Embed Size (px)
Citation preview
mKDPK’de Sonunda Gerçek İlerleme!
Kanıt: Klinik çalışmalarda ZYTIGA
Dr. Sevil Bavbek
5. Türk Tıbbi Onkoloji Kongresi
Mart 2014, Antalya
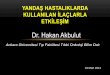
Endocrine therapies
Testosterone
DNA
Cell division
Testis Adrenals
Autocrine
secretion
Castration
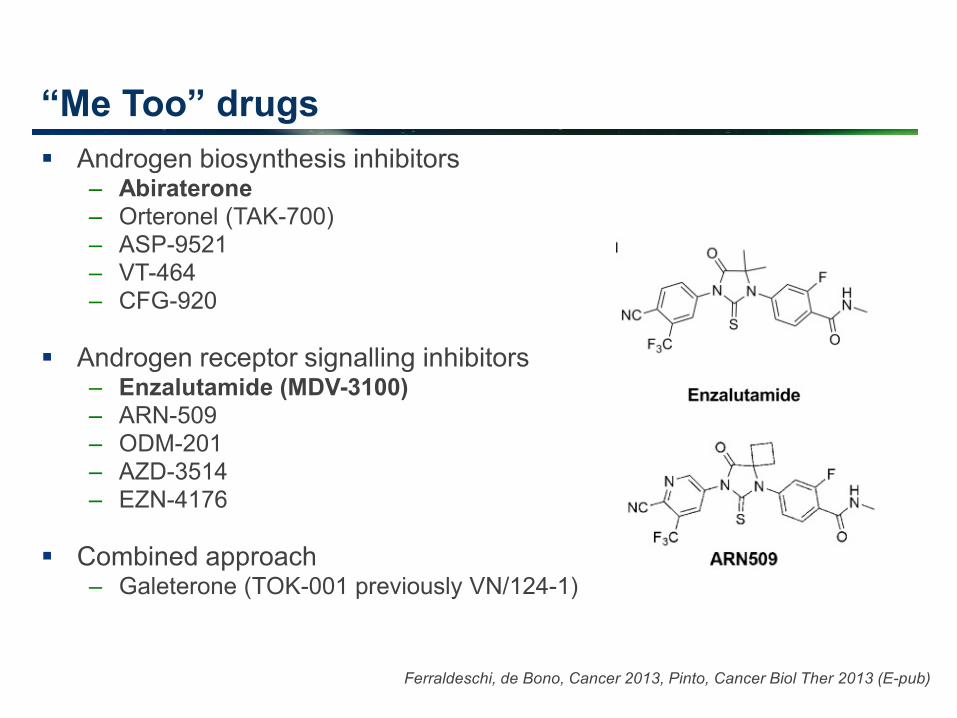
(aLHRH or Surg.) Abiraterone
Orteronel
Abiraterone
Orteronel
Androgen Receptor inhibitors:
-Bicalutamide
-MDV 3100
-ODM-201
-ARN 509
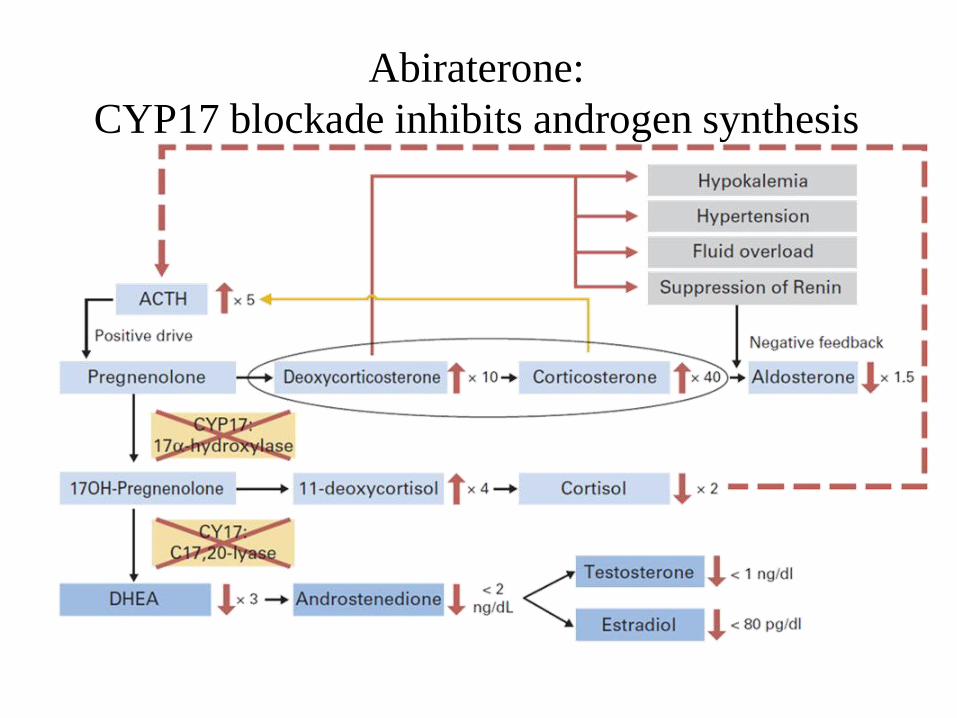
Abiraterone:
CYP17 blockade inhibits androgen synthesis b
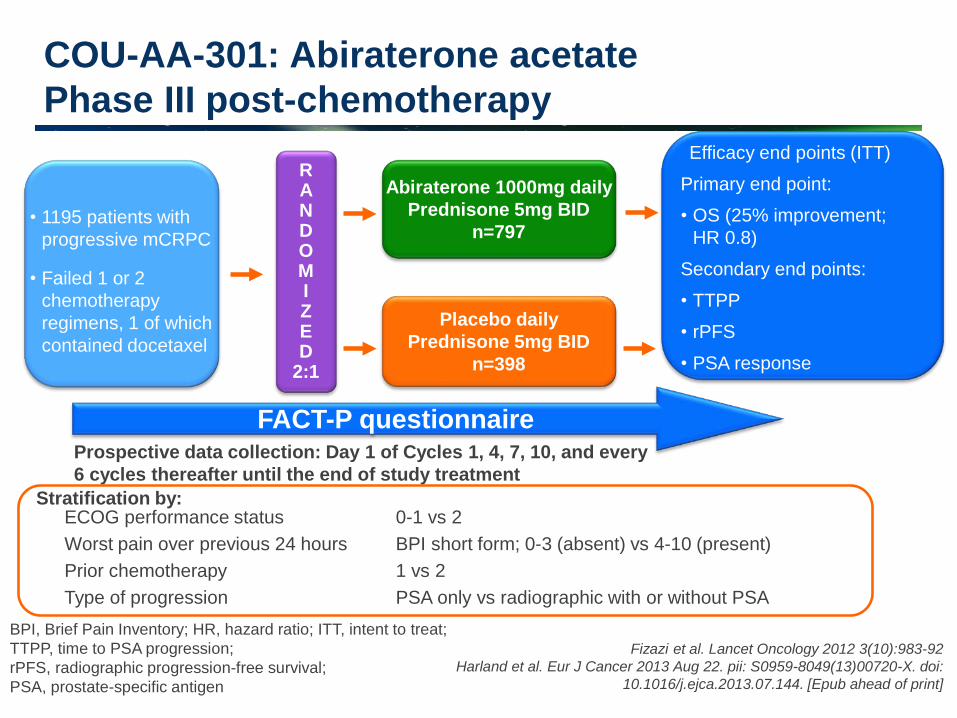
COU-AA-301: Abiraterone acetate
Phase III post-chemotherapy
Abiraterone 1000mg daily
Prednisone 5mg BID
n=797
Primary end point:
• OS (25% improvement;
HR 0.8)
Secondary end points:
• TTPP
• rPFS
• PSA response
Efficacy end points (ITT)
Placebo daily
Prednisone 5mg BID
n=398
R A N D O M I Z E D
2:1
• 1195 patients with
progressive mCRPC
• Failed 1 or 2
chemotherapy
regimens, 1 of which
contained docetaxel
BPI, Brief Pain Inventory; HR, hazard ratio; ITT, intent to treat;
TTPP, time to PSA progression;
rPFS, radiographic progression-free survival;
PSA, prostate-specific antigen
Fizazi et al. Lancet Oncology 2012 3(10):983-92
Harland et al. Eur J Cancer 2013 Aug 22. pii: S0959-8049(13)00720-X. doi:
10.1016/j.ejca.2013.07.144. [Epub ahead of print]
