Embed Size (px)
Citation preview

HEALTH POLICY AND ANALYTICS
Public Employees’ Benefit Board
Kate Brown, Governor
Chair Shaun Parkman will convene a public meeting of the PEBB Board on Tuesday, September 18, 2018, at 9:30 a.m. The meeting will be held in the boardroom of the Health Licensing Office at 1430 Tandem Ave., Ne, Suite 180, Salem, Oregon.
PEBB BOARD AGENDA
I. 9:30 a.m. – 9:35 a.m. Attachment 1
Welcome & Approval of August 21, 2018 meeting synopses (action) Shaun Parkman, Chair
II. 9:35 a.m. – 9:55 a.m. Attachment 2
Financial Update (information/discussion) Ali Hassoun, OEBB/PEBB Interim Director
III. 9:55 a.m. – 10:15 a.m. Attachment 3
Opt-out and Double Coverage Elimination (SB 1067) Cindy Bowman, OEBB/PEBB Director of Operations Linda Freeze - Benefit Manager
IV. 10:15 a.m. – 10:55 a.m. Attachments 4, 4a and 4b
Network/Access (information/discussion) Dr. Keith Bach, PEBB Medical Director and Sophary Sturdevant, Executive Account Manager, Kaiser Permanente Dr. Jim Rickards, Senior Medical Director and Jill Harland, Director Provider Relations, Moda Health Plans Stephanie Dreyfus, Vice President of Network Development, Providence Health Plans
V. 10:55 a.m. – 12:20 p.m. Attachment 5
Strategic Planning Continued – Next Steps Emery Chen and Robert Valdez, Mercer Health & Benefits, LLC
VI. 12:20 p.m. – 12:25 p.m. Other Business
VII. 12:25 p.m. – 12:30 p.m.
Public Comment

Public Employees’ Benefit Board Page 2 of 2
Adjourn

Page 1 of 2
Attachment 1 PEBB Board Meeting
September 18, 2018
Public Employees’ Benefit Board Meeting Synopsis
August 21, 2018
The Public Employees’ Benefit Board held a regular meeting on August 21, 2018, at the Health Licensing Office, 1430 Tandem Ave. NE, Suite 180, Salem, Oregon. Chair Shaun Parkman called the meeting to order at 10:00 a.m. Attendees Board Members: Shaun Parkman, Chair Kimberly Hendricks, Vic Chair Bill Barr Representative Mitch Greenlick Kim Harman (via phone) Siobhan Martin Jeremy Vandehey Board Members Excused/Absent: Senator Betsy Johnson Dana Hargunani, MD Mark Perlman OEBB Staff: Ali Hassoun, Interim Director Cindy Bowman, Director of Operations Rose Mann, Executive Assistant Brian Olson, Contracts Specialist Consultants (WTW): Nick Albert, Mercer Health and Benefits, LLC (via phone) Emery Chen, Mercer Health and Benefits, LLC Robert Valdez, Mercer Health and Benefits, LLC View meeting agenda and attachments. View the meeting recording

Page 2 of 2
Attachment 1 PEBB Board Meeting
September 18, 2018
I. Welcome and approval of July 17, 2018, Board Meeting Synopsis (Attachment 1) - Video Recording 0:02:39
Shaun Parkman introduced new Board member, Jeremy Vandehey, Director of Health Policy and Analytics with OHA.
MOTION - Video Recording 0:04:21 Bill Barr moved to approve the synopsis of the July 17, 2018 PEBB Board meeting. Kim Harman seconded the motion. The motion carried 5 – 0 - 1. Jeremy Vandehey abstained.
II. PEBB Member Advisory Committee (PMAC) Introduction and Health Engagement
Model (HEM) Recommendation (Attachment 2) - Video Recording 00:04:56 Brian Olson, Theresa Cross and Lesa Dixon-Grey presented information on the PMAC and Health Engagement Model.
III. Mercer National Survey of Employer-sponsored Health Plans 2017 (Attachment 3) - Video Recording 00:41:22
Robert Valdez, Mercer Health & Benefits LLC, reported on the results of PEBB’s member utilization for July.
IV. Strategic Planning Presentation (Attachment 4) - Video Recording 01:36:32
Emery Chen and Robert Valdez, Mercer Health and Benefits, LLC, presented information and recommendations for PEBB strategic planning for the future.
V. Other Business/Public Comment - Video Recording 02:54:38
Deborah Tremblay gave public comment requesting Kaiser Dental cover nitrous oxide without additional co-pay.
There being no further business to come before the Board, Chair Shaun Parkman adjourned the meeting at 1:10 p.m.

Place Your Logo Here - Align Center
SB1067“Elimination of Double Coverage and Opt-Out
Incentives”
2
SB1067-What it Does
Double Coverage Elimination“The board may approve more than one carrier for each type of benefit plan offered, but the board shall limit the number of carriers to a number consistent with adequate service to eligible employees and family members who are not enrolled in another health benefit plan offered by the board or the Public Employees’ Benefit Board.”

3
SB1067-What it Does
Opt Out Elimination“An eligible employee who declines coverage in a health benefit plan offered by the Oregon Educators Benefit Board or the Public Employees’ Benefit Board and who is enrolled as a spouse or family member in another health benefit plan offered by the Oregon Educators Benefit Board or the Public Employees’ Benefit Board may not be paid the employer contribution for the plan that was declined.”

Definitions
Health Benefit PlanMedical/RX Plan only (does not include Dental or Vision)
Employer ContributionThis could mean the entire employer contribution or a subset of the employer contribution
4

Double Coverage Scenarios
#1 (PEBB/PEBB)Jack and Diane both work for different state agencies. Jack and Diane usually both take the PEBB Medical Plan and cover their entire family.• Effective January 1, 2020, either Jack OR Diane can cover the
entire family with a PEBB Medical Plan.• Jack could take the coverage for himself and their children and
Diane could take employee only coverage. She would not be able to cover the children with medical if Jack covers them.
• Both Jack and Diane can still double cover the entire family on Dental and Vision.
5

Double Coverage Scenarios#2 (OEBB/PEBB)Jack works for DOC and Diane works for Astoria SD. Jack and Diane usually both take medical coverage via PEBB and OEBB and cover their entire family.• Effective October 1, 2019, Diane will not be able to take the OEBB
medical coverage for Jack, herself or their children if Jack is showing these dependents covered in PEBB.
• PEBB may have to open up their system for a QSC to allow Jack to drop Diane and their children from coverage to allow Diane to enroll them in OEBB coverage during OEBB’s OE.
• OEBB may have to open up their system for a QSC to allow Diane to drop Jack and their children form coverage to allow Jack to enroll them in PEBB coverage during PEBB’s OE.
• Both Jack and Diane can still double cover the entire family on Dental and Vision.
6

Double Coverage Scenarios
#3 (PEBB/PGE)Jack works for DOC and Diane works for PGE. Jack and Diane usually both take medical coverage via PEBB and PGE and cover their entire family.• Jack and Diane will see no difference in how their plan works.
7

Opt Out Scenarios#1 (PEBB/PEBB)Jack and Diane both work for different state agencies. Jack usually takes the PEBB Medical Plan for the entire family and Diane usually Opts Out of medical and takes the $233 incentive.• Effective January 1, 2020, either Jack OR Diane can cover the
entire family with a PEBB Medical Plan. Neither can take the incentive.
• Jack could take the coverage for himself and their children and Diane could take employee only coverage. She would not be able to cover the children with medical if Jack covers them.
• Both Jack and Diane can still double cover the entire family on Dental and Vision.
8

Opt Out Scenarios#2 (OEBB/PEBB)Jack works for DOC and Diane works for Astoria SD. Either of them are currently eligible for an Opt Out incentive. But, this incentive now goes away effective October 1, 2019 for Diane and January 1, 2020 for Jack.• Since Diane’s enrollment comes first they may choose to enroll in
the OEBB Medical Plan until January 1, 2020. Jack can still take the incentive until January 1, 2020.
• During Jack’s open enrollment the couple may evaluate PEBB and OEBB Medical Plans. They may evaluate the following:– Out of pocket costs– Richness of medical plan
• It may be likely that we see Diane opt out of the OEBB Medical Plan and Jack enrolls the entire family in the PEBB Medical Plan.
• Both Jack and Diane can still double cover the entire family on Dental and Vision.
9

