Embed Size (px)
Citation preview

Hernia (2007) 11:481–492
DOI 10.1007/s10029-007-0282-8REVIEW
Choice of mesh for laparoscopic ventral hernia repair
J. R. Eriksen · I. Gögenur · J. Rosenberg
Received: 5 March 2007 / Accepted: 17 August 2007 / Published online: 11 September 2007© Springer-Verlag 2007
AbstractBackground Surgical treatment of ventral hernias haschanged dramatically over the past decades by the introduc-tion of laparoscopy and prosthetic biomaterials for rein-forcement of the abdominal wall. There are many meshesavailable on the market for laparoscopic ventral herniarepair (LVHR), and new meshes are introduced regularly.Experimental and clinical documentation for safety andeYcacy are, however, often not available for the clinician.The choice of mesh may therefore be diYcult in clinicalpractice. We present a review of the current literatureregarding safety measures such as adhesions, Wstulas, andinfections as well as the available data on pain, recurrence,mesh shrinkage, and seroma formation after LVHR.Methods The literature was searched systematically usingPubMed/MEDLINE and EMBASE for controlled studies,prospective descriptive series and retrospective case series.Results The literature clearly points in the direction of veryfew mesh-related complications after LVHR. Experimentalstudies and theoretical considerations may argue for using acovered mesh, i.e., a composite mesh, or ePTFE for LVHRin humans, although it is important to stress that there are nohuman data at the moment to support this. Concerns aboutusing pure polypropylene mesh in the intraperitoneal positionmay be re-evaluated with the experience of lightweight mac-ropore meshes from open surgery in mind. There is a ten-dency towards greater shrinkage in ePTFE-based meshes butno diVerences seems to exist between diVerent mesh materi-als in other relevant outcome parameters from clinical series.
Conclusions The literature cannot give general recom-mendations for choice of mesh based on randomized con-trolled trials. The Wnal choice of mesh for LVHR willtherefore typically be based on surgeons’ preference andcost while we await further data from randomized con-trolled clinical trials.
Keywords Ventral hernia · Surgical mesh · Complications · Laparoscopy · Review
Introduction
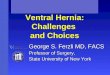
Surgical treatment of ventral hernias has changed dramati-cally over the past decades by the introduction of laparos-copy and prosthetic biomaterials for reinforcement of theabdominal wall. There is increasing evidence and accep-tance that laparoscopic ventral hernia repair (LVHR, seeFig. 1) is superior to open repair in terms of postoperativeinfectious complications, length of stay, recurrence, bloodloss, and cosmetic outcome [1–3]. Insertion of a prostheticmesh for tension-free closure of the hernia defect is stan-dard for laparoscopic repair.
There are many meshes available on the market forLVHR, and new meshes are introduced regularly. A reviewof complication reports on the use of mesh for hernia repairfrom the Food and Drug Administration’s ManufacturerUser Facility Device Experience Database concludes thatspeciWc mesh materials are related to speciWc complications[4]. Experimental and clinical documentation for safety andeYcacy are, however, often not available for the clinician.The choice of mesh may therefore be diYcult in clinicalpractice.
We present a review of the current literature regardingsafety measures such as adhesions, Wstulas, and infections
J. R. Eriksen (&) · I. Gögenur · J. RosenbergDepartment of Surgical Gastroenterology D, Gentofte Hospital, University of Copenhagen, Niels Andersens Vej 65, 2900 Hellerup, Denmarke-mail: [email protected]
123

482 Hernia (2007) 11:481–492
as well as the available data on pain, recurrence, meshshrinkage and seroma formation after LVHR.
Materials and methods
The literature was searched systematically using PubMed/MEDLINE and EMBASE for controlled studies, prospec-tive descriptive series and retrospective case series.Search terms in the databases were ‘laparoscopic ventralhernia repair’ and ‘intraperitoneal mesh’ combined with‘mesh’, ‘pain’, ‘adhesions’, ‘seroma’, ‘recurrence’, ‘Wstulas’,‘infection’ and ‘shrinkage’.
Any additional relevant studies from the reference listsof these papers were also included. Only human and animalstudies published after 1966 in English language wereincluded. Studies with less than 50 patients, letters, editori-als and practice guidelines were excluded.
The ideal mesh
The optimal mesh for LVHR has yet to be found. It shouldfrom a theoretical point of view be non-carcinogenic andchemically inactive, cause no inXammation and change inmesh characteristics after tissue contact, cause no allergicor hypersensitivity reaction, be resistant to physical manip-ulation, and be sterilizable. From the surgeons (andpatients) point of view, the optimal mesh should have cer-tain characteristics such as minimal adhesion formation,excellent tissue ingrowth with minimal shrinkage, no infec-tion or Wstula formation and promote minimal pain and ser-oma formation. Furthermore, it is important that the meshcauses no change in abdominal wall compliance, has a lowprice, and is easy to manipulate.
Products on the market
Currently there are more than 70 meshes for hernia repairavailable on the market. They can be classiWed into diVer-ent categories according to type of material, composition,and pore size [5]. Typically the meshes are made of one ofthree basic prosthetic materials: polypropylene (PP), poly-ester (PE) or expanded polytetraXuoroethylene (ePTFE).
The pure PP meshes Prolene®, Marlex®, Parietene®, etc.,and the pure PE meshes such as Mersilene® are not usuallyrecommended for LVHR. It is generally accepted that purePP or PE meshes should be covered by a protective mem-brane/Wlm against the viscera (degradable or non-degrad-able) to minimize adhesion formation and possible bowelerosion and Wstula formation. These, so-called compositemeshes, and the ePTFE mesh as well, are commonly rec-ommended for intraperitoneal use (see Table 1). Newerbiological meshes have been introduced for intraperitonealapplication, but the clinical experience with these absorb-able meshes is limited.
PTFE meshes
The Wrst ePTFE mesh for intraperitoneal use was the Gore-Tex® soft tissue patch, but in 1993 the MycroMesh® withpores all way through the mesh was introduced to allow bet-ter tissue ingrowth. The two-sided DualMesh® was intro-duced in 1994, and it has afterwards been modiWed withlarge interstices and an irregular “corduroy-like” surface onthe parietal side to increase tissue ingrowth. The DualMesh®
is available with incorporated antimicrobial agents (silver–clorhexidine Wlm, type “Plus”). MotifMESH® is a new mac-roporous non-woven mesh of condensed PTFE (cPTFE) forintraperitoneal application. Although the mesh is macropor-ous (fenestrated) it has a theoretically anti-adhesion barrierbecause of the PTFE content, but unfortunately no clinicaldata are available. The thickness of the MotifMESH® isreduced by 90% compared with older ePTFE meshes.
Composite PE meshes
The Parietex Composite® mesh is composed of multiWla-ment PE with a resorbable collagen-oxidized Wlm made ofoxidized atelocollagen type I, polyethylene glycol and glyc-erol, against the viscera.
Composite PP meshes
TiMesh® is a titanium-coated lightweight (macroporous)PP mesh. Titanium is known for its good biocompatibilityand should theoretically reduce adhesions. It is manufac-tured for intraperitoneal use although it has no “real” solidanti-adhesion barrier or micro-pore/no-pore site against the
Fig. 1 The operative Weld view in laparoscopic ventral hernia repair.The thin-walled translucent hernia sac is clearly visible because of CO2pneumoperitoneum
123

Hernia (2007) 11:481–492 483
bowel loops. Parietene Composite® mesh is a woven PPmesh with a protective collagen-oxidized Wlm on the vis-ceral side. Composix® mesh consists of a Marlex® meshwith a thin layer of ePTFE stitched with polypropylenesutures to the visceral surface. Sepramesh® is a polypropyl-ene mesh coated on the visceral side with an absorbablebarrier of sodium hyaluronate and carboxymethylcellulose.Proceed® mesh is a Prolene® soft mesh encapsulated in apolydioxanone polymer Wlm (PDS®) covered by a layer ofabsorbable oxidised regenerated cellulose (ORC).
