-
8/10/2019 Ld retention and relapse
1/205
Retention and relapse in orthodontics
Introduct
ion
The problem of retention and relapse was born with the science
of Orthodontics
and continues to persistently plague Orthodontic researchers and
clinicians. Most authors of
Orthodontic textbooks, from ngle to the present!day writers,
ha"e included the chapters on
retention and relapse in their publications. #n spite of all the
ad"ances in the acti"e treatment
procedures, "ery few practitioners underrate the significance of
retention. $e are yet pu%%led
how to sol"e the problem&
$ith the establishment of concept of normal occlusion and the
classification schemethat incorporated the line, by the early
'())*s orthodontics was no longer +ust the alignment
of irregular teeth, instead it had e"ol"ed into the treatment of
malocclusion. ince precisely
defined relationships re-uire a full complement of teeth in both
arches, maintaining an intact
dentition becomes an important goal of orthodontic treatment.
ngle and his followers
strongly opposed extraction for orthodontic purposes. Treatment
goal during this period was
#deal Occlusion.'
$ith the entry into 'stcentury, the goals ha"e somewhat appeared
to change. The
goal of Modern Orthodontics is creation of best balance among
occlusal relations, dental and
facial esthetics, stability of the results and its long term
maintenance and restoration of
dentition /T$0012'. ims of orthodontic treatment ha"e been
summari%ed by 3ackson as
3ackson*s triad. The three main ob+ecti"es are4
/a2 5unctional efficacy
/b2 tructural balance
/c2 0sthetic harmony
Retention is that part of orthodontic treatment during which a
passi"e appliance is
used to maintain orthodontic correction of dental and skeletal
structures and thereby
counteract relapse or the tendency for return of characteristics
to original malocclusion.
Retention was defined by Moyers6as the holding of teeth followed
by orthodontic treatment
in the treated position for the period of time necessary for the
maintenance of the results.
'
-
8/10/2019 Ld retention and relapse
2/205
Retention and relapse in orthodontics
Riedel7 defined retention as the holding of teeth in ideal
esthetic and functional
position.
Relapse may be defined as return of the corrected malocclusion
towards the original
condition.
Moyers6defined relapse as loss of any correction achie"ed by
orthodontic treatment.
The retention period has e"en been called econdary orthodontic
treatment. 8lthough it
has been stated that correct diagnosis and planning of
treatment, followed by a careful
stabili%ation of the final result, would minimi%e the importance
of retention, relapse
tendencies still exist in a fairly high percentage of cases
treated. 0"en if these precautions are
taken, howe"er, relapse after tooth mo"ement still remains a
complex problem, with a
"arying number of factors in"ol"ed.
Orthodontists ha"e been concerned by relapse process for
decades. e"eral studies
ha"e been carried out to determine the changes taking place
se"eral years after orthodontic
treatment and the influencing factors. 5actors including growth,
periodontium, age, third
molars, tooth dimensions etc ha"e been held responsible for post
treatment relapse. e"eral
procedures ha"e been de"ised to ensure stability and pre"ent or
at least a"oid post treatment
changes so as to reduce relapse. To achie"e this purpose, a
proper understanding of the
changes occurring, "arious factors affecting relapse and
retention procedures is important.
Thus our Orthodontic forefathers faced the problems of retention
and the continued
trend, which owes to the biological and mechanical limitations,
demands e"ery Orthodontic
student to go through the state of art of this perineal problem
Retention and Relapse which
also is the purpose of this library dissertation.
-
8/10/2019 Ld retention and relapse
3/205
Retention and relapse in orthodontics
Historical background 9
look back at the origins of orthodontics (Weinberger)has shown
that the necessity
of retention was not mentioned until about '( centuries after
the first treatment modality was
described and would pro"ide a clue to establishing the priority
of the esthetic needs of the
prospecti"e orthodontic patient. s Weinbergerstates, lthough
orthodontics had its origins
in medicine, it had its beginnings in aesthetics. :ikewise, the
modern well!trained clinical
orthodontist has recogni%ed that the most desirable
facial!dental esthetics may be +ust as
important as excellent posterior occlusion and good
function!possibly more so from the
standpoint of the patient*s needs. ;owe"er, there appears to be
as much contro"ersy o"er thepresent treatment methods of achie"ing
facial!dental ob+ecti"es as there was in the Case,
Dewey, Cryerextraction!nonextraction contro"ersy in '('', which
still persists three fourths
of a century later in the writings of Tweed, Ricketts, Begg, Ten
Hoeve, and Williamson.
dditional insight into the retention problem may be gained and
our present day
limitations in achie"ing predictable stability appreciated when
we learn about the anti-uity of
some of our still current modes of orthodontic treatment. #n the
beginning, says Weinberger,
people sought relief because of the disfigurement of the crooked
and irregular placed teeth9). #n that year4merson C. $ngell
(+%*),as a byproduct
of his palate!splitting procedure, mentions the necessity to
preser"e or retain space. ngell
6
-
8/10/2019 Ld retention and relapse
4/205
Retention and relapse in orthodontics
described his method of employing a +ackscrew for?rapid opening
of the maxillary median
suture or to enlarge the face in the maxillary dental arches, in
order to establish occlusion
without extraction of teeth?The time for this expansion need not
exceed two weeks, after
which it is only necessary to preser"e or retain the space until
complete eruption and
de"elopment of teeth in -uestion.
Only 8 years later in 0ngland,$l#red Coleman (+%') wrote about
restoration of the
former condition by muscular pressure!in other words, the first
illusion to relapse. More than
a century later, clinicians still refer to abnormal muscular
pressure as a dominant factor in the
cause of relapse. #n the following year, C.$. 5arvin
(+%%)described the physiologic reasons
for retention. #ndeed, he went a step further in his writing and
emphasi%ed the necessity of
the preser"ation of correct facial expression or aesthetics as
one of the ob+ecti"es of
orthodontic treatment. @ot long after, Brown5ason (+-&) (in
4ngland) described a
retaining plate for surgically rotated teeth. Thus, after more
than '( centuries of some kind of
mechanical orthodontic inter"ention, recognition of the possible
instability of treatment
emerged and the concept of a retaining appliance was born.
One of the earliest retaining appliances in the Anited tates was
described by6ames
W. 2mit/ (++) before the ;ar"ard Odontological ociety in Boston.
#t was a simple
"ulcanite plate with a bar extending o"er the labial aspect of
the maxillary incisor teeth. #n
'>>6,H.C. 7"inbeydescribed a slightly more sophisticated
maxillary retaining plate that had
strips of metal extending from the "ulcanite plate o"er the
anterior teeth.
6ackson (+*3)mentioned the importance of retention and designed
many retaining
de"ices!some permanent when necessary. lso, to pre"ent the
tendency of the teeth to change
their positions after the remo"al of the retainer, he suggested
that after they ha"e been
rotated as far as desired, the soft tissue be separated from the
neck of the tooth and allowed to
reunite in the new location, depending upon the cicatrix thus
formed to pre"ent their
retrograde mo"ement!in short fiberotomy.
$nglestated that obtaining normal occlusion /with steep cusp
height2 during the
eruption period would decrease retention time, but added that
when habits are not o"ercome
and the rotations and disturbance to the fibers of the
periodontal membrane are "ery marked,
he described cutting gingi"al fibers to counteract this in his
sixth edition publication /'())2.
;e warned that most appliances were remo"ed too soon before
teeth were thoroughly
7
-
8/10/2019 Ld retention and relapse
5/205
Retention and relapse in orthodontics
established in occlusion, and he ad"ised, #n doubtful cases,
wearing delicate and efficient
appliances indefinitely may be far less ob+ectionable than a
malocclusion.
5inally $ngle de"ised and described many ingenious mechanical
combinations of
cemented bands and spurs, the action of which were, to -uote his
uni-uely descripti"e phase,
to antagoni%e the mo"ement of teeth only on the direction of
their tendencies. lso in his
-uest for the ultimate retainers, it is interesting to note that
ngle*s intricate pin and tube
acti"e treatment appliance was de"eloped primarily as a working
retainer to achie"e bodily
mo"ement or uprighting of teeth that had been tipped outward in
expansion.
#n his article, Crinciples of Retention, Case listed the
following principles4 Cost
treatment influence of surrounding tissues would return to their
former irregular position
after retention primarily because of the more important factor
of hereditary< stretched and
bent fiber structures would be brought to e-uilibrium in their
changed positions by the
physiologic process of nature< retention should be of
ade-uate force to antagoni%e reacti"e
tendencies for relapse and held, often indefinitely by a fixed
appliance, unless teeth are
brought to positions of what he called positi"e self!fixation by
occlusion< o"er correction
and slower mo"ement of teeth< use of inconspicuous fixed
retainer, incorporation of strong
intermaxillary and "ertical elastics with chin cups to o"ercome
the reacti"e or relapsing
forces of the corrected mesial or distal occlusion as well as
open or closed bites< for retaining
diastemata of both the maxillary and mandibular anterior teeth,
gold staples were cemented
into drilled preparations in all lingual cingula, which remained
in place for more than )
years.
hundred years ago,Bonwilldescribed an ideal morphologic
arrangement of teeth
and +aws based on his study of more than ))) skulls. ;e placed
study models in anatomic
articulators, used wax set!ups of plaster teeth for extraction
decisions< and thoroughly
informed his patients on the limits of treatment and the
necessity of ade-uate retention.
