Embed Size (px)
Citation preview
KYLA PATTERSON, M.S.CREATING CONNECTIONS TO SHINING
STARS CONFERENCEJULY 24 , 2013
How to Implement Family Cost Share Practices in Real Family
Situations
Principles
No child denied services due to inability to pay
Families understand their options and implications of choices … informed consent
Agreement regarding family’s financial obligation is in writing
Family cost share practices are standard and equitable
Reminders
Services at no cost – Service coordination, eligibility determination, assessment, IFSP development
All other services subject to family cost share practices
Sliding Fee Scale available to establish monthly cap based on family size and taxable income
Fee appeal process availableDispute resolution available
For Families
No Insurance
Scenario:
No Insurance
Income $60,000
Family size: 4
Checklist
Intake Notice and explanation
Prior to IFSP Meeting Further explanation Complete Agreement form
At Annual Notice and explanation Complete new Agreement form
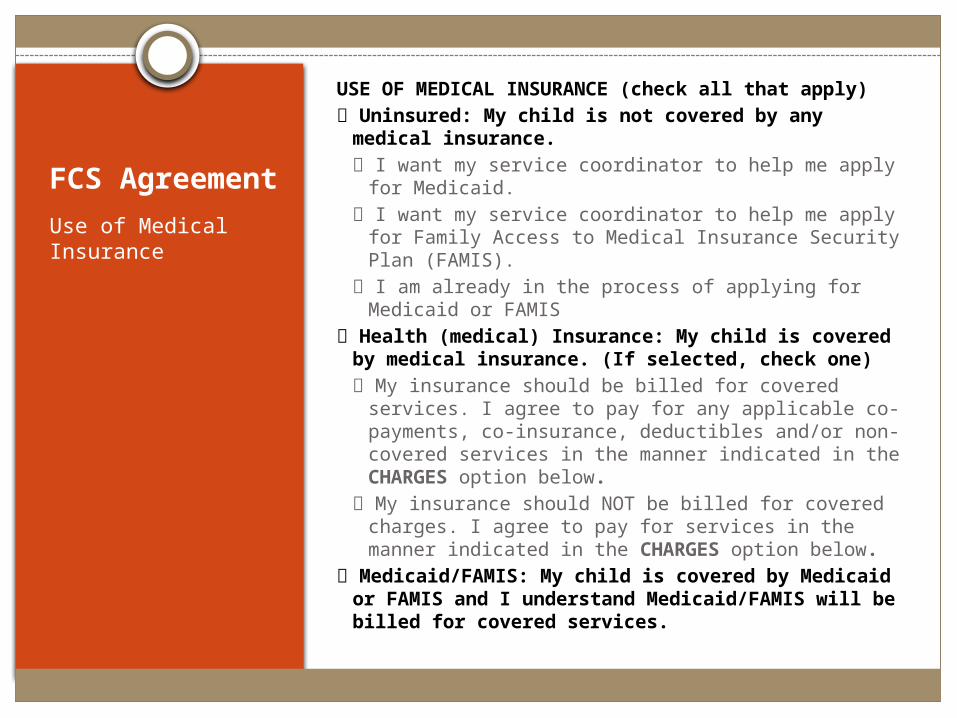
FCS Agreement
Use of Medical Insurance
USE OF MEDICAL INSURANCE (check all that apply) Uninsured: My child is not covered by any medical
insurance. I want my service coordinator to help me apply for
Medicaid. I want my service coordinator to help me apply for
Family Access to Medical Insurance Security Plan (FAMIS).
I am already in the process of applying for Medicaid or FAMIS
Health (medical) Insurance: My child is covered by medical insurance. (If selected, check one) My insurance should be billed for covered services. I
agree to pay for any applicable co-payments, co-insurance, deductibles and/or non-covered services in the manner indicated in the CHARGES option below.
My insurance should NOT be billed for covered charges. I agree to pay for services in the manner indicated in the CHARGES option below.
Medicaid/FAMIS: My child is covered by Medicaid or FAMIS and I understand Medicaid/FAMIS will be billed for covered services.