Biological meshes
Biological meshes are acellular materials derived fromhumans or animals with an intact extracellular matrix. Theybecome vascularised and thereby have a theoretical abilityto clear infections. Acellular porcine dermal collagen [6]and porcine small intestinal submucosa (Surgisis®) has beenused in LVHR with promising results [7], but the use ofxenogeneic tissue carries a potential risk of immunologicrejection. Allogenic acellular dermal matrix (AlloDerm®)can eliminate this risk [8]. Bovine tunica vaginalis andbovine pericardium (Lyoplant®) represent other biomateri-als tested in animal studies for abdominal wall hernia repair.
Mesh pore size
Prosthetic meshes are divided into macro- and microporemeshes according to their pore size [5]. The pore size
describes the size of fenestrations in the mesh and for Dual-Mesh® it describes the texture pattern. Macropore meshes(>75 �m) gives better tissue ingrowth/host integrationwhereas a mesh with small pore size (<10–75 �m) or nopores carries a risk of encapsulation, thus resulting indecreased integration into the abdominal wall (see below).On the other hand, micropore meshes are traditionallythought of as causing a minimal amount of adhesions, whilea macropore mesh may result in a disorganized neoperitone-alization and therefore potentially cause more adhesions.Thus, not only the prosthetic material used but also the poresize determines the adhesive potential of a mesh.
Based on these experimental data, the logic approach inLVHR is to place a macroporous mesh against the parietalperitoneum and a micropore/“no-pore” side against the vis-cera. In this context, “no-pore” refers to bio-Wlms (collagen,cellulose, etc.) and micropore to for example ePTFE. Thisgoal can be obtained with a composite mesh and in someway by using the DualMesh®. There are no clinical studies,however, to support this theory, but there are multipleexperimental studies available regarding use of intraperito-neal mesh, adhesion formation and degree of host tissueinWltration into the mesh (strength of ingrowth) to supportthe choice of a two-sided mesh.
Strength of ingrowth
The majority of tissue ingrowth and strength take placewithin 2 weeks after mesh insertion and thereafter increases
Table 1 Meshes recommended for intraperitoneal use (not fulWlling)
See “Products on the market” for detailed information about each mesha Distributed in USAb Distributed in Europe
Group Name of mesh Material Company name
PTFE Mycromesh® a,b ePTFE W. L. Gore
Dualmesh® a,b ePTFE W. L. Gore
MotifMESH® a,b cPTFE Proxy Biomedical
Composite Glucamesh® a,b Polypropylene with beta glucan coat Genzyme
Proceed® a,b Polypropylene with ORC layer Ethicon
Sepramesh® a,b Polypropylene with resorbable layerc Genzyme
Parietene Composite® a,b Polypropylene with collagen-coating Sofradim
Intramesh T1® b Polypropylene/ePTFE Cousin Biotech
Dulex® a,b Polypropylene/ePTFE C. R. Bard
Composix® a,b Polypropylene/ePTFE C. R. Bard
Parietex Composite® a,b Polyester with collagen-coating Sofradim
Intramesh W3® b Polyester mesh with silicone layer Cousin Biotech
Dynamesh® a,b Polypropylene/polyvinyliden Xuoride FEG Textiltechnik
TiMesh® a,b Polypropylene with titanium coat GfE Medizintechnik GmbH
C-QUR® a,b Polypropylene with omega 3 fatty acid coat Atrium Medical Corp.
123

484 Hernia (2007) 11:481–492
slowly until 3 months postoperatively [9]. The biologicalresponse to prosthetic materials can be characterized mor-phologically by the formation of collagenous tissue, inXam-mation/foreign body reaction, neoperitonealization andneovascularization. The tissue reaction depends on theinserted prosthetic material and its pore size [10, 11].
Tensiometric tests have been used to determine thestrength of ingrowth at the interface between the mesh andthe abdominal wall/parietal peritoneum. Some investigatorshave used hand-held tensiometers, which may conXict withstandard measurement conditions [12], and others haveused advanced automatic computer-linked Newton meters.All data on this issue are based on experimental animalstudies. Anatomical studies have deWned a required maxi-mum limit of tensile strength of 16 N/cm2 to overcomephysical demands, and this could be a reference to whichfuture studies should be compared [10].
Many experimental studies have shown the superiority ofPP meshes to all other mesh materials regarding strength ofingrowth to the surrounding tissue [13]. DiVerences in hosttissue integration between diVerent PP meshes have beenshown, but they all had higher tensile strength values thanobserved for ePTFE [11]. The ePTFE mesh may from a the-oretical point of view incorporate less into the host tissuethan other materials, because of the no-pore/micropore struc-ture on the parietal side. It has been documented that ePTFEmaterials have a tendency to encapsulate instead of beingintegrated into the host abdominal wall [14]. Sepramesh®
has been compared with ePTFE in two experimental rabbitstudies. After 1 month, Sepramesh® had 30% strongerstrength of incorporation (P = 0.01) [15] but no diVerencecould be found after 5 months [16]. Other studies reportedsigniWcant less strength of mesh integration into the abdomi-nal wall for ePTFE or ePTFE-containing meshes comparedwith other mesh materials [17, 18]. Comparison of ePTFE toAlloDerm® was done in a 9-month follow-up ventral herniapig model [19]. The AlloDerm®–fascial interface had a sig-niWcant higher breaking strength than the ePTFE–fascialinterface (P = 0.04). Another biomaterial, bovine tunicavaginalis, has been shown to have similar long-term tensilestrength characteristics as ePTFE, when tested in a rat model.Only one study reported signiWcantly higher mesh–hostinterface strength of ePTFE compared with polypropylenemesh [12]. The study had certain methodological weak-nesses. The mesh material was secured to the peritonealsurface of the anterior abdominal wall with continuoussutures and tensiometric testing was done by a hand-heldtensiometer as early as on the third postoperative day.
A midline laparotomy through a previously insertedmesh may be required if the patient has to undergo abdomi-nal surgery for other conditions. This procedure may alterthe mesh–host interface integration. PP mesh and ePTFEwere compared in an experimental rabbit study to test this
hypothesis. When the ePTFE mesh was cut through a longi-tudinal incision and repaired with sutures, there was a sig-niWcant loss of tensile strength compared to PP mesh. Scartissue fused the cut edges together in the repaired areas ofthe PP mesh, but the ePTFE mesh was encapsulated with-out fusion [20].
In conclusion, these experimental data suggest thatdiVerent mesh materials diVer in their strength of integra-tion into the host tissue, but the clinical relevance of theseWndings are unclear. A hernia recurrence after LVHR dueto insuYcient mesh integration is hard to conWrm, becausemany other factors may inXuence the recurrence rate (Wxa-tion, suYcient overlap, infection, patient-related factors,etc.).
Adhesions
After intraperitoneal insertion of a prosthetic mesh, adhe-sions between the mesh and the greater omentum and/ororgans may be formed until neoperitonealization of themesh is complete in about 1 week [21]. Other factors thanthe mesh itself, such as Wxation materials, may contribute tothe formation of adhesion after LVHR [22].
