Embed Size (px)
Citation preview

Lab values beyond the numbers

Objectives
Recognition of abnormal Lab valuesTreatment of some of the more critical
values
CBC, diff
CBC’S
White Blood cell = WBC Differential
• Segs / polys •Lymphocytes
• Eosinophils •Monocytes
• Basophils •Bands
HemoglobinHematocritPlatelets
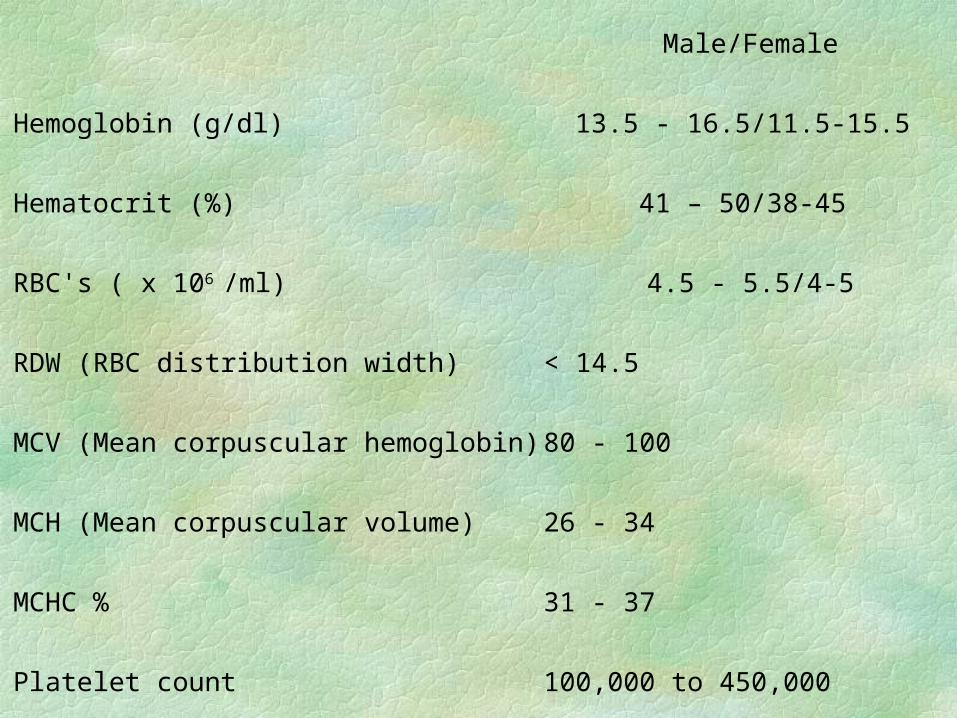
Male/Female
Hemoglobin (g/dl) 13.5 - 16.5/11.5-15.5
Hematocrit (%) 41 – 50/38-45
RBC's ( x 106 /ml) 4.5 - 5.5/4-5
RDW (RBC distribution width) < 14.5
MCV (Mean corpuscular hemoglobin) 80 - 100
MCH (Mean corpuscular volume) 26 - 34
MCHC % 31 - 37
Platelet count 100,000 to 450,000
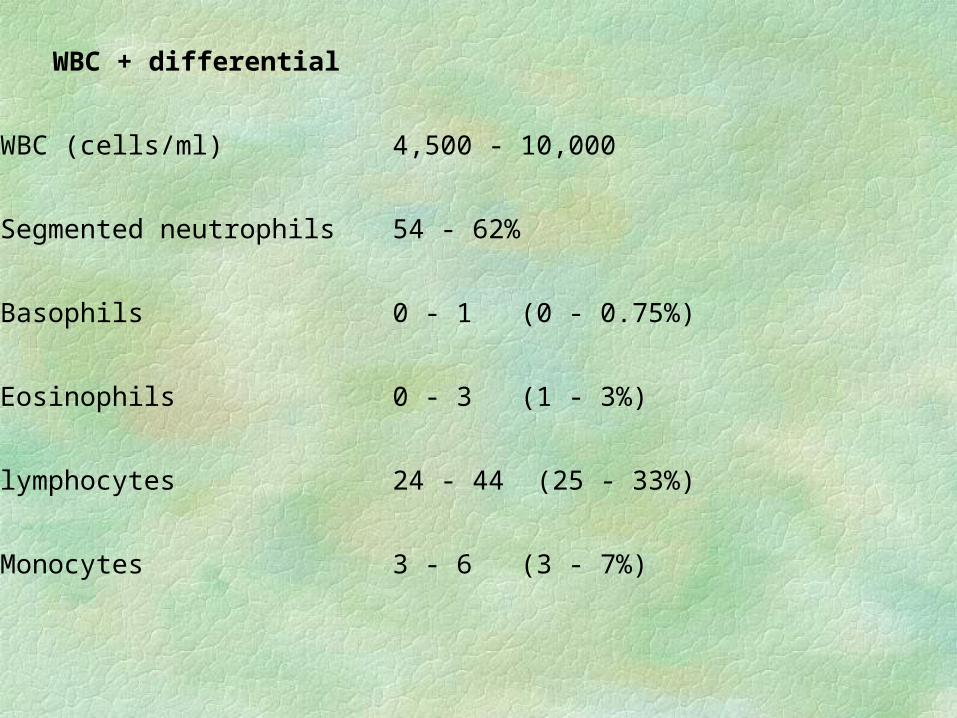
