Embed Size (px)
Citation preview
Stefano Del Prato
LA STRATEGIA TERAPEUTICA
NEL PAZIENTE ANZIANO

Diabetes Mellitus in elderly subjects
0
20
40
60
80
100
120
140
160
180
200
20-44 45-64 65+
Estim
ate
d N
. of
people
with D
M
2010 2030
0
2
4
6
8
10
12
14
<2
0
20-2
4
25-2
9
30-3
4
35-3
9
40-4
4
45-4
9
50-5
4
55-5
9
60-6
4
65-6
9
70-7
4
75-7
9
80+
Pre
vale
nce
of D
M in U
SA
(%
)
Global diabetic
population
Distribution of DM in age-
groups at diagnosis.
Vacante M et al. Arch Gerontol Geriatr. 2011;53:113-9

Diabetes Mellitus in elderly subjects
0
20
40
60
80
100
120
140
160
180
200
20-44 45-64 65+
Estim
ate
d N
. of
people
with D
M
2010 2030
0
2
4
6
8
10
12
14
<2
0
20-2
4
25-2
9
30-3
4
35-3
9
40-4
4
45-4
9
50-5
4
55-5
9
60-6
4
65-6
9
70-7
4
75-7
9
80+
Pre
vale
nce
of D
M in U
SA
(%
)
Global diabetic
population
Distribution of DM in age-
groups at diagnosis.
Vacante M et al. Arch Gerontol Geriatr. 2011;53:113-9

Narayan KM et al. Diabetes Care 2006;29:2114-6
Impact of recent increase in incidence on future
diabetes burden – U.S.A. 2005 - 2050

0
5
10
15
20
25
0-19 20-34 35-49 50-64 65-79 ≥80 Total
Perc
ent
Age (years)
Male Female
Miccoli R. 2012 Personal Communication
Diabetes prevalence per age group –
ARNO-Diabete 2010

0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Diabetes No Diabetes
≥80
65-79
50-64
35-49
20-34
0-19
Age distribution in the population with or
without diabetes - ARNO-Diabete 2010
Age (years)
Miccoli R. 2012 Personal Communication

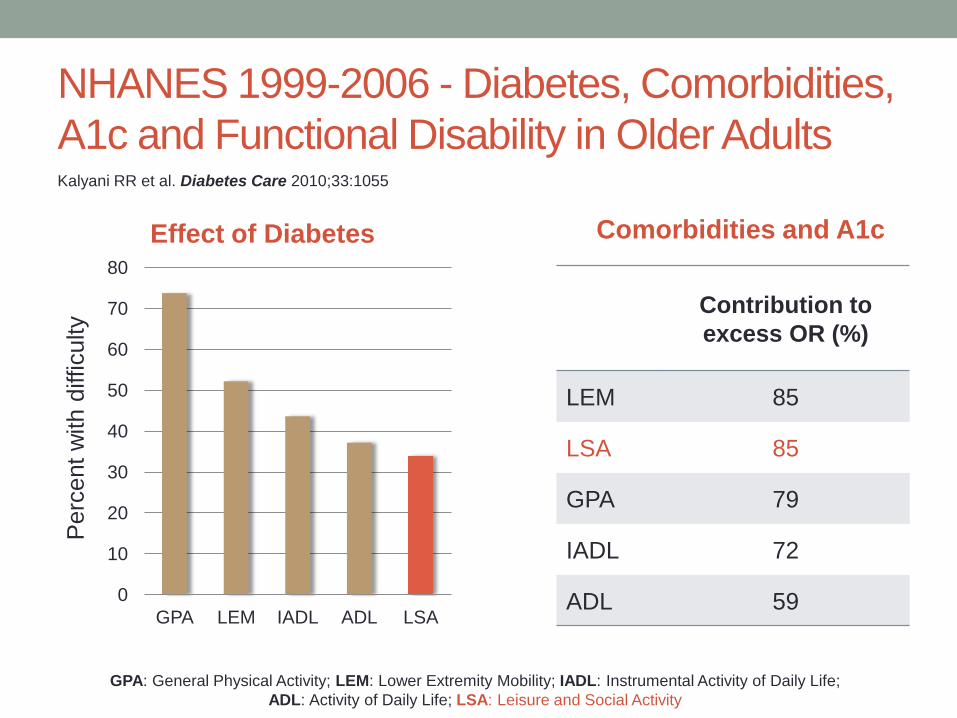
NHANES 1999-2006 - Diabetes, Comorbidities,
A1c and Functional Disability in Older Adults
0
10
20
30
40
50
60
70
80
GPA LEM IADL ADL LSA
Perc
ent
with d
ifficulty
Effect of Diabetes
Contribution to
excess OR (%)
LEM 85
LSA 85
GPA 79
IADL 72
ADL 59
GPA: General Physical Activity; LEM: Lower Extremity Mobility; IADL: Instrumental Activity of Daily Life;
ADL: Activity of Daily Life; LSA: Leisure and Social Activity
Kalyani RR et al. Diabetes Care 2010;33:1055
Comorbidities and A1c
NHANES 1999-2006 - Diabetes, Comorbidities,
A1c and Functional Disability in Older Adults
0
10
20
30
40
50
60
70
80
GPA LEM IADL ADL LSA
Perc
ent
with d
ifficulty
Effect of Diabetes
Contribution to
excess OR (%)
LEM 85
LSA 85
GPA 79
IADL 72
ADL 59
GPA: General Physical Activity; LEM: Lower Extremity Mobility; IADL: Instrumental Activity of Daily Life;
ADL: Activity of Daily Life; LSA: Leisure and Social Activity
Kalyani RR et al. Diabetes Care 2010;33:1055
Comorbidities and A1c

Chang AM et al. Am J Physiol Endocrinol Metab, 2003
Progression
to IGT and
T2DM
Impaired
adaptation:
No
insulin
INSULIN
RESISTANCE
Decreased physical
activity
Increased adiposity
Age effects
on insulin action
Increased adiposity
Medications
Genetics
Coexisting illness
IMPAIRED
INSULIN
SECRETION
Medications
Genetics
Coexisting illness
Age effects on
beta-cell
Pathogenesis of T2DM in aging
Diabetes Risk Factors in
Aging

Zamboni M et al. Nutr Metab Cardiovasc Dis, 2008
A new link between aging and diabetes:
the sarcopenic obesity

The general population is ageing
DM has a high prevalence, which increases substantially with
age
The socio-economic burden of DM will only continue to grow
DM is considered to lead to accelerated aging
The diabetic population has a high prevalence of geriatric
syndrome
DM emerged as a significant predictor of progression in any
frailty characteristics
Rationale for treating elderly diabetic
people
To keep patients aymptomatic
To prevent either acute or chronic
complications
To preserve QoL
To avoid adverse drug reactions
Treatment goals in elederly diabetic
subjects

To keep patients aymptomatic
To prevent either acute or chronic
complications
To preserve QoL
To avoid adverse drug reactions
Treatment goals in elederly diabetic
subjects

Il caso di Aristide…..
77 anni con 4 anni di storia di T2DM. Anamnesi positiva per ischemia cardiaca e
osteoartrite degenerativa della colonna
Terapia
• Metformina 1 g bid, aspirina 75 mg qd, bisoprolol 5 mg qd, ISMO 10 mg bid, ramipril 5
mg bid, simvastatina 40 mg qd
All’obiettività:
• Peso 95 kg; BMI 33 kg/m2; PA140/75 mmHg; polso 65 bpm
Laboratorio:
• HbA1c: 8.6% (70 mmol/mol)
• eGFR: 42 mL/min/1.73 m2
• Total cholesterol: 151 mg/dl (3.9 mmol/L)
• Low-density lipoprotein cholesterol: 77 mg/dl (2.0 mmol/L)
• High-density lipoprotein cholesterol:42 mg/dl (1.1 mmol/L)
• Plasma triglyceride: 185 mg/dl (2.1 mmol/L)
BMI=body mass index; HbA1c=haemoglobin A1c.