Opt Out Scenarios
#3 (PEBB/PGE)Jack works for DOC and Diane works for PGE. Jack and Diane usually both take medical coverage via PEBB and PGE and cover their entire family.• Jack and Diane will see no difference in how their plan works.
10

What have we been doing?
• Rule Construction• DOJ Opinions
• How Incentives Work• Special Contracts• Court Orders• Defining Health Benefit Plan
• Identifying System Changes
11

Rule Construction
• We can add a new SB1067 section• OR• We can add to our existing sections
• Obviously, rules will be a bit more challenging on the OEBB side. Many different monetary incentives exist on the OEBB side than PEBB.
• Rules for system processes will need to be developed• Who gets coverage terminated once double
coverage is discovered via OEBB/PEBB?
12

DOJ Opinion
• What is a monetary incentive versus employer contribution?• The PEBB incentive is $233 and clearly not the employer contribution• The PEBB incentive is cash and added to the payroll• The OEBB incentive could be anything even up to the employer
contribution• The OEBB incentive might not be cash added to the payroll
• Does the incentive have to be paid to the subscriber opting out or can it be paid to their spouse/DP
• Court Orders• Parent has a court order to cover children on medical
• Health Benefit Plan• Can we assume a Health Benefit Plan only refers to medical/RX
13
System Changes• QSCs
– Both OEBB and PEBB will have to allow special QSCs during the other’s enrollment period to add or drop dependents
– Both OEBB and PEBB will have to ask subscribers a series of questions when they click on medical to evaluate their enrollment
• PEBB/PEBB Double Coverage Changes and Language• What if dad is under court order to carry coverage but mom is
enrolled• Who’s coverage gets dropped (birthday rule?)• Stopping subscriber in PEBB/PEBB enrollment when the second
(or third) person tries to double (triple) cover• No matter, extra communication to members for processing
14

System Changes
• OEBB/OEBB Double Coverage Changes and Language• What if dad is under court order to carry coverage but mom is
enrolled• Whose coverage gets dropped (birthday rule?)• Stopping subscriber in OEBB/OEBB enrollment when the
second (or third) person tries to double (triple) cover• We can’t assume the richer plan is the best coverage
– Contributions can differ at each entity (this includes HSA contributions)
15

System Changes• OEBB/PEBB Double Coverage Changes and Language
• This scenario will be the most challenging as the systems are not synchronized
• Instead of stopping the subscriber from enrolling we will have to ask them a series of questions to evaluate their enrollments
• We will have to have protective language in both systems to protect OEBB/PEBB of retro terminations
• Do we hire extra staff to communicate these changes to subscribers
• PEBB Opt Out• PEBB will have to identify an Opt Out that qualifies for the $233
incentive from a subscriber that Opts Out due to other OEBB/PEBB coverage– New codes in PEBB to transfer to payroll– Possibly create a new non-plan called Non- Incentive Opt Out– Rule change around this plan offering
16

OEBB/PEBB Needs• Potential need for OEBB/PEBB to hire staff to facilitate
communications between OEBB/PEBB members needing to drop one coverage
• System changes will be costly and developing sound new processes will take time and effort to complete
17

Thank You!
18

Kaiser PermanenteNETWORK / ACCESS
PEBB Board PresentationSeptember 18, 2018Attachment 4
Presented by: Dr. Keith Bachman, PEBB Medical Director Sophary Sturdevant, Executive Account Manager

10 hospitals
20 dental facilities
47 medical facilities, including6 The Portland Clinic facilities6 PeaceHealth facilities in
Eugene/Springfield
SERVICE AREA
Page 2
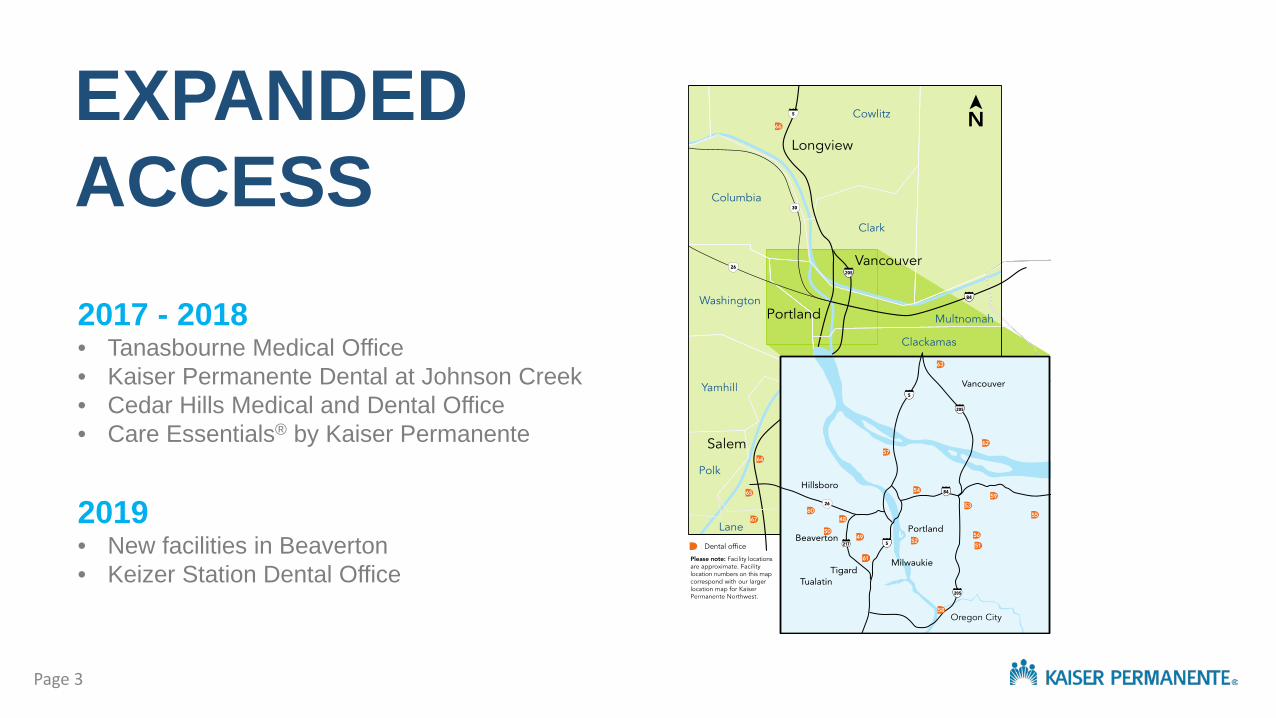
2017 - 2018• Tanasbourne Medical Office • Kaiser Permanente Dental at Johnson Creek• Cedar Hills Medical and Dental Office• Care Essentials® by Kaiser Permanente
2019• New facilities in Beaverton• Keizer Station Dental Office
EXPANDED ACCESS
Page 3

Beaverton Medical and Dental Office• 90,000 SF of integrated Medical/Dental• Public Square• New technology to alleviate wait times and
provide ease of communication• Larger exam rooms that encourage patient-
provider conversation• Patient-centered design and technology
NEW BEAVERTON FACILITY
Page 4
CARE ESSENTIALS
Care Essentials Clinics:• Treat non-emergency health care needs, including minor illnesses and injuries • Provide preventive services, including checkups, vaccinations, and some lab
and diagnostic testing
EasyConvenientNeighborhood-Based
Pearl District
Hawthorne – Open Now!
Page 5