WBC + differential
WBC (cells/ml) 4,500 - 10,000
Segmented neutrophils 54 - 62%
Basophils 0 - 1 (0 - 0.75%)
Eosinophils 0 - 3 (1 - 3%)
lymphocytes 24 - 44 (25 - 33%)
Monocytes 3 - 6 (3 - 7%)
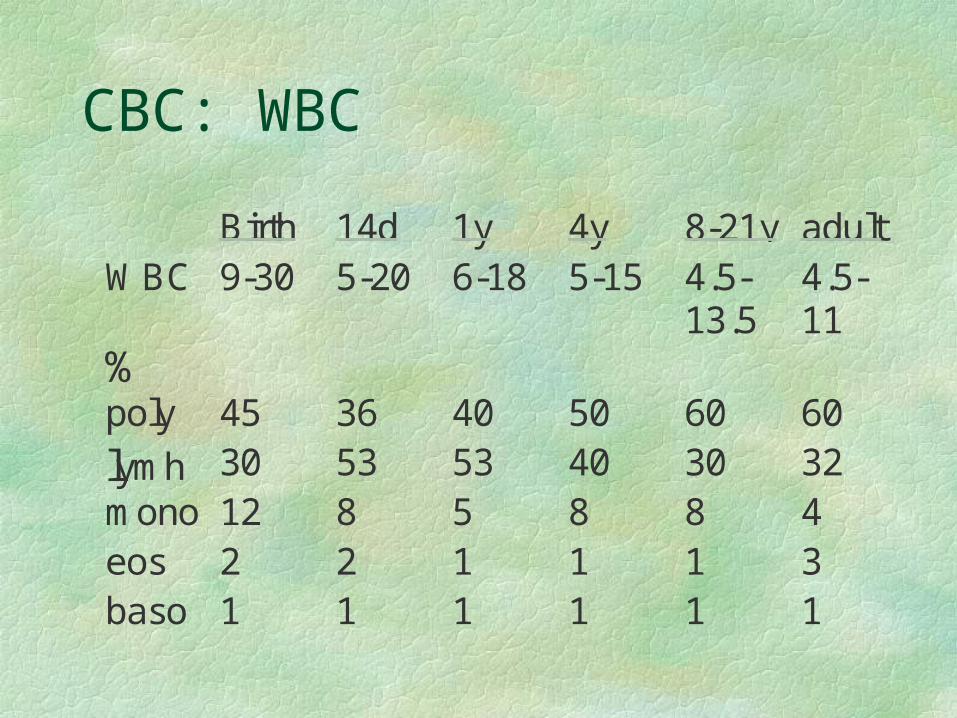
CBC: WBC
Birth 14d 1y 4y 8-21y adultWBC 9-30 5-20 6-18 5-15 4.5-
13.54.5-11
%poly 45 36 40 50 60 60
lymh 30 53 53 40 30 32mono 12 8 5 8 8 4eos 2 2 1 1 1 3baso 1 1 1 1 1 1
CBC: WBC
Increased Neutrophils physiologic
• newborn, pregnancy Pathologic
• acute infection
• inflammatory dz
• metabolic disorder
• tissue necrosis
• drugs
• stress
Decreased neutrophils Infection
• bacterial– typhiod – septicemia
• Viral– Hepatitis –