8ormal 9ingsley (+*),who is referred to as the 5ather of
Orthodontia, in a letter
/his last published article2 to the alumni of the ngle chool of
Orthodontia written 8) years
after his first article appeared, had these prophetic words to
say about retention.
#t is not so difficult to straighten crooked teeth, to get the
dental system into a position
acceptable to your patients and yourself, but to hold it there
until it becomes permanently
8
-
8/10/2019 Ld retention and relapse
6/205
Retention and relapse in orthodontics
settled, is a much more serious problem. #t is the one important
consideration in all your
prognosis, and the success of orthodontia as a science and as
art lies in the DretainerE?
errar (+1+++1),also referred to as one of the fathers of
orthodontics!that is,
scientific orthodontics!the man who introduced the term
intermittent force and wrote,
according to Weinberger, the greatest text on orthodontia in his
experience, said /about
retention2 that when the teeth are fully regulated they should
be retained in position for a
year, perhaps longer.
#n summary, in the little more than one half century following
ngell*s use of a
retaining plate in his palate!splitting techni-ue, there was
general adherence to the necessity
of retention and e"en a similarity of appliances, but the
knowledge gained was based solely
on the clinical experience and obser"ation of the aforementioned
pioneer orthodontic
masters.
The next -uarter century witnessed the much needed addition of a
more scientific
dimension to the retention literature as the clinical reports of
the duration of a "ariety of
retaining appliances and the obser"ations and opinions ad"ocated
by /'2 the following
orthodontic inno"ators and clinical scholars4 Hawley (++), Ha/n
(+33), :"ndstrom
(+&), Hellman (+1%), 5ers/on (+1%), 5arc"s (+1), 5cCa"ley
(+33), Tweed (+'3),
and !rieves (+33); /2 experimentally trained research!oriented
orthodontists, 2kogborg
(+&) and
-
8/10/2019 Ld retention and relapse
7/205
Retention and relapse in orthodontics
likened the final positioning of teeth to an argument in which
mother nature always had the
last word.
Ha/n (+33),dismayed by the apparent lack of will of the ma+ority
of the profession
to study the retention problem ade-uately, obser"ed that
retention in orthodontics is like a
neglected Fstep child*.
#n another "iew, 5cCa"ley (+33) a prophet before his time,
proclaimed the
importance of canine position and referred to the canine rise as
a protecti"e mechanism for
maintaining arch stability.
Goncurrent with the abo"e!mentioned work of clinical scholars,
sgeneric statement that #f regular growth of any
H
-
8/10/2019 Ld retention and relapse
8/205
Retention and relapse in orthodontics
part of the body is interfered with by any cause, related parts
tend towards compensation.
Thus,isc/erbelie"ed that a compensatory ad+ustment of facial
growth would occur after
orthodontics since there has been an interference in the
unfolding of the face. ;e continues4
Iery often the orthodontic forces are but an interlude in the
continuous de"elopment of the
face, and pre!treatment and post!treatment stability is a result
of an e-uilibrium between the
component parts of the dental! facial complex and in the random
and dynamic changes
occurring post! treatment, the denture must be protected or
retained during the acti"e period
of facial!dental growth changes or at least until cessation of
ma+or growth changes.
2c/wart@ reiterated this theme and described internal
oppositional forces or
electric effect that was beyond the control of the orthodontist.
1uring the posttreatment
period, 2c/wart@said #nternal and external forces playing on the
denture lead to %ero and
stability. #t is only a momentary static situation, because
growth and change is occurring and
the e-uilibrium that results must somehow anticipate and include
both growth and change to
insure stability.
#n direct contrast, !eorge !rieves (+33) belie"ed that the cause
of most
malocclusions was the forward translations of teeth /in
agreement with a similar proposal in
the earlier work of6. 2imms Wallace, +&-2 and that when
teeth ha"e been placed backward
and upright o"er basal bone they would be stable and hence ha"e
no need for retention.
lthough Tweedad"ocated placing teeth back and upright o"er basal
bone, he prescribed 8
years retention in most cases and e"en longer periods when
needed.
!eorge $nderson>s (+3&)obser"ations led him to the
conclusion that nothing was
stationary in the human masticatory field.
There has been stability worthy of the name in the de"eloping
masticatory field or in
the fully erupted denture, and that retention was not a minor
but a "ery serious matter and a
basic part of orthodontic therapy.
1uring this same period, the application of facial, +aw and body
muscular exercises
/myofunctional therapy2 with fixed appliances for successful
treatment and retention was
brought forth in a series of publications from '(68 to '(8'
by$l#red P. Rogers (+'+).
#n contrast, Dallas 5cCa"ley (+33)placed great emphasis on
maintaining canine
position, arch form, and width as related to functional +aw
mo"ements to achie"e
posttreatment stability.
>
-
8/10/2019 Ld retention and relapse
9/205
Retention and relapse in orthodontics
2tedman (+%+, +%-), in a comprehensi"e approach to retention,
referred to an
enlarged pharyngeal space, emotionally initiated mentalis or
mimetic muscle hypertension,
and anterior component of force of mandibular third molars
because of insufficient growth as
factors in bringing about undesirable posttreatment changes or
relapse.
2tedmanad"ocated the use of specially constructed, fixed and
remo"able retainers
and he may ha"e implied their long!range use when it was not the
case in his theoretical
statement4
:asting occlusal changes occur only in these particular patients
whose internal forces
ha"e changed in such a manner during treatment and retention as
to support those particular
teeth in the newly ac-uired positions, with new functional and
emotional habits.
Riedel>s (+%*)comprehensi"e re"iew of retention was a
forerunner of his subse-uent
')!year post!retention relapse studies and those of his graduate
students at the Ani"ersity of
$ashington in eattle. These and the multitude of postretention
relapse studies by others
report their extensi"eness, unpredictability, and se"erity, and
are the grim realities facing the
orthodontic clinician.
#n essence, these relapse tendencies were graphically described
by !raber (+%%)and
by9ing (+-3).
Iery often the characteristics of the malocclusions by which we
determine
classification seem to reoccur in an alarming degree
post!retention. Relapses of crowding,
rotations, mesio!distal relations, o"erbite, o"er+et and arch
width and form reappear
subse-uent to retention. There is no assurance that relapse will
not happen e"en when surgery
is combined with orthodontic treatment.
9ingdescribes the characteristics of post!retention relapse as
an o"erall slipping
back or dental changes, "ery much in agreement with !raber.
#n specific postretention relapse studies, attention has been
focused on the stability or
relapse of canines and molar width, mandibular arch form,
mandibular incisor crowding,
rotations, o"erbite and o"er+et, and the presence or absence of
mandibular third molars. #n all
these studies, extraction or nonextraction, there appears to be
sufficient unpredictability of
which cases will or will not relapse for all but a minority of
treatment procedures.
The relapse tendencies reported in the abo"e!mentioned studies
ha"e occurred with
treatment using what has been considered to be con"entional
orthodontic forces. #t is
(
-
8/10/2019 Ld retention and relapse
10/205
Retention and relapse in orthodontics
important to know whether there is a difference in the effect of
the orthopedic palate!splitting
forces reintroduced clinically byDeric/sweiler (+'%)and
continued by9ork/a"s (+%*)in
=ermany. oon after !raber and Haas reported clinical /extraoral
and palate! splitting2
studies, and Mc@amara reported experimental studies.
0xperimental and clinical reports on
the effect of high!pull orthopedic forces byWatson (+-&),
T/om=son (+-3), 4lder and
T"erge (+-3), Cleal (+-3), and Wislander (+-3)differ on the
extent of skeletal stability,
but show high agreement to the effect that dental instability or
relapse, especially mandibular
incisor changes following orthopedic forces, is consistent with
the continuing changes that
occur in con"entional force treatment.
There is a recent trend of orthodontists in the Anited tates to
report the use of
acti"ators andJor functional appliances, alone or as a
preliminary to a secondary period of
treatment, using a multibracketed fixed appliance. long with
this trend, there is also the
belief that the results will be more stable.
Reitan>s (+', +%%, +%-)microscopic studies of postretention
treatment changes
excited the orthodontic community worldwide. ;e demonstrated in
animal studies that the
supracrestal gingi"al fibers /collagenous2 appear histologically
taut and directionally
de"iated after tooth rotation, and that this condition did not
lessen e"en after years of
retention.
#n response to Reitan>swork, many surgical approaches with
experimental animals
and human sub+ects to control or lessen rotational relapse in
orthodontic treatment ha"e been
reported in the literature.
9ole (+')remo"ed the buccal and lingual cortical plates on human
patients before
initiating orthodontic mo"ement, somewhat reminiscent of the
septotomy of Talbot (+%)
and 2kogsborg (+&-). T/om=son (+') /repeated by Boese in
'(9(2 remo"ed all the
attached gingi"al tissue on experimental animals, lea"ing only
the mucosa surrounding
rotated teeth.
4dward>s (+-*) clinical orthodontic study was based on
Ba"er>s (+%1) thesis
describing mesial and distal incisions of transseptal fibers of
rotated teeth in experimental
animals and4dward>s own similar animal study /'(9>2.