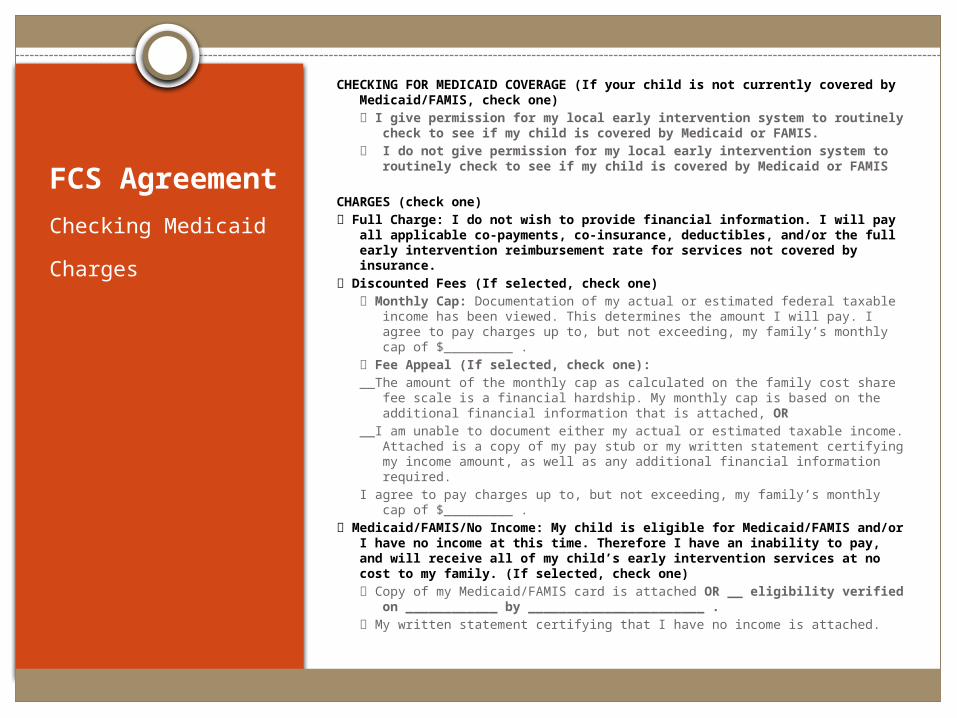
FCS Agreement
Checking Medicaid
Charges
CHECKING FOR MEDICAID COVERAGE (If your child is not currently covered by Medicaid/FAMIS, check one) I give permission for my local early intervention system to routinely
check to see if my child is covered by Medicaid or FAMIS. I do not give permission for my local early intervention system to
routinely check to see if my child is covered by Medicaid or FAMIS
CHARGES (check one) Full Charge: I do not wish to provide financial information. I will pay all
applicable co-payments, co-insurance, deductibles, and/or the full early intervention reimbursement rate for services not covered by insurance.
Discounted Fees (If selected, check one) Monthly Cap: Documentation of my actual or estimated federal taxable
income has been viewed. This determines the amount I will pay. I agree to pay charges up to, but not exceeding, my family’s monthly cap of $_________ .
Fee Appeal (If selected, check one):__The amount of the monthly cap as calculated on the family cost share fee
scale is a financial hardship. My monthly cap is based on the additional financial information that is attached, OR
