Embed Size (px)
Citation preview
Laparoscopic Ventral Hernia Repair
Chan W. Park, MD, FACS
Assistant Professor of Surgery
• Basics
• Bridging
• Defect Closure
• Mesh fixation
• Positioning system

Each hernia is unique…

Approach to the Hernia Patient
• Individualized approach
• Complete History and Physical
• CT Scan – Recurrent hernia
– Atypical location
– Obesity
• Old operative notes whenever possible
• Routine laboratory studies, nutritional panel
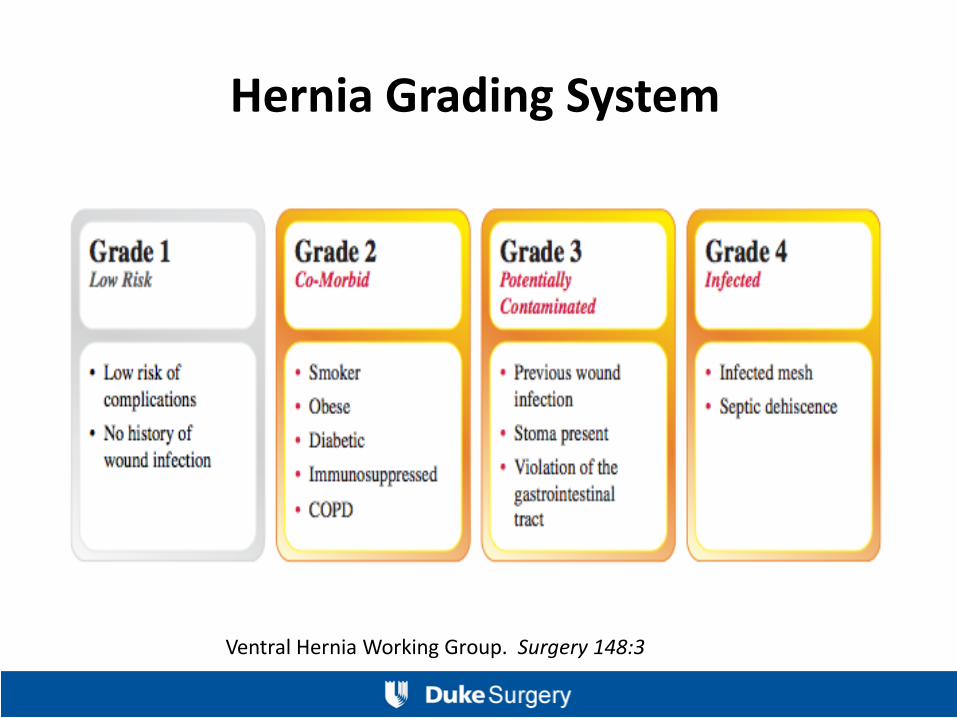
Hernia Grading System
Ventral Hernia Working Group. Surgery 148:3

Risk factors for Hernias
• Obesity • Diabetes Mellitus • Smoking
• COPD • Advanced age • Malnutrition
• Immunosuppression, steroids • Radiation Therapy • Connective tissue Disorders
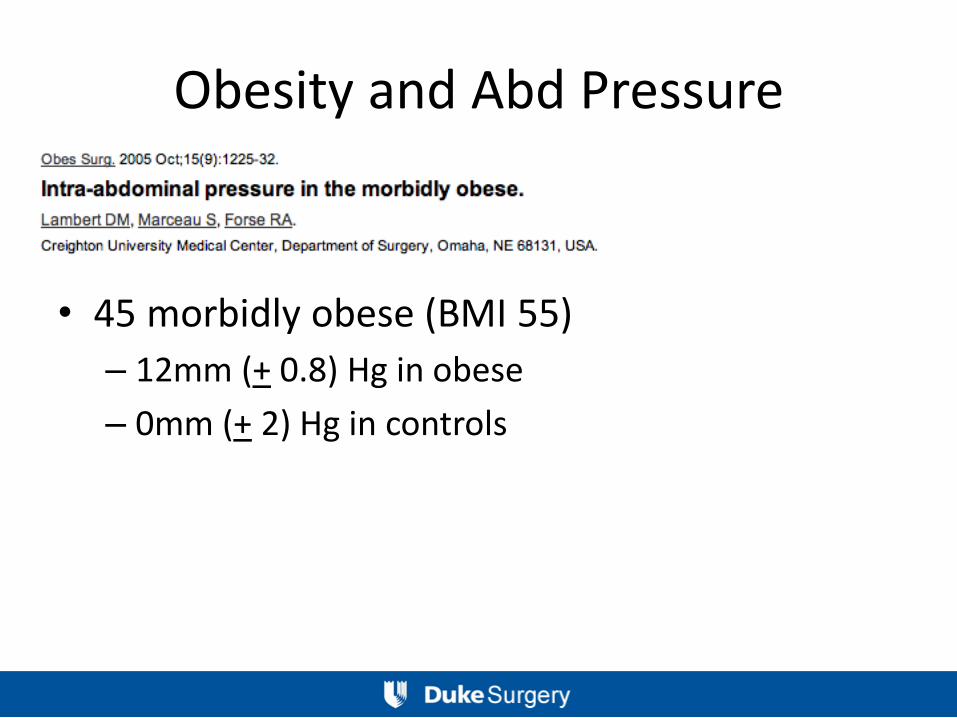
Obesity and Abd Pressure
• 45 morbidly obese (BMI 55)
