Embed Size (px)
Citation preview

Strategie di Prevenzione del Rischio CCV GlobaleBergamo 13 Novembre 2010
Giuseppe Musumeci
USC Cardiologia Ospedali Riuniti di Bergamo
La malattia cardiovascolare nell’anziano: strategie di prevenzione e trattamento

Changes in global population from 2000 to 2030Percent Aged 65 and Over
US Census Bureau 2000
2000
2030

Incremento della popolazione anziana in Italia
Fonte ISTAT
81%
15% 4%
72%
19%
9%
64%15%
21%
2001 2025 2050
< 65 anni
> 65 anni
> 80 anni

0
10
20
30
40
50
60
70
Ipertensione arteriosa Artrosi-artriti CardiopatieM. gastrointestinali Diabete CancroBPCO Depressione Incontinenza
57.2
50.344.5
29.124 24
21 18.516.4
12
Incidenza (n. per 100 persone) di malattie croniche nell’anziano

Cardiopatie: prima causa di morte e ricovero nell’anziano

Normal aging changes in the cardiovascular system
� Increased arterial stiffnessand aortic impedance
� Increased cardiac stiffness.
� LV and myocyte hypertrophy. Loss of myocyte.
� Normal systolic function at rest. Reduced
functional reserve (HR and LVEF) during stress.
� Reduced baroreceptor sensitivity.
Lakatta EG , Circulation 1993;87:631-6.

Prevalence of Coronary Heart Disease by Age and Sex in the U.S. from 1988-94
0%
2%
4%
6%
8%
10%
12%
14%
16%
18%
20%
25-44 45-54 55-64 65-74 75+
Male Female
Age, years
Per
cent
of
Pop
ulat
ion
Source: National Health and Nutrition Examination Survey

0%
5%
10%
15%
20%
25%
30%
35%
0-19 20-49 50-54 55-59 60-64 65-69 70-74 75-79 80-84 85-89 90+
male female
HF: Prevalence and annual mortality by age
letalità
Prevalence 1.2% (0.02%-18.2%)Incidence 3.2/1000 (0.1-49/1000)
Annual mortality 16% (3.6%-31%)
age
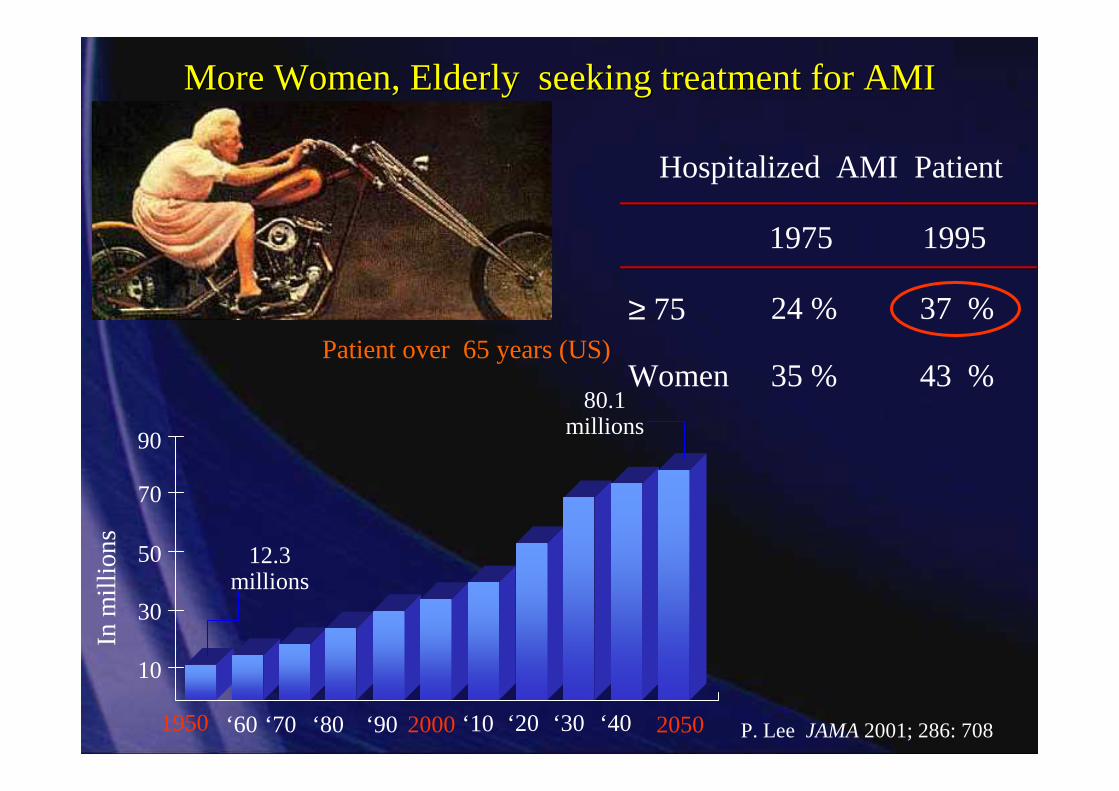
Patient over 65 years (US)
10
30
50
70
90
1950 2000 2050‘60 ‘70 ‘80 ‘90 ‘10 ‘20 ‘30 ‘40
80.1millions
12.3millions
In m
illio
ns
P. Lee JAMA2001; 286: 708
More Women, Elderly seeking treatment for AMIMore Women, Elderly seeking treatment for AMI
Hospitalized AMI Patient
24 % 37 %
43 %
≥ 75
1975 1995
35 %Women

