Katharine D. Wenstrom, MD Director of Maternal-Fetal Medicine Women and Infants Hospital of RI...
77
Preventing the First Cesarean Delivery Katharine D. Wenstrom, MD Director of Maternal-Fetal Medicine Women and Infants Hospital of RI Warren Alpert Medical School, Brown University
Katharine D. Wenstrom, MD Director of Maternal-Fetal Medicine Women and Infants Hospital of RI Warren Alpert Medical School, Brown University
Katharine D. Wenstrom, MD Director of Maternal-Fetal Medicine
Women and Infants Hospital of RI Warren Alpert Medical School,
Brown University
Slide 2
I have no conflicts to disclose
Slide 3
Objectives: Describe medical and social factors that contribute
to the high cesarean rate in the US. Discuss current data on the
normal progression of labor. Describe evidence-based management
approaches to preventing the first cesarean. Describe how hospital
polices, practitioner schedules, financial issues, medical legal
concerns, and other factors all influence the management of
labor.
Slide 4
Important Recent Literature Reviews/Guidelines : Preventing the
first cesarean: Summary of a joint SMFM, NICHD, ACOG Workshop.
Spong CY, Berghella V, Wenstrom K, Mercer BM, Saade GR. Obstet
Gynecol 2012; 120:1181-93 Safe Prevention of the Primary Cesarean
Delivery Obstetric Care Concensus by ACOG and SMFM Obstetrics and
Gynecology 2014; 123(3): 693
Slide 5
Source: CDC/NCHS, National Vital Statistics System.
Slide 6
Data from Martin et al.77 ACOG. Safe prevention of primary
cesarean delivery. Am J Obstet Gynecol 2014.
Slide 7
Slide 8
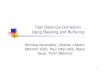
Cesarean Delivery, by Gestational Age: United States, Final
1996-2010 and Preliminary 2011 NOTES: Singletons only. Early
preterm is less than 34 weeks of gestation; late preterm is 34-36
weeks; early term is 37-38 weeks; full term is 39-40 weeks. Access
data table for above at:
http://www.cdc.gov/nchs/data/databriefs/db124_tables.pdf#1.http://www.cdc.gov/nchs/data/databriefs/db124_tables.pdf#1
Source: CDC/NCHS, National Vital Statistics System.
Slide 9
CD, cesarean delivery; VBAC, vaginal birth after cesarean
delivery. *Percent of women who have VBAC; yRate based on total
number of deliveries. Data from National Vital Statistics and from
Martin et al.77 ACOG. Safe prevention of primary cesarean delivery.
Am J Obstet Gynecol 2014.
Slide 10
Repeat Cesarean Rate
Slide 11
Primary cesareans account for 50% of the increasing CS
rate
Slide 12
Neonatal Risk of Adverse Outcomes by Mode of Delivery Vaginal
Cesarean Laceration NA 1.0 2.0 % Resp Morbidity < 1.0 % 1.0 4.0
% Shoulder Dystocia 1.0 2.0 % 0% AJOG 2014; 123: 693-711
Slide 13
Maternal Risk of Adverse Outcomes by Mode of Delivery Vaginal
Cesarean Morbidity and Mortality* 8.6% 9.2% Severe M and M** 0.9%
2.7% Maternal Mortality 3.6:100,000 13.3: 100,000 Amn Fluid
Embolism 3.3-7.7:100,000 15.8: 100,000 3 rd or 4th Laceration 1.0
3.0% NA Placental Abnormalities Increased with cesarean; Risk goes
up with each cesarean Urinary Incontinence No difference Postpartum
Depression No difference AJOG 2014; 123: 693-711 * Cochrane Review
2011, 12 ** CMAJ 2007;176:455
Slide 14
Complications of Subsequent Cesarean Deliveries Compared With
the First Cesarean Delivery Cesarean Placenta Cesarean Delivery
Accreta OR (95% CI) Hysterectomy OR (95% CI) First* 0.2 % 0.7 % 2nd
