-
The Kidneys and Regulation of Water and
Inorganic Ions
-
Human Kidneys and Vascular Supply
Paired retroperitoneal organsIn humans, upper pole lies opposite
T12 vertebra and lower pole lies opposite L3 vertebraWeight:
125-170 g in adult man and 115-155 g in adult womanLength: about
11-12 cmHilum, through which the renal pelvis, renal artery and
vein, the lymphatics and a nerve plexusRenal artery enters the
hilar region and divided into anterior and posterior branch
-
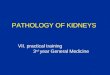
Bisected Kidney Showing Difference between the
Light-staining Cortex and Dark-staining Outer Medulla
Cortex
(about 1 cm in thickness in humans)
Outer medulla
(contains 8 to 18 striated conical masses, the renal
pyramids)
-
Bellini terminate
(10 to 25 small openings on the tip of each papilla that
represent distal ends of collecting ducts)
Renal columns of Bertin
(Renal cortex extends downward between the individual
pyrimads)
Medullary rays of Ferrein
(They are actually considered a part of cortex and formed by
collecting ducts and the straight segments of proximal and distal
tubules)
-
The Nephron Renal Corpuscle (Glomerulus)
Light micrograph of a normal glomerulus Scanning electron
micrograph of a cast of a glomerulus with its capillary loops
-
The Nephron Renal Corpuscle (Glomerulus)
Electron micrograph of a portion of a glomerulus from normal
kidney
Transmission electron micrograph illustrating a segment of
glomerular basement membrane (GBM) from normal rat kidney
-
The Nephron Renal Tubule
Nephron segments in a juxtamedullary nephron (left) and a
superficial nephron (right)
-
The Nephron Proximal Tubule Cell
The endocytic-lysosomal system in a proximal tubule cell
-
The Nephron Collecting Duct
Immunolocalization of the vasopressin-sensitive aquaporin CD
water channel in the rat collecting duct. A. Light micrography of
cryosection from outer medulla. B. Electron micrograph of ultrathin
cryosection of principal cells in the inner medullary collecting
duct
-
Renal Transport of Sodium and Water
-
Schematic Representation of Renal Epithelial Cell
Schematic Representation of Renal Epithelial Cell
-
Na+ Reabsorption at Proximal tubule (1) Na+ Reabsorption at
Proximal tubule (1)
Two mechanisms for Na+ transport from lumen to the cell
(1) Na+/H+ antiporter: H+ secretion & HCO3- reabsorption:
account for 2/3 amount
(2) with Cl-, H2 PO4-, glucose, amino acid & other anions:
account for 1/3 amount greater in the early (pars convoluta) than
in the late (pars recta) proximal nephron
-
Proximal tubule (2)Proximal tubule (2)
Na+ exits out of the cell at the basolateral surface is coupled
with
(1) Na+/K+ ATPase: accounting for 80%
(2) HCO3- reabsorption: 20%
-
Ascending limb of Henles Loop (1)Ascending limb of Henles Loop
(1)
NaCl & KCl are reabsorbed together in a secondary active,
electroneutral mannerNa-K-2Cl cotransporter is driven by the
electrochemical gradient for Na by Na/K ATPase in the peritubular
membraneCl- exits out of the cell at the basolateral surface via
KCl symporter and Cl conductance channel
-
ROMK channel
-
Ascending limb of Henles Loop (2)Ascending limb of Henles Loop
(2)
Resulting in excretion of 20~25% of filtered Na+ load due to
(1) act at a site with substantial Na reabsorption
(2) Na+ escaped transport in the loop have limited opportunities
to be reabsorbed later in the nephron
-
Early Distal Convoluted Tubule
Early Distal Convoluted Tubule
Electroneutral NaCl reabsorptionThiazide group (including
metolazone and indapamide): compete with Cl- binding site of Na-Cl