__I am unable to document either my actual or estimated taxable income. Attached is a copy of my pay stub or my written statement certifying my income amount, as well as any additional financial information required.
I agree to pay charges up to, but not exceeding, my family’s monthly cap of $_________ .
Medicaid/FAMIS/No Income: My child is eligible for Medicaid/FAMIS and/or I have no income at this time. Therefore I have an inability to pay, and will receive all of my child’s early intervention services at no cost to my family. (If selected, check one) Copy of my Medicaid/FAMIS card is attached OR __ eligibility verified on
____________ by _______________________ . My written statement certifying that I have no income is attached.
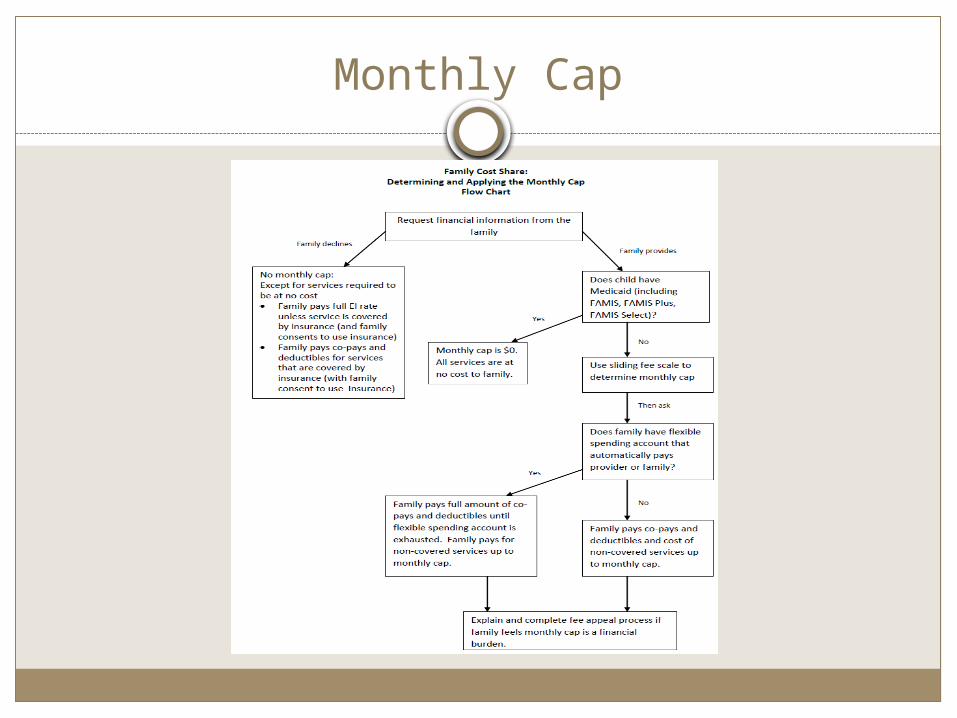
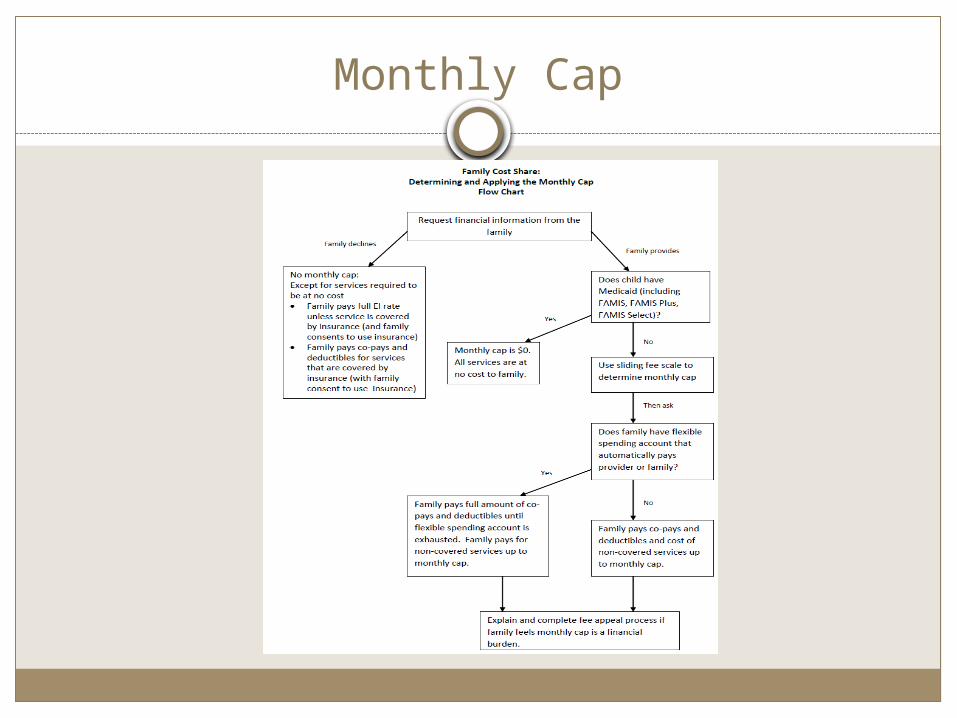
Monthly Cap
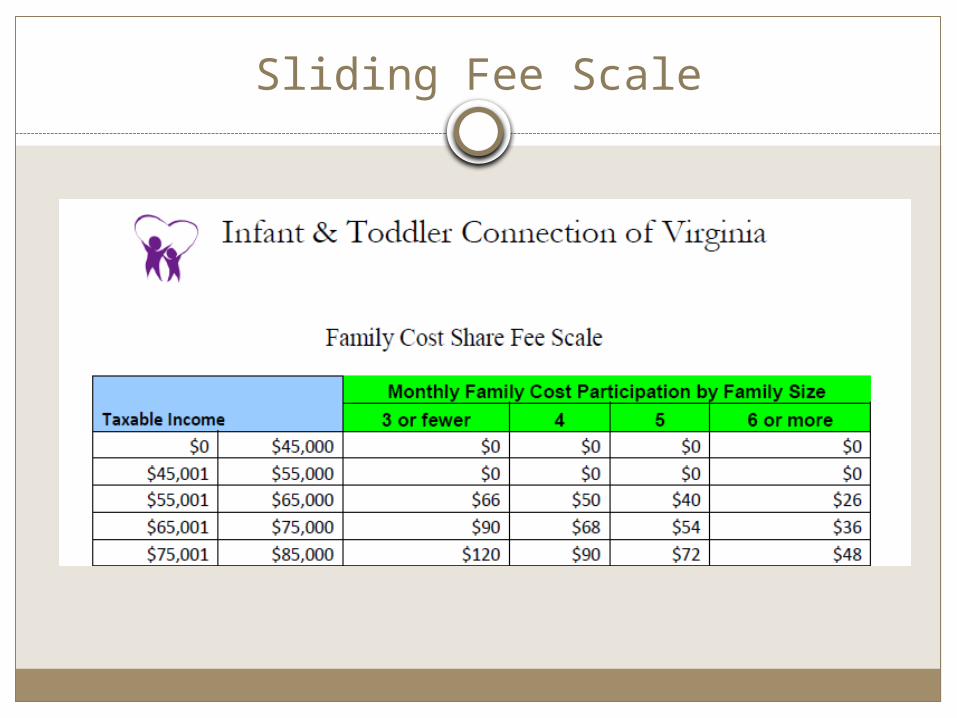
Sliding Fee Scale
FCS Agreement
Flexible Spending Account
Statements of Agreement
These sections are completed the same way for all families
Flexible spending account section explains requirements. Must check the box for all families.

