Embed Size (px)
Citation preview

Pediatric Case Study
By: Ellinor Lagerberg
2014
1
Introduction
Z.M. is a 26 month old female child that was admitted to Florida Hospital January 21,
2014 for diarrhea, vomiting and hypoglycemia. Z.M. contracted a gastrointestinal virus from a
family member and the virus caused her to vomit extensively and to lose fluids. This caused her
blood sugar to plummet and her vital signs to diminish. Z.M. has a genetic disorder called
Stickler Syndrome (SS) that requires her to be fed via enteral feeding. Upon admission, Z.M.’s
weight was recorded at 9 kg and she was 80 centimeters tall. Z.M.’s mother said she had only
grown 4 inches over past year and she is small for her age. Since admission, Z.M. had gained
1.2 kg which was most likely contributed to fluid repletion therapy. This patient was chosen to
understand the nutritional complication of a genetic syndrome. The patient was initially seen
on January 21, 2014 and followed through January 22, 2014. The focus of this study is to
develop an understanding of the importance of initiating enteral feeding in nutritional
compromised children.
Social history
Z.M. lives with both her parents and her two older brothers in Maryland. She was
admitted to the hospital while on vacation at Walt Disney World. None of the family members
smoke and there are no pets in the household. Both of Z.M.’s parents work and her mother is
employed by a healthcare company. Z.M. is insured via private insurance through Carefirst Blue
Choice and by Medicaid. Her maternal grandmother is currently suffering from lung and
bladder cancer.
2

Normal anatomy & physiology of applicable body functions
Stickler Syndrome is a genetic disorder of connective tissue that can cause problems
with vision, hearing, facial and skeletal development. SS is also known as hereditary progressive
arthro-ophthalmopathy and is the result from mutations in at least three collagen genes. SS is
divided into three types and each type is determined by the genetic mutation of the gene. The
three known genes are COL2A1, COL11A1 and COL11A2. However, a fourth gene, COL9A1, has
been observed in a rare autosomal recessive form of SS (1).
Stickler Syndrome Type 1COL2A1 codes for a component of type II collagen that adds structure
and strength to connective tissues and the vitreous.
Type 1, is caused by mutations in COL2A1. It is the most common and is responsible for
more than 80% of all cases of SS. Type 2 is caused by mutations in COL11A1 and type 3 by
mutations in COL11A2. Children born with types 1 and 2 have ocular disabilities and those with
type 3 SS are nonocular (2).
3

Children born with Stickler syndrome often have distinctive facial features such as
prominent eyes, a small nose and a receding chin (3).
Typical Facial & Skeletal Characteristics
Having a small jaw with a tongue that has restricted movement can result in breathing
and feeding difficulties during infancy. Laryngomalacia also impacts feeding capabilities since
the floppy tissue above the vocal cords falls into the airway breathing. Some children with SS
are born with Pierre Robin sequence (PRS). PRS is a triad of symptoms: micrognathia,
glossoptosis, and airway obstruction. Infants are frequently born with a hypoplastic mandible
and difficulties breathing (4).
