Embed Size (px)
Citation preview

969–981www.elsevier.com/locate/bone
Bone 42 (2008)
Large-scale analysis of association between polymorphisms in the transforminggrowth factor beta 1 gene (TGFB1) and osteoporosis: The GENOMOS study
Bente L. Langdahl a,⁎, André G. Uitterlinden b, Stuart H. Ralston c, Thomas A. Trikalinos d,Susanne Balcells e, Maria Luisa Brandi f, Serena Scollen g, Paul Lips h, Roman Lorenc i,Barbara Obermayer-Pietsch j, David M. Reid k, Jácome Bruges Armas l,m, Pascal P. Arp b,
Amelia Bassiti k, Mariona Bustamante e, Lise Bjerre Husted a, Alison H. Carey n, Ramon Pérez Cano o,Harald Dobnig j, Alison M. Dunning g, Astrid Fahrleitner-Pammer j, Alberto Falchetti f,Elzbieta Karczmarewicz i, Marcin Kruk i, Johannes P.T.M. van Leeuwen b, Laura Masi f,Joyce B.J. van Meurs b, Jon Mangion n, Fiona E.A. McGuigan k, Leonardo Mellibovsky p,Leif Mosekilde a, Xavier Nogués p, Huibert A.P. Pols b, Jonathan Reeve g, Wilfried Renner j,
Fernando Rivadeneira b, Natasja M. van Schoor h, John P.A. Ioannidis d
APOSS investigatorsDOPS investigatorsEPOS investigators
EPOLOS investigatorsFAMOS investigatorsLASA investigatorsERGO investigators
for the GENOMOS Study 1,2
⁎ Corresponding author. Department of Endocrinology, Aarhus University, DK-8000 Aarhus C, Denmark.E-mail address: [email protected] (B.L. Langdahl).
1 The GENOMOS Study is a collaboration between the Department of Internal Medicine, Erasmus MC, Rotterdam, The Netherlands; Rheumatic Diseases Unit,University of Edinburgh, UK, Western General Hospital Edinburgh, UK; Department of Medicine and Therapeutics, University of Aberdeen Medical School,Aberdeen, UK; Oxagen Limited, Abingdon, UK; Department of Internal Medicine, University of Florence, Florence, Italy; Department of Genetics, University ofBarcelona, Barcelona, Spain; Department of Endocrinology, Aarhus University Hospital, Aarhus, Denmark; Department of Biochemistry and Experimental Medicine,The Children's Memorial Health Institute, Warsaw, Poland; Department of Endocrinology and Nuclear Medicine, Department of Internal Medicine, MedicalUniversity, Graz, Austria; Strangeways Research Laboratory, Cambridge University, Cambridge, UK; EMGO Institute, VU University Medical Center, Amsterdam,The Netherlands; Hospital del Mar-IMIM, UAB, Barcelona, Spain; and Clinical and Molecular Epidemiology Unit, Department of Hygiene and Epidemiology,University of Ioannina School of Medicine and Biomedical Research Institute, Foundation for Research and Technology-Hellas, Ioannina, Greece.2 Additional investigators participating in GENOMOS include the following: University of Ioannina School of Medicine: Despina G. Contopoulos-Ioannidis,
Department of Internal Medicine, Erasmus MC, Rotterdam: Wendy Hugens; Institute of Medical Sciences, University of Aberdeen Medical School: Omar M.E.Albagha, Helen Macdonald, Alison Stewart; Aarhus University Hospital: Mette Carstens, Liselotte Stenkjaer; Oxagen Limited, Abingdon, UK: Bryan Dechairo, IanMackay, Simon Bennett; University of Florence Medical School, Annalisa Tanini; Department of Genetics, Faculty of Biology, Barcelona, Spain: Daniel Grinberg;Hospital del Mar, Barcelona, Spain: Adolfo Diez Perez, Anna Enjuanes; Abteilung Endokrinologie/Nuklearmedizin, Medizinische Universitat Graz, Graz, Austria:DanielaWalter, Ursula Hartl, MarkusGugatschka, Christine Bonelli; Department ofMedical Genetics, University of Antwerp, Antwerp, Belgium:Wim vanHul and thefollowing study group members: APOSS Study Group: Claire Parsons, Stuart Bear, Rosie Farmer; DOPS Study Group: Kim Brixen, Jens-Erik Beck Jensen, Pia Eiken;EPOLOS Study Group: J. Lukaszkiewicz, P. Bilinski, E. Czerwinski, A. Lewinski, E. Marcinowska-Suchowierska, A. Milewicz, M. Spaczynski, M. Jaworski; EPOSStudy Group: R Nuti (Siena, IT), S Grazio (Zagreb, CR), T Miazgowski (Szczecin, PL), R Boonen (Leuven, BE), P Masaryk (Piestany, SK), JJ Stepan (Prague, CZ), ALopesVaz (Porto, PT), J Cannata (Oviedo, ES), KWeber (Graz, AT), LI Benevolenskaya (Moscow, RU), C Todd andK-TKhaw (Norfolk, Cambridge andHarrow,UK),J da Silva (Coimbra PT), A Bhalla (Bath, UK), G Poor (Budapest HU), J Bruges Armas (Azores, PT), G Lyritis (Athens, GR), TW O'Neill, M Lunt (Cambridge andManchester UK, Co-ordination); FAMOS Study Group: Juliet Compston (University of Cambridge, Cambridge, UK), Cyrus Cooper (University of Southampton,Southampton, UK), Emma Duncan (Nuffield Orthopaedic Centre, Oxford, UK), Richard Keen, (University College, London, UK), Alastair McLellan (University ofGlasgow, Glasgow, UK) and John Wass (Nuffield Orthopaedic Centre, Oxford, UK); LASA Study Group: Ebbo Dekema, Huub van Essen, Saskia Pluijm, NatalieBravenboer; Rotterdam Study Group: Albert Hofman, Cornelia M van Duijn, Paulus J de Jong, Monique M Breteler, Bruno H Stricker, Jacqueline C Witteman.
8756-3282/$ - see front matter © 2007 Elsevier Inc. All rights reserved.doi:10.1016/j.bone.2007.11.007

970 B.L. Langdahl et al. / Bone 42 (2008) 969–981
a Department of Endocrinology, Aarhus University Hospital, Aarhus, Denmarkb Department of Internal Medicine, Erasmus MC, Rotterdam, The Netherlands
c Rheumatic Diseases Unit, University of Edinburgh, Western General Hospital Edinburgh, UKd Clinical and Molecular Epidemiology Unit, Department of Hygiene and Epidemiology, University of Ioannina School of Medicine and
Biomedical Research Institute, Foundation for Research and Technology-Hellas, Ioannina, Greecee Department of Genetics, University of Barcelona, Barcelona, Spain
f Department of Internal Medicine, University of Florence, Florence, Italyg Strangeways Research Laboratory, Cambridge University, Cambridge, UK
h EMGO Institute, VU University Medical Center, Amsterdam, The Netherlandsi Department of Biochemistry and Experimental Medicine, The Children's Memorial Health Institute, Warsaw, Poland
j Department of Endocrinology and Nuclear Medicine, Department of Internal Medicine, Medical University, Graz, Austriak Department of Medicine and Therapeutics, University of Aberdeen Medical School, Aberdeen, UK
l Servico Especializado de Epidemiologia e Biologia Molecular, Hosptial de Santo Espiroto, Azores, Portugalm Genetics and Arthritis Research Group (GARG), Porto, Portugal
n Oxagen Limited, Abingdon, UKo Department of Internal Medicine, University Hospital Virgin Macarena, Sevilla, Spain
p Hospital del Mar-IMIM, UAB, Barcelona, Spain
Received 27 June 2007; revised 5 November 2007; accepted 12 November 2007Available online 3 December 2007
Abstract
Introduction: The TGFB1 gene which encodes transforming growth factor beta 1, is a strong candidate for susceptibility to osteoporosis andseveral studies have reported associations between bone mineral density (BMD), osteoporotic fractures and polymorphisms of TGFB1, althoughthese studies have yielded conflicting results.Methods: We investigated associations between TGFB1 polymorphisms and BMD and fracture in the GENOMOS study: a prospective multicenterstudy involving 10 European research studies including a total of 28,924 participants. Genotyping was conducted for known TGFB1 polymorphismsat the following sites: G−1639-A (G−800-A, rs1800468), C−1348-T (C−509-T, rs1800469), T29-C (Leu10Pro, rs1982073), G74-C (Arg25Pro,rs1800471) and C788-T (Thr263Ile, rs1800472). These polymorphisms were genotyped prospectively and methodology was standardized acrossresearch centers. Genotypes and haplotypes were related to BMD at the lumbar sine and femoral neck and fractures.Results: There were no significant differences in either women or men at either skeletal site for any of the examined polymorphisms with the possibleexception of a weak association with reduced BMD (−12 mg/cm2) in men with the T−1348 allele ( pb0.05). None of the haplotypes was associatedwith BMD and none of the polymorphisms or haplotypes significantly affected overall risk of fractures, however, the odds ratio for incident vertebralfracture in carriers of the rare T788 allele was 1.64 (95% CI: 1.09–2.64), pb0.05.Conclusions: This study indicates that polymorphic variation in the TGFB1 gene does not play a major role in regulating BMD or susceptibility tofractures. The weak associations we observed between the C−1348-T and lumbar spine BMD in men and between C788-T and risk of incidentvertebral fractures are of interest but could be chance findings and will need replication in future studies.© 2007 Elsevier Inc. All rights reserved.