Medicaid/FAMIS
Scenario:
Child covered by Medicaid
Income $30,000
Family Size: 3
Reminders for Use of Medicaid
Consent requirements Does not have Medicaid yet Release of information for billing
No cost protectionsMust provide written notice to parents

Checklist
Intake: Complete Family Cost Share Agreement Consent to release personally identifiable information
for billing Medicaid number in ITOTS
Service Delivery Confirm Medicaid coverage at least monthly
FCS Agreement
Use of Medical Insurance
USE OF MEDICAL INSURANCE (check all that apply) Uninsured: My child is not covered by any medical
insurance. I want my service coordinator to help me apply for
Medicaid. I want my service coordinator to help me apply for
Family Access to Medical Insurance Security Plan (FAMIS).
I am already in the process of applying for Medicaid or FAMIS
Health (medical) Insurance: My child is covered by medical insurance. (If selected, check one) My insurance should be billed for covered services. I
agree to pay for any applicable co-payments, co-insurance, deductibles and/or non-covered services in the manner indicated in the CHARGES option below.
My insurance should NOT be billed for covered charges. I agree to pay for services in the manner indicated in the CHARGES option below.
Medicaid/FAMIS: My child is covered by Medicaid or FAMIS and I understand Medicaid/FAMIS will be billed for covered services.
FCS Agreement
Checking Medicaid
Charges
CHECKING FOR MEDICAID COVERAGE (If your child is not currently covered by Medicaid/FAMIS, check one) I give permission for my local early intervention system to routinely
check to see if my child is covered by Medicaid or FAMIS. I do not give permission for my local early intervention system to
routinely check to see if my child is covered by Medicaid or FAMIS
CHARGES (check one) Full Charge: I do not wish to provide financial information. I will pay all
applicable co-payments, co-insurance, deductibles, and/or the full early intervention reimbursement rate for services not covered by insurance.
Discounted Fees (If selected, check one) Monthly Cap: Documentation of my actual or estimated federal taxable
income has been viewed. This determines the amount I will pay. I agree to pay charges up to, but not exceeding, my family’s monthly cap of $_________ .
Fee Appeal (If selected, check one):__The amount of the monthly cap as calculated on the family cost share fee
scale is a financial hardship. My monthly cap is based on the additional financial information that is attached, OR
__I am unable to document either my actual or estimated taxable income. Attached is a copy of my pay stub or my written statement certifying my income amount, as well as any additional financial information required.
I agree to pay charges up to, but not exceeding, my family’s monthly cap of $_________ .
Medicaid/FAMIS/No Income: My child is eligible for Medicaid/FAMIS and/or I have no income at this time. Therefore I have an inability to pay, and will receive all of my child’s early intervention services at no cost to my family. (If selected, check one) Copy of my Medicaid/FAMIS card is attached OR __ eligibility verified on
____________ by _______________________ . My written statement certifying that I have no income is attached.
FCS Agreement
Information Release
Private Insurance
Scenario:
Agree to use private insurance
Income: $90,000
Family Size: 6
Flexible spending account that auto-pays provider: $500
Reminders for Use of Private Insurance
Written consent requiredMust provide copy of family cost share
policies when seeking consentMust identify potential costs for use of
private insurance
Checklist
Intake/Prior to IFSP Explain potential costs of using insurance
IFSP Review New consent if services are increasing
Service Delivery Confirm at least monthly whether insurance has
changed
FCS Agreement
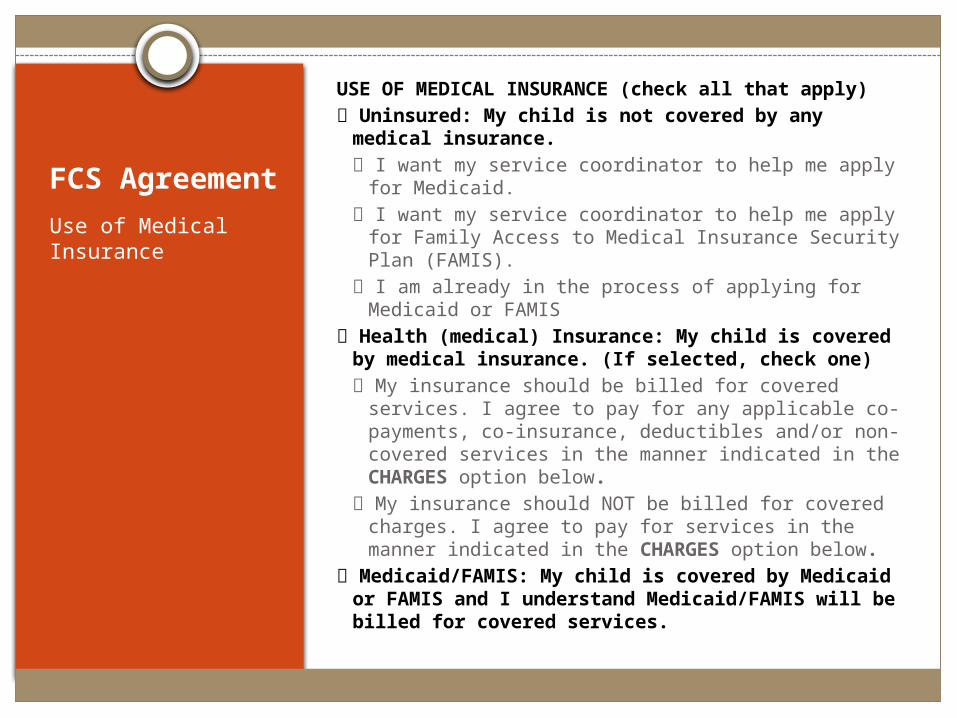
Use of Medical Insurance
USE OF MEDICAL INSURANCE (check all that apply) Uninsured: My child is not covered by any medical
insurance. I want my service coordinator to help me apply for
Medicaid. I want my service coordinator to help me apply for
Family Access to Medical Insurance Security Plan (FAMIS).