')
-
8/10/2019 Ld retention and relapse
11/205
Retention and relapse in orthodontics
Parker (+-&),in a clinical study of transseptal fibers,
states4 Rotational relapse is a
normal, predictable, physiological response to abnormal forces ?
The paralleling of tooth
roots, discriminate transection of free gingi"al fibers and
ade-uate retention time are "ery
important and useful ad+uncts to stability in treated
orthodontic cases.
$ith the growing e"idence that the presence of intact
transseptal fibers was the ma+or
"illain in rotational relapse,9a=lan (+-%) undertook a natural
sur"ey of '))) orthodontists
to determine the extent of circumferential supracrestal
fiberotomy as an ad+unct to retention
procedures. ;e concluded4
$hile it appears that this surgical techni-ue is not widely
prescribed, it seems
reasonably problem free and its use will probably be increasing
in the future. D;e cautions,E
There are as yet no follow!up studies of the efficacy of this
treatment procedure.
5inally, 2c/acter and Bernick>s (+-3) conclusion, in an
experimental study on
nonhuman primates that their study did not answer the problem of
why certain rotations do
not occur e"en after surgical transection of the fibers must be
pertinent to all
aforementioned fiberotomy studies.
lmost in lieu of retention or in retreatment, there ha"e been
studies of stripping
either to pre"ent rerotation of the mandibular incisor or to
correct the relapse of the
mandibular incisors, followed with or without retaining
appliances. Kelston (+%)presented
a techni-ue for realignment with wires and ligatures after
stripping of crowded lower incisor
teeth. Paskow (+-*) reported self!alignment following
interproximal stripping of lower
incisors and was indefinite about retainers.Boesereported a
combined procedure of stripping
and circumferential supracrestal fiberotomy with no lower
retainer placed. #n his 7!( years
follow L up, he noted that the lower incisor segment did mo"e,
but mo"ed in a unit rather
than each tooth indi"idually. ;e concluded4
G5 and reproximation is not a guarantee for permanent ideal
lower anterior tooth
alignment, but was percei"ed as a useful process, which appears
to work within a framework
of natural changes that ine"itably will occur.
Williams (+'),in addition to stripping, added fi"e other
treatment keys, which he said
will eliminate the need for lower retainers, but he showed a
!year follow!up of one case.
These approaches and that ofPeck and Peck>s (+-&)
reproximation studies are seemingly
''
-
8/10/2019 Ld retention and relapse
12/205
Retention and relapse in orthodontics
based upon the theoretical concept of polished broad contact
areas described by Begg in
tone ge men. Begg made the deduction that it was the primiti"e
rough diet of the
ustralian aborigines that was responsible for well!aligned
teeth. On the other hand, it was
belie"ed that failure to achie"e polished broad contact areas
during and following orthodontic
treatment of modern ci"ili%ed man with a lack of comparable
attrition would re-uire a
techni-ue for realignment and stripping of crowded lower
incisors to pre"ent or correct
relapse.
Waldron (+3&) designed his retaining appliances on the basis
of the rationale of
-
8/10/2019 Ld retention and relapse
13/205
Retention and relapse in orthodontics
anterior hooks using latex elastics and a bite!plate, which
would permit the maxillary incisor
teeth to tip slightly labially.
Tweedreferred to a retrospecti"e study /8 years posttreatment2
on retention that he
had conducted on a follow!up group of his own patients
consisting of ')) extraction and '))
nonextraction cases. ;e said that in general while many patients
/had2 lo"ely faces teeth,
in others, the picture DwasE the opposite and that the
extraction cases seemed to be nicer
than nonextraction cases many years after treatment.
Tweedacknowledged that in his opinion abnormal muscle function
was a ma+or
factor in relapse e"en though he did not know how much one could
change muscle function
as a result of orthodontic procedure. @e"ertheless, he said he
would try to o"ercome the
per"erse muscle and tongue habits.
2and"sky (+3)reported a postretention relapse study /')!year
a"erage2 of >8 Tweed
treated cases!78 by Tweedhimself and 7) by Tweed #o"ndation
members.The mandibular
incisor relapse was shown to be -uite small less than ')N using
the :ittle index!but other
changes occurred, namely, forward mo"ement of lower incisors and
change of occlusal
plane.
t the same time,:ittle (+3)reported on a ')!year postretention
relapse study of
78) cumulati"e cases from the Ani"ersity of $ashington group at
eattle, led by Riedel.
:ittle showed that 99N of these cases exhibited mandibular
incisor relapse with no statistical
support of predictability of which cases would relapse and which
would remain stable.
Philosophies or schools of thought of retention
'6
-
8/10/2019 Ld retention and relapse
14/205
Retention and relapse in orthodontics
5or many years clinicians did not agree about the need for
retention. O"er the years,
different philosophies or schools of thought ha"e de"eloped in
regard to the retention and our
present!day concepts generally combine se"eral of these.H
1) The occlusion school:
9ingsley (+*) stated, The occlusion of the teeth is the most
potent factor in
determining the stability in a new position. Many early writers
considered that proper
occlusion was of primary importance in retention and has been
repeatedly stressed in the
literature (Reitan, 2c/"dy, 9a/l 8ieke). $nglebelie"ed that
permanency of treatment result
could be ensured by creating a normal occlusion with a full
complement of teeth, pro"ided
there was ade-uate retention and "igorous masticatory
function.
2) The apical base school:
#n the middle '()*s a second school of thought formed around the
writings of $0el
:"ndstrom,who suggested that the apical base was one of the most
important factors in the
correction of malocclusion and maintenance of a correct
occlusion. ;is clinical studies on
apical base did much to counteract the dominance of the
expansionists led by $ngle. ;e
stated that occlusal function alone could not control the form
and amount of apical base
rather the apical base is in largely capable of affecting the
dental occlusion.Dallas 5cCa"ley
(+33)placed great emphasis on maintaining canine position, arch
form and width as related
to functional +aw mo"ements to achie"e post treatment stability.
;e suggested that
intercanine width intermolar width should be maintained as
originally presented to
minimi%e retention problems. 2trangfurther enforced and
substantiated this theory. 8ance
(+3-) noted that, arch length may be permanently increased to a
limited extent. This
school of thought suggested that mandibular intercanine width
and intermolar width
dimensions show a strong tendency to relapse and should be
considered in"iolate.
3) The mandibular incisor school:
'7
-
8/10/2019 Ld retention and relapse
15/205
Retention and relapse in orthodontics
!eorge !rieves (+33) stated that cause of most malocclusions was
the forward
translation of teeth and that when teeth ha"e been placed
backward and upright o"er basal
bone they would be stable and hence ha"e no need for retention.
Tweed (+33,+'&) also
suggested that the mandibular incisors must be kept upright and
o"er the basal bone.
4) The musculature school:
$l#red P. Rogers (+&&) introduced a consideration of the
necessity of establishing
proper functional muscle balance. Other corroborated this
theory. 2trang (+'%) stated as
follows!The width as measured occurs from one canine to another
in the mandibular
denture, is an accurate index to the muscular balance inherent
to the indi"idual and dictates
the limits of the denture expansion in this area of treatment.
d"erse J abnormal muscle
acti"ity has been "ariously proposed by many authors including
Coleman, $ngle, Case,
2trange, Tweed, 2tedman andRogersas, if not the cause, then
atleast a ma+or contributing
factor of relapse.
Orthodontists ha"e come to reali%e that retention is not
separate from orthodontic
treatment but that it is part of treatment itself and must be
included in treatment planning.
tability has become a primary ob+ecti"e in orthodontic
treatment, for without it
either ideal function or ideal esthetics, or both, may be lost.
Retention depends on what is
accomplished during treatment. Gare must be exercised to
establish a proper occlusion within
the bounds of normal muscle balance and with careful regard to
the apical base or bases
a"ailable and the relationships of these bases to one
another.
Basic theorems of retentionH, >
'8
-
8/10/2019 Ld retention and relapse
16/205
Retention and relapse in orthodontics
Theorem 1: Teeth that hae been moed tend to return to their
former positions!
There is little agreement as to the reason for this tendency<
suggested influences
include musculature, apical base, transseptal fibers, and bone
morphology. $hate"er the
reason, there seems to be general agreement that teeth should be
held in their corrected
positions for some time after changes are made in their
positions. Only a few orthodontists
ha"e suggested that retention is routinely unnecessary. The
-uestion of why teeth ha"e a
tendency to return to their former positions has, to this date,
no real answer.
Theorem 2: "limination of the cause of malocclusion #ill preent
recurrence!
Antil more is known about the causati"e factors that are related
to particular types of
malocclusion, little can be done about their elimination.
Therefore, a proper diagnosis based
on determining the cause of the malocclusion is in"aluable.
$hen ob"ious habits such as thumb or finger sucking or lip
biting or tongue thrusting
are the causes of malocclusion, little difficulty is presented
in diagnosis of the determining
cause. Anfortunately many of our malocclusions appear with
apparently unknown origins or
at least origins about which we can do little. Gertainly
heredity plays a most important part in
determining the presence of many malocclusions. #t is important,
howe"er, in regard to
retention, that the causati"e factors for a gi"en malocclusion
be pre"ented for recurring.
Theorem 3: $alocclusion should be oercorrected as a safet%
factor!
Therefore, it is well to o"ercorrect the "arious malpositions
and malrelations of teeth
and +aws. #t is common practice on the part of many
orthodontists to o"ercorrect class ##
malocclusions into an edge!to!edge incisor relationship.