RCTs of early invasive treatment in NSTEACS
Trial Average age % pts >75y Outcome
TIMI IIIB 59 3 Benefit only >65 y
VANQWISH 61 8 No difference
FRISC II 65 Excluded Benefit only >65 y
RITA 3 63 No age classes reported
Not reported by age
TACTICS 62 12.5 39% RR >65
56% RR >75
ICTUS 61 Not reported Trend towards > benefit >65y
…but not in trials

CADILLAC Trial30 Day Outcomes Stratified by Age
< 55 yrs 55-64 yrs 65-74 yrs ≥ 75 yrs
0,8
1,7
0
1,2
3,6
0,2
3,64,1
0,2
4,8
6,7
0,4
0
2
4
6
8
10
Death Bleeding Stroke
%
p < .0001
p = 0.02
Guagliumi G, Musumeci G. et al Circulation 2004; 110: 1598
p < .005

CADILLAC : Elderly Patients (≥ 75 years) treated with primary PCI
1 year free from death
100
95
9085
8075706560
100 150 200 250 300 250 400500
Time in Days
Per
cent
Sur
vivi
ng98 %98 %93 %88 %
G . Guagliumi, G. Musumeci et al. Circulation 2004
Age < 55Age < 55
55 ≤ age < 6555 ≤ age < 6565 ≤ age < 7565 ≤ age < 75Age ≥75Age ≥75
%
Log-Rank p = .0001

0
5
10
15
20
25
30
35
40
<65 65-74 75-84 85+
Stroke Renal Insuff CHF
Age and Comorbid Illness%
of p
opul
atio
n

Rischio nei pazienti con sindrome coronarica acutaRelazione con l’età

Sindrome metabolica: prevalenza in relazione all’etàP
rev a
len
ce, %
Age, yrAdapted from: Ford ES, et al. JAMA. 2002;287:356-359.
47 million or 23% of US Adults Have Metabolic Syndrome
0
5
10
15
20
25
30
35
40
45
20-29 30-39 40-49 50-59 60-69 ?70
Men (n=4265)
Women (n=4559)