0.3 % 1.3 (0.72.3) 0.4 % 0.7 (0.40.97) 3rd 0.6 % 2.4 (1.34.3) 0.9%
1.4 (0.92.1) 4th 2.1 % 9.0 (4.816.7) 2.4 % 3.8 (2.46.0) 5th 2.3 %
9.8 (3.825.5) 3.5 % 5.6 (2.711.6) 6 6.7 % 9.8 (11.378.7) 9.0 % 15.2
(6.933.5) Silver et al Obstet Gynecol 2006; 107: 1226
Slide 15
Target Cesarean Rate Healthy People 2020 Low risk, full term,
singleton, vertex: 23.9%* *Healthy People 2010 : 15%
Slide 16
Core Issues Provider practices Induction of labor Diagnosis of
labor arrest Fetal Intolerance of Labor Provider practice
preferences, workload, financial incentives/disincentives Patient
perceptions/education and societal attitudes (Medical-Legal
Issues)
Slide 17
Systems Based Approaches Primary cesarean incidence
HospitalsPayors OB Providers Patients
Slide 18
Consortium on Safe Labor L and D data from 228,668 deliveries
at 23 weeks, at 19 US hospitals, 2002-2008: First delivery in
database selected: 206,969 women Overall CS rate = 30.5% (Nullips =
31.2%) Zhang et al Am J Obstet Gynecol 2010; 203: 326
Slide 19
Non -Obstetric Factors Influencing Cesarean Rate Maternal age
(age < 20 = 21%; age 35 = 42%) Obesity (BMI
Slide 20
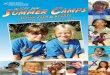
Birth Rates, by Selected Age of Mother: USA, Final 1990-2012
and Preliminary 2013
Slide 21
Trends in Overweight and Obesity Among Adults, United States,
19622010 Overweight Obesity Extreme obesity
Slide 22
Percent of Women with Cesarean Deliveries by BMI: Nulliparas
Deliveries Cesareans(%) TOTAL 57,230 21.8 BMI Category < 25.0
9,113 11.1 25.0 29.9 23,553 17.7 30.0 34.9 14,674 25.1 35.0 39.9
6,045 33.0 40.0 3,845 42.8 Kominiarek et al AJOG, 2010; 203:126
e1
Slide 23
Percent of Women with Cesarean Deliveries, by BMI: Multips,
Prior CS Deliveries Cesareans(%) TOTAL 5,288 37.4 BMI Category <
25.0 523 24.9 25.0 29.9 1,891 32.6 30.0 34.9 1,503 38.8 35.0 39.9
831 43.7 40.0 540 52.8 Kominiarek et al AJOG, 2010; 203:126 e1
Slide 24
Slide 25
Slide 26
Obstetric Factors Influencing the Cesarean Rate Pre-Labor
Cesarean: Previous cesarean (45.1%) Elective* (26.4%)
Malpresentation (17.1%) Intrapartum: FTP or CPD (47.1%)
Nonreassuring fetal status (27.3%) *Declined TOL, AMA, muliparity,
post term, diabetes, chorio, chronic HTN, PROM, HPV, GBS,
polyhydramnios, IUFD, desires TL, social/religious Zhang et al Am J
Obstet Gynecol 2010; 203: 326
Slide 27
Potentially Modifiable Obstetric Indications for the First
Cesarean Diagnostic Effect on Pre-Labor Maternal Indication
Accuracy Preventing CS Preeclampsia High Small Prior shoulder
dystocia Limited Small Prior myomectomy Limited Small Prior
third-degree or 4th-degree High Small laceration, prior breakdown
of repair, fistula Marginal and low-lying High Small
placentation
Slide 28
Potentially Modifiable Maternal Indications for the First
Cesarean Diagnostic Effect on Pre-Labor Maternal Indication
Accuracy Preventing CS Obesity (BMI>30) High Small Infection (
HSV, HCV, HIV) High Small Cardiovascular Disease High Small (HTN
crisis, cardiomyopathy, pulmonary HTN, CVA or aneurysm) Inadequate
Pelvis Limited Small Maternal Request NA Small
Slide 29
Potentially Modifiable Fetal Indications for the First Cesarean
Pre-Labor Diagnostic Effect on Fetal Indication Accuracy Preventing
CS Malpresentation High Large Multiple gestation High Small
Macrosomia Limited Small Malformations Moderate Small (eg NTD,
hydrops)
Malpresentation External Cephalic Version at 36 weeks: Success