Secondo voi, qual’è la principale considerazione da
fare rispetto alla terapia del Sig. Aristide?
1. Evitare l’ipoglicemia
1. Evitare l’aumento del peso
2. Ridurre i potenziali rischi di interazione tra farmaci
3. Valutare la sicurezza di ogni ulteriore trattamento
farmacologico
4. Altro

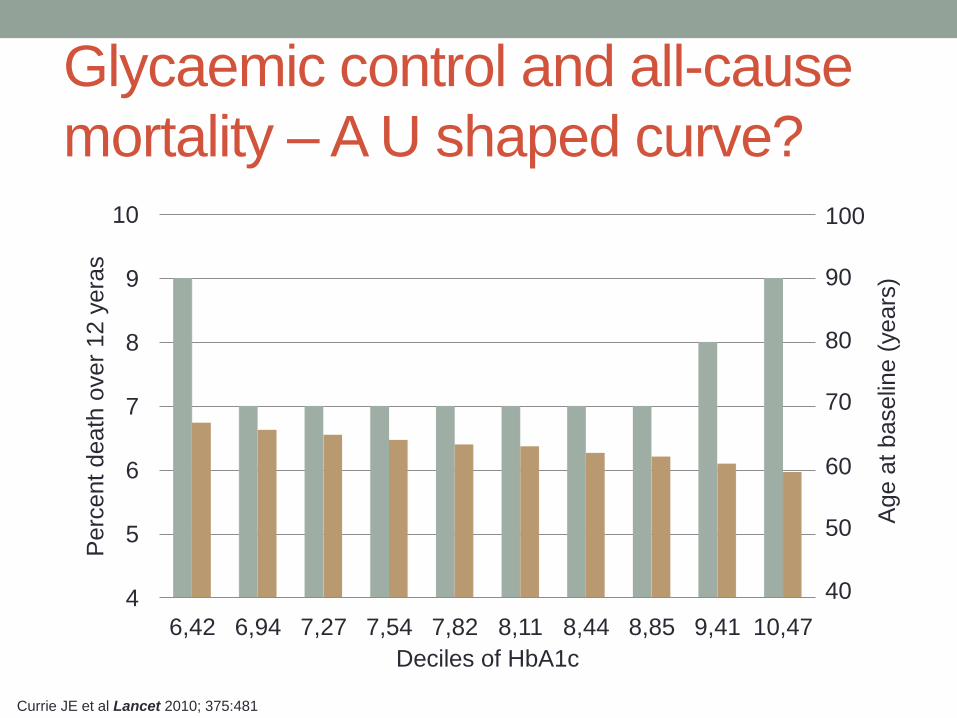
Glycaemic control and all-cause
mortality – A U shaped curve?
4
5
6
7
8
9
10
6,42 6,94 7,27 7,54 7,82 8,11 8,44 8,85 9,41 10,47
Perc
ent
death
over
12 y
era
s
Deciles of HbA1c
100
90
80
70
60
50
40
Age a
t baselin
e (
years
)
Currie JE et al Lancet 2010; 375:481
Glycaemic control and all-cause
mortality – A U shaped curve?
4
5
6
7
8
9
10
6,42 6,94 7,27 7,54 7,82 8,11 8,44 8,85 9,41 10,47
Perc
ent
death
over
12 y
era
s
Deciles of HbA1c
100
90
80
70
60
50
40
Age a
t baselin
e (
years
)
Currie JE et al Lancet 2010; 375:481
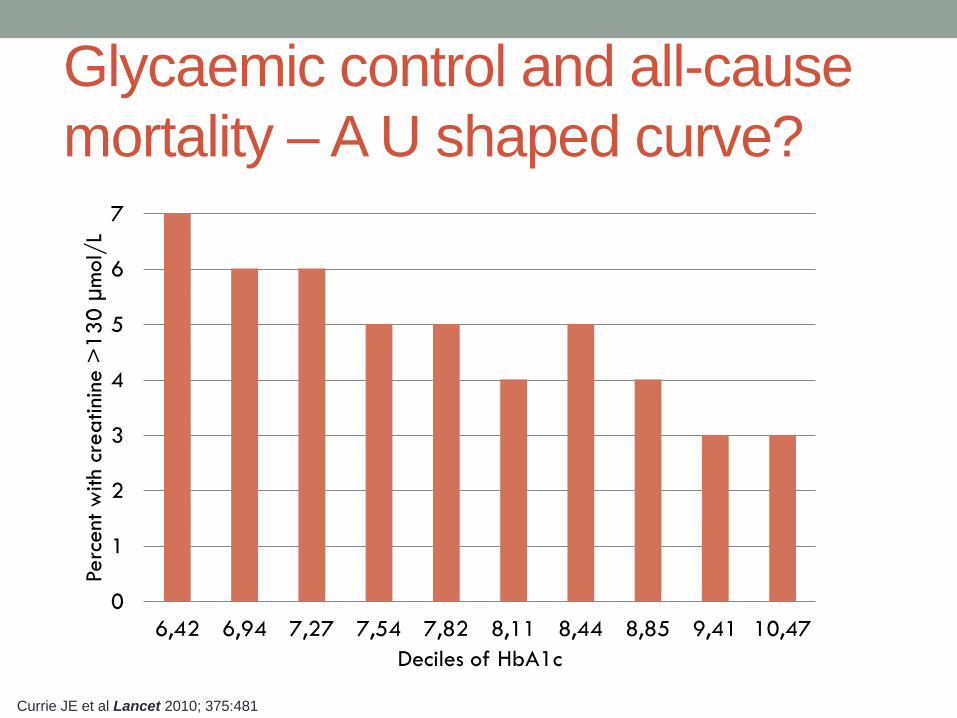
Glycaemic control and all-cause
mortality – A U shaped curve?
0
1
2
3
4
5
6
7
6,42 6,94 7,27 7,54 7,82 8,11 8,44 8,85 9,41 10,47
Perc
ent w
ith c
rea
tini
ne >
13
0 µ
mol/
L
Deciles of HbA1c
Currie JE et al Lancet 2010; 375:481

Intervention trials in T2DM patients –
Age at entry
TRIAL Age recruitment
criterion AGE AT ENTRY
UKPDS 25-65 54
UKPDS-FU 25-65 62
ProACTIVE 35-75 62
ADVANCE >55 66±6
ACCORD 40-79 62±7
VADT 45-79 60
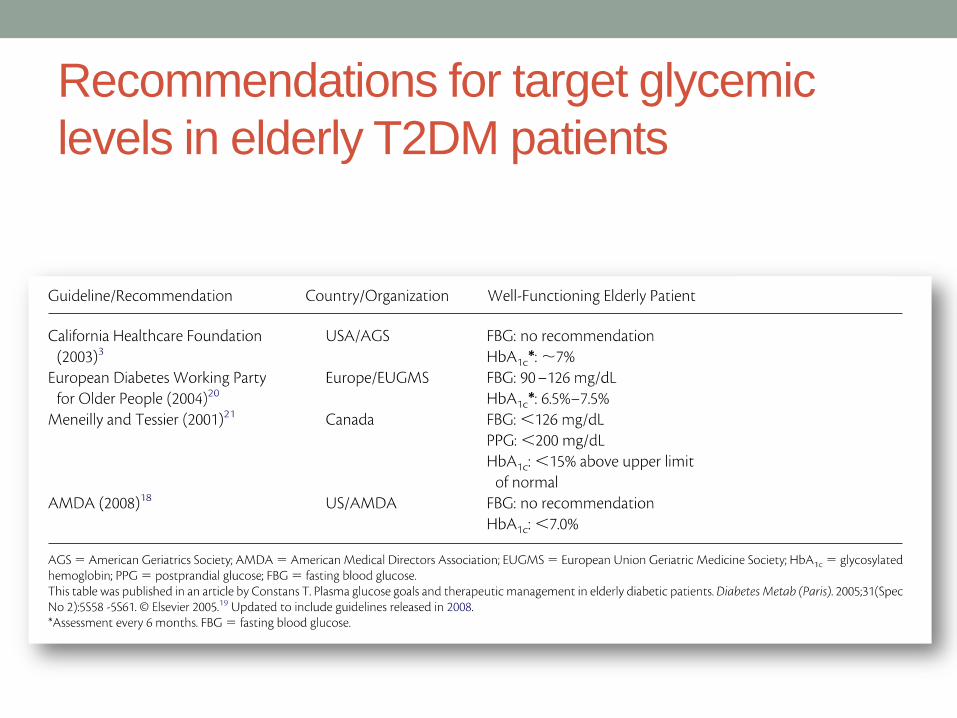
Recommendations for target glycemic
levels in elderly T2DM patients