The tendency of diVerent mesh materials to form adhe-sions has been investigated in numerous experimental stud-ies, but none of the meshes eliminated adhesion formationcompletely. Adhesions are often measured in terms ofgrade (% of mesh covered by adhesions) and type of adhe-sions (Wlmy, blunt/sharp dissection, solid organ or omentaladhesions). Typically, these experimental studies have beenperformed using small animal models, undersized non-physiologic mesh sizes and diVerent Wxation methods. Itmay be questioned whether the results from such small ani-mal models with low intraabdominal pressure, no herniasand open surgical technique can be extrapolated to the clin-ical situation of LVHR in humans.
Small animals
Several studies have compared PP mesh with ParieteneComposite®, Sepramesh®, DualMesh®, Parietex®, Compo-six® and porcine dermal collagen (Permacol®), and pure PPmeshes were associated with signiWcantly more adhesionsin all studies. Sepramesh® was compared to DualMesh® inthree studies. In the studies by Johnson et al. [16] andYoung et al. [15] there were no diVerence in adhesion for-mation but in the study by Matthews et al. [23] DualMesh®
formed less adhesions. Sepramesh® was found superior toComposix® mesh regarding adhesion formation in a rabbitventral hernia model [11]. Another study by Gonzalez et al.[24] showed Parietex® and Parietene Composite® to pro-duce fewer adhesions than Sepramesh®.
123

Hernia (2007) 11:481–492 485
A recent experimental study in 200 rats compared themajority of meshes available for LVHR [17]. A2.5 £ 3.5 cm pieces of the following meshes were tested:Prolene®, DualMesh®, Ultrapro®, TiMesh®, Sepramesh®,Parietex Composite®, Proceed® and Tutomesh®. Adhesionformation was evaluated on day 7 and 30 post-implanta-tion. Tutomesh®, Sepramesh® and Parietex Composite®
showed the smallest amount of adhesions on day 30.Harrell et al. [25] implanted 4£4 cm pieces of mesh in 30rabbits and adhesion formation was assessed after 1, 4, 8and 16 weeks through a 2 mm laparoscope. DualMesh® hadsigniWcantly less adhesions than Proceed®, Composix® andMarlex® at all times. There were no diVerence in adhesionsbetween Proceed® and Composix® mesh. Another newlypublished adhesion study in rabbits showed signiWcantlylower adhesion degrees with Proceed® and ePTFE meshcompared with Mersilene®, Prolene® and Vypro® mesh,measured 4 weeks post implantation [26].
Large animals
Only a few experimental studies have been performed inlarge animals with proper mesh size and laparoscopic tech-nique. In one study, eight pigs had Prolene®, Parietex® andDualMesh® meshes placed in the intraperitoneal positionand the outcome parameters were measured after 4 weeks.The Parietex® mesh produced the fewest adhesions [18]. Arecent study by DuVy et al. [27] compared Composix® andParietex Composite® mesh in eight pigs after 4 weeks fol-low-up. Through a mini-laparotomy, bowel abrasion wasperformed prior to laparoscopic placement of 10 £ 15 cmmesh pieces. The Parietex® mesh induced a signiWcantlysmaller area of adhesions and less adhesion density than theComposix® mesh. In another recent study comparingTiMesh® and DualMesh® after 3 months follow-up, therewas no diVerence in adhesion formation [28]. Likewise, nodiVerence in adhesion formation between ePTFE and Allo-Derm® was found in a pig study evaluated 3 and 9 monthspost implantation [19].
The largest laparoscopic animal study regarding adhe-sion formation was performed in 21 pigs [29]. DualMesh®,Sepramesh® and Prolene® mesh was tested and Sepra-mesh® had signiWcantly fewer adhesions on day 28 than PPmesh. No signiWcant diVerence between Prolene®/Dual-Mesh® or Sepramesh®/DualMesh® was found.
The hypothesis that the amount of PP material inXuencesthe amount of adhesions formed (because of diVerent localinXammatory response in light- and heavy weight PPmeshes) was tested in a pig study (n = 20) by Zieren et al.[30]. They found no diVerence in adhesion formationbetween lightweight Vypro® mesh (macropore PP) andheavy-weight Prolene® (micropore PP) mesh in the intra-peritoneal position.
Human studies
Few studies concerning intraperitoneal adhesions afterLVHR have been published. In a prospective ventral herniastudy by Balique et al. [31], 29 of 80 patients had a laparo-scopic operation using Parietex® mesh. Adhesion formationwas evaluated 12 months after surgery by ultrasound (US)examination. The validation of the US method was per-formed by comparing a preoperative US examination withthe perioperative Wndings, and showed a negative predic-tive value of 85% and a positive predictive value of 67%.Evaluated by this method, it was shown that 86% of thepatients were adhesion-free after 12 months. Moreno-Egeaet al. [32] used Parietex mesh in 86 consecutive patients.They found that nearly 95% of the patients were adhesion-free 3 years after LVHR. The dynamic ultrasoundtechnique has also been used by others. After laparoscopicventral hernia repair with PP mesh and omental interposi-tion 65% of the patients were adhesion-free after 14 monthsfollow-up and only one patient had visceral adhesions [33].In a case-control study, patients with intraperitoneal Parie-tex® and Mersilene® mesh was compared [34]. Seventy-seven percent of the patients in the Mersilene® groupexhibited visceral adhesions to the mesh compared with18% in the Parietex® group (P < 0.001). In a retrospectiveuncontrolled study, Kohler et al. [35] measured the occur-rence of adhesions to ePTFE mesh at reoperation in patientswho previously had a LVRH. Sixty-Wve patients whereoperated by nine diVerent surgeons in a 10-year follow-upperiod. Ninety-one percent of the patients were describedhaving no or only “Wlmy” intraabdominal adhesions at thereoperation.
A correlation between mesh induced intraabdominaladhesions and ileus or Wstulas after LVHR has not beenshown, although small bowel obstruction after LVHR hasbeen reported in diVerent series [36]. The causes of obstruc-tion were adhesions to Wxation materials (tacks), interposi-tion of small bowel between the abdominal wall and themesh and Wbrinous adhesions to the mesh, among others.
In conclusion, the literature supports a tendency towardsfewer adhesions when using composite meshes or ePTFEfor LVHR. However, the clinical relevance of adhesionsafter LVRH is not known and experimental studies of adhe-sions after LVHR may be a surrogate outcome parameterfor safety. Of more clinical concern is ingrowth into themesh, because it leads to diYcult re-operations if necessaryand potential Wstula formation.
Fistulas
Formation of an enterocutaneous Wstula is a serious compli-cation with a mortality rate up to 10% [37]. Concerns about
123

486 Hernia (2007) 11:481–492
increased risk of Wstula formation when using pure PP andPE mesh in the intraperitoneal position have been evokedby the publication of a few case reports and uncontrolledretrospective series in open ventral hernia repair [37, 38].The often-cited study by Leber et al. [38] was a retrospec-tive study in 200 patients after open incisional hernia repair.Sixty percent of the operations were performed with an on-lay technique and diVerent meshes were used (Marlex®,Prolene® and ePTFE). Five Wstulas were reported afterMersilene® mesh (pure PE) compared with no Wstulas afterthe other meshes (P = 0.02). Colocutaneous Wstula due toPP mesh, Mersilene® and ePTFE [39] has been reported,and Wstula formation has been reported up to 14 years afteropen repair with a Marlex® mesh [40]. Mesh-related Wstula-tion is a late complication and may be a life-long risk afterinsertion of a prosthetic mesh. On the other hand, Vrijlandet al. [41] found no Wstulas after open ventral hernia repairwith Prolene® mesh placed intraperitoneally in 136 patientswith a median follow-up period of 34 months.