Orthodontists must be aware,
howe"er, that these o"ercorrections may be the result of
o"ercoming muscular balance rather
than absolute tooth mo"ement. The unrestricted use of class ##
elastics sometimes produces a
mesial displacement of the mandible, which is almost impossible
to detect until elastics ha"e
been discontinued long enough to allow normal mandibular
posture.
The same phenomenon may be seen in the use of class ### elastic
forces. The use of
elastics must be likened to the use of traction forces in
orthopedic surgery, in which muscular
forces are o"ercome by constant pull. ;owe"er, absolute
o"ercorrection is possible and has
'9
-
8/10/2019 Ld retention and relapse
17/205
Retention and relapse in orthodontics
been demonstrated in many instances. O"ercorrection of deep
o"erbite is an accepted
procedure in many practices.
Gertainly, satisfactory maintenance of o"erbite correction
depends on the
establishment of satisfactory correction during treatment.
One of the most irritating types of relapse is the tendency for
a pre"iously rotated
tooth to rotate towards its former position. :ittle e"idence is
a"ailable to show that
o"errotation has been carried out and there is e"en less
e"idence to indicate that such
o"errotation is successful in pre"enting the return to the
former position.
Theorem 4: Proper occlusion is a potent factor in holding teeth
in their corrected
positions!
n orthodontist should attempt to produce the best possible
occlusion of the teeth.
The influence of occlusion is a factor in retention which has
often been mentioned and
certainly the best possible occlusion is a factor in the
retention of corrected malocclusions.
$hether or not it is the most important factor is certainly
debatable. #n too many instances
we ha"e seen teeth, e"en with high cusps, locked into normal
occlusion that will still tend to
return to their former positions. #t is e"ident that many
orthodontists consider the denture
from a static "iewpoint, i.e., with the teeth in occlusion. The
functional relationships of teeth
are certainly important factors in retention and this has been
recently emphasi%ed by
numerous authors directing our efforts toward proper occlusal
e-uilibration. 5rom the
standpoint of reducing the potential of irritations to the
periodontium, an excellent functional
occlusion is certainly to be desired.
Orthodontists often blame o"erfunction or pounding of the
mandibular canines by the
maxillary canines as a cause of relapse in the mandibular
anterior area. The e"eryday
e"idence presented by the tremendous wear that may teeth undergo
would indicate that they
do not mo"e in response to repeated grinding and tapping until
the bone has either been so
thoroughly destroyed that it allows their migration, or until
fibrous tissue builds up to a
degree where it actually mo"es the teeth and function on these
teeth is actually not possible.
Gertainly instances of mandibular anterior irregularity or
collapse are common, in which
canines either ha"e not yet erupted or are not actually in
occlusion. @o doubt, we can say that
a perfectly normal denture functions best.
'H
-
8/10/2019 Ld retention and relapse
18/205
Retention and relapse in orthodontics
Theorem &: Bone and ad'acent tissues must be allo#ed to
reorgani(e around ne#l%
positioned teeth!
ome type of retaining appliance should be used either fixed and
rigid or an appliance
that is inhibitory in nature and not dependant on the teeth for
some length of time.
;istological e"idence indicates that both bone and tissue around
teeth which ha"e been
mo"ed by orthodontic appliances are altered and that
considerable time must elapse before
complete reorgani%ation occurs. ome authors ha"e indicated that
retainers should be fixed
and rigid such as$ngle, who suggested = wire, band and spur type
attachments, bands
soldered together etc. Others ha"e indicated that retainers
should only be inhibitory and ha"e
no positi"e fixation to allow for the natural functioning of
teeth. #t has been suggested that
the mandibular lingual arch admirably suits this
description.
-
8/10/2019 Ld retention and relapse
19/205
Retention and relapse in orthodontics
perpendicular to the mandibular plane, or a plus or minus 8 from
mandibular plane, or a
relation to occlusal plane, or 5rankfort hori%ontal plane. s to
what is basal bone, there is no
experimental e"idence to indicate that anyone can specify that
where this bone begins or
ends, and there seems to be no satisfactory method of measuring
it.
#t has sometimes been assumed that teeth that are upright are
also o"er basal bone.
;owe"er, in certain cases the roots of mandibular incisors ha"e
been mo"ed labially to a
considerable degree in the process of uprighting these teeth. #t
is significant that many
malocclusions present with mandibular incisors upright and o"er
basal bone, and yet these
teeth are both crowded and rotated. ;ence the teeth that
supposedly ha"e the attributes of
stability can actually be in a state of malocclusion.
5rom a purely mechanical standpoint a certain amount of "irtue
exists in inclining the
mandibular incisors slightly to the lingual. Those who ha"e set
mandibular anterior teeth
during fabrication of a diagnostic set up ha"e noted that if the
teeth are aligned with a labial
inclination, attempts to push them lingually results in
expansion in the canine area or collapse
of the teeth. On the other hand, if the anterior teeth are
inclined lingually, further pressure to
the lingual does not cause collapse, and tipping to the labial
only creates spacing. ;ence, if
we are to make any errors in positioning our mandibular incisor
teeth, it is probably well to
err in the direction of a lingual rather than a labial
inclination.
#f the patient is growing, the mandibular anterior segment may
exhibit a physiologic
migration in relation to the mandibular body in a distal
direction that is apart from the
orthodontic treatment. Mandibular arch form plays a more
important role in stable
mandibular tooth alignment than does the relati"e
antero!posterior relationship of mandibular
denture to base.
Theorem +: ,orrections carried out during periods of gro#th are
less likel% to relapse!
Therefore orthodontic treatment should be instituted at the
earliest possible age.
There seems to be little possible e"idence to substantiate this
statement< howe"er, it has a
good deal in its fa"or from a logical standpoint if
orthodontists are in any way able to
influence the growth and de"elopment of the maxilla andJor the
mandible. #t is certainly
logical to presume that the growth of maxilla or mandible can
only be influenced while the
indi"idual is growing and that once growth has been completed
this potential is no longer
'(
-
8/10/2019 Ld retention and relapse
20/205
Retention and relapse in orthodontics
a"ailable. $hen treatment depends on a retardation or change of
direction of growth,
treatment must be instituted early during periods of acti"e
growth.
0arly diagnosis and treatment planning appear to afford certain
ad"antages in long!
term stability. #nstitution of early treatment can pre"ent
progressi"e, irre"ersible tissue or
bony changes, maximi%e the use of growth and de"elopment with
concomitant tooth
eruption, allow interception of the malocclusion before
excessi"e dental and morphologic
compensations, and allow correction of skeletal malrelationships
while structures are
morphologically immature and more amenable to alteration.
Much has been said about the change in muscular balance
established by changing
the positions of teeth, which in turn will promote rather than
retard normal growth. $hether
malrelations in muscle balance ha"e as much influence on growth
and de"elopment as has
been supposed is "ery difficult to say. Ghanges in muscle
balance in a normal direction allow
for more normal de"elopment of the dentition< in relation to
retention, normal muscle balance
should allow for normal arch alignment.
$e can say here, howe"er, that where treatment depends on
retardation or change in
direction of growth such as is effected in headgear therapy,
treatment must be instituted
during a period of growth.
Theorem -: The further teeth hae been moed* the less likelihood
of relapse!
Thus, cases in which it has been necessary to mo"e teeth a great
distance are in need
of lesser retenti"e attention or it is desirable to mo"e teeth
farther in the process of
orthodontic treatment.
#t is possible that positioning far from the original
en"ironment will produce
e-uilibrium states permitting more satisfactory occlusions, but
the wisdom of this rule has
not yet been put to the test. 5or e.g.4 in bimaxillary
protrusions produced during orthodontic
treatment ha"e not shown a tendency to relapse inspite of the
fact that there is a pronounced
labial axial inclination of both maxillary and mandibular
incisor teeth. #t might well be that in
some of these cases the teeth are mo"ed far enough to be outside
of the influence of labial
musculature, actually there is little real e"idence to support
the statement that the farther
teeth ha"e been mo"ed the less relapse tendency they will ha"e.
#n fact, the opposite may be
true. #t may be more desirable through guidance of eruption and
early interception of skeletal
)
-
8/10/2019 Ld retention and relapse
21/205
Retention and relapse in orthodontics
dysplasias to minimi%e the need for future extensi"e tooth
mo"ement with the resultant
influence on the functional en"ironment and such local factors
as supracrestal fibers.
Theorem .: /rch form* particularl% in the mandibular arch*
cannot be permanentl%
altered b% appliance therap%!
Therefore, treatment should be aimed at maintaining, in most
instances, the arch form
presented by the original malocclusion as much as possible.
The e"idence brought to the author*s attention by8ance that
attempts to alter arch
form in the human dentition generally met with failure has been
accepted realistically by
most orthodontist. tudies of treated orthodontic cases out of
retention ha"e lent credence to
this type of thinking. #n '(77, 5cCa"ley made the following
statement4 ince these two
mandibular dimensions, molar width and canine width are of such
an uncompromising
nature, one might establish them as fixed -uantities and build
the arches around them.