mono– flu –
measles
• myeloid hypoplasia• drugs
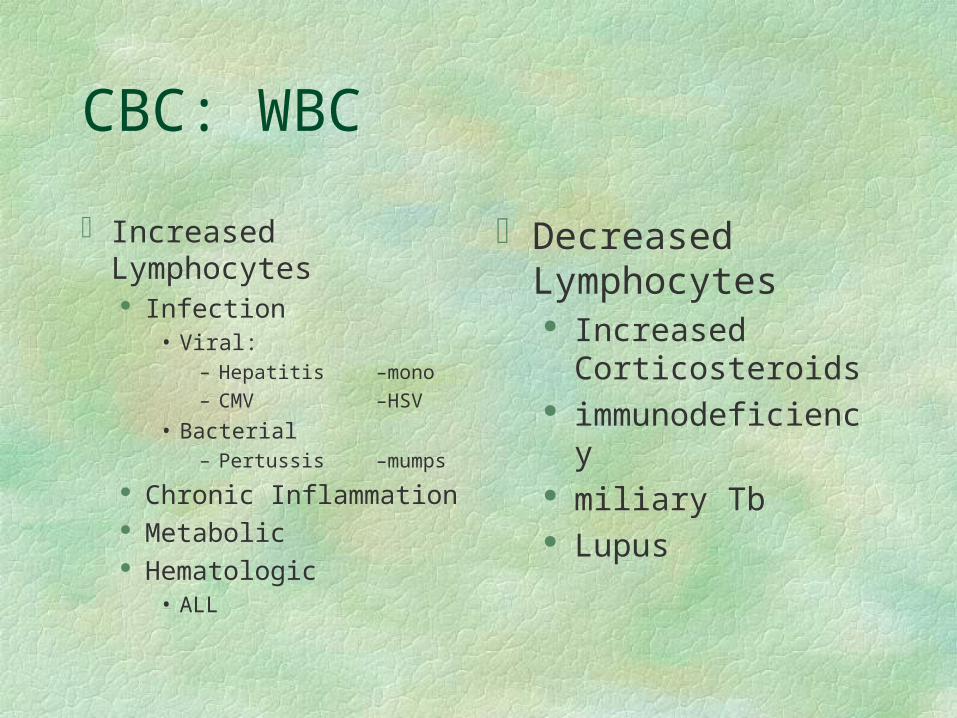
CBC: WBC
Increased Lymphocytes Infection
• Viral:– Hepatitis –mono
– CMV –HSV
• Bacterial– Pertussis –
mumps
Chronic Inflammation Metabolic Hematologic
• ALL
Decreased Lymphocytes
Increased Corticosteroids
immunodeficiency miliary Tb Lupus
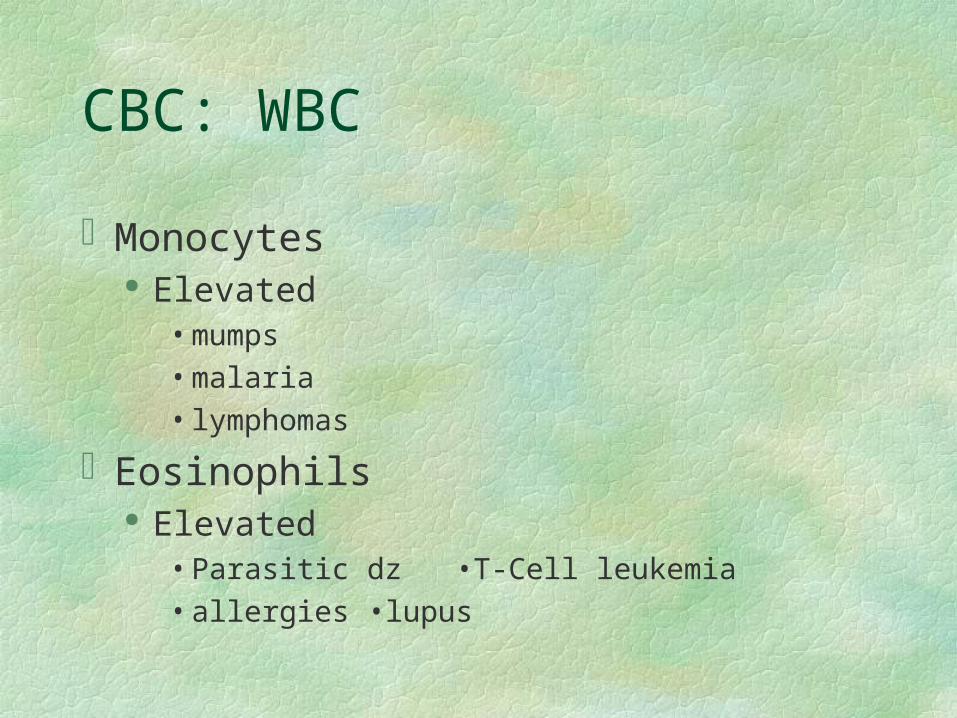
CBC: WBC
Monocytes Elevated
• mumps
• malaria
• lymphomas
Eosinophils Elevated
• Parasitic dz •T-Cell leukemia
• allergies •lupus
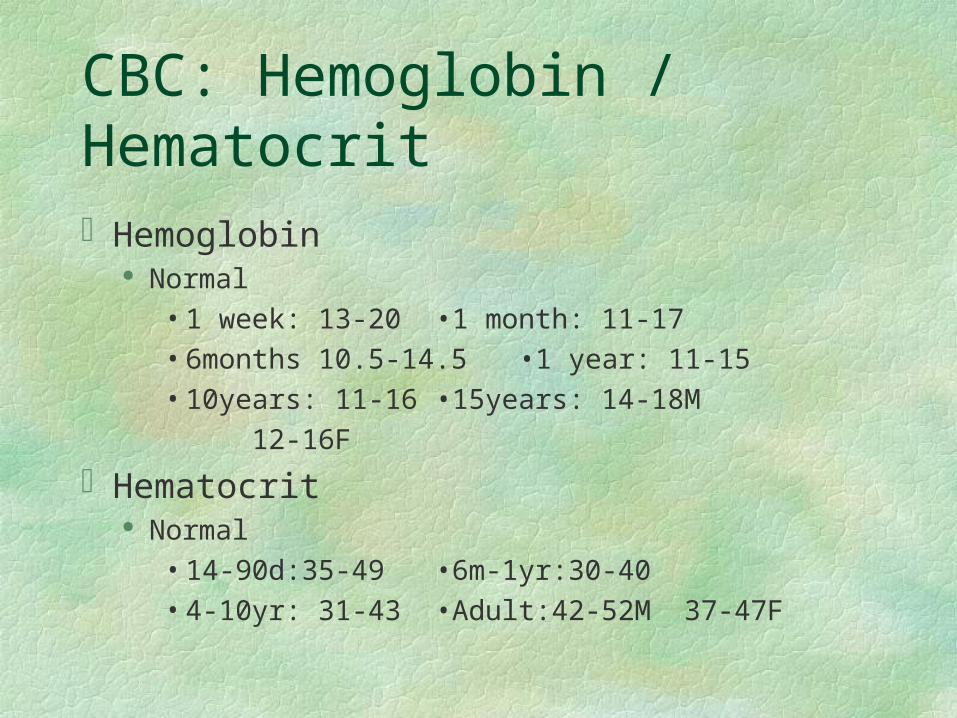
CBC: Hemoglobin / Hematocrit
Hemoglobin Normal
• 1 week: 13-20 •1 month: 11-17
• 6months 10.5-14.5 •1 year: 11-15