The above-mentioned situation in open repairs does notapply for most cases of elective laparoscopic ventral herniarepair. Although, pure PP mesh is not routinely used forLVHR in Europe and the USA, it is still used in other partsof the world. In this context it is interesting that Wstulas hasbeen reported several times after open and laparoscopicinguinal hernia repair with PP mesh and after plug-repairwith PP material in umbilical hernia. Only four cases ofWstulas have been reported after LVHR and none of thesehave been published as speciWc case reports. A colocutane-ous Wstula after ePTFE mesh insertion has been reported byDeMaria et al. [42]. Bageacu et al. [43] reported 2 entero-cutaneous Wstulas in 159 patients reviewed retrospectivelywith a 49 months follow-up period. Both PP and ePTFEmesh were used. Carbajo et al. [44] reported a small-bowelWstula with ePTFE mesh in a large prospective study with a44 months follow-up period. These Wstulas may havedeveloped from tacks or missed/delayed serosal bowel inju-ries and not from the mesh itself.
Large prospective and retrospective studies (n = 736)with pure PP mesh placed in the intraperitoneal positionhave not shown any Wstulas [45–47]. However, the follow-up period in these studies is limited (range 32–47 months)but comparable to other series with diVerent mesh types(see Table 2). The only study that has addressed a correla-tion between a speciWc mesh (Composix® mesh) and Wstulaswas based on 252 voluntarily reports of adverse mesh-related events to the FDA database from 1996 to 2004 [4].Detailed information about patients, type of surgery, poten-tial contamination and total number of operations usingspeciWc meshes was unknown.
It is possible that reports of Wstulas with pure PP and PEmesh (after open repair) represents a positive publicationbias, over-reporting Wstulas, as these meshes have been
used for a much longer time period than other mesh types.The mechanism of Wstula formation after open versus lapa-roscopic ventral hernia repair may also diVer because of theincreased risk of mesh infection in open repair. Neverthe-less, prospective studies regarding Wstula formation with along follow-up period after LVHR are missing. Based onthe sparse literature on mesh-related Wstulas there are nodata to support abandoning PP meshes for intraperitonealuse in LVHR.
Infection
Although many surgeons routinely administer a single pro-phylactic dose of antibiotic preoperatively to reduce infec-tious complications after LVHR, no studies support its use.A meta-analysis from 2006 could not show any eVect ofantibiotic prophylaxis after groin hernia surgery (open andlaparoscopic) and no valid conclusion could be made forLVHR because no high-quality studies were available [68].In general, adherence of bacteria to the mesh is needed toproduce an infection. The greater total surface area in amultiWlament based mesh (for example PE based meshes)will theoretically increase the risk of bacteria adherence asknown from studies comparing multiWlament versus mono-Wlament sutures [69]. However, regarding intraperitonealmesh placement, no diVerence in infection rate after experi-mental contamination of mono- and multiWlament mesheswith Staphylococcus aureus in rats was found [70] butmicropore mesh material has been associated with higherinfection rates, compared with macropore mesh materials[5]. This was explained by the bacteria’s adhesion and pen-etration of the small pores, which cannot be penetrated byleukocytes, thus protecting it from immunological clear-ance.
In a recent experimental study, seven diVerent mesheswere tested for resistance against inoculation withStaphylococcus aureus. After 5 days the rats were sacri-Wced and meshes were investigated. DualMesh Plus®
showed to be least susceptible to bacterial adhesion com-pared with AlloDerm®, DualMesh®, Sepramesh®, Surgisis®,Composix® and Marlex® mesh [71]. The use of antibiotic-impregnated meshes has not been investigated in random-ized human trials and the clinical relevance is unknown.
The incidence of mesh infection varies between 6 and9% after open ventral hernia repair [39, 41]. The ePTFEmesh had a signiWcant higher infection rate than Marlex®
mesh in a controlled retrospective study (n = 37) publishedby Diaz et al. [72] in 2004.
The mesh infection rate after LVHR has been reported tobe from 0 to 3.6% (see Table 2). A large prospective study(n = 850) by Heniford et al. [67] using ePTFE meshreported a mesh infection rate of 0.6% and Franklin et al.
123

Hernia (2007) 11:481–492 487
[46] reported a 0.3% infection rate using mainly PP mesh ina prospective study with 47 months follow-up period.Three randomized trials comparing open and laparoscopicrepair of incisional hernias all showed signiWcantly fewerinfectious complications in the laparoscopic groups [1–3].These Wndings are comparable to many non-randomizedcontrolled series [73]. In the study by Beldi et al. [73] 92consecutive patients had an open ventral hernia repair usingVypro® mesh and 49 consecutive patients had LVHR usinga Parietene Composite® mesh. In the open group 13patients had a surgical site infection compared with one inthe laparoscopic group (P = 0.03).
Mesh placement in potentially contaminated Welds isanother problem that surgeons have to consider in somepatients. In situations of removal of an infected mesh, oper-ation for strangulated hernia or LVHR plus another simul-
taneously performed procedure, insertion of a mesh is notgenerally recommended because of the risk of infectiouscomplications. Biological meshes are absorbable and with-out permanent foreign body material and may be an alterna-tive in these situations. Franklin et al. [7] published a seriesof 58 laparoscopic hernia repairs (mostly ventral hernias)using Surgisis® with a 19 months median follow-up period.Fifty-six percent of the procedures were performed inpotentially or grossly contaminated Welds and there were noreported mesh-related complications. AlloDerm® has alsobeen used successfully in the closure of contaminatedabdominal hernias [8] and Cobb et al. [6] published a seriesof 55 LVHRs using cross-linked acellular porcine dermalcollagen matrix (CPDC). This group was compared to ahistorical group with PP/ePTFE composite mesh. No infec-tious complications were observed in the CPDC-group but
Table 2 Published series of laparoscopic ventral hernia repair with 50 or more patients
LOS length of stay in hospital, PPM polypropylene mesh, ePTFE expanded polytetraXuoroethylenea Predominant mesh usedb Requiring mesh removalc Not speciWed
No. of patients
References Follow-up (months)
Mesh materiala
Pain (%)
Recurrence (%)
Seroma (%)
LOS (days)
Infection (%)b
50 Lomanto [48] 19 Parietex –c 2 10 2 0
53 Kyzer [36] 12 ePTFE –c 1.8 –c 3.3 1.9
56 Park [49] 24 ePTFE 3.6 10.7 3.6 3.4 3.6
79 Eid [50] 34 ePTFE 3.8 5 3.8 1.7 0
85 Sanchez [51] 18 ePTFE –c 3.5 9 4 –c
86 Moreno-Egea [32] 42 Parietex –c 3.5 5.8 –c –c
86 Aura [52] 37 ePTFE 5.9 7 14.1 4.8 0
96 Rosen [53] 30 ePTFE –c 17 4 1.8 2.1
97 Ujiki [54] 3 ePTFE –c 6 13 2 –c
100 Bower [55] 6.5 ePTFE 3 2 1 –c 2
100 Ben-Heim [56] 19 ePTFE –c 2 11 5 –c
103 Kirshtein [57] 26 ePTFE –c 3.9 –c 3 1.9
140 Morales-Conde [58] 40 ePTFE –c 2.1 2.1 –c –c
144 Toy [59] 7 ePTFE –c 4 16 2 1.4
146 Topart [60] 27 ePTFE 20.7 5.8 8 4.9 0.7
150 Yavuz [45] 32 PPM 1.3 3 3 2.5 –c
150 Berger [61] 15 ePTFE –c 2.7 93 9 0
159 Bageacu [43] 49 PPM, ePTFE 26 15.7 15.9 3.5 0
170 McKinlay [62] 25 ePTFE 1.2 5.9 3.5 2.2 1.8
178 Olmi [63] 29 Parietex 1.9 2.5 4.4 2.1 0.6
200 LeBlanc [64] 36 ePTFE 4.5 4 7.5 1.25 1.5
202 Cowbey [47] 35 PPM –c 1 18–32 1.8 –c
208 Frantzides [65] 24 PPM/ePTFE. ePTFE –c 1.4 –c 1.4 0
270 Carbajo [44] 44 ePTFE 7.4 4.4 11.8 1.5 0
277 Cobb [66] 21 ePTFE 3.2 4.7 0.7 3 0.7
384 Franklin [46] 47 PPM 2 2.9 3 2.9 0.3
850 Heniford [67] 20 ePTFE 1.6 4.7 2.6 2.3 0.6
123

488 Hernia (2007) 11:481–492
in the control group three meshes had to be removed due toinfection.