Glycaemic targets in diabetes.
The ADA/AHA position statement
A1c <7.0%
• Short duration of diabetes
• Long life expectancy
• No significant
cardiovascular disease
• A1c >7.0%
• History of severe
hypoglycemia
• Limited life expectancy
• Long-standing diabetes
• Advanced micro- and
macrovascular
complications
Skyler J. et al Diabetes Care 2009;32:187
MAY GAIN ADDITIONAL
MICROVASCULAR BENEFIT AS
WELL AS MACROVASCULAR
PROTECTION
Patient’s phenotype B=body weight
C=complications
D=duration
A1c >7.0%
A= age

The A1C and ABCD of glycaemia management in
T2DM: a physician’s personalized approach
YOUNG MIDDLE
AGE ELDERLY
– – – + + +
<6.0 <6.5 <6.5 6.5-7.0 <7.0 7.0-8.0
Age
Complications* or
Disease duration
>10yrs
A1c target
>9.0 A1c at
diagnosis
Initial
therapy
<9.0%
Metformin Consider
insulin
*Micro- and macrovascular complications Pozzilli P …. Del Prato S Diabetes Metab Res Rev 2010; 26:239

Management of Hyperglycemia in Type 2 Diabetes: A Patient-Centered Approach
Diabetes Care – Diabetologia June 2012
Quale sarebbe la vostra opzione
terapeutica per il Sig. Aristide?
1. Sulfonilurea
2. Glinide
3. Pioglitazone
4. Insulina
5. Agonista del recettore GLP-1
6. Inibitore DPP-4
DPP-4=dipeptidyl peptidase-4; GLP-1=glucagon-like peptide-1.

Alcuni problemi nella cura di Aristide
• Ipoglicemia
• Peso corporeo
• Sottostante malattia cardiovascolare
• Farmacoterapia multipla e complessa – interazione tra
farmaci
• Insufficienza renale

With increasing age, potential reaction time between awareness and onset of
symptoms is decreased, contributing to an increased risk for asymptomatic
hypoglycaemia and greater susceptibility to cognitive impairmenta,1,2
Thresholds for hypoglycaemia symptoms
vary with agea,1,2
aBased on data in non-diabetic patients with no family history of diabetes.
1Zammitt NN, Frier BM. Diabetes Care. 2005;28:2948–2961; 2Matyka K, et al. Diabetes Care. 1997;20:135–141.
Blo
od
glu
co
se
co
nce
ntr
ation
1
(mg/d
L)
36
45
54
63
72
Men aged 23 ± 2 years (n=7)
Greater reaction
time for corrective
action
Hypoglycaemic
awareness
Onset of
cognitive dysfunction
36
45
54
63
72
Men aged 65 ± 3 years (n=7)
Less reaction time
for corrective
action
Blo
od
glu
co
se
co
nce
ntr
ation
1
(mg/d
L)
Hypoglycaemic
awareness
Onset of
cognitive dysfunction

Lifestyle risk factors
• Poor nutrition or fasting
• Prolonged physical exercise
• Alcohol (ethanol)
Drug risk factors
• Use of SU and / or insulin
• Drug interactions with SUs
Patient risk factors
• Advanced age
• Recent hospitalisation
• Intercurrent illness
• Chronic liver, renal or
cardiovascular disease
• Endocrine deficiency (thyroid,
adrenal, pituitary)
• Loss of normal counter-regulation
• Hypoglycaemic unawareness
SU=sulfonylurea.
Adapted from Chelliah A, Burge MR. Drugs Aging. 2004;21:511–530.
Hypoglycaemia is a major challenge in
the treatment of diabetes in the elderly

Lifestyle risk factors
• Poor nutrition or fasting
• Prolonged physical exercise
• Alcohol (ethanol)
Drug risk factors
• Use of SU and / or insulin
• Drug interactions with SUs
Patient risk factors
• Advanced age
• Recent hospitalisation
• Intercurrent illness
• Chronic liver, renal or
cardiovascular disease
• Endocrine deficiency (thyroid,
adrenal, pituitary)
• Loss of normal counter-regulation
• Hypoglycaemic unawareness
SU=sulfonylurea.
Adapted from Chelliah A, Burge MR. Drugs Aging. 2004;21:511–530.
Hypoglycaemia is a major challenge in
the treatment of diabetes in the elderly

Lifestyle risk factors
• Poor nutrition or fasting
• Prolonged physical exercise
• Alcohol (ethanol)
Drug risk factors
• Use of SU and / or insulin
• Drug interactions with SUs
Patient risk factors
• Advanced age
• Recent hospitalisation
• Intercurrent illness
• Chronic liver, renal or
cardiovascular disease
• Endocrine deficiency (thyroid,
adrenal, pituitary)
• Loss of normal counter-regulation
• Hypoglycaemic unawareness
SU=sulfonylurea.
Adapted from Chelliah A, Burge MR. Drugs Aging. 2004;21:511–530.
Hypoglycaemia is a major challenge in
the treatment of diabetes in the elderly

Lifestyle risk factors
• Poor nutrition or fasting
• Prolonged physical exercise
• Alcohol (ethanol)
Drug risk factors
• Use of SU and / or insulin
• Drug interactions with SUs
Patient risk factors
• Advanced age
• Recent hospitalisation
• Intercurrent illness
• Chronic liver, renal or
cardiovascular disease
• Endocrine deficiency (thyroid,
adrenal, pituitary)
• Loss of normal counter-regulation
• Hypoglycaemic unawareness
SU=sulfonylurea.
Adapted from Chelliah A, Burge MR. Drugs Aging. 2004;21:511–530.
Hypoglycaemia is a major challenge in
the treatment of diabetes in the elderly