Lake Saints Hospital Study
0
5
10
15
20
25
30
35
<50 50-59 60-69 70-79 >80
No statine Statine
Classi d’età
N. P
azie
nti c
on r
ecid
iva
di e
vent
i car
diov
asco
lari
P=0.35P=0.04
P=0.04
P=0.01
P=0.004

Dislipidemici trattati con statine nelle varie classi d’etàStudio FADOI 3
0
5
10
15
20
25
30
35
35 - 44 45 - 54 55 - 64 65 - 74 75 - 84 > 85
% receiving statins
etàFADOI 3,2002

Medical Treatment vs Coronary Revascularization in the Elderly: The TIME study
MED
0 1 2 3 4 5 6
INV
Log Rank p=<0.0001
Time scince randomization (years)
Pro
port
ion
with
out M
AC
E
0
2
4
6
8
10
Extracted from Pfisterer M. Circulation 2004;110:1213-1218
INV
MED

Cardiac Surgery in the Elderly
0
10
20
30
<65 years 65 - 74 >74 years
30-day mortality
Major complications
Jarvinen et al, World J Surg 2003
RISK
AGE (per 5 years) OR 1.2; 95%CI 0.9-1.6
Renal failure OR 1.4; 95%CI 0.9-2.1
History of CHF OR 1.4; 95%CI 1.0-1.9
COPD OR 1.7; 95%CI 1.2-2.3
Vascular disease OR 1.5; 95%CI 1.2-1.9
Emergency OR 3.6; 95%CI 2.8-4.8
*Alexander et al, JACC, 35:731-8

PCI vs. CABG in Elderly Patients: the BARI Trial
0
1
2
3
4
5
6
<65 years >65 years <65 years >65 years <65 years >65 ye ars
Rat
e (%
)CABG
Stent
Death Q-wave-MI Stroke
Mullany et al, Ann Thorac Surg 1999

STEMI: Thrombolysis vs Primary PCI Mortality differences
0
5
10
15
20
25
PCI
LYSIS
PAMIAge>65
PCATAge>70
GUSTOIIbAge>70
DeBoerAge>75
GRACEAge>75
%

Reperfusion strategy in elderly patients in the real world
59
54
34
19
2231
57
9
15
0%
25%
50%
75%
100%
<55 55 - 75 >75
NO TREATPCITL
DEATH 7.5%
<55 0.8%
55-75 4.9%
>75 19.9%
Di Chiara A. EHJ 2003;24:1616
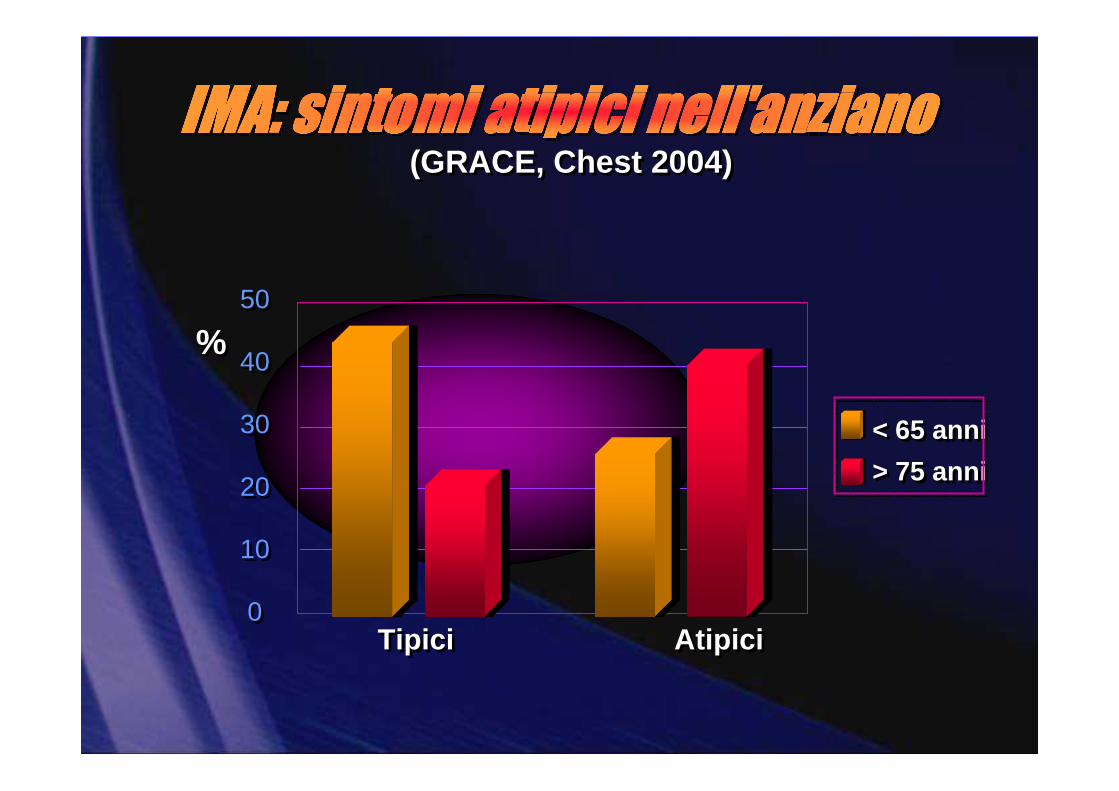
(GRACE, Chest 2004)(GRACE, Chest 2004)
Tipici AtipiciTipici Atipici
%%50
40
30
20
10
0
50
40
30
20
10
0
< 65 anni
> 75 anni
< 65 anni
> 75 anni