Keywords: Transforming growth factor beta 1; Fracture; Bone mineral density; Osteoporosis; Meta-analysis
Introduction
Osteoporosis is a common disease, affecting one in threewomen and one in eight men above the age of 50. Osteoporosisis characterized by reduced bone mineral density, deteriorationof the microarchitecture of bone tissue and increased risk offractures [1]. Diagnosis and treatment is based on measurementof bone mineral density (BMD), however, reduced BMD is onlyone aspect of fracture risk; other contributors include bonequality, previous fracture and genetic predisposition. During thelast 10–15 years many research groups have investigated spe-cific genetic variants but the results have been varying, and insome cases even contradictory.
Transforming growth factor (TGF) β1 (TGFB1; 19q13.1)was one of the first suggested candidate genes to contributeto genetic risk for osteoporosis for several reasons. TGFβ1 is
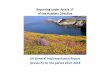
expressed by osteoblasts, is present in high concentrations inbone tissue and involved in the control of bone resorption andformation [1–3]. TGFB1 knockout mice display reduced BMDand bone elasticity [4]. Furthermore, Camurati–Engelmann dis-ease, an autosomal dominant, progressive diaphyseal dysplasia,characterized by hyperostosis and sclerosis of the diaphyses oflong bones, is caused by mutations in the TGFB1 gene (OMIN131300)[5–8] (Fig. 1). Several polymorphisms have been iden-tified in the TGFB1 gene [9–11] (Fig. 1). These polymorphismsare located in the promoter or in a region of TGFB1 whichencodes the latent associated peptide (LAP). Following mRNAtranslation, the LAP is cleaved from the mature TGFβ1 peptideand subsequently binds to mature TGFβ1 to form an inactivatedsecretory complex. Polymorphisms in the promoter may in-fluence transcription [12] whereas polymorphisms that interferewith binding of LAP may lead to increased levels of bioactive

Fig. 1. Exon–intron structure of the TGFB1 gene with mutations causing Camurati–Engelmann disease in the upper part and polymorphisms previously associatedwith osteoporotic phenotypes in the lower part. Location of the genetic variants is indicated by vertical lines within the 31 kb gene region. The indicated haplotypeblock is from Hapmap data, the vertical lines indicate polymorphisms used in the Hapmap to identify the block. Haplotype allele structure is shown in the bottom part.The haplotypes are numbered 1–4 by decreasing frequency.
971B.L. Langdahl et al. / Bone 42 (2008) 969–981
TGFβ1 [6] and thereby increased bone turnover [13,14].Previously, the promoter polymorphism C−1348-T has beenassociated with changes in BMD, although with different andcontradictory results [9,15]. The T-allele of the T29-C poly-morphism in the LAP was associated with reduced BMD inJapanese and Danish populations [9,16–19], but with increasedBMD in German and Australian populations [20,21]. Further-more, the T29-C and C−1348-T polymorphisms are in stronglinkage disequilibrium and an additive effect of the twopolymorphisms on BMD was identified by some investigators[15], but not by others [9]. None of the above mentioned studieshas investigated the effects of TGFB1 haplotypes on BMD andfracture risk.
We therefore aimed to investigate the effects of G−1639-A,C−1348-T, T29-C, G74-C and C788-Tseparately and as haplotypeson BMD and fracture risk in a large-scale collaborativeassociation study with standardized genotyping and outcomedefinitions.
Methods
The GENOMOS consortium [22] performed a collaborative analysisincluding 28,924 participants enrolled from 10 European studies (Table 1).The consortium used prospective genotyping with cross-center standardization.
Main outcomes were BMD at the lumbar spine and femoral neck, all fractures;and vertebral fractures.
Organizational issues
The GENOMOS project is a large-scale study of several candidate genepolymorphisms for osteoporosis outcomes [22]. This report includes 10 studiesincluded in previous meta-analyses of ESR1, COLIA1 and VDR genespolymorphisms [22–24]. One study (BARCOS) provided additional fractureand genotype data for this meta-analysis.
The characteristics of the 10 studies included in this meta-analysis werepreviously reported [22–24]. The 5 longitudinal cohorts are the AberdeenProspective Osteoporosis Study (APOSS) [25], the Longitudinal Aging StudyAmsterdam (LASA) [26], the Danish Osteoporosis Prevention Study (DOPS)[27], the European Prospective Osteoporosis Study (EPOS) [28], including datafrom the European Polish Osteoporosis Study (EPOLOS), and the Rotterdamstudy (ERGO) [29]. The 5 cross-sectional studies included are the AarhusOsteoporosis Study (AROS) [30], the Barcelona Cross-sectional Study(BARCOS) [31], the Florence Cross-sectional Study (FLOS), the Graz Cross-sectional Study (AUSTRIOS) [32], and the Familial Osteoporosis Study(FAMOS) [33]. Only the clinic-based studies (AROS, AUSTRIOS, BARCOS,DOPS and FLOS) excluded patients with chronic steroid use, hyperthyroidismand hyperparathyroidism.