• 10years: 11-16 •15years: 14-18M
12-16F
Hematocrit Normal
• 14-90d:35-49 •6m-1yr:30-40
• 4-10yr: 31-43 •Adult:42-52M 37-47F
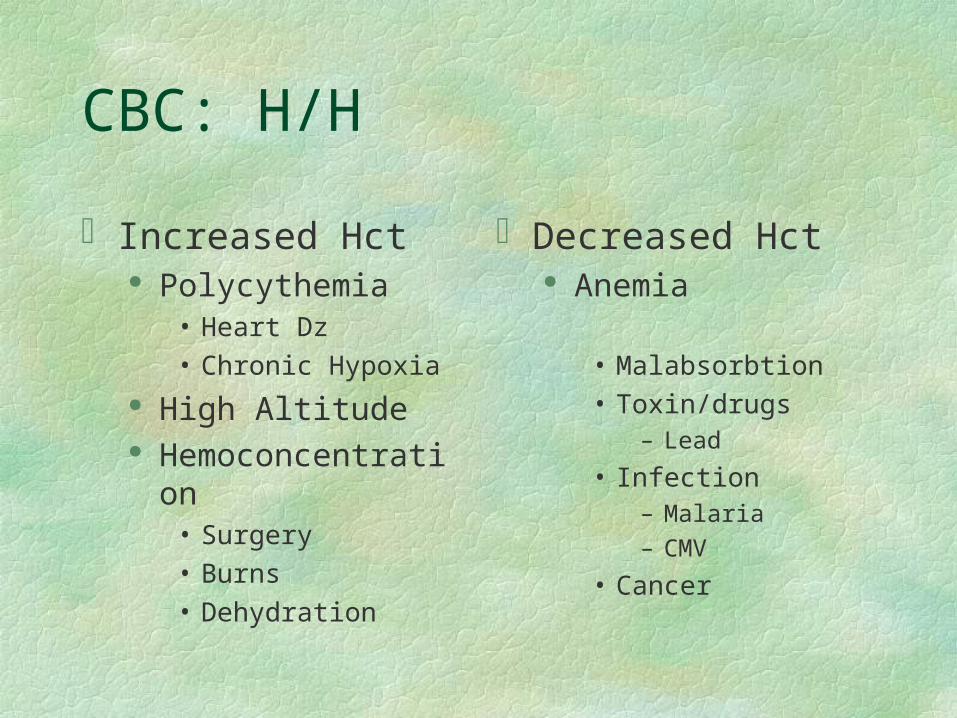
CBC: H/H
Increased Hct Polycythemia
• Heart Dz
• Chronic Hypoxia High Altitude Hemoconcentration
• Surgery
• Burns
• Dehydration
Decreased Hct Anemia
• Malabsorbtion
• Toxin/drugs– Lead
• Infection– Malaria
– CMV
• Cancer
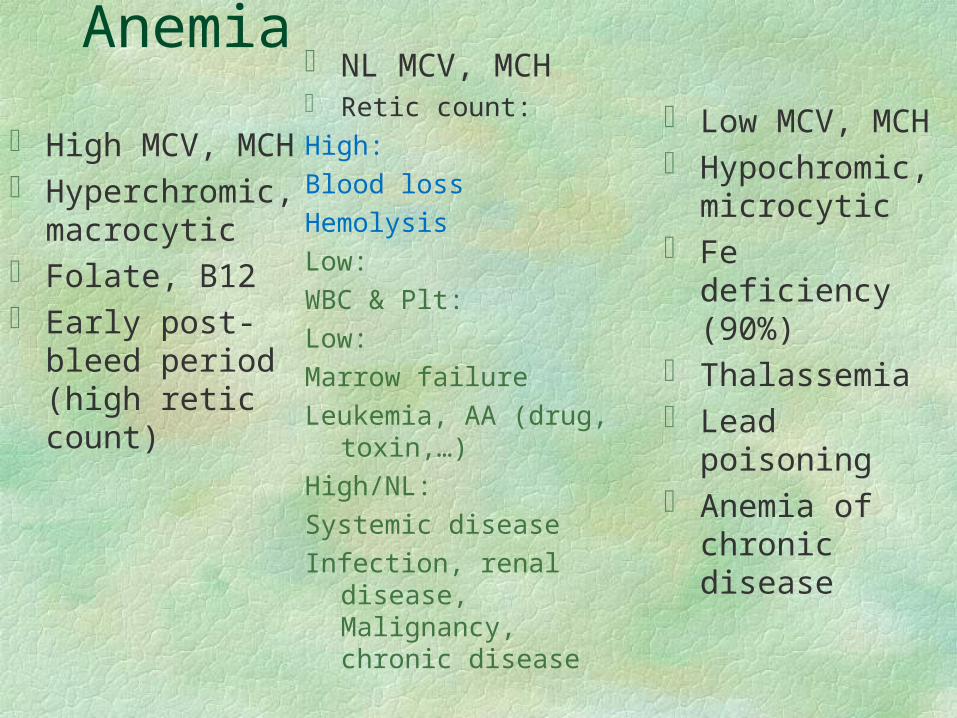
Anemia
High MCV, MCH Hyperchromic,
macrocytic Folate, B12 Early post-bleed
period (high retic count)
Low MCV, MCH Hypochromic,
microcytic Fe deficiency
(90%) Thalassemia Lead poisoning Anemia of chronic
disease
NL MCV, MCH Retic count:
High:
Blood loss