Prospective data collection: Day 1 of Cycles 1, 4, 7, 10, and every
6 cycles thereafter until the end of study treatment
FACT-P questionnaire
ECOG performance status 0-1 vs 2
Worst pain over previous 24 hours BPI short form; 0-3 (absent) vs 4-10 (present)
Prior chemotherapy 1 vs 2
Type of progression PSA only vs radiographic with or without PSA
Stratification by:
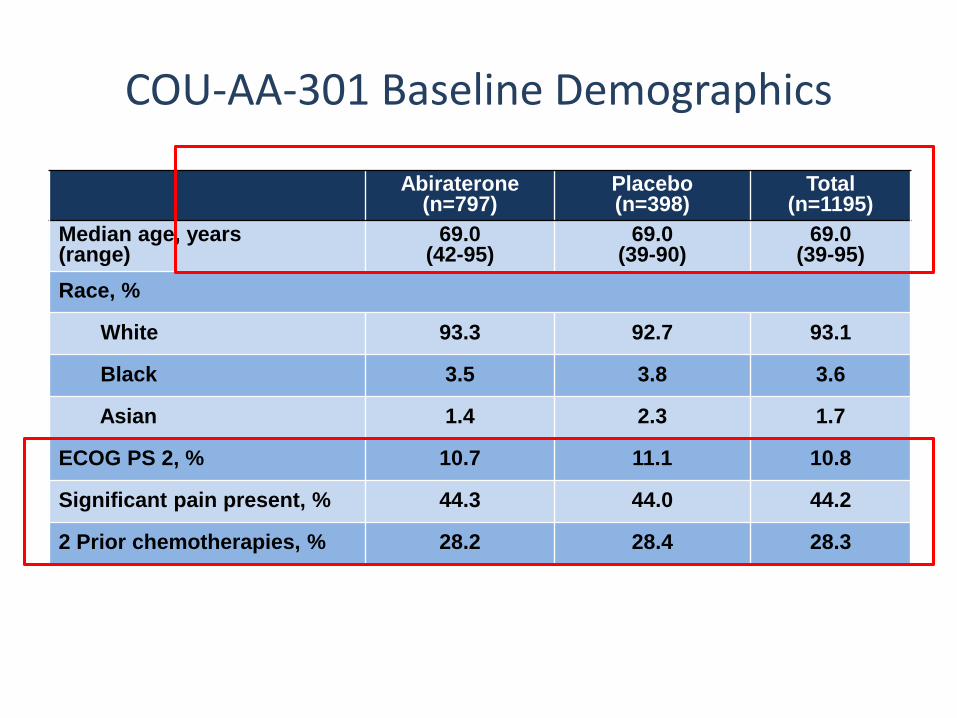
COU-AA-301 Baseline Demographics
Abiraterone(n=797)
Placebo (n=398)
Total (n=1195)
Median age, years (range)
69.0 (42-95)
69.0 (39-90)
69.0(39-95)
Race, %
White 93.3 92.7 93.1
Black 3.5 3.8 3.6
Asian 1.4 2.3 1.7
ECOG PS 2, % 10.7 11.1 10.8
Significant pain present, % 44.3 44.0 44.2
2 Prior chemotherapies, % 28.2 28.4 28.3
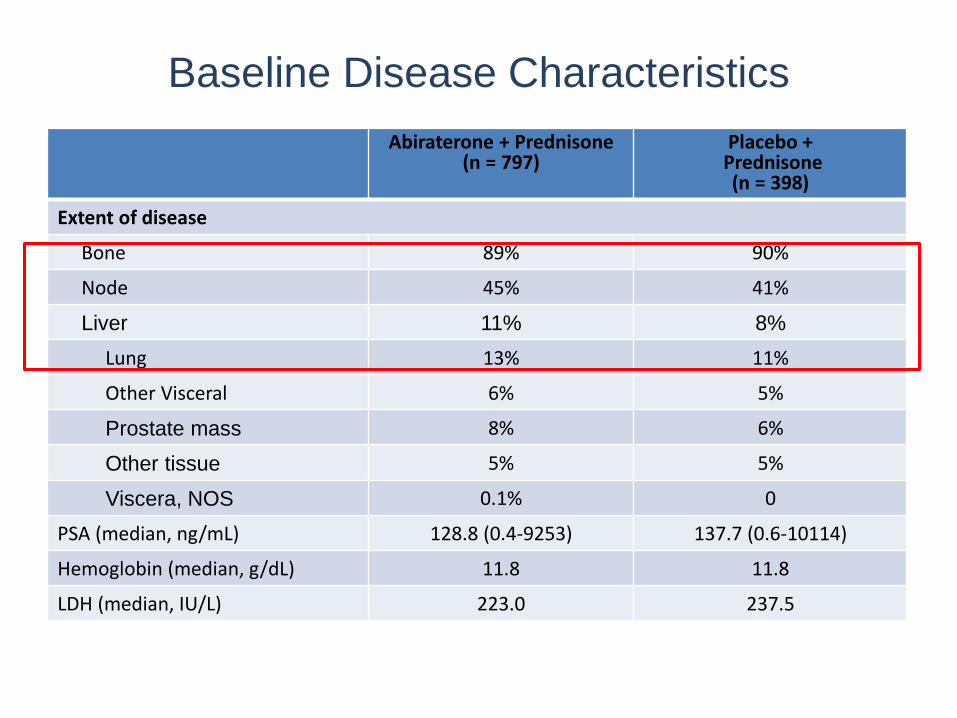
Baseline Disease Characteristics
Abiraterone + Prednisone(n = 797)
Placebo +Prednisone(n = 398)
Extent of disease
Bone 89% 90%
Node 45% 41%
Liver 11% 8%
Lung 13% 11%
Other Visceral 6% 5%
Prostate mass 8% 6%
Other tissue 5% 5%
Viscera, NOS 0.1% 0
PSA (median, ng/mL) 128.8 (0.4-9253) 137.7 (0.6-10114)
Hemoglobin (median, g/dL) 11.8 11.8
LDH (median, IU/L) 223.0 237.5
de Bono et al. N Engl J Med 2011; 346(21): 1995-2005
de Bono et al. N Engl J Med 2011; 346(21): 1995-2005 (Supplementary Data)
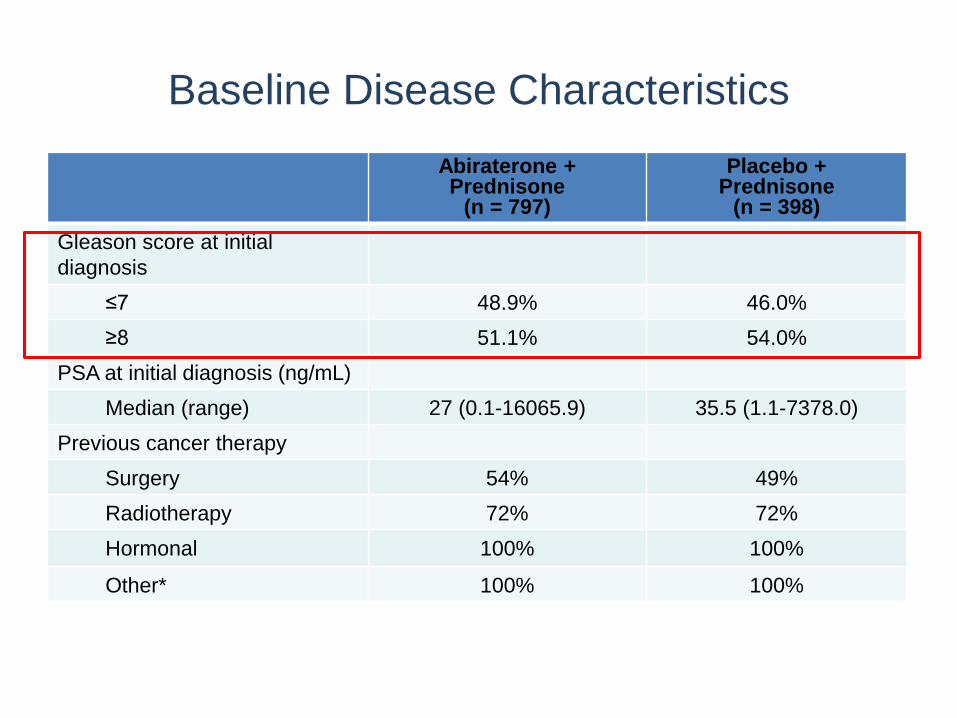
Baseline Disease Characteristics
Abiraterone + Prednisone
(n = 797)
