Embed Size (px)
Citation preview

Lateral flow antigen tests and
diagnosis of import mycoses
Katrien Lagrou, PharmD, PhD
University Hospitals Leuven and KU Leuven, BELGIUM

Co
nve
ntio
na
l Te
sts Histopathology
Direct Microscopy
Culture
Mass Spectrometry (MALDI-TOF)
Susceptibility testing
An
tige
n/A
ntibo
dyl/D
NA
Antigen detection
Galactomannan (GM)
1,3 β-D-glucan (BDG)
Lateral Flow Assays (LFA)
PCR
Which tests can the lab offer to you?
Antibody detection

Co
nve
ntio
na
l Te
sts Histopathology
Direct Microscopy
Culture
Mass Spectrometry (MALDI-TOF)
Susceptibility testing
An
tige
n/A
ntibo
dy/D
NA
Antigen detection
Galactomannan (GM)
1,3 β-D-glucan (BDG)
Lateral Flow Assays (LFA)
PCR
Which tests can the lab offer to you?
Antibody detection
Diagnosis of
cryptococcosis and
aspergillosis



• Cryptococcus neoformans var grubii (serotype A),
affects mainly immunocompromised individuals
• Cryptococcus neoformans var neoformans
(serotype D)
• Cryptococcus gattii (serotype B and C), causes
disease mainly in apparently healthy individuals
The pathogen
• Cryptococcus neoformans species complex
• Cryptococcus gattii species complex
OR

• Antigen: the major capsular polysaccharide glucuronoxylomannan
(shed during infection)
• Detection in serum/CSF
• Latex-agglutination/Lateral flow assay
• “One of the most useful serologic tests in mycology”
Cryptococcus antigen detection

• Correlation between antigen and number of yeast cells
• Highly sensitive and specific
– False positive results possible in serum by rheumatoid factor or in
case of infection with Trichosporon asahii
– False negatives:
• Prozone effect
• Organism load is low or organisms not well encapsulated
Detecting cryptococcal antigen in CSF or serum is rapid,
specific, and virtually diagnostic of meningo-encephalitic
or disseminated cryptococcosis.
Cryptococcal antigen test

LFA for Cryptococcal antigen
• Dipstick format
• Glucuronoxylomannan (GXM) has variable levels of O-
acetylation that contribute to serotype specificity
• CrAg LFA high sensitivity for GXM for the four serotypes as
follows A=B>C=D
• Stable at room temperature, costs about 2 $/strip in low-
income countries
• Can not be used to monitor treatment response, clearance of
the cryptococcal capsule polysaccharide by macrophages is
an independent and slower process than killing of the yeast
by antifungal therapy
• More sensitive than culture and latex agglutination

M. A. Gates-Hollingsworth and T.R. Kozel, CVI, 2013, 20: 634-635

LFA provides prognostic value
High correlation between log10 CFU and log2 LFA titers on day 1
T. Kabanda et al. CID 2014, 58: 113-116.
Samples were collected
as part of 2 prospective
cohorts in Uganda

Pre-emptive treatment of cryptococcosis
Window of a median of 22 days during which cryptococcal antigen can be
detected in serum but patients have not yet developed symptoms and clinical
disease
= asymptomatic cryptococcal antigenemia
= independent predictor of mortality in patients initiating ART

Screening recommendation may need expansion to ≤ 200 cells/µL to maximize detection of
patients in whom fluconazole pre-emptive therapy may be life-saving (or only in
combination with certain symptoms?)
KA Magambo et al, JIAS, 2014, 14: 19040

• Murine MAb JF5: IgG3 immunoglobulin
• Recognizes an extracellular, constitutive, glycoprotein antigen
• Antigen is secreted during active growth of hyphae and is not produced by dead
or quiescent spores
• Displays superior specificity to rat MAb EB-A2 (Bio-Rad Platelia GM-EIA)
• Used to develop a rapid, user-friendly, diagnostic test for detection of IA
Thornton CR. Clin Vaccine Immunol. 2008 Jul;15(7):1095-105
The lateral flow device: a point-of-care test
1 Cryptococcus neoformans 2 Candida albicans3 Fusarium solani4 Rhizopus oryzae5 Aspergillus fumigatus
LFA for the diagnosis of invasive aspergillosis

Monoclonal antibody: Mab JF-5
Antibody source: mouse
Step 1
Step 2
Positive reaction Negative reaction
Capillary flow
Step 3
BA
Control line Test line Control line
BA
Aspergillus lateral flow assay
Sample padCapture zone
Clinical specimen
Test line(mAb)
Control line(anti-mouse IgG)
Sample pad Sample pad
Ag No-Ag
Pretreatment of
serum samples
necessary, not of
BAL samples

Current Fungal Infection Reports (2013) 7: 244-251.
Expert Review of Clinical Immunology (2014)
Localisation of JF5 antigen

Commercialisation of the
Aspergillus LFD, when?

• 286 BAL from 221patients with underlying respiratory diseases
(without hematological malignancy or SOT)
• 14% proven/probable IPA
• 02/2012 – 05/2014, Graz, Austria
Prattes J et al. Am J Resp Crit Care Med 2014; 190: 922-929
Novel tests for diagnosis of IA in patients with
underlying respiratory disease
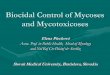
Combined assay performance for blood screening
in high risk hematology patients
Case-control design: 22 proven/probable IA versus 59 controls
White PL et al, JCM 2013, 51: 1510-1515.