The consequences of hypoglycaemia
1Whitmer RA, et al. JAMA. 2009;301:1565–1572; 2Bonds DE, et al. BMJ. 2010;340:b4909; 3Barnett AH. Curr Med Res Opin.
2010;26:1333–1342; 4Jönsson L, et al. Value Health. 2006;9:193–198; 5Foley JE, Jordan J. Vasc Health Risk Manag. 2010;6:541–548; 6Begg IS, et al. Can J Diabetes. 2003;27:128–140; 7McEwan P, et al. Diabetes Obes Metab. 2010;12:431–436.
HYPOGLYCAEMIA
Cardiovascular
complications3
Weight gain by
defensive eating5
Coma3
Increased risk
of car accident6
Hospitalisation
costs4
Loss of
consciousness3
Increased risk
of seizures3
Death2,3
Increased risk
of dementia1
Reduced
quality of life7
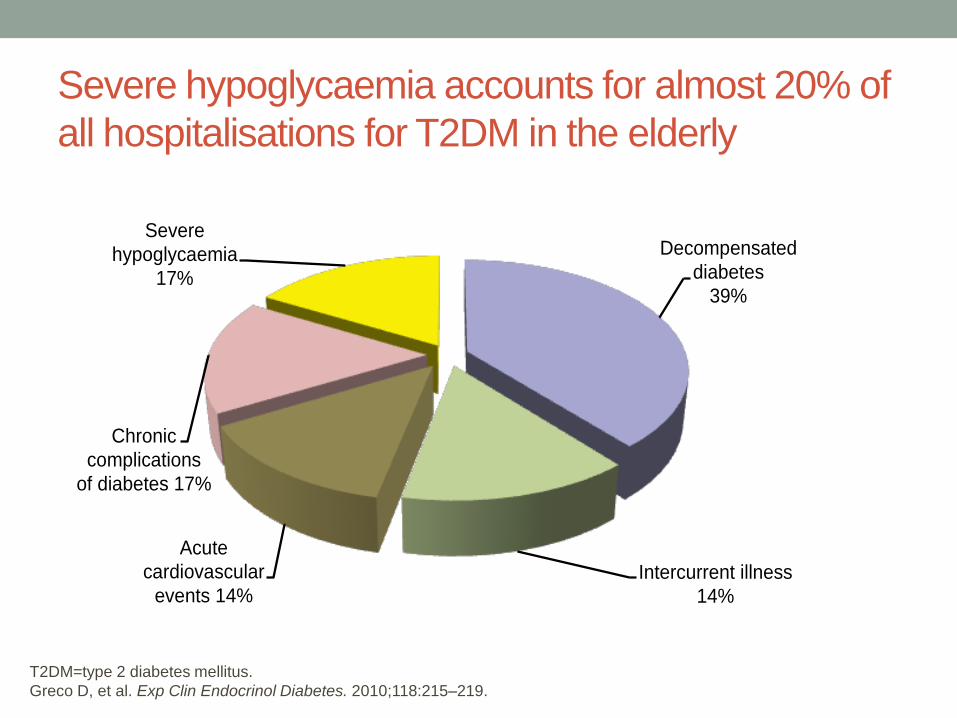
Severe hypoglycaemia accounts for almost 20% of
all hospitalisations for T2DM in the elderly
T2DM=type 2 diabetes mellitus.
Greco D, et al. Exp Clin Endocrinol Diabetes. 2010;118:215–219.
Decompensated
diabetes
39%
Intercurrent illness
14%
Acute
cardiovascular
events 14%
Chronic
complications
of diabetes 17%
Severe
hypoglycaemia
17%

Budnitz DS et al. N Eng J Med, 2012
Estimated rates of emergency hospitalizations for
adverse drug events in older U.S. adults, 2007 - 2009
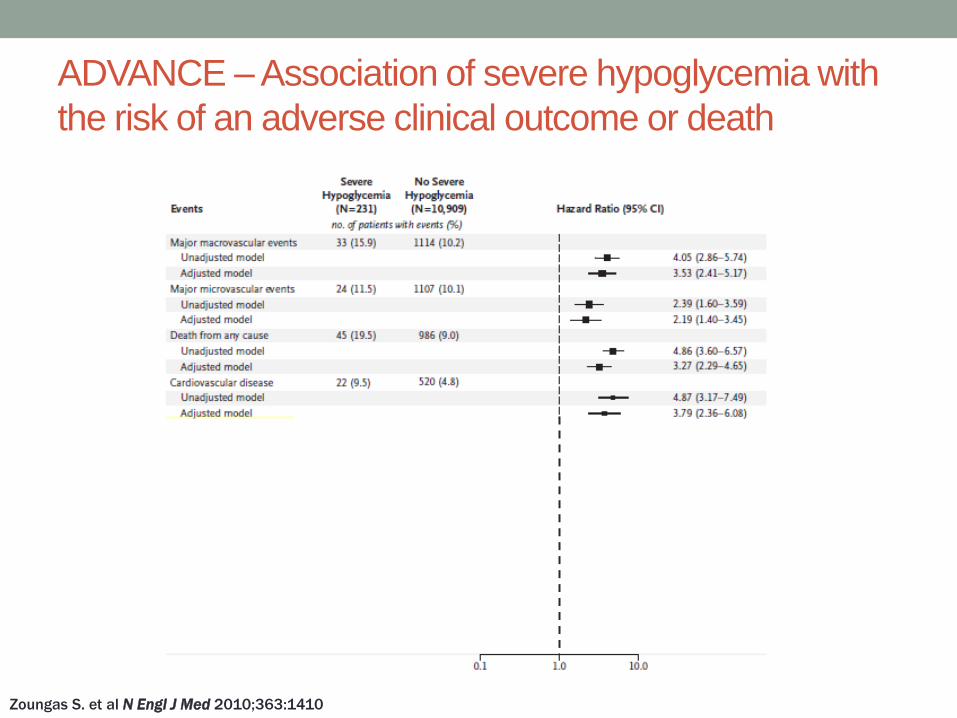
ADVANCE – Association of severe hypoglycemia with
the risk of an adverse clinical outcome or death
Zoungas S. et al N Engl J Med 2010;363:1410

Clinical criteria Biological criteria
ApoE carriers
Plasma osmolarity (> 300
mOsm/l)
Low serum albumin (< 38 g/l)
Increased CRP
Increased IL6
Low total cholesterol
Sarcopenia is a major
cause of disability and
frailty in the elderly
Xue QL. Clin Geriatr Med, 2011; Bourdel-Marchasson I et al. Diabetes Metab, 2005
Frailty and vulnerability

