Embed Size (px)
Citation preview

Fredric D. Gordon, MD
WhatWhat’’s New in Transplant?s New in Transplant?
Fredric D. Gordon, MDFredric D. Gordon, MD
Medical Director of Liver TransplantationMedical Director of Liver Transplantation
Director of HepatologyDirector of Hepatology
LaheyLahey Hospital and Medical CenterHospital and Medical CenterLaheyLahey Hospital and Medical CenterHospital and Medical Center
Associate Professor of MedicineAssociate Professor of Medicine
Tufts University School of MedicineTufts University School of Medicine
AgendaAgenda
•• Organ allocationOrgan allocation
•• Transplantation in HCCTransplantation in HCC
•• Live donor liver transplantationLive donor liver transplantation
•• Hepatitis C treatment in liver transplant Hepatitis C treatment in liver transplant recipientsrecipients
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
1

Fredric D. Gordon, MD
New Look at an Old Problem:New Look at an Old Problem:Regional Disparity
Mean MELD Match Score 2009D d D N E tiDeceased Donor, No Exceptions
ELD
Sco
reM
E
Region
Median months to liver transplant for adult patients transplanted in
2009
1
29
3
118
67
5
10
34
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
2

Fredric D. Gordon, MD
Evolving Concepts in Allocation:Mortality Rates by MELD – “Transplant Benefit”Evolving Concepts in Allocation:Mortality Rates by MELD – “Transplant Benefit”
1000010000WaitlistWaitlist
100100
10001000TransplantTransplant
Mortality rate per 1000 patients
Mortality rate per 1000 patients
HR=3.64P<0.001
HR=2.35P<0.001
HR=1.21P=0.41
HR=0.62P<0.01
HR=0.38P<0.001
HR=0.22P<0.001
HR=0.18P<0.001
HR=0.07P<0.001
HR=0.04 P<0.001
11
1010
6-116-11 12-1412-14 15-1715-17 17-2017-20 21-2321-23
MELDMELD
24-2624-26 27-2927-29 30-3930-39 40+40+
HR=hazard ratioHR=hazard ratioMerion, et al. Am J Transpl, 2005;5:307-13
Organ AllocationOrgan AllocationChange from Regional to National Share 15Change from Regional to National Share 15
•• ““Livers from adult deceased donors will be offered to Livers from adult deceased donors will be offered to did t h li t d St t 1A 1B h hdid t h li t d St t 1A 1B h hcandidates who are listed as a Status 1A or 1B or who have a candidates who are listed as a Status 1A or 1B or who have a
MELD or PELD score of 15 or higher at the local, regional and MELD or PELD score of 15 or higher at the local, regional and national levels before they are offered to any candidates of national levels before they are offered to any candidates of lesser urgency within the local service area of the donor lesser urgency within the local service area of the donor hospital.hospital.””
•• Mortality rates were 6.3% for those with MELD scores of <15.Mortality rates were 6.3% for those with MELD scores of <15.
•• Implementation of National Share 15 would result in a Implementation of National Share 15 would result in a decrease of 25 deaths per year nationally when compared to decrease of 25 deaths per year nationally when compared to the current policy.the current policy.
UNOS Concept Document: Next Steps Towards Improving Liver Distribution, Jan 4, 2011
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
3

Fredric D. Gordon, MD
Organ AllocationOrgan AllocationRegional Share 35Regional Share 35
•• ““Livers from adult deceased donors will be Livers from adult deceased donors will be id d f did t ith MELDid d f did t ith MELDconsidered for candidates with a MELD or considered for candidates with a MELD or
PELD score of 35 or higher at the local PELD score of 35 or higher at the local and regional level before being offered to and regional level before being offered to any candidate with a lower score.any candidate with a lower score.””
•• Facilitates transplantation for the most Facilitates transplantation for the most urgent patients.urgent patients.
UNOS Concept Document: Next Steps Towards Improving Liver Distribution, Jan 4, 2011
UNOS Regional Map Redrawn
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
4

Fredric D. Gordon, MD
Impact of Hepatocellular
Carcinoma on Liver Allocation
Impact of Hepatocellular
Carcinoma on Liver AllocationAllocationAllocation
Anticipated that the number of HCV related tumors Anticipated that the number of HCV related tumors will double over the next 20 yearswill double over the next 20 years
The Milan Criteria set the stage for The Milan Criteria set the stage for orthotopicorthotopic liver liver transplantation to be widely accepted as a curative transplantation to be widely accepted as a curative
Anticipated that the number of HCV related tumors Anticipated that the number of HCV related tumors will double over the next 20 yearswill double over the next 20 years
The Milan Criteria set the stage for The Milan Criteria set the stage for orthotopicorthotopic liver liver transplantation to be widely accepted as a curative transplantation to be widely accepted as a curative treatment for early stage HCCtreatment for early stage HCC
Multiple treatments available but liver transplantation Multiple treatments available but liver transplantation offers a potential cure for both the HCC and offers a potential cure for both the HCC and underlying liver diseaseunderlying liver disease
treatment for early stage HCCtreatment for early stage HCC
Multiple treatments available but liver transplantation Multiple treatments available but liver transplantation offers a potential cure for both the HCC and offers a potential cure for both the HCC and underlying liver diseaseunderlying liver disease
Adult Non-Status 1 DDLTJanuary 1, 2009 - June 30, 2012
~40%~20%
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
5