THE PORTLAND CLINICSince 2011 Kaiser Permanente and The Portland Clinic have partnered with the shared goal to improve community health and make care more affordable.• Primary Care plus over 30 specialties • Six locations with a seventh opening soon• Members can utilize services with ease at Kaiser Permanente or The Portland Clinic
Page 6
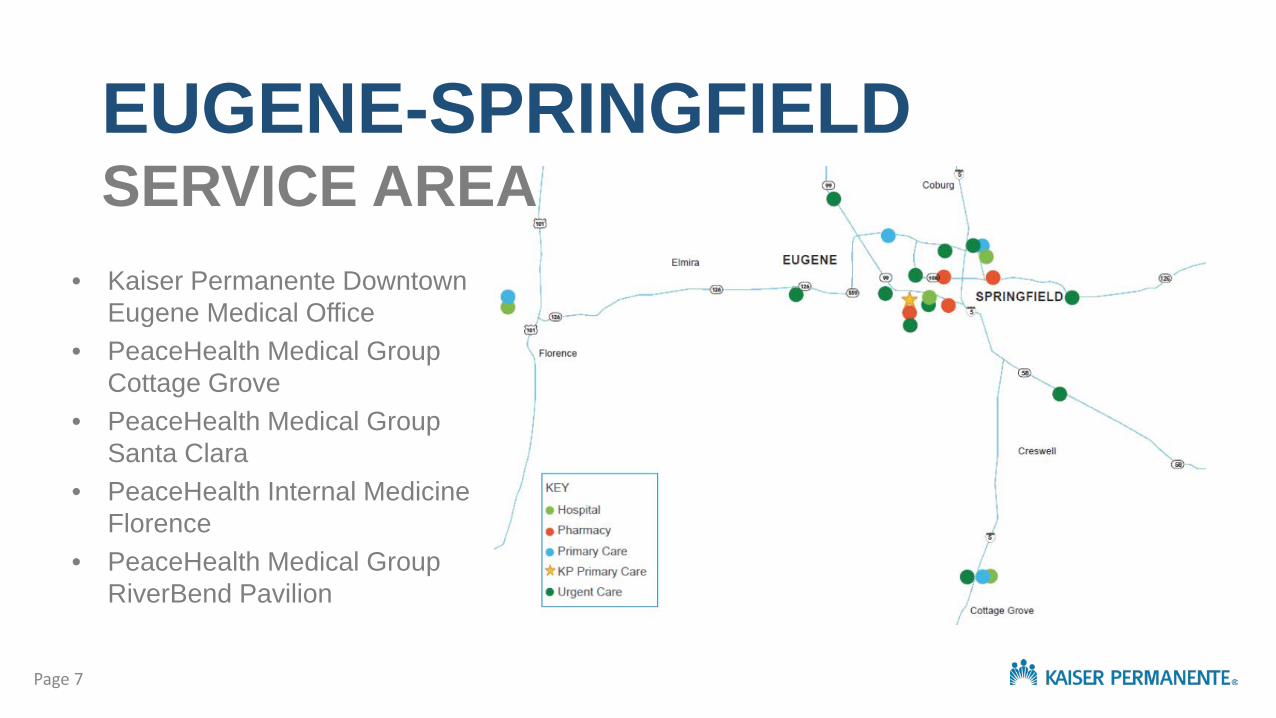
• Kaiser Permanente Downtown Eugene Medical Office
• PeaceHealth Medical Group Cottage Grove
• PeaceHealth Medical Group Santa Clara
• PeaceHealth Internal Medicine Florence
• PeaceHealth Medical Group RiverBend Pavilion
EUGENE-SPRINGFIELDSERVICE AREA
Page 7
Provider Stats• 1,255 NW Physicians • Average tenure of NW Physicians is 8 yrs.• 176 new physicians hired in 3 years
KP Specialty Care• Integrated model allows for coordinated
care among PCP and Specialty Care• Kaiser Permanente has over 60 specialty
care departments in house
Partner Hospitals• OHSU• Doernbecher• Legacy Salmon Creek Medical Center• Salem Hospital• PeaceHealth
• 38 Hospitals• 19,000+ Physicians• 651 Medical Offices• 1 Medical School (opening in 2019)
Care and Expertise Beyond the NW
Page 8

CARE WHEN AND WHERE YOU WANT IT
ADVICE NURSE SECURE EMAIL PHONE APPOINTMENTS VIDEO VISITS
Page 9

TELEHEALTH STATISTICS
Page 10

PEBB VIRTUAL ACCESS2017 Data
Services Office Visits Telephone Appointments
Coded Unscheduled
CallsVideo Visits
Virtual Dermatology
Assist% Virtual
Continuing Care 93 19 96 2 0 56%Mental Health/ADDM 7,834 1,288 977 116 0 23%Peds Sub Specialty 377 97 19 5 0 24%Primary Care 43,366 8,005 1,012 204 0 18%Specialty Care 33,797 3,122 757 337 714 13%TRC 0 0 601 0 0 100%Total 85,467 12,531 3,462 664 714 17%
Services Email Threads Individual Emails
Continuing Care 50 155Mental Health/ADDM 4,090 9,362Peds Sub Specialty 395 852Primary Care 29,450 60,844Specialty Care 16,725 32,918Total 50,710 104,131
Page 11

Thank you!

PEBB Synergy/Summit Network OverviewSeptember 18, 2018
1
Dr. Jim Rickards, Senior Medical DirectorJill Harland, Director Provider Relations
Attachment 4a
• Focus on Primary Care & PCPCH Model
• Network Access
• Telemedicine
Presentation Overview
2

Primary Care & PCPCH Model

Synergy - Organized System of CareNetwork Management Primary Care Support
Per member per month payments to recognized Medical Homes based on tier
Population Based payments
Coordinated care model promoting regional collaboration
Regional Risk Model
Primary care providers incentivized for meeting quality metrics
Performance Based payments
Statewide payer alignmentCPC+ program
• Hospital• Primary Care• Specialty Care• Pharmacy
Risk Areas
4

Synergy background
Developed in collaboration with major health system providers in 2014
Modeled on the CCO concept of regional risk models & provider collaboration
More than 9,000 primary care and specialty care providers
Promotes Oregon’s Patient Centered Primary Care home program through care management
5

Provider risk model overview
Premium-based allocation model
Expected costs used to develop the premium are the budget
Actual costs are compared to expected costs at a regional level
If actual costs are less than expected costs, the model generates a surplus that is shared with providers
If actual costs are higher than expected costs, the model is in deficit
Providers at risk for their share of the deficit
6

Network Access – Focus on Primary Care
CPC+ - Comprehensive Primary Care + Program
PCPCH - Patient Centered Primary Care Home
SB934 – Primary Care Payment Reform Workgroup
7

Support a PCPCH focus in the following domains:
Network Design –Migrate to a PCPCH focused network
Payment Strategy – Align PCPCH Value Based Contracting with SB934 & Purchaser Performance Guarantees
Benefit Design – Incentivize members for PCPCH participation
Member Tools – Engage & educate members to PCPCH value
Delivery System Partnership – Member outreach plan to connect members with PCPs, if needed
PCPCH Support
8
For all networks, Moda is implementing a payment model with four key components:
• Advanced Primary Care Infrastructure - (Per-member, per-month [PMPM] payments) - Risk stratified care management, care coordination, behavioral health integration, integrated pharmacist, and non-visit-based care
• Performance-based Incentive payments – Measure performance
• Fee-for-service payments – Value added services eg. mental health
Primary Care Payment Reform
9

Network Access

Synergy and Summit Network Service Area
11

• Total Number of PCPs: 4,350
• Total Number of High Volume/High Impact Specialists: 2,185− High Volume specialties
◦ Cardiology◦ Dermatology◦ OB/GYN◦ Orthopedics◦ Radiology
− High Impact specialties◦ Endocrinology◦ Gastroenterology◦ Oncology◦ Rheumatology
Synergy/Summit Network Access
12