2trangsaid essentially the same thing in '(794 # am firmly
con"inced that axiom of the
mandibular canine width may be stated as follows4 The width as
measured across from one
canine to the other in mandibular denture is an accurate index
to the muscular balance
inherent to the indi"idual and dictates the limits of denture
expansion in this area of
treatment.
e"eral instances of three or more millimeters of expansion of
intercanine width were
found, but in these instances mandibular canines had been
considerably constricted and were
blocked lingually to the general outline form in the mandibular
arch. Gertainly there are
exceptions to the rule of in"iolability of mandibular arch form
and intercanine width, but we
cannot expect all our patients to be exceptions. 0xtraction of
two mandibular incisors
sometimes satisfies the re-uirements of the arch form without
intercanine expansion /with
remo"al of two maxillary bicuspids2.
Of these theorems the following seem to be the most
important4
'2 Teeth do tend to mo"e back toward their former position62
'(coined a phrase Gountdown to Retention, which he ga"e
to describe the time when retention should begin. The countdown
begins when the patient*s
teeth ha"e been properly positioned L Gentric relation achie"ed,
roots at extraction sites
parallel, mandibular canine width not expanded, proper buccal
and labial tor-ue, normal
o"erbiteJo"er+et relationships, and Glass # relationships.
ny retention procedure before beginning should fulfill the
following criteria4
1) ,orrection and oercorrection of the /P 'a# relationship:
Gonsiderations of anteroposterior skeletal and dental
corrections are "ery essential
part of any appliance systems.
O"ercorrection of the Glass ## case is the greatest challenge in
this area. #f corrected
only to the desired end position, many Glass ## cases will show
a relapse of o"er+et and a
deepening of the bite. These patients benefit from
o"ercorrection to an edge!to!edge position
and maintenance of that position with nighttime Glass ##
elastics for 9 to > weeks, followed
by setting into an ideal Glass # relationship.)
2) "stablishing correct tip of the upper and lo#er anterior
teeth:
#t is necessary to establish correct tip of the upper and lower
anterior teeth at the end
of the treatment by mode of any appliance system. 5or all teeth,
the gingi"al portion of long
axis of each crown should be distal to the occlusal portion of
the long axis of each crown.)
3) "stablishing correct torue of the upper and lo#er anterior
teeth:
#t is often necessary to ad+ust the tor-ue in the upper and
lower anterior segments at
"arious stages of treatment.
>
-
8/10/2019 Ld retention and relapse
29/205
Retention and relapse in orthodontics
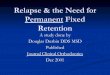
A. Moderate-to-severe Class II case before treatment. B. After
overjet reduction, torque
has been lost in upper anterior segment and lower incisors are
angulated forward. C.
Additional torque needed in archwires to recover correct incisor
angulation.
The most common example is during o"er+et correction of the
moderate!to!se"ere
Glass ## cases, when the tor-ue is fre-uently lost in the upper
anterior segment while the
lower incisors are angulated forward. #n this situation, it may
be necessary to compensate by
adding lingual root tor-ue to the upper anterior teeth and
labial root tor-ue to the lower
anteriors.)
4) ,oordinating arch #idths and archform:
Gareful coordination of archwires from the beginning of
treatment through the
rectangular wire phase will pre"ent unwanted and troublesome
crossbites from de"eloping. #f
the patient*s archwidths are not properly coordinated at the
start of treatment, this can be
compensated for by narrowing or widening the appropriate
archwires from the earliest stages
of treatment.)
A. Cross-elastics in cuspid areas used to
compensate for asmmetrical upper
archform !smmetrical arch indicated b dashed line". B.
Modi#ed upper
archform !dotted line"$ archwire canted in direction
opposite
to asmmetr.
&) "stablishing correct posterior cro#n torue:
(
-
8/10/2019 Ld retention and relapse
30/205
Retention and relapse in orthodontics
Gorrect posterior crown tor-ue is essential to pre"ent posterior
interferences from
de"eloping and to allow the seating of centric cusps. The tor-ue
built into pread+usted
posterior brackets usually eliminates the need for wire
bending.)
6)
-
8/10/2019 Ld retention and relapse
31/205
Retention and relapse in orthodontics
) "stablishing marginal ridge relationships and contact
points:
Marginal ridges of ad+acent teeth should be at the same le"el or
within ).8 mm of the
same le"el. Radiographically, the cementoenamel +unctions should
be at the same relati"e
height, resulting in a flat bone le"el between ad+acent
teeth.
Croper marginal ridge relationships in the finishing stage are
primarily a function of bracket
height. $ith the standard edgewise appliance, the most common
method of determining
bracket height in"ol"ed is by placing the brackets a specified
distance from the incisal or
occlusal surfaces of the teeth. The brackets were thus located
relati"ely more incisally or
occlusally on large teeth than on small teeth, which could
result in tor-ue or in!out errors.
A. Brac%ets placed &mm above incisal edges,
according to standard edgewise technique. 'ith (mm
central incisor !left", brac%et is )* percent of distance
up crown surface. 'ith +*mm central incisor !right",
brac%et is * percent of distance up crown surface. B.
ame teeth with brac%ets positioned in center of
clinical crowns, according to Andrews.
more reliable guideline is the center of the clinical crown, as
described by ndrews,
which pro"ides a consistent bracket position regardless of tooth
si%e.
#ncorrect bracket height becomes apparent early in the le"eling
and aligning stage of
treatment. ;ence, it is effecti"e to reposition brackets as
early as possible, so that time is not
wasted stepping archwires or repositioning brackets during the
finishing stage. )
A. pper central incisor with incorrect brac%et height and
compensating step
in ./+0 archwire. B. Brac%et repositioned at ne1t
appointment, with ./+)0 archwire.
6'
-
8/10/2019 Ld retention and relapse
32/205
Retention and relapse in orthodontics
+) ,orrection of midline discrepancies:
Most minor midline discrepancies of 6 mm or less can be
corrected with rectangular
wires in the finishing stage, whereas greater discrepancies
re-uire attention earlier in
treatment. There are fi"e methods of elastic wear for specific
situations4
/2 single class ## elastic on one side and a double class ##
elastic on the other, for cases
with a bilateral class ## component.
/B2 single class ## elastic on one side only, when the o"er+et
results in a slight class ##
relationship on that side and the opposite side is in a class #
position.
/G2 Glass ### elastics on one side and class ## elastics on the
other, for cases with the
corresponding dental relationships.
Methods of elastic wear to correct minor midline
discrepancies during #nishing stage. A. Case with
bilateral Class II component$ double Class II elastics on
right side, single Class II elastic on left. B. Case with
Class II molar relationship on right side and Class I on
left$ single Class II elastic on right side. C. Case with
Class II molar relationship on right side and Class III on
left$ corresponding interma1illar elastics.
/12 single class ### elastic on one side only, when that side is
in a class ### position and
the opposite side has a class # dental relationship.
/02 n anterior cross!elastic, when the discrepancy occurs
primarily in the anterior
segments.
2. Case with Class I dental relationship on
right side and Class III on left$ single Class III
6
-
8/10/2019 Ld retention and relapse
33/205
Retention and relapse in orthodontics
elastic on left side. 3. Case with discrepanc primaril in
anterior segment$ anterior
cross-elastic.
symmetrical elastics should be used for a minimum period of
time, and only with
rectangular archwires, because of their tendency to cant the
occlusal plane. The archwires
should be tied back while these elastics are worn so that the
wires do not slide around the
arch, causing unwanted space opening and distortion of the
archform.)
-) "stablishing the interdigitation of teeth:
Maximum intercuspation should be established between the buccal
cusps of the
mandibular posterior teeth and the lingual cusps of the
maxillary posterior teeth. 0ach
functional cusp should be in contact with the opposing arch.
$hen the rectangular wires ha"e been placed for a long period,
the teeth are often
unable to settle into an ideally finished position. #t is
helpful to allow each case to settle
before debonding by using a lower .)'7 round archwire and an
upper .)'7 round sectional
wire from lateral incisor to lateral incisor. This is
accompanied by "ertical triangular elastics.
4ertical triangular elastics used in settling phase before
debonding.
#f the teeth ha"e settled properly after two to four weeks, then
the patient can be
scheduled for debonding. #f the teeth are not properly
positioned, the patient can return to
hea"ier archwires for additional finishing.
The retainers will fit more properly after settling than if they
immediately follow
rectangular wires.)
66
-
8/10/2019 Ld retention and relapse
34/205
Retention and relapse in orthodontics
.) ,hecking cephalometric ob'ecties:
Crogress headfilms should be taken about halfway through
treatment to allow time for
reassessment of anchorage and possible changes in the di"ision
of treatment time. Taking a
headfilm in the end of treatment may be important for the
orthodontist*s education and for
e"aluating the success or failure of treatment, but it pro"ides
no practical ad"antage to the
patient.
#mportant factors to e"aluate with progress and final
cephalometric x!rays include the
anteroposterior position of the incisors, the incisor
angulations, changes in the occlusal plane,
the degree to which "ertical de"elopment has occurred or been
restricted, and the success of
the correction of hori%ontal and skeletal components of the
case. uperimposition of the
progress and final x!rays on the pretreatment x!ray will help
determine the orthodontic
changes that ha"e occurred.)