Placebo + Prednisone
(n = 398)
Gleason score at initial
diagnosis
≤7 48.9% 46.0%
≥8 51.1% 54.0%
PSA at initial diagnosis (ng/mL)
Median (range) 27 (0.1-16065.9) 35.5 (1.1-7378.0)
Previous cancer therapy
Surgery 54% 49%
Radiotherapy 72% 72%
Hormonal 100% 100%
Other* 100% 100%
de Bono et al. N Engl J Med 2011; 346(21): 1995-2005
de Bono et al. N Engl J Med 2011; 346(21): 1995-2005 (Supplementary Data)
* Includes chemotherapy

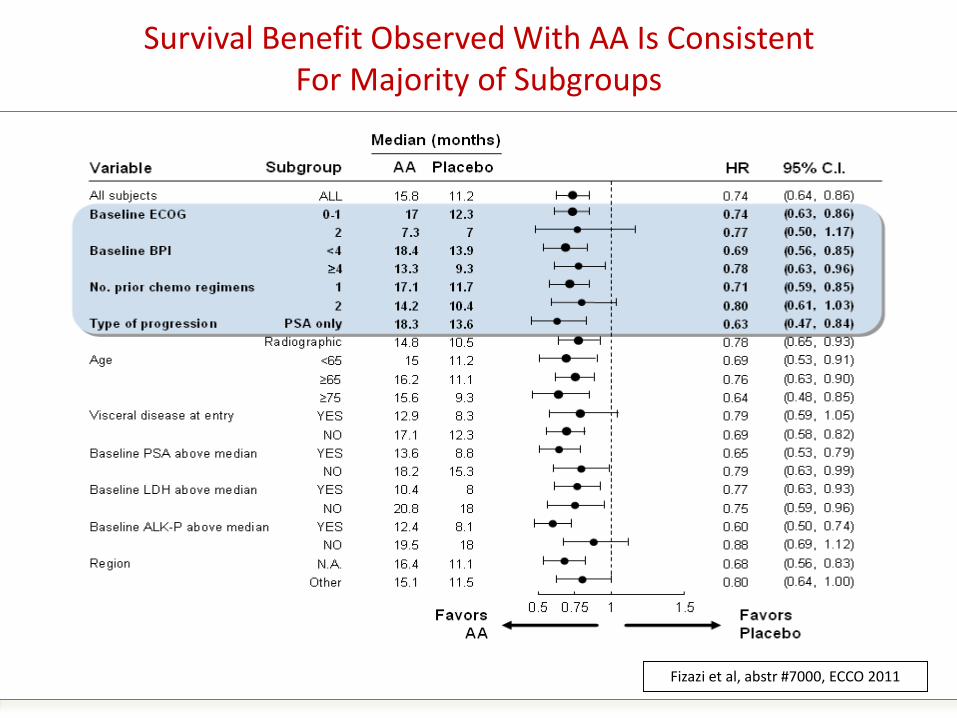
Survival Benefit Observed With AA Is Consistent For Majority of Subgroups
Fizazi et al, abstr #7000, ECCO 2011

Survival by Baseline ECOG Status
Favors AA for ECOG 0-1, but not for ECOG 2;
May be Attributed by the Small Sample Size
Median OS – Abiraterone + prednisone vs. Placebo + prednisoneECOG 0-1: 17 vs. 12.3 months (HR=0.74; 95% CI: 0.63-0.87; p=0.0002)
ECOG 2: 7.3 vs. 7 months (HR=0.77; 95% CI: 0.50-1.17; p=0.2166)
ECOG 0-1
20
0
0 6 12 18 24
715353
608281
452174
26397
146
Time to Death (Months)
Surv
ival
(%
)
30
00
ECOG 2 (10% of patients)
100
80
60
40
20
0
0 6 12 18 24
8245
4925
219
103
10
Time to Death (Months)
Surv
ival
(%
)30
00
100
80
60
40
Abiraterone + prednisone:
7.3 months
Abiraterone + prednisone:
17 months
Placebo +
prednisone:
7 months
Placebo + Prednisone:
12.3 months
Fizazi et al. Lancet Oncol 2012; 13(10): 983-992 (Supplementary Appendix)
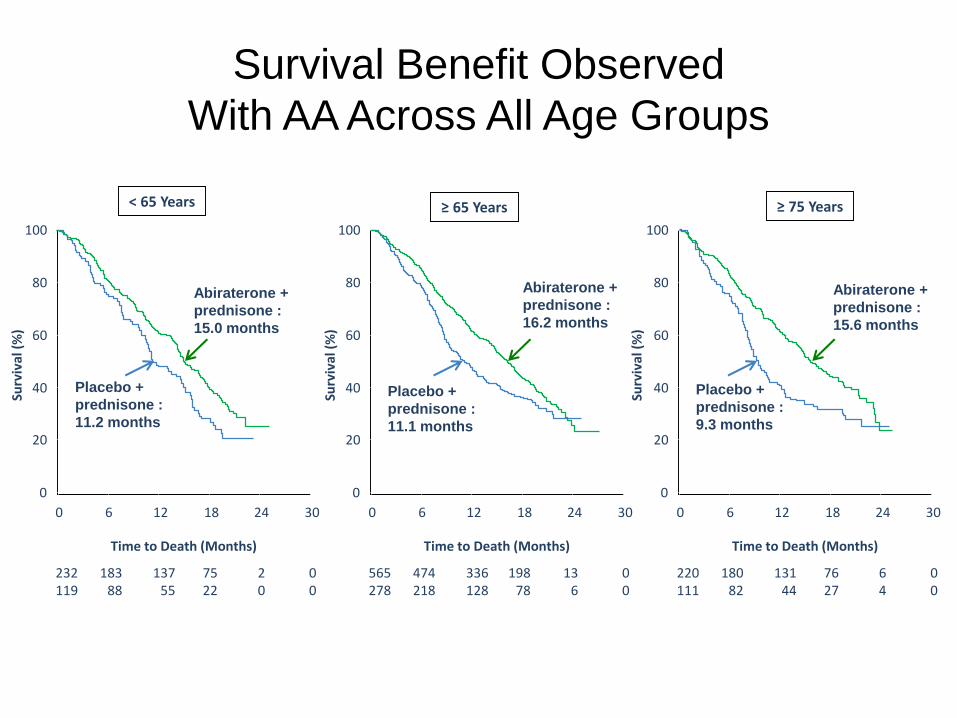
