Embed Size (px)
Citation preview

Keeping Current with COPD Management in
Family Practice

2
Friday 4:45 pm visit
• Nancy—56 yo with cc of bronchitis• Coughing >2 weeks, productive-yellow• ?Fever, some breathlessness climbing stairs• Does not want to go to the ED again• Does not want chest x-ray• Wants antibiotics before the weekend
– The last kind she received worked

What Will You Do?
A. Give her the prescription and have her return in 2 weeks for evaluation
B. Take more historyC. Explain that she has no fever, no purulent
sputum and does not need antibioticsD. Begin smoking cessation discussion—she
smells like tobacco smoke
3
4
What Should We Do?
• Take more history– Smoker 35 pack years– Third episode of “bronchitis” in past 2 years
• Colds last for weeks• Always worse than others
– Decrease in activities due to trouble breathing with walking. Now SOB with 6 stairs.
– Has “smoker’s cough” for past 3 years– Mother developed “asthma” at age 60 and died of CHF at
age 68
• Think chronic lung disease!
5
Definition of COPD
• Chronic Obstructive Pulmonary Disease (COPD), a common preventable and treatable disease, is characterized by persistent airflow limitation that is usually progressive and associated with an enhanced chronic inflammatory response in the airways and the lung to noxious particles or gases
• Exacerbations and comorbidities contribute to the overall burden of disease in individual patients
Vestbo J et al. Am J Respir Crit Care Med 2013; 187: 347-65.
6
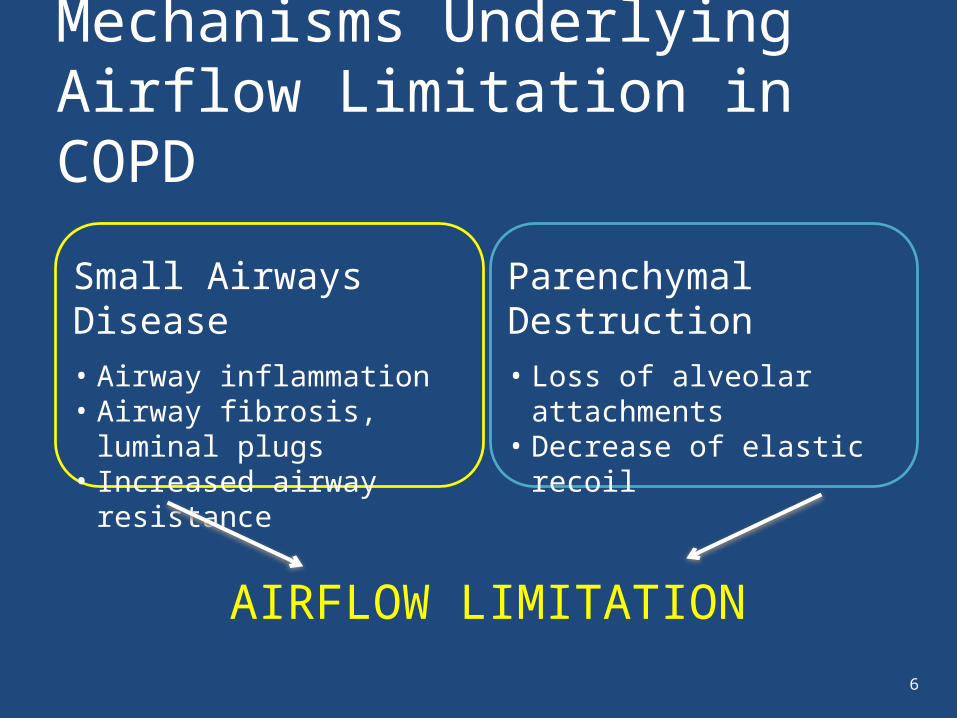
Small Airways Disease• Airway inflammation• Airway fibrosis, luminal plugs• Increased airway resistance
Parenchymal Destruction• Loss of alveolar attachments• Decrease of elastic recoil
AIRFLOW LIMITATION
Mechanisms Underlying Airflow Limitation in COPD
7
Burden of COPD
• COPD is a leading cause of morbidity and mortality worldwide and third leading cause of death in the US
• The burden of COPD is projected to increase in coming decades due to continued exposure to COPD risk factors and the aging of the world’s population
• COPD is associated with significant economic burden
12
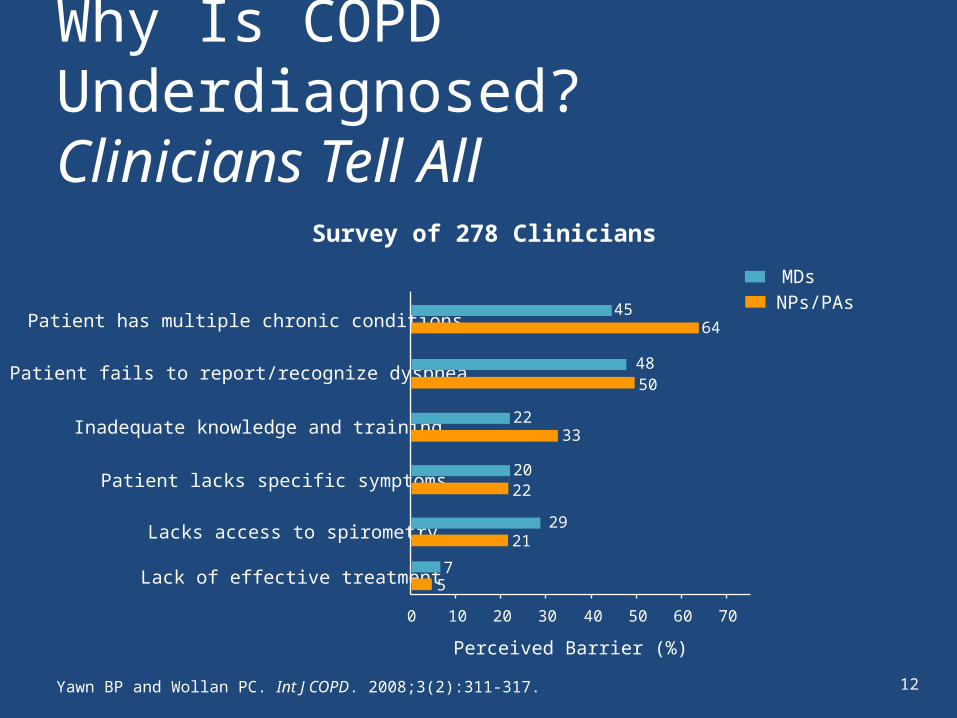
Why Is COPD Underdiagnosed?Clinicians Tell All
Yawn BP and Wollan PC. Int J COPD. 2008;3(2):311-317.
5
2220
22
50
64
0 10 20 30 40 50 60 70
Lack of effective treatment
Lacks access to spirometry
Patient lacks specific symptoms
Inadequate knowledge and training
Patient fails to report/recognize dyspnea
Patient has multiple chronic conditions
Perceived Barrier (%)
45
48
33
2129
7
MDsNPs/PAs
Survey of 278 Clinicians
13
Key Barriers to COPD Diagnosis• COPD not in differential diagnosis• Failure of patients to notice and
report symptoms– Early symptoms often do not interfere with
activities of daily living– Symptom severity increases very slowly
• Failure of health professionals to inquire about respiratory issues– Tools to help– Be specific
• Misdiagnosis of COPD as asthma or bronchitis • Underuse of spirometry
14
More about Nancy
• Need to treat acute episode but with what? Antibiotics, SABA, steroids?
• Diagnosis what she has—asthma, COPD or something else?
• Chest x-ray—little help?• Spirometry—can she do it now
with cough?• Stress test—maybe breathlessness
is CV in origin?• Smoking cessation—Never wrong,
time to try!
PMHHypertension—diureticOsteopenia—Ca and Vit DHysterectomy—age 5135 pack year historyMultiple ED visits—bronchitisNo asthmaFamily history—CVD, late asthma
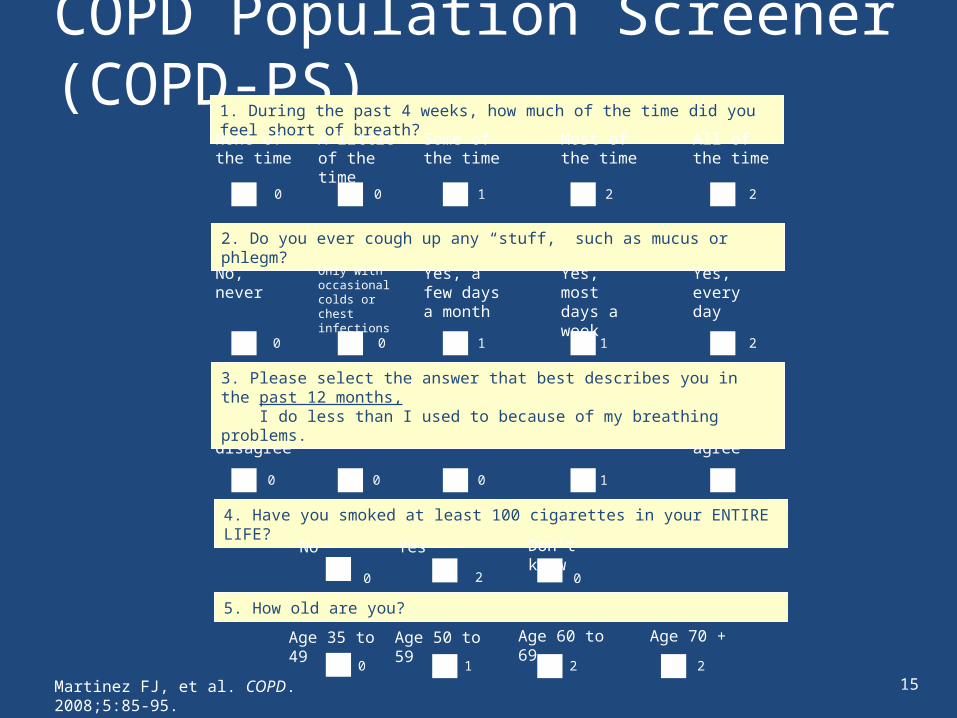
COPD Population Screener (COPD-PS)
1 2 20
Martinez FJ, et al. COPD. 2008;5:85-95.
1. During the past 4 weeks, how much of the time did you feel short of breath?
2. Do you ever cough up any “stuff,” such as mucus or phlegm?
4. Have you smoked at least 100 cigarettes in your ENTIRE LIFE?
Yes
A little of the time
Some of the time
Most of the time
All of the time
None of the time
0 1 2 20
Only with occasional colds or chest infections
Yes, a few days a month
Yes, most days a week
No, never Yes, every day
0 1 1 20
Disagree Unsure Agree Strongly agree
Strongly disagree
0 0 10 2
5. How old are you?
Don’t knowNo
0 2 0
Age 35 to 49 Age 50 to 59 Age 60 to 69 Age 70 +
3. Please select the answer that best describes you in the past 12 months, I do less than I used to because of my breathing problems.
15