Pierre Robin Sequence
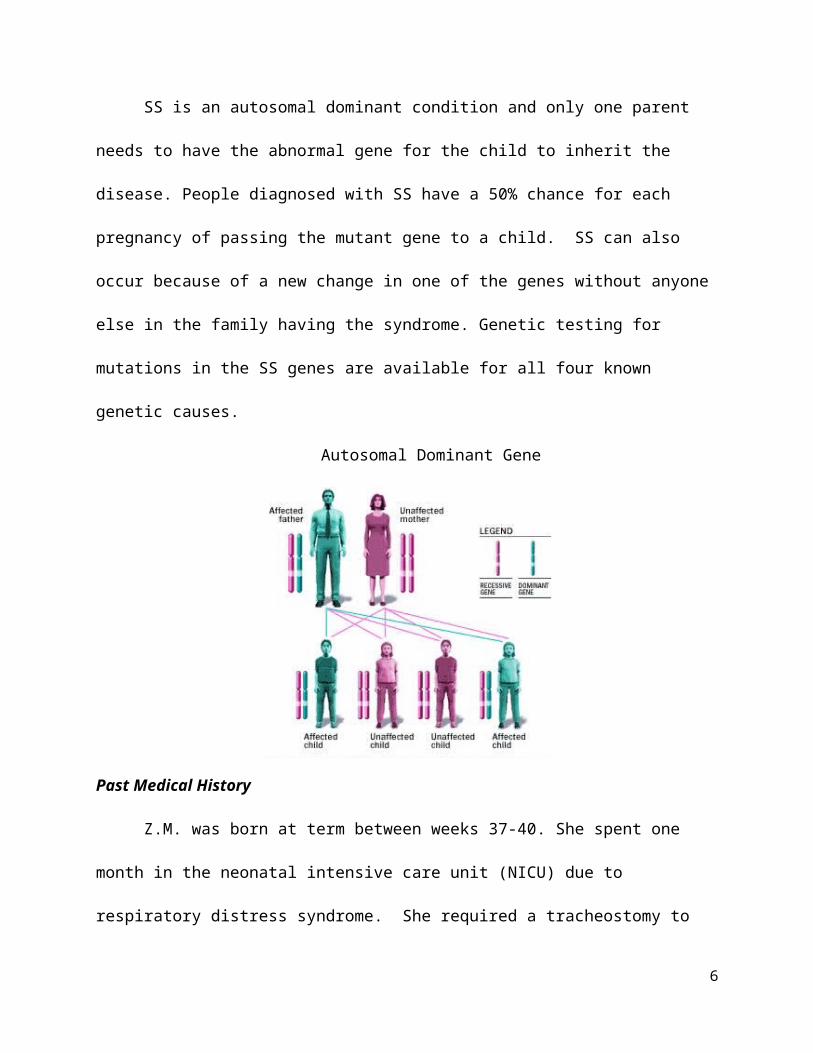
SS is an autosomal dominant condition and only one parent needs to have the abnormal
gene for the child to inherit the disease. People diagnosed with SS have a 50% chance for each
4

pregnancy of passing the mutant gene to a child. SS can also occur because of a new change in
one of the genes without anyone else in the family having the syndrome. Genetic testing for
mutations in the SS genes are available for all four known genetic causes.
Autosomal Dominant Gene
Past Medical History
Z.M. was born at term between weeks 37-40. She spent one month in the neonatal
intensive care unit (NICU) due to respiratory distress syndrome. She required a tracheostomy
to assist with breathing due to airway obstructions. Tracheostomy is usually reversed once the
baby has grown large enough that the airway is no longer blocked. Airway obstruction in
infants with SS frequently improves with time since the mandible grows more in the postnatal
period or because glossoptosis improves with growth and neurologic development (4).
Z.M. was born with a cleft palate and laryngomalacia, thus preventing her from feeding
orally. She had a gastrostomy tube placed shortly after birth. In 2012, she contracted
tracheitis, a bacterial infection of the trachea. Tracheitis is most often caused by the bacteria
5
Staphylococcus aureus (5). In October 2012, she had a bronchoscopy exam to evaluate her
respiratory system related to tracheitis.
Present medical status and treatment
There is no cure for SS; but treatment includes managing signs and symptoms of the
disorder. Pharmacologic treatments include pain and glaucoma medication. Speech therapy,
physical therapy, hearing aids, and special education may be needed for some children. Surgical
treatments include jaw surgery, cleft palate repair, ear tubes, eye surgery and joint
replacement due to early onset of arthritis (6).
Z.M. was admitted with gastroenteritis and hypoglycemia. Z.M.’s mother reported her
and her husband did their normal feeding routine feeding the day before the onset of vomiting.
While Z.M. was receiving her continuous tube feeding infusion she had multiple episodes of
emesis throughout the night. Z.M.’s parents kept a close eye on her. Around 6am Z.M’s
showed signs of lethargy and weakness. She was not responding the way she usually does.
Z.M.’s mother took her to the emergency room at Florida Hospital Celebration. Z.M. was
admitted to the hospital. She had blood glucose at 19 mg/dL. Low blood glucose can impair
the brain’s ability to function. Severe or prolonged hypoglycemia may result in seizures and
serious brain injury. Due to her condition she was transferred via ambulance to Florida Hospital
South for specialized care.