Survival Benefit Observed
With AA Across All Age Groups
Median OS – Abiraterone + prednisone vs. Placebo + prednisone: < 65 years: 15.0 vs. 11.2 months (HR=0.69; 95% CI: 0.53-0.91)≥ 65 years: 16.2 vs. 11.1 months (HR=0.76; 95% CI: 0.63-0.90)≥ 75 years: 15.6 vs. 9.3 months (HR=0.64; 95% CI: 0.48-0.85)
Placebo +
prednisone :
11.2 months
Placebo +
prednisone :
11.1 months
Placebo +
prednisone :
9.3 months
< 65 Years ≥ 65 Years ≥ 75 Years
0
232119
18388
13755
7522
20
Time to Death (Months)
Surv
ival
(%
)
0
6 12 18 24 30
00
20
40
60
80
100
0
565278
474218
336128
19878
136
Time to Death (Months)
Surv
ival
(%
)
0
6 12 18 24 30
00
20
40
60
80
100
0
220111
18082
13144
7627
64
Time to Death (Months)
0
6 12 18 24 30
00
20
40
60
80
100
Surv
ival
(%
)
Abiraterone +
prednisone :
15.0 months
Abiraterone +
prednisone :
16.2 months
Abiraterone +
prednisone :
15.6 months
Fizazi et al. ECCO 2011: Abstract 7000 (oral presentation)
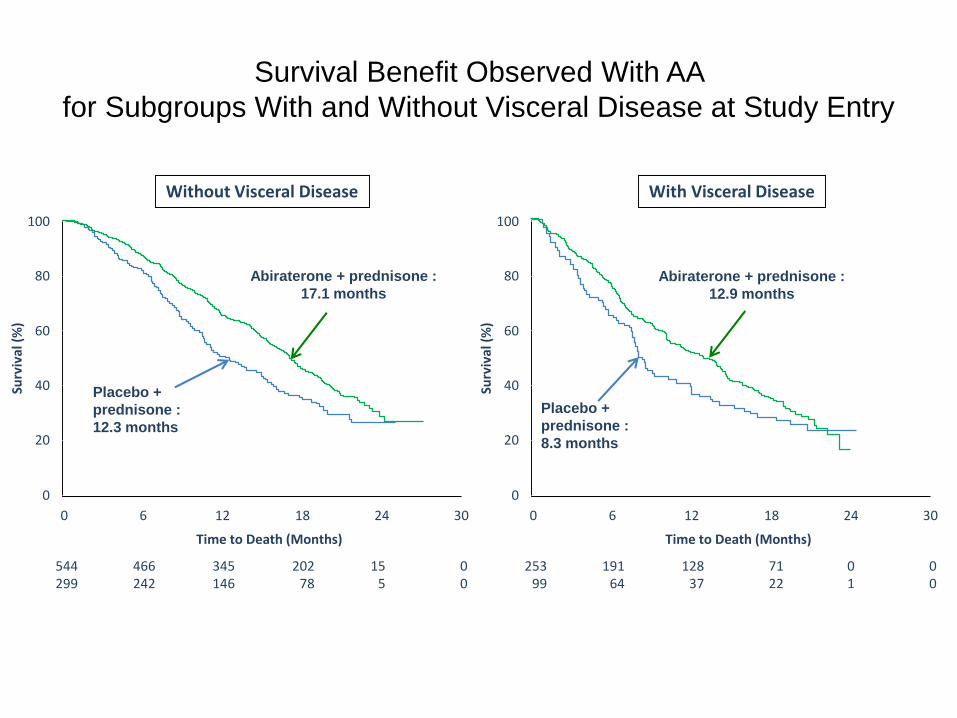
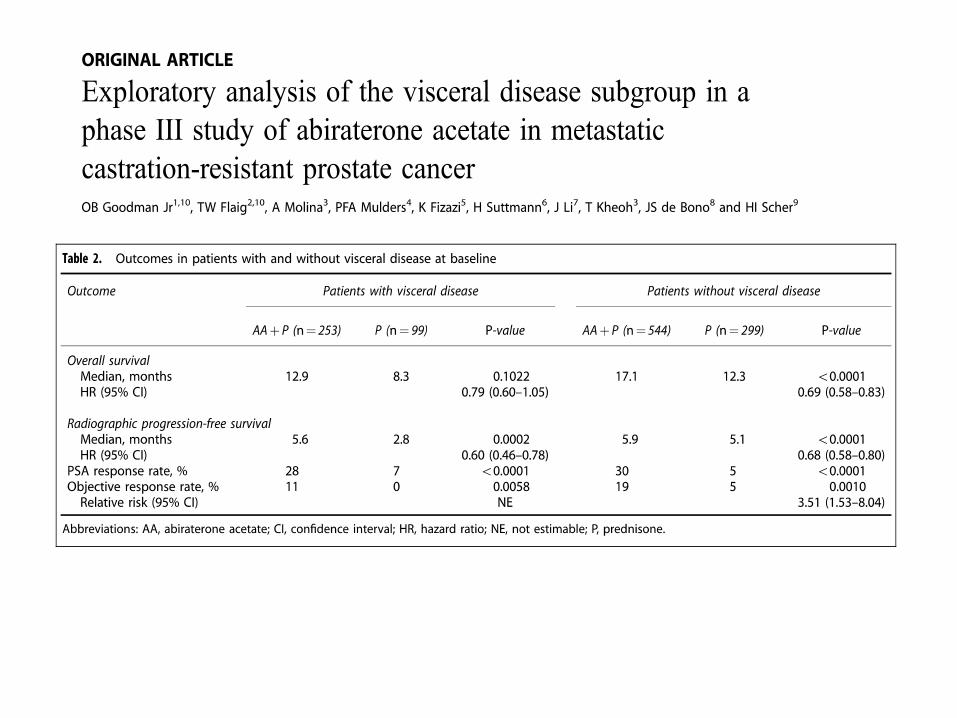
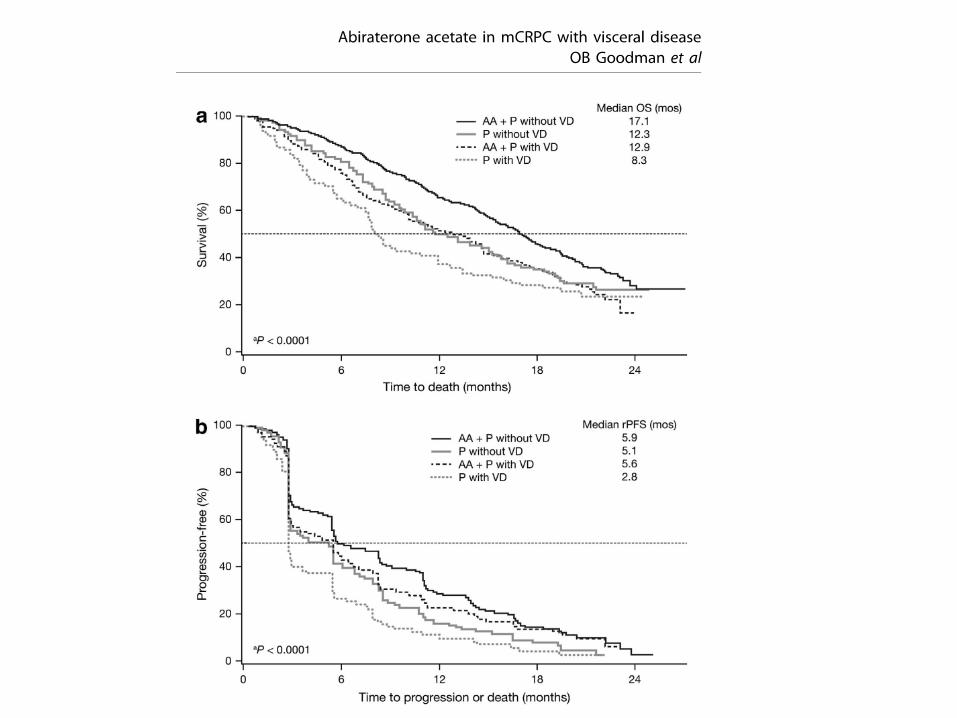
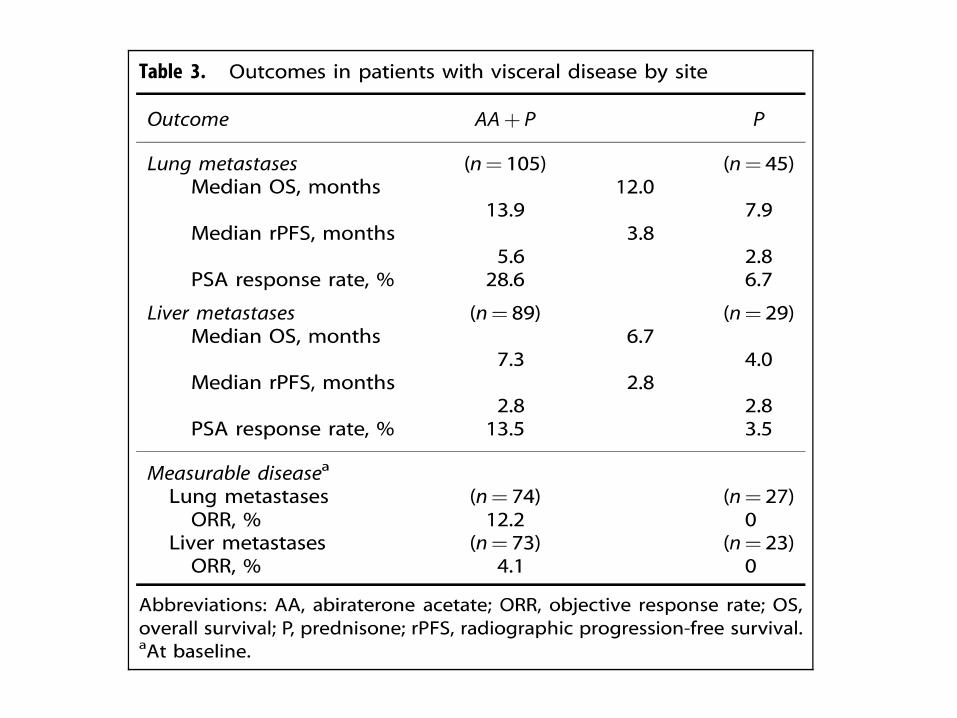
Survival Benefit Observed With AA
for Subgroups With and Without Visceral Disease at Study Entry
Median OS – Abiraterone + prednisone vs. Placebo + prednisone: Without visceral disease: 17.1 vs. 12.3 months (HR = 0.69; 95% CI: 0.58-0.82)
With visceral disease: 12.9 vs. 8.3 months (HR = 0.79; 95% CI: 0.59-1.05)