Hemolysis
Low:
WBC & Plt:
Low:
Marrow failure
Leukemia, AA (drug, toxin,…)
High/NL:
Systemic disease
Infection, renal disease, Malignancy, chronic disease
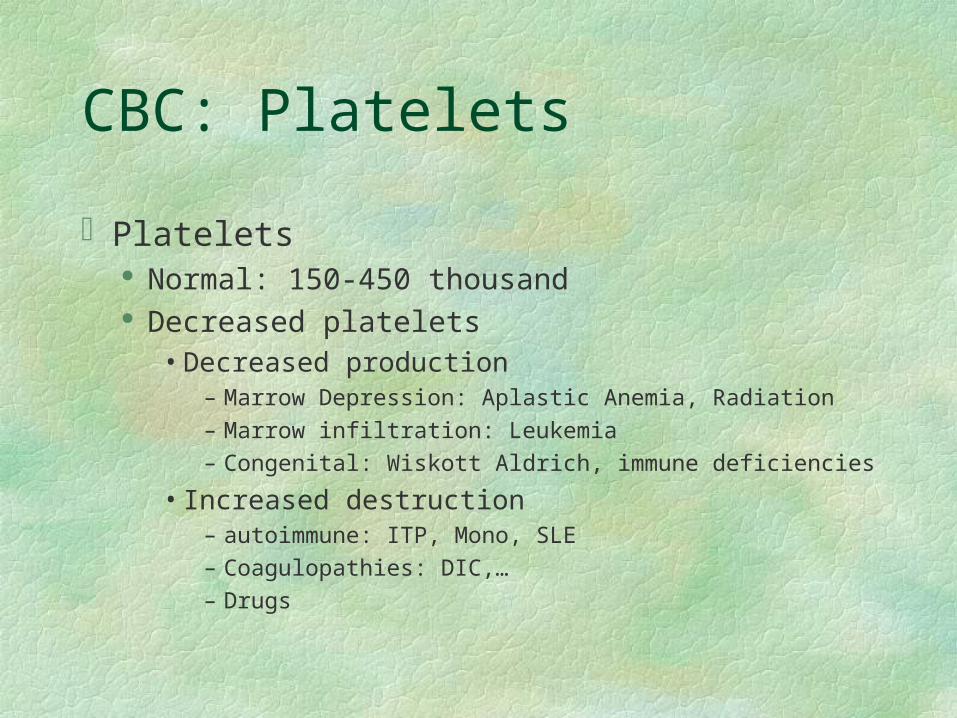
CBC: Platelets
Platelets Normal: 150-450 thousand Decreased platelets
• Decreased production– Marrow Depression: Aplastic Anemia, Radiation– Marrow infiltration: Leukemia– Congenital: Wiskott Aldrich, immune deficiencies
• Increased destruction– autoimmune: ITP, Mono, SLE– Coagulopathies: DIC,…– Drugs
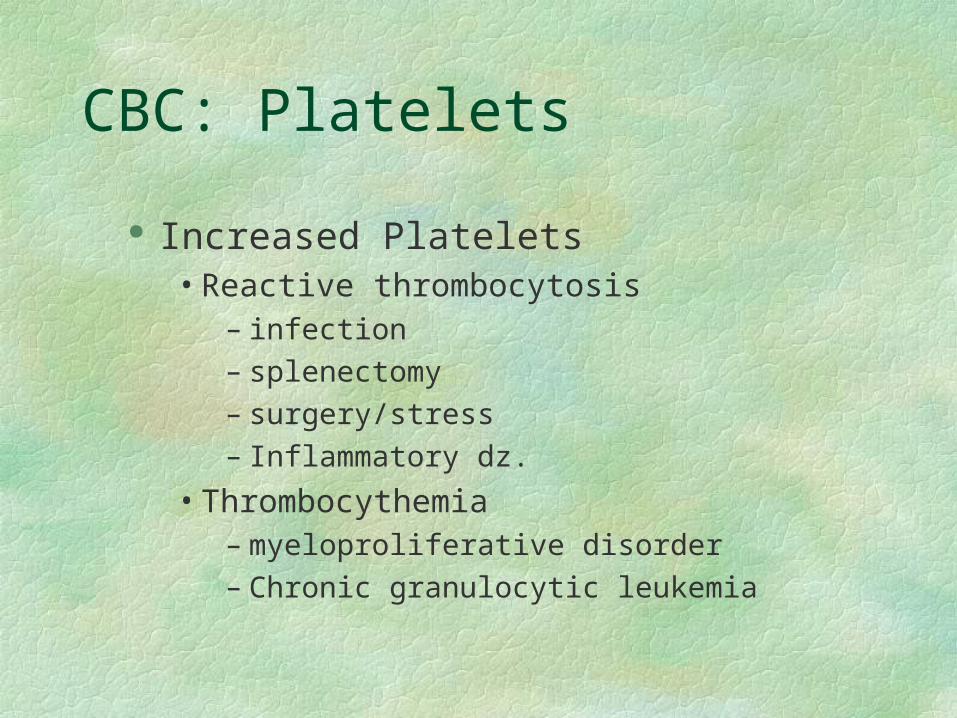
CBC: Platelets
Increased Platelets• Reactive thrombocytosis
– infection
– splenectomy
– surgery/stress
– Inflammatory dz.