The risk of severe hypoglycaemia: post hoc
epidemiological analysis of the ACCORD study
0
0,2
0,4
0,6
0,8
1
1,2
1,4
1,6
1,8
Diabetes duration (years)
BMI (kg/m2)
Serum creatinine ( mol/l)
*History of peripheral neuropathy (yes vs. no); **per 1 year increase
P=0.03
P=0.01
P<0.0001
P<0.0001
P<0.0001
P<0.03
P<0.0001
Miller ME et al . BMJ 2010;340: b5444
A B C C D
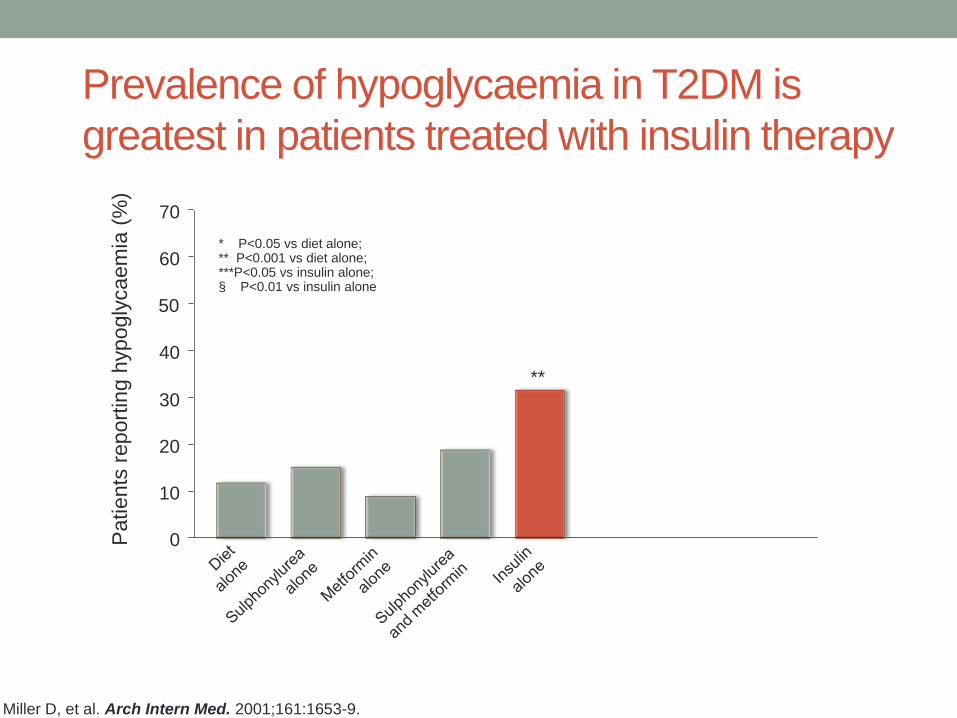
Prevalence of hypoglycaemia in T2DM is
greatest in patients treated with insulin therapy
Miller D, et al. Arch Intern Med. 2001;161:1653-9.
Patients
report
ing h
ypogly
caem
ia (
%)
* P<0.05 vs diet alone; ** P<0.001 vs diet alone; ***P<0.05 vs insulin alone; § P<0.01 vs insulin alone
0
10
20
30
40
50
60
70
**
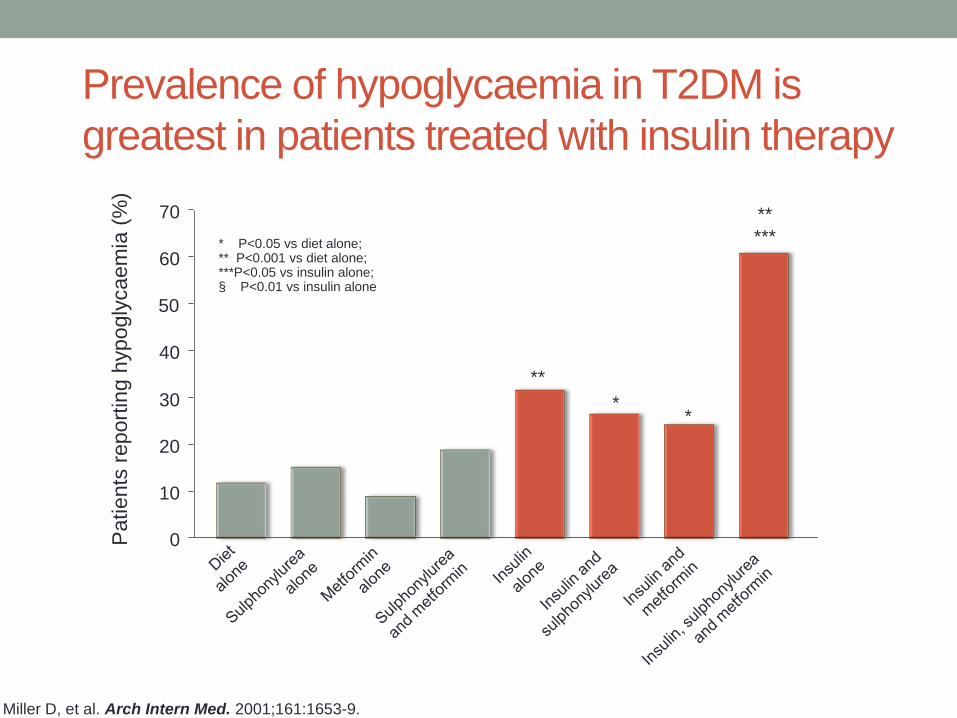
Prevalence of hypoglycaemia in T2DM is
greatest in patients treated with insulin therapy
Miller D, et al. Arch Intern Med. 2001;161:1653-9.
Patients
report
ing h
ypogly
caem
ia (
%)
* P<0.05 vs diet alone; ** P<0.001 vs diet alone; ***P<0.05 vs insulin alone; § P<0.01 vs insulin alone
0
10
20
30
40
50
60
70
* *
**
**
***

Incidence of hypoglycaemia with different
glucose-lowering agents for T2DM
Bolen S, et al. Ann Intern Med. 2007;147:386-399.

AMI, stroke, CHF and all-cause mortality in elderly
medicare patients treated with pio- or rosiglitazone
Graham at al., JAMA 2007; 304:411
Bone fracture!
Heart failure!
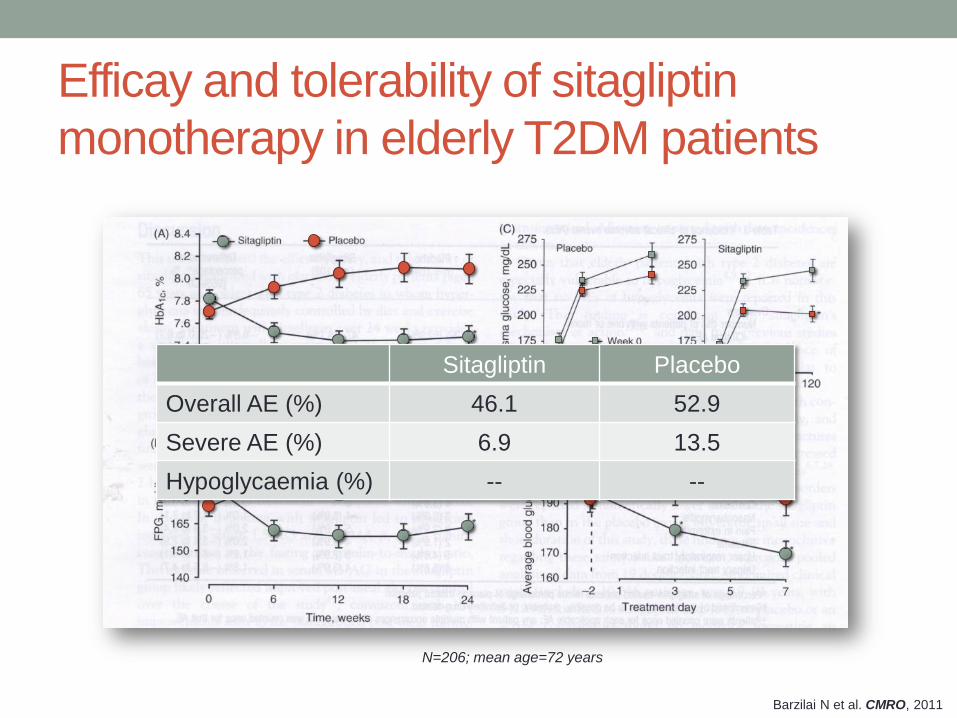
Barzilai N et al. CMRO, 2011
Efficay and tolerability of sitagliptin
monotherapy in elderly T2DM patients
Sitagliptin Placebo
Overall AE (%) 46.1 52.9
Severe AE (%) 6.9 13.5
Hypoglycaemia (%) -- --
N=206; mean age=72 years