16
Feature COPD Asthma
Onset Often in midlife Often in childhood
Family history Variable Often
Medical or social history
Smoking (often ≥20 pack-years)
Atopy(ie, allergy and/or eczema)
Patients report symptoms as . . .
Most notable during exercise
“Mostly bad days”
Most notable at night or early morning
“Mostly good days”
Airflow obstruction May be some reversibility with bronchodilation
Largely reversiblewith bronchodilation
Briggs DD Jr, et al. J Respir Dis. 2000;21(9A):S1-S21. • Doherty DE. Am J Med. 2004;117(12A):11S-23S.
Characteristics That Help Distinguish COPD From Asthma
17
Key Indicators of COPD
• Chronic cough– Present intermittently or every day– Often present throughout the day;
seldom only nocturnal
• Chronic sputum production– Any pattern chronic sputum production
may indicate COPD
• Dyspnea that is– Progressive (worsens over month/years)– Persistent (present every day)– Worse with exercise– Worse during respiratory infections
18
Key Indicators of COPD
• Presence of risk factors– Host factors
• Genetics (alpha-antitrypsin)• Hyperresponsiveness• Lung growth
– Exposure to• Tobacco smoke• Smoke from home cooking
and heating fuels• Occupational dusts and chemicals
19
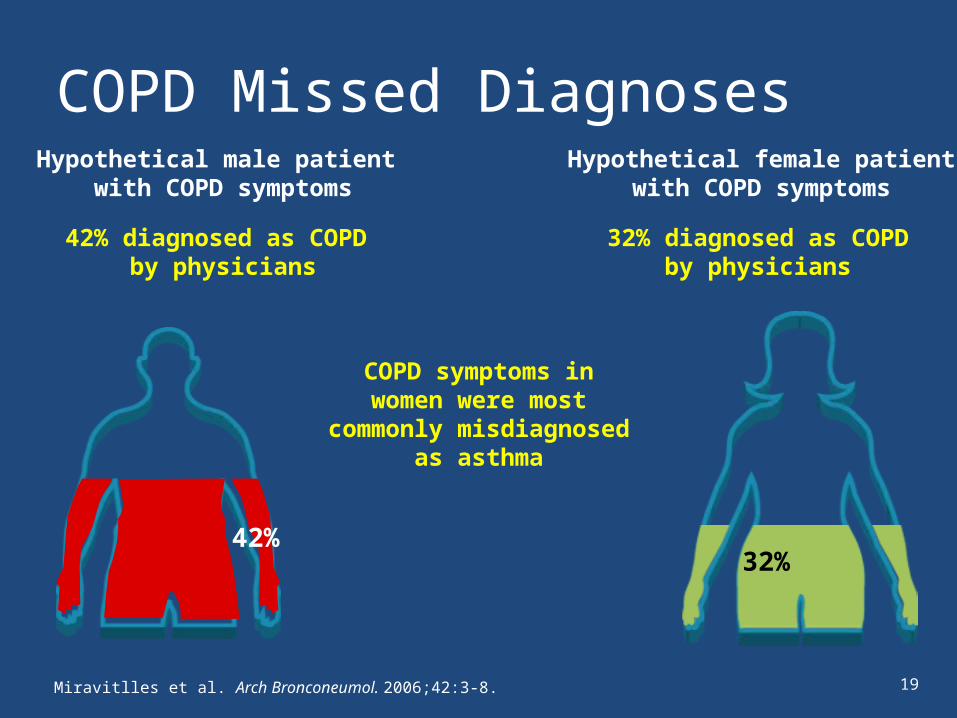
COPD Missed Diagnoses
Miravitlles et al. Arch Bronconeumol. 2006;42:3-8.
Hypothetical male patient with COPD symptoms
Hypothetical female patientwith COPD symptoms
42% diagnosed as COPD by physicians
32% diagnosed as COPDby physicians
32%
COPD symptoms in women were most commonly
misdiagnosed as asthma
42%
20
Nancy Needs Spirometry!
• Often have to wait 4 to 6 weeks to return to baseline after acute event (exacerbation)
• See her before you obtain test or at least evaluate over the phone
• Needs pre and post bronchodilator to see about reversibility and if she meets obstruction definition
• Need FEV1 and FVC to determine severity and how to begin maintenance therapy
21
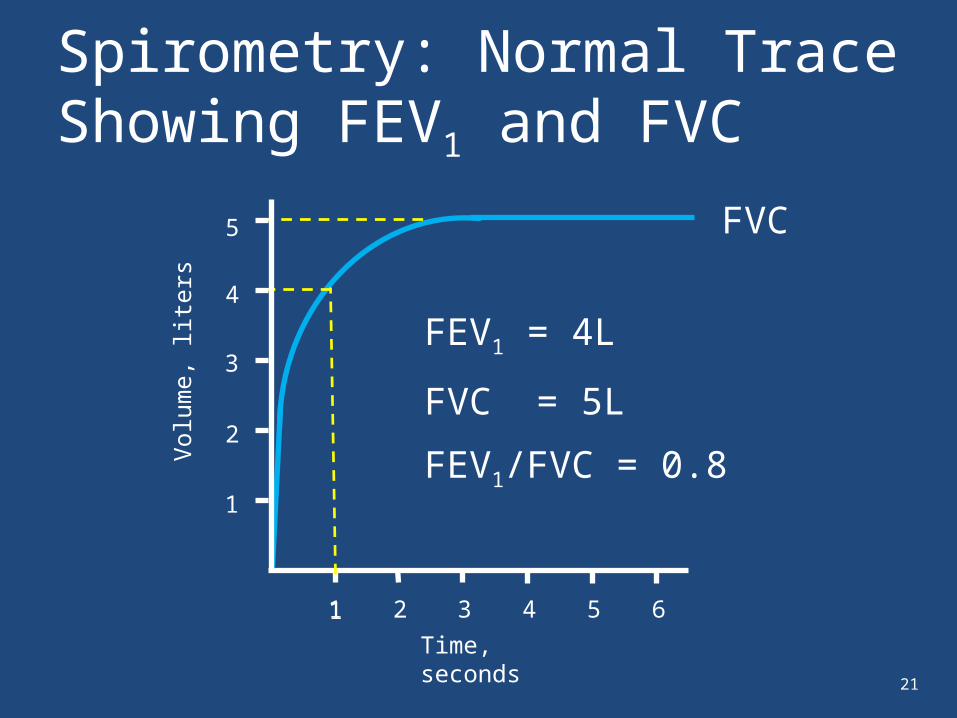
Spirometry: Normal Trace Showing FEV1 and FVC
1
1
Volu
me,
lite
rs
Time, seconds
FVC
2 3 4 5 61
FEV1 = 4L
FVC = 5L
FEV1/FVC = 0.82
3
4
5

