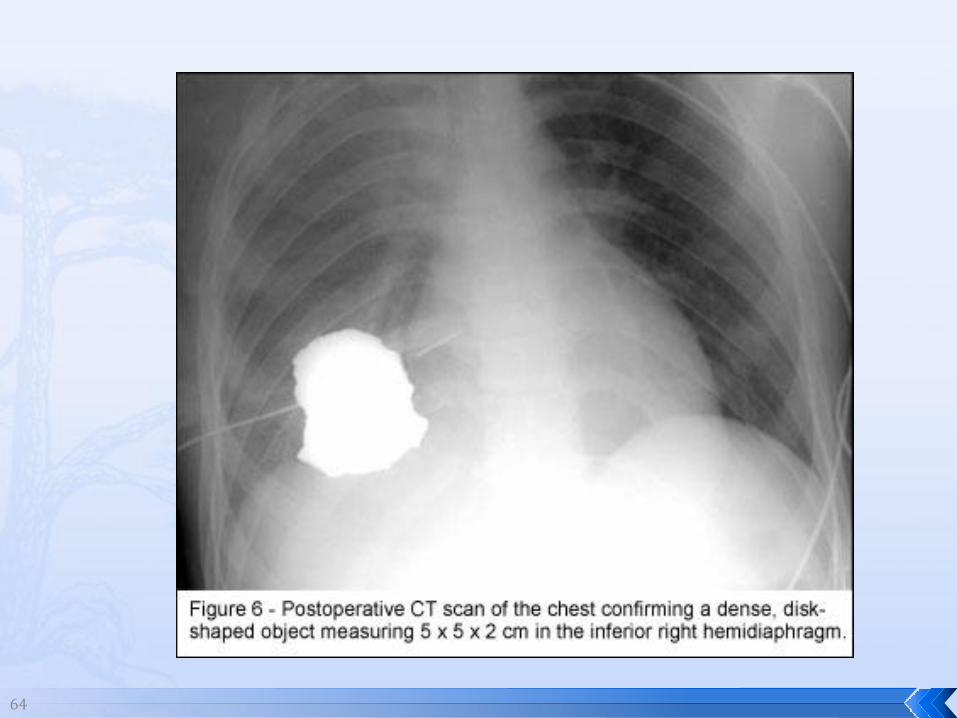
64
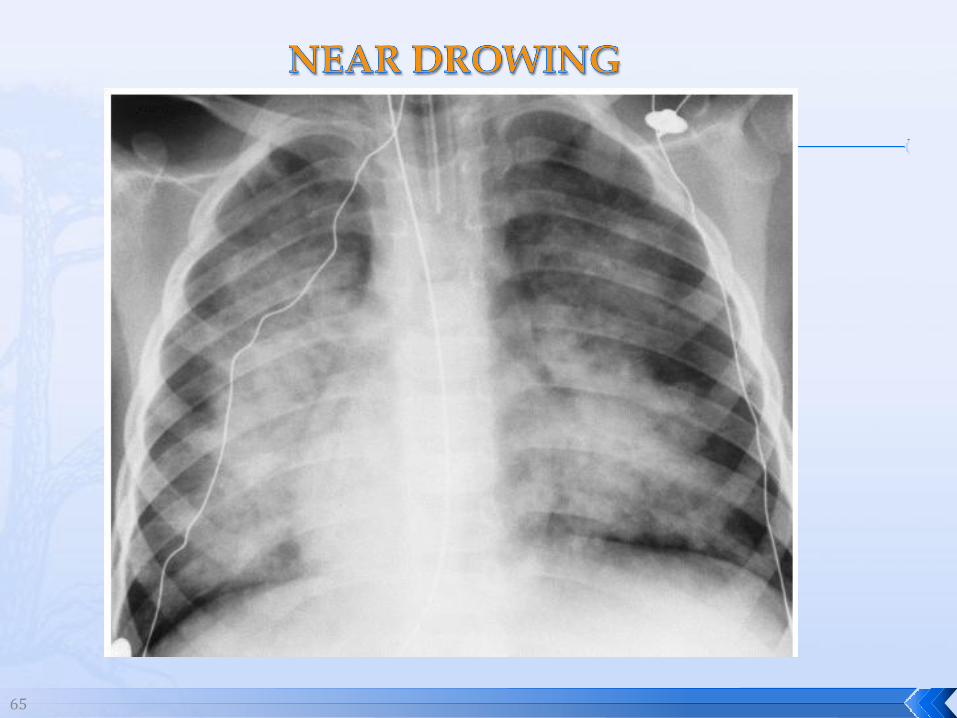
65
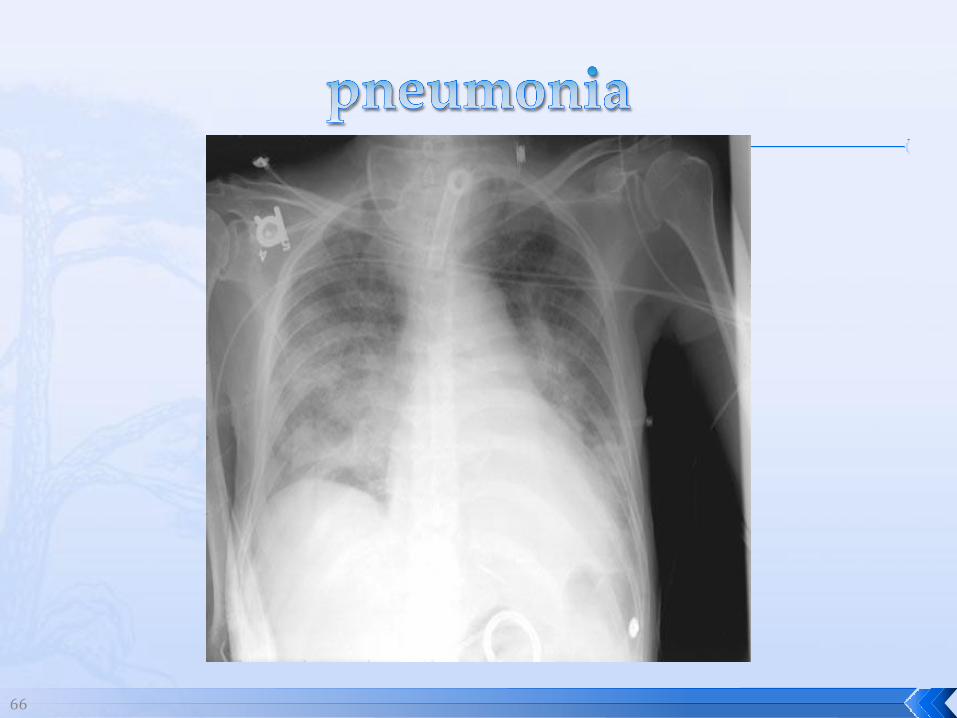
66
67
68
69
70

71
72
BASIC TYPES OF MOBILE RADIOGRAPHY
Battery Powered Unit
Capacitor-discharge Unit
High Frequency Units
Mobile Fluoroscopic ( C-ARM)
More on this later this semester
& in RT 244………..
73
C-ARM UNIT - Carltons pg 547