Vildagliptin in the very elderly T2DM patients
-1,5
-1,0
-0,5
0,0
0,5
1,0
1,5
MonoRx* Met Add-on**
(Pe
rce
nt)
-1,0
-0,8
-0,6
-0,4
-0,2
0,0
MonoRx Met Add-on
(kg
)
0
10
20
30
40
50
60
MonoRx Met Add-on
(Perc
ent
)
Monotherapy Add-on to met
≥75 yr <75 yr ≥75 yr <75 yr
N (%) N (%) N (%) N (%)
Any
events 0 (0) 8 (0.3) 0 (0) 0 (0)
Severe
events 0 (0) 0 (0) 0 (0) 0 (0)
HBA1c Body Weight
Achieving A1c ≤7.0 Hypoglycemia
Age ≥75 yr (MonoRx, N=62; Add-on, N=25) Age <75 yr (MonoRx, N=2303; Add-on, N=910)
Schweizer A et al. Diabetes Obes Metab 2011; 13:55
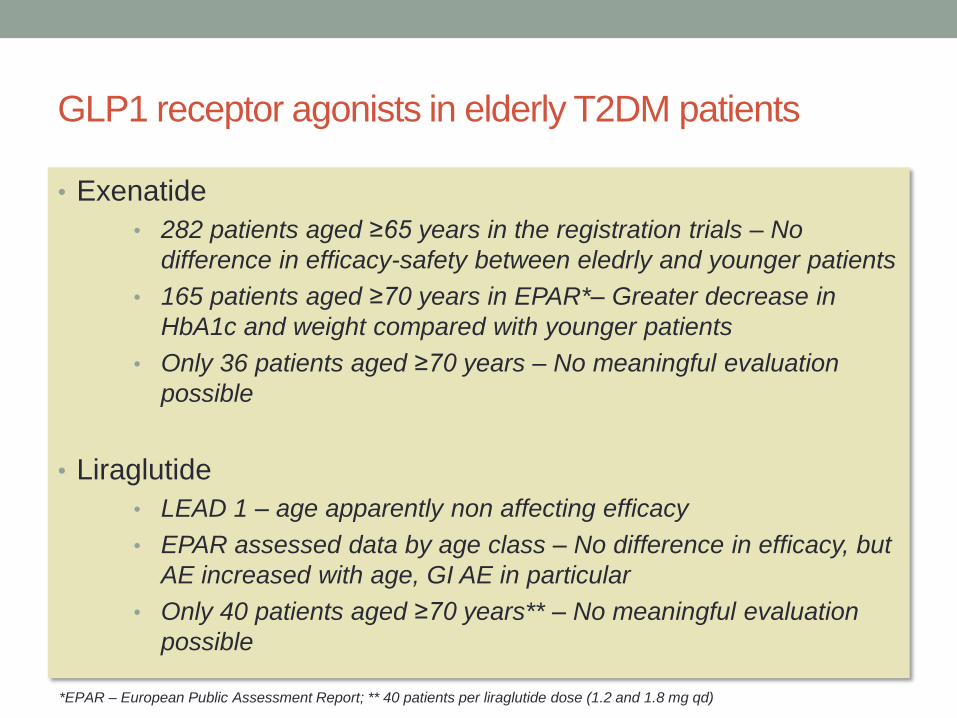
GLP1 receptor agonists in elderly T2DM patients
• Exenatide
• 282 patients aged ≥65 years in the registration trials – No
difference in efficacy-safety between eledrly and younger patients
• 165 patients aged ≥70 years in EPAR*– Greater decrease in
HbA1c and weight compared with younger patients
• Only 36 patients aged ≥70 years – No meaningful evaluation
possible
• Liraglutide
• LEAD 1 – age apparently non affecting efficacy
• EPAR assessed data by age class – No difference in efficacy, but
AE increased with age, GI AE in particular
• Only 40 patients aged ≥70 years** – No meaningful evaluation
possible
*EPAR – European Public Assessment Report; ** 40 patients per liraglutide dose (1.2 and 1.8 mg qd)
Alcuni problemi nella cura di Aristide
• Ipoglicemia
• Peso corporeo
• Insufficienza renale
• Sottostante malattia cardiovascolare
• Farmacoterapia multipla e complessa – interazione tra
farmaci

RIACE Study Group, unpublished data
0
20
40
60
80
100
≤45 n. 113 (21.4%)
n. 528
46-60 n. 1,067 (26.8%)
n. 3,986
61-75 n. 3,100 (37.0%)
n. 8,374
>75 n. 1,628 (56.4%)
n. 2,885
eGFR <60 ml/min Both Albuminuria
Perc
ent
The Renal Insufficiency And Cardiovascular Events
(RIACE) Italian Multicentre Study
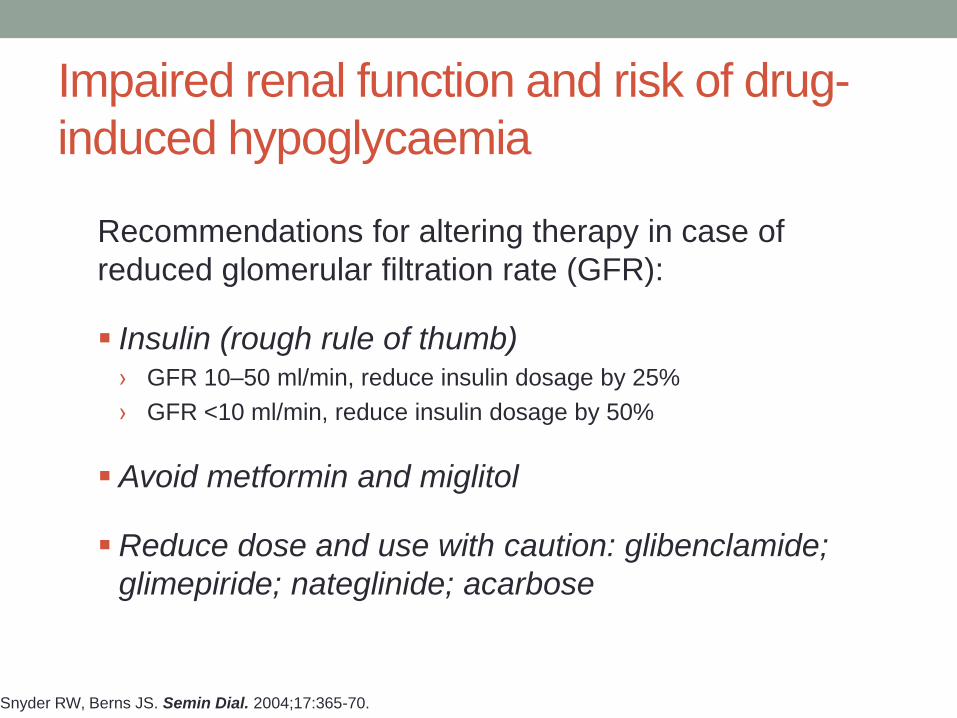
Snyder RW, Berns JS. Semin Dial. 2004;17:365-70.
Recommendations for altering therapy in case of
reduced glomerular filtration rate (GFR):
Insulin (rough rule of thumb) › GFR 10–50 ml/min, reduce insulin dosage by 25%
› GFR <10 ml/min, reduce insulin dosage by 50%
Avoid metformin and miglitol
Reduce dose and use with caution: glibenclamide;
glimepiride; nateglinide; acarbose
Impaired renal function and risk of drug-
induced hypoglycaemia

Snyder RW, Berns JS. Semin Dial. 2004;17:365-70.
Recommendations for altering therapy in case of
reduced glomerular filtration rate (GFR):
Insulin (rough rule of thumb) › GFR 10–50 ml/min, reduce insulin dosage by 25%
› GFR <10 ml/min, reduce insulin dosage by 50%
Avoid metformin and miglitol
Reduce dose and use with caution: glibenclamide;
glimepiride; nateglinide; acarbose
Impaired renal function and risk of drug-
induced hypoglycaemia