All participating studies contributed information on sex, age, height, weight,TGFB1 genotypes, and BMD at lumbar spine and femoral neck (in g/cm2). Thestudies also provided information on menopausal status and use of hormonereplacement therapy (HRT) for women. All the studies contributed informationon fracture (any fracture, and vertebral fractures). However, the participating

Table 1Study population characteristics and genotype/haplotype distribution
Study acronym AROS APOSS LASA BARCOS DOPS EPOS FLOS AUSTRIOS FAMOS ERGO
Research center Aarhus Aberdeen Amsterdam Barcelona Aarhus Cambridge Florence Graz Oxagen Rotterdam
CharacteristicsDesign Case-control Cohort Cohort Cross-sectional Cohort Cohort Cross-sectional Cross-sectional Cross-sectional CohortSex F: 588 M: 157 F: 3886 F:785 M:728 F: 876 F:2016 F: 2513 M:1733 F: 2057 M:743 F:1464 M:415 F: 341 M: 221 F: 4878 M: 3105Mean age (SD) 61.4 (13.2) 53.5 (15.8) 48.5 (2.4) 76.0 (6.7) 75.9 (6.6) 55.0 (8.7) 50.6 (2.8) 64.9 (10.8) 64.4 (12.2) 61.8 (13.0) 62.3 (16.3) 70.8 (20.5) 67.4 (17.0) 46.8 (14.7) 48.6 (14.9) 70.1 (9.3) 68.4 (8.2)Mean height
(SD), cm161.6 (6.6) 176.4 (7.3) 161.2 (5.9) 160.0 (6.4) 173.0 (6.8) 156.3 (6.3) 164.6 (6.0) 158.3 (6.6) 171.1 (7.2) 158.2 (7.1) 169.6 (9.2) 157.5 (8.6) 172.4 (9.1) 163.2 (6.9) 177.6 (7.2) 161.1 (6.7) 174.6 (6.8)
Mean weight(SD), kg
64.2 (10.9) 78.4 (12.2) 66.2 (12.2) 70.8 (13.0) 77.9 (11.9) 64.6 (9.9) 68.0 (12.1) 67.9 (11.8) 79.3 (11.5) 63.6 (10.5) 76.3 (13.0) 61.9 (11.6) 77.6 (13.9) 66.0 (14.3) 80.8 (13.3) 69.3 (11.4) 78.2 (10.8)
Mean BMI (SD) 24.6 (4.1) 25.3 (3.7) 25.5 (4.5) 27.7 (4.9) 26.0 (3.4) 26.4 (3.9) 25.1 (4.3) 27.1 (4.7) 27.1 (3.6) 25.5 (4.3) 26.4 (3.6) 25.0 (4.6) 26.0 (3.8) 24.7 (4.5) 25.6 (3.9) 26.7 (4.1) 25.6 (3.0)Post-menopausal
(%)486 (82.7) Not
pertinent1779 (46.1) 781 (100) Not pertinent 854 (99.0) 2016 (100) 2082 (88.4) Not pertinent 1849 (90.1) Not pertinent 1173 (80.1) Not pertinent 158 (46.3) Not pertinent 4865 (99.7) Not
pertinentHRT (%) 0 (0.0) Not
pertinent2266 (58.6) 101 (13.0) Not pertinent 0 (0.0) 0 (0.0) 306 (15.6) Not pertinent 107 (5.2) Not pertinent 71 (4.8) Not pertinent 79 (23.2) Not pertinent 692 (15.0) Not
pertinentActivity/ability⁎⁎
Index range No data No data 0.76–3.26 0–624 0–625 No data 0–80 0–24 0–24 No data No data 0–4 0–4 3–14 3–14 0–3 0–3Median No data No data 1.77 156 102 No data 15 21 23 No data No data 1 1 7.00 8.33 2.75 2.88
Mean BMD,g/cm2
Method Hologic(Cal)
Hologic(Cal)
Norland Hologic Hologic Hologic Hologic(Cal)
Various(ESP)
Various(ESP)
Hologic Hologic Hologic Hologic Various(ESP)
Various(ESP)
Lunar Lunar
LS (SD) 0.827(0.179)
0.829(0.178)
1.052(0.161)
0.915 (0.167) 1.036 (0.189) 0.853 (0.153) 1.027 (0.139) 0.928 (0.190) 1.032 (0.185) 0.870 (0.173) 0.997 (0.171) 0.940 (0.152) 1.013 (0.144) 1.000 (0.205) 1.088 (0.247) 1.036 (0.180) 1.165(0.197)
N for LS data 567 155 3882 274 260 870 2008 861 546 2001 733 512 236 335 215 3381 2463FN (SD) 0.671
(0.129)0.683(0.116)
0.881(0.125)
0.662 (0.107) 0.742 (0.136) 0.682 (0.109) 0.797 (0.114) 0.727 (0.137) 0.850 (0.150) 0.693 (0.146) 0.865 (0.170) 0.751 (0.120) 0.855 (0.120) 0.775 (0.150) 0.846 (0.171) 0.811 (0.131) 0.876(0.133)
N for FN data 561 154 3881 263 259 721 1998 2008 1497 930 131 512 241 336 217 3239 2435Any fracture (%) 247 (42.0) 56 (35.7) 784 (20.2) 391 (63.2) 327 (59.0) 138 (21.4) 410 (20.5) 815 (32.6) 407 (23.6) 294 (14.5) 86 (11.6) 577 (39.4) 172 (41.4) 131 (38.9) 104 (47.7) 1197 (24.5) 400 (12.9)Incident (%) No data No data 344 (9.0) 150 (19.2) 87 (12.0) No data No data 323 (16.7) 73 (5.7) No data No data 1113 (22.8) 317 (10.2)No/lowtrauma (%)
247 (42.0) 56 (35.7) No data 190 (38.0) 160 (33.8) 113 (21.0) 141 (7.0) 815 (32.6) 407 (23.6) 294 (14.5) 86 (11.6) No data No data 79 (23.4) 47 (21.5) 1014 (20.8) 269 (8.7)
Vertebralfracture (%)
247 (42.0) 56 (35.7) 16 (0.4) 136 (50.9) 128 (49.2) 52 (9.6) 32 (1.6) 228 (9.1) 123 (7.1) 133 (6.6) 12 (1.6) 401 (27.4) 60 (14.5) 14 (4.2) 11 (5.0) 316 (15.5) 161 (10.6)
Incident (%) No data No data 6 (0.2)⁎⁎ 21 (6.6) 16 (5.4) No data No data 67 (3.7) 21 (1.6) No data No data 213 (4.4) 68 (2.2)
972B.L.Langdahl
etal.
/Bone
42(2008)
969–981

Genotypes n (%)G-1639-AGG 371 (78.1) 94 (76.4) 2528 (80.9) 385 (83.7) 366 (83.8) 672 (82.4) 1281 (81.3) 2132 (85.0) 1468 (85.1) 1383 (85.7) 510 (84.3) 1183 (85.7) 341 (87.7) 274 (82.5) 178 (85.2) 3158 (82.3) 2201 (84.1)GA 98 (20.6) 28 (22.8) 565 (18.1) 71 (15.4) 67 (15.3) 132 (16.2) 279 (17.7) 354 (14.1) 249 (14.4) 216 (13.4) 88 (14.5) 191 (13.8) 48 (12.3) 58 (17.5) 31 (14.8) 654 (17.0) 396 (15.1)AA 6 (1.3) 1 (0.8) 33 (1.1) 4 (0.9) 4 (0.9) 12 (1.2) 15 (1.0) 21 (0.8) 9 (0.5) 14 (0.9) 7 (1.2) 6 (0.4) 0 (0.0) 0 (0.0) 0 (0.0) 26 (0.7) 21 (0.8)
C-1348-TCC 230 (48.2) 71 (57.7) 1639 (51.2) 230 (51.6) 205 (46.7) 358 (44.5) 799 (49.6) 1150 (46.3) 805 (47.0) 652 (35.8) 267 (38.6)⁎ 626 (43.7) 166 (41.9 162 (48.8) 100 (47.4) 1934 (50.4) 1301
(49.9)⁎
CT 195 (40.9) 46 (37.4) 1296 (40.6) 179 (40.1) 197 (44.9) 355 (44.2) 683 (42.4) 1.078 (43.4) 739 (43.1) 850 (46.7) 297 (43.0)⁎ 650 (45.4) 183 (46.2 137 (41.3) 92 (43.6) 1584 (41.3) 1038(39.3)⁎
TT 52 (10.9) 6 (4.9) 269 (8.4) 37 (8.3) 37 (8.4) 91 (11.3) 128 (8.0) 256 (10.3) 169 (9.9) 317 (17.4) 127 (18.4)⁎ 156 (10.9) 47 (11.9) 33 (9.9) 19 (9.0) 318 (8.3) 268 (10.3)⁎
T29-CTT 200 (42.0) 64 (52.0) 1310 (41.6) 183 (40.0) 160 (36.4) 283 (36.5) 724 (47.5)⁎ 857 (36.1) 611 (37.6) 487 (28.2)⁎ 175 (28.5)⁎ 499 (35.0) 135 (34.4 131 (39.2) 80 (37.9) 1539 (40.2) 994 (38.)TC 209 (43.9) 51 (41.5) 1446 (45.9) 216 (47.3) 223 (50.8) 356 (45.9) 622 (40.8)⁎ 1124 (47.4) 757 (46.6) 799 (46.3)⁎ 280 (45.6)⁎ 708 (49.7) 193 (49.1 151 (45.2) 103 (48.8) 1788 (46.7) 1214 (46.5)CC 67 (14.1) 8 (6.5) 269 (8.4) 58 (12.6) 56 (12.8) 136 (17.5) 177 (11.6)⁎ 390 (16.4) 258 (15.9) 438 (25.4)⁎ 159 (25.9)⁎ 218 (15.3) 65 (16.5) 52 (15.6) 28 (13.3) 502 (13.1) 405 (15.5)
G74-CGG 419 (88.2) 104 (85.2) 2540 (85.6) 374 (84.0) 377 (86.7)⁎ 676 (86.2) 1370 (84.5) 2134 (85.1)⁎ 1475 (85.6) 1455 (89.5)⁎ 566 (84.7) 1220 (87.5) 349 (88.8 277 (85.2) 179 (86.9) 3302 (86.2) 2206 (84.7)GC 52 (10.9) 17 (13.9) 412 (13.9) 67 (15.1) 50 (11.5)⁎ 106 (13.5) 240 (14.8) 349 (13.9)⁎ 235 (13.6) 158 (9.7)⁎ 98 (14.7) 167 (12.0) 42 (10.7) 47 (14.5) 26 (12.6) 510 (13.3) 385 (14.8)CC 4 (0.8) 1 (0.8) 14 (0.5) 4 (0.9) 8 (1.8)⁎ 2 (0.3) 11 (0.7) 25 (1.0)⁎ 14 (0.8) 13 (0.8)⁎ 4 (0.6) 8 (0.6) 2 (0.5) 1 (0.3) 1 (0.5) 20 (0.5) 14 (0.5)
C788-TCC 459 (95.6) 121 (98.4) 3069 (96.9) 448 (96.1) 433 (95.4) 783 (94.5) 1579 (96.0) 2360 (94.2)⁎ 1637 (94.7) 1659 (87.7) 571 (89.5) 1323 (92.0) 361 (90.5 315 (95.2) 200 (95.2) 3721 (96.5) 2539 (96.2)⁎