– 12mm (+ 0.8) Hg in obese
– 0mm (+ 2) Hg in controls
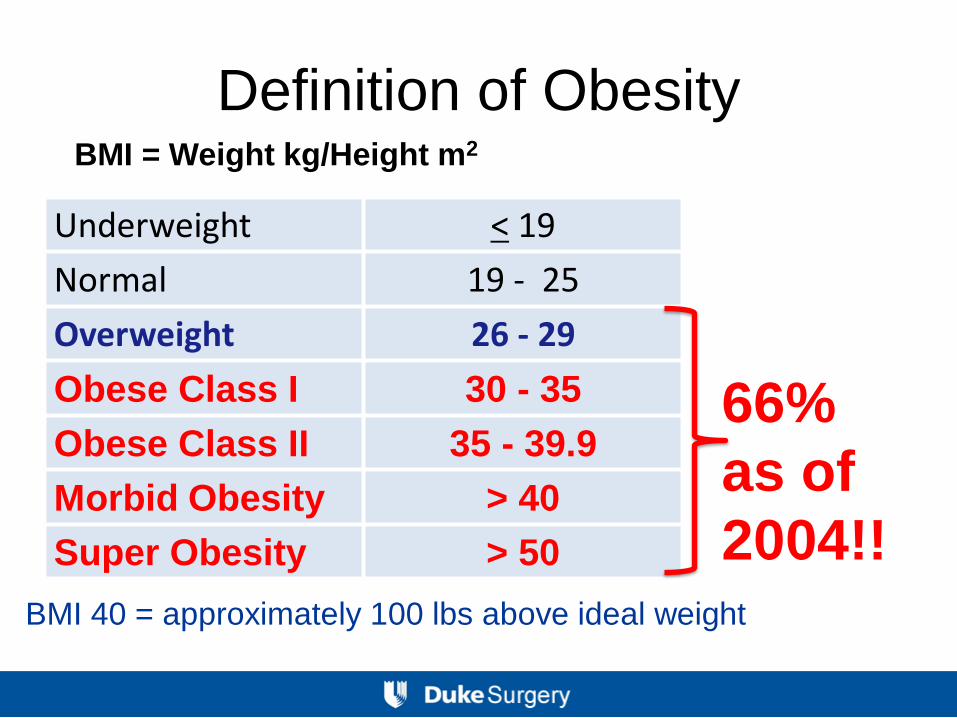
Underweight < 19
Normal 19 - 25
Overweight 26 - 29
Obese Class I 30 - 35
Obese Class II 35 - 39.9
Morbid Obesity > 40
Super Obesity > 50
BMI = Weight kg/Height m2
BMI 40 = approximately 100 lbs above ideal weight
Definition of Obesity
66%
as of
2004!!
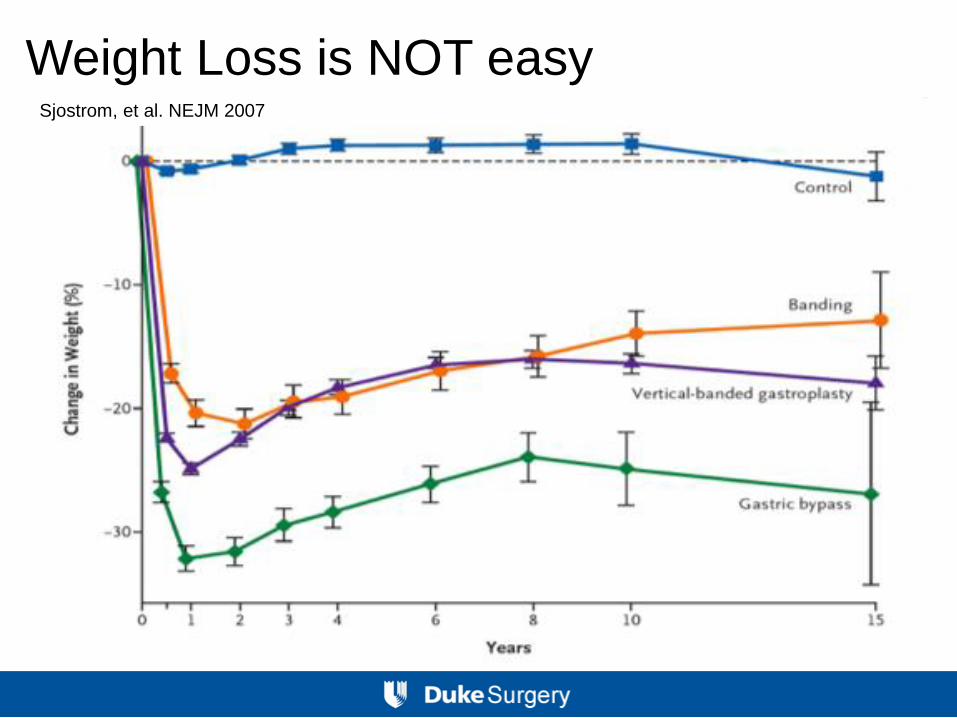
Sjostrom, et al. NEJM 2007
Weight Loss is NOT easy