I am already in the process of applying for Medicaid or FAMIS
Health (medical) Insurance: My child is covered by medical insurance. (If selected, check one) My insurance should be billed for covered services. I
agree to pay for any applicable co-payments, co-insurance, deductibles and/or non-covered services in the manner indicated in the CHARGES option below.
My insurance should NOT be billed for covered charges. I agree to pay for services in the manner indicated in the CHARGES option below.
Medicaid/FAMIS: My child is covered by Medicaid or FAMIS and I understand Medicaid/FAMIS will be billed for covered services.
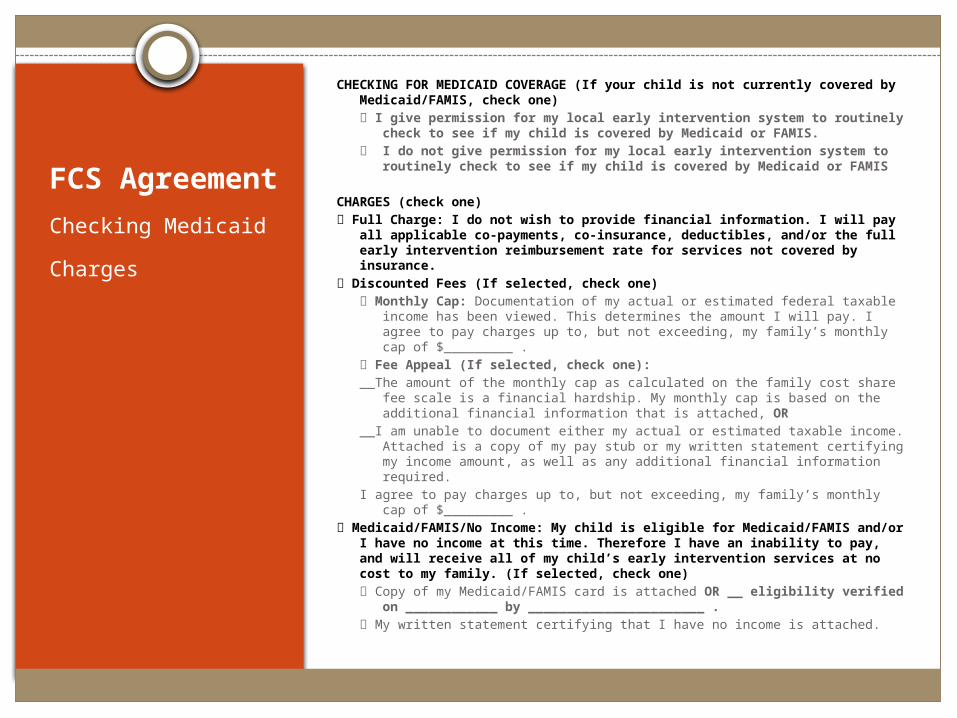
FCS Agreement
Checking Medicaid
Charges
CHECKING FOR MEDICAID COVERAGE (If your child is not currently covered by Medicaid/FAMIS, check one) I give permission for my local early intervention system to routinely
check to see if my child is covered by Medicaid or FAMIS. I do not give permission for my local early intervention system to
routinely check to see if my child is covered by Medicaid or FAMIS
CHARGES (check one) Full Charge: I do not wish to provide financial information. I will pay all
applicable co-payments, co-insurance, deductibles, and/or the full early intervention reimbursement rate for services not covered by insurance.
Discounted Fees (If selected, check one) Monthly Cap: Documentation of my actual or estimated federal taxable
income has been viewed. This determines the amount I will pay. I agree to pay charges up to, but not exceeding, my family’s monthly cap of $_________ .
Fee Appeal (If selected, check one):__The amount of the monthly cap as calculated on the family cost share fee
scale is a financial hardship. My monthly cap is based on the additional financial information that is attached, OR
__I am unable to document either my actual or estimated taxable income. Attached is a copy of my pay stub or my written statement certifying my income amount, as well as any additional financial information required.
I agree to pay charges up to, but not exceeding, my family’s monthly cap of $_________ .