Although the risk of lactic acidosis on metformin is 10–20 times lower than
that on phenformin and does not differ from the risk in patients not taking
the drug, this agent still carries the historic burden of its predecessors. It is
even doubtful whether metformin plays a causal role in the pathogenesis of
lactic acidosis at all……….. We believe that standard contraindications to
the use of metformin should be relaxed, and that the benefits of reducing
the number of patients excluded from using it would by far outweigh the
potential risks. We propose removal of the following contraindications from
the list:
1. old age;
2. chronic renal insufficiency (as long as GFR >40 ml/min);
3. chronic heart failure (NYHA stages I and II); and
4. discontinuation of metformin therapy 2 days before surgery and i.v.
contrast medium administration.
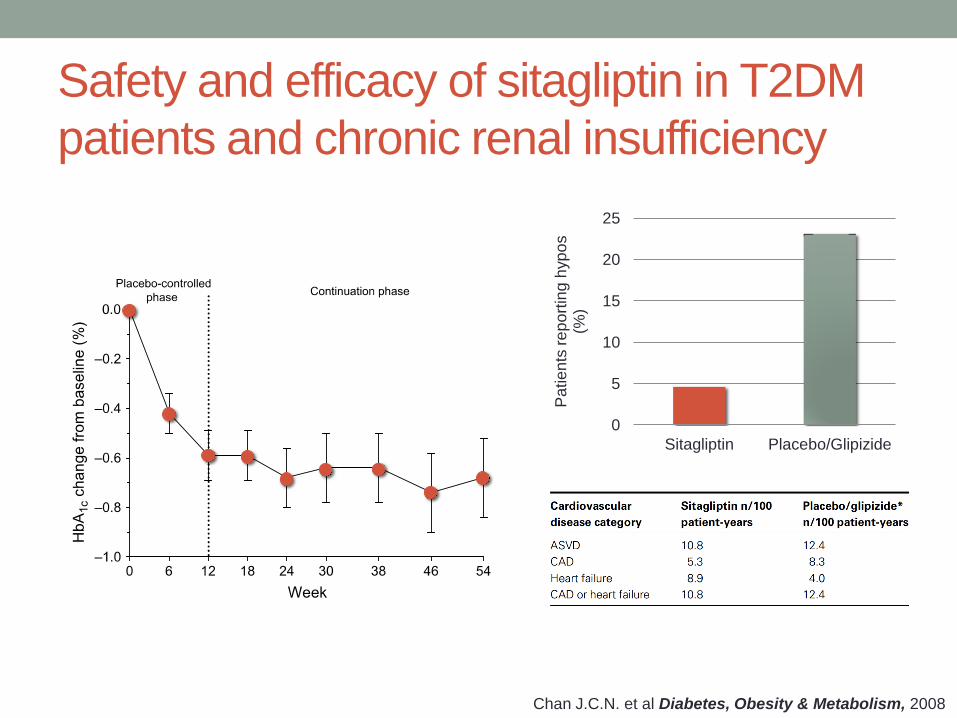
Chan J.C.N. et al Diabetes, Obesity & Metabolism, 2008
Safety and efficacy of sitagliptin in T2DM
patients and chronic renal insufficiency
0
5
10
15
20
25
Sitagliptin Placebo/Glipizide
Pa
tie
nts
re
po
rtin
g h
yp
os
(%)

52-week efficacy and safety study of saxagliptin
(2.5 mg) in T2DM patients with renal impairment
-1,2
-1
-0,8
-0,6
-0,4
-0,2
0
0,2
0,4
Moderate Severe ESRD
HbA
1c (
%)
0
5
10
15
20
25
30
35
40
45
Moderate Severe ESRD
Patients
report
ed h
ypogly
cem
ia (
%)
Baseline HbA1c (%) 8.5 8.04 8.65
Nowicki M et al. Int J Clin Pract 2011; 65:1230
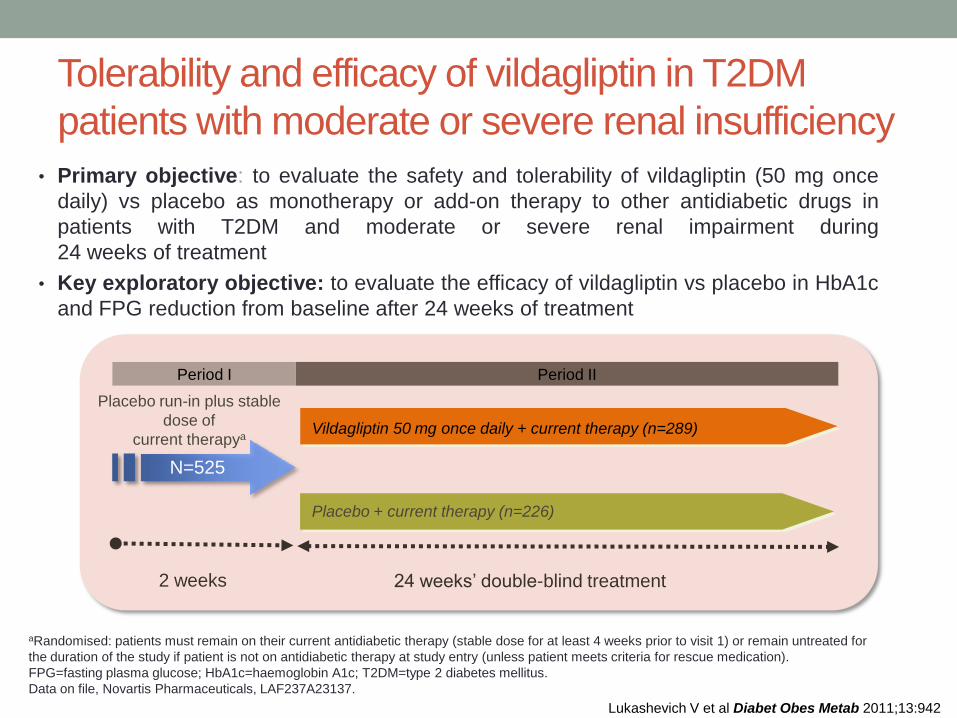
Tolerability and efficacy of vildagliptin in T2DM
patients with moderate or severe renal insufficiency
• Primary objective: to evaluate the safety and tolerability of vildagliptin (50 mg once
daily) vs placebo as monotherapy or add-on therapy to other antidiabetic drugs in
patients with T2DM and moderate or severe renal impairment during
24 weeks of treatment
• Key exploratory objective: to evaluate the efficacy of vildagliptin vs placebo in HbA1c
and FPG reduction from baseline after 24 weeks of treatment
aRandomised: patients must remain on their current antidiabetic therapy (stable dose for at least 4 weeks prior to visit 1) or remain untreated for
the duration of the study if patient is not on antidiabetic therapy at study entry (unless patient meets criteria for rescue medication).
FPG=fasting plasma glucose; HbA1c=haemoglobin A1c; T2DM=type 2 diabetes mellitus.
Data on file, Novartis Pharmaceuticals, LAF237A23137.
Placebo + current therapy (n=226)
Vildagliptin 50 mg once daily + current therapy (n=289)
Placebo run-in plus stable
dose of
current therapya
Period I Period II
24 weeks’ double-blind treatment 2 weeks
N=525
Lukashevich V et al Diabet Obes Metab 2011;13:942
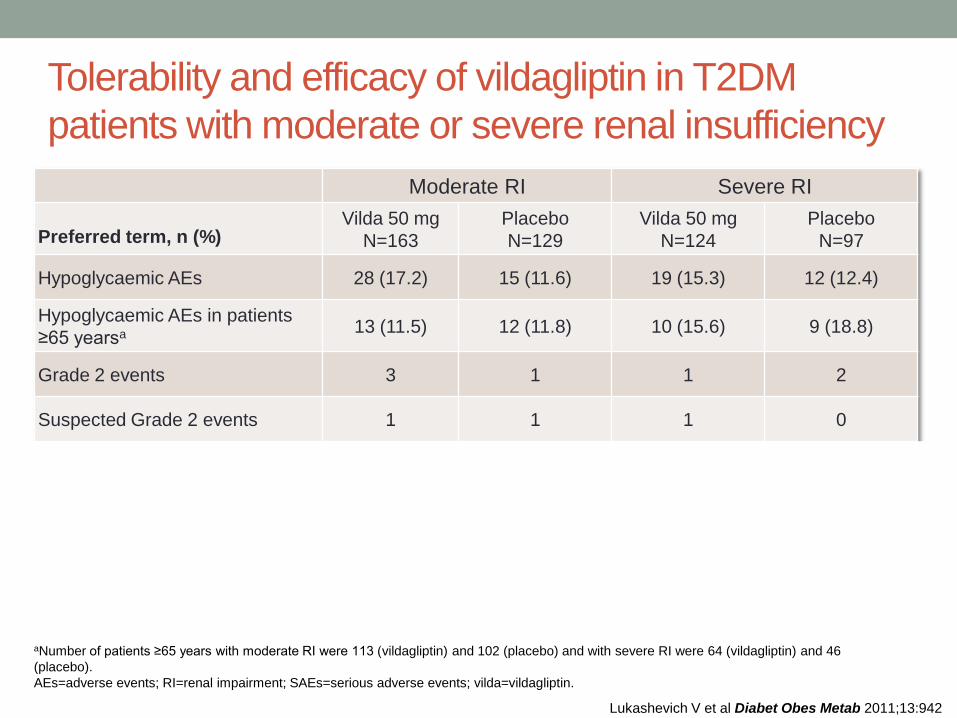
aNumber of patients ≥65 years with moderate RI were 113 (vildagliptin) and 102 (placebo) and with severe RI were 64 (vildagliptin) and 46
(placebo).
AEs=adverse events; RI=renal impairment; SAEs=serious adverse events; vilda=vildagliptin.
Moderate RI Severe RI
Preferred term, n (%) Vilda 50 mg
N=163
Placebo
N=129
Vilda 50 mg
N=124
Placebo
N=97
Hypoglycaemic AEs 28 (17.2) 15 (11.6) 19 (15.3) 12 (12.4)
Hypoglycaemic AEs in patients
≥65 yearsa 13 (11.5) 12 (11.8) 10 (15.6) 9 (18.8)
Grade 2 events 3 1 1 2
Suspected Grade 2 events 1 1 1 0
GFR (MDRD) (mL/min/1.73 m2)
Mean Baseline (BL) 39.3 40.3 21.9 20.9
Mean change from BL 0.9 0.6 -1.5 -1.1
Median change from BL -0.1 -0.1 -1.3 -1.9
Lukashevich V et al Diabet Obes Metab 2011;13:942
Tolerability and efficacy of vildagliptin in T2DM
patients with moderate or severe renal insufficiency