PEBB Membership by CountyCurrent as of August 2018
Total PEBB Membership: 10,42213
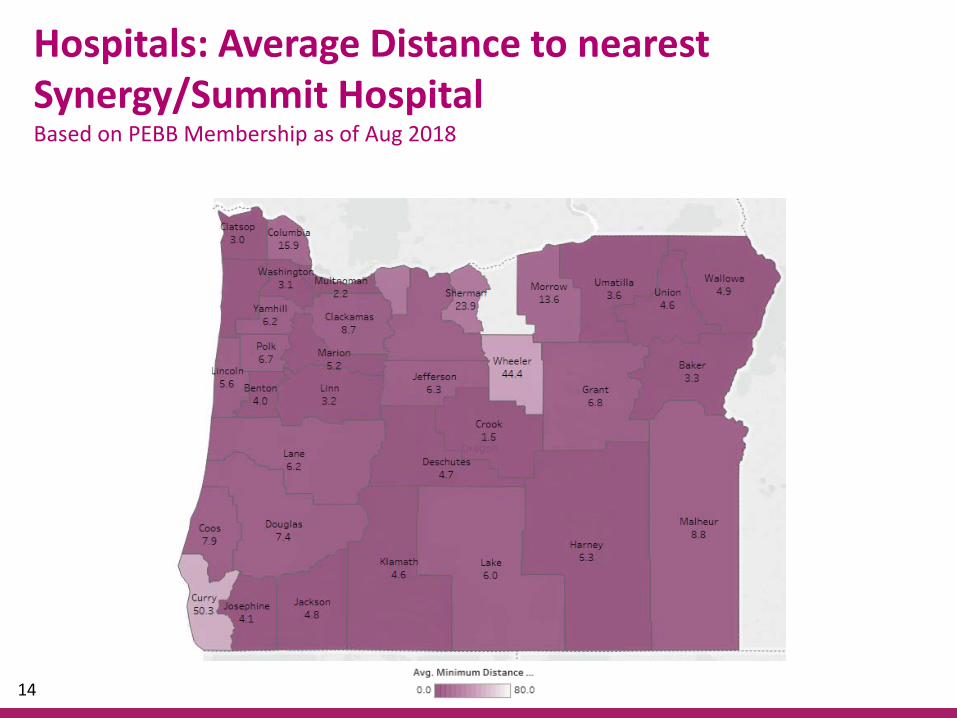
Hospitals: Average Distance to nearest Synergy/Summit HospitalBased on PEBB Membership as of Aug 2018
14
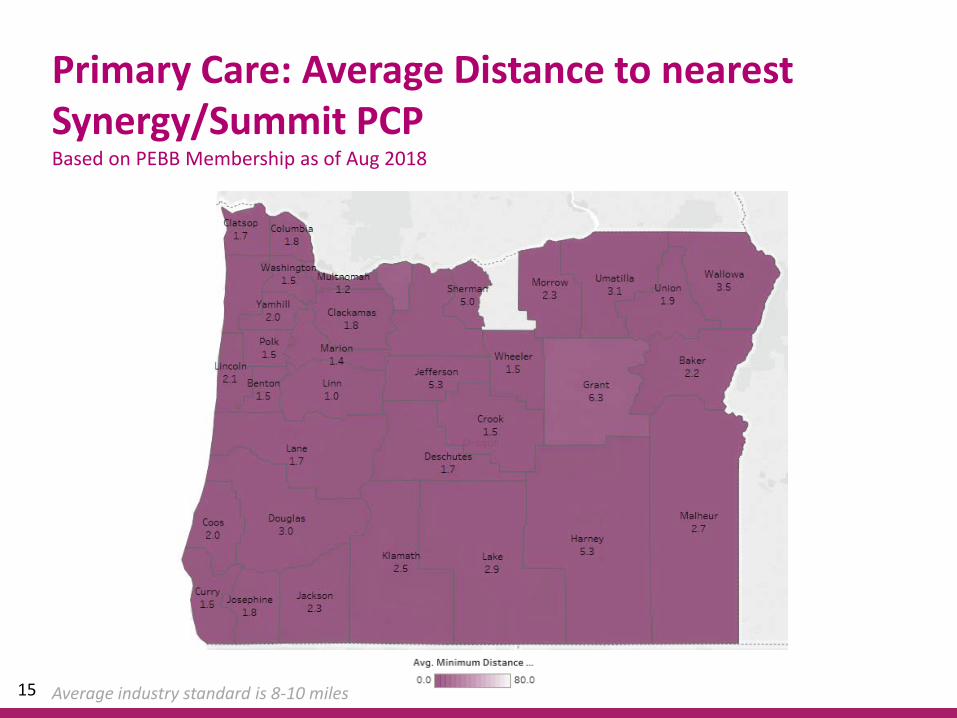
Primary Care: Average Distance to nearest Synergy/Summit PCPBased on PEBB Membership as of Aug 2018
Average industry standard is 8-10 miles15

• Areas where challenges exist due to the rural nature of the county:
− Dermatology: Harney County− Endocrinology: Lake County− Gastroenterology: Grant, Lake
and Harney Counties
• There are currently no providers available to recruit in these areas to increase access
Specialty Care: Average Distance to nearest Synergy/Summit High Volume or High Impact SpecialistBased on PEBB Membership as of Aug 2018
16

• OHSU Specialty Care− High Volume/High Impact Specialists:
◦ Cardiology: 71◦ Dermatology: 30◦ Endocrinology: 30◦ Gastroenterology: 36◦ OB/GYN: 39◦ Oncology: 105◦ Orthopedics: 27◦ Radiology: 55◦ Rheumatology: 11
− Other specialists: 1,389
Synergy/Summit Network in the Portland Metro
17

• Includes the state’s two premier Pediatric Hospitals –Doernbecher and Randall’s
Synergy/Summit Network in the Portland Metro
Pediatric Services Offered Doernbecher at OHSU Randall's at LegacyAllergy x xBurn xCardiology x xChild Abuse x xCraniofacial xCritical Care x xDermatology x xDevelopment x xEar, Nose & Throat x xEndocrincology x xEye Care x xGastroenterology x xGenetics & Birth Defects xHematology Oncology x xInfectious Diseases x xMetabolism xNeonatology x xNephrology x xNeurology x xOrthopedics x xPain Management xPhysical Therapy x xPschiatry x xPulmonology x xRheumatology xSleep Medicine x xSurgery x xUrology x
18

• Synergy/Summit − Total BH Practitioners: 4,007 (17.0% growth since 2016)− Total Clinics: 2,371− Total Chemical Dependency Facilities: 180− Total Inpatient Psychiatric Facilities : 21
• Behavioral Health providers include− Psychiatrists, Licensed Professional Counselors, Licensed Marriage &
Family Therapists, Licensed Clinical Social Workers, and Mental Health Counselors
• Annual recruitment outreach based on PEBB member utilization− This year we are targeting 202 providers/clinics statewide
Behavioral Health Network
19

Telemedicine

• A telehealth solution bringing behavioral health providers to areas with limited access by means of real time interaction
• Available to PEBB members statewide
• If you are a member and are experiencing limited access to a behavioral healthcare provider that can treat your condition, you can call Moda Health and ask to speak to a Behavioral Health Care Coordinator, and we will tell you about Forefront Telecare. Our Behavioral Health Care team will then send your information to Forefront, where they will connect you with a credentialed Behavioral Health provider via webcam in either your PCPs office or in the comfort of your own home
• Forefront TeleCare became available to PEBB members on 8/10/18.
Forefront TeleCare
21

22
Sample communications that we have shared with our groups
Moda-OHSU Virtual Visits partnership


© 2018 Private & Confidential
PEBB Board PresentationPHP Network Access and Availability
Attachment 4bPEBB Board - September 18, 2018

© 2018 Private & Confidential 2
Choice Medical Homes
2006 2007 2008 2009 2010 2011 2012 2013 2014 2015 2016 2017 2018Total 24 25 29 33 51 106 109 150 188 227 266 291 330
0
50
100
150
200
250
300
350
Num
ber o
f Med
ical
Hom
es
© 2018 Private & Confidential 3
PEBB Statewide PPO
Full access to the national Providence Signature Network and non-network providers
In network providers across the U.S. through our national network
Enrolled subscribers*19,503
Enrolled members*52,558
*as of 09/07/18

© 2018 Private & Confidential 4
Total Number of Hospitals: 58
Total Number of PCPs: 3,127At 5,528 Locations
Total Number Specialists: 11,581At 24,057 Locations
Signature Network Access (Statewide)
PCPCH Clinics included in Signature

© 2018 Private & Confidential 5
PEBB Providence Choice
Collaborative medical home model emphasizing patient-centered primary care
Available in most Oregon counties
Enrolled subscribers*18,989
Enrolled members*48,979
*as of 09/07/18

© 2018 Private & Confidential 6
Total Number of Hospitals: 35
Total Number of PCPs: 2289At 4286 Locations
Total Number of Specialists: 11451At 19709 Locations
PEBB Choice Network Access
© 2018 Private & Confidential 7
PCPCH Clinics
Total PCPCH: 655
PCPCH In Network: 497
PCPCH not In Network: 158• Over 100 in Portland Metro area with 91 within 5 provider organizations • Cannot meet credentialing or PCP criteria• Indian Health Services, School Based Clinic• Not interested in being a medical home in the network• Other
76% of all PCPCH Clinics are in Network
53 Medical Homes are Providence Clinics

© 2018 Private & Confidential
Thank you!