Medicaid/FAMIS/No Income: My child is eligible for Medicaid/FAMIS and/or I have no income at this time. Therefore I have an inability to pay, and will receive all of my child’s early intervention services at no cost to my family. (If selected, check one) Copy of my Medicaid/FAMIS card is attached OR __ eligibility verified on
____________ by _______________________ . My written statement certifying that I have no income is attached.
Monthly Cap
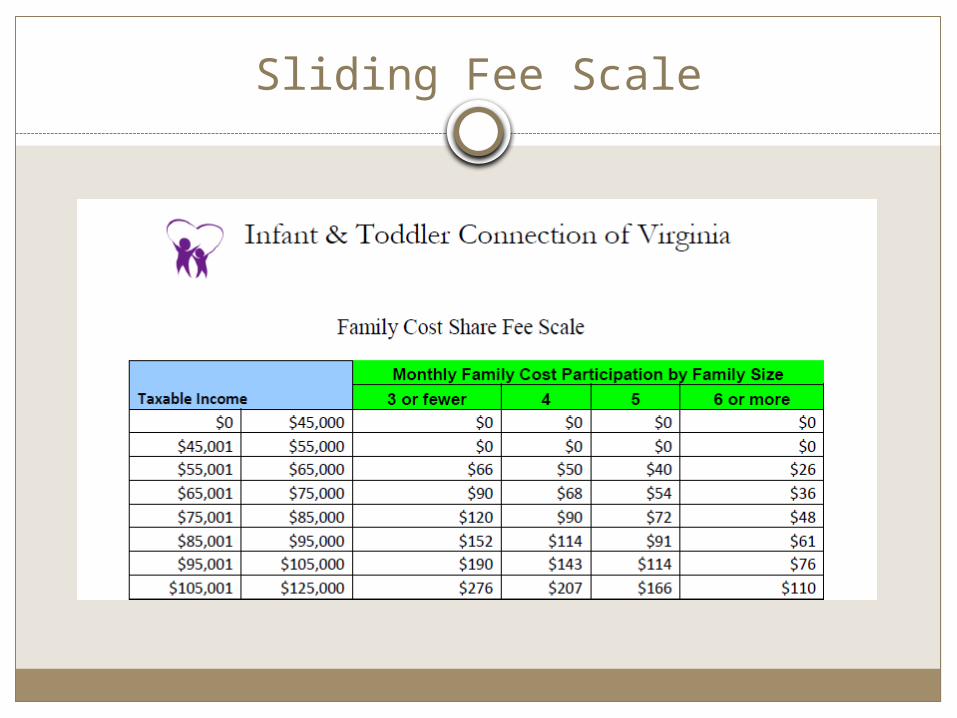
Sliding Fee Scale
FCS Agreement
Flexible Spending Account
Explain carefully.Family will need to pay full
amount of co-pays and deductibles until the $500 is gone.
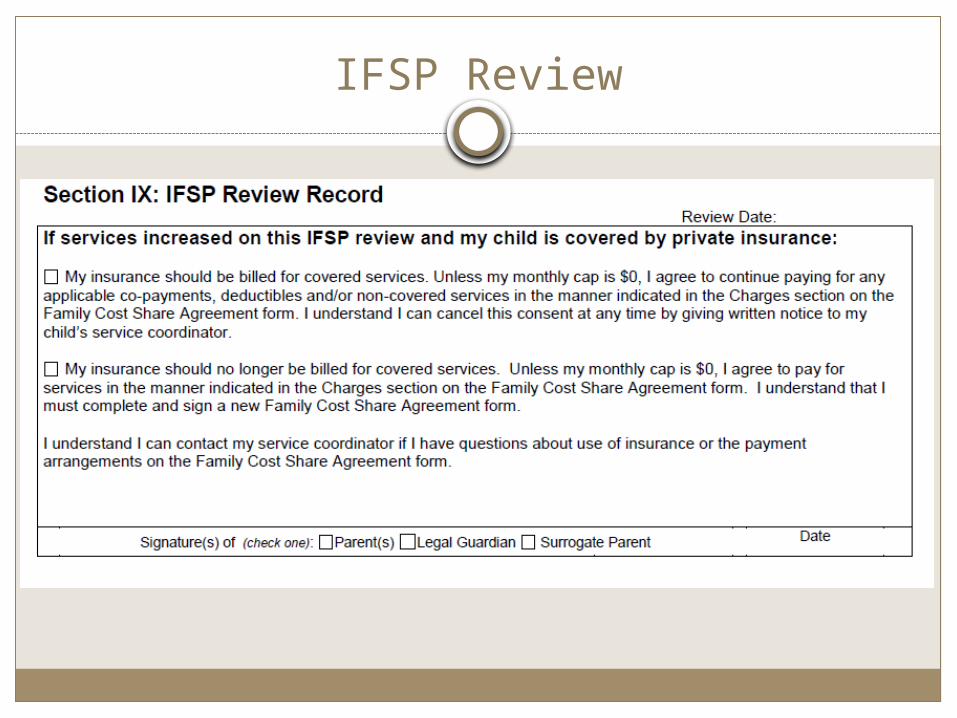
IFSP Review
Preparing for IFSP Review
Review current Agreement ahead of meetingDiscuss options ahead of meeting, if
appropriateBring copy of current AgreementBring a blank Agreement form

Private Insurance and Medicaid
Private Insurance
Medicaid
Income $50,000
Family Size: 5
No flexible spending account
Checklist
Intake Explain both Medicaid and private insurance
information Complete Family Cost Share Agreement
IFSP Review New consent if services increasing
Service Delivery Confirm Medicaid and private insurance coverage at
least monthly
FCS Agreement
Use of Medical Insurance
USE OF MEDICAL INSURANCE (check all that apply) Uninsured: My child is not covered by any medical
insurance. I want my service coordinator to help me apply for
Medicaid. I want my service coordinator to help me apply for
Family Access to Medical Insurance Security Plan (FAMIS).