• Thrombocythemia– myeloproliferative disorder
– Chronic granulocytic leukemia
Case-study
Ferritin, TIBC, Serum Iron, Transferrin
Total iron binding capacity (TIBC) 250 - 420 mcg/dl Transferrin > 200 mg/dl Iron (mcg/dl) 65 – 150 Ferritin (ng/ml) 13 - 300
B12, Folate
Folate (ng/dl) 3.6 – 20B12 (pg/ml) 200-800
Stool/Exam (S/E)
×3 (ova, parasite, …)Occult Blood

Inflammatory Index
ESRhs CRP
Chemistries: BUN
Blood Urea Nitrogen Normal: 5-20 mg/dl Elevated
• GI Bleed •High Protein Diet •Steroids• Shock •Dehydration •Diarrhea• Burns •Tissue Necrosis Renal Dz
Decreased• Anabolic Steroids •Malnutrition• Liver Dz •Pregnancy
Chemistries: Cr
Creatinine Normal: Child usually less than 1 Increased:
• Renal Dz
• Muscle necrosis
• hypovolemia
Chemistries: Glucose
Glucose Normal: 60-110mg/dl (infants >40) Hyperglycemia
• diabetes •Pancreatitis
• Cushing's dz •Pheochromocytoma
• drugs (ie: Steroids) Hypoglycemia
• Malaria •liver dz •Malignancy
• enzyme deficiency •Malnutrition
Types of glucose tests
Random Blood sugar (not fasting)
Fasting Blood sugar (nothing to eat or drink except H2O for 12
hrs)Glucose Tolerance Test (Starts fasting, then given sweet drink and
measured over time)Hemoglobin A1c (Measures glucose control over 3 month)
Glucose, fasting (mg/dl) 60 - 110Glucose (2 hours postprandial) (mg/dl) Up to 140Hemoglobin A1c 6 - 8
Diabetes
Casual plasma glucose concentration >200 mg/dl + symptoms of diabetes. Casual is defined as any time of day without regard to time since last meal. The classic symptoms of diabetes include polyuria, polydipsia and unexplained weight loss.
• FPG >126 mg/dl. Fasting is defined as no caloric intake for at least 8 h.
• 2-hour post-load glucose >200 mg/dl during an OGTT.
Chemistries: Glucose
Treatment of Hypoglycemia Neonate or child: 0.5 to 1 gram / kg
• if using D25 would be 2-4 cc / kg
– dilute D50 1:1 with sterile water
• if using D10 5-10 cc / kg
– dilute D50 1:4 Adult: ampule of D50
Chemistries: Glucose
Treatment of Hyperglycemia Fluid bolus 10cc/kg NS insulin 0.05u - 1 unit/kg
If diabetic in DKA be very judicious of fluid administration and no NHCO3 unless cardiac instability
CASE-STUDY
Uric Acid
Uric acid (male) 2.0 - 8.0 mg/dl
(female) 2.0 - 7.5 mg/dl