Spirometry: Obstructive DiseaseVo
lum
e, li
ters
Time, seconds
5
4
3
2
1
1 2 3 4 5 6
FEV1 = 1.8L
FVC = 3.2L
FEV1/FVC = 0.56
Normal
Obstructive
22

23
Prebronchodilator andPostbronchodilator Testing• Bronchodilator reversibility testing can help rule out asthma
diagnosis and guide initial treatment decisions– Complete or very nearly complete reversibility (return to normal lung
function metrics) suggests asthma, whereas partial reversibility (not returning to normal or near normal) suggests COPD1
– Some reversibility is possible in people with COPD2
– Basic Protocol• Give 1 puff, wait 1 minute, then administer the second dose• Wait 20 minutes for the inhaler to take effect• Repeat the pulmonary function study • Compare post results to pre results
1. Doherty DE. Am J Med. 2004;117(12A):11S-23S. 2. Celli BR et al.Resp Med.2011;105(8):1176-1188
24
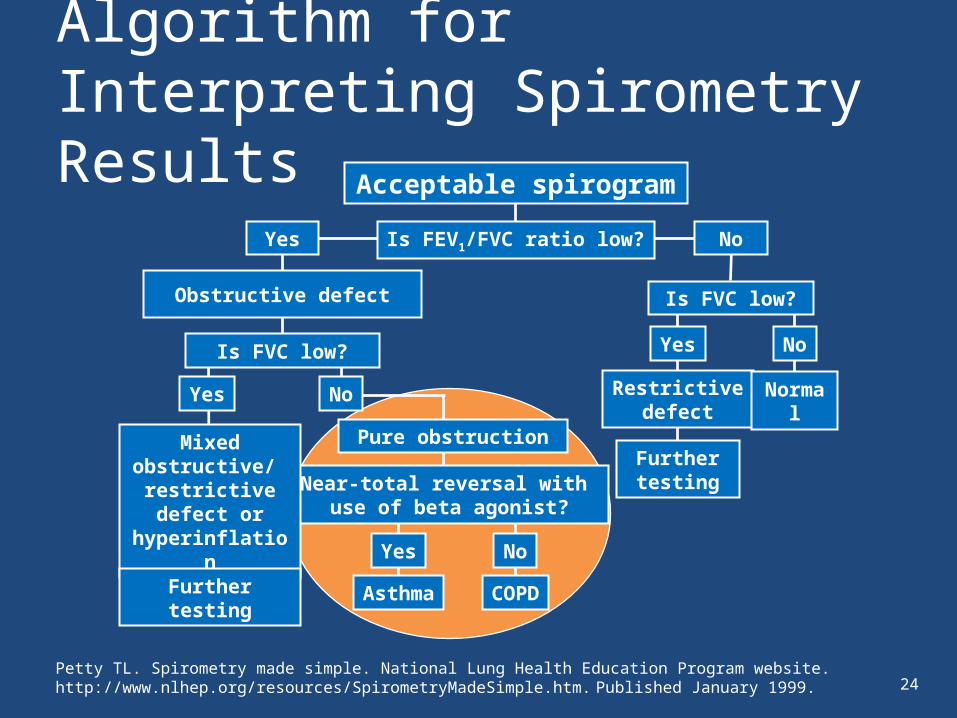
Algorithm for Interpreting Spirometry Results
Petty TL. Spirometry made simple. National Lung Health Education Program website. http://www.nlhep.org/resources/SpirometryMadeSimple.htm. Published January 1999.
Acceptable spirogram
Restrictivedefect
Is FVC low?
Yes
Furthertesting
Normal
Yes
Obstructive defect
Is FVC low?
Near-total reversal with use of beta agonist?
Yes
Mixed obstructive/ restrictive defect or hyperinflation
No
Pure obstruction
No
Is FEV1/FVC ratio low?
No
Yes No
Asthma COPDFurther testing

25
Nancy’s Numbers
• You do spirometry on Nancy and get the following results – Good quality tracing—rated B
Pre-bronchodilator Post-bronchodilator
FEV1 2.2 L 65% pred FEV1 2.7 L 68% pred
FVC 4.0 L FVC 4.1 L
FEV1/FVC 0.55 FEV1/FVC 0.66

26
What is Your Spirometry-Confirmed Diagnosis?1. Normal spirometry2. Poor quality can’t interpret3. Asthma4. Obstructive lung disease consistent with COPD5. Restrictive lung disease
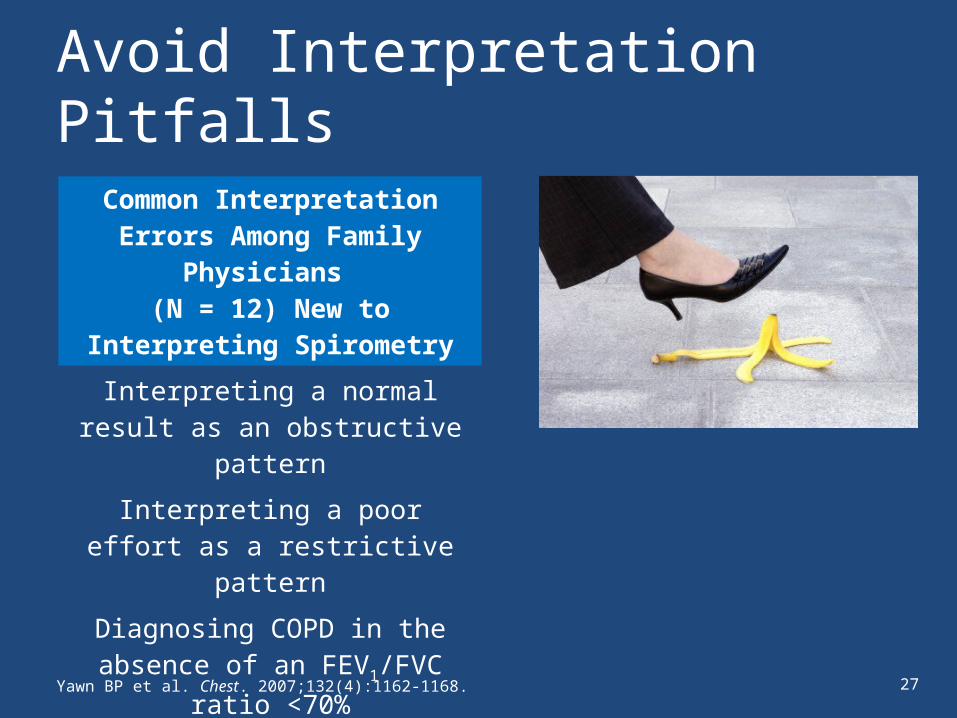
Avoid Interpretation Pitfalls
Common Interpretation Errors Among Family Physicians
(N = 12) New to Interpreting Spirometry
Interpreting a normal result as an obstructive pattern
Interpreting a poor effort as a restrictive pattern
Diagnosing COPD in the absence of an FEV1/FVC ratio <70%
Yawn BP et al. Chest. 2007;132(4):1162-1168. 27