Tube at one end - I.I. at other end
TV Monitor control cart separate from unit
Uses Digital Fluoroscopy
Last Image Hold, Image Enhancement
Save for hard copies from disk, Video
Photographic Magnification, Subtraction
Static (pulsed) and continuous fluoro
Maneuverable and Versatile

74
75
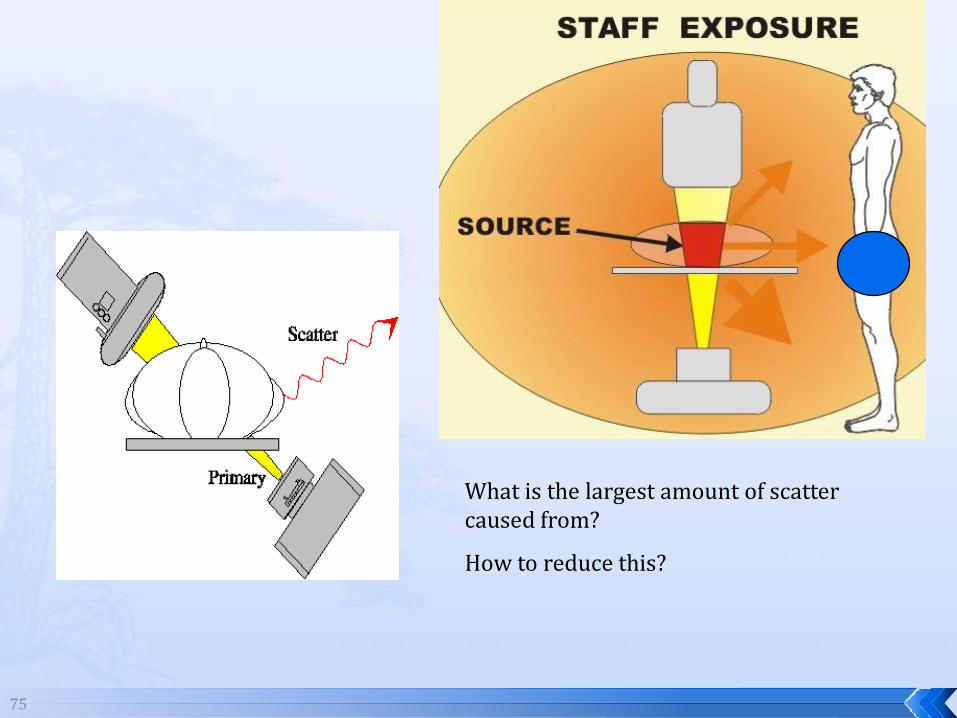
What is the largest amount of scatter caused from?
