Embed Size (px)
DESCRIPTION
Kidneys and Hypertension. Dr. Shahrzad Shahidi Nephrologist Isfahan University of Medical sciences. Hypertension (HTN). Persistent elevation of arterial blood pressure (BP) 31% of Americans have BP > 140/90 mmHg Most patients asymptomatic - PowerPoint PPT Presentation
Citation preview

Kidneys and Hypertension
Dr. Shahrzad Shahidi
Nephrologist
Isfahan University of Medical sciences
1

Hypertension (HTN)
2
Persistent elevation of arterial blood pressure (BP)
31% of Americans have BP > 140/90 mmHg
Most patients asymptomatic Single most preventable cause of
premature death in developed countries.
Chobanian AV, et al. Hypertension 2003;42(6):1206–1252

3

Adult Classification
4
Classification Systolic BP (mmHg)
Diastolic BP (mmHg)
Normal Less than 120 and Less than 80
PreHTN 120-139 or 80-89
Stage 1 HTN 140-159 or 90-99
Stage 2 HTN > 160 or > 100
Chobanian AV, et al. Hypertension 2003;42(6):1206–1252

Classification for Adults
5
Classification based on average of > 2 properly measured seated BP measurements from > 2 clinical encounters
If systolic & diastolic BP values give different classifications, classify by highest category
Prehypertension: patients likely to develop hypertension

Pathogenesis. No one gene is responsible. Studies shows that several difft
genes may have an effect on BP.
RARE SINGLE GENE CAUSES OF HTN HAVE BEEN IDENTIFIED.
6

Single Gene Causes of HTN
Glucocorticoid remediable aldosteronism Syndrome of minerelocorticoid excess Pheochromocytoma - may occur with
MEN type 2, Von Hippel Lindau disease, Neurofibromatosis type 1
Liddle’s Syndrome
7

Renin angiotensin system Renin –secreted by the juxtaglomerular
apparatus. It converts angiotensinogen (inactive) to
angiotensin 1 .It then converts to angiotensin 2 by ACE.
Increased renin – RAS, Renal cell carcinoma & rarely some renin secreting tumours.
8

99

Actions of angiotensin II
Arteriolar vasoconstriction. Efferent arteriolar vasocnstriction. Aldosterone secretion. Epinephrine release (adrenaline). Smooth muscle hypertrophy. Inhibit renin release (negative feed
back). Myocardial growth.
10

Other pathogenesis Arterial stiffness – Aging , DM,
Kidney disease. Sympathetic nervous system-
Activation associated with sudden rise in BP.- By increasing stroke volume, HR , systemic vascular resistance and activation of RAS.
11

Secondary Hypertension
Renovascular DiseaseRenal parenchymal disease:
CKDGlomerulonephritisADPKDObstructive uropathy,…
12

Renal artery stenosis Atherosclerotic or fibromuscular
dysplasia as etiology Clinically difficult to control HTN Renal dysfuntion Resistant fluid retention Worsening Cr with ACEI or ARB
13

Investigations US Kidneys- assymmetry. Doppler of renal arteries. Captopril renogram - affected kidney
may show a 30% decline in function. MRA. Angiogram- secure diagnosis & allow
intervention.
14

Treatment - in Atheroslerotic RAS
Modify risk factors. Control BP with loop diretics, CCBs,
centrally acting agents, B blockers, Treatment by angioplasty & stenting
OR surgery.
15

Indications for surgery Single kidney with stenosis. Bilateral RAS. Uncontrolled BP/ flash pulm edema. Rapidly deteriorating kidney
function. Meaningful nephron mass in the
kidneys.
16

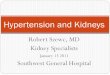
Fibromuscular dysplasia.
Otherwise healthy young women aged 15-50 yrs.
Angiography with “string of beads” pattern
Angioplasy is the treatment.
17

Fibromuscular Dysplasia, before& after PTRA
Atherosclerotic RAS before & after stent
Safian & Textor. NEJM 344:6 18

Initial assessment
Duration of HTN Other CVD risk factors. Anything to suggest secondary HTN.
(50<Age <30, sudden onset, presents as malignant HTN, sudden deterioration in BP control, resistant HTN)
19