“Staged” hernia repair


Preoperative Goals: Patient Discussion
• Set realistic expectations:
– Goals of repair
– Timing of repair
– Understanding magnitude of procedure
– Complications
– Recovery
Preoperative Goals
• Weight Loss – Set specific goals
– Bariatric surgery first if necessary
• Smoking cessation (ideally ≥ 4 weeks)
• Heal chronic wounds
• Increase physical activity
• Optimize nutritional status
• Optimize cardiopulmonary status
Surgical Planning
• OPEN vs. Laparoscopic
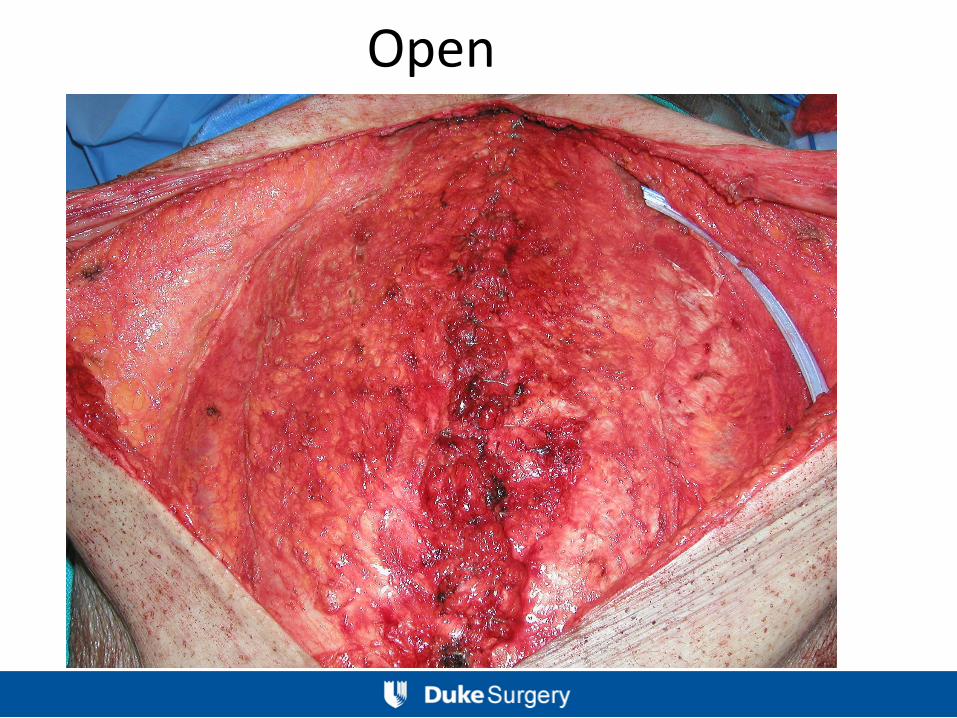
Open
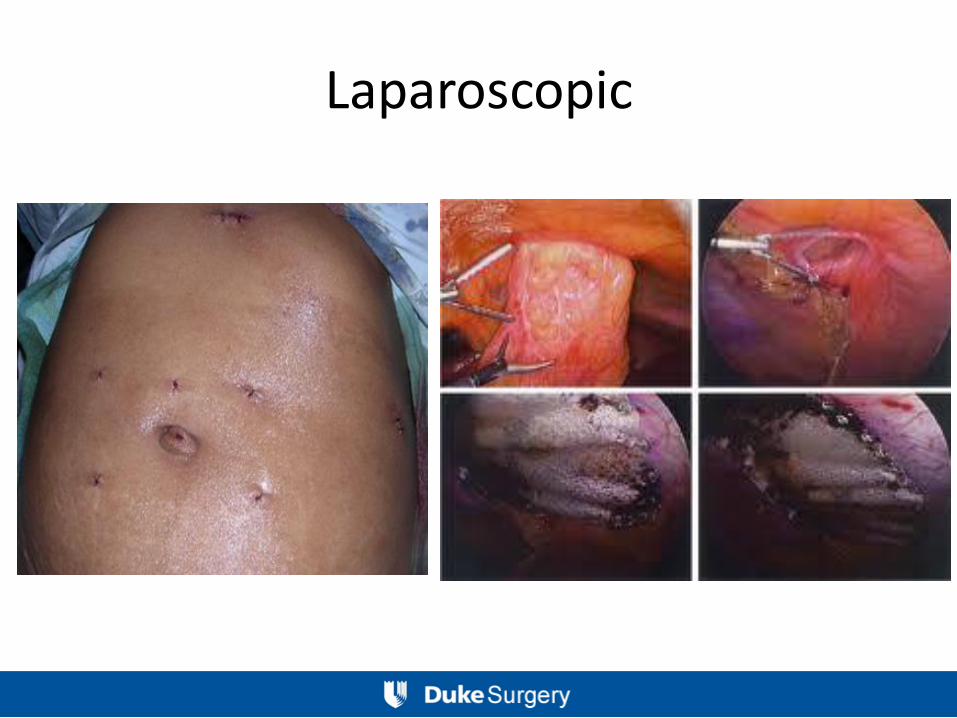
Laparoscopic
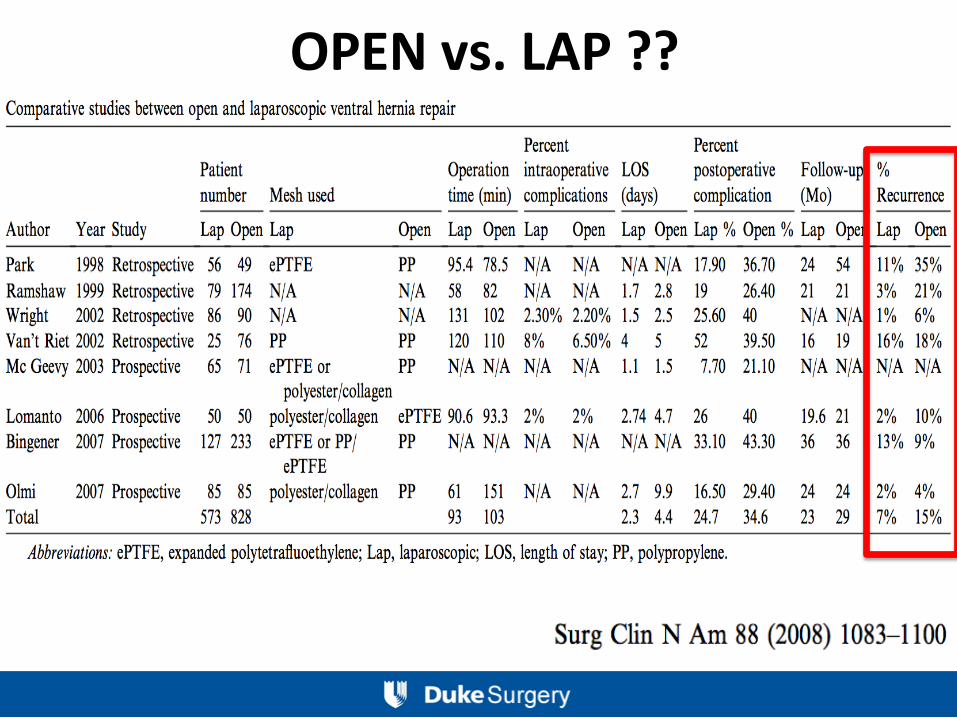
OPEN vs. LAP ??
Surgical Planning
• Mesh or NO Mesh?
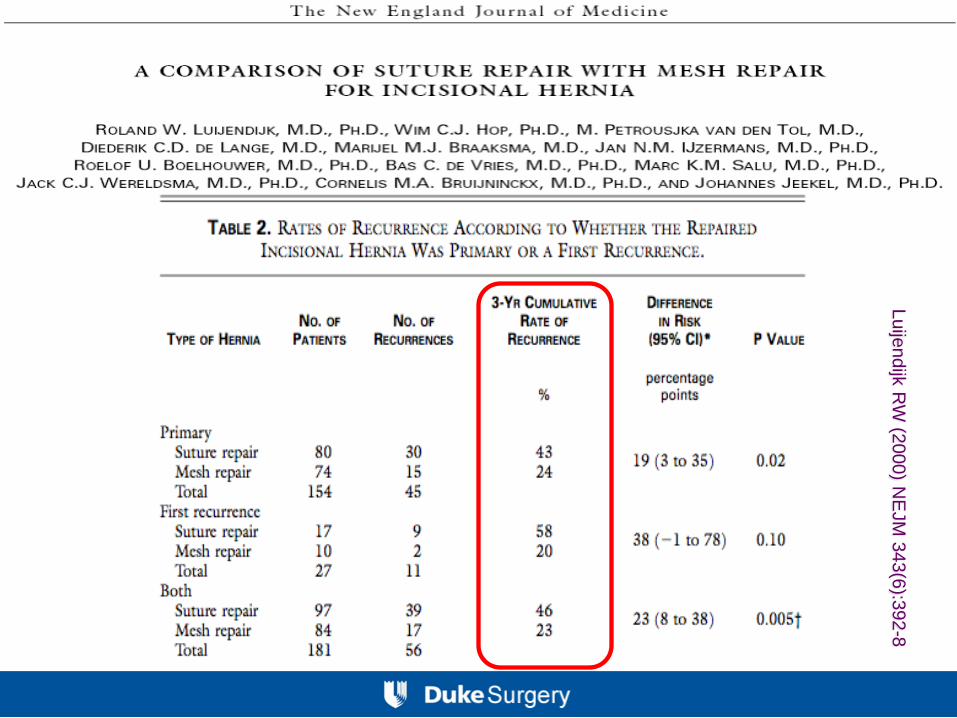
Luije
ndijk
RW
(2000) N
EJM
343(6
):392
-8
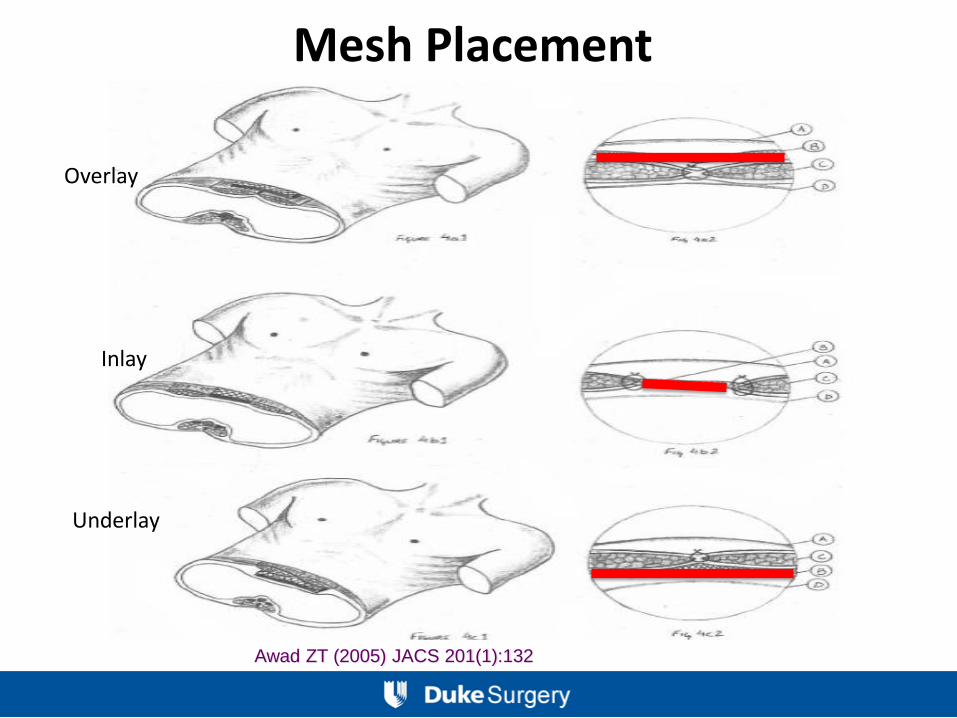
Mesh Placement
Overlay
Inlay
Underlay