Placebo +
prednisone :
8.3 months
With Visceral Disease
100
80
60
40
20
0
0 6 12 18 24
544299
466242
345146
20278
155
Time to Death (Months)
Surv
ival
(%
)
30
00
100
80
60
40
20
0
0 6 12 18 24
25399
19164
12837
7122
01
Time to Death (Months)
Surv
ival
(%
)
30
00
Without Visceral Disease
Abiraterone + prednisone :
17.1 months
Placebo +
prednisone :
12.3 months
Abiraterone + prednisone :
12.9 months
Fizazi et al. ECCO 2011: Abstract 7000 (oral presentation)
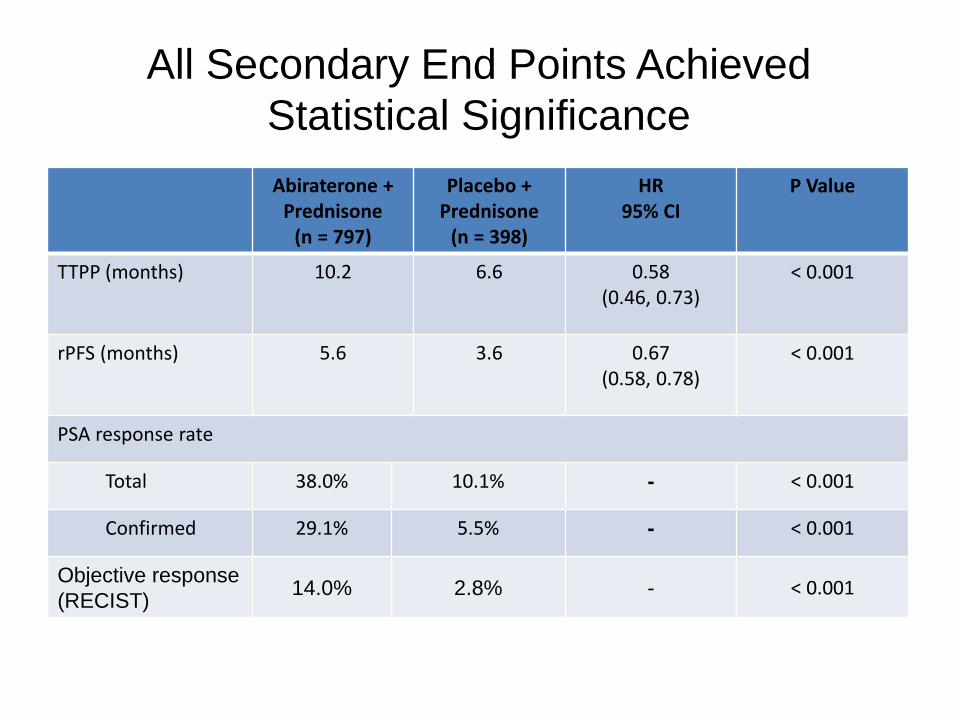
All Secondary End Points Achieved
Statistical Significance
Abiraterone + Prednisone
(n = 797)
Placebo + Prednisone
(n = 398)
HR95% CI
P Value
TTPP (months) 10.2 6.6 0.58(0.46, 0.73)
< 0.001
rPFS (months) 5.6 3.6 0.67(0.58, 0.78)
< 0.001
PSA response rate
Total 38.0% 10.1% - < 0.001
Confirmed 29.1% 5.5% - < 0.001
Objective response
(RECIST)14.0% 2.8% - < 0.001
de Bono et al. N Engl J Med 2011; 346(21): 1995-2005
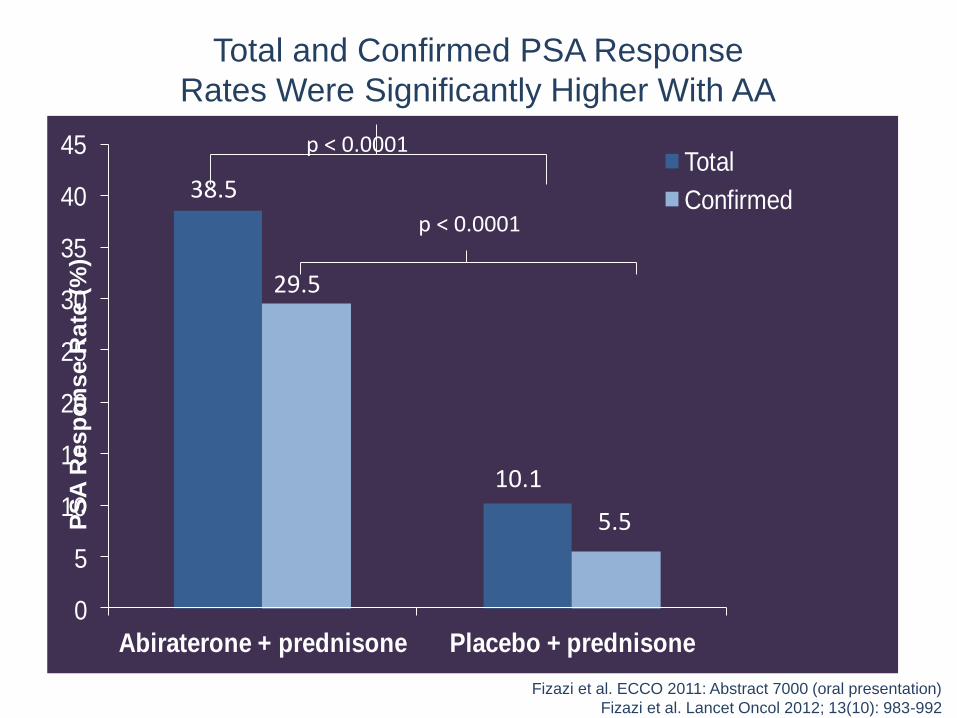
Total and Confirmed PSA Response
Rates Were Significantly Higher With AA
0
5
10
15
20
25
30
35
40
45
Abiraterone + prednisone Placebo + prednisone
Total
Confirmed38.5
29.5
10.1
5.5
p < 0.0001
p < 0.0001
PS
A R
esp
on
se R
ate
(%
)
Fizazi et al. ECCO 2011: Abstract 7000 (oral presentation)
Fizazi et al. Lancet Oncol 2012; 13(10): 983-992
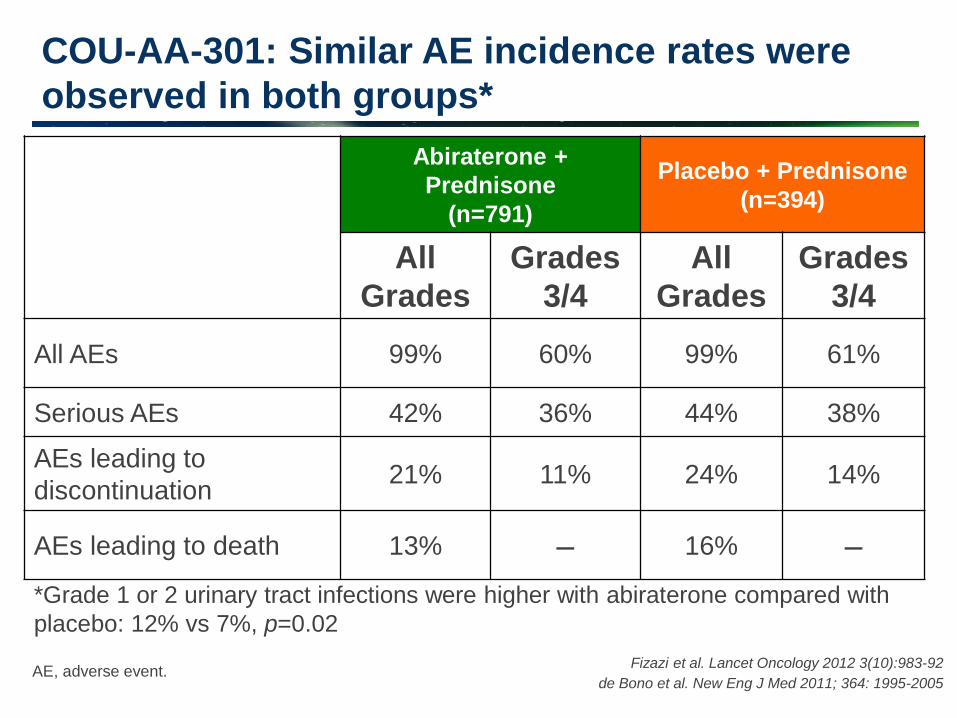
AE, adverse event.