18) ,hecking the parallelism of the roots:
=enerally, the roots of the maxillary and mandibular teeth
should be parallel to each
other and perpendicular to the occlusal plane, as "iewed in the
panaromic radiograph. ;ence,
a panaromic x!ray should be taken before debanding to e"aluate
root parallelism. #f roots are
properly angulated, sufficient bone will be present between
ad+acent roots, an important
consideration in periodontal health. #f crown!root angulation is
beyond normal standards,
bracket repositioning or archwire bending may be re-uired to
modify the root positions.)
11) $aintaining the closure of all spaces:
ll spaces within the dental arches should be closed. #t is
important that space closure
be maintained, particularly in extraction cases, by using
passi"e tiebacks in the finishing
stage.
67
-
8/10/2019 Ld retention and relapse
35/205
Retention and relapse in orthodontics
Maintenance of lower arch space closure with passive wire
tiebac% between molar
brac%et and soldered archwire hoo%.
Otherwise, spaces fre-uently open during finishing and must be
reclosed. Open
spaces not only are unaesthetic, but also may lead to food
impaction.)
12) "aluating facial and profile esthetics:
0sthetic e"aluation is an ongoing process during all stages of
orthodontic treatment.
pro+ection of esthetic goals should be made as part of the
treatment plan. The facial and
profile esthetics can then be monitored clinically, as well as
with progress and final
cephalometric x!rays.)
13) ,hecking for T$9 d%sfunctions such as clicking and
locking:
TM3 dysfunction is a broad sub+ect and the following are some of
the recommendations
gi"en which a clinician should take into account4
/i2 1ocument any e"idence of TM3 dysfunction prior to treatment,
and inform the
patient that such symptoms exist.
/ii2 Monitor the patient for symptoms of TM3 dysfunction during
treatment. #f
problems are managed before the de"elopment of true internal
derangement, then
+oint function can often be re!established without permanent
damage with the help
of a short phase of splint and physical therapy, concurrent with
the orthodontic
treatment, until the symptoms are eliminated. ;eadgears and
elastic forces should
be stopped while managing the TM3 problems.
/iii2 Monitor the patient for symptoms of TM3 dysfunction during
retention. Taking
tomographic x!rays before treatment, as well as to 6 months
before debonding,
is helpful in detecting irregularities within the +oint and in
e"aluating the clinical
position of the condyle.
A. 5atient showing anterior
s%id with corresponding
anterior condlar position.
6eadgear or Class II
mechanics should be
68
-
8/10/2019 Ld retention and relapse
36/205
Retention and relapse in orthodontics
continued to eliminate anterior s%id and allow condle to seat in
fossa. B. 5atient
showing signi#cantl posterior condlar position with no evidence
of anterior s%id. light
amount of anterior s%id should be provided b ceasing headgear or
Class II
3lastics, or using Class III elastics, to achieve more centered
position
The orthodontic patients generally benefit from the
establishment of a seated and
reasonably concentric condylar position. forward or retruded
condyle can often be
corrected during the finishing stage, in con+unction with minor
changes in antero!posterior
and "ertical +aw position.)
14) ,hecking functional moements:
Before debonding, the patient should be checked for
interferences during protrusi"e
mo"ements and lateral excursions. #t is important that the lower
eight most anterior teeth
make contact with the upper six most anterior teeth during
protrusi"e mo"ements. This
normally re-uires a slight widening of the archform in the
bicuspid area, so that the mesial of
the lower bicuspids contacts the distal of the upper
cuspids.
#n lateral excursions, the patient should experience cuspid rise
with slight anterior
contact and disclusion of posterior teeth on both the working
and balancing sides. econd
molars should normally be banded to pre"ent interferences in
this critical area during lateral
excursions.)
1&) etermining if all habits hae been corrected:
;abits such as tongue thrusting will usually ha"e been corrected
before the finishing
stage is reached, because as the patient grows, airway si%e
increases and the tongue can
assume a more posterior position. lso, as the dental en"ironment
that that supported the
habit is impro"ed orthodontically, the tongue and lip
musculature adapt to the impro"ed
en"ironment and normal function begins to occur.)
1) ,orrection of rotations and oercorrection #here needed:
Most rotations will ha"e been eliminated before the finishing
stage, particularly if
force le"els are kept low. ny remaining rotations can be
corrected during finishing by one of
three methods4
69
-
8/10/2019 Ld retention and relapse
37/205
Retention and relapse in orthodontics
/i2 Rubber rotation wedges under the rectangular archwire.
/ii2 teiner rotation wedges L these are useful because they can
be placed after the
archwire is in position.
/iii2 :ingual elastics L most effecti"e method.
These rotations should be slightly o"ercorrected during
finishing to minimi%e relapse,
particularly in extraction cases.)
1+) "stablishing a relatiel% flat plane of occlusion:
Reasons for completing cases to a relati"ely flat occlusal plane
to a slight arc in the
second molar region, according to ndrews, include the proper fit
of the upper dentition
against the lower dentition. $hen a cur"e of spee is left in the
lower arch, for example, there
is a tendency towards increased o"er+et, since the lower teeth
occupy less room than the
opposing upper teeth. 1eep bite cases also benefit from
o"ercorrection of the cur"e of spee,
because most deep bites tend to relapse.
#f the occlusal planes are not le"eled before finishing and
detailing, the archwires will
not slide easily through the bracket slots during space closure
with sliding mechanics.)
6H
-
8/10/2019 Ld retention and relapse
38/205
Retention and relapse in orthodontics
uration of retention
;ow long should the orthodontist continue retention& The
answer to this -uestion
"aries from not at all to fore"er. The answer also depends on
the type of case treated, the ageof the patient, what the parent
and the patient expect of the orthodontic treatment, all of the
limitations inherent in the case, and finally, what the
orthodontist himself expects of his
treatment. #n the a"erage adolescent, when considerable growth
and remodeling of the bony
en"ironment can be expected, it is reasonable to expect that
retention should logically be
continued until the effect of these changes has slowed down.
=enerally, this occurs at the
time the third molars erupt< hence it has been a rule for
many to continue retention until these
teeth ha"e erupted or ha"e been remo"ed.'
o, to conclude some form of retention will probably be
maintained until e"idence of
completion of growth is forthcoming, and consideration should be
gi"en to the use of
retainers on and as needed basis indefinitely to ensure
maintenance of tooth relationships. #t
should be4'
0ssentially full!time for the first 6 to 7 months, except that
the retainers not only can
but should be remo"ed while eating /unless periodontal bone loss
or other special
circumstances re-uire permanent splinting2.
Gontinued on a part!time basis for at least ' months, to allow
time for remodeling of
gingi"al tissues.
#f significant growth remains, continued part!time until
completion of growth.
5or practical purposes this means that nearly all patients
treated in the early
permanent dentition will re-uire retention of incisor alignment
until the late teens, and in
those with skeletal disproportions initially, part!time use of a
functional appliance or
extraoral force probably will be needed.
6>
-
8/10/2019 Ld retention and relapse
39/205
Retention and relapse in orthodontics
Ph%siologic recoer% or relapse
5or a successful result to an orthodontic experience, retention
must be anticipated and
planned as a "ery important part of treatment of the dentition
rather than as an apatheticallyundertaken aftermath or necessary
e"il to the patient and orthodontist alike, which would
otherwise lead to a relapse process.
#n orthodontics it is important to differentiate between relapse
and normal
de"elopmental changes in order to resol"e our responsibilities
during retention.
Relapse is a return of detrimental features of the original
malocclusion< while
de"elopmental changes refer to the indi"idual*s maturation
process. To make this distinction,
we should ha"e a general understanding of growth, de"elopment,
maturation to old age,
response to treatment techni-ues, and those factors necessary
for an impro"ed or healthier
dentofacial en"ironment.
;orowit% and ;ixson', suggested that the term relapse should be
replaced by the
term physiologic reco"ery as the dentition continuously changes
throughout life. Biologically
these changes represent a reco"ery and rebound of indi"idual
dental de"elopment pattern.
=rowth and remodeling are =erman factors of physiologic
ad+ustments after acti"e
treatment< this remodeling ne"er stops, but the balance
between apposition and resorption
change with ageing. #n addition to physiologic reco"ery, normal
growth changes must be
included as contributing to continuous adaptation process that
sustains the long!term stability
of dental apparatus.
malocclusion represents nature*s best effort to approach balance
under the handicap
of asymmetric parts and disharmony. #t is as stable as the
existing balance between muscle
and bone but can change until growth and maturation, +ust as in
normal occlusion.
To establish an esthetically harmonious, functionally efficient
and structurally balanced
dental arches in the area of functional tolerance "arious
cardinal points like establishment of
proper static functional occlusion, archform and intercanine
width maintenance, lower
incisors positioning, proper understanding of growth and
de"elopment etc are "ery important.
Iiolation of the law of optimality is likely to re+ect the
alteration imposed on an existing
orofacial en"ironment leading to relapse.