Table 1
Lab Normal range L.M. Labs from 1/20/14Sodium 134-145 mEq/L 144Potassium 3.6-5.2 mEq/L 3.4BUN 7-20 mg/dL 30Creatinine 0.2-0.5 mg/dL 0.4Glucose 65-99 mg/dL 21
6
Glucose Accucheck 65-99 mg/dL 111, 108, 112, 137, 54, 47Z.M. was admitted to Florida Hospital South in the morning. She was observed sleeping
most of the day. She was most likely sleeping as a side effect from the medications she was
given. Z.M. did not have to undergo any medical or surgical procedures during her admission.
Medications: see table 4 p. 10
Medical Nutrition therapy
Z.M. has received enteral feedings via g-tube since birth due to her oral complications.
Children with SS have increased energy expenditures because of the increased work of
breathing and feeding challenges. Her home tube feeding regiment consisted of 4 bottles of
Pediasure Peptide 1.0 calorie concentrated at 24/kcal/oz. The precise recipe for the home tube
feeding is unknown. Concentrated infant formulas can be appropriate for infants and toddlers
that are not growing fast enough (7). Z.M.‘s mother describes that Z.M. is tolerating her tube
feedings well and this is the first time she has had an episode of emesis. Z.M.’s mother also
provided information that Z.M.’s tube feeding volume was increased about two weeks ago after
her local physician and R.D. reassessed her needs. The physician had also approved
introduction of small amounts of pureed foods after Z.M. passed a recent swallow study.
Usual Intake
Table 2
Home tube feeding per Z.M.’s mother: ~ 4 bottles of Pediasure Peptide 1.0 cal 24 kcal concentrate + ½ bottle of water: 1080ml total ~0.89 kcal/ml.
Z.M. is feed 150ml TID bolus + 500ml continuously overnight = 950ml/24hrs. 85% of DRIsFluids: TF + flush = 808ml water, 85% DRIs, additional flushes 5ml after each feed = 25ml/day; TF + flushes =833ml/dayKcal Protein CHO Fiber Fat Iron Calcium Vitamin D Vitamin A Vitamin C