H E A LT H W E A LT H C A R E E R
SEPTEMBER 18, 2018
O R E G O N P E B B S T R A T E G I C P L A N N I N G P A R T I I D I S C U S S I O N G U I D E
Attachment 3

2 Copyright © 2018 Mercer (US) Inc. All rights reserved.
A G E N D A & O B J E C T I V E S
WHERE WE LEFT OFF 1
STRATEGY FOR ACTION—DELIVERY
AND ASSOCIATED PAYMENTS
2
NEXT STEPS 4
A G E N D A O B J E C T I V E S
Y O U R S T R A T E G Y
F O R A C T I O N
• Setting ground on where we
left off, and where PEBB has
been
• Start developing a strategic
plan to support PEBB’s vision
• Explore priority areas for
future consideration
• Agree on timing and next
steps
CARE TRANSFORMATION AND
ALTERNATIVE PAYMENT MODELS
3

3 Copyright © 2018 Mercer (US) Inc. All rights reserved.
WHERE WE LEFT OFF

4 Copyright © 2018 Mercer (US) Inc. All rights reserved.
W H E R E W E L E F T O F F
W H AT W E H E A R D
• What strategies has PEBB tried and what are the results? • Minimal care transformation, mostly vendor driver, and mostly related to
benefit plan design changes
What have we done?
• Multiple stakeholders have responsibility: local communities, legislature, health plans, providers, members, the board
Who is responsible?
• Consider multiple segmented strategies with staged timeframes (this will be a multi-year process, not a quick fix)
• Include a specific rural strategy
• Drive what the innovations workgroup will address
How should we approach strategy?
• Focus on payment reform, including alternative payment models
• Social determinants of health
• Expert medical opinion to improve outcomes
Are there specific actions of interest?
• Wellness subcommittee
• CCO 2.0 - How can PEBB utilize this transformation?
• Potential board retreat in November
What is on the calendar?

5 Copyright © 2018 Mercer (US) Inc. All rights reserved.
W H E R E W E L E F T O F F
W H E R E TO TA R G E T ?
PROVIDERS — To adhere to evidence-based clinical guidelines, improve quality, and enhance
the patient experience
R E S P O N S I B I L I T Y F O R E N S U R I N G P L A N M E M B E R S
R E C E I V E H I G H Q U A L I T Y C A R E I S S H A R E D
PEBB — To select health plans and provider networks with the highest quality standards
and optimal plan design
CARE MANAGERS — To navigate patients across the care continuum to the right providers
at the right time
HEALTH PLANS — To manage high quality provider networks, improve the member experience,
and promote transparency
PLAN MEMBERS — To be informed, self-manage whenever possible, and seek the best care
COMMUNITY — To provide leadership via legislative and local initiatives to shape health care
6 Copyright © 2018 Mercer (US) Inc. All rights reserved.
W H E R E W E L E F T O F F
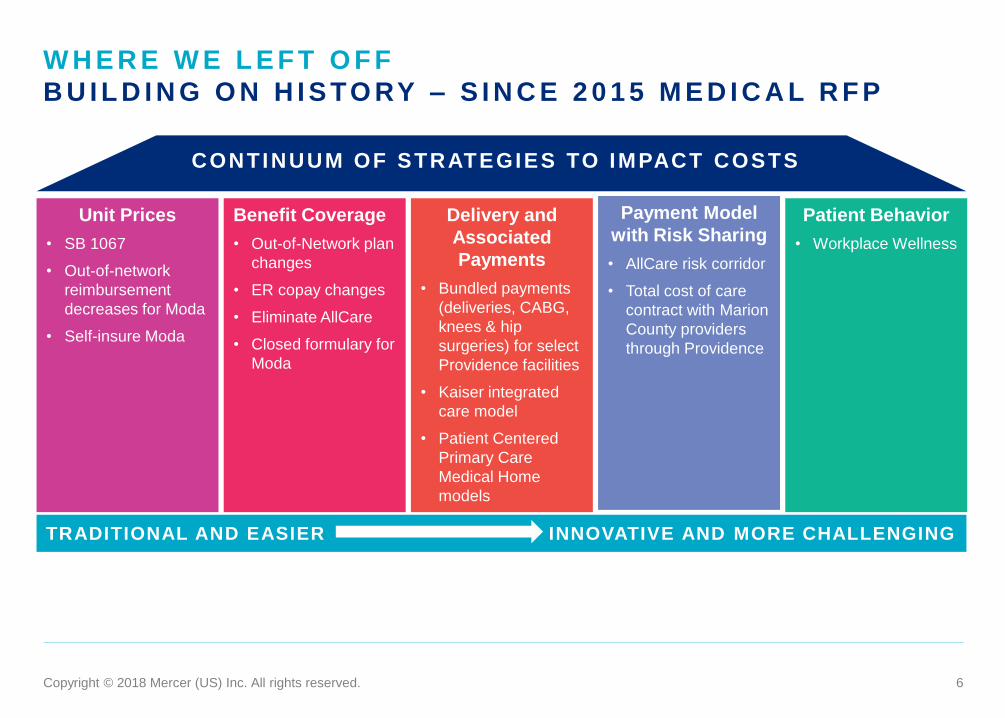
B U I L D I N G O N H I S TO RY – S I N C E 2 0 1 5 M E D I C A L R F P
Unit Prices
• SB 1067
• Out-of-network
reimbursement
decreases for Moda
• Self-insure Moda
Benefit Coverage
• Out-of-Network plan
changes
• ER copay changes
• Eliminate AllCare
• Closed formulary for
Moda
Delivery and
Associated
Payments
• Bundled payments
(deliveries, CABG,
knees & hip
surgeries) for select
Providence facilities
• Kaiser integrated
care model
• Patient Centered
Primary Care
Medical Home
models
Patient Behavior
• Workplace Wellness
CONTINUUM OF STRATEGIES TO IMPACT COSTS
TRADITIONAL AND EASIER INNOVATIVE AND MORE CHALLENGING
Payment Model
with Risk Sharing
• AllCare risk corridor
• Total cost of care
contract with Marion
County providers
through Providence

7 Copyright © 2018 Mercer (US) Inc. All rights reserved.
Short term solutions do not adequately address long standing
issues with medical costs and member outcomes 1
Developing a strategic plan aligned with PEBB’s
vision is critical 2
Agreeing on timing and next steps for priorities, vetting of
solutions, and follow up discussions 4
Need to identify and address the barriers to deciding,
adopting and implementing new programs 5
Creating a path with specific, measurable initiatives can
improve focus 3
W H E R E W E L E F T O F F
C A L L TO A C T I O N
How can we help the Board move forward? 6