CASE - STUDY
Cu, Ceruloplasmin, zinc
Copper 70-155mcg/dlCeruloplasmin 23-43mg/dl
Zinc 0.85-1.25mcg/ml
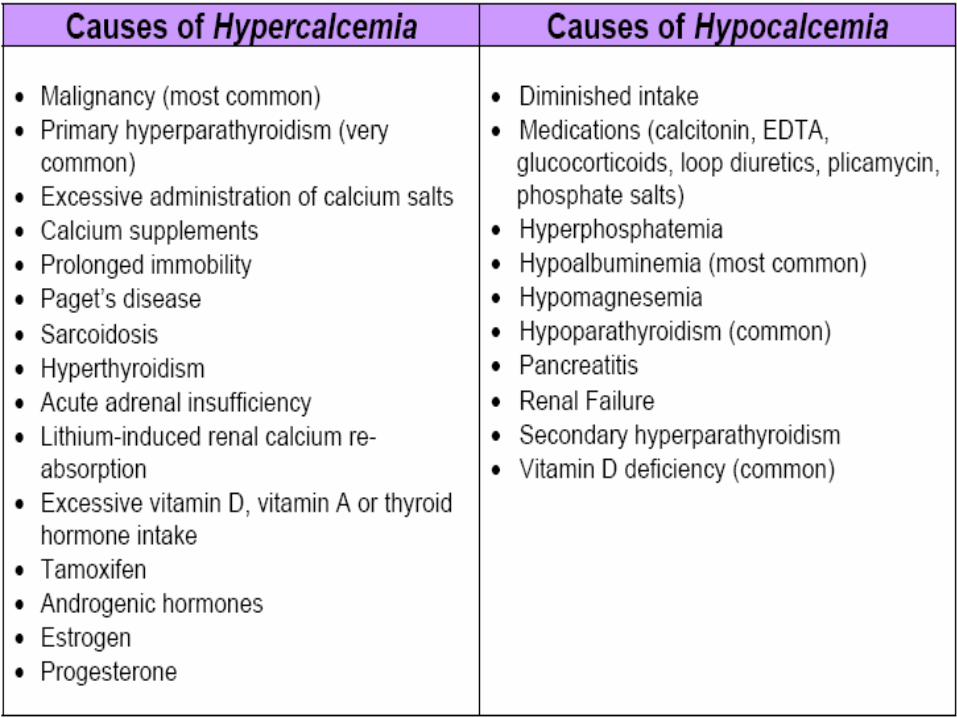
Chemistries: Ca+
Calcium Normal 8-11mg/dl Panic Value:<7 or > 12 (tetni, Sz, arrhythmia) Hypercalcemia (CHIMPS)
• C= Cancer
• H= Hyperthyroid
• I= Iatrogens
• M= Multiple Myeloma
• P= Primary Hyperparathyroid
• S= Sarcoid
Chemistries: Ca+
Hypocalcemia• renal failure
• hypoparathyroidism
• magnesium deficiency
• anticonvulsants
• Rickets
• Pancreatitis
• Blood transfusions
CASE-STUDY
25 hydroxy vitamin D >30nmol/l
T3, T4, TSH, Free thyroxinAlbPTHMgP

CASE-STUDY
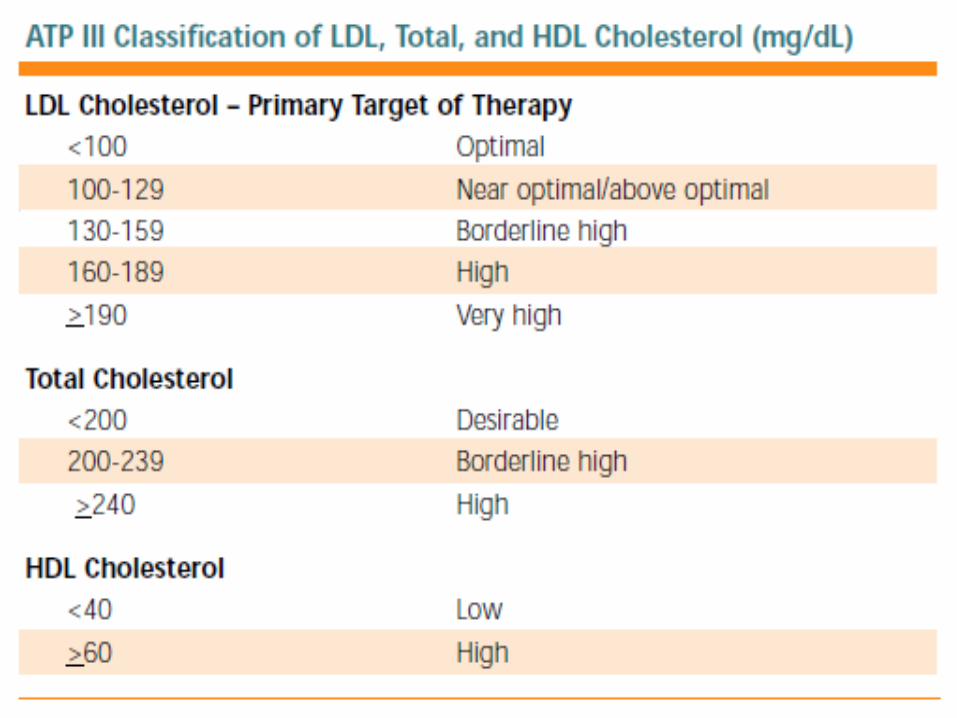
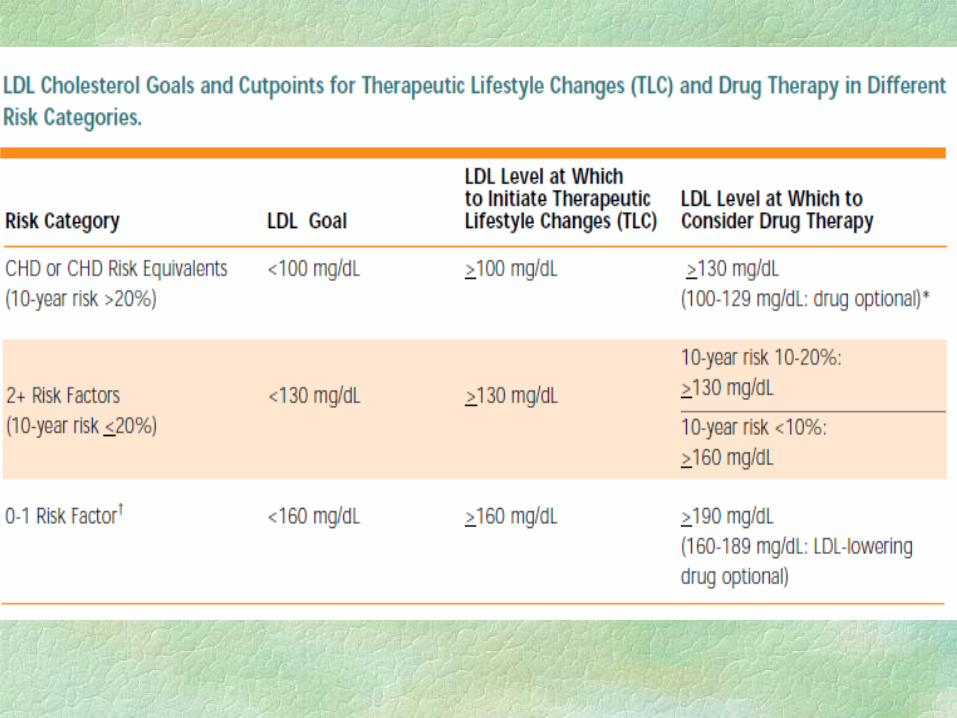
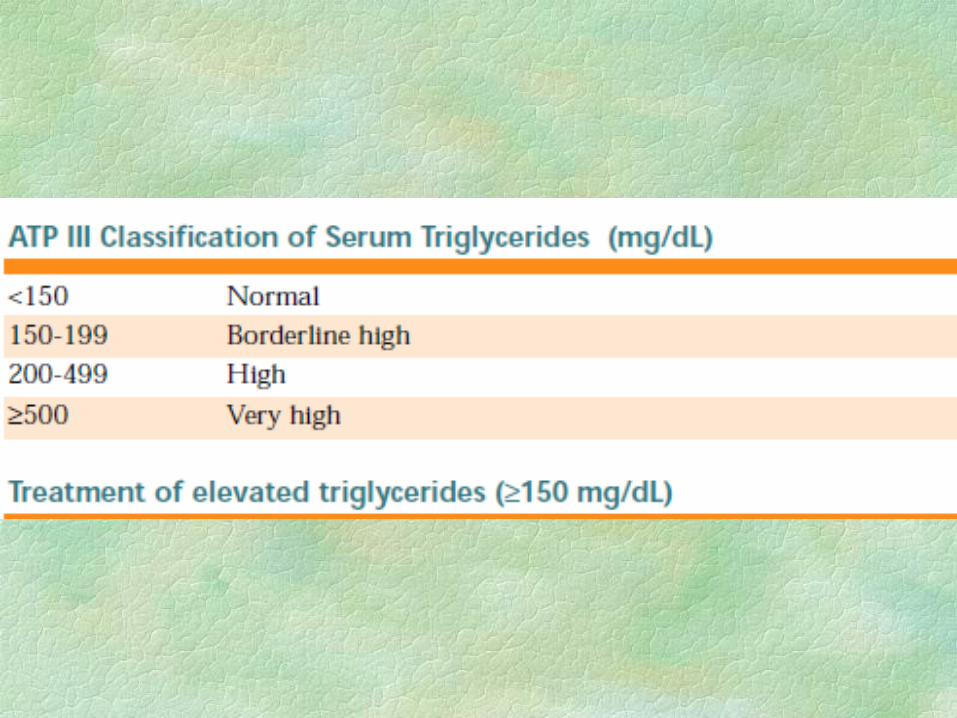
Lipids
Cholesterol
HDL (good cholesterol)
Ratio
LDL (bad cholesterol)
Triglycerides

CASE-STUDY
U/A, U/C
COLOR (Normal: Yellow to Amber)
– Urochrome gives urine its color. Factors that may alter color include specific gravity, foods, bilirubin, and drugs
CHARACTER (Normal: Clear)
– If urine is cloudy or hazy instead of normally clear, it may be due to white blood cells, bacteria, fecal contamination, prostatic fluid, or vaginal secretions.
SPECIFIC GRAVITY (Normal: 1.015-1.025) is the weight of urine.
A low specific gravity indicates dilute urine and a high specific gravity indicates concentrated urine.
pH (Normal: 4.5 –8.0)
- Changes seen with acid base imbalances. Values will increase with urinary tract infections and if the specimen is old (ammonia – a base, is produced).
GLUCOSE (Normal: Negative) – The renal threshold for blood sugar is 160-180 mg/dl.
Pregnancy, endocrine, and renal problems can lower the renal threshold – thus glucose spills over more easily.
KETONES (Normal: Negative) – Ketones are a product of fat metabolism.
Causes of ketonuria include DKA, starvation, fasting, vomiting, strenuous exercise, and dehydration.
PROTEIN (Normal: Negative)
– Benign conditions that increase protein in urine are stress, pregnancy, cold, fever, strenuous exercise, and vaginal secretions.
-Non-benign conditions are hypertension, diabetes (renal damage), post-renal infection (renal damage), and multiple myeloma (also serum protein elevated, A/G ratio abnormal, urine protein up, Bence-Jones proteins up).