Diagnosis of import mycoses:
histoplasmosis
• Pathogen:
– Histoplasma capsulatum var. capsulatum
Most common endemic mycosis in North America
Also Central and South America, Central and South Africa, Asia, Middle
East, Australia, very rare in Europe
– Histoplasma capsulatum var. duboisii
African histoplasmosis – Central and West Africa
• Thermally dimorphic
• Diagnosis
– Direct examination and histopathology of biopsies, respiratory
samples, blood and bone marrow
– Culture: 2-6 weeks incubation needed, molecular identification

Histoplasma capsulatum var. duboisii: thick-walled
yeast cells with narrow-based buds
Yeast form, narrow based buds
Histoplasma capsulatum

Histoplasma capsulatum

Diagnosis of histoplasmosis
– Antibody detection:
• Negative results may be obtained during the first month, repeat testing
• NPV is not 100%
• Immunodiffusion (M and H band: active histoplasmosis, M alone: early or
chronic histoplasmosis, test performed in ITM Antwerp) and
complement fixation tests (more sensitive but less specific)
– Antigen detection:
• Particularly useful in immunocompromised individuals with disseminated
disease
• Sensitivity is greatest with urine (95-100% in aids patients with
disseminated disease)
• Sensitivity about 75% in acute pulmonary histoplasmosis if samples are
obtained within 2 weeks after exposure
• Cross reactions with blastomycosis, paracoccidioidomycosis,
penicillinosis, less frequent in coccidioidomycosis
– Aspergillus Galactomannan may be positive in histoplasmosis

Coccidioidomycosis
• Pathogens: Coccidioides immitis and Coccidioides posadasii
• Most Southwestern US but also Central and South America
• Diagnosis:
– Direct examination/histopathology
– Culture: fast growing in 3-5 days, white – gray to buff
– Antibody detection: CF and ID
• ID:
– with heated coccidioidin as antigen, detects IgM, present in 75% of
patients within 1 week after the onset of symptoms and 90% within 3
weeks
– unheated: detects IgG antibodies, 2-6 weeks after onset of
symptoms
• CF: IgG antibodies, 4-12 weeks after infections, more sensitive but less
specific than the ID test
– Antigen test: sensitivity highest in urine (about 70% in severe cases),
cross reaction with histoplasmosis, blastomycosis and
paracoccidioidomycosis

Coccidioides immitis
D.Wilmes et al, Case report in preparation

Blastomycosis
• Pathogen: Blastomyces dermatitidis
• North-America, sporadic cases in Central America, South
America, the Middle East, Asia, Poland, Italy, …
• Diagnosis:
– Direct examination and histopathology: unipolar budding on a broad
base with a thick wall, free or in giant cells
– Culture: incubate up to 4 weeks, white-brown cottony colonies
– Antibody detection: CF (lacks specificity) and ID (specific and
diagnostic but negative in 10% of patients with disseminated disease
and 60% of localized infections)
– Antigen detection: highest sensitivity in urine, cross reaction with
histoplasmosis, paracoccidioidomycosis, penicillinosis and less
frequently coccidioidomycosis

Blastomyces dermatitidis
Mycology online
Yeasts: large, with broad-budding

• http://miravistalabs.com/

Diagnosis of endemic mycosis:
general considerations
• Also immunocompetent patients may develop disease
(large inoculum)
• BSL-3 for propagating and manipulating sporulating cultures!
• Reversion to yeast phase is an identification criterion but
molecular techniques often provide faster results
• High level of suspicion, especially if a fungus initially grows as
a yeast (37°C) and as filamentous fungus upon subculture
(25-30°C)
• Diagnosis may be unexpected!

• Man, 61 y
• 16/05/2015: Lung transplantation for end stage COPD
• 12/09/2015: Hospitalization because of CMV reactivation
• 14/09/2015: 1 blood culture bottle with fungal hyphae
• ‘Yeast like cells’ grow the next day
• Subculture on diluted Sabouraud:
Penicillium species - a red pigment diffuses in the agar ….
BUT the patient was never in South-East Asia!
BUT the donor was!
Stayed a few weeks in Myanmar Feb 2015
My conclusion: this is most likely Penicillium marneffei
Recent case UZ Leuven
• Additional positive blood cultures on 25/09/2015, 28/09/2015,
30/09/2015 + molecular identification of the fungus as P. marneffei

Organization:
KU Leuven, Department of Microbiology & Immunology
AND
The Belgian Society for Human and Animal Mycology
In collaboration with:
Prof. dr. P.E. Verweij, UMC St. Radboud, Nijmegen,
The Netherlands
The course aims at laboratory technicians and scientists who
want to develop or expand their practical knowledge of medical
mycology. Also medical microbiologists and physicians are
welcome (a more clinically oriented 9 day mycology course
will be organized in September 2017).

Mycology Course: practical information
• 5-day course: September 5-9, 2016
• Place: at the KU Leuven Campus Gasthuisberg.
• Language of the course: The theoretical sessions will be given
simultaneously in Dutch (Dr. Ignace Surmont) and French (Prof. M.P.
Hayette). The practical sessions are supported by highly trained laboratory
technologists.
• Registration fee for the course is 1000 €. This includes the textbook
«Medically Important Fungi: A Guide to Identification, Fifth Edition» from
D. Larone, slides and lunches.
• An assessment test will be organized about 3 weeks after the course.
• The participant receives a «Certificate of medical mycology».
• Registration before 1 May 2016. Maximum 20 students are allowed (the
course was full in 2014 !)
• Registration: [email protected]