8 Copyright © 2018 Mercer (US) Inc. All rights reserved.
STRATEGY FOR ACTION
– STRATEGIC PLAN

9 Copyright © 2018 Mercer (US) Inc. All rights reserved.
S T R AT E G Y F O R A C T I O N
E X P L O R I N G T H E P O S S I B I L I T I E S
Unit Prices
• Directly negotiate
rural fee schedule
prices
• Contract with efficient
CCMs by county
• Reference based
pricing
• Exclusive specialty
drug vendor
• High cost claim
management
Benefit Coverage
• RFP for medical plans
• Advocacy care
management
• Stricter medical and
benefit policies
• Adjust plan values to
benchmark
• Risk adjust premiums
for contributions
• Point solutions
Delivery and
Associated
Payments
• Bundled payments
• Centers of Excellence
• Health alliance to
influence how
providers operate
• Better integration of
behavioral health and
EAP with medical
• Single electronic
health record provider
Patient Behavior
• Concierge vendor
Statewide Plan
• Transparency tool
• Require use of shared
decision support tool
• Single telemedicine
solution
• Consumer directed
medical plan
• Expert medical
opinion vendor
• Address social
determinants of health
CONTINUUM OF STRATEGIES TO IMPACT COSTS
TRADITIONAL AND EASIER INNOVATIVE AND MORE CHALLENGING
Payment Model
with Risk Sharing
• Upside and downside
risk
• Create ACO
• Changing in-network
to only include risk
bearing providers
PEBB’s focus has historically been on
these four categories
Changing patient behavior can be challenging, and
a possible area of focus for long-term strategy
10 Copyright © 2018 Mercer (US) Inc. All rights reserved.
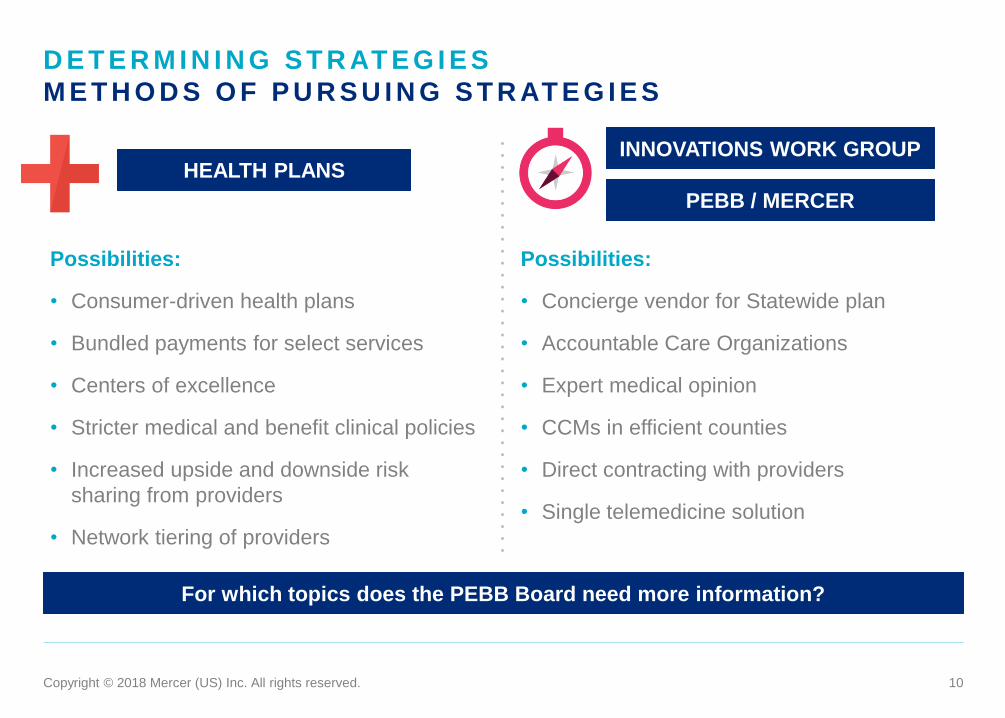
D E T E R M I N I N G S T R AT E G I E S
M E T H O D S O F P U R S U I N G S T R AT E G I E S
Possibilities:
• Consumer-driven health plans
• Bundled payments for select services
• Centers of excellence
• Stricter medical and benefit clinical policies
• Increased upside and downside risk
sharing from providers
• Network tiering of providers
Possibilities:
• Concierge vendor for Statewide plan
• Accountable Care Organizations
• Expert medical opinion
• CCMs in efficient counties
• Direct contracting with providers
• Single telemedicine solution
HEALTH PLANS INNOVATIONS WORK GROUP
PEBB / MERCER
For which topics does the PEBB Board need more information?

11 Copyright © 2018 Mercer (US) Inc. All rights reserved.
I L L U S T R AT I V E R O A D M A P
SHORT TERM MEDIUM TERM LONG TERM
• Introduce concierge vendor for
Statewide PPO
• Implement expert medical opinion
vendor to provide second
opinions for non-urgent care for
members while helping to select
high quality providers
• Introduce HSA-qualified
consumer directed health plan(s)
• Restrict counties where CCM
plans are offered to those with
demonstrated efficiencies and
improved outcomes
• Select and implement bundled
payments for high volume
services with high variance in
costs. Enhance travel benefit or
in conjunction with Centers of
Excellence
• Investigate areas of misuse or
overuse and work with providers
to address issues
• Evolve CCM to ACO model with a
closed network of coordinated
providers with lower
reimbursement, risk sharing, and
performance guarantees based
on quality metrics and trend
• Address social determinants of
health for holistic approach
towards healthcare
• Form health alliance of employers
and government entities to
reshape how healthcare is
delivered

12 Copyright © 2018 Mercer (US) Inc. All rights reserved.
S T R AT E G Y F O R A C T I O N
I L L U S T R AT I V E S AV I N G S
2020 2021 2022 2023
Needed Savings $3 Million $36 Million $72 Million $111 Million
Savings Opportunities
• Concierge for Statewide $5 Million $11 Million $17 Million $23 Million
• Expert Medical Opinion $2 Million $3 Million $5 Million $7 Million
• HSA Plan $3 Million $7 Million $10 Million $14 Million
• Double Spousal Surcharge $3 Million $5 Million $8 Million
• CCMs In Efficient Counties $1 Million $2 Million $3 Million
• Bundled Payments $2 Million $4 Million $6 Million
• Accountable Care Organization $6 Million $12 Million
Total Savings $9 Million $27 Million $49 Million $73 Million
Remaining Gap None $9 Million $23 Million $38 Million
Annual savings from members selecting CCM plans has historically been between $4M and $7M

13 Copyright © 2018 Mercer (US) Inc. All rights reserved.
CARE TRANSFORMATION
AND ALTERNATIVE
PAYMENT MODELS

14 Copyright © 2018 Mercer (US) Inc. All rights reserved.
A LT E R N AT I V E PAY M E N T M O D E L S
• Fee for service with no link to quality and value
Category 1
• Fee for service linked to quality and value
‒ Foundational payments for infrastructure & operations (e.g. care coordination, Health Information Technology investments)
‒ Pay for reporting
‒ Pay for Performance (bonuses for quality)
Category 2
• Alternative payment models built on fee-for-service
‒ Shared savings (upside risk only)
‒ Shared savings (episode-based payments and upside and downside risk)
Category 3
• Population-based payments
‒ Condition-specific (e.g. payments for specialty services, such as oncology or mental health)
‒ Comprehensive population-based payments (global budget or percent of premium)
‒ Integrated finance & delivery (global budget or percent of premium in integrated systems)
Category 4