COU-AA-301: Similar AE incidence rates were
observed in both groups*
Abiraterone +
Prednisone
(n=791)
Placebo + Prednisone
(n=394)
All
Grades
Grades
3/4
All
Grades
Grades
3/4
All AEs 99% 60% 99% 61%
Serious AEs 42% 36% 44% 38%
AEs leading to
discontinuation 21% 11% 24% 14%
AEs leading to death 13% – 16% –
Fizazi et al. Lancet Oncology 2012 3(10):983-92
de Bono et al. New Eng J Med 2011; 364: 1995-2005
*Grade 1 or 2 urinary tract infections were higher with abiraterone compared with
placebo: 12% vs 7%, p=0.02
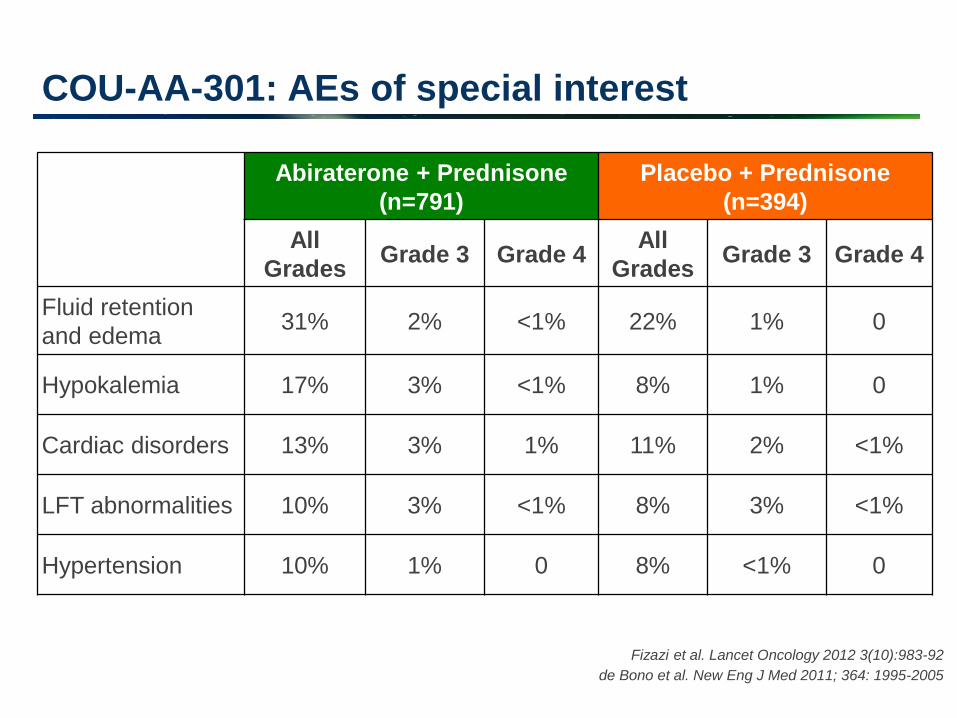
COU-AA-301: AEs of special interest
Abiraterone + Prednisone
(n=791)
Placebo + Prednisone
(n=394)
All
Grades Grade 3 Grade 4
All
Grades Grade 3 Grade 4
Fluid retention
and edema 31% 2% <1% 22% 1% 0
Hypokalemia 17% 3% <1% 8% 1% 0
Cardiac disorders 13% 3% 1% 11% 2% <1%
LFT abnormalities 10% 3% <1% 8% 3% <1%
Hypertension 10% 1% 0 8% <1% 0
Fizazi et al. Lancet Oncology 2012 3(10):983-92
de Bono et al. New Eng J Med 2011; 364: 1995-2005
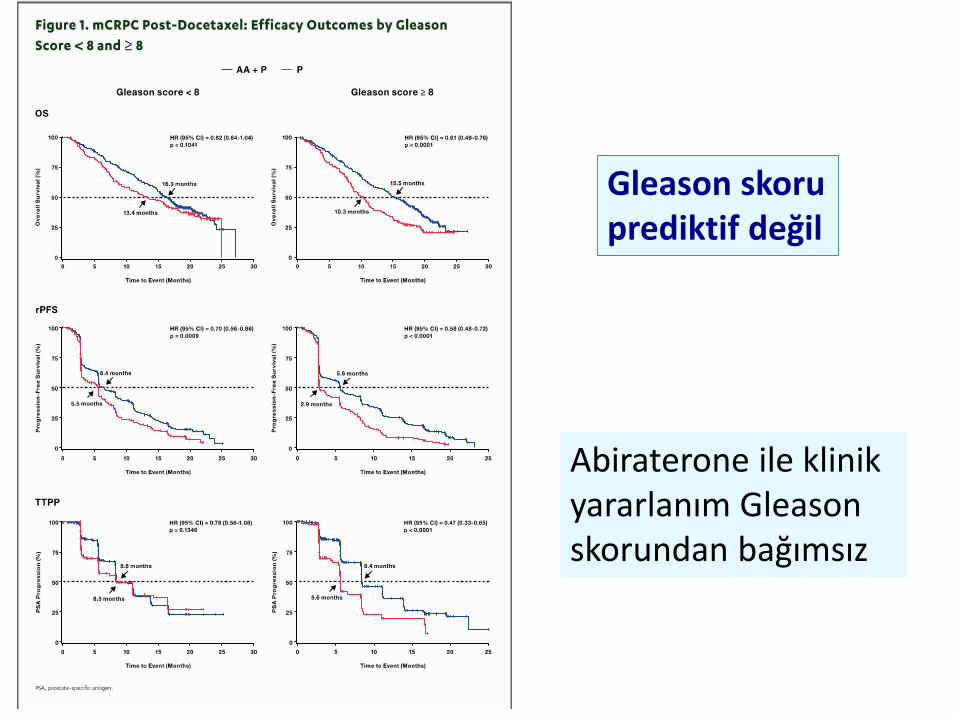
Abiraterone ile klinikyararlanım Gleason skorundan bağımsız
Gleason skoruprediktif değil
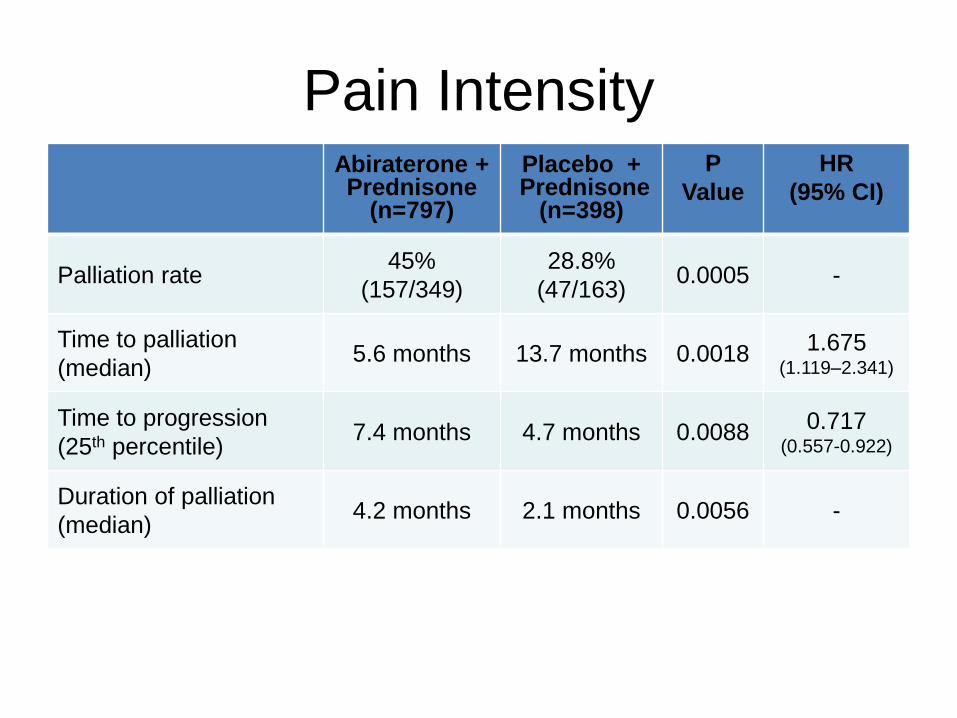
Pain IntensityAbiraterone + Prednisone
(n=797)
Placebo +Prednisone
(n=398)
P
Value
HR
(95% CI)
Palliation rate45%
(157/349)
28.8%
(47/163)0.0005 -
Time to palliation