cotransporterExcretion of 5-8% of filtered Na loadBasolateral
3Na+/Ca2+ exchanger: Na+ into and Ca2+ out of the cell of DCT
-
3
-
Comparison of Stoichiometric Relationship between TNa + and
either
QO2 or ATP Utilization
Comparison of Stoichiometric Relationship between TNa+ and
either
QO2 or ATP Utilization
-
Distribution of Body Fluid
Total Body Water (TBW) : 60% of body weightIntracellular fluid:
40% of TBWExtracellular fluid: 20% of TBW 15% interstitial fluid 5%
plasma water
-
Body Fluid Composition
ECF volume: renal Na+ regulationICF volume: effective
osmolality
KK++ NaNa++2828
140140
1414
140140
ICFICF ECFECF
-
Plasma Osmolality
Plasma Osmolality (mOsm/Kg H2 O) = 2 x [Na] (mEq/L) +
[glucose]/18 (mg/dl)
+ [BUN]/2.8 (mg/dl)
Effective Posm = 2 x [Na] (mEq/L) + [glucose]/18 (mg/dl)
-
Osmolar vs Volume Regulation (1)
1. Osmotic threshold : the level of Posm when serum ADH is
detectable (usually about 280 mOsm/Kg)
2. Threshold for thirst , Posm about 2-5 mOsm/Kg higher than
Osmotic threshold
3. Under steady state ( [Na] 137mEq/L, Osm 285mOsm/Kg), ADH is
average 2.5 pg/ml
4. Serum Osm < 280, ADH is unmeasurable; urine is maximally
dilure ( 50 mOsm/Kg)
5. When serum Osm >295mOsm/kg, ADH is 5 pg/ml; urine is
maximally concentrated ( about 1200 mOsm/Kg)
-
Regulation of thirst
Osmoreceptor: at anterolateral hypothalamus
Factors stimulate thirst: Increase in serum osmolality
(tonicity) Decrease in blood volume Hypokalemia Hypercalcemia
-
6. Volume regulation of ADH: Hypotension or 8-10% reduction of
blood volume=> release of ADH
7. Osmoregulation of ADH: 1-2% increase of Posm will stimulate
release of ADH
8. Osmoregulation is more sensitive than volume regulation
9. Volume regulation has higher priority to osmoregulation (
Persistent ADH secretion will be noted in hypotensive and
hypovolemic patients in spite of hyponatremia)
Osmolar vs Volume Regulation (2)
-
Body Fluid Composition
ECF volume: renal Na+ regulationICF volume: effective
osmolality
KK++ NaNa++2828
140140
1414
140140
ICFICF ECFECF
-
Prevalence Rate of Hyponatremia
If hyponatremia is defined as Plasma [Na] < 135 mEq/L =>
15~22%Plasma [Na] < 130 mEq/L => 1~4%
-
Symptoms of Hyponatremia
Acute: headache, hypertension, coma, seizure, blurred vision,
etc.Chronic: non-specific symptoms such
as general malaise, weakness, leg cramps, memory loss, altered
mental status or personality, insomnia, etc.
-
Defense Mechanism in Hyponatremia
First line: outward shift of intracellular and interstitial
fluid of brain into CSFSecond line: loss of intracellular osmogenic
particles such as K+, Na+, Cl-, etc
-
K+, Na+
Osmolytes /H2 O
NaNa++/H/H22 OO
NaNa++/H/H22 OO
NaNa++/H/H22 OO
NormonatremiaNormonatremia
AcuteAcuteHyponatremiaHyponatremia
ChronicChronicHyponatremiaHyponatremia
11
22
K+, Na+
Osmolytes/H2 O
K+, Na+
Osmolytes /H2 O
33
-
Renal Transport of Potassium
-
Total Body K+ Content (mmol/kg)
Age (years) Male Female10 37 3720 58 4540 52 4060 48 3780 45
33
Pierson et al. Am J Physiol 1984: 246, 234-9
-
Distribution of Total Body K+
Muscle 2650 mmolLiver 250 mmolRed blood cells 250 mmol[K+] 150
mmol/L
Bone 33 mmolInterstitialfluid 35 mmol
Plasma 15 mmol[K+] 4 mmol/L
Intracellular fluid (ICF)
Extracellular fluid (ECF)
-
Physiologic Roles of K+Physiologic Roles of K+
Roles of intracellular K+: * Cellular volume maintenance *
Intracellular pH regulation * Cell enzyme function * DNA/protein
synthesis * Cell growthRoles of transcellular K+ ratio: * Resting
cell membrane potential * Neuromuscular excitability * Cardiac