It seems obvious that open ventral hernia repair carries asubstantial risk of infection and subsequent removal of themesh compared with the laparoscopic technique. The pro-tective mechanism of the peritoneal cavity against infectionmay be of major importance and could explain the lowerinfection rate observed in LVHR. No randomized clinicalstudy comparing diVerent mesh materials and their suscep-tibility to infection in LVHR has been published.
Postoperative pain
No studies have focused speciWcally on pain after LVHR.Postoperative pain has been described in many descriptivestudies with incidences up to 26% (see Table 2). Often,clear deWnitions of pain, pain location, method and time ofpain measurement and prescribed postoperative medicationwere not described. Studies with detailed measurement ofpostoperative pain and convalescence after LVHR are obvi-ously needed. An indirect measure of postoperative paincould be the length of stay in hospital which varies between1 and 9 days in the published series (Table 2). Someauthors have described successfully planned outpatientLVHR with low readmission rates.
Whether the mesh itself contributes to pain after LVHRas a result of local inXammation and the body’s reaction tothe foreign material is unclear, but there is no evidence thatone type of mesh causes more pain than others. The impactof polypropylene amount in the mesh on postoperativepain/discomfort has been investigated for open incisionalhernia repair and Lichtenstein hernia repair. In these proce-dures there was a tendency towards less chronic pain whenlightweight meshes were used. LeBlanc et al. [74] reportedtwo cases with persistent pain after intraperitoneal Compo-six® mesh placement. Both meshes were removed andreplaced with ePTFE meshes. The patients recovereduneventfully without pain. Mechanical Wxation devicesmay also cause postoperative pain, but again, no compara-tive study between diVerent Wxation techniques has beenconducted in LVHR. Transfascial sutures for additionalmesh Wxation are used by several surgeons and have beenfound as a likely explanation for prolonged pain (>6–8 weeks)after LVHR in some patients. This problem has been solvedby local anaesthetic injections or even laparoscopicremoval of suture material [73]. Mesh contraction/shrink-age resulting in tension on the abdominal wall could beanother cause of chronic pain, but this hypothesis has notbeen investigated. Thus, pain after LVHR may be consider-able and has to be included in patient information and plan-ning of the perioperative regimen for this patient category.Future studies should in detail describe pain patterns after
LVHR in order to rationalize further controlled interven-tional studies to improve outcome after LVHR.
Recurrence
Numerous uncontrolled personal series of LVHR have beenpublished. The recurrence rates vary between 1 and 17%with a mean rate of 4.5% (208 recurrences in 4,574LVHRs, see Table 2). Many of the studies have been pub-lished by enthusiastic surgeons within the Weld of LVHRand it may therefore be diYcult to extrapolate these resultsto daily clinical practice. There are no obvious link betweenthe reported recurrence rates and the mesh material used.
No experimental animal studies or human studies com-paring diVerent mesh materials regarding recurrence havebeen published. Such studies are indeed diYcult to performbecause the cause of hernia recurrence after LVHR may bemulti-factorial. Patient’s co-morbidity, hernia size, woundinfection, steroid use, previous hernia repair, surgical tech-nique and improper mesh Wxation with insuYcient meshoverlap (minimum 3 cm) at the fascial margin of the herniamay be factors of importance. The only study published isan experimental rat study comparing ePTFE and PP meshin open repair [75]. The authors found signiWcantly higherrecurrence rate when ePTFE was used after 8 weeks. Byhistological examinations the authors were able to concludethat insuYcient ingrowth of Wbrocollagenous tissue into theePTFE mesh caused the reherniations.
In conclusion, no obvious diVerence in recurrence rateexists between diVerent mesh materials, but no randomizedtrials have been conducted so far. Since the mesh materialseems to be of minor importance in terms of hernia recur-rence after LVHR, studies should be conducted to testwhether transfascial sutures reduce the recurrence rate.
Seroma
In LVHR a mesh is placed to cover the hernia defect. Thehernia sac is left untouched and thereby Xuids can collect inthe subcutaneous dead space/hernia sac resulting in a ser-oma. Host inXammatory reaction to the implanted materialand haematoma may contribute to the formation of a ser-oma. Micropore meshes may have a higher tendency toform seromas than macropore materials, because passivedrainage of the Xuid to the peritoneal cavity through themesh is diminished, but no study conWrms this theory.
The incidence of seroma formation after LVHR isextremely varying and is reported to be between 0.7 and93% (see Table 2). Such varying incidence is primarily dueto heterogeneous deWnitions and methods of measuringseromas and the time of measurement after the operation.
123

Hernia (2007) 11:481–492 489
No randomized or prospective controlled trials have beenconducted comparing diVerent mesh materials and theirsusceptibility to form seromas. Thus, there is no evidencethat certain mesh types result in higher seroma rates thanothers.
When ultrasound examination is used to detect seromas,Susmallian et al. [76] showed that all patients undergoingLVHR with ePTFE mesh developed a seroma in the Wrstpostoperative week. Symptomatic seroma causing abdomi-nal discomfort and pain was detected by clinical examina-tion in 35% of the patients and 20% of the patients hadpersistent seromas after 3 months. In another prospectivestudy seromas were measured by computer tomographyscan (CT scan). One-week postoperatively 95% of thepatients had a seroma and all seromas disappeared within3 months after LVHR [77]. Tsimoyiannis et al. [78]showed in a randomized trial in 51 patients undergoingLVHR with ePTFE mesh that intraoperative electro-coagu-lation at the hernia sac reduced seroma formation from 25to 4%, detected by clinical examination and CT scan.
In the largest series by Heniford et al. [67] 2.6% of thepatients had prolonged seromas. Therefore, seroma forma-tion still remains an important clinical problem in a fewpatients after LVHR and randomized clinical trials, testingdiVerent prophylactic procedures should be performed.
Shrinkage
The tendency of prosthetic materials to shrink/contract overtime has been studied in several animal studies. The phe-nomenon is a well-known clinical observation at reopera-tion in patients with formerly inserted mesh. Though, someauthors have questioned if all materials shrink whenimplanted in the human body and some may even expand,as shown by structural alterations in the size of the meshpores when aVected by diVerent (body) Xuids [79].