Awad ZT (2005) JACS 201(1):132
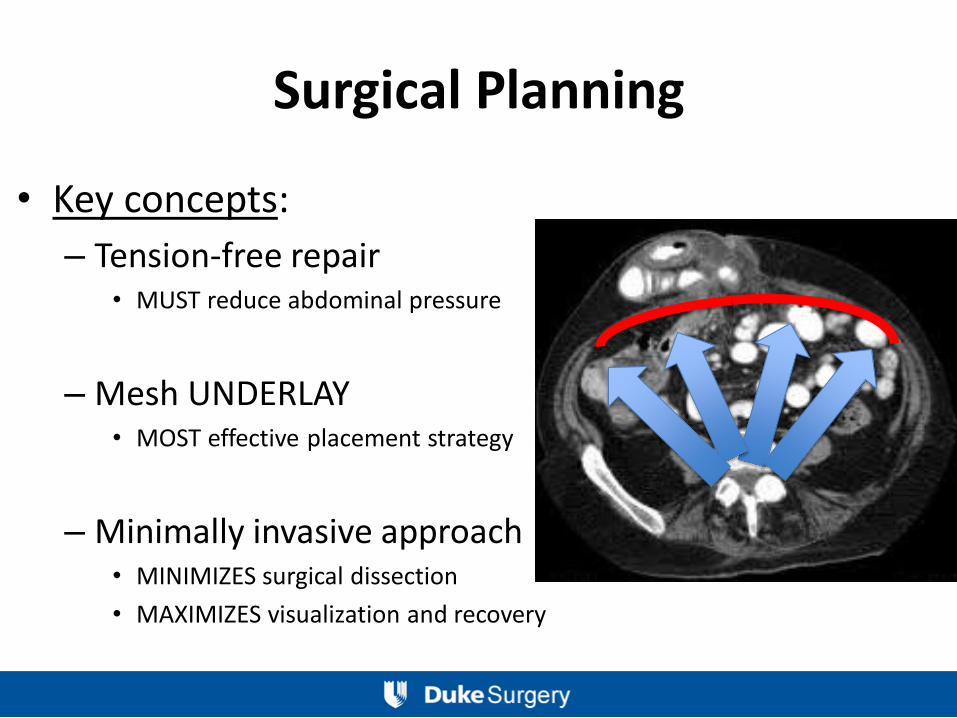
Surgical Planning
• Key concepts:
– Tension-free repair • MUST reduce abdominal pressure
– Mesh UNDERLAY • MOST effective placement strategy
– Minimally invasive approach • MINIMIZES surgical dissection
• MAXIMIZES visualization and recovery
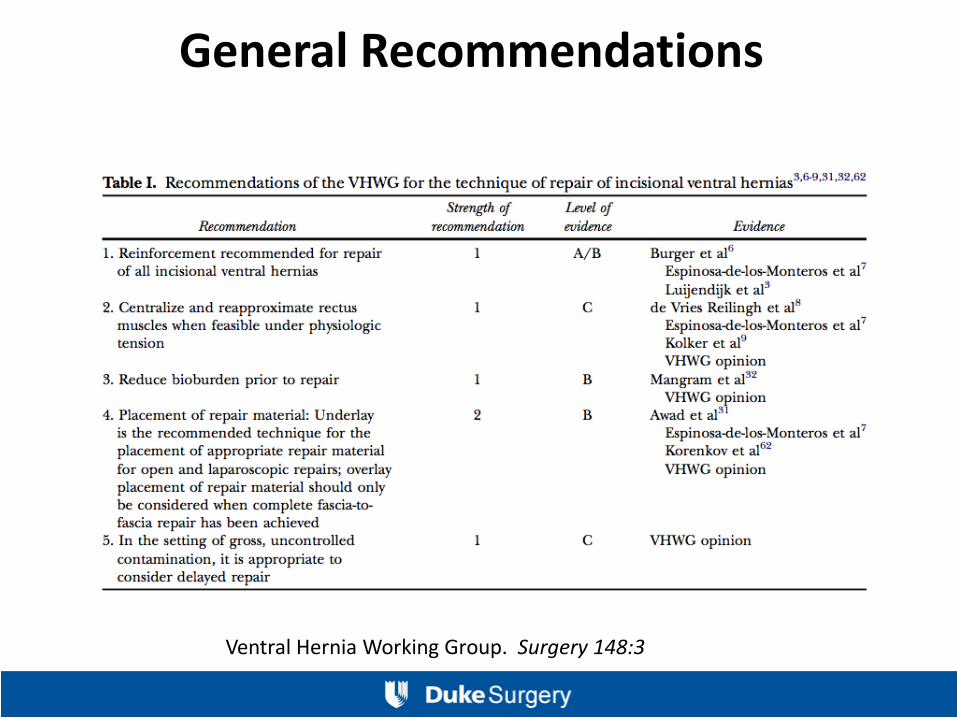
Ventral Hernia Working Group. Surgery 148:3
General Recommendations