CT 21 (4.4) 2 (1.6) 97 (3.1) 17 (4.6) 21 (4.6) 46 (5.5) 65 (4.0) 137 (5.5)⁎ 88 (5.1)⁎ 220 (11.6) 65 (10.2) 133 (7.9) 38 (9.5) 16 (4.8) 10 (4.8) 132 (3.4) 97 (3.7)⁎
TT 0 (0.0) 0 (0.0) 2 (0.1) 1 (0.2) 0 (0.0) 0 (0.0) 1 (0.1) 7 (0.3)⁎ 4 (0.2)⁎ 13 (0.7) 2 (0.3) 2 (0.1) 0 (0.0) 0 (0.0) 0 (0.0) 3 (0.1) 4 (0.2)⁎
Haplotype alleles (%)
G-1639-A, C-1348-T, T29-C, G74-C1. G-C-T-G 50.6 57.4 53.1 55.3 53.1 48.8 52.2 51.8 53.0 45.0 43.3 56.8 52.7 53.4 53.0 54.3 52.72. G-T-C-G 29.4 19.7 27.0 27.3 31.1 32.4 25.4 31.9 31.1 41.0 40.1 36.2 34.5 29.9 32.0 28.7 30.03. A-C-T-G 11.3 11.5 9.9 8.6 8.6 9.7 9.8 7.8 7.8 7.3 8.1 8.0 6.0 8.9 7.7 9.2 8.44. G-C-C-C 5.9 7.0 7.1 8.3 7.0 7.4 6.7 8.0 7.7 5.7 7.4 7.0 5.9 7.2 5.2 7.1 8.0Other 2.7 4.5 3.0 0.5 0.1 1.8 5.9 0.6 0.4 0.7 1.2 1.0 0.9 0.6 1.5 0.7 0.9
Pb.95 n (%)⁎⁎⁎ 1 (0.2) 2 (1.6) 29 (1.0) 0 0 2 (0.3) 13 (1) 0 0 1 (0.1) 0 0 0 1 (0.4) 3 (1.5) 14 (0.4) 3 (0.1)
BMD: bone mineral density; Cal: calibration of a few Norland values to Hologic equivalents; ESP: European Spine Phantom calibration; LS: lumbar spine; HRT: hormone replacement therapy (at any time up to the tim f BMD measurement); FN: femoral neck; SD: standard deviation;Reported percentages are estimated based on participants with available data for the respective characteristic. “Oxagen” represents the FAMOS study. EPOLOS data are combined with EPOS.⁎The genotype distribution was not in Hardy–Weinberg equilibrium.⁎⁎Physical activity/ability data were measured in different scales capturing various activities and abilities across cohorts.⁎⁎⁎Data where haplotypes were inferred with credibility b95%.
973B.L.Langdahl
etal.
/Bone
42(2008)
969–981
)
)
))
)
)
e o

974 B.L. Langdahl et al. / Bone 42 (2008) 969–981
centers had gathered this information differently. Thus we also examinedseparately in sensitivity analyses incident fractures, incident vertebral fracturesand low/no trauma fractures.
Prevalent fracturesIn AROS, BARCOS, DOPS, and ERGO fractures at or before the time of
enrolment had radiographic documentation. In AUSTRIOS, BARCOS, EPOS,FLOS, FAMOS, and LASA fractures had clinical history or questionnairedocumentation. All vertebral fractures had radiographic documentation withclinical or morphometric criteria [34], except for APOSS (questionnaire only).DOPS, FLOS, FAMOS, and LASA counted fractures occurring at any time oflife. APOSS excluded fractures occurring under age 18. AUSTRIOS and EPOSexcluded fractures occurring under age 20. BARCOS excluded fracturesoccurring under age 45. AROS and ERGO only counted vertebral fracturesdocumented radiographically at enrolment. BARCOS excluded fractures of thehands, fingers, toes, feet, face and skull. AUSTRIOS excluded fractures of thehands, face, skull and clavicle. BARCOS, EPOS, and FLOS excluded hightrauma fractures.
Incident fracturesLongitudinal studies had also available data on incident fractures that had
occurred during the period of follow up. Radiographs at the time of the clinicalpresentation were obtained for all incident vertebral fractures. If the incidentfractures were caused by high- low-energy or no traumas were evaluated frommedical records or questionnaires.
Ethical considerationsAll participating centers received ethics committee approval per local reg-
ulations and informed consent followed the requirements of each center.
Fig. 2. Unadjusted differences in BMD at the lumbar spine (mg/cm2) per minor allelemen and women separately, as a random effects summary difference in BMD and 9
Genotyping
Genotyping of rs1800468 (G−1639-A, C−800-T), rs1800469 (C−1348-T,C−509-T), rs1982073 (T29-C, Leu10Pro), rs1800471 (G74-C, Arg25Pro) andrs1800472 (C788-T, Thr263Ile) was performed using various techniques: Taqman(Aberdeen Cambridge, Florence, Graz, Oxagen and Rotterdam), pyrosequencing(Oxagen), restriction fragment length methods (Aarhus, Aberdeen, Barcelona),sequencing (Aberdeen), and SNaPshot (Barcelona). Some centers genotypedmore than one cohort: Aarhus genotyped AROS and DOPS, Cambridgegenotyped EPOS and EPOLOS and Rotterdam genotyped ERGO, part ofFAMOS, FLOS and LASA. We cross-validated these different methods byblinded genotyping of 50 randomly selected samples by all genotyping centers.The coordinating center in Rotterdam evaluated the results and reported anydiscrepancies in the reference plate to improve calling of genotypes. We repeatedgenotyping of the reference plate and centers had to switch genotypingtechniques if they were still generating N5% errors in the reference plate. Onecenter changed from restriction fragment length method to Taqman and anotherfrom sequencing to restriction fragment length method. In addition, each centerchecked their own cohort genotyping afterwards by re-analyzing at least 5% oftheir samples with random selection. Less than 1% discrepancies were observedfor each center. Hardy–Weinberg equilibrium (HWE) was calculated after cohortgenotypes were submitted to the genotyping coordinating center. When HWEproblems were encountered, the contributing center was asked to re-check theircohort genotypes.
BMD measurements
BMD was measured by dual-energy X-ray absorptiometry. AROS,AUSTRIOS, BARCOS, DOPS, FLOS, and LASA used Hologic bone
copy for the five SNPs. The results are presented for the individual studies and in5% CI.

975B.L. Langdahl et al. / Bone 42 (2008) 969–981
densitometers (Hologic, Bedford, Mass, USA). APOSS used Norland XR26 andXR36 densitometers (Norland, Cooper Surgical, Trumbull, Conn, USA). ERGOused Lunar DPX-L or DPX densitometers (Lunar, GE Medical Systems,Madison, Wis, USA). EPOS and FAMOS used a variety of devices cross-calibrated with the European Spine Phantom [35]. Syntheses of BMD dataacross studies always include a study-effect to account for differences acrosspopulations and between centers. The interpretation of the meta-analysisresults for BMD was performed with emphasis on the BMD differences(absolute differences in the mean values of BMD across genotypes). We did notfocus on absolute BMD values, since these values may depend on the measuringdevice.
Outcomes
The main outcomes include BMD of the lumbar spine and femoral neck,all fractures (as defined by each cohort), and vertebral fractures by clinicalor morphometric criteria [34]. Sensitivity analyses for incident fractures,incident vertebral fractures, and low/no trauma fractures were performed.The latter exclude fractures occurring with high trauma, as assessed by thecircumstances in which they had occurred and/or their location. Allstudies except APOSS and AUSTRIOS had information on low/no traumafractures.