Rate 58% (35-86%) Breech Delivery of Second Twin: In experienced
hands: Breech extraction and vaginal delivery of the nonvertex
second twin does not increase morbidity Attempted external cephalic
version is a reasonable alternative Boggess and Chisholm. Obstet
Gynecol Surv, 1997; 52(12):728
Slide 32
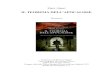
Major Indications for Primary Cesarean Delivery Stage
Indication % In labor First-stage arrest 1530* Second-stage arrest
1025 Failed induction 10 Nonreassuring FHR 10
Slide 33
FIGURE 3 Indications for primary cesarean delivery Data from
Barber et al.16 ACOG. Safe prevention of primary cesarean delivery.
Am J Obstet Gynecol 2014.
Slide 34
Potentially Modifiable Intrapartum Indications for the First
Cesarean Diagnostic Effect on Labor Indication Accuracy Preventing
CS Failed induction Limited Large Arrest of labor Limited Large
Nonreassuring ante- Moderate Large or intrapartum fetal
surveillance
Slide 35
Friedmans Curve
Slide 36
500 Primips at term with complete data: 70% age 20 30 (range
13-42) 67% had gynecoid pelvis 13.8% required pitocin (18% for
induction) 98.2% delivered vaginally Obstet Gynecol 1955; 5:
567
Slide 37
Friedmans Curve Stage Mean (Hours) Latent Phase 8.6 Active
Phase 4.9 First Stage 13.3 Second Stage 0.95 Obstet Gynecol 1955;
5: 567
Slide 38
Consortium on Safe Labor Multicenter retrospective study of
228,668 deliveries 62,415 parturients selected: Term, singleton,
vertex, spontaneous labor, spontaneous vaginal delivery, normal
outcome Zhang et al; Obstet Gynecol 2010; 116(6): 1281
Slide 39
Consortium on Safe Labor
Slide 40
Slide 41
Friedmans Curve
Slide 42
Consortium on Safe Labor Stage Mean 95 th percentile Latent
Phase 6.0 hrs 15.7 hrs First Stage 8.4 hrs 20.4 hrs Zhang et al;
Obstet Gynecol 2010; 116(6): 1281
Slide 43
Friedmans Curve Stage Mean SD* 1 SD* 2 SDs* Latent Phase 8.6
6.0 14.6 20.6 Active Phase 4.9 3.4 8.3 11.7 First Stage 13.3 7.6
20.9 28.5 Second Stage 0.95 0.8 1.75 2.5 *Hours Obstet Gynecol
1955; 5: 567
Slide 44
Friedmans Curve Protracted Latent Phase 27 women has latent
phase > 20 hours; 2 delivered by CS (7%) Failure to Progress
(Inertia) 46 patients had First Stage = 25.2 1.8 hours Second Stage
= 1.6 0.22 hours; 6 delivered by CS (13%) Obstet Gynecol 1955; 5:
567
Slide 45
Friedmans Ideal Curve, Based on 200 Ideal Labors Stage Mean SD*
1 SD* 2 SDs* Latent Phase 7.1 4.0 11.1 15.2 Active Phase 3.4 3.0
6.4 9.4 First Stage 10.6 4.6 15.2 19.8 Second Stage 0.76 0.6 1.4
2.0 *Hours Obstet Gynecol 1955; 5: 567
Slide 46
Consortium on Safe Labor Stage Mean* 95th%* [Friedman 2SD**]
Latent Phase 6.0 15.7 [15.2] First Stage 8.4 20.4 [19.8] * Hours
after admission at 2-2.5 cm ** Ideal Labor Zhang et al; Obstet
Gynecol 2010; 116(6): 1281
Slide 47
Definitions of Failed Induction and Arrest Disorders
First-Stage Arrest 6 cm or greater dilation with membrane rupture
and no cervical change for: 4 h or more of adequate contractions
(eg, 200 Montevideo units) or 6 h or more if contractions
inadequate Obstet Gynecol 2012; 120:1181 AJOG 2014;123(3): 693
Slide 48
Consortium on Safe Labor
Slide 49
Second Stage Duration in Nulliparas Rouse et al: 4,126 women
enrolled in the Pulse Ox trial who reached the second stage: Hours
in Second Stage < 1 hr 1 to < 2 2 to < 3 3 to < 4 4
to
Second Stage Duration Similar findings reported by: Moon et al.
