Embed Size (px)
DESCRIPTION
fkkkkkkk
Citation preview

Irwan M. Loebis, dr., SpJP
ELECTROCARDIOGRAPHY
UNSWAGATI, CIREBONUNSWAGATI, CIREBON

Lecture outlinePart oneInformation provided by ECGCardiac conduction system: anatomy and
physiology (Normal) ECG interpretationPart two Abnormal ECG

ECG is…?Printout as a result of a particular
electrical function of the heart
The standard 12-lead electrocardiogram is a representation of the heart's electrical activity recorded from electrodes on the body surface

Information provided by Information provided by ECG: what do you think?ECG: what do you think?

Cardiac conduction system
SA nodeAV nodeBundle His

Impulse Transmission
SA Node Internodal branch AV Node Hiss Bundle Purkinje Fiber Contraction


the sequentialactivation (depolarization) of the right
and left atria
right and left ventricular depolarization (normally the ventricles are activated simultaneously)
ventricular repolarization
One ‘complex’ of ECG waveform

Leads positionLeads position

Limb leadsLimb leads

Einthoven Triangle

Chest lead

Chest leadChest lead

Chest leadChest lead

ECG interpretation…?1. Calibration2. Rate and rhythm3. QRS axis4. P morphology5. PR interval6. QRS duration7. QRS morphology8. ST segment morphology9. T morphology10. U morphology11. Others: LVH, LV strain, BBB, QT interval12. Conclusion: normal/abnormal

Calibration1 mV = 1 cmImportant in
assessing tall waves in hypertrophic state

Paper speed and normal value
One small box: 0.04 sOne small box: 0.04 sOne large box: 0.2 sOne large box: 0.2 sPR Interval: 0,12’’ - PR Interval: 0,12’’ - 0,20’’0,20’’QRS duration: 0,04’’ - QRS duration: 0,04’’ - 0,12’’0,12’’

Rate calculation Method:
300 divided by number of large boxes between R-R
1500 divided by number of small boxes between R-R,
Number of QRS complexes in 6 seconds times 10.

Rate calculationpaper 25 mm/s

Sinus Rhythm Sinus Rhythm
Rhythm: RegularRate: 60 – 100P wave: Normal in configuration; precede each QRSPR: Normal (0. 12 – 0.20 s)QRS: Normal (<0.12 s)

QRS Axis (N: - 30 s/d + 110)

P wave Wave of atrial depolarization Normal characteristic:1. Smooth and rounded2. ≤ 3 mm tall3. Upright in leads I, II avF

PR intervalIncluding P wave until the beginning of QRS
complexNormal duration is 0.12-0.2 seconds

QRS complex Wave of ventricular depolarization 5-20 mm tall Duration 0.06-0.10 seconds

QRS morphology qRs Rs R rS
QR Q/QS RsR’ rSr’

ST segmentBegins at J pointBetween ventricular depolarization and
ventricular repolarizationGenerally isoelectric

T wave Ventricular repolarization, followed by
ventricular relaxation Positive in lead : I, II, V3-V6 Negative in lead avR

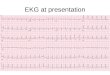
Interpret this ECG..

And this..

Abnormal ECG Myocardial ischemia/infarct Hyperthrophy Hyperkalemia Arrhythmia

ACUTE CORONARY SYNDROMEACUTE CORONARY SYNDROME
No ST ElevationNo ST Elevation ST ElevationST Elevation
Unstable Angina
NSTEMI

Acute myocardial infarction

STEMI Non STEMI



Mid LAD occlusion after the first septal perforator (arrow) ECG : large anterior MI

Occlusion of diagonalbranch ( arrow )
ST elevation in I and aVL

ECG demonstrates large anterior infarction


Proximal large RCA occlusion
ST elevation in leads II, III, aVF, V5, and V6 with precordial ST depression

Small inferior distal RCA occlusion
ECG changes in leads II, III, and aVF


Acute inferoposterior MI






Questions…??

• Peaking T• Shortening QT interval
• Widening P wave, QRS complex• Prolongation PR interval
HIPERKALEMIA


PPM

How to identify arrhythmias ?

QRS complex Regular / irregular ?
QRS complexNormal-looking QRS complex?
Wide / narrow ?
P wave ?
Relationship between P and QRS ?

NORMAL SINUS RHYTHM

PSVT :-due to re-entry mechanism-narrow QRS complex-regular-retrograde atrial depolarization-P wave ?

PSVT

Atrial Fibrillation :
-from multiple area of re-entry within atria-or from multiple ectopic foci-irregular, narrow QRS complex-very rapid atrial electrical activity (400-700 x/min).-no uniform atrial depolarization

Atrial Flutter :
-The result of a re-entry circuit within the atria-Irregular / regular QRS rate-Narrow QRS complex-Rapid P waves (300x/min), “sawtooth”

Junctional rhythm:-AV junction can function as a pace maker (40-60 x/min).-due to the failure of sinus node to initiate time impulse or conduction problem.-normal-looking QRS.-retrograde P wave.-P wave may preceede, coincide with, or follow the QRS

VES
SR

SR SR SR SRSR SR
VES VES
Sinus rhythm with Multifocal VES

Sinus rhythm with VES couplet

Sinus Rhythm with VES, R on T

Ventricular Tachycardia



Torsade de Pointes

Ventricular Fibrillation


Prolonged PR interval
1st degree AV block

Missing QRS Missing QRS
2nd degree AV block, type 1

2nd degree AV block, type 2
Missing QRS

P P P P P P P
QRS QRS QRS
Total AV Block / 3rd degree AV block

![KULIAH CARDIO1 baru.ppt [Read-Only] - ocw.usu.ac.idocw.usu.ac.id/.../kesehatan_anak_slide_kardiologi_anak1.pdf · EKG / Ro N AUSKULTASI JANTUNG A. B.JTG I :PENUTUPAN KATUP MITRAL](https://img.pdfslide.net/doc/110x75/5b0e15c67f8b9a8b038e9e2d/kuliah-cardio1-baruppt-read-only-ocwusuacidocwusuacidkesehatananakslidekardiologianak1pdfekg.jpg)
























![kuliah coass 5 [ekg dasar].ppt](https://img.pdfslide.net/doc/110x75/56d6be221a28ab301690c44d/kuliah-coass-5-ekg-dasarppt.jpg)