6(
-
8/10/2019 Ld retention and relapse
40/205
Retention and relapse in orthodontics
,auses of orthodontic relapse
The complexity of the dento!maxillofacial organ, the marked
changes that ha"e taken
place in its en"ironment since the time it e"ol"ed to its
present form, and many otherinfluences L some of them understood
and others not understood L contribute to instability of
the end results of acti"e orthodontic appliance therapy.
mong the goals of orthodontic treatment beyond facial and dental
aesthetics,
function, and the health and longe"ity of the dentition is the
achie"ement of stable or
relati"ely stable results. The reality of our present knowledge
is that no form of treatment
guarantees absolute stability, nor does a well!treated case
treated by the highest standards by
itself assure stability.
tability is not an absolute, and what one tries to do for a
patient is to obtain
acceptable stability. The concept of acceptable stability is not
an alibi for treatment but
recognition of biological limitations. The success of our
treatment should be measured based
upon some type of ratio between the magnitude of patient
impro"ement and the relapse.
uccess index')P Magnitude of #mpro"ement
Magnitude of Relapse
5ear of relapse is "ery real to most orthodontists and some are
affected to a degree
that causes them to institute retention ad infinitum to all
treated cases without regard to
indi"idual conditions.
$hy do successfully treated malocclusions fail& The sub+ect
of failure is as "ast as
the field of orthodontics itself. #n fact, e"ery time we as
orthodontist undertake to treat a
malocclusion we assume that the odds fa"or success but the
possibility of failure, if not total,
exists in some degree.6
,auses of relapse:
The tendency of the teeth to undergo change of position
immediately upon the
remo"al of the orthodontic appliances can be attributed to
"arious factors like bone changes,
periodontal ligament tension, general metabolism, endocrine
dysfunction, functional
adaptation of occlusion, inherent growth, tooth!si%e
discrepancies, axial inclinations, soft
tissue maturation, connecti"e tissue changes and interference
with the tra+ectorial forces
7)
-
8/10/2019 Ld retention and relapse
41/205
Retention and relapse in orthodontics
established in function. $hen the aforementioned factors react
fa"orably, the changes on
completion of treatment actually may help as time elapses to
produce better esthetic tooth
arrangement and occlusion.
1);ate mandibular gro#th:
:ate mandibular growth may result in increased pressure at the
front of the mouth.
Typically, the mandible grows and displaces forward at a faster
rate than the maxilla
/measured to occlusal plane2 and the lower basal bone more than
al"eolar bone. Tooth
compensations include the tendency of the lower incisors to mo"e
lingually. #f the
mandibular incisors are not free to mo"e forward because of the
restraining influence of the
upper arch, it is likely that they will become retroclined and,
could be a contributing factor to
crowding in the lower anterior region. ;owe"er, no direct
relationship between the increase
in crowding and the change in incisor inclination or position
has been demonstrated.
:undstrom7examined 8 pairs of twins between the ages of ' and '8
years and 6 and 9
years. ;e found no relationship between anterior growth of
gnathion and increased crowding,
or between changes in lower incisor inclination and increased
crowding.
Richardson7measured changes in lower incisor inclination and
position of the incisal
edge relati"e to the maxillary plane in 8' sub+ects with intact
lower arches. Between the ages
of '6 and '> years, the a"erage change was proclination of
+ust o"er ' with forward
mo"ement of '.) mm. #ncisor inclination was measured on the most
procumbent lower
incisor. s contacts slip to permit imbrication, one or more
incisors may procline as the
others retrocline in response to increased lingually directed
force. This may mask any
relationship between increased crowding and incisor
angulation.
3)
-
8/10/2019 Ld retention and relapse
42/205
Retention and relapse in orthodontics
remains stable in most cases, increase in labial segment
crowding is often associated with
dentoal"eolar adaptation. Mesial drift of buccal teeth
contributes to the de"elopment of labial
segment crowding. Many causes of mesial drift ha"e been
postulated, including the anterior
component of force, tensions in the supra!al"eolar connecti"e
tissues and impactions of third
molars.8
@anda and @anda9 found that the pubertal growth spurt for
patients with skeletal
deep bite occurs on a"erage '.8 to years later than is the case
for open bite cases. 5or this
reason, a longer retention period for the skeletal deep bite
patients is ad"ocated to counteract
the continuing effect of dentofacial growth after the completion
of orthodontic treatment.
4) $andibular incisor dimensions5 Tooth structure:
Growding is slightly more common in persons whose teeth ha"e
large mesiodistal
dimensions than in those with smaller teeth. mall but
statistically significant correlations
between crowding and tooth width ha"e been found by some. Others
found nonsignificant
correlations between these "ariables.
@o direct relationship has been established between an increase
in lower arch
crowding and tooth structure. #t might be argued that teeth with
large labiolingual dimensions
and broader contacts would be more stable and less likely to
slip under pressure or tension.
The notation that mandibular incisor dimensions were correlated
with lower incisor
crowding was reintroduced by Ceck and Ceck9, H after a study of
78 untreated normal
occlusions. They concluded that the ratio of mesiodistal /M12 to
faciolingual /5:2
dimensions of lower incisors was an important factor in
producing well!aligned mandibular
incisors. ;ence, they ad"ocated reduction of mandibular incisors
to a gi"en faciolingualJ
mesiodistal ratio to increase stability. Ceck and Ceck*s work,
howe"er, was critici%ed for the
following reasons. Their recommendations were based on a study
in"ol"ing untreated rather
than treated cases. Qoung patients with ideal lower incisor
alignment were used in the study.
#t is possible that these cases would show crowding if followed
long term.
To e"aluate whether the Ceck and Ceck ratio had long!term "alue,
=illmore and
:ittle9, H studied '67 treated and control cases a minimum of ')
years presentation. They
showed a weak association between long!term irregularity and
either incisor width or the
faciolingualJmesiodistal ratio. :ess than 9N of crowding can be
explained by this ratio. #n
7
-
8/10/2019 Ld retention and relapse
43/205
Retention and relapse in orthodontics
addition, the actual mean difference in incisor widths between
crowded and uncrowded cases
was only ).8 mm.
mith et al.7found nonsignificant correlations between crowding
and labiolingual
incisor width in ')) untreated orthodontic sub+ects and '))
untreated adults, and low
significant correlations between crowding and
mesiodistalJlabiolingual incisor ratio.
Cunky et al.7found nonsignificant correlations between
labiolingual lower incisor
dimensions, or their labiolingualJ mesiodistal ratio and lower
arch alignment in HH treated
cases or >9 untreated adult malocclusions.
=len et al.7could find no relationship between
mesiodistalJlabiolingual ratio and
incisor irregularity in > nonextraction orthodontically
treated cases, either before treatment
or 6 years after!retention.
0"idence from these studies suggests that tooth structure plays
only a minor role /if
any2 in the etiology of late mandibular incisor crowding.
Boese>, ( introduced a concept of lower incisor reproximation
to pro"ide broader
contact points and increase the a"ailable arch space in the
mandibular anterior region. ;e did
a retrospecti"e study that in"ol"ed continued inter"ention
during the retention period, e"en in
the presence of minor relapse. ;ence, we are unable to compare
the results of this study with
results from other retention studies.
&) =cclusal factors:
The attachment apparatus of all teeth is an effecti"e
hydrodynamic damping system,
like an automobile shock absorber, and is well!designed to
withstand occlusal forces. #f teeth
did reposition themsel"es in response to occlusal forces, it
would not be necessary for
dentists to be so careful with occlusal relationships. The teeth
would make minor corrections
for themsel"es. This does happen +ust after the completion of
orthodontic treatment, when the
teeth are hypermobile and the attachment apparatus is
reorgani%ing. lterations in functional
occlusion may produce a different pattern of masticatory forces
or an occlusion with
premature contacts. The importance of functional and stable
occlusion posttreatment is
repeatedly stressed in the literature.
Brodie7suggested that with each stroke of mastication, the upper
incisors recei"e a
separating impulse, whereas the lowers tend to come into closer
contact. This implies
76
-
8/10/2019 Ld retention and relapse
44/205
Retention and relapse in orthodontics
retroclination of lower incisors. The principle may also be
applied to indi"idual teeth coming
into premature contact, being displaced by the force of
occlusion, and allowing ad+acent teeth
to mo"e toward each other, thus creating a crowded situation.
Ganine guidance in lateral
excursion may cause a lingually directed force on lower canines,
with a reduction of inter!
canine width.
On the other hand, Croffit7pointed out that the supporting
structures of the teeth are
designed to withstand hea"y, short acting, forces, such as those
of occlusion. @e"ertheless, it
seems possible that these forces, in combination with other
factors, may contribute to tooth
mo"ement and crowding. Carafunctional acti"ity could exacerbate
this phenomenon.
Occlusal relations may be altered by orthodontic treatment of
the upper arch. 1ifferent types
of upper arch treatment may ha"e differing effects on the lower
arch.
:ombardi7 suggested that there may be a relationship between
o"ercorrection of
maxillary canines and mandibular incisor crowding.
Occlusal changes may also be caused by restorations, tooth loss
with drifting, or the
de"elopment of grinding habits.
de-uate interincisal contact angle may pre"ent o"erbite relapse
and good posterior
intercuspation pre"ents relapse of both crossbite and
anteroposterior correction. :ess relapse
of mesiodistal mo"ement occurs in the absence of occlusal
stress.
) Influence of the elements of the original malocclusion:
The most basic cause of relapse to occur is the persistence of
the elements of original
malocclusion or the etiology. #f the underlying etiology is not
remo"ed, the treatment is
destined to relapse. #t is mandatory for all clinicians to first
diagnose a case properly, and
plan the treatment and retention initially itself, keeping the
etiology in mind. The remo"al of
the etiologic factor before finishing is mandatory.