J Reprod Med, 1990; 35(3): 229 Retrospective review of1432 women
with second stage > 2 hours No adverse neonatal outcomes Cheng
et al. AJOG 2004; 191: 933 Retrospective review of 15,759 multips
No adverse neonatal outcomes; maternal morbidity increased after 4
hours
Slide 53
Definitions of Failed Induction and Arrest Disorders
Second-Stage Arrest No progress (descent or rotation) for: 2 h or
more in multiparous women without an epidural 3 h or more in
nulliparous women without an epidural [ 3 h or more in multiparous
women with an epidural ]* [ 4 h or more in nulliparous women with
an epidural ]* Obstet Gynecol 2012; 120:1181* AJOG 2014;123(3):
693
Slide 54
Slide 55
Effect of Delivery Route on Neonatal Injury Delivery Method
Death ICH Other Spont Vag Del 1:5,000 1:1,900 1:216 CS no labor
1:1,250 1:2,040 1:105 CS during labor 1:1,250 1:952 1:71 Vacuum
1:3,333 1:860 1:122 Forceps 1:2,000 1:664 1:76 Towner et al N Engl
J Med 1999;341: 1709
Slide 56
Operative Vaginal Delivery Maternal outcomes: Pelvic floor
injury related to episiotomy, prolonged second stage, large fetus
Pelvic floor dysfunction similar one year after operative vag
delivery versus cesarean for 2 nd Stage Arrest UI rates similar
after 2 deliveries or in older women regardless of CS vs vaginal
Demisse K et al BMJ 2004; 329:24 Seidman DS et al Lancet 1992; 33:
1583 Crane AK. Female Pelvic Med Reconstr Surg 2013;19:13
Slide 57
Consortium on Safe Labor Rate of Labor Induction: 36.2% (All)
43.8% (Women Attempting SVD) Zhang et al; Obstet Gynecol 2010;
116(6): 1281
Slide 58
What is the Definition of a Failed Induction?