846 (83g/kg)
25g (2.4g/kg)
126g (12.3g/kg)
2.8g 38g 13.3 mg 1000mg 500 IU 2375 IU 96mg
7
Robin Sequence and Stickler Syndrome Clinical Evaluation (2)Protocol outlining clinical evaluation and medical and surgical management of Robin Sequence and Stickler
Syndrome related to airway obstruction.
Z.M.’s diet order in the hospital was NPO per physician however she did receive 245 kcal
from IV medications. Her nutrition diagnosis was inadequate EN infusion related to schedule of
infusion interrupted as evidenced by nausea, vomiting and diarrhea. Z.M. was monitored for
initiation of tube feeding and once initiated she would be placed back on home feeds, since she
previously tolerated feeds. A follow up was scheduled for the next day and she would then be
assessed for bowel sounds and her fluid and electrolyte status would be monitored. When
reviewing Z.M.’s chart the following day, it was noted that she had been discharged.
8
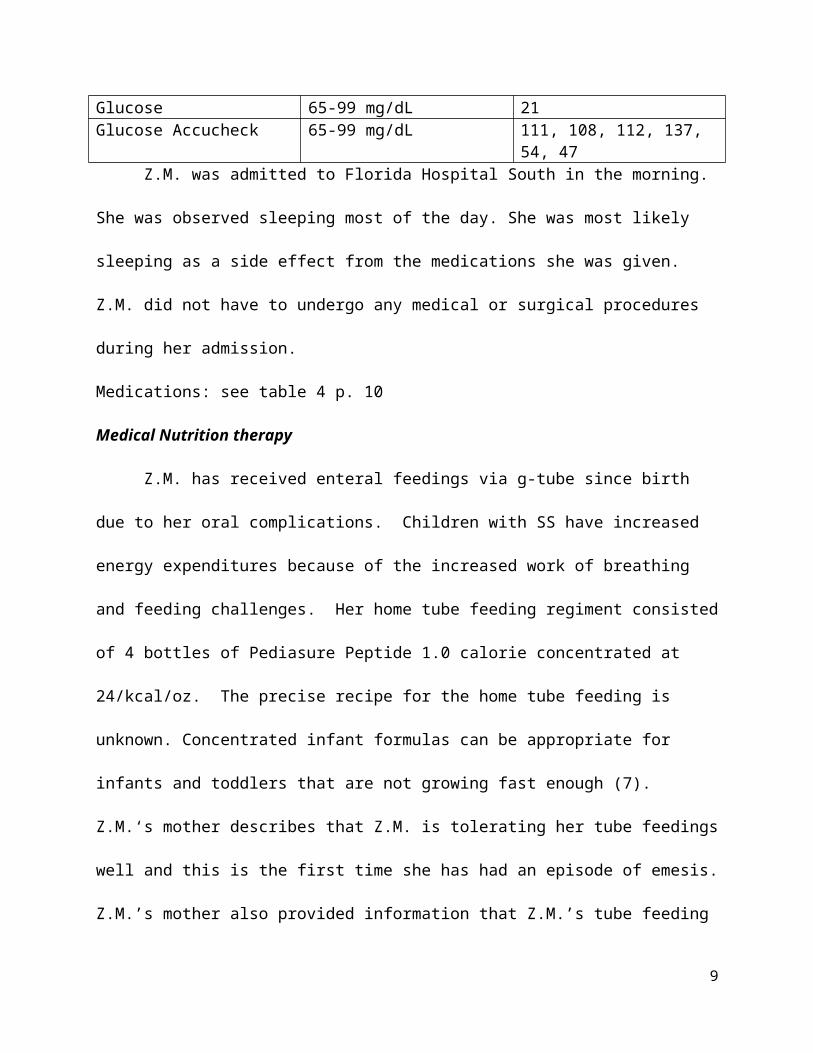
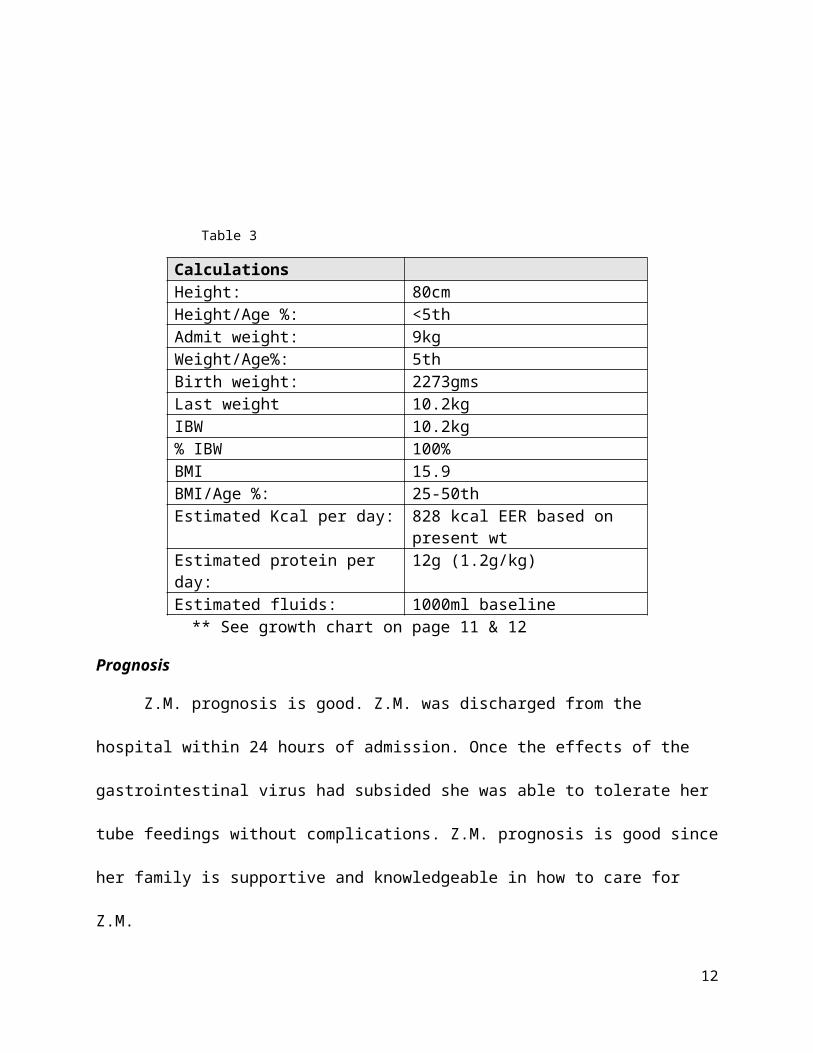
Table 3
CalculationsHeight: 80cmHeight/Age %: <5thAdmit weight: 9kgWeight/Age%: 5thBirth weight: 2273gmsLast weight 10.2kgIBW 10.2kg% IBW 100%BMI 15.9BMI/Age %: 25-50thEstimated Kcal per day: 828 kcal EER based on present wtEstimated protein per day: 12g (1.2g/kg)Estimated fluids: 1000ml baseline
** See growth chart on page 11 & 12
Prognosis
Z.M. prognosis is good. Z.M. was discharged from the hospital within 24 hours of
admission. Once the effects of the gastrointestinal virus had subsided she was able to tolerate
her tube feedings without complications. Z.M. prognosis is good since her family is supportive
and knowledgeable in how to care for Z.M.
