Embed Size (px)
DESCRIPTION
Journal of Pediatric Surgery (2008) 43, E21–E26www.elsevier.com/locate/jpedsurgFibroepithelial papillomatosis (“skin tags”) in Rabson-Mendenhall syndromeEmily J. Kirby a,⁎, Daniel A. Beals ba bDivision of Plastic Surgery, University of Kentucky, Lexington, KY 40536, USA Division of Pediatric Surgery, University of Kentucky, Lexington, KY 40536, USAKey words:Rabson-Mendenhall syndrome; Skin tag; Fibroepithelial papilloma; Acrochordon; Hyperinsulinemia; Acanthosis nigricans; Diabetes me
Citation preview

www.elsevier.com/locate/jpedsurg
Journal of Pediatric Surgery (2008) 43, E21–E26
Fibroepithelial papillomatosis (“skin tags”) inRabson-Mendenhall syndromeEmily J. Kirbya,⁎, Daniel A. Bealsb
aDivision of Plastic Surgery, University of Kentucky, Lexington, KY 40536, USAbDivision of Pediatric Surgery, University of Kentucky, Lexington, KY 40536, USA
0d
Key words:Rabson-Mendenhallsyndrome;
Skin tag;Fibroepithelial papilloma;Acrochordon;Hyperinsulinemia;Acanthosis nigricans;Diabetes mellitus
Abstract Rabson-Mendenhall syndrome is a rare autosomal recessive syndrome in children involving adefective insulin receptor gene. Several phenotypic features are common to this syndrome, includingsevere hyperinsulinemia, growth retardation, acanthosis nigricans, dental dysplasia, hirsutism, coarsefacial features, and pineal hyperplasia. The authors evaluated and treated a patient with Rabson-Mendenhall syndrome who presented with additional notable syndromic sequelae including extensivefibroepithelial papillomatosis (“skin tags”), not previously described to this extent.© 2008 Elsevier Inc. All rights reserved.
1. Case report
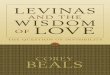
MC is a 9-year-old white male who has been followed bymultiple medical specialties since the time he was diagnosedwith Rabson-Mendenhall syndrome (RMS) several yearsago. MC presented to the pediatric surgery clinic withabundant acrochordons (“skin tags”) that often bled,secondary to the patient's habit of aggravating the lesions.Upon clinical examination, MC exhibits many of thecharacteristics first described by Rabson and Mendenhallin 1955 [1] (Fig. 1). Most notably, MC exhibits a coarse,senile-appearing, and prognathic facies with dental dyspla-sia. His skin is thickened and dry, with acanthosis nigricansin the intertriginous areas of his axillae, neck, and groins.Countless acrochordons cover the axillae, neck, and groin
⁎ Corresponding author.E-mail address: [email protected] (E.J. Kirby).
022-3468/$ – see front matter © 2008 Elsevier Inc. All rights reserved.oi:10.1016/j.jpedsurg.2008.01.001
areas as well as several areas in between (Fig. 2). He ishirsute with a full head of thick hair. Hand and fingernailabnormalities are also present, with short, thick fingers andsmall, brittle fingernails. His stature is short with aprotuberant abdomen and phallic enlargement. As is typicalin RMS patients, MC demonstrates normal intelligence.
MC was taken to the operating room where he wasadministered general endotracheal anesthesia. Initially,Adson forceps were used to retract skin tags for sharpexcision, followed by Bovie electrocautery for hemostasis.With the high volume of lesions to be removed, however,surgical technique was modified so that Bovie cautery wasused to simultaneously excise and cauterize each individualacrochordon. This technique yielded similar and cosmeti-cally acceptable results. Lidocaine-soaked gauze was placedin bilateral axillae and groin regions in efforts to optimizepostoperative pain control.
Removal of the lesions was staged, with acrochordons onthe axilla, neck, chest, and back excised first. This wasfollowed by an additional procedure a fewmonths later during