Spirometry Reimbursement
• Billing codes and reimbursement for simple spirometry vary by state
Final rule Medicare program’s fee schedule for physician’s services for calendar year 2007 and the Tax Relief and Health Care Act of 2006. Fed Reg. November 2006;70(216):68132-68215.
Procedure CPT Code 2006 National Average Medicare Reimbursement
Simple spirometry 94010 $33.32
Prebronchodilator and postbronchodilator 94060 $56.61
Smoking cessation counselinga 99406b
99407c$12.13$23.12
Inhaler traininga 94664 $14.02
a Append Modifier -25 code to CPT code in order to be reimbursed for these procedures. b 3 to 10 minutes.c >10 minutes.
28
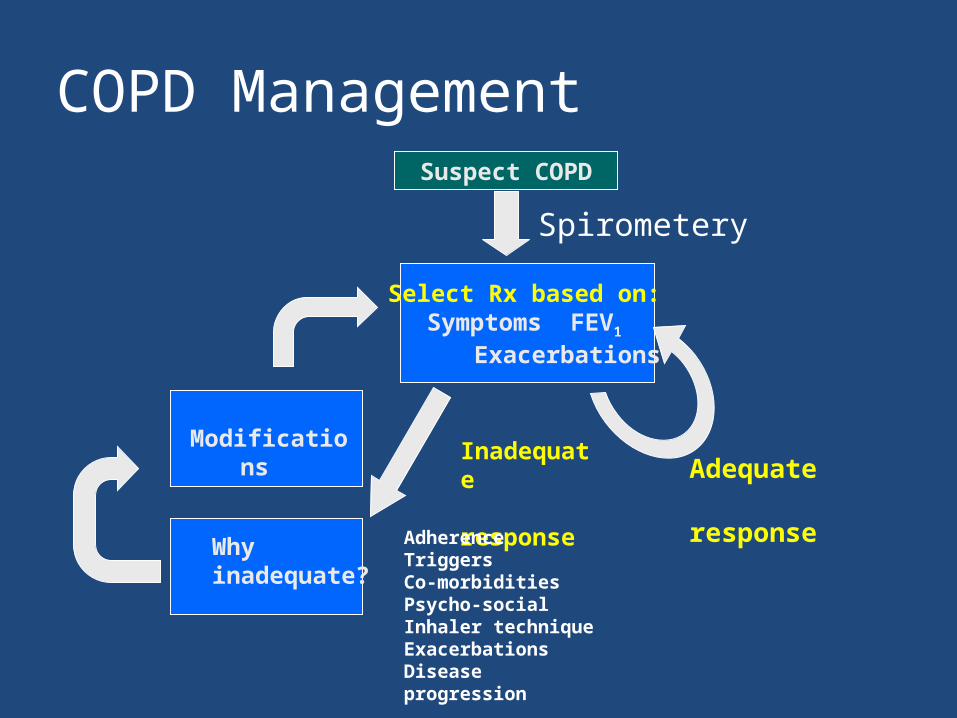
COPD ManagementSuspect COPD
Select Rx based on:Symptoms FEV1
Exacerbations
Modifications
Whyinadequate?
Inadequate response Adequate
responseAdherenceTriggersCo-morbiditiesPsycho-socialInhaler techniqueExacerbationsDisease progression
Spirometery

Using the Global Initiative for Chronic Obstructive Lung
Disease™ (GOLD) Guidelines
A Discussion
See full 2014 GOLD guidelines at www.goldcopd.org
32
Assessment of COPD: Goals
See full 2014 GOLD guidelines atwww.goldcopd.org
33
Assessment of COPD
See full 2014 GOLD guidelines atwww.goldcopd.org
34
Symptoms of COPD
See full 2014 GOLD guidelines atwww.goldcopd.org

Modified MRC (mMRC) Questionnaire
35
36
Assessment of COPD
See full 2014 GOLD guidelines atwww.goldcopd.org
Classification of Severity of Airflow Limitation in COPD*: 2013
See full 2014 GOLD guidelines atwww.goldcopd.org
38
Assessment of COPD
See full 2014 GOLD guidelines atwww.goldcopd.org
39
Assess Risk of Exacerbations
See full 2014 GOLD guidelines atwww.goldcopd.org
40
Nancy Again
• MMRC is 2• Exacerbations? Probably 2 per year• FEV1—68% of predicted• On no therapy until you treated “bronchitis”
and began SABA.

Combined Assessment of COPD
41
See full 2014 GOLD guidelines atwww.goldcopd.org

42
Combined Assessment of COPD
See full 2014 GOLD guidelines atwww.goldcopd.org
Additional Investigations
43
See full 2014 GOLD guidelines atwww.goldcopd.org
Manage Stable COPD:Goals of Therapy
44
See full 2014 GOLD guidelines atwww.goldcopd.org
45
Therapeutic Options: Key Points
See full 2014 GOLD guidelines atwww.goldcopd.org
46
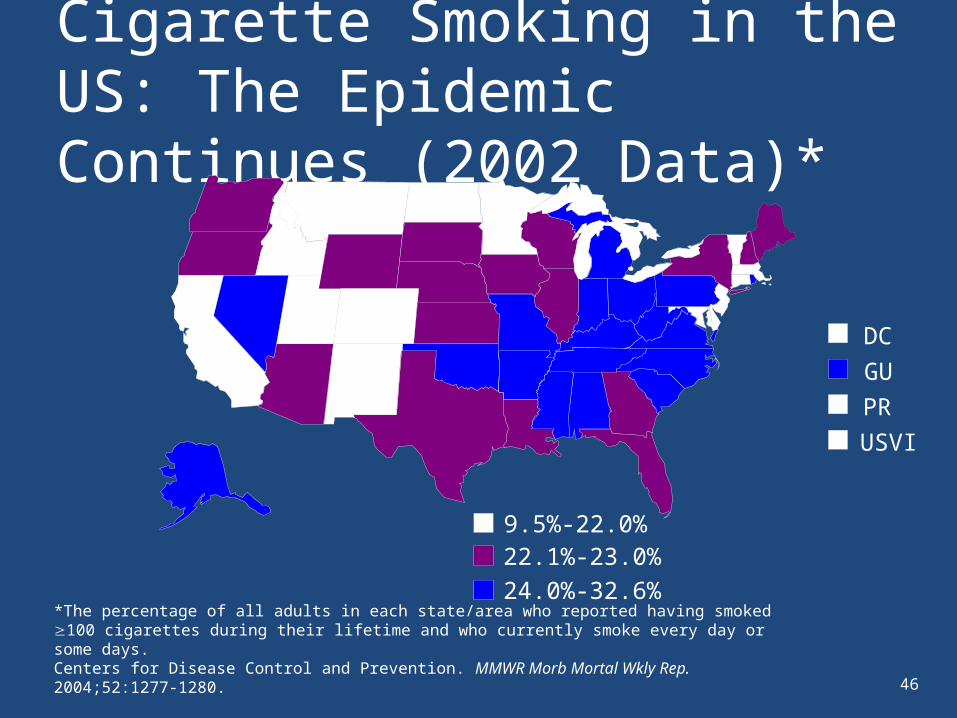
Cigarette Smoking in the US: The Epidemic Continues (2002 Data)*
*The percentage of all adults in each state/area who reported having smoked 100 cigarettes during their lifetime and who currently smoke every day or some days.Centers for Disease Control and Prevention. MMWR Morb Mortal Wkly Rep. 2004;52:1277-1280.
9.5%-22.0%22.1%-23.0%24.0%-32.6%
DCGUPRUSVI

47
Addressing Smoking Cessation
• Best thing parents can do for themselves and their children
• Clinician intervention is effective and cost effective
• Nicotine is addictive, relapse is prevalent

48
Smoking Cessation Interventions
Intervention Studies evaluated (n) Absolute Increase in Cessation Rate
Brief physician contact 16 (Cochrane)7 (US DHHS)
2%2.3%
Group counseling 6 (Cochrane)58 (US DHHS)
10%3.1%
Nicotine gum 51 (Cochrane)13 (US DHHS)
8%6.6%
Nicotine nasal spray 4 (Cochrane)3 (US DHHS)
12%16.6%
Bupropion(300 mg/day SR)
7 (Cochrane)2 (US DHHS)
10%13.2%
Marlow SP et al. Resp Care 2003;48:1238-1256

49
Therapeutic Options for COPD: Formulations and Duration of Action
Drug Class Inhaled Nebulizer Solution Oral Duration of Action,
Hours
β2-agonists
Short acting X X X 4-8
Long acting X X X (transdermal) 12-24
Anticholinergics
Short acting X X 6-9
Long acting X 12-24
Combination short-acting β2-agonists plus anticholinergic X X 6-8
Methylxanthines X Up to 24
Inhaled corticosteroids X X
Combination long-acting β2-agonists plus inhaled steroid X
Combination long-acting β2-agonists plus anticholinergic X
Systemic corticosteroids X
Phosphodiesterase-4 inhibitors X 24
Global Strategies for the Diagnosis, Management and Prevention of Chronic Obstructive Pulmonary Disease. Updated 2011.