Participants were unrelated in all studies except FAMOS which is a family-based study co-ordinated by the company Oxagen until January 2005 and sinceby Erasmus MC. From FAMOS, one participant was selected per pedigree(using random number selection in each pedigree). Sensitivity analysis using allFAMOS participants revealed similar results (not shown).
Fig. 3. Unadjusted differences in BMD at the femoral neck (mg/cm2) per minor allelemen and women separately, as mean and 95% CI.
Analyses
Hardy–Weinberg equilibrium and haplotype reconstructionWe performed exact tests for Hardy–Weinberg equilibrium proportions [36]
using the GENEPOP program (http://wbiomed.curtin.edu.au/genepop/). Thistest evaluates whether the distribution of genotypes differs from the expectedproportions p2, 2p(1-p) and (1-p)2 where p is the minor allele frequency. Weinferred haplotypes of the four linked polymorphisms (G−1639-A, C−1348-T, T29-C and G74-C) using the PHASE program (version 2.0), applying a Bayesianapproach. It estimates how alleles from different polymorphisms in linkagedisequilibrium coexist on the same chromosome. The approach also estimatesthe uncertainty for each inferred haplotype [37]. Only common haplotypes withfrequency above 5% were considered separately in the analyses, the more rarehaplotypes were grouped as “other haplotypes”.
Assessment of genetic effectsWe assessed the impact of genetic factors on phenotype with mixed models;
treating study as the random factor [38]. Gender was a fixed factor in theseanalyses. Both single SNP analyses and haplotype-based analyses wereperformed. For each of the five polymorphisms marginal differences in theBMD across different genotypes were calculated. Corresponding mixed modelswere used for fracture data. We relied on a likelihood ratio test to assess whethera regression model taking into account the genetic factors provided better fit(explained data better) than a constant only model.
Because of Mendelian randomization, there is no apparent reason to accountfor potential confounders [39]. Thus, main analyses were unadjusted. Moreover,there is no strong biological plausibility in favour of a specific genetic model.
copy for the five SNPs. The results are presented for the individual studies and in

Table 2Differences in adjusted BMD values per haplotype allele copy for comparisons involving haplotype alleles estimated from the G−1639-A, C−1348-T, T29-C and G74-Cpolymorphisms
Difference in estimated means of BMD in mg/cm2 (95% CI)
Lumbar spine P-value comparing haplotypes P-value overall Femoral neck P-value comparing haplotypes P-value overall
Haplotype allele 1 (GCTG) Reference 0.58 Reference 0.72Haplotype allele 2 (GTCG) −2 (−6 to 3) 0.40 0 (−3 to 4) 0.87Haplotype allele 3 (ACTG) 1 (−6 to 8) 0.74 3 (−3 to 8) 0.33Haplotype allele 4 (GCCC) −2 (−10 to 6) 0.65 0 (−6 to 6) 0.97Other haplotype alleles 9 (−6 to 24) 0.22 6 (−5 to 17) 0.28
BMD, bone mineral density, CI: confidence interval.The table may be used to calculate all pairwise comparisons (as in Table 1) by subtracting the presented differences, e.g. the comparison of haplotype allele 2 versushaplotype allele 3 has a BMD lumbar spine difference of (−2)−1=3 mg/cm2.Values are derived from mixed-effects model (random effects for study and fixed effects for genotype) and adjusted for age, weight and height for males andadditionally for menopausal status and hormone use in females. P-values take into account all haplotype pairs and do not adjust for multiple comparisons.For all effects, comparison between female and male shows no statistically significant differences (pN0.10 for all).
976 B.L. Langdahl et al. / Bone 42 (2008) 969–981
For BMD measurements, main analyses used a “model-free” approach thatconsiders the three genotypes as independent factors. For fracture data, allele-based contrasts were selected, in symmetry with previous GENOMOS reports[24]. Additional analyses used the dominant model and allele-based contrasts forBMD measurements, and the dominant model for fractures. Only the two mostcommon polymorphisms (C−1348-T and T29-C) were assessed with a recessivemodel (data not shown).
Secondary analyses for single TGFB1 polymorphisms adjusted for age,height and weight (as continuous variables). Whenever statistically significantgenetic effects were identified, additional adjustments for postmenopausal status(yes versus no) and use of hormone replacement therapy (yes versus no) amongfemales were undertaken.
Fig. 4. Unadjusted OR for fracture per variant allele copy. The results are presentedsummary OR and 95% CI.
Unadjusted and adjusted differences in the BMD and the unadjusted andadjusted odds ratios for fractures for the various genetic contrasts were calculatedfor each study-gender stratum and synthesized across studies with generalvariance fixed and random effects models [38]. Fixed effects models assume asingle “truth” for the pertinent genetic effects across the participating studies.Random effects models allow for between-study heterogeneity and incorporate itin the calculations. In the absence of heterogeneity, estimates from both modelscoincide. Random effects models are preferable when heterogeneity exists [40].We tested for between study heterogeneity with Cochran's Q and quantified itsextent with I2 [39].
Analyses were performed using SPSS 12.0 (SPSS, Inc., Chicago, IL),Intercooled Stata 8.2 (Stata Corporation, College Station, TX), PHASE 2.0, and
for the individual studies and in men and women separately, as random effect

Table 3Random effects (DerSimonian and Laird) odds ratios (95% confidence intervals) for fracture risk by TGFβ1 genotype with per allele (rare) model
Participants All fractures Vertebral Incident Incident vertebral Low/no trauma
G−1639-A All 1.05 (0.97–1.14) 1.08 (0.95–1.23) 1.02 (0.90–1.15) 0.96 (0.74–1.25) 1.05 (0.95–1.15)Women 1.04 (0.96–1.14) 1.01 (0.86–1.20) 1.03 (0.91–1.18) 0.91 (0.67–1.24) 1.02 (0.91–1.14)Men 1.08 (0.92–1.28) 1.28 (1.01–1.63)⁎ 0.88 (0.60–1.29 1.12 (0.68–1.85) 1.13 (0.94–1.35)
C−1348-T All 1.00 (0.96–1.05) 1.02 (0.94–1.10) 1.02 (0.95–1.10) 1.09 (0.93–1.27 0.98 (0.92–1.04)Female 0.99 (0.94–1.05) 1.00 (0.91–1.09) 1.01 (0.92–1.10) 1.05 (0.87–1.26) 0.97 (0.91–1.04)Male 1.03 (0.94–1.13) 1.07 (0.92–1.24) 1.07 (0.90–1.28) 1.24 (0.82–1.88) 0.95 (0.81–1.13)
T29-C All 1.00 (0.95–1.04) 1.00 (0.92–1.07) 1.02 (0.95–1.10) 0.98 (0.83–1.16) 0.98 (0.92–1.04)Female 0.98 (0.93–1.04) 0.96 (0.88–1.05) 1.03 (0.95–1.12) 0.91 (0.76–1.09) 0.98 (0.91–1.04)Male 1.04 (0.95–1.14) 1.09 (0.94–1.25) 1.05 (0.81–1.35) 1.24 (0.84–1.83) 0.93 (0.79–1.10)#
G74-C All 1.01 (0.93–1.10) 0.96 (0.83–1.10) 0.99 (0.83–1.18) 0.93 (0.53–1.64)# 0.99 (0.87–1.13)Female 0.99 (0.90–1.09) 0.87 (0.73–1.03) 1.09 (0.94–1.25) 0.68 (0.45–1.04) 0.95 (0.82–1.09)Male 1.08 (0.90–1.28) 1.16 (0.91–1.48) 0.84 (0.51–1.37 1.32 (0.48–3.59)# 1.10 (0.86–1.41)
C788-T All 1.05 (0.91–1.20) 1.12 (0.91–1.37) 1.11 (0.70–1.76) 1.64 (1.09–2.64)⁎ 0.89 (0.73–1.08)Female 1.05 (0.88–1.26) 1.03 (0.81–1.31) 0.98 (0.66–1.47) 1.60 (0.98–2.62) 0.92 (0.69–1.22)Male 1.03 (0.78–1.35) 1.38 (0.94–2.02) 1.05 (0.72–1.53) 1.74 (0.81–3.73) 0.81 (0.58–1.14)
Data from all 10 studies are included for all fractures and for vertebral fractures; data for incident fractures are derived from 4 studies and data for low/no traumafractures are derived from 8 studies (see Methods for details). There is no adjustment for covariates.⁎pb0.05.#Significant between study heterogeneity with 0.10NpN0.01.Between study heterogeneity with pb0.01 was not seen for any comparison and comparison of female versus male summary estimates always showed non-significantdifferences (pN0.01 for all). In the presence of significant between study heterogeneity I2 was 60% adn 73% for the G74-C polymorphism with respect to incidentvertebral fractures in all participants and men, respectively. I2 was 47% for the T29-C polymorphism with respect to low-trauma fractures in men.