Initial evaluation Other contributory factors like –drugs,
overweight, Excess alcohol, excess salt intake, Lack of exercise, Environmental stress, smoking.
Evidence of Complications- stroke, TIA, Carotid bruit, IHD, CHF, Cardiomegaly, PVD, Hypertensive retinopathy, Renal impairment, Proteinuria, Sexual dysfunction.
20

Initial Evaluation
Previous drug treatment and side effects.
Contraindication to specific drugs.
Family history
21

Initial basic investigations
Hematocrit FBS HDL, LDL (after 9-
12 h fast)
TG Cr K Ca
Urinalysis ECG Optional tests:
urinary albumin excretion or ACR
22

Target organ damage Heart- LVH, IHD, LVD,CHF. Brain- Stroke, TIA, Vasular dementia. Kidney- Chronic Kidney Disease. Eyes- Retinopathy. Peripheral Vasculature - Peripheral
arterial disease.
23

24

Treatment Goals
25
Reduce morbidity & mortality Select drug therapy based on evidence
demonstrating risk reduction
Patient Population Target BPMost patients < 140/90 mmHg
DM < 130/80 mmHg
CKD <130/80 mmHg
Chobanian AV, et al. Hypertension 2003;42(6):1206–1252

26

Lifestyle Modifications
27
Modification RecommendationApproximate Systolic BP Reduction (mm Hg)
Weight lossMaintain normal body weight
(BMI 18.5–24.9 kg/m2)5–20 per 10-kg
weight loss
DASH-type diet
Consume a diet rich in fruits, vegetables, and low-fat dairy
products with a reduced content of fat
8–14
Reduced salt intake
Reduce dietary Na intake to no more than 100 mmol per day(2.4 g Na or 6 g NaCl)
2–8
Physical activity
Regular aerobic physical activity (at least 30 min/d, most days of the
week)4–9
Moderation of alcohol intake
Limit consumption to 2 drinks/d in men and 1 drink/d in women &
lighter-weight persons2–4
DASH, Dietary Approaches to Stop Hypertension

28

2929

30

What Drug in CKD
In all proteinuric renal disease ACEI & ARB has a beneficial role.
Dcreases intraglomerular pressure & thus reduce proteinuria.
Dual blockade with ACEI & ARB is a useful combination.
31

In CKD Expect the need of 3 meds. First life style modification. If proteinuria ACEI or ARB. If fluid overload diuretics. If persistant proteinuria add ARB or ACEI. Last vascular smooth muscle relaxant:
Minoxidil
32

Remember side effects
Hyperkalemia (ACE, ARB) Fluid retension (Amlodipine) Bradycardias (B blocker, Clonidine) Massive fluid overload & Tachycardia
(Minoxidil)
33

Antihypertensives - ACEIs No ACEI shown to be superior to any
other ACEI 1˚ goal: treat BP to target 2˚ goal: control proteinuria
ACEIs generally more cost-effective than ARBs
Adverse effects with an ACEI; switch to an ARB may be appropriate
34

Antihypertensives - ACEIsBegin at a low dose; increase dose at
4-week intervals to reduce microalbuminuria (even normotensive patients)
Antiproteinuric effects not necessarily attained at antihypertensive doses
Increase dose until proteinuria reduced by 30-50%
35

Antihypertensives: ARBs
ARBs have similar efficacy to ACEIs for kidney protection in patients with several forms of GN
Proteinuria reduction: 25 to 47% Most clinicians use ACEI/ARB
therapy in patients with nondiabetic CKD & proteinuria
36

Selection of ACEIs vs ARBsCost of therapyPatient toleranceClinician preference
37
Antihypertensives: ARBs

Nondihydropyridine CCBs
Diltiazem/verapamil decrease glomerular injury without negatively changing renal hemodynamics
May have beneficial effects on proteinuria similar to ACEIs
38

Nondihydropyridine CCBs Studies suggest efficacy of
combination therapy with ACEIs & nondihydropyridine CCBs may be superior in proteinuria reduction than either agent alone
Generally 2nd line when ACEIs or ARBs not tolerated
39

40

41

Speculations on JNC VIII
42
Diuretics will remain first line therapy Chlorthalidone vs. HCTZ
Beta blockers will be dropped to 2nd or 3rd line therapy
Combination RAAS inhibition may carry more risk than benefit and will probably not be recommended (some exceptions)
Strong emphasis on combination therapy

43