Fredric D. Gordon, MD
22 25 28 29 31 33 35 etc.22 25 28 29 31 33 35 etc.
Problems With Current MELD Problems With Current MELD HCC AllocationHCC Allocation
HCC priority too high relative to nonHCC priority too high relative to non--HCCsHCCsStudies of drop-out rates (Washburn, Segev)
High % of transplants for HCC
HCC scores at transplant vary across the HCC scores at transplant vary across the countrycountry
HCC scores driving up all MELD/PELD HCC scores driving up all MELD/PELD scoresscores
TREATMENT OPTIONS FOR HCC
SURGERYSURGERYResectionResectionTransplantationTransplantation
ABLATIONABLATIONABLATIONABLATIONPercutaneous Ethanol Injection (PEI)Percutaneous Ethanol Injection (PEI)Radiofrequency Hyperthermia (RFA)Radiofrequency Hyperthermia (RFA)
CHEMOTHERAPYCHEMOTHERAPYTransarterial Chemoembolization (TACE) Transarterial Chemoembolization (TACE) SorafenibSorafenib
RADIATION THERAPYRADIATION THERAPYRadiation TherapyRadiation TherapyRadiation TherapyRadiation TherapyRadioactive Microspheres (Y90)Radioactive Microspheres (Y90)
Multidisciplinary HCC Review BoardMultidisciplinary HCC Review BoardHBP & Transplant Surgeons, Hepatologists, Interventional Radiologists, HBP & Transplant Surgeons, Hepatologists, Interventional Radiologists,
Medical Oncologists, Radiation Oncologists, traineesMedical Oncologists, Radiation Oncologists, traineesWeekly review of protocols, new cases, and ongoing therapyWeekly review of protocols, new cases, and ongoing therapyProvide consistent approach to HCCProvide consistent approach to HCC
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
6

Fredric D. Gordon, MD
Survival Following Resection for HCC in Survival Following Resection for HCC in ChildChild’’s A Cirrhoticss A Cirrhotics
Summary of Reported Series Since 2008
Author Country nStudy
DesignSURVIVAL (%)
1 year 3 year 5 year
Hiraoka, 2008 Japan 59 OBS 88 59
Guglielmi, 2008 Italy 69 OBS 90 72 57
Santabrogio, 2009 Italy 78 OBS 93 85 54
Abu-Hilal, 2008 UK 34 OBS 91 56
Ueno, 2009 Japan 123 OBS 99 92 80
H 2010 Chi 75 RCT 96 79 71Huang, 2010 China 75 RCT 96 79 71
Kagawa, 2010 Japan 55 OBS 93 83 77
Hung, 2011 Taiwan 229 OBS 97 88 79
TOTALS 722 94 84 67
21.723.225
% Dropout within 12 Months: HCC and Non-HCC Candidates by Region
Candidates Added 7/1/08 – 6/30/11
4.8
13.912
17.7
5
10
15
20
% D
ropo
ut
0
5
1 2 3 4 5 6 7 8 9 10 11 US
RegionHCC (Standard) Non-HCC
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
7

Fredric D. Gordon, MD
92.4
66 367.88090
100d
% Transplanted within 12 Months: HCC and Non-HCC Candidates by Region
Candidates Added 7/1/08 – 6/30/11
39.4
66.367.8
25.5
39.1
10203040506070
% T
rans
plan
te
01 2 3 4 5 6 7 8 9 10 11 US
RegionHCC (Standard) Non-HCC
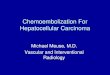
HCC Drop Out RatesHCC Drop Out Rates
> 3 cm +> 3 cm +
≤ 3 cm
Yao, et al, Liver Transplantation 2003 9:684-92
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
8

