Embed Size (px)
Citation preview
Knowledge translation and implementation of frontline screening and early intervention for substance abuse: why are we moving slowly?
Emily Campbell, MPHCIHR Team in Substance Abuse Treatment
Research Coordinator, Addictions UnitMcGill University Health Centre (MUHC)
CIHR Team in Substance Abuse Treatment
Kathryn Gill, PhD (MUHC)Gail Gauthier, PhD (MUHC)Dara Charney, MD (MUHC)
Spyridoula Xenocostas, MSc (CSSS de la Montagne (DLM))
Ann Macaulay, CM, MD (Participatory Research at McGill
(PRAM))
Marlene Yuen, BA (CSSS DLM) Donald Desrosiers, RN (CSSS DLM)
Anita Cugliandro, MA (CSSS DLM)Jon Salsberg, PhD(c) (PRAM) Jorge Palacios-Boix, MD (MUHC)
Ronald Fraser, MD (MUHC) Juan C. Negrete, MD (MUHC)
Co-Investigators Collaborators
Research Coordinator: Emily Campbell, MPHAddiction Program Coordinator: Antonis Paraherakis, MSc
Research Assistant: Katie Boodhoo, BScFocus Group Leader, Qualitative & Quantitative Data Analysts
Rationale for the CIHR Team Project
Natural laboratory for studying the implementation of evidence-based interventions within multiple primary care sites
New provincial action plans and mandates in addictions from the Quebec government
Screening, early (brief) intervention and referral to treatment
Why screen in primary care settings?
misuse of alcohol and other drugs is prevalent in many clinical settings
substance use often linked to presenting symptoms (e.g. injuries, hypertension, family problems, depression)
given the setting, clinicians have a mandate to assess, and ask questions related to risky behaviour
stigma can be minimized in non-specialized settings detection of those at risk is a form of early
intervention and secondary prevention
Evidence-based screening & brief intervention
WHO Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) and the ASSIST-linked brief interventions. http://www.who.int/substance_abuse/publications/media_assist/en/index.html
Integrated Knowledge Translation
Those who must live with the results of the innovation must be involved in the design and execution of its implementation, to facilitate ownership and to decrease resistance .
(Backer et al., 1995)
Collaborative Partnership: Throughout the process of program implementation, the CIHR TEAM has used an integrated knowledge translation (iKT) strategy equal partners build collaborative mechanisms for knowledge
exchange joint decision making between researchers,
clinic supervisors, psychiatrists, addiction specialists and frontline clinicians
integrated approach with the insertion of an addictions specialist into the CSSS for 18 months
Project Overview at CSSS
Time 1 (2010): Pre-implementation data collection: 34 participants (clinicians/managers): focus groups, interviews, (explored knowledge, skills, attitudes, barriers, training needs); questionnaires, chart review
Training Program Implementation (2010-11): Addictions Program Coordinator on site to help train and support staff and program development
Time 2 (2011): Post-data collection: 34 participants Time 3 (2013): Internal Addictions Specialist: Training,
consultation, co-intervention and support, questionnaire