I am already in the process of applying for Medicaid or FAMIS
Health (medical) Insurance: My child is covered by medical insurance. (If selected, check one) My insurance should be billed for covered services. I
agree to pay for any applicable co-payments, co-insurance, deductibles and/or non-covered services in the manner indicated in the CHARGES option below.
My insurance should NOT be billed for covered charges. I agree to pay for services in the manner indicated in the CHARGES option below.
Medicaid/FAMIS: My child is covered by Medicaid or FAMIS and I understand Medicaid/FAMIS will be billed for covered services.
FCS Agreement
Checking Medicaid
Charges
CHECKING FOR MEDICAID COVERAGE (If your child is not currently covered by Medicaid/FAMIS, check one) I give permission for my local early intervention system to routinely
check to see if my child is covered by Medicaid or FAMIS. I do not give permission for my local early intervention system to
routinely check to see if my child is covered by Medicaid or FAMIS
CHARGES (check one) Full Charge: I do not wish to provide financial information. I will pay all
applicable co-payments, co-insurance, deductibles, and/or the full early intervention reimbursement rate for services not covered by insurance.
Discounted Fees (If selected, check one) Monthly Cap: Documentation of my actual or estimated federal taxable
income has been viewed. This determines the amount I will pay. I agree to pay charges up to, but not exceeding, my family’s monthly cap of $_________ .