Three small animal studies with small mesh sizes (2.5–4 cm in diameter) showed signiWcantly greater shrinkage ofePTFE mesh compared with other mesh types (Proceed®,Marlex® and Composix® [25], Proceed®, Prolene®, Ultr-apro®, TiMesh®, Sepramesh® and Parietex® [17] andSepramesh® [16]). Two laparoscopic studies with intraperi-toneal insertion of more clinical relevant mesh sizes(10 £ 15 cm) have been conducted in pigs, and the resultswere similar. The ePTFE mesh shrank 37% compared withParietex® (21%) and PP mesh (6%) (P < 0.001) after1 month [18], and 44% after 3 months compared withTiMesh® (18%) (P < 0.006) [28]. A 5-months follow-upstudy in rabbits showed 51% shrinkage of ePTFE mesh[16]. In another experimental study with PP materialstested for shrinkage in the extraperitoneal position, shrink-age was measured to 33–46% [80, 81] compared with 13%
for PE mesh, P < 0.006 [80]. One retrospective humanstudy evaluating mesh shrinkage at open re-operation afterprimary open ventral hernia repair in 77 patients has beenpublished [82]. Fifty-eight percent of micropore PP mesh,5% of macropore PP mesh and 57% of ePTFE meshes werenoted to be “heavily shrunken” at the time of reoperation.
To conclude, most mesh materials undergo some degreeof shrinkage after implantation in living tissue. Meshshrinkage has been related to hernia recurrence and thedegree of shrinkage varies between diVerent mesh materialswith a tendency towards most shrinkage occurring afterePTFE implantation. The causal factors behind meshshrinkage are not fully known, but contraction as a conse-quence of the physiological wound healing process, poresize and weight of the mesh (total mesh material) may playa role [81]. The shrinkage of speciWc mesh materials mayhave implications for the overlap needed to adequatelyrepair a ventral hernia.
Future
Through the years, great eVort has been put into the chal-lenge of creating a mesh that completely fulWls the crite-ria’s for “the ideal mesh”. Biologic mesh materials havebeen introduced and the preliminary results are encourag-ing. These acellular materials have an intact extracellularmatrix that facilitates the ingrowth of connective tissue thusimproving the strength of mesh integration. Furthermorethey become vascularised and thereby have the theoreticalability to clear bacteria growth/infections. Unfortunately,biologic meshes are quite expensive at the moment. In thefuture, bioactive meshes with local drug release such asgrowth factors may be introduced to further optimize meshintegration.
Conclusions
The literature clearly points in the direction of very fewmesh related complications in LVHR. There have beenreports of major complications such as Wstulas and meshinfections, but the incidence of these complications seemsrelatively low compared to open repair, regardless of thetype of mesh used.
Experimental studies and theoretical considerations mayargue for using a covered mesh, i.e., a composite mesh, orePTFE for LVHR in humans, although it is important tostress that there are no human data at the moment to supportthis. Concerns about using PP mesh in the intraperitonealposition may be re-evaluated with the experience of light-weight macropore meshes from open surgery in mind. Thismesh has resulted in less pain, induces less inXammation
123

490 Hernia (2007) 11:481–492
because of less implanted mesh material and thereby poten-tially forms fewer adhesions.
Thus, the literature can not give general recommenda-tions for choice of mesh based on randomized controlledtrials and no diVerence seems to exist in relevant outcomeparameters from clinical series between diVerent meshmaterials. The Wnal choice of mesh for LVHR will there-fore typically be based on surgeons’ preference and costwhile we await further data from randomized controlledclinical trials.
References
1. Carbajo MA, Martin del Olmo JC, Blanco JI, de la Cuesta C,Toledano M, Martin F, Vaquero C, Inglada L (1999) Laparoscopictreatment vs open surgery in the solution of major incisional andabdominal wall hernias with mesh. Surg Endosc 13:250–252
2. Misra MC, Bansal VK, Kulkarni MP, Pawar DK (2006) Compar-ison of laparoscopic and open repair of incisional and primary ven-tral hernia: results of a prospective randomized study. Surg Endosc(Epub ahead of print)
3. Barbaros U, Asoglu O, Seven R, Erbil Y, Dinccag A, Deveci U,Ozarmagan S, Mercan S (2006) The comparison of laparoscopicand open ventral hernia repairs: a prospective randomized study.Hernia (Epub ahead of print)
4. Robinson TN, Clarke JH, Schoen J, Walsh MD (2005) Majormesh-related complications following hernia repair: events report-ed to the Food and Drug Administration. Surg Endosc 19:1556–1560
5. Amid PK (1997) ClassiWcation of biomaterials and their relatedcomplications in abdominal wall hernia surgery. Hernia 1:15–21
6. Cobb GA, ShaVer J (2005) Cross-linked acellular porcine dermalcollagen implant in laparoscopic ventral hernia repair: case-con-trolled study of operative variables and early complications. IntSurg 90:S24–S29
7. Franklin ME Jr, Gonzalez JJ Jr, Glass JL (2004) Use of porcinesmall intestinal submucosa as a prosthetic device for laparoscopicrepair of hernias in contaminated Welds: 2-year follow-up. Hernia8:186–189
8. Butler CE, Langstein HN, Kronowitz SJ (2005) Pelvic, abdominal,and chest wall reconstruction with AlloDerm in patients at in-creased risk for mesh-related complications. Plast Reconstr Surg116:1263–1275
9. Majercik S, Tsikitis V, Iannitti DA (2006) Strength of tissueattachment to mesh after ventral hernia repair with synthetic com-posite mesh in a porcine model. Surg Endosc 20:1671–1674
10. Klinge U, Klosterhalfen B, Birkenhauer V, Junge K, Conze J,Schumpelick V (2002) Impact of polymer pore size on the inter-face scar formation in a rat model. J Surg Res 103:208–214
11. Greenawalt KE, Butler TJ, Rowe EA, Finneral AC, Garlick DS,Burns JW (2000) Evaluation of sepramesh biosurgical compositein a rabbit hernia repair model. J Surg Res 94:92–98
12. LeBlanc KA, Bellanger D, Rhynes KV 5th, Baker DG, Stout RW(2002) Tissue attachment strength of prosthetic meshes used inventral and incisional hernia repair. A study in the New ZealandWhite rabbit adhesion model. Surg Endosc 16:1542–1546
13. Bellon JM, Bujan J, Contreras LA, Carrera-San Martin A, JuradoF (1996) Comparison of a new type of polytetraXuoroethylenepatch (Mycro Mesh) and polypropylene prosthesis (Marlex) for re-pair of abdominal wall defects. J Am Coll Surg 183:11–18
14. Bujan J, Contreras LA, Carrera-San Martin A, Bellon JM (1997)The behavior of diVerent types of polytetraXuoroethylene (PTFE)