Fig. 1 Characteristics of Rabson-Mendenhall syndrome. A and B, Coarse, senile-appearing, and prognathic facies, dental dysplasia, andhirsutism. C, Protuberant abdomen. D, Hand and nail abnormalities.
E22 E.J. Kirby, D.A. Beals
which lesions on the patient's groin, genitals, arms, andabdomen were excised (Fig. 3). Approximately 500 lesionswere removed in entirety during the 2 procedures. The patienttolerated the procedures well without any complications.
Twelve months after his initial operative procedure, thepatient returned to the operating room for one of severalotolaryngological procedures. Parents of the child requestedremoval of multiple, recurrent skin lesions while underanesthesia. Results of the examination of the child revealedseveral acrochordons in areas of previous excision, thoughall areas remained much improved from initial consultation
(Fig. 4). There was marked improvement of the acanthosisnigricans in bilateral axillae and neck regions and mildimprovement in bilateral groin regions. Thorough examina-tion revealed that many “recurrent” skin tags were notactually recurrent at all. Comparing photographs, it wasnoted that several of the “recurrent” skin tags were present atthe initial procedure but were not removed at that timebecause of their small size. Several of the new skin tags alsoappear to have emerged from areas of dense acanthosisnigricans, which were not targeted during initial excisions(only acrochordons were targeted excision).

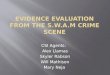
Fig. 2 Preoperative photos detailing the extent of involvement of neck and bilateral axillae (A), left axilla (B), right axilla (C), and bilateralinguinal regions (D).
E23Skin tags in Rabson-Mendenhall syndrome
2. Discussion
Rabson-Mendenhall syndrome is a rare autosomal reces-sive syndrome that exists on a continuum of extreme insulinresistance that includes leprechaunism, RMS, and Type Aform of severe insulin resistance [1]. Type A is the mildestdisease of the three, presenting with insulin resistance andpolycystic ovarian syndrome without obesity [2].
Rabson-Mendenhall syndrome and leprechaunism aresimilar syndromes, differentiated mostly by the severity ofdisease [3]. Patients with leprechaunism perish by 2 years ofage from severe manifestations of extreme insulin resistance[4]. Both syndromes exhibit coarse facies, gingival hyper-plasia, acanthosis nigricans, and extreme insulin resistancewith hyperinsulinemia [5]. Unique to RMS is dentaldysplasia and extreme growth retardation. The lifespan ofRMS patients typically ranges anywhere from 2 years topuberty [6].
Rabson-Mendenhall syndrome is defined by a primarydefect in the insulin receptor [7,8]. Moncada et al (1986) [9]reported a greater than 90% decrease in the number offunctional insulin receptors at the cell surface in RMS anddisproved that accelerated degradation and rate of receptorsynthesis were contributing causes. Kadowaki et al (1990)[8] describe 2 defects in insulin receptor function—impairedposttranslational processing and impaired transport of thereceptor to the plasma membrane. This was noted to result ina reduced number of receptors at the cell surface and a 5-folddecrease in affinity of the receptor for insulin. Longo et al(2002) [10] demonstrated that heterogeneity in the degree ofinsulin resistance in these syndromes exists secondary to thelevel of binding impairment of the receptor. This strength-ened the findings of Takahashi et al (1998) [11] bysuggesting that mutated receptors that allow residual bindingare correlated with longer survival. Extremely impairedinsulin binding yields the most severe phenotype. Unlikeother related endocrine abnormalities, such as diabetes