BILIRUBIN (Normal: Negative) - Bilirubin in urine is water-soluble – When bilirubin is present in the urine, it is usually due to a hepatobiliary obstruction.
BLOOD (Normal: Negative) –
If positive, urine is usually cloudy. If dipstick is positive, must look at urine microscopically in the lab for:
(1) Red Blood Cells (RBCs) (stone, urinary tract infection, pyelonephritis, glomerulonephritis, renal cancer, bladder cancer, strenuous exercise, or menses)
(2) Myoglobin (MI, trauma, crush injuries, or burns) (3) Hemoglobin (transfusion reaction, sickle cell, DIC, or
hypertension). NITRITE (Normal: Negative)
– Bacteria is broken down into urinary nitrites and nitrate. Nitrites are positive when bacteria are in urine. LEUKOCYTE ESTERASE (Normal: Negative)
– Reflects presence of white blood cells. Positive findings suggest urinary tract infection.
BACTERIA (Normal: Negative)
– If positive, suspect either your patient has a urinary tract infection or the specimen was contaminated.
RBCs (RED BLOOD CELLS) (Normal: Negative)
– If >5, think glomerulonephritis, pyelonephritis, renal trauma, tumor, kidney stones, cystitis, or genitourinary malignancy.
WBCS (WHITE BLOOD CELLS) (Normal: Negative)
– If > 50, think urinary tract infection.
If < 50, it is usually due to exercise, fever, renal disease, or urinary tract disease.
EPITHELIAL CELLS (Normal: Negative)
– When present in large to moderate amounts, worry about either acute tubular necrosis or acute glomerulonephritis.
CASTS (Normal: Negative)
- When present, may be due to nephrotic syndrome, glomerulonephritis, kidney failure, or renal malignancy.
CASE-STUDY
Liver Function Tests
High enzymes can signal liver damage
(meds, hepatitis, alcohol, drugs) ALT (SGPT) AST (SGOT) Bilirubin yellow fluid produced when RBC’s break down
(liver disease; indinavir and atazanavir can elevate bili)
Alkaline Phosphatase PT, PTT
CASE-STUDY
Other Tests
Albumin:
major protein in blood
maintains balance in cells;carries nutrients;can affect other lab tests
CASE-STUDY











![Understanding Lab Values When on Dialysis-2[1]](https://img.pdfslide.net/doc/110x75/577cd2d21a28ab9e789610e7/understanding-lab-values-when-on-dialysis-21.jpg)