prostheses in the reparative scarring process of abdominal wall de-fects. Histol Histopathol 12:683–690
15. Young RM, Gustafson R, Dinsmore RC (2004) Sepramesh vs. Du-almesh for abdominal wall hernia repairs in a rabbit model. CurrSurg 61:77–79
16. Johnson EK, Hoyt CH, Dinsmore RC (2004) Abdominal wall her-nia repair: a long-term comparison of Sepramesh and Dualmesh ina rabbit hernia model. Am Surg 70:657–661
17. Burger JW, Halm JA, Wijsmuller AR, ten Raa S, Jeekel J (2006)Evaluation of new prosthetic meshes for ventral hernia repair.Surg Endosc 20:1320–1325
18. McGinty JJ, Hogle NJ, McCarthy H, Fowler DL (2005) A compar-ative study of adhesion formation and abdominal wall ingrowth af-ter laparoscopic ventral hernia repair in a porcine model usingmultiple types of mesh. Surg Endosc 19:786–790
19. Silverman RP, Li EN, Holton LH III, Sawan KT, Goldberg NH(2004) Ventral hernia repair using allogenic acellular dermal ma-trix in a swine model. Hernia 8:336–342
20. Bellon JM, Contreras LA, Bujan J, Pascual G, Carrera-San MartinA (1999) EVect of relaparotomy through previously integratedpolypropylene and polytetraXuoroethylene experimental implantsin the abdominal wall. J Am Coll Surg 188:466–472
21. Matthews BD, Pratt BL, Backus CL, Kercher KW, Heniford BT(2002) Comparison of adhesion formation to intra-abdominalmesh after laparoscopic adhesiolysis in the New Zealand Whiterabbit. Am Surg 68:936–940
22. Memisoglu K, Saribeyoglu K, Pekmezci S, Karahasanoglu T, SenB, Bayrak I, Arbak S, Sirvanci S (2006) Mesh Wxation devices andformation of intraperitoneal adhesions. J Laparoendosc Adv SurgTech A 16:439–444
23. Matthews BD, Mostafa G, Carbonell AM, Joels CS, Kercher KW,Austin C, Norton HJ, Heniford BT (2005) Evaluation of adhesionformation and host tissue response to intra-abdominal polytetraXu-oroethylene mesh and composite prosthetic mesh. J Surg Res123:227–234
24. Gonzalez R, Rodeheaver GT, Moody DL, Foresman PA, Ram-shaw BJ (2004) Resistance to adhesion formation: a comparativestudy of treated and untreated mesh products placed in the abdom-inal cavity. Hernia 8:213–219
25. Harrell AG, Novitsky YW, Peindl RD, Cobb WS, Austin CE,Cristiano JA, Norton JH, Kercher KW, Heniford BT (2006)Prospective evaluation of adhesion formation and shrinkage ofintra-abdominal prosthetics in a rabbit model. Am Surg 72:808–813
26. Kiudelis M, Jonciauskiene J, Deduchovas O, Radziunas A,Mickevicius A, Janciauskas D, Petrovas S, Endzinas Z, PundziusJ (2006) EVects of diVerent kinds of meshes on postoperativeadhesion formation in the New Zealand White rabbit. Hernia(Epub ahead of print)
27. DuVy AJ, Hogle NJ, LaPerle KM, Fowler DL (2004) Comparisonof two composite meshes using two Wxation devices in a porcinelaparoscopic ventral hernia repair model. Hernia 8:358–364
28. Schug-Pass C, Tamme C, Tannapfel A, Kockerling F (2006) Alightweight polypropylene mesh (TiMesh) for laparoscopic intra-peritoneal repair of abdominal wall hernias: comparison of bio-compatibility with the DualMesh in an experimental study usingthe porcine model. Surg Endosc 20:402–409
29. Borrazzo EC, Belmont MF, BoVa D, Fowler DL (2004) EVect ofprosthetic material on adhesion formation after laparoscopic ven-tral hernia repair in a porcine model. Hernia 8:108–112
30. Zieren J, Neuss H, Ablassmaier B, Muller JM (2002) Adhesionsafter intraperitoneal mesh repair in pigs: Prolene “vs. Vypro”. JLaparoendosc Adv Surg Tech A 12:249–252
31. Balique JG, Benchetrit S, Bouillot JL, Flament JB, Gouillat C,Jarsaillon P, Lepere M, Mantion G, Arnaud JP, Magne E, BrunettiF (2005) Intraperitoneal treatment of incisional and umbilical
123

Hernia (2007) 11:481–492 491
hernias using an innovative composite mesh: four-year results of aprospective multicenter clinical trial. Hernia 9:68–74
32. Moreno-Egea A, Torralba JA, Girela E, Corral M, Bento M, Carta-gena J, Vicente JP, Aguayo JL, Canteras M (2004) Immediate, ear-ly, and late morbidity with laparoscopic ventral hernia repair andtolerance to composite mesh. Surg Laparosc Endosc PercutanTech 14:130–5
33. Bingener J, Kazantsev GB, Chopra S, Schwesinger WH (2004)Adhesion formation after laparoscopic ventral incisional hernia re-pair with polypropylene mesh: a study using abdominal ultra-sound. JSLS 8:127–131
34. Arnaud JP, Hennekinne-Mucci S, Pessaux P, Tuech JJ, Aube C(2003) Ultrasound detection of visceral adhesion after intraperito-neal ventral hernia treatment: a comparative study of protectedversus unprotected meshes. Hernia 7:85–88
35. Koehler RH, Begos D, Berger D, Carey S, LeBlanc K, Park A,Ramshaw B, Smoot R, Voeller G (2003) Minimal adhesions toePTFE mesh after laparoscopic ventral incisional hernia repair: re-operative Wndings in 65 cases. JSLS 7:335–340
36. Kyzer S, Alis M, Aloni Y, Charuzi I (1999) Laparoscopic repair ofpostoperation ventral hernia. Early postoperation results. Surg En-dosc 13:928–931
37. Draus JM Jr, Huss SA, Harty NJ, Cheadle WG, Larson GM (2006)Enterocutaneous Wstula: are treatments improving? Surgery140:570–576
38. Leber GE, Garb JL, Alexander AI, Reed WP (1998) Long-termcomplications associated with prosthetic repair of incisional her-nias. Arch Surg 133:378–382
39. Bauer JJ, Harris MT, Kreel I, Gelernt IM (1999) Twelve-yearexperience with expanded polytetraXuoroethylene in the repair ofabdominal wall defects. Mt Sinai J Med 66:20–25
40. Chew DK, Choi LH, Rogers AM (2000) Enterocutaneous Wstula14 years after prosthetic mesh repair of a ventral incisional hernia:a life-long risk? Surgery 127:352–353
41. Vrijland WW, Jeekel J, Steyerberg EW, Den Hoed PT, Bonjer HJ(2000) Intraperitoneal polypropylene mesh repair of incisionalhernia is not associated with enterocutaneous Wstula. Br J Surg87:348–352
42. DeMaria EJ, Moss JM, Sugerman HJ (2000) Laparoscopic intra-peritoneal polytetraXuoroethylene (PTFE) prosthetic patch repairof ventral hernia. Prospective comparison to open prefascial poly-propylene mesh repair. Surg Endosc 14:326–329
43. Bageacu S, Blanc P, Breton C, Gonzales M, Porcheron J, ChabertM, Balique JG (2002) Laparoscopic repair of incisional hernia: aretrospective study of 159 patients. Surg Endosc 16:345–348
44. Carbajo MA, Martp del Olmo JC, Blanco JI, Toledano M, de laCuesta C, Ferreras C, Vaquero C (2003) Laparoscopic approach toincisional hernia. Surg Endosc 17:118–122
45. Yavuz N, Ipek T, As A, Kapan M, Eyuboglu E, Erguney S (2005)Laparoscopic repair of ventral and incisional hernias: our experiencein 150 patients. J Laparoendosc Adv Surg Tech A 15:601–605
46. Franklin ME Jr, Gonzalez JJ Jr, Glass JL, Manjarrez A (2004) Lap-aroscopic ventral and incisional hernia repair: an 11-year experi-ence. Hernia 8:23–27