Safety Concerns in the Elderly ACS PatientsBleeding Risks by Age
N=74,271
4,5
10,3
14,1
9,7
17,9 18,5
0
5
10
15
20
<65 yrs 65-75 yrs > 75 yrs
% R
BC
Tra
nsfu
sion
Non-CABG Overall
4,5
10,3
14,1
9,7
17,9 18,5
0
5
10
15
20
<65 yrs 65-75 yrs > 75 yrs
% R
BC
Tra
nsfu
sion
Non-CABG Overall
Excluded CABG, transfer outs, missing dataExcluded CABG, transfer outs, missing dataPeterson, E ACC 2005Peterson, E ACC 2005

1,7 3 4,26,14,3 5,7 6,7
12,3
0
5
10
15
20
25
30
35
40
45
<55 55-64 65-74 >=75
Bleeding Bivalirudin Bleeding UFH+GPI NNT
Patient Age
38 3740
16
Number Needed to Treat (NNT) and Risk Reduction of Major Bleeding with Bivalirudin vs. Heparin/GPI
Lopes RD et al. J Am Coll Cardiol. 2009 Mar 24;53:1021-30


Conclusioni
� I pazienti anziani rappresentano una popolazione complessa in progressivo aumento
� L’incidenza e la prognosi delle malattie cardiovascolari sono più severe nei pazienti anziani
� La prevenzione delle malattie cardiovascolari riveste un ruolo cruciale negli anziani
� La rivascolarizzazione coronarica per via percutanea èefficace nell’anziano
� Il trattamento dei pazienti anziani con PCI primaria si èdimostrato superiore alla trombolisi
� L’età avanzata rimane un potente predittore di mortalità e di complicanze emorragiche

Net Clinical BenefitBleeding Risk Subgroups
OVERALL
>=60 kg
< 60 kg
< 75
>=75
No
Yes
0.5 1 2
PriorStroke / TIA
Age
Wgt
Risk (%)
+ 37
-16
-1
-16
+3
-14
-13
Prasugrel Better Clopidogrel BetterHR
Pint = 0.006
Pint = 0.18
Pint = 0.36
Post-hoc analysis
Wiviott SD et al New Eng J Med 2007; 357: 2001-15Wiviott SD et al New Eng J Med 2007; 357: 2001-15