Fig. 3 Postoperative views of the patient's neck (A), left axilla (B), right axilla (C), right groin (D), and left groin (E).
E24 E.J. Kirby, D.A. Beals
mellitus, the primary defect in the RMS insulin receptor isunaffected by diet and starvation.
Decades ago, researchers began investigating a possiblecorrelation between glucose intolerance and the presence ofacrochordons. Margolis and Margolis (1976) [12] identifiedthis relationship and investigated further. They found that47 of 500 patients had acrochordons, with 34 of them testingpositive for diabetes mellitus (72.3%). Agarwal and Nigam(1987) [13] examined 118 acrochordon patients and foundthat 40.6% of them demonstrated impaired glucose tolerance.In 1995, Thappa [14] examined 5000 referrals, finding 35patients with skin tags, 22 of whom also had tested positivefor diabetes mellitus (62.8%). Demir and Demir (2002) [15]looked at 1250 patients and found that 81.7% of patients withacrochordons demonstrated impaired carbohydrate metabo-lism. Each of these studies attempted to reveal a link betweenimpaired carbohydrate metabolism and the location, size,color, or number of skin tags, but none was established.Demir and Demir (2002) [15] identified a significant
correlation only between elevated body mass index and thenumber of skin tags.
Acrochordons are more common in the presence of ahormone imbalance such as pregnancy or acromegaly [16].Several mechanisms have been proposed to explain this link,including the involvement of growth factors such as epidermalgrowth factor and tissue growth factor α; infective agents suchas human papillomavirus; and neoplasm production andrelease of growth factors. Mathur and Bhargava (1997) [17]suggest that the fibroblast proliferation in syndromes ofinsulin resistance such as RMS is due to hyperinsulinemia thatactivates insulinlike growth factor 1 (IGF-1) on fibroblast cellsurfaces. Neely et al (1991) [18] found that keratinocytegrowth is maximally stimulated by growth factors IGF-1followed by IGF-2 (mediated through the type I IGF receptor).Furthermore, insulin was found to be mitogenic through boththe insulin receptor and the type I IGF receptor, suggesting apotential mechanism for increased production of acrochor-dons associated with hyperinsulinemia.

Fig. 4 Twelve-month follow-up views of the patient's left neck (A), right neck (B), left axilla (C), right axilla (D), right groin (E), and leftgroin (F) (circled areas are marked for reexcision).
E25Skin tags in Rabson-Mendenhall syndrome
To date, treatments for RMS have been ineffective andunpredictable. Insulin-sensitizing oral hypoglycemic agentssuch as the glitazones and metformin have been shown tohave a limited effect on the disease in most cases [19]. U500insulin (500 U in 1 mL) is somewhat effective in limitingpolyuria and glycosuria but does not prevent diabeticcomplications associated with severe insulin resistance[10]. Recombinant IGF-1, thought to act metabolically atthe type I IGF receptor, has had varying results [20].Recently, recombinant human methionyl leptin (r-metHu-Leptin, Amgen Inc, Thousand Oaks, Calif) has been heraldedas an effective therapy in RMS. r-metHuLeptin improvesboth insulin-stimulated hepatic and peripheral glucosemetabolism [21]. Increases in insulin sensitivity are seenafter therapy, though the mechanism remains unclear,possibly related to decreases in liver and muscle triglycerides[22]. Although the treatment appears to be effective, it seems
to be only partial, with RMS patients showing a continuedclinical decline with worsening diabetes and ketoacidosis.
Historically, textbooks agree that acrochordons are“insignificant” and can be removed at will without furtherinvestigation. Research into the correlation between acro-chordons and insulin resistance suggests otherwise. Acro-chordons are routinely treated with simple sharp excision,electrocautery, or cryosurgery using liquid nitrogen. Occa-sionally, a suture is tied at the base of the lesion to causenecrosis and amputation of the lesion. Rarely, however, areacrochordons so abundant that general anesthesia is requiredto tolerate their excision.
It is clear that the presence of acrochordons is notcompletely benign, as once thought. Physicians and surgeonsneed to remain cognizant of the evidence linking theselesions to chronic medical conditions that necessitate earlydiagnosis and treatment. Children who present to surgeons