47. Chowbey PK, Sharma A, Khullar R, Mann V, Baijal M, VashisthaA (2000) Laparoscopic ventral hernia repair. J Laparoendosc AdvSurg Tech A 10:79–84
48. Lomanto D, Iyer SG, Shabbir A, Cheah WK (2006) Laparoscopicversus open ventral hernia mesh repair: a prospective study. SurgEndosc 20:1030–1035
49. Park A, Birch DW, Lovrics P (1998) Laparoscopic and open inci-sional hernia repair: a comparison study. Surgery 124:816–821
50. Eid GM, Prince JM, Mattar SG, Hamad G, Ikrammudin S, SchauerPR (2003) Medium-term follow-up conWrms the safety and dura-bility of laparoscopic ventral hernia repair with PTFE. Surgery134:599–603
51. Sanchez LJ, Bencini L, Moretti R (2004) Recurrences after lapa-roscopic ventral hernia repair: results and critical review. Hernia8:138–143
52. Aura T, Habib E, Mekkaoui M, Brassier D, Elhadad A (2002) Lap-aroscopic tension-free repair of anterior abdominal wall incisionaland ventral hernias with an intraperitoneal Gore-Tex mesh: pro-spective study and review of the literature. J Laparoendosc AdvSurg Tech A 12:263–267
53. Rosen M, Brody F, Ponsky J, Walsh RM, Rosenblatt S, DuperierF, Fanning A, Siperstein A (2003) Recurrence after laparoscopicventral hernia repair. Surg Endosc 17:123–128
54. Ujiki MB, Weinberger J, Varghese TK, Murayama KM, Joehl RJ(2004) One hundred consecutive laparoscopic ventral hernia re-pairs. Am J Surg 188:593–597
55. Bower CE, Reade CC, Kirby LW, Roth JS (2004) Complicationsof laparoscopic incisional-ventral hernia repair: the experience ofa single institution. Surg Endosc 18:672–675
56. Ben-Haim M, Kuriansky J, Tal R, Zmora O, Mintz Y, Rosin D,Ayalon A, Shabtai M (2002) Pitfalls and complications with lapa-roscopic intraperitoneal expanded polytetraXuoroethylene patchrepair of postoperative ventral hernia. Surg Endosc 16:785–788
57. Kirshtein B, Lantsberg L, Avinoach E, Bayme M, Mizrahi S(2002) Laparoscopic repair of large incisional hernias. Surg En-dosc 16:1717–1719
58. Morales-Conde S, Cadet H, Cano A, Bustos M, Martin J, Morales-Mendez S (2005) Laparoscopic ventral hernia repair without su-tures—double crown technique: our experience after 140 caseswith a mean follow-up of 40 months. Int Surg 90:S56–S62
59. Toy FK, Bailey RW, Carey S, Chappuis CW, Gagner M, JosephsLG, Mangiante EC, Park AE, Pomp A, Smoot RT Jr, Uddo JF Jr,Voeller GR (1998) Prospective, multicenter study of laparoscopicventral hernioplasty. Preliminary results. Surg Endosc 12:955–959
60. Topart P, Ferrand L, Vandenbroucke F, Lozac�h P (2005) Laparo-scopic ventral hernia repair with the Goretex Dualmesh: long-termresults and review of the literature. Hernia 9:348–352
61. Berger D, Bientzle M, Muller A (2002) Postoperative complica-tions after laparoscopic incisional hernia repair. Incidence andtreatment. Surg Endosc 16:1720–1723
62. McKinlay RD, Park A (2004) Laparoscopic ventral incisional her-nia repair: a more eVective alternative to conventional repair ofrecurrent incisional hernia. J Gastrointest Surg 8:670–674
63. Olmi S, Erba L, Magnone S, Bertolini A, Croce E (2006) Prospec-tive clinical study of laparoscopic treatment of incisional and ven-tral hernia using a composite mesh: indications, complications andresults. Hernia 10:243–247
64. LeBlanc KA, Whitaker JM, Bellanger DE, Rhynes VK (2003)Laparoscopic incisional and ventral hernioplasty: lessons learnedfrom 200 patients. Hernia 7:118–124
65. Frantzides CT, Carlson MA, Zografakis JG, Madan AK, MooreRE (2004) Minimally invasive incisional herniorrhaphy: a reviewof 208 cases. Surg Endosc 18:1488–1491
66. Cobb WS, Kercher KW, Matthews BD, Burns JM, Tinkham NH,Sing RF, Heniford BT (2006) Laparoscopic ventral hernia repair:a single center experience. Hernia 10:236–242
67. Heniford BT, Park A, Ramshaw BJ, Voeller G (2003) Laparo-scopic repair of ventral hernias: nine years’ experience with 850consecutive hernias. Ann Surg 238:391–399
68. Aufenacker TJ, Koelemay MJ, Gouma DJ, Simons MP (2006)Systematic review and meta-analysis of the eVectiveness of antibi-otic prophylaxis in prevention of wound infection after mesh re-pair of abdominal wall hernia. Br J Surg 93:5–10
69. Merritt K, Hitchins VM, Neale AR (1999) Tissue colonizationfrom implantable biomaterials with low numbers of bacteria. JBiomed Mater Res 44:261–265
70. Klinge U, Junge K, Spellerberg B, Piroth C, Klosterhalfen B,Schumpelick V (2002) Do multiWlament alloplastic meshes increase
123

492 Hernia (2007) 11:481–492
the infection rate? Analysis of the polymeric surface, the bacteriaadherence, and the in vivo consequences in a rat model. J BiomedMater Res 63:765–771
71. Carbonell AM, Matthews BD, Dreau D, Foster M, Austin CE,Kercher KW, Sing RF, Heniford BT (2005) The susceptibilityof prosthetic biomaterials to infection. Surg Endosc 19:430–435
72. Diaz JJ Jr, Gray BW, Dobson JM, Grogan EL, May AK, MillerR, Guy J, O’Neill P, Morris JA Jr (2004) Repair of giant abdom-inal hernias: does the type of prosthesis matter? Am Surg70:396–401
73. Beldi G, Ipaktchi R, Wagner M, Gloor B, Candinas D (2006) Lap-aroscopic ventral hernia repair is safe and cost-eVective. Surg En-dosc 20:92–95
74. LeBlanc KA, Whitaker JM (2002) Management of chronic postop-erative pain following incisional hernia repair with Composixmesh: a report of two cases. Hernia 6:194–197
75. Simmermacher RK, Schakenraad JM, Bleichrodt RP (1994) Re-herniation after repair of the abdominal wall with expanded poly-tetraXuoroethylene. J Am Coll Surg 178:613–616
76. Susmallian S, Gewurtz G, Ezri T, Charuzi I (2001) Seroma afterlaparoscopic repair of hernia with PTFE patch: is it really a com-plication? Hernia 5:139–141
77. Morales-Conde S (2004) Laparoscopic ventral hernia repair: ad-vances and limitations. Semin Laparosc Surg 11:191–200
78. Tsimoyiannis EC, Siakas P, Glantzounis G, Koulas S, Mavridou P,Gossios KI (2001) Seroma in laparoscopic ventral hernioplasty.Surg Laparosc Endosc Percutan Tech 11:317–321
79. Coda A, Bendavid R, Botto-Micca F, Bossotti M, Bona A (2003)Structural alterations of prosthetic meshes in humans. Hernia7:29–34
80. Gonzalez R, Fugate K, McClusky D III, Ritter EM, Lederman A,Dillehay D, Smith CD, Ramshaw BJ (2005) Relationship betweentissue ingrowth and mesh contraction. World J Surg 29:1038–1043
81. Klinge U, Klosterhalfen B, Muller M, Ottinger AP, SchumpelickV (1998) Shrinking of polypropylene mesh in vivo: an experimen-tal study in dogs. Eur J Surg 164:965–969
82. Conze J, Krones CJ, Schumpelick V, Klinge U (2006) Incisionalhernia: challenge of re-operations after mesh repair. LangenbecksArch Surg (Epub ahead of print)
123