Excessive Dosing of Antithrombotics by AgeExcessive Dosing of Antithrombotics by Age
12,5
28,7
8,512,5
3733,1
16,5
38,5
64,5
0
10
20
30
40
50
60
70
LMW Heparin UF Heparin GP IIb/IIIa
% E
xces
sive
Dos
e
< 65 yrs 65-75 yrs >75 yrs
12,5
28,7
8,512,5
3733,1
16,5
38,5
64,5
0
10
20
30
40
50
60
70
LMW Heparin UF Heparin GP IIb/IIIa
% E
xces
sive
Dos
e
< 65 yrs 65-75 yrs >75 yrs
Q1-Q2 2004 CRUSADE dataQ1-Q2 2004 CRUSADE data


Very easy to find the elderly in the CCU…
21
31
13
7 7 62 2 2 2 1 1 1 1 0,5 0,4 0,3 0,3 0,2
0
20
40
60
STEMI
SCA NSTE
Scomp ensoFA/T
PSVBra
diari t
mi eDolo
re T
or.TV/F
VSin
cope
post-PCI/B
PAC
Alt ro
Embolia
Polm
.Arr
esto
CC
Shock
no S
CA
Mio-
peric
ard
itePost-
PM/A
ICD
Tampo
nam.
Dissez
i one
CADEnd
ocar
dite
%
332 CCUs 6986 patients
Mean age: 70 ±±±± 13 years
Median (range 25-75 °°°°): 72 (61-80) years
Age > 75 years: 39% of the patients
Casella G. J Cardiovasc Med 2010

Crusade: ACS in Elderly
2,8
67,4
8,5
13,3
16,1
02468
1012141618
Death Death/MI CHF
<75 Years >75 Years
Kulkarni S et al ACC 2003 CRUSADE Presentation

CCP (Shlipak, Ann Intern Med 2002 )CCP (Shlipak, Ann Intern Med 2002 )
< 1.5 1.5-2.5 >2.5 creatinina< 1.5 1.5-2.5 >2.5 creatinina
mor
talit
à1
anno
mor
talit
à1
anno
100
80
60
40
20
0
100
80
60
40
20
0
24%24%
46%46%
66%66%

0
5
10
15
0 30 60 90 180 270 360 450
HR 0.81(0.73-0.90)P=0.0004
Prasugrel
Clopidogrel
Days
End
poin
t (%
)
12.1
9.9
HR 1.32(1.03-1.68)
P=0.03
Prasugrel
Clopidogrel1.82.4
138events
35events
Efficacy and SafetyN=13608
CV Death / MI / Stroke
TIMI Major NonCABG Bleeds
NNT = 46
NNH = 167
Wiviott SD et al New Eng J Med 2007; 357: 2001-15Wiviott SD et al New Eng J Med 2007; 357: 2001-15

Riduzione degli eventi avversi nei pazienti trattati con statine

Soggetto che fornisce assistenza in caso di necessità (val. %)
Fonte: indagine Censis, 2004
< 2% istituzioni

-48-46
-28
-39-37
-50
-25
0Age >75 Renal
FailureFemale
UHFpre-treat Diabetes
Bivalirudin provides consistent relative risk reductionBivalirudin provides consistent relative risk reduction
30-day Major Bleeding
30-day bleeding and one-year mortality in Replace-2 high risk subgroups
30-day bleeding and one-year mortality in Replace-2 high risk subgroups
-41
-28
-47
-37
-48
Age >75RenalFailure Female UHF
pre-treatDiabetes
One-year Mortality

The aging failing heart
Cardiac disease
Comorbidities and
Life- Stile
Normal aging
CV Changes
Complexity

Strategie di Prevenzione del Rischio CCV GlobaleBergamo 13 Novembre 2010
Giuseppe Musumeci
USC Cardiologia Ospedali Riuniti di Bergamo
La malattia cardiovascolare nell’anziano: strategie di prevenzione e trattamento