15 Copyright © 2018 Mercer (US) Inc. All rights reserved.
A LT E R N AT I V E PAY M E N T M O D E L S
R B P, C O E , A N D B U N D L E D PAY M E N T S
Centers of Excellence
• Expertise and facilities for a specific medical condition
• Provides services in a comprehensive fashion
• Selected due to a high level of quality
• Potential COEs (2017 Allowed Cost)
• Deliveries - $24 Million
• Knee and Hip replacement - $15 Million
• Spinal Fusion - $6 Million
• Circulatory System - $21 Million
Bundled Payment
• A set of services to treat a condition or perform a procedure
• Expected total costs for a clinically defined episode of services
• Potentially improves quality and outcomes
• Best practices include shared decision support
• Typically included improvements
• Lower out-of-pocket costs for members
• Transportation and accommodations (with COE)
• Warranties for specified complications
• Shared decision making support
Reference Based Payment
• Maximum allowed price for a condition or procedure
• Set for a clinically defined set of services
• Charges above the reference price are paid for by the member
• In 2016, Montana set pricing for all hospital services at 234% of Medicare
• All but one hospital agreed to reduce allowed fees to the reference price
• Estimated 2018 savings of $15 million.
16 Copyright © 2018 Mercer (US) Inc. All rights reserved.
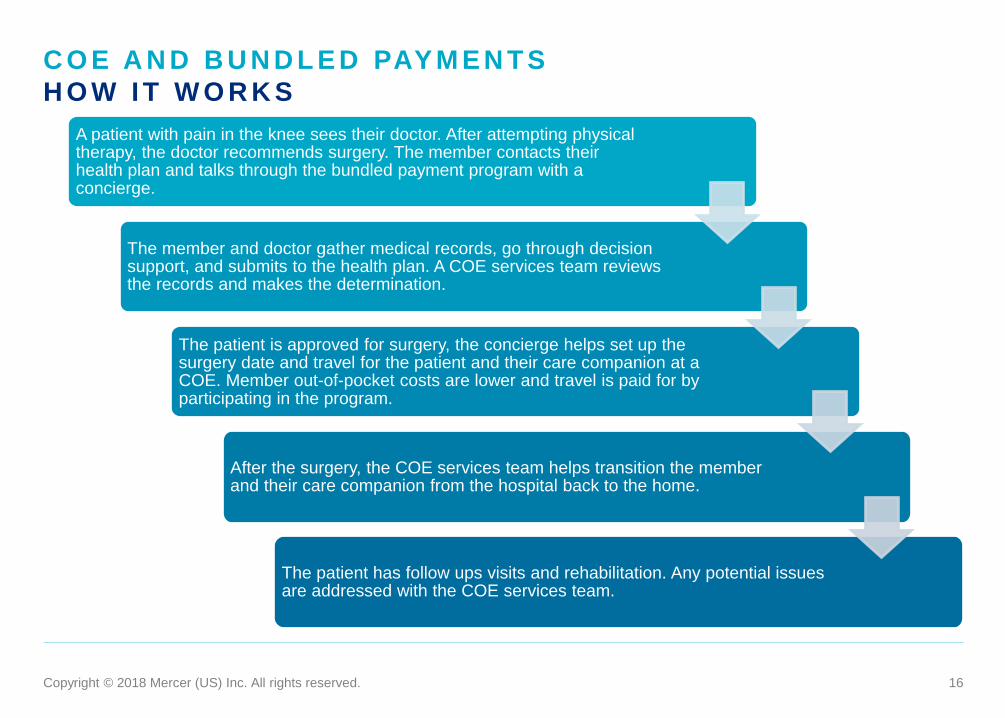
C O E A N D B U N D L E D PAY M E N T S
H O W I T W O R K S
A patient with pain in the knee sees their doctor. After attempting physical therapy, the doctor recommends surgery. The member contacts their health plan and talks through the bundled payment program with a concierge.
The member and doctor gather medical records, go through decision support, and submits to the health plan. A COE services team reviews the records and makes the determination.
The patient is approved for surgery, the concierge helps set up the surgery date and travel for the patient and their care companion at a COE. Member out-of-pocket costs are lower and travel is paid for by participating in the program.
After the surgery, the COE services team helps transition the member and their care companion from the hospital back to the home.
The patient has follow ups visits and rehabilitation. Any potential issues are addressed with the COE services team.

17 Copyright © 2018 Mercer (US) Inc. All rights reserved.
C O M PA R I N G C C M S TO A C O S
• Health care providers contracted through
Providence and Moda
• Members select a medical home (typically a
tiered Patient-Centered Primary Care Home)
• Services can be obtained outside the contracted
network at a decreased benefit level
• Plans support data sharing with providers
• Hospital and physician systems, while contracted,
are often financially separate
• Moda determines risk sharing with providers by
region based on expected versus actual cost;
primary care providers have upside risk for their
attributed members, while specialists and
hospitals have upside and downside risk
• Bonuses are available for meeting quality goals
• Providence in Salem has a total cost of care
agreement with providers and facilities with a
3.4% total cost of care trend guarantee
• Health care providers who offering services across
the continuum who agree to share responsibility
for the quality, cost, member experience and
engagement
• Members primarily receive care within the ACO
• Entire organization of providers assume risks for
meeting financial and performance (quality and
satisfaction) benchmarks with upside and
downside risk sharing
• Electronic medical records, claims data, and
reporting is shared among all providers to increase
the coordination between providers
• Focus is patient centered, to improved customer
service and create higher patient satisfaction
• ACOs must meet quality and member experience
and engagement scores to qualify for bonus
payments
OREGON PEBB COORDINATED
CARE PLANS
ACCOUNTABLE CARE ORGANIZATIONS
(ACO) – IDEAL STATE
18 Copyright © 2018 Mercer (US) Inc. All rights reserved.
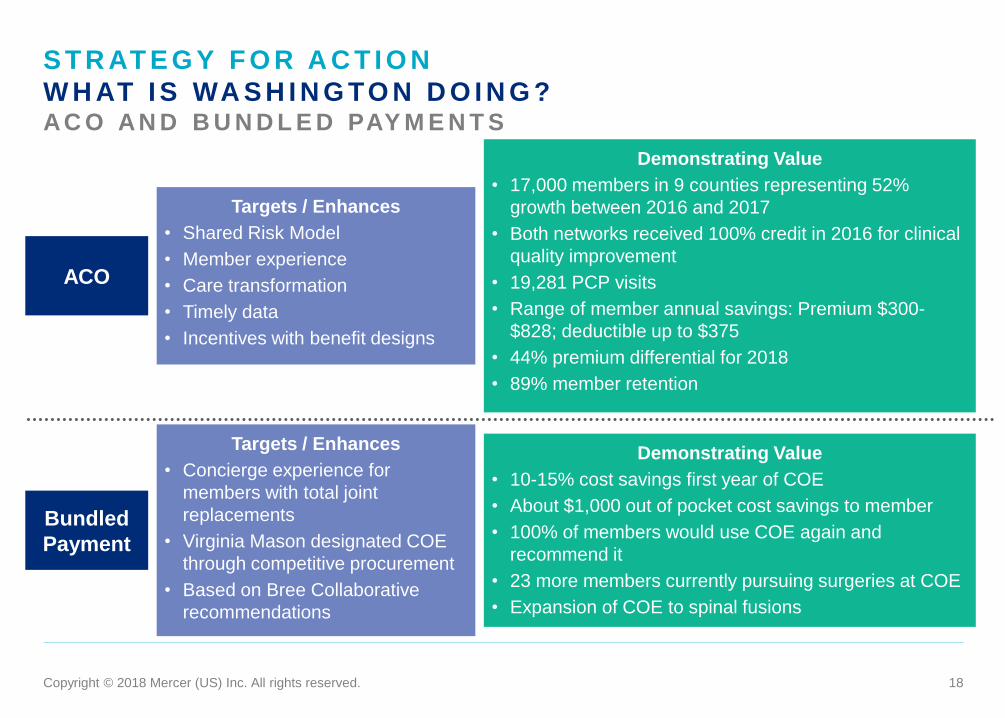
S T R AT E G Y F O R A C T I O N
W H AT I S WA S H I N G TO N D O I N G ? AC O AN D B U N D L E D PAY M E N T S
ACO
Bundled
Payment
Targets / Enhances
• Shared Risk Model
• Member experience
• Care transformation
• Timely data
• Incentives with benefit designs
Demonstrating Value
• 17,000 members in 9 counties representing 52%
growth between 2016 and 2017
• Both networks received 100% credit in 2016 for clinical
quality improvement
• 19,281 PCP visits
• Range of member annual savings: Premium $300-
$828; deductible up to $375
• 44% premium differential for 2018
• 89% member retention
Targets / Enhances
• Concierge experience for
members with total joint
replacements
• Virginia Mason designated COE
through competitive procurement
• Based on Bree Collaborative
recommendations
Demonstrating Value
• 10-15% cost savings first year of COE
• About $1,000 out of pocket cost savings to member
• 100% of members would use COE again and
recommend it
• 23 more members currently pursuing surgeries at COE
• Expansion of COE to spinal fusions