O"erbite increase postretention is related to the amount reduced
during treatment,
although generally 6)N to 8)N of the correction is retained. #t
is suggested that o"erbite
relapse tends to occur in the first years posttreatment and
maintenance of the intercanine
width is thought to increase stability. #n the anterior open
bite correction e"aluated in 7'
patients, 7)N showed marked relapse and the other 9)N showed
stability of the result. The
relapse subgroup showed a greater increase in lower anterior
face height during the
77
-
8/10/2019 Ld retention and relapse
45/205
Retention and relapse in orthodontics
postretention period than did the stable group, but no
posttreatment "ariable could be used to
predict posttreatment relapse or stability.
Most studies do not support a greater relapse in class ##
di"ision ' cases when
compared with other malocclusion groups, howe"er, a slight
change in o"er+et toward
pretreatment "alues was demonstrated in all malocclusion groups.
:abially inclined incisors
pretreatment tend to be associated with less long!term crowding.
#t is postulated that the
weaker labial muscular forces do not induce lingual mo"ement of
the dentition and
subse-uent arch length shortening.
$hen teeth are aligned by orthodontic treatment, there is a
documented tendency for
a return toward the original pattern of malocclusion. 5or this
reason, rotational o"ercorrection
has been ad"ocated. :ittle et al., howe"er, note that there are
many exceptions to this rule
with greater than 8)N of the rotations or displacements
relapsing in an opposite direction. 9
Adhe et al.'7formed a multiple regression analysis of o"er+et,
o"erbite, intercanine
width, and intermolar width changes. They re"ealed that 7'N of
late lower incisor crowding
could be explained by these "ariables. The relati"e contribution
by these "ariables "aries
between indi"iduals with a similar degree of irregularity.
+) /lteration of arch form:
#t is generally agreed that arch form and width should be
maintained during
orthodontic treatment.H, 9 #n certain cases, where arch
de"elopment has occurred under
ad"erse en"ironmental conditions, arch expansion as a treatment
goal may be tolerated.
There is e"idence to show that intercanine and intermolar width
decreases during the
postretention period, especially if expanded during treatment
/mott, rnold, $elch, and
others2. 5or this reason, the maintenance of arch form rather
than arch de"elopment is
generally recommended. 0xpansion is thought to be better
tolerated in class ## di"ision
cases that show a significantly greater ability to maintain
intercanine expansion than class #
and class ## di"ision ' cases. This statement, howe"er, was
based on a sample of 9 patients
and was not accepted by :ittle et al6)who maintained that
intercanine and intermolar width
will relapse if expanded in class ## di"ision cases as much as
in other ngle classifications.
nother exception to the maintenance of arch width may be found
in cases of
mandibular expansion concurrent with rapid palatal expansion.
;aas6'and andstrom et al.6
78
-
8/10/2019 Ld retention and relapse
46/205
Retention and relapse in orthodontics
found that maintenance of 6 to 7 mm intercanine width and up to
9 mm intermolar width was
possible when expansion was carried out concurrently with
maxillary apical base expansion.
These two studies, howe"er, are -uite misleading. ;aas study was
based on ') cases and
primary canines were present in the initial records for two of
these. ;ence, one cannot
extrapolate on the amount of canine expansion achie"ed, when in
)N of this small sample,
the permanent canines were not present at the time of the
original records. andstrom*s
statement that mandibular incisor stability is increased when
the mandibular intercanine
width is expanded in con+unction with maxillary expansion is
based on a sample of 'H
patients only years postretention.
Moussa et al.66reported on a sample of 88 patients who had
undergone rapid palatal
expansion in con+unction with edgewise mechanotherapy a minimum
of > years
postretention. Their results showed good stability for upper
intercanine and upper and lower
intermolar widths. tability of the mandibular intercanine width,
howe"er, was poor with the
posttreatment position closely approximating the pretreatment
dimension.
1e :a Gru% et al.67 carried out a ')!year postretention study on
>H patients to
determine the long!term stability of orthodontically induced
changes in maxillary and
mandibular arch form. The results showed that although there was
considerable indi"idual
"ariability, arch form tended to return toward the pretreatment
shape. They concluded that the
patient*s pretreatment arch form appeared to be the best guide
to future stability.
-) Periodontal forces:
#n series of experiments on monkeys, Cicton and Moss 7and
Cicton7demonstrated
that the teeth are +oined together by a system of transeptal
fibers under tension.
Croffit7claimed that a slight imbalance of force between the
tongue on one side and
the lips and cheeks on the other is normally present. ;e
suggested that the teeth are stabili%ed
against this slight imbalance by forces produced in the
periodontal membrane by acti"e
metabolism.
outhard et al.7demonstrated the presence of a continuous
periodontal force on the
mandibular dentition, acting to maintain proximal contacts in a
state of compression. This
force was increased after occlusal loading. They found
significant correlations between
79
-
8/10/2019 Ld retention and relapse
47/205
Retention and relapse in orthodontics
interproximal force and mandibular anterior malalignment. They
concluded that periodontal
forces could contribute to the de"elopment of late lower arch
crowding.
.) Periodontal and gingial tissues:
Orthodontic tooth mo"ement to correct tooth rotations is
proposed to result in
stretching of the collagen fibers. These stretched fibers
/transeptalJcollagen2 ha"e been
implicated in rotational relapse by pulling the teeth back
toward their pretreatment position.68,
69
Brain and 0dwards9ad"ocated gingi"al fiber surgery
/Gircumferential upracrestal
5iberotomy2 to allow for the release of soft tissue tension and
reattachment of the fibers in a
passi"e orientation after orthodontic tooth rotation.
The theory of stretched collagen fibers as the cause of
rotational relapse has recently
been -uestioned by Redlich et al.6Hwho analy%ed gingi"al tissue
samples obtained from
rotated incisors in dog. They found that the rotational forces
caused significant changes in the
integrity and spatial arrangement of the gingi"al tissues,
changes that are inconsistent with
stretching. fter fiberotomy, reorgani%ation of the fibers
similar to the control group was
e"ident. They concluded that the rotational relapse may actually
originate in the elastic
properties of the whole gingi"al tissue rather than stretching
of the gingi"al fibers as
pre"iously belie"ed.
18) >oft tissue maturation:
#t is generally accepted that dentoal"eolar structures are
responsi"e to soft tissue
pressures and adapt to a position of balance between the muscles
of the lips, cheeks and
tongue.
5rankel and :offler7showed that the reduction in mandibular arch
length found in an
untreated control group was pre"ented in sub+ects treated with
the functional regulator /5R2
appliance. They claimed that the "estibular shields of the
functional regulator appliance
fa"orably influence the saggital de"elopment of the mandibular
dental arch by eliminating
the restraining forces of the external muscular en"ironment.
$oodside et al.7and :inder!ronson and $oodside7showed that the
lower incisors
of children who were mouth breathers were more retroclined and
crowded compared with
7H
-
8/10/2019 Ld retention and relapse
48/205
Retention and relapse in orthodontics
controls, and proclined after adenoidectomy and a changed mode
of breathing that altered the
muscular en"ironment.
These studies show that lower arch alignment can impro"e after
the remo"al of
ad"erse muscular forces and, although no direct relationship has
been found between changes
in soft tissue forces and increased lower arch crowding, it is
likely that such changes may
ad"ersely affect arrangement of the teeth.
:ate mandibular growth changes may bring the lower incisors into
a different soft
tissue en"ironment.
ubtently and akuda7compared 8 patients who were orthodontically
treated and
de"eloped late lower incisor crowding with 8 patients who did
not. They found a strong
tendency to maintain the original intercanine width in all
cases. The crowded cases had a
narrower intercanine width before treatment, which returned to
its original dimension after
treatment expansion. They surmised that the lip musculature did
not permit the necessary
intercanine expansion to maintain incisor alignment. They
claimed as the mandible increases
in si%e, the lips exert greater pressure than the tongue,
creating a lingually directed force that,
counteracted the mesial forces, causes incisor crowding.
Bench7 studied growth of the cer"ical "ertebrae, hyoid bone, and
tongue in relation to
the facial skeleton and denture. ;e found that the hyoid bone
and tongue descend with age,
relati"e to surrounding structures, and continue to do so after
facial growth slows down. ;e
claimed that this was particularly true in persons with long
faces and with lack of forward
growth and suggested that it could explain the de"elopment of
late lower arch crowding.
Gohen and Iig7studied tongue growth on serial cephalograms of 8)
sub+ects from
ages 7 to ) years. They found that tongue si%e relati"e to the
intermaxillary space increased
with age. This might imply more forward pressure on lower teeth.
They pointed out that the
descent of the tongue, as it grows, may compensate for any
possible increase in forward
pressure because of larger tongue si%e.
Iig and Gohen7examined lip growth on the same sample and found
that it continued
up to '( years and exceeded growth of anterior lower face
height.
#n a longitudinal study of










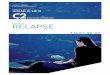

![RETENTION LECTURE 5-30-04.ppt [Read-Only] LECTURE_BW...1 RETENTION RELAPSE AND THE OCCURANCE OF MALOCCLUSION From Riolo, M. and Avery, J. Eds., Essentials for Orthodontic Practice,](https://img.pdfslide.net/doc/110x75/5acf1ae97f8b9ae2138c1e64/retention-lecture-5-30-04ppt-read-only-lecturebw1-retention-relapse-and-the.jpg)