Fee Appeal (If selected, check one):__The amount of the monthly cap as calculated on the family cost share fee
scale is a financial hardship. My monthly cap is based on the additional financial information that is attached, OR
__I am unable to document either my actual or estimated taxable income. Attached is a copy of my pay stub or my written statement certifying my income amount, as well as any additional financial information required.
I agree to pay charges up to, but not exceeding, my family’s monthly cap of $_________ .
Medicaid/FAMIS/No Income: My child is eligible for Medicaid/FAMIS and/or I have no income at this time. Therefore I have an inability to pay, and will receive all of my child’s early intervention services at no cost to my family. (If selected, check one) Copy of my Medicaid/FAMIS card is attached OR __ eligibility verified on
____________ by _______________________ . My written statement certifying that I have no income is attached.
Temporary Agreement
At initial or annualIf family unable to provide financial
information and complete Family Cost Share Agreement prior to IFSP meeting
Part C funds may be used to ensure timely start of services
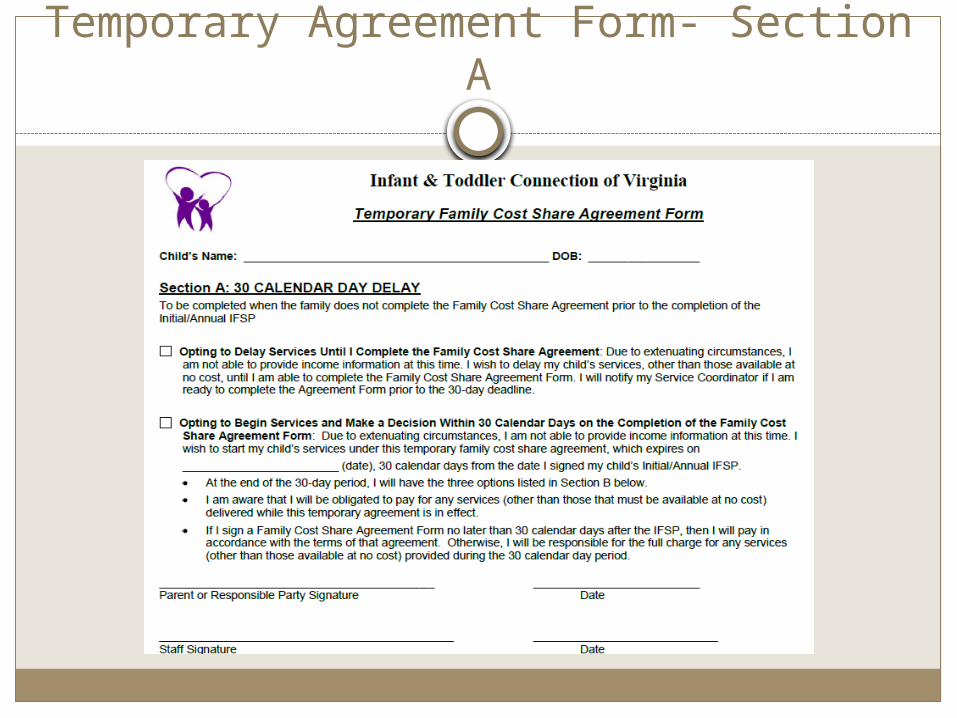
Temporary Agreement Form- Section A
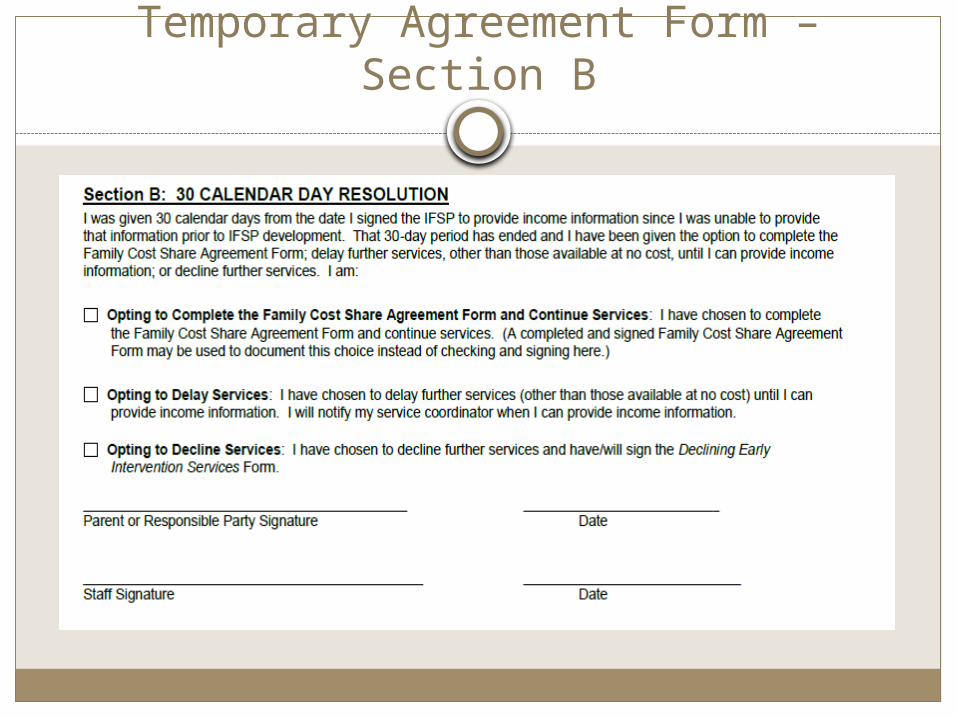
Temporary Agreement Form – Section B
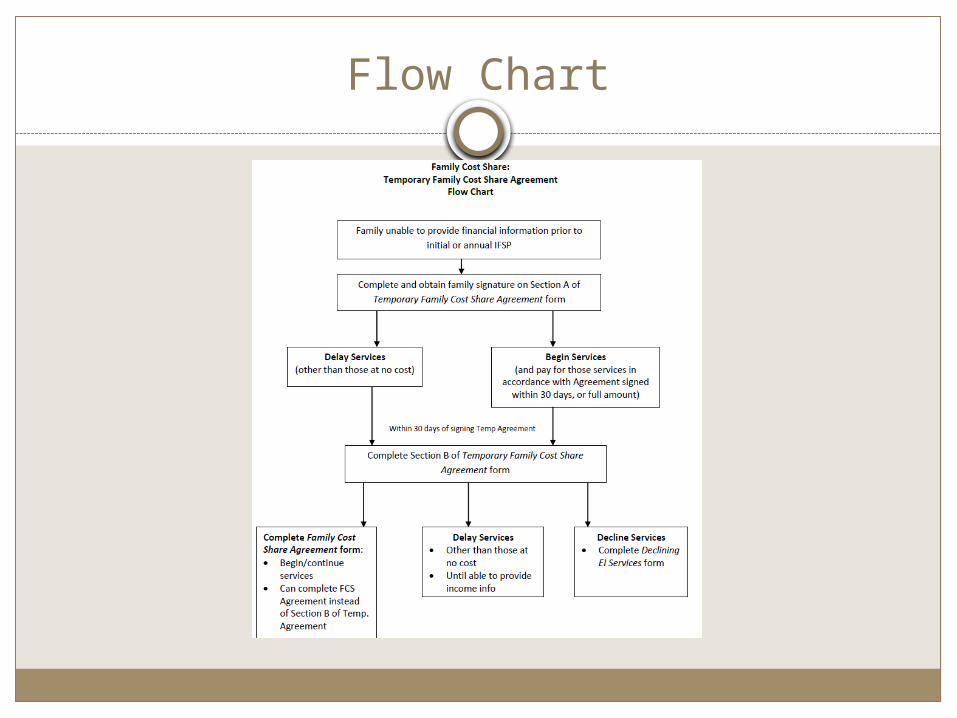
Flow Chart
Resources
www.eipd.vcu.edu Local Systems Oversight and Management Tools of the Trade
www.infantva.org Coming soon – Fiscal Section Strengthening Partnerships Notice/Facts About Family Cost Share Practice Manual Forms




