-1,0
-0,8
-0,6
-0,4
-0,2
0,0
Moderate RI
*P <0.0001 vs placebo. Full analysis set. BL=baseline; HbA1c=haemoglobin A1c; RI=renal impairment; T2DM=type 2 diabetes mellitus.
Severe RI
-1,0
-0,8
-0,6
-0,4
-0,2
0,0
Vildagliptin 50 mg once daily Placebo
BL= 7.86 7.79
Mean Change from
Baseline to End Point
Between-treatment
Difference vs Placebo
N= 157 128
*
Ad
juste
d M
ea
n C
ha
ng
e fro
m
Ba
se
line
in H
bA
1c (
%)
BL= 7.69 7.65
N= 122 95
* A
dju
ste
d M
ea
n C
ha
ng
e fro
m
Ba
se
line
in H
bA
1c (
%)
Mean Change from
Baseline to End Point
Between-treatment
Difference vs Placebo
Lukashevich V et al Diabet Obes Metab 2011;13:942
Tolerability and efficacy of vildagliptin in T2DM
patients with moderate or severe renal insufficiency
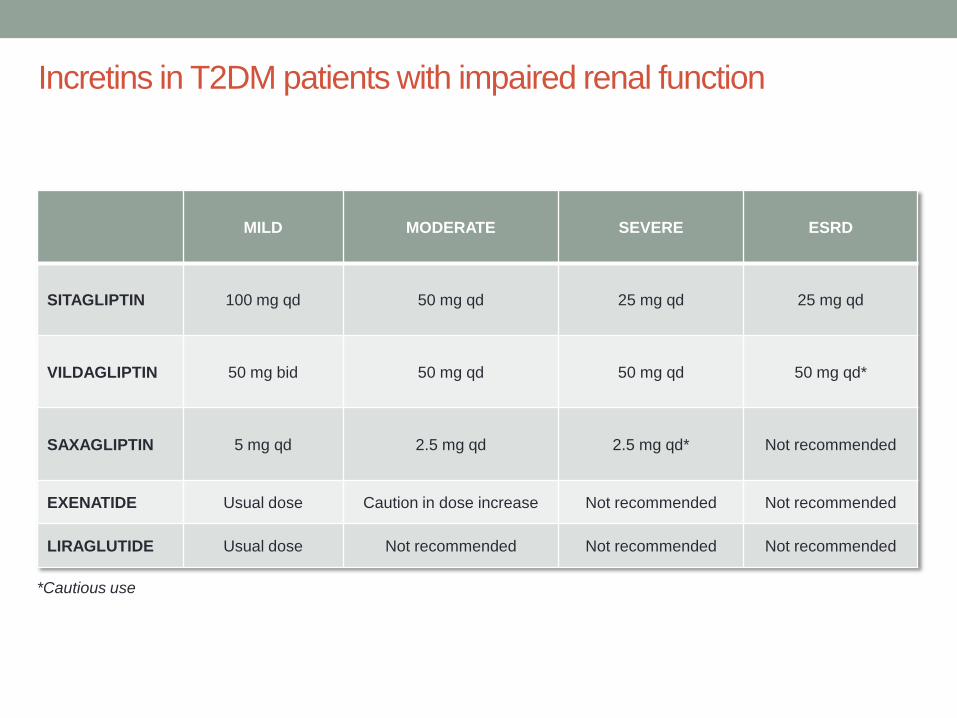
MILD MODERATE SEVERE ESRD
SITAGLIPTIN 100 mg qd 50 mg qd 25 mg qd 25 mg qd
VILDAGLIPTIN 50 mg bid 50 mg qd 50 mg qd 50 mg qd*
SAXAGLIPTIN 5 mg qd 2.5 mg qd 2.5 mg qd* Not recommended
EXENATIDE Usual dose Caution in dose increase Not recommended Not recommended
LIRAGLUTIDE Usual dose Not recommended Not recommended Not recommended
Incretins in T2DM patients with impaired renal function
*Cautious use

Alcuni problemi nella cura di Aristide
• Ipoglicemia
• Peso corporeo
• Insufficienza renale
• Sottostante malattia cardiovascolare
• Farmacoterapia multipla e complessa – interazione tra
farmaci

0
10
20
30
40
50
60
70
80
90
100
Gruppi di farmaci più prescritti nei pazienti
con diabete – ARNO 2010
Claritromicina i
Eritromicina i
Fluconazolo i
Ketoconazolo i
Rifampicina h
Metoprololo
(s)
Warfarin (s)
Diltiazem (s)
Atorvastatina (s)
Rosuvastatina (s)
Simvastatina (s)
Desametazone h
Diclofenach
Carbamazepina h
Fenobarbital h
Fentoina h
Fluoxetina i
Midazolam (s)
(s) – substrato; i – inibitore; h – induttore del citocromo p-450

Vildagliptin Sitagliptin Saxagliptin
Substrate forCYP3A4 No Low Yes
CYP3A5 No No Yes
CYP2C8 No Very low No
Dose proportion Yes Yes Yes
Meal effect No No No
Drug interaction No No Yes
Dose reduction with
CYP3A4 inhibitors No No Yes (2.5 mg)
Scheen A J. Diabetes, Obesity and Metabolism 2010; 12 (8):648–658
Interaction of DPP4 inhibitors with cytochrome p450

The choice of anti-hyperglycaemic agent should focus on:
Drug safety
Heart failure
Renal dysfunction
Bone fractures
Drug-drug interactions
Performance status
Strategies specifically minimising the risk of low
blood glucose may be preferred
In the elderly, the basic principle should be
“START LOW, GO SLOW”
Treatment in the elderly: summary