19 Copyright © 2018 Mercer (US) Inc. All rights reserved.
S T R AT E G Y F O R A C T I O N
R U R A L PAY M E N T S T R AT E G Y
Vermont ACO
Model
Washington
State
• Limits per capita health care growth to 3.5% annually
• Focuses on outcomes and quality, specifically on access to care, substance abuse
disorder, suicides, and chronic conditions
Pennsylvania
• Prospectively sets global budget for participating rural hospitals, based on historical
revenue
• Rural hospitals will redesign delivery of care to improve quality and meet health needs
of local communities
• Patient centered solutions to reward rural providers for value of care and incent based
on improved outcomes
• Address access and sustainability concerns along with community needs
• Integrated delivery systems and redefine primary care for rural populations
• Ensure that members are engaged with local health delivery systems
• Create payments based on total cost of care with encounter-based payments

20 Copyright © 2018 Mercer (US) Inc. All rights reserved.
NEXT STEPS

21 Copyright © 2018 Mercer (US) Inc. All rights reserved.
B O A R D C O N S I D E R AT I O N S
Work with PEBB to determine which items need to procured and in what methods
Distinguish PEBB-led strategies from Innovations Workgroup strategies
Determine acceptable level of member impact/disruption to drive savings
Determine level of cooperation and involvement in strategy setting between PEBB, OEBB, and Innovations Workgroup
Work with carriers to gain commitment to taking an active role in finding solutions to the challenges facing PEBB
Narrow list of considerations to get PEBB closer to the savings needed

22 Copyright © 2018 Mercer (US) Inc. All rights reserved.
APPENDIX

23 Copyright © 2018 Mercer (US) Inc. All rights reserved.
S T R AT E G Y F O R A C T I O N
U N I T P R I C E S ACTION POTENTIAL STEPS POTENTIAL BARRIERS SAVINGS TIMEFRAME
Addressing
Provider
Reimbursements
Direct negotiations with rural area
providers or creating a narrower
network with mandated
reimbursement levels and annual
increases
Maintaining adequate access,
ensuring quality providers,
disruption to members
$ Medium
Addressing
Provider
Reimbursements
Restricting counties where CCM
plans are offered to those with
demonstrated efficiencies and
improved outcomes
Member noise, shifting members
into the unmanaged Statewide
PPO plan
$$ Medium
Referenced
Based Pricing
Determining high volume services
with large regional cost variations,
e.g. knee and hip surgeries,
colonoscopies
Provider acceptance, travel
benefits, member
communications and usage,
coordination of care and referrals
with PCPs
$ Medium
Pharmacy
Contracting
Contract with one pharmacy vendor
for all self-insured plans
Impact on contracting with
current vendors
$ Medium
Specialty Drug
Management
Carving out all specialty drug
coverage to a specialized vendor,
preemptive specialty drug
contracting, direct contracting with
infusion centers
Contractual agreements with
vendors, care integration, direct
contracting with facilities, impact
on members including travel
$$ Medium
High Cost Claim
Management
Add clinical oversight /surveillance
services for self-funded plans
Cooperation from vendors $ Short

24 Copyright © 2018 Mercer (US) Inc. All rights reserved.
S T R AT E G Y F O R A C T I O N
B E N E F I T C O V E R A G E ACTION POTENTIAL STEPS POTENTIAL BARRIERS SAVINGS TIMEFRAME
Request for
Proposal or
Information
Conduct a marketing exercise of
medical plan vendors
Timing and expense of new
marketing
$-$$ Medium
Concierge vendor
for Statewide
PPO
Adjusting plan design to add third
network where members receive
the highest level of benefit when
receiving care through a concierge
care management vendor.
Communication with members,
member noise, contractual
agreements with Providence
$$ Short
Stricter medical
and benefit
policies
Audit for deficiencies, identify areas
for stricter utilization controls, and
implement best practices care
management.
Communication with members,
member noise, provider
acceptance due to administrative
burden
$ Short
Benchmarking Adjust benefit design based on
comparison with a representative
group of companies, unions, and
governments.
Member impact $$ Medium
Risk Adjust
Premiums
Incent members to select more
efficient plans by normalizing plan
premiums to an average PEBB
member with risk adjustment.
Member noise, shifting members
into most efficient plans creates
communication challenges
$ Short
Point Solutions Review and implement third party
vendors for key conditions to
provide targeted solutions for higher
cost PEBB members
Integration with current plans
may be an issue, integration and
coordination challenges
$-$$ Short

25 Copyright © 2018 Mercer (US) Inc. All rights reserved.
S T R AT E G Y F O R A C T I O N
C A R E D E L I V E RY A N D A S S O C I AT E D PAY M E N T S ACTION POTENTIAL STEPS POTENTIAL BARRIERS SAVINGS TIMEFRAME
Bundled
Payments
Select and implement bundled
payments for high volume services
with high variance in costs.
Enhance travel benefit or in
conjunction with Centers of
Excellence
Multiple carrier partners; carrier
contracting and agreements;
member disruption
$-$$ Medium
Centers of
Excellence
Create a network for certain
services around facilities with high
quality metrics and outcomes.
Maybe be in conjunction with APM.
Multiple carrier partners; carrier
contracting and agreements;
member disruption
$-$$ Medium
Oregon Health
Alliance
Create alliance with companies,
purchasers, providers, and hospital
systems to improve quality and cost
by reducing overuse, underuse, and
misuse of health care services
Multiple stakeholders $-$$ Long
Integration of
Physical Health,
Behavioral
Health, and EAP
Improve integration between
medical, behavioral health, and EAP
ensuring provider access and
improved coordination
Behavioral health integration is
still a challenge for providers,
carriers, and vendors
$ Medium
Data from
Electronic Health
Records
Require providers serving PEBB
members to provide clinically
relevant data using a common data
feed for information on improvement
opportunities
Defining the data format, multiple
carrier partners, diverse provider
groups
$$ Long

26 Copyright © 2018 Mercer (US) Inc. All rights reserved.
S T R AT E G Y F O R A C T I O N
PAY M E N T M O D E L W I T H R I S K S H A R I N G ACTION POTENTIAL STEPS POTENTIAL BARRIERS SAVINGS TIMEFRAME
Revisiting
Performance
Guarantees with
Current Vendors
Strengthening performance
guarantees with upside and
downside risk sharing with
outcomes and additional metrics
Carrier contracting; willingness of
providers to “play-ball” and
accept downside risk
$ Medium
Accountable Care
Organization
Work with provider groups and
hospital organizations to create a
closed network of coordinated
providers with lower reimbursement,
risk sharing, and performance
guarantees based on quality metrics
and trend
Carrier contracting and
agreements; member disruption
$$ Long
Changing
Preferred
Network of
Providers
Require the in-network providers to
be high performing health systems
using evidence-based clinical
guidelines, patient experience
metrics, and accepting fees at risk
Carrier contracting and
agreements; member disruption
$$ Medium

27 Copyright © 2018 Mercer (US) Inc. All rights reserved.
S T R AT E G Y F O R A C T I O N
PAT I E N T B E H AV I O R ACTION POTENTIAL STEPS POTENTIAL BARRIERS SAVINGS TIMEFRAME
Transparency
Tool
Implement a cost and quality tool for
members to search for low cost,
high quality providers
Member education,
communication, and usage rate.
Increased usage potentially
when in conjunction with
advocacy program
$ Short
Shared Decision
Tools
Require health plans and providers
to incorporate and document the
use of patient decision aids
Multiple carrier partners;
member usage, selection of
tools
$ Medium
Telemedicine Offer PEBB-wide telemedicine
solution
Multiple carrier partners;
member usage
$ Medium
Consumer
Directed Health
Plans
Include a high deductible medical
plan with health savings account to
incent consumerism in members
and potential tax savings
Incenting members to select
consumer directed health plans
with current contribution
structure, member education
and communication
$$$ Short
Expert Medical
Opinion
Implement third party vendor to
provide second opinions on care for
members or help in selecting high
quality providers
Member usage, integration with
health plans and providers
$ Short
Social
Determinants of
Health
Identify environmental factors
impacting members’ health and
implement actions to address those
factors
Segmenting population and
determining factors to address,
cost and scope of actions to
address factors
$$ Long

28 Copyright © 2018 Mercer (US) Inc. All rights reserved.