Fredric D. Gordon, MD
Hepatocellular CancerHepatocellular CancerChanges in MELD PrioritizationChanges in MELD Prioritization
OriginalOriginal April 2003April 2003 Jan 2004Jan 2004 Jan 2005Jan 2005
Stage IStage I
1 tumor < 2cm1 tumor < 2cm
15% Risk 15% Risk =MELD 24=MELD 24
8% Risk 8% Risk =MELD 20=MELD 20
0 Risk 0 Risk =MELD =MELD calculatedcalculated
0 Risk 0 Risk =MELD =MELD calculatedcalculated
Stage IIStage II1 tumor 1 tumor ≥≥ 2CM 2CM but ≤ 5 cm or 2but ≤ 5 cm or 2--3 tumors 3 tumors largest < 3 CMlargest < 3 CM
30% Risk 30% Risk =MELD 29=MELD 29
15%Risk 15%Risk =MELD 24=MELD 24
15% Risk 15% Risk =MELD 24=MELD 24
15% Risk 15% Risk =MELD 22=MELD 22
HCC Consensus Conference, 2008HCC Consensus Conference, 2008
HCC ALLOCATION POLICY: HCC ALLOCATION POLICY: Where Are We Today?Where Are We Today?
RecommendationsRecommendations Imaging Criteria
Pathology Form
Revise HCC allocation policy: “Allocation policy should result in similar risks of removal from the
waiting list and similar transplant rates for HCC and non-HCCwaiting list and similar transplant rates for HCC and non-HCC candidates.”
“Similar post-transplant outcomes for HCC and non-HCC recipients.”
“Development of a calculated continuous HCC priority score”
Downstaging, Expansion of Milan, LRT – on hold
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
9

Fredric D. Gordon, MD
MELD Policy Principles Applied to HCC
• Use objective risk factors associated with drop-out.
MELD• MELD• Maximum tumor size• Tumor number• AFP
• Use time from diagnosis (meeting criteria) as selection for less aggressive biologygg gy
• Continuous scale• Use continuous score, “HCC MELD”
6008000
T
Live Donor Liver Transplant Live Donor Liver Transplant TrendTrend
200
300
400
500
3000
4000
5000
6000
7000
of d
ecea
sed
dono
r LT
# of
live
don
or L
T
0
100
200
0
1000
2000
1 3 5 7 9 11 13 15 17 19 21 23 25
# o
19
88
19
90
19
92
19
94
19
96
19
98
20
00
20
02
20
04
20
06
20
08
20
10
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
10

Fredric D. Gordon, MD
Should Living Donors Be Used for Should Living Donors Be Used for Patients with Hepatocellular Carcinoma?Patients with Hepatocellular Carcinoma?
Pre-MELD Post-MELD
, 2012
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
11

Fredric D. Gordon, MD
Freedom From RecurrenceFreedom From Recurrence
DDLT(%
)
LDLT
HR=2.35, p=0.0408
dom
from
Rec
urre
nce
(
Recurrence
LDLT: 38% DDLT: 11%
Kulik et al. American Journal of Transplantation Nov 2012
Fre
ed
Years from Transplant
LDLT: 38%, DDLT: 11%
• Even in countries with adequate access to DDLT, that live liver donation is appropriate due to organ shortages.
• Organ allocation policies prioritizing pts with HCC within MC do not apply
Ethical Considerations
Organ allocation policies prioritizing pts with HCC within MC do not apply to LDLT since the needs of the other candidates without HCC are not being disadvantaged.
• Donor safety is of paramount importance in living donor liver transplantation and yet living donor complications and deaths occur even in the most experienced hands (0.1%-0.5% mortality, 10%-38% morbidity)morbidity)
• “Vancouver Forum” (2008) established practice principles for LDLT: – Live liver donation should only be performed if the risk to the donor
is justified by the expectation of an acceptable outcome in the recipient.
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
12

Fredric D. Gordon, MD
Liver Transplantation and Treatment of Hepatitis C
• HCV is a major cause of morbidity and mortality after liver transplantation
• Significant resource utilization
O’Leary et al., Liver Transpl 2009:15:360-8
EVR
Peginterferon alfa-2b and Ribavirin for Hepatitis C Recurrence Post–Orthotopic Liver Transplantation (OLT)
HCV RNAEVR
HCV RNA
PEGPEG--IFN alfaIFN alfa--2b 1.5 2b 1.5 µg/kg/wk +µg/kg/wk +RBV 400RBV 400--1200 mg/day1200 mg/day
48 weeks48 weeks
FollowFollow--upup24 weeks24 weeks
ScreeningScreening
RVRHCV RNA HCV RNA
Day 1
Bas
elin
eB
asel
ine
Treatment week 1–2: RBV 400 mg/dayTreatment week 3–4: RBV 800 mg/dayTreatment week 5–48: RBV dose increased to maximum of 1200 mg/day
(weight based) if well tolerated
Wk 24Wk 4 Wk 12 Wk 48
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
13