(median)5.6 months 13.7 months 0.0018 1.675
(1.119–2.341)
Time to progression
(25th percentile)7.4 months 4.7 months 0.0088 0.717
(0.557-0.922)
Duration of palliation
(median)4.2 months 2.1 months 0.0056 -
Logothetis et al. Lancet Oncol 2012: 2012; 13: 1210–17
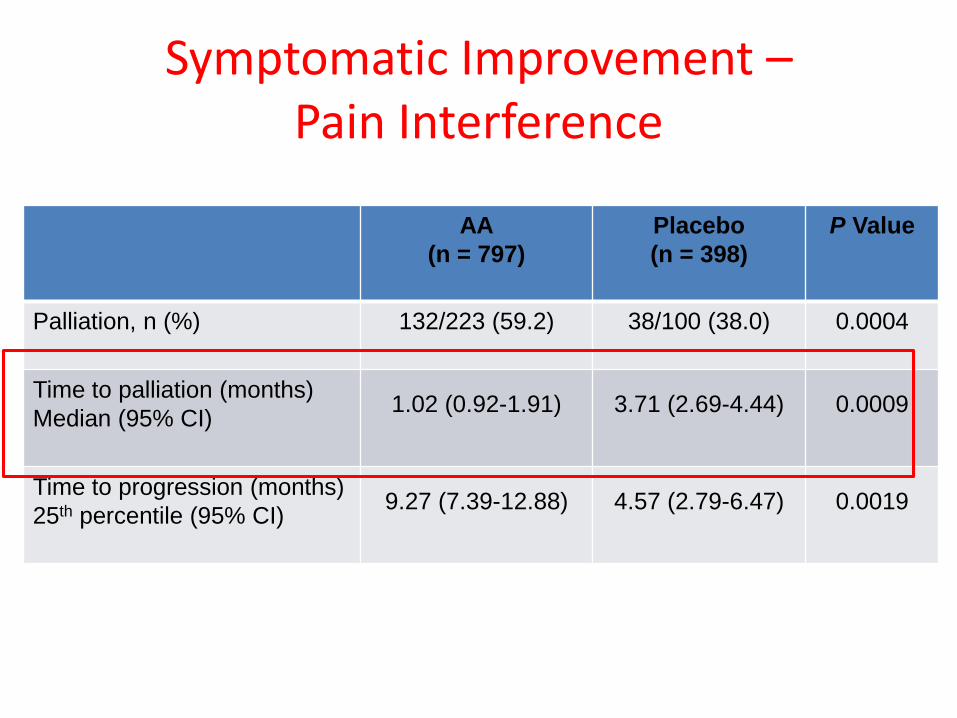
Symptomatic Improvement –Pain Interference
AA
(n = 797)
Placebo
(n = 398)
P Value
Palliation, n (%) 132/223 (59.2) 38/100 (38.0) 0.0004
Time to palliation (months)
Median (95% CI)1.02 (0.92-1.91) 3.71 (2.69-4.44) 0.0009
Time to progression (months)
25th percentile (95% CI)9.27 (7.39-12.88) 4.57 (2.79-6.47) 0.0019
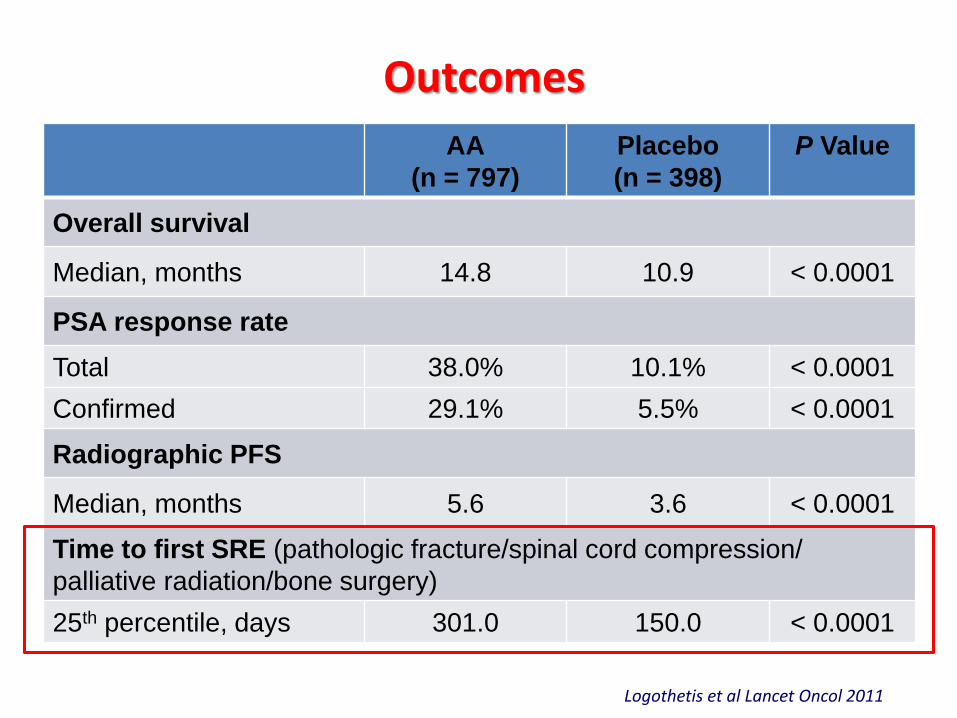
Outcomes
AA
(n = 797)
Placebo
(n = 398)
P Value
Overall survival
Median, months 14.8 10.9 < 0.0001
PSA response rate
Total 38.0% 10.1% < 0.0001
Confirmed 29.1% 5.5% < 0.0001
Radiographic PFS
Median, months 5.6 3.6 < 0.0001
Time to first SRE (pathologic fracture/spinal cord compression/
palliative radiation/bone surgery)
25th percentile, days 301.0 150.0 < 0.0001
Logothetis et al Lancet Oncol 2011
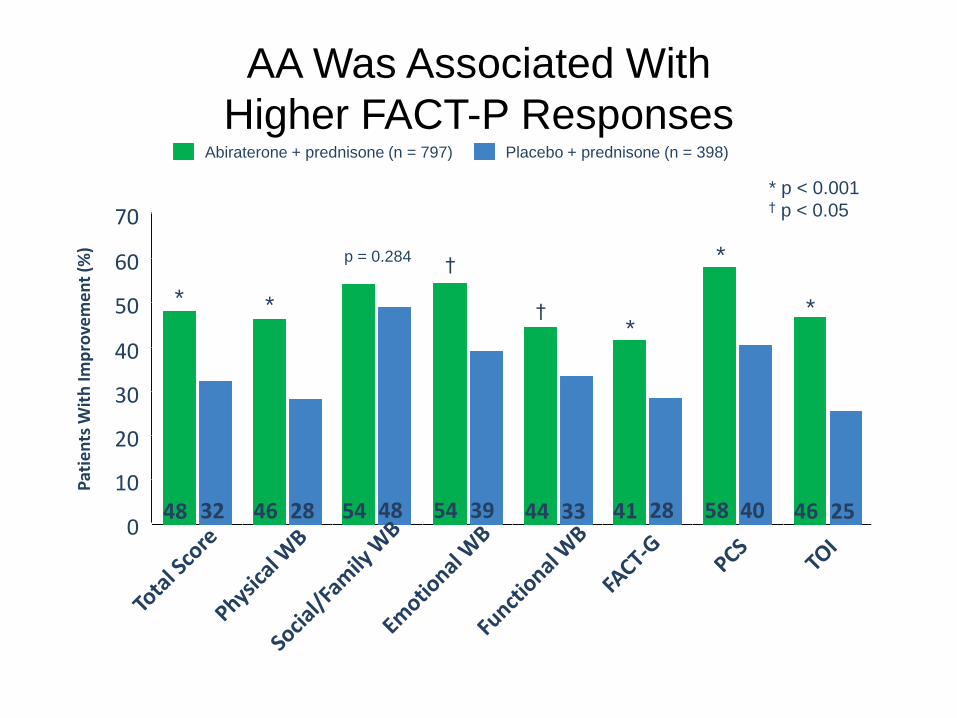
AA Was Associated With
Higher FACT-P ResponsesPlacebo + prednisone (n = 398)Abiraterone + prednisone (n = 797)
* **
*p = 0.284 †
† *
70
40
30
10
0
Pat
ien
ts W
ith
Imp
rove
me
nt
(%)
20
60
50
* p < 0.001† p < 0.05
48 32 46 28 54 48 54 39 41 28 58 40 46 2544 33