Portrait of Current Practice
Use of formal screening tools for alcohol/drugs is rare resistance to using formal tools
Most clinicians do not feel adequately equipped to deal with clients with substance problems inadequately equipped to deal with dual diagnosis
Competing priorities; clients often present in crisis Lack of knowledge of evidence-based practices for
substance abuse
Summary of Clinician Needs
Practical, up-to-date knowledge of substance abuse/addictions: case based, clinical practice
Intervening with co-morbid substance abuse and psychiatric problems
Motivational approaches; dealing with resistance Supervision by an Addictions Specialist New screening tool: simple, clear, quick, practical Improved collaboration with external resources
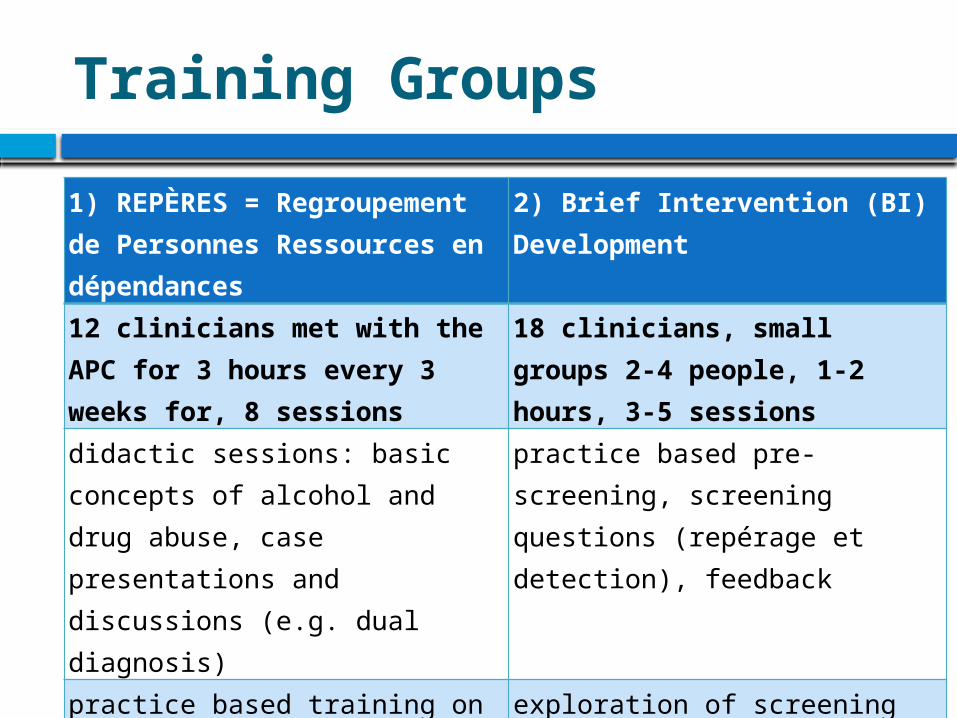
Training Groups
1) REPÈRES = Regroupement de Personnes Ressources en dépendances
2) Brief Intervention (BI) Development
12 clinicians met with the APC for 3 hours every 3 weeks for, 8 sessions
18 clinicians, small groups 2-4 people, 1-2 hours, 3-5 sessions
didactic sessions: basic concepts of alcohol and drug abuse, case presentations and discussions (e.g. dual diagnosis)
practice based pre-screening, screening questions (repérage et detection), feedback
practice based training on screening methods (DEBA-A/D, WHO ASSIST)
exploration of screening for psychiatric problems (depression, anxiety, psychotic disorders, internet use)
referral to specialized treatment centres (decision tree)
development of intervention plan and BI sessions
Changes from Time 1 to Time 2
Changes in attitudes: heightened awareness regarding addictions; increased comfort and openness in addressing substance abuse
Minimal change in actual interventions Tool Use: little use of screening tools Training group knowledge transfer was limited Systematic screening and brief interventions not
implemented (pre-screening implemented in 2012) Full-time internal addictions worker: training/co-
intervention
Lessons Learned
Didactic training methods (lectures, powerpoint presentations) are not preferred by frontline staff, material considered to be too complex/theoretical not able to retain or use information
Case presentations and discussion + ongoing case based supervision was the preferred method of learning and considered to be most useful
Follow-up supervision post training Adoption time frame for new practices is much slower
than expected
Slow Adoption Time Frame – Why?
Difficult to implement? specialized training and on-going supervision required;
lack of knowledge: many staff do not have the skills to appraise, apply and understand evidence-based practices
Organizational climate? lack of time, lack of staff/turnover, lack of managerial
support, competing priorities, lack of access to resources Incompatibility with clinicians’ beliefs?
screening and brief interventions conflict with belief that substance abuse is difficult to treat, requires lengthy treatment; focus on client priorities
Emily Campbell, MPHResearch Coordinator, Addictions Unit
McGill University Health Centre [email protected]
Questions?
Thank you!