50
Hierarchy
Short-acting beta2-agonists or Short acting anticholinergics or Combination
Long-acting beta2-agonists or Long-acting anticholinergics or Combination
Inhaled corticosteroids usually in combination with LABA or LAMA or both
Phosphodiesterase-4 inhibitors
Methylxanthines
Systemic corticosteroids
Therapeutic Options: COPD Medications

51
Pharmacotherapy Overview
Minimal SymptomsMild-Moderate &
Exacerbations (0-1/yr)
Severe symptomsMild-Moderate &
Exacerbations (0-1/yr)
Minimal SymptomsSevere-Very Severe &/or
Exacerbations( ≥2/yr)
Severe SymptomsSevere-Very Severe &/or
Exacerbations (≥2/yr)
Short-acting bronchodilator (prn)
Scheduled: Long-acting bronchodilator
A B C D
Adapted by Adams SG: from the Global Strategy for Diagnosis, Management, and Prevention of COPD 2013, Global Initiative for Chronic Obstructive Lung Disease (GOLD), www.goldcopd.org.
Consider adding other agents**
Scheduled: *Inhaled corticosteroid + long-acting beta2 agonist or Long-acting muscarinic antagonist
*Never use an inhaled corticosteroid as a single agent in patients with COPD (inhaled corticosteroids are not approved by the FDA as a single agent for COPD and they should always be prescribed with a long-acting bronchodilator)** Other possible agents: PDE-4 inhibitor = phosphodiesterase-4 inhibitor and/or theophylline

52
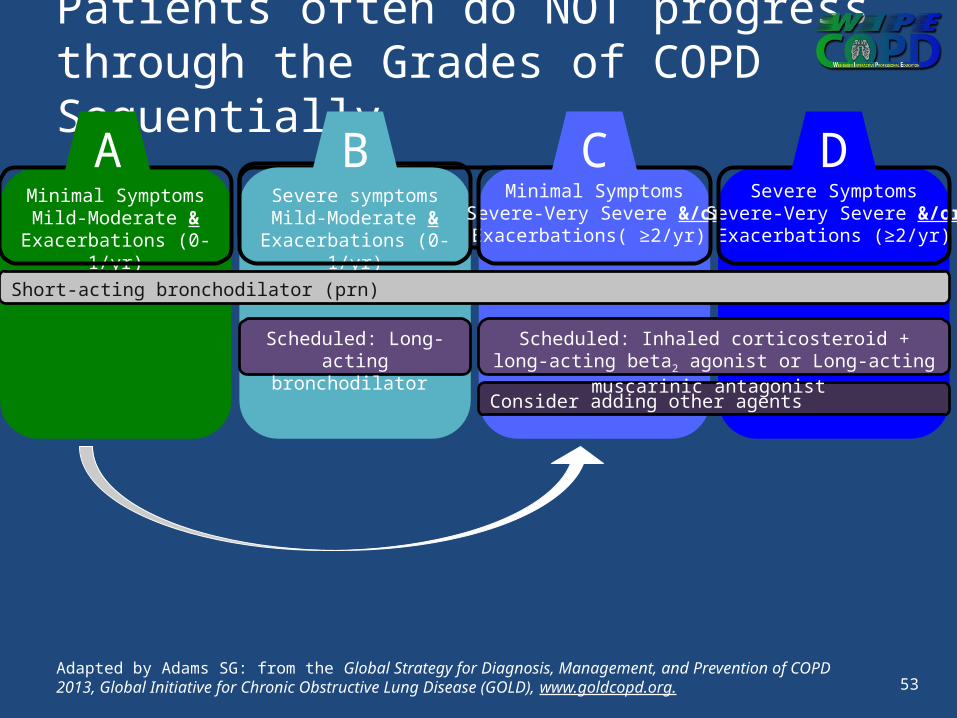
Patients often do NOT progress through the Grades of COPD Sequentially
Minimal SymptomsMild-Moderate &
Exacerbations (0-1/yr)
Severe symptomsMild-Moderate &
Exacerbations (0-1/yr)
Minimal SymptomsSevere-Very Severe &/or
Exacerbations( ≥2/yr)
Severe SymptomsSevere-Very Severe &/or
Exacerbations (≥2/yr)
Short-acting bronchodilator (prn)
Scheduled: Long-acting bronchodilator
A B C D
Consider adding other agents
Scheduled: Inhaled corticosteroid + long-acting beta2 agonist or Long-acting muscarinic antagonist
Adapted by Adams SG: from the Global Strategy for Diagnosis, Management, and Prevention of COPD 2013, Global Initiative for Chronic Obstructive Lung Disease (GOLD), www.goldcopd.org.
53
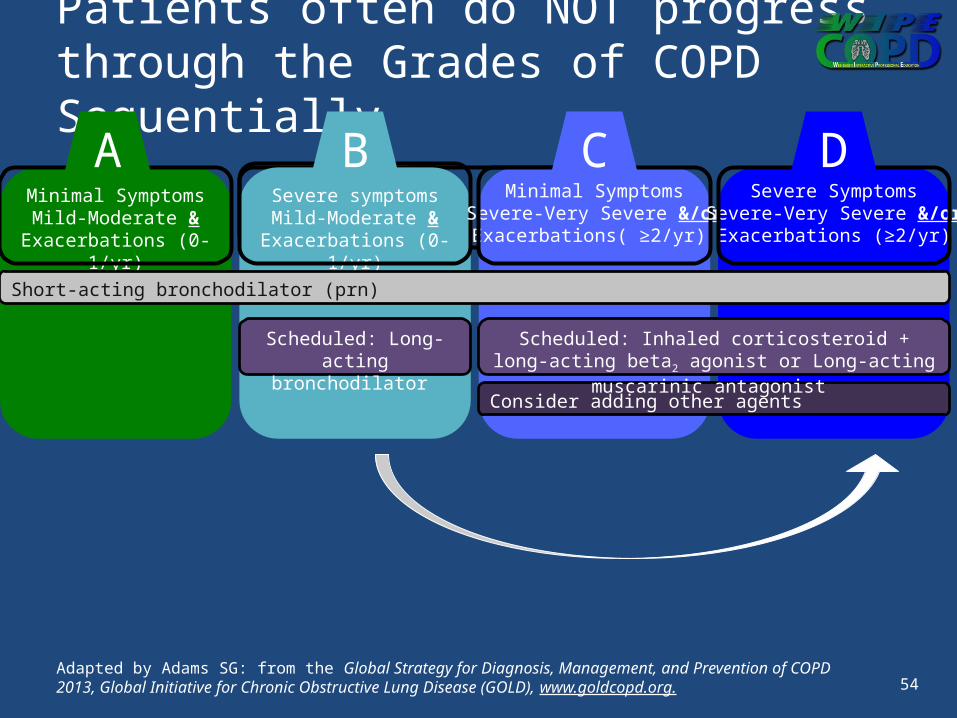
Patients often do NOT progress through the Grades of COPD Sequentially
Minimal SymptomsMild-Moderate &
Exacerbations (0-1/yr)
Severe symptomsMild-Moderate &
Exacerbations (0-1/yr)
Minimal SymptomsSevere-Very Severe &/or
Exacerbations( ≥2/yr)
Severe SymptomsSevere-Very Severe &/or
Exacerbations (≥2/yr)
Short-acting bronchodilator (prn)
Scheduled: Long-acting bronchodilator
A B C D
Consider adding other agents
Scheduled: Inhaled corticosteroid + long-acting beta2 agonist or Long-acting muscarinic antagonist
Adapted by Adams SG: from the Global Strategy for Diagnosis, Management, and Prevention of COPD 2013, Global Initiative for Chronic Obstructive Lung Disease (GOLD), www.goldcopd.org.
54
Patients often do NOT progress through the Grades of COPD Sequentially
Minimal SymptomsMild-Moderate &
Exacerbations (0-1/yr)
Severe symptomsMild-Moderate &
Exacerbations (0-1/yr)
Minimal SymptomsSevere-Very Severe &/or
Exacerbations( ≥2/yr)
Severe SymptomsSevere-Very Severe &/or
Exacerbations (≥2/yr)
Short-acting bronchodilator (prn)
Scheduled: Long-acting bronchodilator
A B C D
Consider adding other agents
Scheduled: Inhaled corticosteroid + long-acting beta2 agonist or Long-acting muscarinic antagonist
Adapted by Adams SG: from the Global Strategy for Diagnosis, Management, and Prevention of COPD 2013, Global Initiative for Chronic Obstructive Lung Disease (GOLD), www.goldcopd.org.
55
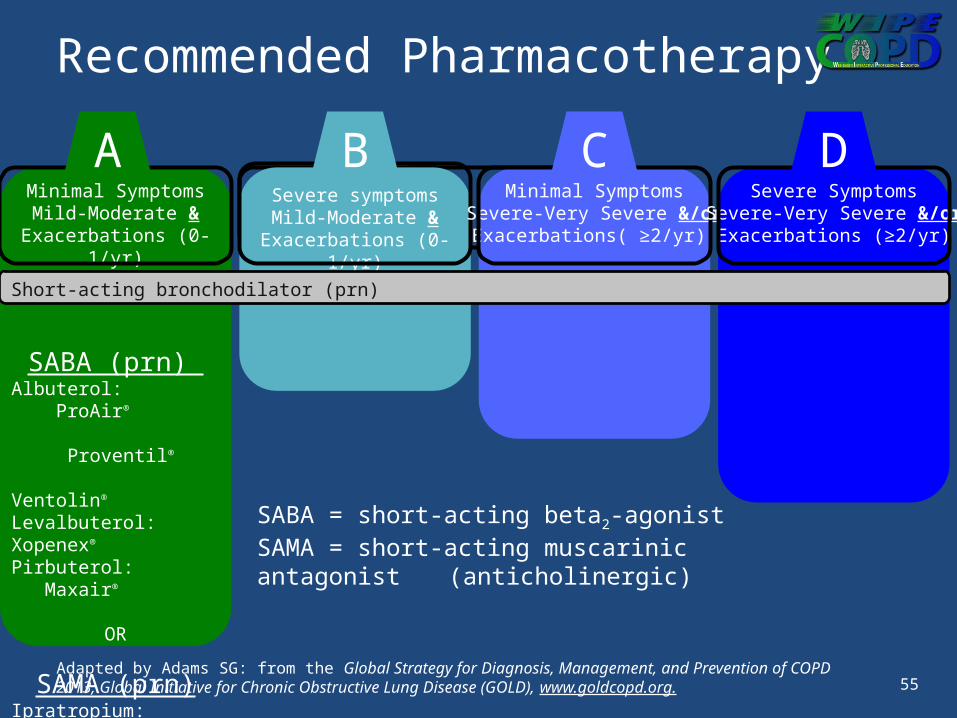
Recommended Pharmacotherapy
Minimal SymptomsMild-Moderate &
Exacerbations (0-1/yr)
SABA (prn) Albuterol: ProAir®
Proventil®
Ventolin®
Levalbuterol: Xopenex® Pirbuterol: Maxair®
OR
SAMA (prn)Ipratropium: Atrovent®
Severe symptomsMild-Moderate &
Exacerbations (0-1/yr)
Minimal SymptomsSevere-Very Severe &/or
Exacerbations( ≥2/yr)
Severe SymptomsSevere-Very Severe &/or
Exacerbations (≥2/yr)
SABA = short-acting beta2-agonistSAMA = short-acting muscarinic antagonist
(anticholinergic)
Short-acting bronchodilator (prn)
A B C D
Adapted by Adams SG: from the Global Strategy for Diagnosis, Management, and Prevention of COPD 2013, Global Initiative for Chronic Obstructive Lung Disease (GOLD), www.goldcopd.org.