E26 E.J. Kirby, D.A. Beals
with multiple acrochordons need to be identified forscreening for occult insulin resistance, and body massindex should be addressed. Such patients should beevaluated at regular intervals to monitor for recurrence oflesions. If lesions are treated more often, it is likely thatless invasive measures will be necessary for palliation ofthis condition.
References
[1] Rabson SM, Mendenhall EN. Familial hypertrophy of pineal body,hyperplasia of adrenal cortex and diabetes mellitus. Am J Clin Pathol1955;26:283-90.
[2] Insulin receptor no. 147670: defect in insulin receptor, with insulin-resistant diabetes mellitus, acanthosis nigricans, and Type A. OnlineMendelian Inheritance in Man (OMIM). Johns Hopkins University.Victor A. McKusick. 6/2/1986. http://www.ncbi.nlm.nih.gov/entrez/dispomim.cgi?id=147670.
[3] Donohue WL, Uchida IA. Leprechaunism: a euphemism for a rarefamilial disorder. J Pediatr 1954;45:505-19.
[4] Leprechaunism no. 246200: defect in insulin receptor, with Donohuesyndrome. Online Mendelian Inheritance in Man (OMIM). JohnsHopkins University. Victor A. McKusick: 6/3/1986. http://www.ncbi.nlm.nih.gov/entrez/dispomim.cgi?id=246200.
[5] Kumar S, Tullu MS, Muranjan MN, et al. Rabson-Mendenhallsyndrome. Indian J Med Sci 2005;59:70-3.
[6] Rabson-Mendenhall syndrome. No. 262190: pineal hyperplasia,insulin-resistant diabetes mellitus, and somatic abnormalities. OnlineMendelian Inheritance in Man (OMIM). Johns Hopkins University.Victor A. McKusick. 6/4/1986. http://www.ncbi.nlm.nih.gov/entrez/dispomim.cgi?id=262190.
[7] Takata Y, Kobayashi M, Maegawa H, et al. A primary defect in insulinreceptor in a young male patient with insulin resistance. Metabolism1986;35:950-5.
[8] Kadowaki T, Kadowaki H, Accili D, et al. Substitution of lysine forasparagine at position 15 in the alpha-subunit of the human insulin
receptor: a mutation that impairs transport of receptors to the cellsurface and decreases the affinity of insulin binding. J Biol Chem1990;265:19143-50.
[9] Moncada VY, Hedo JA, Serrano-Rios M, et al. Insulin-receptorbiosynthesis in cultured lymphocytes from an insulin-resistant patient(Rabson-Mendenhall syndrome): evidence for defect before insertionof receptor into plasma membrane. Diabetes 1986;35:802-7.
[10] Longo N, Wang Y, Smith SA, et al. Genotype-phenotype correlation ininherited severe insulin resistance. Hum Mol Genet 2002;11:1465-75.
[11] Takahashi Y, Kadowaki H, Ando A, et al. Two aberrant splicingscaused by mutations in the insulin receptor gene in culturedlymphocytes from a patient with Rabson-Mendenhall's syndrome.J Clin Invest 1998;101:588-94.
[12] Margolis J, Margolis LS. Skin tags—a frequent sign of diabetesmellitus. New Engl J Med 1976;294:1184.
[13] Agarwal JK, Nigam PK. Acrochordon: a cutaneous sign ofcarbohydrate intolerance. Australas J Dermatol 1987;28:132-3.
[14] Thappa DM. Skin tags as markers of diabetes mellitus: anepidemiological study in India. J Dermatol 1995;22:729-31.
[15] Demir S, Demir Y. Acrochordon and impaired carbohydratemetabolism. Acta Diabetologica 2002;39:57-9.
[16] Nabarro JDN. Acromegaly: review. Clin Endocrinol 1987;26:481-512.[17] Mathur SK, Bhargava P. Insulin resistance and skin tags. Dermatology
1997;195:184.[18] Neely EK, Morhenn VB, Hintz RL, et al. Insulin-like growth factors
are mitogenic for human keratinocytes and a squamous cell carcinoma.J Invest Dermatol 1991;96:104-10.
[19] Musso C, Cochran E, Moran SA, et al. Clinical course of geneticdiseases of the insulin receptor (Type A and Rabson-Mendenhallsyndromes): a 30-year prospective. Medicine 2004;83:209-22.
[20] Quin JD, Fisher BM, Paterson KR, et al. Acute response torecombinant insulin-like growth factor I in a patient with Mendenhall'ssyndrome. N Engl J Med 1990;323:1425-6.
[21] Cochran E, Young JR, Sebring N, et al. Efficacy of recombinantmethionyl human leptin therapy for the extreme insulin resistanceof the Rabson-Mendenhall syndrome. J Clin Endocrinol Metab2004;89:1548-54.
[22] Petersen KF, Oral EA, Dufour S, et al. Leptin reverses insulinresistance and hepatic steatosis in patients with severe lipodystrophy.J Clin Invest 2002;109:1345-50.









![[Beals R., Wong R.] Special Functions a Graduate](https://img.pdfslide.net/doc/110x75/577cc3071a28aba71194fdfe/beals-r-wong-r-special-functions-a-graduate.jpg)