Summary & Conclusion
This study allowed me to realize how vulnerable a small child can be especially while
receiving enteral feeding and how important it is to initiate feedings for nutrition. This case
study also allowed me to research a genetic disorder and the complications associated with the
disease. It also allowed me to gain experience in pediatric nutrition therapy and to understand
how important it is to interact with and build a good report with family members of a sick child.
9

Medications (8)
Table 4
Medication Treatment Drug/food Interaction
Side effect
Acetaminophen Used to relieve mild to moderate pain and to reduce fever. It works by changing the way the body senses pain and by cooling the body.
N/A Hives, itching, swelling of the face, throat, tongue, lips, eyes, hands, feet, ankles, or lower legs
Zofran Used to prevent nausea and vomiting. It works by blocking the action of serotonin, a natural substance that may cause nausea and vomiting.
N/A Diarrhea, constipation, weakness, tiredness.
IV D5 ¼ NS (dextrose, kCL, NaCl)60ml/16.7hrs =245 kcalHome MedicationFlovent Used to prevent difficulty breathing,
chest tightness, wheezing, and coughing caused by asthma. It works by decreasing swelling and irritation in the airways to allow for easier breathing.
Talk to physician about drinking grapefruit juice while taking this medication.
Headache, stuffy or runny nose, difficulty speaking, sore or irritated throat, painful white patches in the mouth or throat. May cause children to grow more slowly.
Xopenex Used to prevent or relieve the wheezing, shortness of breath, coughing, and chest tightness caused asthma or other pulmonary conditions
N/A Headache, dizziness, nervousness, uncontrollable shaking of a part of the body, heartburn, vomiting, diarrhea, muscle pain
10

11
Z.M. weight-for-age on the 5th%
12
Z.M. stature-for-age below 5th%

References
1. Richards. A., Fincham. G., McNich. A., et.al. (2013). Alternate splicing modifies the effect of mutations in COL11A1 and results in recessive type 2 Stickler syndrome with profound hearing loss. Journal of Medical Genetics 50(11), 765-771. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3812854
2. Evans. K., Sie. K., Hopper. R., et.al. (2011). Robin Sequence: From Diagnosis to Development of an Effective Management Plan. Journal of American Academy of Pediatrics 127(5), 936-948. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3387866/#!po=5.17241
3. Seattle Children’s Hospital. (n.d.). Stickler Syndrome. Retrieved from http://www.seattlechildrens.org/medical-conditions/chromosomal-genetic-conditions/stickler-symptoms
4. Gangopadhyay. N., Mendonca. D., Woo. A. (2012). Pierre Robin Sequence. Seminars in Plastic Surgery 26(2), 76-82. Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3424697
5. Medline Plus. (n.d.). Tracheitis. Retrieved from http://www.nlm.nih.gov/medlineplus/ency/article/000988.htm
6. Mayo Clinic. (n.d.). Stickler Syndrome. Treatment and Drugs. Retrieved from http://www.mayoclinic.org/diseases-conditions/stickler-syndrome/basics/treatment/con-20027976
7. Mahan, K. L., Escott-Stump, S., (2008). Medical Nutrition Therapy for Low-Birth-Weight Infants. In Krause's Food and Nutrition therapy. (12th ed., p 1131). Canada: Saunders Elsevier
8. Medline plus. (n.d.). drugs, supplements, Herbal information, retrieved from http://www.nlm.nih.gov/medlineplus/druginformation.html
13

14





