56
Minimal SymptomsMild-Moderate &
Exacerbations (0-1/yr)
SABA or SAMA (prn)
Severe symptomsMild-Moderate &
Exacerbations (0-1/yr)
LABA (scheduled) Arformoterol: Brovana®
Formoterol: Foradil® Perforomist®
Indacaterol: Arcapta®
Salmeterol: Serevent®
OR
LAMA (scheduled)Tiotropium: Spiriva®
Aclidinium: Tudorza® Pressair®
Minimal SymptomsSevere-Very Severe &/or
Exacerbations( ≥2/yr)
Severe SymptomsSevere-Very Severe &/or
Exacerbations (≥2/yr)
LABA = long-acting beta2-agonistLAMA = long-acting muscarinic antagonist
(anticholinergic)
A B C D
Recommended Pharmacotherapy
Short-acting bronchodilator (prn)
Adapted by Adams SG: from the Global Strategy for Diagnosis, Management, and Prevention of COPD 2013, Global Initiative for Chronic Obstructive Lung Disease (GOLD), www.goldcopd.org.

Minimal SymptomsMild-Moderate &
Exacerbations (0-1/yr)
SABA or SAMA (prn)
Severe symptomsMild-Moderate &
Exacerbations (0-1/yr)
LABA or LAMA(scheduled)
Minimal SymptomsSevere-Very Severe &/or
Exacerbations( ≥2/yr)
ICS/LABABudesonide/Formoterol
(Symbicort®)Fluticasone/Salmeterol
(Advair®)Fluticasone/Vilanterol
(Breo®)
OR
LAMATiotropium: Spiriva®
Aclidinium: Tudorza® Pressair®
Severe SymptomsSevere-Very Severe &/or
Exacerbations (≥2/yr)
ICS = inhaled corticosteroidLABA = long-acting beta2-agonistLAMA = long-acting muscarinic antagonist
(anticholinergic)
A B C D
57
Recommended Pharmacotherapy
Short-acting bronchodilator (prn)
Adapted by Adams SG: from the Global Strategy for Diagnosis, Management, and Prevention of COPD 2013, Global Initiative for Chronic Obstructive Lung Disease (GOLD), www.goldcopd.org.

Minimal SymptomsMild-Moderate &
Exacerbations (0-1/yr)
SABA or SAMA (prn)
Severe symptomsMild-Moderate &
Exacerbations (0-1/yr)
LABA or LAMA(scheduled)
Minimal SymptomsSevere-Very Severe &/or
Exacerbations( ≥2/yr)
ICS/LABA or LAMA(scheduled)
Severe SymptomsSevere-Very Severe &/or
Exacerbations (≥2/yr)
ICS/LABABudesonide/Formoterol
(Symbicort®)Fluticasone/Salmeterol
(Advair®)Fluticasone/Vilanterol
(Breo®)
AND/OR
LAMATiotropium: Spiriva®
Aclidinium: Tudorza® Pressair®
ICS = inhaled corticosteroidLABA = long-acting beta2-agonistLAMA = long-acting muscarinic antagonist
(anticholinergic)
A B C D
58
Recommended Pharmacotherapy
Short-acting bronchodilator (prn)
Adapted by Adams SG: from the Global Strategy for Diagnosis, Management, and Prevention of COPD 2013, Global Initiative for Chronic Obstructive Lung Disease (GOLD), www.goldcopd.org.

Pharmacotherapy (Summary)
Minimal SymptomsMild-Moderate &
Exacerbations (0-1/yr)
First choice:SABA or SAMA (prn)
Alternative choice:LABA
or LAMA
orSABA + SAMA
(scheduled)
Consider Theophylline
Severe symptomsMild-Moderate &
Exacerbations (0-1/yr)
First choice:LABA or LAMA
Alternative choice:
LABA & LAMA
Consider Theophylline
Minimal SymptomsSevere-Very Severe &/or
Exacerbations( ≥2/yr)
First choice:ICS/LABA or LAMA
Alternative choice:LABA + LAMA
orLABA + PDE-4 inhibitor
orLAMA + PDE-4 inhibitor
Consider Theophylline
Severe SymptomsSevere-Very Severe &/or
Exacerbations (≥2/yr)
First Choice:ICS/LABA &/or LAMA
Alternative choice:ICS/LABA + LAMA
orICS/LABA + PDE-4 inh
orLABA + LAMA
orLAMA + PDE-4 inh
Consider Theophylline
A B C D
59
Short-acting bronchodilator (prn)
Adapted by Adams SG: from the Global Strategy for Diagnosis, Management, and Prevention of COPD 2013, Global Initiative for Chronic Obstructive Lung Disease (GOLD), www.goldcopd.org.