pacemaker rhythmicity
-
Resting Membrane Potential
Vm = - k
ln {[ K+]i
[ K+]o } ----- (1)This equation can be expressed at 37C as
follows:Vm = -61.5 mV x log [ K+]i /[ K+]o ----- (2)Vt = - ln {k1x
[Mg2+]i+k2x[Na+]i+k3x[Ca2+]i+
+k4x[H+]o}
{k5x[Mg2+]o+k6x[Na+]o +k7 x[Ca2+]o +k8 x[H+]i } -- (3)
Ki is the K+ activity of the intracellular fluid Ko is the K+
activity of the extracellular fluid
-
Components of K+ Homeostasis
Internal balance ( ICF and ECF K+ distribution)External balance
( Renal excretion of K+)
-
Distribution of K+ in the Body: routes of acquisition and
excretion
-
Factors Influencing K+ Shift from ICF to ECF (1)
Factors Influencing K+ Shift from ICF to ECF (1)
Hormones: 2 -adrenergic antagonist, lack of insulin or
aldosterone, Acid-base disturbances: acute acid gain or bicarbonate
lossICF anion change: catabolism, loss of organic phosphatesCell
necrosis
-
Renal Regulation of K+ Excretion
Renal Regulation of K+ Excretion
Overview of the renal handling of K+
Cellular mechanisms ( Principal cells in CCD)
-
Cortical collecting duct ( CCD)
-
Factors Modifing K+ Secretion by the Distal Nephron
FactorsK+ secretionPlasma [K+ ] Flow rate, glucocorticoidsLumen
[Na+] Transepithelial potential difference Anions (except
Cl-)AlkalemiaVasopressin2- agonists Dietary K+
intakeAldosterone
FactorsK+ secretionPlasma [K+ ] Dietary K+
intakeAcidemiaAmmoniaLumen [Cl-] at DCTInsulin1- agonists
-
Components of K+ ExcretionComponents of K+ ExcretionGenerate a
lumen-negative transepithelial potential difference (TEPD) in
CCD
Movement of K+ via specific K+ channel
Flow rate through the CCD
-
Bartter SyndromeHypokalemia: Cl reabsorption at TAHL=> JGA
hyperplasia & Na +,K +,Cl - to the distal nephron (CCD) =>
H+,K+ secretion at CCDCl--resistant metabolic alkalosis, High urine
[Na+], [K+],[Cl-], [Ca+ +]; mimicking furosemide effect
Hyperreninic hyperaldosteronismHyperprostaglandin due to[K+] &
RAAHyporesponsiveness of BP to angiotensin II infusionAutosomal
recessive inheritance with malfunction of NKCC2, ROMK, ClC-kb
channel at TAHLTreatment: KCl supplement, K+-sparing agent (
Spironolactone, Triamterene, Amiloride), NSAID
-
(ROMK channel)
-
Gitelman SyndromeHypokalemiaCl--resistant metabolic
alkalosisHyperreninic hyperaldosteronismHypocalciuria: urine Ca2+
< 100 mg/dayRenal Mg wasting and hypomagnesemiaBiochemical data
similar to thiazide effectAutosomal recessive inheritance with
mutation of Na+/Cl- cotransporter at distal convoluted tubule
-
Renal Transport of Hydrogen Ion (H+)
-
Stages of Acid-Base BalanceAcid synthesis:1. S-containing
AA:
H2SO42. Phosphoesters:
H3PO43. Oxid. foods:
organic acids* Total production1~1.5 mEq/kg/day
Buffering1. HCO3-
/H2CO32. Albumin3. Hemoglobin
* Loss of alkali1~1.5 Eq/kg/day
Renal acid Excretion
1.H+ secretion
2. Titration of urinary buffers
* Total excretion:
1~1.5mEq/kg/dayHA H+A-
+NaHCO3
CO2+ Na+A- Kidney
H+A-Resynthesis
excretion
-
Acid BalanceAcid Balance
In: acid production
Out: net acid excretion (NAE) = NH4+ + TA (H2 PO4-) HCO3-
-
Medullary Metabolism of NH3+ & H+
-
Classical Distal RTA
-
Back Leakage & Hypokalemic Distal RTA
H+K+
-
Voltage Defect & Hyperkalemic Distal RTA
-
Renal Transport of Calcium (Ca2+) &
Magnesium (Mg2+)
-
47% Ionized47% Ionized
37% Albumin37% Albumin
ECF 1%
Distribution and Normal Ranges of Calcium inDistribution and
Normal Ranges of Calcium inA 70 Kg Healthy AdultA 70 Kg Healthy
Adult
0
20
40
60
80
100
10% Globulin10% Globulin
FilterableFilterable
Body content 1300 g Plasma level
8.4-10.2 mg/dl(2.1-2.55 mmol/L)
Tissue 1%