Fig. 5. Unadjusted OR for incident vertebral fractures per variant allele copy ofthe C788-T polymorphism. The results are presented for the individual studiesand in men and women separately, as summary random effects OR and 95% CI.
977B.L. Langdahl et al. / Bone 42 (2008) 969–981
GENEPOP (http://wbiomed.curtin.edu.au/genepop/). All reported P-values aretwo-tailed and we have not adjusted them for multiple comparisons.
Results
Database
We gathered data on 28,924 participants (20,878 women) and26,597 participants were analyzed (19,404 women) afterselecting only one participant for each FAMOS pedigree. Ofthe 26,597 participants, data on lumbar spine BMD, femoralneck BMD, all fractures, and vertebral fractures existed on19,299, 19,383, 25,861, and 20,673 participants, respectively.There were 6536 participants with fracture, 2126 with vertebralfractures, 2407 with incident fractures (412 had incidentvertebral fractures), and 3918 with low/no-trauma fractures.Genotype information on G−1639-A, C−1348-T, T29-C, G74-Cand C788-Twas available in 22,230, 22,625, 22,086, 22,132, and22,803 individuals, respectively. Information on all five SNPswas available in 20,612 individuals. Genotype and haplotypefrequencies were similar across the 10 participating studiesalthough in FLOS the T−1348 allele and the C29 allele were 1.5–2fold higher (Table 1). All datasets were in Hardy–Weinbergequilibrium, except for DOPS (for T29-C), ERGO (for C−1348-T,C788-T), EPOS (for G74-C, C788-T), FLOS (for C−1348-T, T29-C,G74-C) and LASA (for G74-C). Exclusion of these data did notaffect summary estimates or conclusions (not shown).
BMD analyses
Overall, there were no substantial differences in BMD be-tween the three genotypic groups of homozygotes for eachallele or heterozygotes. The marginal overall differences in theBMD, both in the adjusted and in the unadjusted analyses were
rather small for all contrasts between genotypes (less than 6 mg/cm2). Results were consistent across female and male par-ticipants. After adjustment for age, height, weight, as well ashormone use and menopausal status for women (Figs. 2 and 3)the difference in lumbar spine BMD between men with thenormal genotype CC and men carrying the variant T alleleat the C−1348-T polymorphism was −12 mg/cm2 (−23 to −1),pb0.05. No significant differences were found at the hip, for anyof the four other polymorphisms in men or for any of thepolymorphisms in women. Comparisons of the four haplotypeswith frequencies more than 5% (Table 2) showed that haplotypeswere not significantly associated with differences in BMD.Compared to the most prevalent haplotype (GCTG) lumbar spineand femoral neck BMD differences were smaller than 10 mg/cm2
overall, in adjusted analyses for both genders. The corresponding

Table 4Random (mixed) effects logistic regression analyses
All fractures Vertebral Incident Incident vertebral Low/no trauma
Haplotype allele 1: GCTGHaplotype allele 2: GTCG 0.96 (0.87–1.05) 1.00 (0.89–1.12) 1.18 (0.92–1.49) 1.01 (0.79–1.29) 0.89 (0.80–0.99)⁎
Haplotype allele 3: ACTG 1.02 (0.88–1.19) 1.12 (0.93–1.35) 0.73 (0.47–1.13) 0.93 (0.62–1.40) 0.97 (0.81–1.15)Haplotype allele 4: GCCC 1.02 (0.86–1.21) 1.09 (0.89–1.34) 0.87 (0.57–1.33) 0.76 (0.49–1.20) 0.95 (0.78–1.15)Other haplotype alleles 1.10 (0.83–1.45) 0.66 (0.40–1.08) 3.62 (1.10–11.88)⁎ No data 0.76 (0.51–1.11)P-value 0.75 0.31 0.052 0.82 0.22
Data from all 10 studies are included for all fractures and for vertebral fractures; data for incident fractures are derived from 4 studies and data for low/no traumafractures are derived from 8 studies (see Methods for details).Odds ratios (95% confidence intervals) for fracture risk by TGFβ1 haplotypes.⁎pb0.05 versus haplotype 1.
978 B.L. Langdahl et al. / Bone 42 (2008) 969–981
differences were less than 10 mg/cm2 among females and lessthan 13 mg/cm2 among males (Table 2).
Fracture analyses
For all alleles of interest, when all fractures were considered(Fig. 4), the point estimates of the ORs were closed to 1.00(range, 0.91–1.20). The 95% CIs excluded more than 20%differences in the odds of fractures between carriers and non-carriers of the rare alleles. For vertebral fractures, the odds ratiofor fracture in men carrying the variant A-allele of the G−1639-Apolymorphism increased by 28% (OR=1.28 (95% CI, 1.01–1.63%) (Table 3). This increased risk of vertebral fractures wasnot observed in women. Furthermore, none of the other fourpolymorphisms affected risk of vertebral fractures. In a subsetof the participating studies, information on incident vertebralfractures has been collected, prospectively. Carriers of the T-allele of the C788-T polymorphism had 74% higher odds ratiofor incident vertebral fractures when both genders wereconsidered together (OR=1.74 (95% CI, 1.09–2.64). The sex-specific analyses showed statistically non-significant effects ofsimilar magnitude, with odds ratios of 1.60 and 1.64 for menand women, respectively (Fig. 5). Risk of incident vertebralfractures was not influenced by any of the other fourpolymorphisms. Risk of all incident fractures and low traumafractures was not affected by the polymorphisms.
Adjustment for age (as well as gender, height and weight) didnot change any of the summary estimates for fracture risk.Interaction terms between age or study and genotype were notformally significant for any of the main outcomes and did notimprove model fit. Different studies used very different scalesfor physical activity or ability, but genetic effects were similarwhen adjusted for physical activity or ability per cohort.
Considering the haplotypes that could be estimated from thefour polymorphisms in the promoter and first exon we found noconvincing effect on the risk of all fractures, incident fractures,vertebral fractures, incident vertebral fractures or low traumafractures (Table 4).
Discussion
In this large-scale study, we obtained some evidence of aneffect of the C788-T polymorphism in the TGFB1 gene onvertebral fracture risk and of the C−1348-T polymorphism on
BMD in men. The C788-T polymorphism has not previouslybeen found to be associated with any bone phenotype, whereasthe C−1348-T has been associated with serum levels of TGFβ1and BMD. For the G−1639-A, T29-C and the G74-C, we found noconvincing effect on BMD or fracture risk. This is contradictoryto the findings of previous smaller studies, which showed thatthe T29-C polymorphism is associated with changes in BMDand fracture risk. However, the very large sample size allows fortight CIs that exclude even small differences between genotypesand haplotype pairs.
The C788-T polymorphism is very rare with a MAF of 2–3%and only 5.4% of participants were carriers of the T-allele. Only412 individuals had incident vertebral fractures. This makes theestimates of risk of fracture for this rare variant less certain,which is also reflected in the relatively wide confidence intervalsof the odds ratios. On the other hand, incident vertebral fractureswere a pre-defined event, documented by spinal radiography andthe estimated increased risk was approximately 70% and similarin both women and men. This polymorphism changes the 263rdamino acid fromThreonine to Isoleucine and is located in an areaof the gene that is highly conserved among species, however, thepossible effect on functionality of TGFβ1 has not been ex-amined so far.