Operative Technique • Access
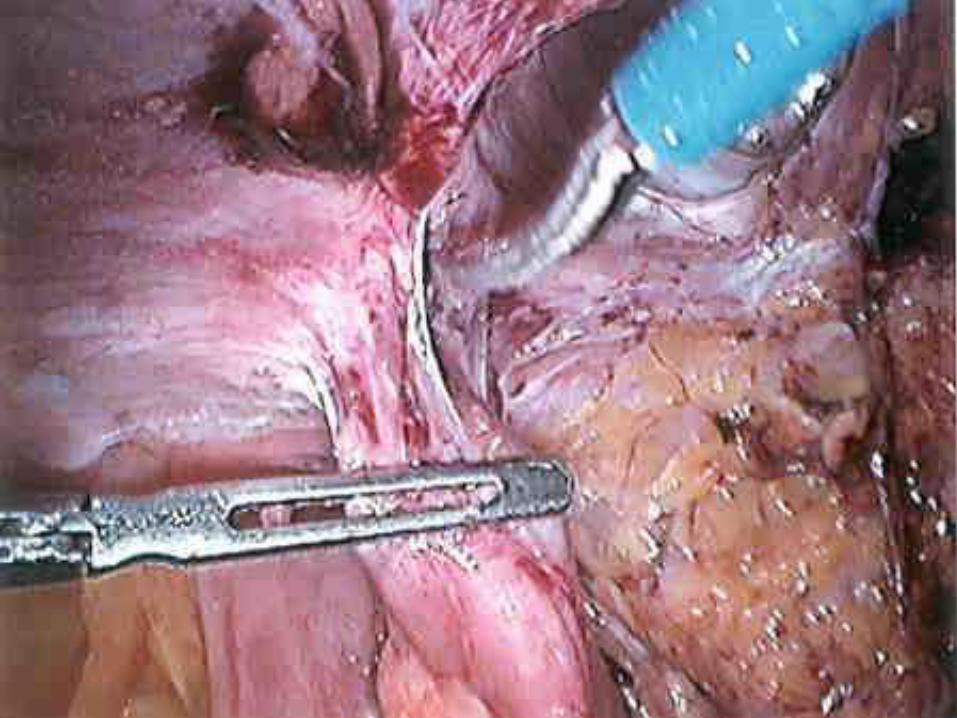
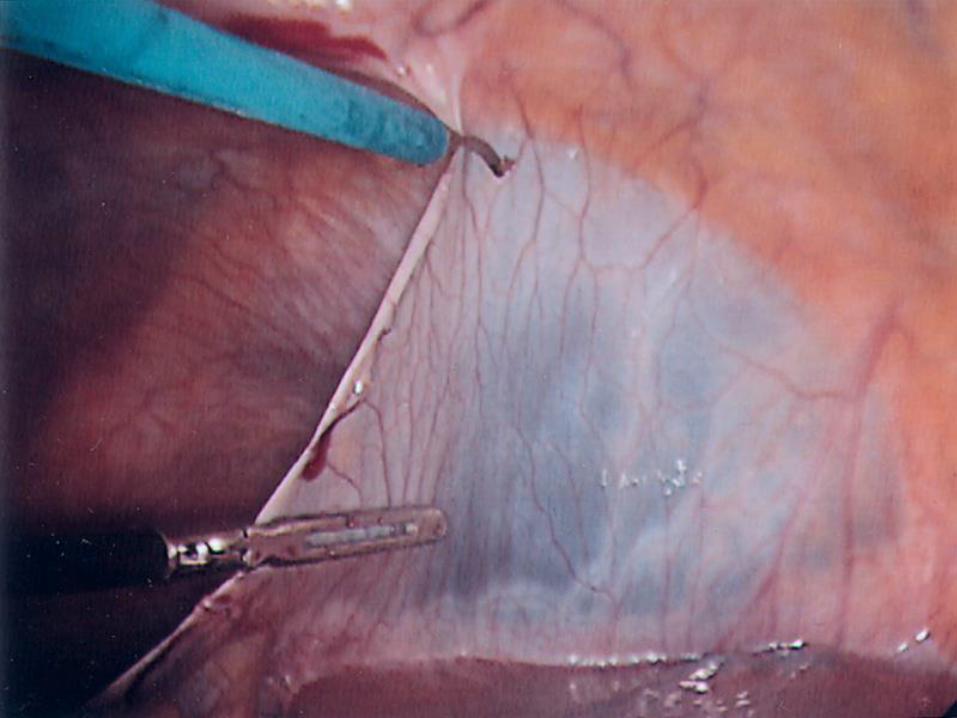
• Adhesiolysis – Sharp dissection
– Energy source only if unavoidable – accept some bleeding
– Direct visualization
• Assess and measure defect – Techniques for doing this?
• Mesh/prosthetic preparation
• Mesh placement – Overlap
– Tacks, sutures, how many sutures?

Access?
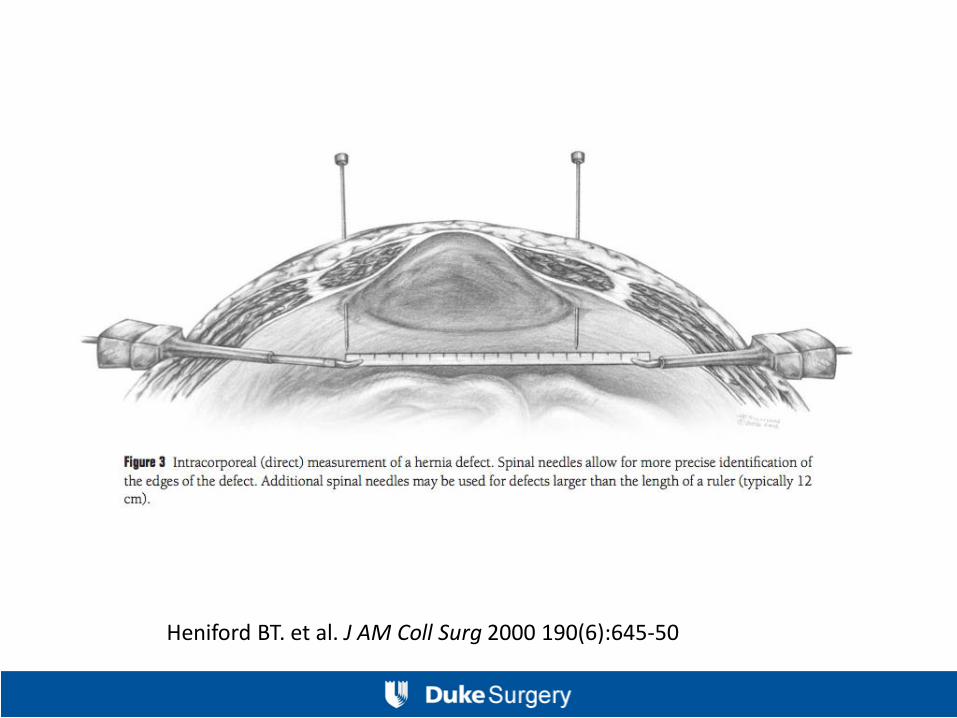