ECF 1%
Skeleton 98%
6% Complexed6% Complexed
BoundBound
-
Typical daily calcium intake and output for a normal adult in
neutral Ca2+ balance
-
Intestinal Calcium Transport
-
Renal Calcium Reabsorption
-
Segmental Handling of CaSegmental Handling of Ca2+2+
along the Renal Tubule along the Renal Tubule
NEPHRON SEGMENT
FRACTIONAL REABSORPTION
(%)
CELLULAR TRANSPORT MECHANISM
Proximal tubule 5060 Passive, paracellular
Thin descending & ascending limbs
0
TAL (Thick ascending limb of Henles loop)
15 Passive, paracellularActive component stimulated by PTH
DCT/CNT 1015 Active, transcellular
Collecting duct Unknown
-
Renal Tubule Handling of CaRenal Tubule Handling of Ca2+2+
-
Parathyroid Hormone (PTH)
Net effectBlood calcium Blood phosphateUrine calcium: increase
in filtered Ca load >> increase in tubular reabsorption
-
Calcium Sensing Receptor
Parathyroid gland: G protein-coupled receptor Abundant
expression Central role in PTH secretion:
Ca2+ decreases PTH secretionKidney: mRNA present along entire
nephron Protein: proximal tubulebrush border
IMCD brush border cTAL,mTAL-basolateral surface DCT-basolateral
surface
-
Action of 1,25 (OH)2 D3
Kidney: * effect on Ca and P reabsorption is not
clearBone: * necessary to maintain Sca and Sp for
proper mineralization * administration mobilizes Ca and
PIntestine: Ca and P absorption in small intestine
-
Hypercalcemia due to Thiazide
The mechanism of thiazide action is complexChronic thiazide
administration sodium depletion
proximal tubular resorption of
sodium and calcium hypocalciuria
-
Urine [Ca2+]
-
MgMg2+2+ MetabolsimMetabolsim in in Normal AdultsNormal
Adults
-
Renal Tubule Handling of MgRenal Tubule Handling of Mg2+2+
-
Thank You for Your Attention
The Kidneys and Regulation of Water and Inorganic IonsHuman
Kidneys and Vascular SupplyBisected Kidney Showing Difference
between the Light-staining Cortex and Dark-staining Outer Medulla
4The NephronRenal Corpuscle (Glomerulus)The NephronRenal Corpuscle
(Glomerulus)The NephronRenal TubuleThe NephronProximal Tubule
CellThe NephronCollecting DuctRenal Transport of Sodium and
WaterSchematic Representation of Renal Epithelial Cell Na+
Reabsorption at Proximal tubule (1) 13 14Proximal tubule (2)
16Ascending limb of Henles Loop (1) 18Ascending limb of Henles Loop
(2)Early Distal Convoluted Tubule 21 22Comparison of Stoichiometric
Relationship between TNa+ and either QO2 or ATP Utilization 24 25
26Distribution of Body FluidBody Fluid CompositionPlasma
OsmolalityOsmolar vs Volume Regulation (1) 31Regulation of
thirstOsmolar vs Volume Regulation (2)Body Fluid
CompositionPrevalence Rate of HyponatremiaSymptoms of
HyponatremiaDefense Mechanism in Hyponatremia 38Renal Transport of
PotassiumTotal Body K+ Content (mmol/kg)Distribution of Total Body
K+Physiologic Roles of K+ 43Resting Membrane Potential 45Components
of K+ HomeostasisDistribution of K+ in the Body:routes of
acquisition and excretionFactors Influencing K+ Shift from ICF to
ECF (1) Renal Regulation of K+ Excretion 50Factors Modifing K+
Secretion by the Distal Nephron Components of K+ ExcretionBartter
Syndrome 54Gitelman Syndrome 56Renal Transport of Hydrogen Ion
(H+)Stages of Acid-Base BalanceAcid Balance 60 61Medullary
Metabolism of NH3+ & H+ 63 64Voltage Defect & Hyperkalemic
Distal RTARenal Transport of Calcium (Ca2+) & Magnesium (Mg2+)
67 68Intestinal Calcium Transport 70Renal Calcium Reabsorption 72
73 74 75Parathyroid Hormone (PTH)Calcium Sensing Receptor 78 79
80Action of 1,25 (OH)2D3Hypercalcemia due to Thiazide 83 84 85 86
87