The C−1348-T polymorphism is more common with MAF of29%, and 52.7% of the participants being carriers of the T-allele.The T-allele was associated with decreased BMD at the lumbarspine in men. Previously, this polymorphism has been demon-strated to be significantly associated with plasma concentration ofTGFβ1 in a UK population, explaining 8.2% of the additivegenetic variation in TGFβ1 concentration. Individuals with the T-allele had higher levels of TGFβ1 and this increase was morepronounced among individuals homozygous for T than in hete-rozygotes, in agreement with a dose-response effect of the T-allele[41]. The same trend was found in a Japanese study although thedifferences did not reach statistical significance [15]. Further-more, Luedecking et al. demonstrated that the T-allele had sig-nificantly higher transcriptional activity in a luciferase reporterassay in COS-1 cells [12]. Previous studies on the effect of thispolymorphism on BMD have found contradictory results; theT-allele of the C−1348-T polymorphism was associated with re-duced BMD in postmenopausal Japanese women [15], whereasthe same allele, was associated with higher BMD in Danish menandwomen [9] and higher heel ultrasound stiffness index in youngCanadian women [42]. The results obtained in the present study

979B.L. Langdahl et al. / Bone 42 (2008) 969–981
are in opposite direction to what would be expected from thefunctionality studies of this polymorphism. However, a very largenumber of polymorphisms in the human genome are likely to havefunctional effects at the molecular level, but few have subse-quently been tested and found to be related to specific outcomes.Therefore, epidemiological and functional data provide indepen-dent lines of evidence for an effect of a specific genetic variationon a phenotype or disease [43]. Even though we followed a pre-determined analysis plan, these findingsmay still represent chancefindings, given the very large number of analyses.
We found no effect on BMD or fracture risk of the twopolymorphisms in exon 1, T29-C and G74-C. Previous studies ofthe functionality of the T29-C (Leu10Pro) polymorphism havebeen inconclusive. The T29-allele is being associated with re-duced serum levels of TGFβ1 in one study [16], but withincreased serum levels in another [20]. In previous clinicalstudies, the T29-allele was associated with reduced BMD at thelumbar spine and vertebral fractures in Japanese and Danishpopulations [9,16–19,44], but with increased BMD in Germanand Australian populations [20]. The previous studies hadlimited statistical power and it is most likely that the reportedfindings were chance findings. Based on results of the presentstudy, it can be concluded that the T29-C polymorphism does notaffect BMD or fracture risk in European populations.
In this study, there was no convincing effect of haplotypes onBMD and fracture risk. This is in agreement with a previousDanish study [9], whereas in a Japanese population interactionbetween the T29-C and C−1348-T polymorphisms was demon-strated [15].
This investigation has several strengths, but also a numberof limitations. The strengths of our study include the very largesample size, cross-validation of the genotyping techniques, inter-national collaboration and lack of publication bias within theconsortium. The limitations include the fact that different groupsused different definitions for fracture and that some of the fractureevents were not validated but based on patient reports which areprone to error and recall bias. This could introduce some un-avoidable heterogeneity in the analyses, but it is unlikely that thiswould result in bias in distribution of fractures according to anyspecific genotype. It is also important to emphasise that many ofthe fractures recorded in this study are not related to osteoporosis,since the majority of fractures that occur in the general populationaffect people who do not fulfill the WHO definition of oste-oporosis [45]. However, we performed sensitivity analyses thattargeted only incident fractures, incident vertebral fractures andlow/no trauma fractures and found similar results. Reassuringly,we found similar results. Another potential limitation is due tomissing data in some cohorts. In particular not all participants hadBMD measurements. However, participants and their physiciansmade the decision to measure BMD without any knowledge ofgenotype data. We therefore presume lack of BMD data to begenotype-independent.Wewere able to perform the analyses afteradjustment for height, weight, menopause and HRT and theresults were similar in unadjusted and adjusted analyses. Manyother parameters may affect the risk of fractures. However, it canbe expected that exposure to these risk factors is unrelated to thedifferent TGFB1 genotypes.
In conclusion, none of the five TGFB1 polymorphisms andhaplotypes thereof was generally associated with BMD orfracture risk. The isolated effects of C−1348-T (C−509-T) onlumbar spine BMD in men and of C788-T (Thr263Ile) on risk ofincident vertebral fractures may be chance findings andwill needreplication. Furthermore, with the strong evidence provided thatthe T29-C polymorphisms does not affect BMD or fracture risk,our study demonstrates the important contribution that large-scale studies with standardized genotyping and phenotypemeasurements combined with predefined plans of analyses canprovide to the understanding of complex genetic diseases, suchas osteoporosis.
Sources of funding
The European Commission supported this study under grantQLK6-CT-2002-02629. The funding organization had no rolein the design and conduct of the study; collection, management,analysis, and interpretation of the data; and preparation, reviewor approval of the manuscript.
The EPOS study was financially supported by a Eu-ropean Union Concerted Action Grant under Biomed-1(BMH1CT920182), and also EU grants C1PDCT925102,ERBC1PDCT 930105 and 940229. The central coordinationwas also supported by the UK Arthritis Research Campaign, theMedical Research Council (G9321536), and the EuropeanFoundation for Osteoporosis and Bone Disease. The EU'sPECO program linked to BIOMED 1 funded in part theparticipation of the Budapest, Prague, Piestany, Szczecin andMoscow centers. Data collection from Zagreb was supported bya grant from the Wellcome Trust. The central X-ray evaluationwas generously sponsored by the Bundesministerium furForschung and Technologie, Germany. The remaining fundingwas provided by or through the following centers: RadiologicalEvaluation: Department of Radiology and Nuclear Medicine,Free University, Berlin, Germany (DF, WG, GA); ParticipatingInvestigative Centers: Institute of Rheumatology, Moscow,Russia (LI Benevolenskaya); Royal National Hospital forRheumatic Diseases, Bath, U.K (A Bhalla); Hospital de Angrado Herismo, Azores, Portugal (J Bruges Armas); AsturiasGeneral Hospital, Oviedo, Spain (J B Cannata Andia andManuel Naves Diaz); University Hospital, Leuven, Belgium (SBoonen); Charles University, Prague, Czech Republic (J JStepan); Zagreb, Croatia (I Jajic); Hospital de San Joao, Oporto,Portugal (A Lopes Vaz); University of Athens, Greece (GLyritis); Institute of Rheumatic Diseases, Piestany, Slovakia (PMasaryk); Academy of Medicine, Szczecin, Poland (T Miaz-gowski); University of Siena, Italy (RNuti); National Institute ofRheumatology and Physiotherapy, Budapest, Hungary (G Poor);University Hospital, Graz, Austria (K Weber).
The Longitudinal Aging Study Amsterdam (LASA) isfunded by the Ministry of Health, Welfare and Sports of TheNetherlands.
The Rotterdam study (ERGO) is supported by the ErasmusMedical Center and Erasmus University, Rotterdam. The Nether-lands Organization for scientific research (NWO), the Nether-lands Organization for the Health Research and Development

980 B.L. Langdahl et al. / Bone 42 (2008) 969–981
(ZonMw), the Research Institute for Diseases in the Elderly(RIDE), the Ministry of Education, Culture and Science, theMinistry for Health, Welfare and Sports, the European Commis-sion (DG XII), and the Municipality of Rotterdam.
Potential financial conflicts
All authors have no conflicts of interest.
References
[1] Bonewald LF, Mundy GR. Role of transforming growth factor-beta inbone remodeling. Clin Orthop 1990;250:261–76.
[2] Pfeilschifter J, D'Souza SM, Mundy GR. Effects of transforminggrowth factor-beta on osteoblastic osteosarcoma cells. Endocrinology1987;121(1):212–8.
[3] Chenu C, Pfeilschifter J, Mundy GR, Roodman GD. Transforming growthfactor beta inhibits formation of osteoclast-like cells in long-term humanmarrow cultures. Proc Natl Acad Sci U S A 1988;85(15):5683–7.
[4] Geiser AG, Zeng QQ, Sato M, Helvering LM, Hirano T, Turner CH.Decreased bone mass and bone elasticity in mice lacking the transforminggrowth factor-beta1 gene. Bone 1998;23(2):87–93.
[5] Janssens K, Gershoni-Baruch R, Guanabens N, et al. Mutations in the geneencoding the latency-associated peptide of TGF-beta1 cause Camurati–Engelmann disease [in process citation]. Nat Genet 2000;26(3):273–5.
[6] Kinoshita A, Saito T, Tomita H, et al. Domain-specific mutations inTGFB1 result in Camurati–Engelmann disease. Nat Genet 2000;26(1):19–20.
[7] Janssens K, Vanhoenacker F, Bonduelle M, et al. Camurati–Engelmanndisease: review of the clinical, radiological, and molecular data of24 families and implications for diagnosis and treatment. J Med Genet2006;43(1):1–11.
[8] Wu S, Liang S, Yan Y, et al. A novel mutation of TGF beta1 in a Chinesefamily with Camurati–Engelmann disease. Bone 2007;40(6):1630–4.
[9] Langdahl BL, Carstens M, Stenkjaer L, Eriksen EF. Polymorphisms in thetransforming growth factor beta1 gene and osteoporosis. Bone 2003;32(3):297–310.