Fredric D. Gordon, MD
Sustained Virologic ResponseITT Analysis
70
80
2924
55
30
40
50
60
70S
VR
, %
0
10
20
All Patients Genotype 1 Genotype 2/3
36/125 25/105 11/20
Sustained Virologic ResponseStudy Completion Analysis*
69
80
5550
30
40
50
60
70
SV
R, %
ITT: ITT: 29%29% ITT: ITT:
24%24%
ITT: ITT: 55%55%
0
10
20
All Patients Genotype 1 Genotype 2/3
•28
36/66 25/50 11/16
*Patients who completed 48 weeks of treatment and 24 weeks of follow-up.
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
14

Fredric D. Gordon, MD
Safety
All Patients(N = 125),
n (%)Adverse Event
Treatment-emergent adverse events 125 (100)
Adverse events leading to study drug discontinuation 38 (30)
Serious adverse events 32 (26)
Severe/life-threatening treatment-related adverse 44 (35)
•29
gevents
44 (35)
Rejection episodes 4 (3)
Treatment-emergent infections 50 (40)
Protease inhibitorsProtease inhibitors
A Multicenter Study of Protease Inhibitor-Triple Therapy in HCV-Infected Liver Transplant Recipients:
Report From The CRUSH-C Group
LILI Triple Triple TherapyTherapy P+RP+RLI <90 days: 29
(N=87)
Protease inhibitors Protease inhibitors available midavailable mid--20112011Median Median
Days LIDays LIMedian Days Median Days
Total TreatmentTotal Treatment
154
Time
LILI Triple Triple TherapyTherapy P+RP+RLI ≥90 days: 189
(N=14)398
101 patients from 5 centersBurton JR, et al., AASLD Oct 2012, Boston
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
15

Fredric D. Gordon, MD
HCV RNA <LOD at Weeks 4-12 of Triple Therapy
The median time to HCV RNA <LOD: Start of P+R LI = 54 days (IQR: 46-84)
V R
NA
<LO
D
Start of P+R LI = 54 days (IQR: 46-84)Start of PI = 23 days (IQR: 13-34)
% H
CV
N=83 N=68 N=69
*HCV RNA negative at 4 and 12 weeks; missing week 4 (N=1), missing week 12 (N=15)
N=71
Early Discontinuation of Triple Therapy
• 12% had virologic breakthrough– LI <90 days: 10%
– LI ≥90 days: 21%
• 14% had AE leading to early D/CLI <90 days: 11% (data missing in 11)– LI <90 days: 11% (data missing in 11)
– LI ≥90 days: 40% (data missing in 4)
Burton JR, et al., AASLD Oct 2012, Boston
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
16

Fredric D. Gordon, MD
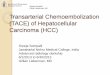
Immunosuppression Dosing after PIm
g
mg75%
reduction 90% reduction
Burton JR, et al., AASLD Oct 2012, Boston
Adverse EventsBlood transfusions 49%
# units in 1st 16 weeks, median (IQR) 2.5 (2.0-6.5)( ) ( )Use of growth factors 86%
G-CSFErythropoietin
44%79%
Dose reduction during triple therapyPeginterferon 27%Ribavirin*Both
78%23%
*Median (IQR) ribavirin dose (mg):Max dose = 800 (600-1000)Reduction in dose during triple therapy = 400 (200-600)
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
17

Fredric D. Gordon, MD
Adverse Events
Creatinine >0.5mg/dL from baseline 32%Max Δ creat from baseline median (IQR) 0 4 (0 2 0 7)Max Δ creat from baseline, median (IQR) 0.4 (0.2-0.7)
Rash* 6%Treated rejection (1-transition off PI, 1- late) 2%Hospitalization due to AE 21%
Indication for hospitalization: AnemiaInfection
7%4%Infection 4%
Deaths (1-sepsis, 1-HRS) 2%
*Requiring more than topical therapy
Burton JR, et al., AASLD Oct 2012, Boston
ConclusionsConclusions
•• Organ allocation disparity remains a major Organ allocation disparity remains a major problem on a national levelproblem on a national levelpp
•• HCC is the indication for transplantation in HCC is the indication for transplantation in a high percentage of patientsa high percentage of patients
•• Live donor liver transplantation is Live donor liver transplantation is diminishing in frequency but may have diminishing in frequency but may have
t ti l f b d li tit ti l f b d li tipotential for broader applicationpotential for broader application
•• Treatment of HCV with triple therapy after Treatment of HCV with triple therapy after transplantation will likely have less transplantation will likely have less success than in nonsuccess than in non--transplant patientstransplant patients
ACG Regional Postgraduate Course - Los Angeles, CA Copyright 2013 American College of Gastroenterology
18