Fe
ma
le
UH
F p
ost
-PC
I
UA
MI<
12
hrs
IAB
P
Ag
e >
75
Ab
cixi
ma
b
Re
na
l Fa
ilure
Dia
be
tes
2,9
22,3 2,4
3
1,6 1,81,6
1,3
0
1,5
3
OROR
Factor associated to higher incidence of major bleeding
Montalescot et al. Heart 2005;91:89Montalescot et al. Heart 2005;91:89 Kinnaird et al. Am J Cardiol 2003;92:930Kinnaird et al. Am J Cardiol 2003;92:930Manoukian SV, Voeltz MD, Feit F et al. TCT 2006

.
Mortalità ospedaliera Mortalità 6 mesi
Devlin G, Gore M, Elliott J et al. Eur Heart J 2008;29:1275-82
GRACE – Anziani con Sindrome coronarica acuta ad alto rischio

Mortality benefit of myocardial revascularization in the Elderly
Extracted from Pfisterer M. Circulation 2004;110:1213-1218
0
2
4
6
8
10
0 4 6 8Time since intervention (years)
Pro
port
ion
with
out d
eath
Revascularized
Not revascularized
Log Rank p=0,0027
All patients
Revascularized 174 159 149 115 72 34Not revascularized 127 113 101 80 48 28
No. At risk

Acute Coronary Care in the ElderlyA Scientific Statement From the
American Heart Association
Circulation 2007;115;2549-2569
≥ 75 years of age

RCTs vs Observational studies
0
10
20
30
40
66-70 71-80 81-90 91-00
Decade
% A
ge>7
5Community Practice
Trials
Lee, JAMA, 2001
GRACE
VIGOUR RCT’s
CRUSADE

n = 252
n = 229
Grines C. TCT; Washington DC 2005

Age related impairments(common reasons for nonadherence
and lack of self-management)
• Visual and hearingimpairment (20-50%)
• Cognitive impairment(26-78%: dementia, depression, etc)
Possibly related to cerebral hypoperfusion and CVA
• Lack of social support: social isolation; marital functioning vs living alone
• Health illiteracy (25%): difficulties to understandwritten and oral informations concerning their illness and treatment
� “do you understand what I have told you?” is not enough