[10] Cambien F, Ricard S, Troesch A, et al. Polymorphisms of the transforminggrowth factor-beta 1 gene in relation to myocardial infarction and bloodpressure. The Etude Cas-Temoin de l'Infarctus du Myocarde (ECTIM)Study [see comments]. Hypertension 1996;28(5):881–7.
[11] Awad MR, El Gamel A, Hasleton P, Turner DM, Sinnott PJ, HutchinsonIV. Genotypic variation in the transforming growth factor-beta1 gene:association with transforming growth factor-beta1 production, fibroticlung disease, and graft fibrosis after lung transplantation. Transplantation1998;66(8):1014–20.
[12] Luedecking EK, DeKosky ST, Mehdi H, Ganguli M, Kamboh MI.Analysis of genetic polymorphisms in the transforming growth factor-beta1 gene and the risk of Alzheimer's disease. Hum Genet 2000;106(5):565–9.
[13] McGowan NW, MacPherson H, Janssens K, et al. A mutation affectingthe latency-associated peptide of TGFbeta1 in Camurati–Engelmanndisease enhances osteoclast formation in vitro. J Clin Endocrinol Metab2003;88(7):3321–6.
[14] Hernandez MV, Peris P, Guanabens N, et al. Biochemical markers of boneturnover in Camurati–Engelmann disease: a report on four cases in onefamily. Calcif Tissue Int 1997;61(1):48–51.
[15] Yamada Y, Miyauchi A, Takagi Y, Tanaka M, Mizuno M, Harada A.Association of the C-509–NT polymorphism, alone of in combinationwith the T869–NC polymorphism, of the transforming growth factor-beta1 gene with bone mineral density and genetic susceptibility toosteoporosis in Japanese women. J Mol Med 2001;79(2–3):149–56.
[16] Yamada Y, Miyauchi A, Goto J, et al. Association of a polymorphism ofthe transforming growth factor-beta1 gene with genetic susceptibility toosteoporosis in postmenopausal Japanese women. J Bone Miner Res1998;13(10):1569–76.
[17] Yamada Y, Ando F, Niino N, Shimokata H. Transforming growth factor-beta1 gene polymorphism and bone mineral density. JAMA 2001;285(2):167–8.
[18] Yamada Y, Miyauchi A, Takagi Y, et al. Association of a polymorphism ofthe transforming growth factor beta-1 gene with prevalent vertebralfractures in Japanese women. Am J Med 2000;109(3):244–7.
[19] Yamada Y, Hosoi T, Makimoto F, Tanaka H, Seino Y, Ikeda K.Transforming growth factor beta-1 gene polymorphism and bone mineraldensity in Japanese adolescents. Am J Med 1999;106(4):477–9.
[20] Hinke V, Seck T, Clanget C, Scheidt-Nave C, Ziegler R, Pfeilschifter J.Association of transforming growth factor-beta1 (TGFbeta1) T29–NCgene polymorphism with bone mineral density (BMD), changes inBMD, and serum concentrations of TGF-beta1 in a population-basedsample of postmenopausal German women. Calcif Tissue Int 2001;69(6):315–20.
[21] Dick IM, Devine A, Li S, Dhaliwal SS, Prince RL. The T869C TGF betapolymorphism is associatedwith fracture, bonemineral density, and calcanealquantitative ultrasound in elderly women. Bone 2003;33(3): 335–41.
[22] Ioannidis JP, Ralston SH, Bennett ST, et al. Differential genetic effects ofESR1 gene polymorphisms on osteoporosis outcomes. JAMA 2004;292(17):2105–14.
[23] Ralston SH, Uitterlinden AG, Brandi ML, et al. Large-scale evidence forthe effect of the COLIA1 Sp1 polymorphism on osteoporosis outcomes:the GENOMOS study. PLoS Med 2006;3(4):e90.
[24] Uitterlinden AG, Ralston SH, Brandi ML, et al. The association betweencommon vitaminD receptor gene variations and osteoporosis: a participant-level meta-analysis. Ann Intern Med 2006;145(4):255–64.
[25] Torgerson DJ, Thomas RE, Campbell MK, Reid DM. Randomized trial ofosteoporosis screening. Use of hormone replacement therapy and quality-of-life results. Arch Intern Med 1997;157(18):2121–5.
[26] Pluijm SM, van Essen HW, Bravenboer N, et al. Collagen type I alpha1Sp1 polymorphism, osteoporosis, and intervertebral disc degeneration inolder men and women. Ann Rheum Dis 2004;63(1):71–7.
[27] Mosekilde L, Hermann AP, Beck-Nielsen H, Charles P, Nielsen SP,Sorensen OH. The Danish Osteoporosis Prevention Study (DOPS): projectdesign and inclusion of 2000 normal perimenopausal women. Maturitas1999;31(3):207–19.
[28] Ismail AA, O'Neill TW, Cooper C, et al. Mortality associated with vertebraldeformity in men and women: results from the European ProspectiveOsteoporosis Study (EPOS). Osteoporos Int 1998;8(3): 291–7.
[29] Burger H, De Laet CE, van Daele PL, et al. Risk factors for increased boneloss in an elderly population: the Rotterdam Study. Am J Epidemiol1998;147(9):871–9.
[30] Langdahl BL, Carstens M, Stenkjaer L, Eriksen EF. Polymorphisms in theosteoprotegerin gene are associated with osteoporotic fractures. J BoneMiner Res 2002;17(7):1245–55.
[31] Garcia-Giralt N, Nogues X, Enjuanes A, et al. Two new single-nucleotidepolymorphisms in the COL1A1 upstream regulatory region and theirrelationship to bone mineral density. J Bone Miner Res 2002;17(3): 384–93.
[32] Obermayer-Pietsch BM, Bonelli CM, Walter DE, et al. Genetic predisposi-tion for adult lactose intolerance and relation to diet, bone density, and bonefractures. J Bone Miner Res 2004;19(1):42–7.
[33] Ralston SH, Galway N, MacKay I, et al. Loci for regulation of bonemineral density in men and women identified by genome wide linkagescan: the FAMOS study. Hum Mol Genet 2005;14(7).
[34] McCloskey EV, Spector TD, Eyres KS, et al. The assessment of vertebraldeformity: a method for use in population studies and clinical trials.Osteoporos Int 1993;3(3):138–47.
[35] Reid DM, MacKay I, Wilkinson S, et al. Cross-calibration of dual-energyX-ray densitometers for a large, multi-center genetic study of osteoporosis.Osteoporos Int 2006;17(1):125–32.
[36] Rousset F, Raymond M. Testing heterozygote excess and deficiency.Genetics 1995;140(4):1413–9.
[37] Stephens M, Donnelly P. A comparison of Bayesian methods forhaplotype reconstruction from population genotype data. Am J Hum Genet2003;73(5):1162–9.
[38] McCullochCE, Searle SR.Generalised, linear andmixedmodels. 2001.WileySeries in Probability and Statistics. Ref Type: Serial (Book,Monograph).

981B.L. Langdahl et al. / Bone 42 (2008) 969–981
[39] Davey SG, Ebrahim S. qMendelian randomizationq: can genetic epide-miology contribute to understanding environmental determinants of disease?Int J Epidemiol 2003;32(1):1–22.
[40] DerSimonian R, Laird N. Meta-analysis in clinical trials. Control ClinTrials 1986;7(3):177–88.
[41] Grainger DJ, Heathcote K, Chiano M, et al. Genetic control of thecirculating concentration of transforming growth factor type beta1. HumMol Genet 1999;8(1):93–7.
[42] Tzakas P, Wong BY, Logan AG, Rubin LA, Cole DE. Transforminggrowth factor beta-1 (TGFB1) and peak bone mass: association between
intragenic polymorphisms and quantitative ultrasound of the heel. BMCMusculoskelet Disord 2005;6:29.
[43] Rebbeck TR, Spitz M, Wu X. Assessing the function of genetic variants incandidate gene association studies. Nat Rev Genet 2004;5(8):589–97.
[44] Yamada Y, Harada A, Hosoi T, et al. Association of transforming growthfactor beta1 genotype with therapeutic response to active vitamin D forpostmenopausal osteoporosis. J Bone Miner Res 2000;15(3):415–20.
[45] Schuit SC, van der KM, Weel AE, et al. Fracture incidence and associationwith bone mineral density in elderly men and women: the RotterdamStudy. Bone 2004;34(1):195–202.