60
Therapeutic Options: Phosphodiesterase-4 Inhibitors
See full 2014 GOLD guidelines atwww.goldcopd.org

61
What Will Be Nancy’s Initial Therapy?She is a “C”1. SABA or SAMA2. LABA or LAMA3. LABA + LAMA4. LABA or LAMA + ICS

Therapeutic Options: Other Pharmacologic Treatment
See full 2014 GOLD guidelines atwww.goldcopd.org
62

63
Manage Stable COPD: Non-pharmacologic
See full 2014 GOLD guidelines atwww.goldcopd.org

64
Activity in People with COPD
• COPD patients are very inactive
• This inactivity is present in all GOLD-stagesFEV1 65%
FEV1 38%FEV1 25%
0
10
20
30
40
50
60
70
80
90
100
Walking
HealthyGOLD I & IIGOLD IIIGOLD IV
min
utes
Pitta et al., AJRCCM 2005; 171: 972-977
65
Therapeutic Options: Rehabilitation
See full 2014 GOLD guidelines atwww.goldcopd.org
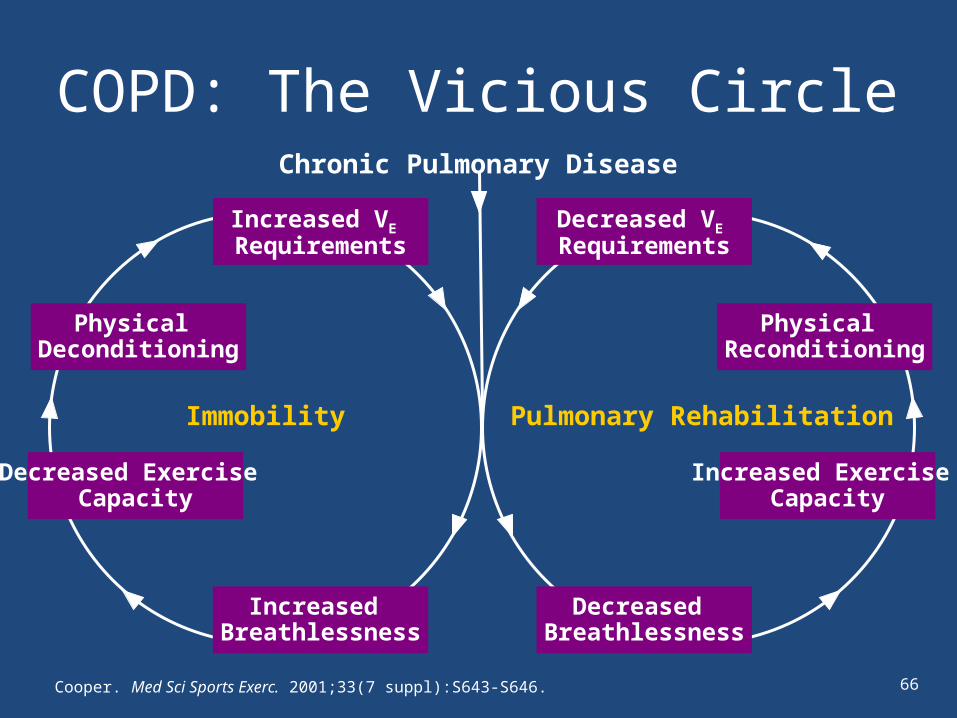
COPD: The Vicious Circle
Cooper. Med Sci Sports Exerc. 2001;33(7 suppl):S643-S646.
Chronic Pulmonary Disease
Physical Deconditioning
Physical Reconditioning
Decreased Exercise Capacity
Increased Exercise Capacity
Increased Breathlessness
Decreased Breathlessness
Immobility Pulmonary Rehabilitation
Increased VE Requirements
Decreased VE
Requirements
66
67
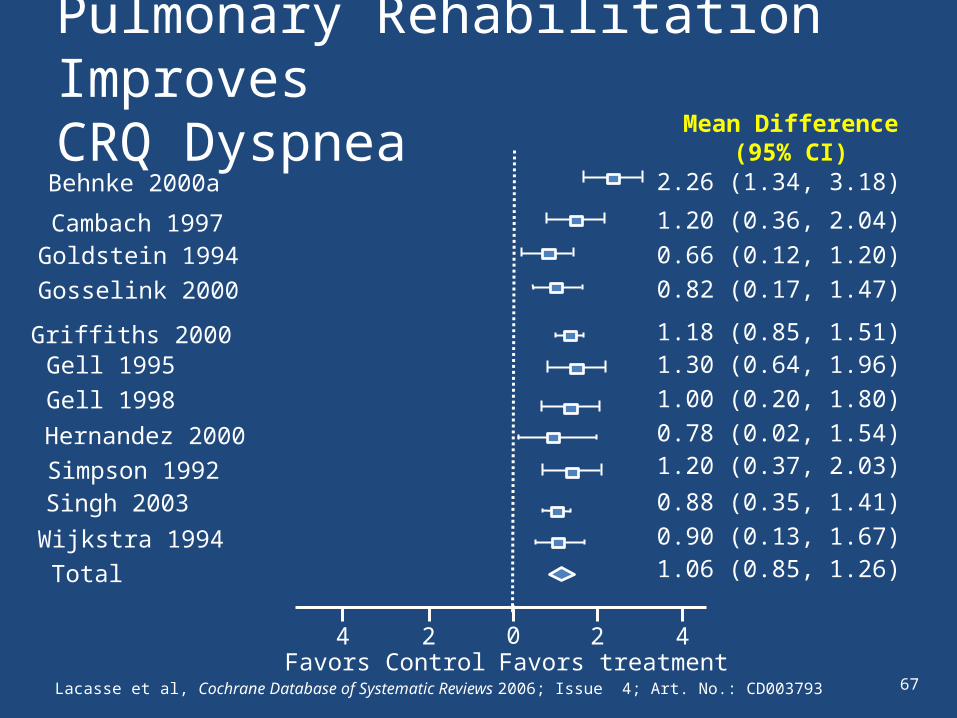
Pulmonary Rehabilitation Improves CRQ Dyspnea
Lacasse et al, Cochrane Database of Systematic Reviews 2006; Issue 4; Art. No.: CD003793
4 2 2 4
Behnke 2000a
Cambach 1997
Favors Control Favors treatment
Goldstein 1994
Mean Difference(95% CI)
2.26 (1.34, 3.18)
1.20 (0.36, 2.04)0.66 (0.12, 1.20)
0
Gosselink 2000
Griffiths 2000Gell 1995
0.82 (0.17, 1.47)
1.18 (0.85, 1.51)1.30 (0.64, 1.96)
Gell 1998Hernandez 2000Simpson 1992
1.00 (0.20, 1.80)0.78 (0.02, 1.54)1.20 (0.37, 2.03)
Singh 2003Wijkstra 1994Total
0.88 (0.35, 1.41)0.90 (0.13, 1.67)1.06 (0.85, 1.26)
68
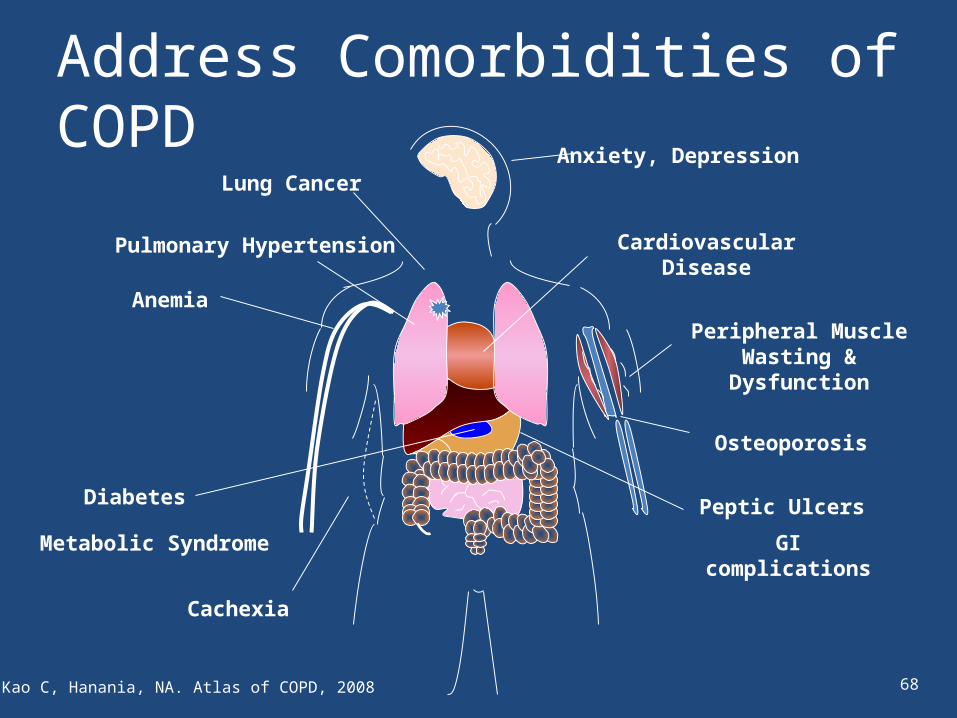
Cardiovascular Disease
Lung CancerAnxiety, Depression
Peripheral Muscle Wasting & Dysfunction
Osteoporosis
Cachexia
Peptic Ulcers
GI complications
Anemia
Pulmonary Hypertension
Diabetes
Metabolic Syndrome
Address Comorbidities of COPD
Kao C, Hanania, NA. Atlas of COPD, 2008
69
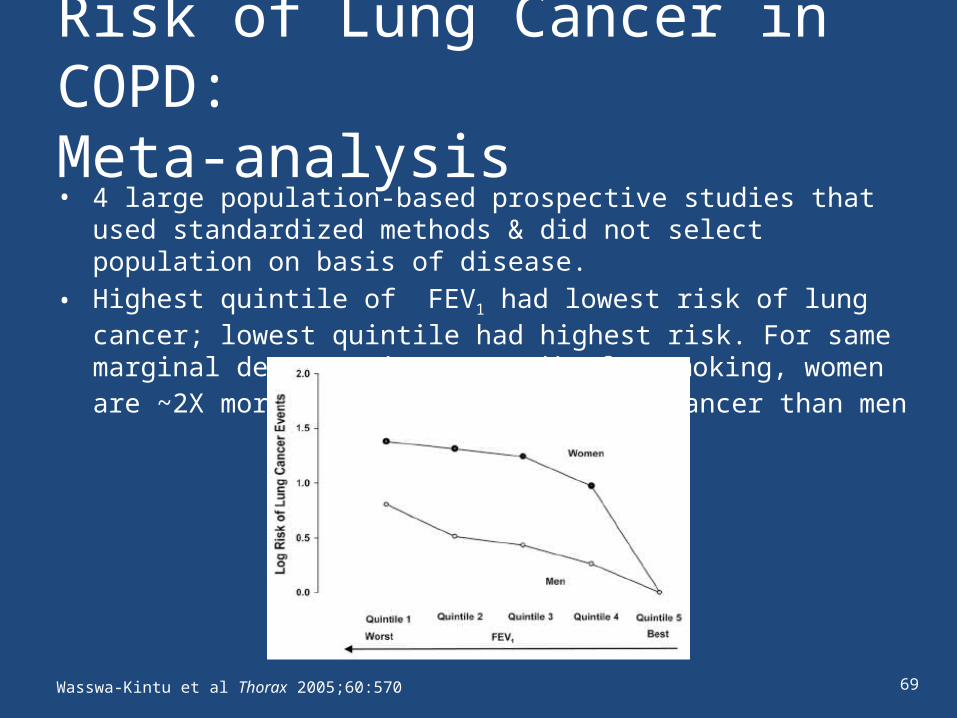
Risk of Lung Cancer in COPD: Meta-analysis• 4 large population-based prospective studies that used standardized
methods & did not select population on basis of disease.• Highest quintile of FEV1 had lowest risk of lung cancer; lowest quintile had
highest risk. For same marginal decrease in FEV1, adj. for smoking, women are ~2X more likely to develop lung cancer than men
Wasswa-Kintu et al Thorax 2005;60:570

