Embed Size (px)
Citation preview

Koronare Revaskularisation
4 Jahre nach Syntax: PCI versus Bypass
Prof Dr Jochen WöhrleProf. Dr. Jochen WöhrleKlinik für Innere Medizin II
Universitätsklinikum Ulm
Chiemgauer Kardiologie Tage 2012

Two goals of therapy in patients with stableangina and coronary artery diseaseangina and coronary artery disease
1.Improve symptoms and quality of life (soft
)endpoints)
2 Improve prognosis (hard endpoints)2.Improve prognosis (hard endpoints)

ESC guidelines 2010

Koronare Revaskularisation
4 Jahre nach Syntax: PCI versus Bypass
• Koronare 3‐Gefäßerkrankung• Hauptstammstenose plus 1, 2 oder 3‐
Gefäßerkrankungg• Druckdraht – Fame
L itli i d ESC• Leitlinien der ESC• „Langzeit“‐Follow‐up (4 Jahre)

N=2776
76%
Prior coronary artery bypass grafting was the only variable independently associated with
Cavender et al, Am Heart J 2009; 158:933‐40
protection from death, cardiac rehospitalization, and late revascularization.






• Koronare 3‐Gefäßerkrankung
H l 1 2 d 3• Hauptstammstenose plus 1, 2 oder 3‐
GefäßerkrankungGefäßerkrankung
• Druckdraht – Fame
• Leitlinien der ESC
• „Langzeit“‐Follow‐up (4 Jahre)








Global Risk Score


48%48%

ESC guidelines 2010

ESC guidelines 2010

• Koronare 3‐Gefäßerkrankung
H l 1 2 d 3• Hauptstammstenose plus 1, 2 oder 3‐
GefäßerkrankungGefäßerkrankung
• Druckdraht – Fame
• Leitlinien der ESC
• „Langzeit“‐Follow‐up (4 Jahre)

Fraktionelle Flussreserve (FFR) - Definition / Messung
Die FFR ist der Quotient
maximal erreichbare Blutfluss in einem stenosierten Gefäß * maximalen Blutfluss in dem gleichen Gefäß ohne Stenose
PPa (MIt dem Katheter gemessener Aortendruck)
FFR =Pd (Mit dem Druck-
draht gemessenerdistaler Druck )PdFFR = Pa
d
* Unter maximaler Hyperämie
25

Tonino et al, NEJM 2009

Angiographic vs. Functional severity of CAD
of 509 patients with angiographically‐defined MVDof 509 patients with angiographically defined MVD 46% had „functional MVD“
Tonino et al, NEJM 2009

Downgrading MVD
86% 3VD and 57% 2VS reclassified86% 3VD and 57% 2VS reclassified
Tonino et al, J Am Coll Cardiol 2010

Change in SYNTAX Score after FFR
Nam et al, J Am Coll Cardiol 2011;58:1211‐8

CARDia
• 18‐80 years
Si ifi CAD i bl f PCI d CABG• Significant CAD suitable for PCI and CABG
proximal / complex LADproximal / complex LAD
2 or 3 VD
• Diabetes mellitus
• Stable angina or NSTEMI
ESC 2012





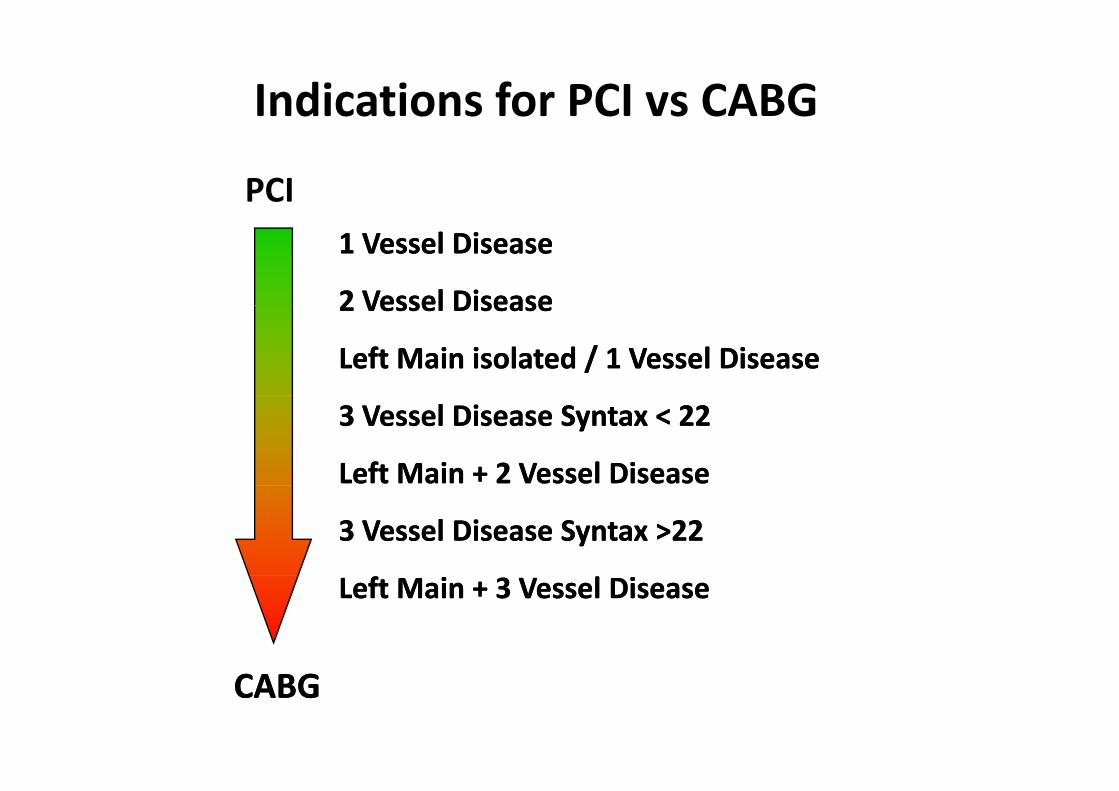
Indications for PCI vs CABG
PCI1 1 VesselVessel DiseaseDisease
22 VesselVessel DiseaseDisease2 2 VesselVessel DiseaseDisease
LeftLeft Main Main isolatedisolated / 1 / 1 VesselVessel DiseaseDisease
3 3 VesselVessel DiseaseDisease Syntax < 22Syntax < 22
LeftLeft Main + 2 Main + 2 VesselVessel DiseaseDisease
3 3 VesselVessel DiseaseDisease Syntax >Syntax >2222
LeftLeft Main + 3 Main + 3 VesselVessel DiseaseDisease
CABGCABG

Summary• PCI and CABG are complementary
Th j it f ti t ith 3VD d LM b fit f CABG• The majority of patients with 3VD and LM benefit from CABG• PCI can be performed in 30‐40% according to the SYNTAX study with
similar results
• Anatomical complexity (Syntax) and clinicalsituation (EuroScore) have to be consideredsituation (EuroScore) have to be considered
• Use FFR for downgrading of MVD to focust t t l t l i ith b fit ftreatment on relevant lesions with benefit forour patients
• Scores do not replace clinical judgment• Long‐term follow‐ups are important for ourLong term follow ups are important for our
patients.