Harland et al. ECCO 2011: Abstract 7001 (oral presentation)
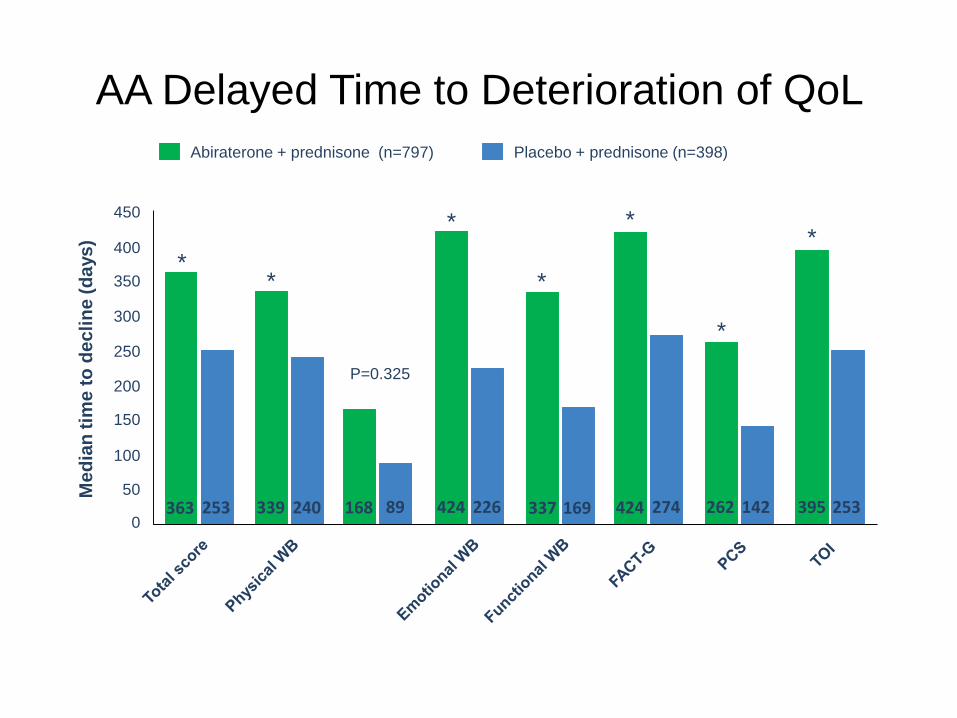
AA Delayed Time to Deterioration of QoL
* p<0.001450
250
200
100
0
Me
dia
n t
ime
to
de
cli
ne
(d
ays
)
150
300
400
350
50
*
P=0.325
*
* *
*
*
Placebo + prednisone (n=398)Abiraterone + prednisone (n=797)
363 253 339 240 168 89 424 226 424 274 262 142337 169 253395
*
Harland et al. ECCO 2011: Abstract 7001 (oral presentation)
COU-AA-301 Conclusions
Median OS improvement of approximately 5 months
– 36% improvement in median survival
– 35% risk reduction of death (HR = 0.65)
Improved TTPP, PFS, and PSA response rate
– 38% of patients had a >50% reduction in PSA
Clinical benefit for treatment of bone metastases:
–Improved pain palliation
–Delayed pain progression and time to SRE
–Effect sustained over treatment cycles
Favorable Safety Profile
Abiraterone acetate prolonged OS in patients with mCRPCwho have progressed after docetaxel-based chemotherapy
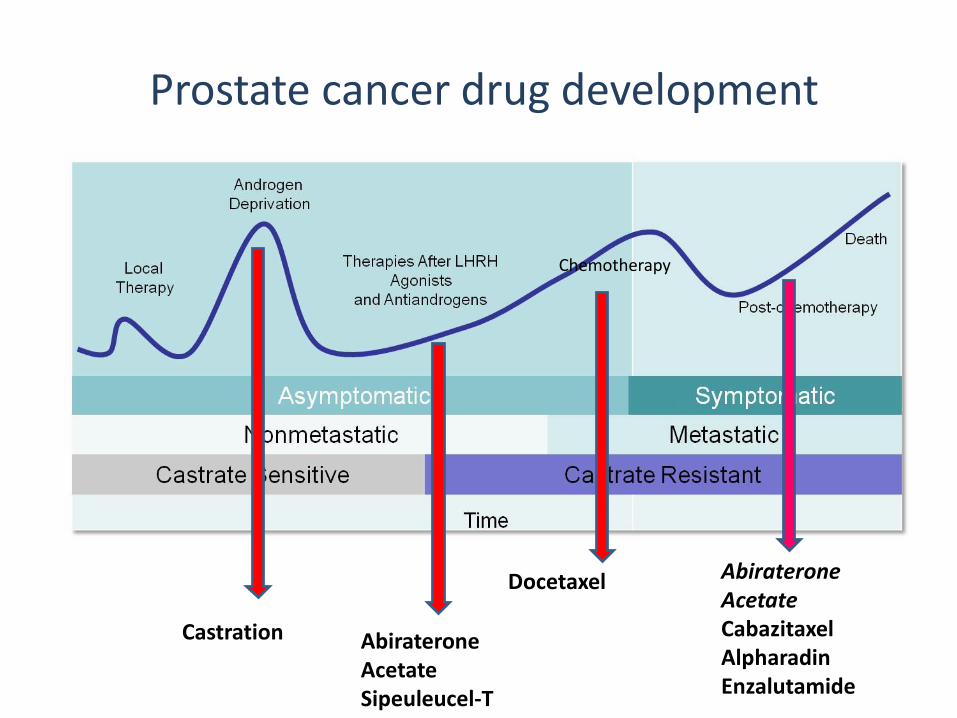
Prostate cancer drug development
Chemotherapy
Tum
or
volu
me
& a
ctiv
ity
NOTE: This diagram represents typical disease progression. Some patients are metastatic at diagnosis and are thus still castrate sensitive. Abiraterone
AcetateSipeuleucel-T
Castration
Docetaxel AbirateroneAcetateCabazitaxelAlpharadinEnzalutamide