Heniford BT. et al. J AM Coll Surg 2000 190(6):645-50

Heniford BT. et al. J AM Coll Surg 2000 190(6):645-50
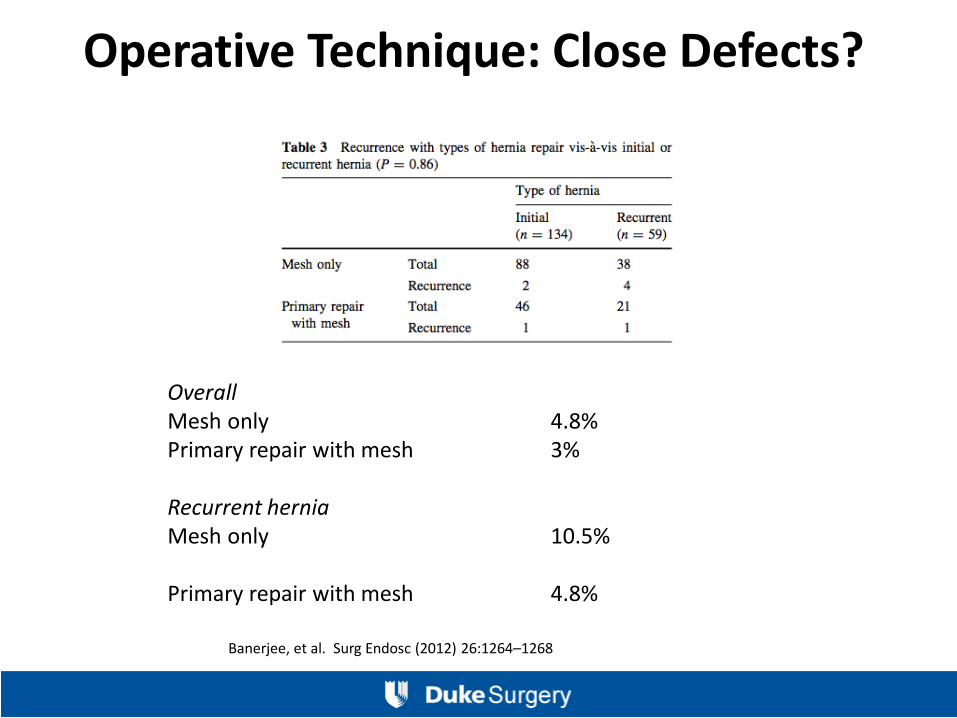
Operative Technique: Close Defects?
Overall Mesh only 4.8% Primary repair with mesh 3% Recurrent hernia Mesh only 10.5% Primary repair with mesh 4.8%
Banerjee, et al. Surg Endosc (2012) 26:1264–1268
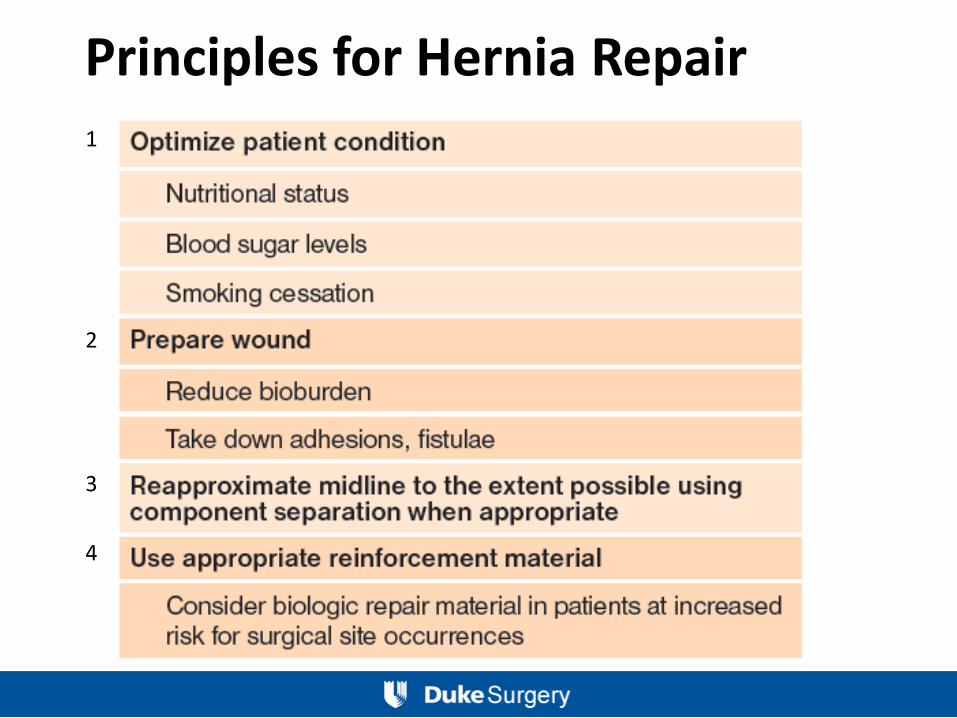
Principles for Hernia Repair 1 2 3
4