How to reduce this?
76
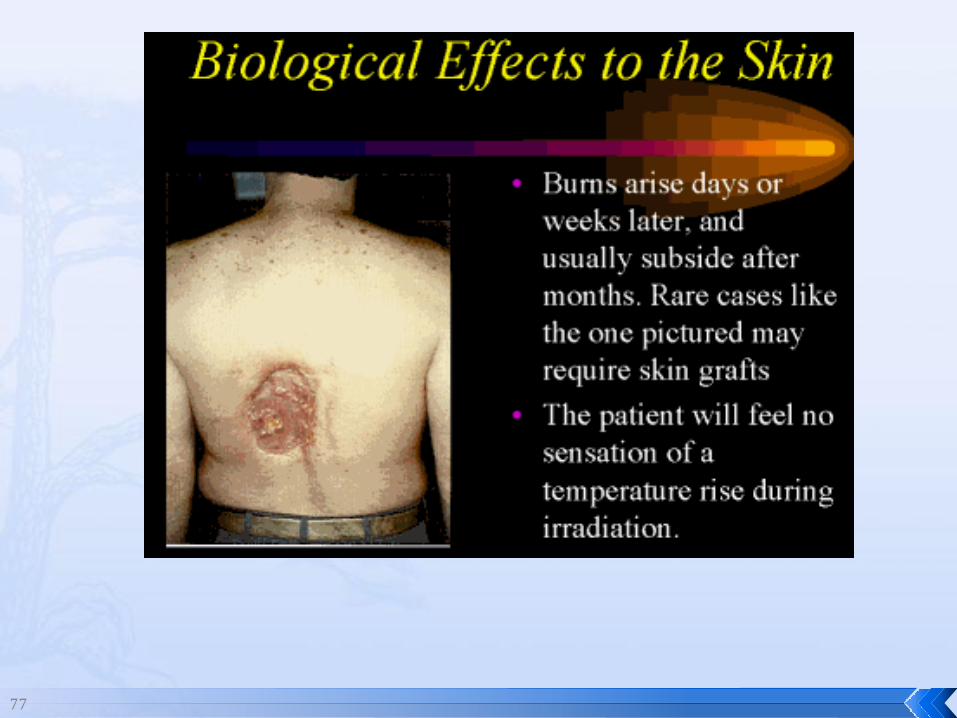
77

78
79
RADIOGRAPHIC
6 ‘ exposure cord
Minimum source to skin distance = 12”
Preferred SID of 40”to 72”+ (mag detail)
Distance from tube and patient
At least .25mm lead apron
FLUOROSCOPIC
Minimum source to skin distance = 12”
Preferred SSD OF 18”
Distance from tube and patient
5 min Audible Alarm
At least .25mm lead apron to be worn
5 R/min - 10 R/min
80
?? QUESTIONS??
Portable Equipment




![[XLS] · Web viewSHANMUGANATHAN A/L SUBRAMANIAM HJA1555 SHAMSUDIN BIN MOHD AJID HJ9849 SHAMSUDIN BIN BACHOK @ MOHD AMIN HJ6620 SHAMSUDIN B SULAIMAN HJA689 SHAMSUDDIN BIN A BAKAR HJA4454](https://img.pdfslide.net/doc/110x75/5aa40bf67f8b9a2f048bb171/xls-viewshanmuganathan-al-subramaniam-hja1555-shamsudin-bin-mohd-ajid-hj9849.jpg)