70
Anxiety in COPD
• Anxiety is independently associated with:– poorer exercise performance– greater disability– greater hospitalizations for acute exacerbations– decreased quality of life
• Independent of lung function, dyspnea ratings, and other chronic diseases
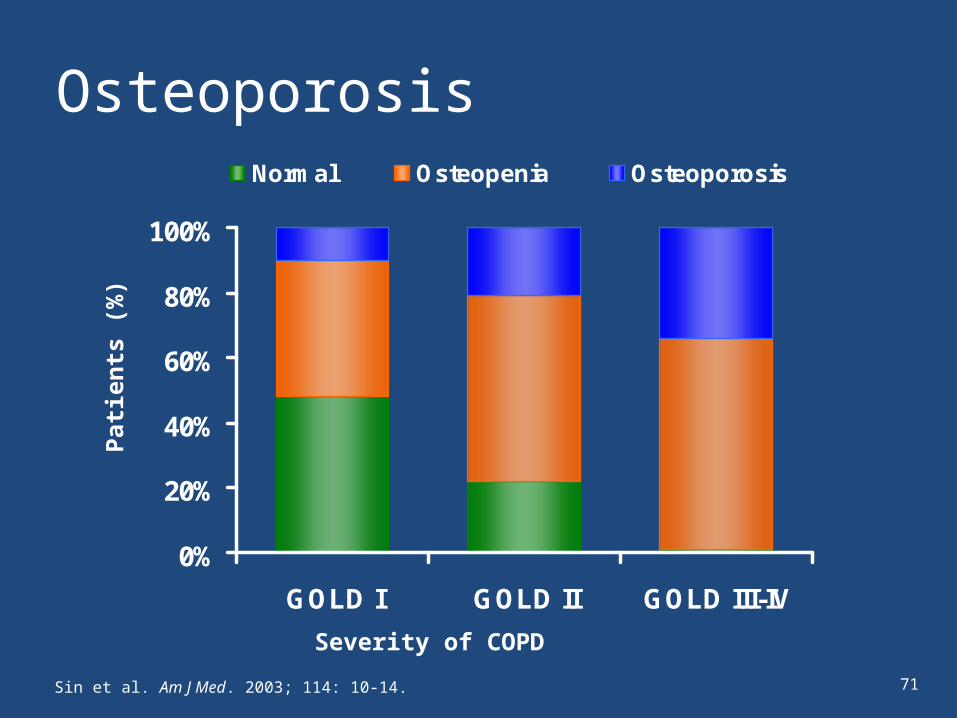
0%
20%
40%
60%
80%
100%
GOLD I GOLD II GOLD III-IV
Normal Osteopenia Osteoporosis
Patie
nts
(%)
Severity of COPD
Sin et al. Am J Med. 2003; 114: 10-14.
Osteoporosis
71

From What Do COPD Patients Die?
ASCVD=arteriosclerotic cardiovascular disease.Mannino et al. Thorax. 2003;58:388-393.Executive Summary: Global Strategy for the Diagnosis, Management and Prevention of COPD. Updated 2005. Available at: http://www.goldcopd.com/Guidelineitem.asp?l1=intId=996. Accessed June 6, 2006 (A).
COPD ASCVD Lung cancer Pneum/Inf Other
1000 20 40 60 80
Severe COPDGOLD Stage III
Patients (%)
72
73
Kurt
• Kurt is 58-year-old retired man with COPD diagnosed 3 years ago during hospitalization for “pneumonia”
• Today he comes in for follow up of visit to the ED for “bronchitits”• He has a 40-year pack history of smoking cigarettes, stopped smoking
3 years ago, 2 years ago and last year • Spirometry FEV1/FVC = 0.55, FEV1 is 61, 1 “exacerbation” past
3 years• MMRC-”2”—walks slower than others his age• He has moderate COPD and has been prescribed tiotropium
once daily • Additional medications include a diuretic for his hypertension, calcium and
vitamin D for his osteopenia (had non-traumatic FX) and escitalopram oxalate (Lexapro) for his “mood”

74
Kurt’s Comorbidities?
• Depression: very common in COPD– Decreases adherence– Antidepressant stopped in 1 to 2 months– Not followed like the chronic disease it is– Considered PHQ-9 to reassess
• Osteopenia– Unusual for a relatively young man– Good workup after FX
• What about CVD?– Stress test?
• What about his recurrent attempts at smoking cessation?
75
Kurt’s Management Program
1. Smoking cessation2. Pulmonary rehabilitation/activity3. May need CV evaluation4. Tiotropium and SABA5. Plan and education for exacerbation recognition6. Monitoring and managing comorbidities7. Regular visits
76
An exacerbation of COPD is:
“an acute event characterized by a worsening of the patient’s respiratory
symptoms that is beyond normal day-to-day variations and leads to a
change in medication.”
Manage Exacerbations

77

78
Manage Exacerbations: Key Points
See full 2014 GOLD guidelines atwww.goldcopd.org

79
Impact on symptoms
and lungfunction
Negativeimpact on
quality of life
Increasedeconomic
costs
Acceleratedlung function
decline
IncreasedMortality
EXACERBATIONS
Consequences of COPD Exacerbations
80
See full 2014 GOLD guidelines atwww.goldcopd.org
Manage Exacerbations: Treatment Options
81
Manage Exacerbations: Treatment Options
See full 2014 GOLD guidelines atwww.goldcopd.org

82
Must Haves for COPD
• Spirometry• Smoking cessation• Pulmonary rehabilitation• Pharmacotherapy• Assessment and therapy of co-morbidities• Good across group communications• Team approach
83
Question
Joel’s COPD was diagnosed 5 years ago. Hislatest FEV1 was 62% last year and his MRC todayis 2. He is taking Tiotropium once a day. He hashad 1 exacerbation (outpatient RX) last year.
Which COPD control square is Joel in?• A• B• C• D

84
Question
• Why is Joel not a candidate for ICS?– Only 1 exacerbation past 2 years– His FEV1 is too high– His insurance company won’t pay– His is afraid of ICS
• Evaluate the risk and benefits!

85





