Slide 59
Rouse, et al. Failed Labor Induction: Toward an Objective
Diagnosis 1,347 nullips at 36 weeks; cervix no more than 2 cm,
Length of Latent Phase with ROM ROM with Pitocin Vaginal
Cesarean 0 to > 3 hours 63.2% 36.8% 3 to < 6 hours 59.6%
40.4% 6 to < 9 hours 50.7% 49.3% 9 to
Fetal Outcomes ROM / Pit Time n NICU NICU>48 Composite* 0 to
< 3 hours 1,347 6.2% 3.3% 4.2% 3 to < 6 hours 918 6.0% 3.4 %
4.4% 6 to < 9 hours 408 7.4% 3.7% 5.2% 9 to < 12 hours 162
8.6% 4.3% 6.2% 12 hours 71 9.9% 2.8% 5.6% *5 min Apgar < 4; UA
pH < 7.0; seizures; intubation in DR; death, NICU > 48 hours
Obstet Gynecol 2011;117:267
Slide 62
Maternal Outcomes ROM /Pit Time n Infection 3rd /4th Lac Atony
0 to < 3 hours 1,347 13.2% 9.2% 4.7% 3 to < 6 hours 918 15.9%
10.1 % 5.7% 6 to < 9 hours 408 22.8% 11.6% 8.6% 9 to < 12
hours 162 27.8% 9.4% 9.9% 12 hours 71 31.0% 10.7% 11.3% Obstet
Gynecol 2011;117:267
Slide 63
Induction of Labor Simon et al. Obstet Gynecol 2005; 105: 705
397 Nullips undergoing induction of labor Only latent phase > 18
hours increased rate of CS, chorio, hemorrhage No adverse neonatal
outcomes Harper et al. Obstet Gynecol 2012; 119: 1113 5388 women
laboring at term (1647 undergoing IOL) Time required for each cm of
cervical change in latent phase was 2.0 5.5 hours longer in induced
labor
Slide 64
Definitions of Failed Induction and Arrest Disorders Arrest of
Labor Failure to generate regular (eg, every 3 min) contractions
and cervical change: After at least 24 h of oxytocin
administration, and At least 12 -18 hours after ROM Obstet Gynecol
2012; 120:118 AJOG 2014;123(3): 693
Slide 65
Slide 66
Management of FHR Tracings
Slide 67
Moderate FHR variability is reassuring FHR acceleration after
fetal scalp stimulation is reassuring
Slide 68
Non-Medical Factors Influencing Cesarean Rate Institutional
Factors: Time constraints for scheduling in L and D OR staff
availability Inability to support prolonged inductions Physician
Factors: Fatigue, workload, anticipated sleep deprivation Financial
incentives and disincentives
Slide 69
Financial Incentives/ Disincentives for Cesarean Spetz et al:
Birth certificate and hospital financial data from >500,000
births in California, 1995 Cesarean rates for patients with Kaiser
(salaried MDs, profit sharing, standard shifts for MDs, utilization
review / education / guidelines) versus Other HMOs, private
insurance, Medicaid, other payment forms Medical Care 2001; 39(6):
536
Slide 70
Slide 71
Strategies to Reduce Cesarean Rates Aggressive Laboring
Techniques Evidence Based Protocols Confidential Provider Feedback
on CS Rate Perinatal Outcomes Feedback Second Opinion /Peer Review
Review of Facilities. Staffing, Medical Care
Slide 72
Common Myths Among Patients Cesarean is better for my baby
Operative vaginal delivery is bad Labor is bad for the baby Normal
labor is a relatively short & predictable process Long labor is
bad for you and your baby Induced labor is the same as spontaneous
labor
Slide 73
Patient Perceptions/Education More realistic patient
expectations of labor onset, understanding the differences between
spontaneous vs. induced labor, and inability to predict timing or
provider Improve patients understanding of labor benefits; labor
can be/is safe and beneficial for both mother & baby Help
patients understand that cesarean has risks for both mother &
baby
Slide 74
Medical Legal Issues!
Slide 75
Quality Measures to Track and Provide Feedback for Each Ob Gyne
Rate of non-medically indicated cesarean delivery Rate of
non-medically indicated induction Rate of labor arrest or failed
induction diagnosed without meeting accepted criteria Rate of
cesarean deliveries for nonreassuring fetal heart rate (by NICHD
category)
Slide 76
Summary A cesarean performed without an accepted indication
should be labeled nonindicated Labor induction should be performed
only for medical indications Diagnosis of failed induction should
be made only after an adequate attempt Adequate time for normal
latent, first, and second stages should be allowed
Slide 77
Summary If maternal and fetal status is reassuring, diagnosis
of arrest of labor should be made only after adequate time has
elapsed Medically indicated operative vaginal delivery is
acceptable When discussing the first cesarean, its effects on
subsequent pregnancy should be explained Financial incentives to
limit the time spent managing labor should be eliminated