Senior PAMI: 30- day Outcome Based on Age-Stratified Randomization
7,1 7,7 7,7
11,3 12
17
0
5
10
15
20
25
Death Death/CVA D/CVA/reMI
Age 70-80 (n=351)
%
PCI Lysis
19 2022
16 16
22
0
5
10
15
20
25
Death Death/CVA D/CVA/reMI
Age >80 (n=130)
%
PCI Lysis
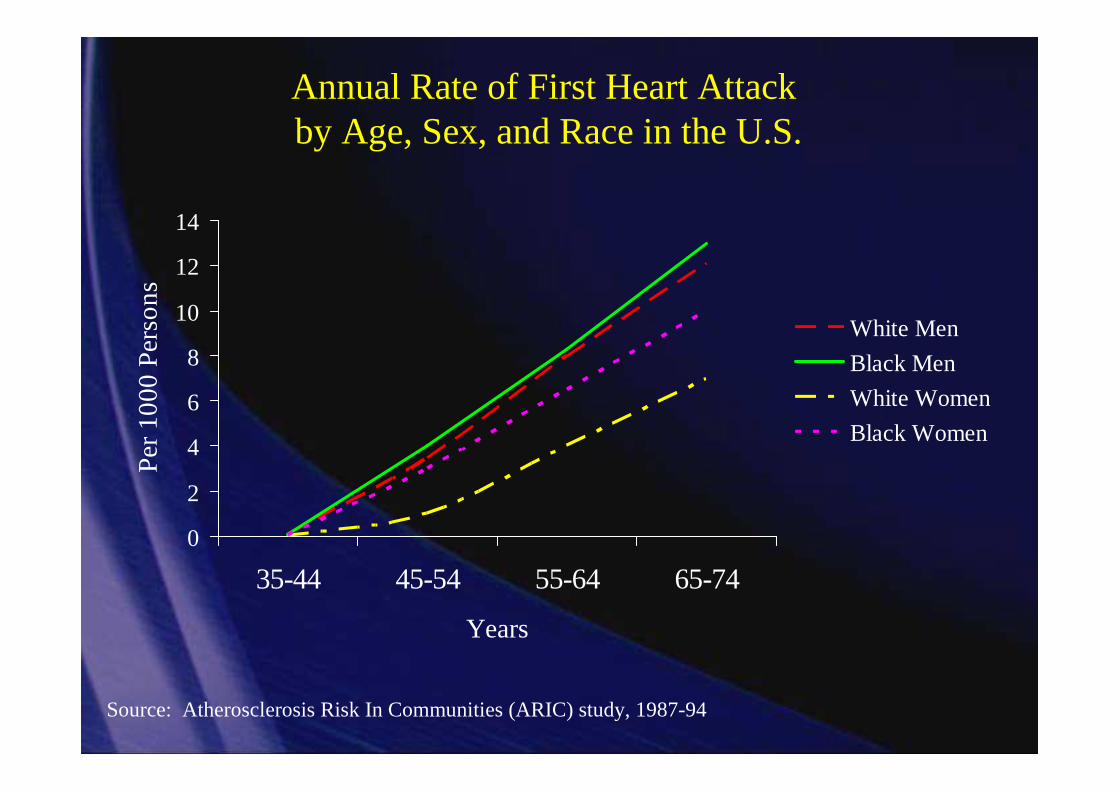
Annual Rate of First Heart Attackby Age, Sex, and Race in the U.S.
0
2
4
6
8
10
12
14
35-44 45-54 55-64 65-74
Years
Per
10
00
Per
son
s
White Men
Black Men
White Women
Black Women
Source: Atherosclerosis Risk In Communities (ARIC) study, 1987-94

Rapporto ISTAT 2008
Italiani, i più anziani
• 20% di ultrasessantacinquenni
• 5,5% di ultraottantenni
• Aspettativa di vita: 78 anni uomini, 83 donne
• 85% degli anziani assume farmaci
http://www.istat.it/dati/catalogo/20081112_00/PDF/cap2.pdf

Fried L. 2005
Heterogeneity of health with aging

14,9
30,2
54,4
100
0102030405060708090
100
FSS
grade 1grade 2grade 3grade 4
Frailty and 1-year mortality
21,1
47,6
81,8
100
0102030405060708090
100
FSS
grade 1grade 2grade 3grade 4
Frailty and 1-year HF admissions
Log Rank 20,345; df 2; p<0,0001
FSS 1
FSS 2
FSS 3-4
FSS 1
FSS 2
FSS 3-4
Log Rank 41,207; df 2; p<0,0001
G.Pulignano et al Eur Heart J 2006
•deficit cognitivo, incontinenza urinaria e disturbi della motilità

Zuccalà G et al Am J Medicine 2003; 115: 97-103.
Deficit cognitivo e prognosi di scompenso cardiacostudio GIFA Osservatorio Geriatrico Campano
Abete P et al,
Del Sindaco, et al.

11-25% of older persons use 5 or more meds
simultaneously
•Multiple physicians, multiple drugs
•Errors in self-administration caused by age related impairments,
complexity of medication regimen, duration of treatment
•More than 20% of adverse drug reactions in the elderly are due to
drug interactions (Drug-drug / -nutrient /-alcohol)
•Multiple organ system changes (CV, GI, liver, kidney)
Pharmacodynamics /Pharmacokinetics
Polypharmacy and Drug interactions in elderly patients





























